 Caroline Billings
Caroline Billings David E. Anderson
David E. Anderson
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Vet. Sci., 26 April 2022
Sec. Comparative and Clinical Medicine
Volume 9 - 2022 | https://doi.org/10.3389/fvets.2022.879630
This article is part of the Research TopicThe Use of Large Animal Models to Improve Pre-Clinical Translational ResearchView all 13 articles
Osteomyelitis is an inflammatory bone disease typically caused by infectious microorganisms, often bacteria, which causes progressive bone destruction and loss. The most common bacteria associated with chronic osteomyelitis is Staphylococcus aureus. The incidence of osteomyelitis in the United States is estimated to be upwards of 50,000 cases annually and places a significant burden upon the healthcare system. There are three general categories of osteomyelitis: hematogenous; secondary to spread from a contiguous focus of infection, often from trauma or implanted medical devices and materials; and secondary to vascular disease, often a result of diabetic foot ulcers. Independent of the route of infection, osteomyelitis is often challenging to diagnose and treat, and the effect on the patient's quality of life is significant. Therapy for osteomyelitis varies based on category and clinical variables in each case. Therapeutic strategies are typically reliant upon protracted antimicrobial therapy and surgical interventions. Therapy is most successful when intensive and initiated early, although infection may recur months to years later. Also, treatment is accompanied by risks such as systemic toxicity, selection for antimicrobial drug resistance from prolonged antimicrobial use, and loss of form or function of the affected area due to radical surgical debridement or implant removal. The challenges of diagnosis and successful treatment, as well as the negative impacts on patient's quality of life, exemplify the need for improved strategies to combat bacterial osteomyelitis. There are many in vitro and in vivo investigations aimed toward better understanding of the pathophysiology of bacterial osteomyelitis, as well as improved diagnostic and therapeutic strategies. Here, we review the role of animal models utilized for the study of bacterial osteomyelitis and their critically important role in understanding and improving the management of bacterial osteomyelitis.
Osteomyelitis is an inflammatory bone disease that results in progressive bone destruction and bone loss and is typically caused by infectious microorganisms (1–4). The most common causative organisms are bacteria (1), specifically Gram-positive Staphylococci such as Staphylococcus aureus (S. aureus) (1–3, 5–8). There are three main etiologies of osteomyelitis: hematogenous, trauma or surgery associated, and secondary to vascular disease. Hematogenous osteomyelitis is most common among pediatric patients (5, 7, 8). Injury associated osteomyelitis may be spread from a contiguous focus of infection, may be secondary to trauma, or may be associated with surgery, especially where implanted medical devices are used. This may occur in individuals of any age (2, 3, 5–7). Osteomyelitis also commonly occurs secondary to vascular insufficiency and is often a result of diabetic foot ulcers (DFU) (2, 6, 7). The annual incidence rate of osteomyelitis in the United States is not precisely known. In 1999, the incidence was reported to be as high as one out of every 675 hospital admissions, which translates to approximately 50,000 cases annually (9). Since that time, the incidence of osteomyelitis cases of all categories has been increasing (8). The rise in caseload is partially due to increases in cases of diabetes (8), trauma (10), numbers of reconstructive orthopedic procedures and implanted prosthetic materials (6, 11–13), and also may be associated with improvements in diagnosis (2).
Clinical presentation of patients suffering from osteomyelitis is variable. Acute osteomyelitis may present with fever, redness, pain and draining lesions. Symptoms of chronic osteomyelitis may be vague, with a wide array of clinical features which may be as subtle as simple focal swelling and tenderness on physical examination (2, 6, 7, 11, 14, 15). Nonspecific clinical presentation necessitates a thorough patient workup for successful diagnosis (16). Diagnostic testing often includes physical examination, hematology and biochemistry panels, measurement of C-reactive protein (CRP), culture and sensitivity testing of bone and wound samples, and imaging such as radiographs and ultrasound. Radiographic evidence of boney changes lag behind pathologic changes, so early disease may not be apparent on standard radiographs (7, 11, 17). Advanced imaging can be helpful, and magnetic resonance imaging (MRI) or computed tomography (CT) (1, 11, 16) may be required. Despite the abundance of available tests that may be employed, there are few early pathognomonic findings for osteomyelitis (7, 18, 19). Therefore, while osteomyelitis may be suspected, the gold standard of diagnosis requires a bone biopsy for culture (2, 5, 11, 18–20) and histopathologic examination (7, 11, 18–21).
Osteomyelitis results in significant morbidity and mortality to the patient (6, 10, 14, 22, 23), and expedient, intensive treatment is indicated. The most common clinical approach to treatment of bacterial osteomyelitis involves a combination of medical and surgical management (4, 6, 11, 18, 24, 25). Systemic antibiotic therapy should be guided by microbial cultures whenever possible (11). In the absence of culture and sensitivity results, empirical, broad-spectrum antibiotics are usually administered (4, 5, 18). Antimicrobial therapy is typically administered for a minimum of 4–6 weeks (2, 19, 20, 24, 26) and is often continued for longer periods of time in an attempt to mitigate risks of chronic osteomyelitis (20). Some clinicians advocate treatment for up to six months after diagnosis (19, 20, 26). Local antibiotic therapy may be instituted to complement systemic antimicrobial therapy (27). Surgical debridement of affected tissue is routine treatment in conjunction with medical management (2, 15, 18, 19). A hallmark of osteomyelitis is the presence of necrotic bone (2, 6, 15), which is readily colonized and surrounded by biofilm (11, 28). Biofilms often result in persistence of bacterial infection. Persistence is multifactorial and is partially due to the protective slime matrix that provides a physical barrier between immune cells and bacterial cells (6, 11, 14) and can impair diffusion of antibacterial substances (29). Persistence also results from the physiologic environment of biofilms, which allows for enhanced antimicrobial resistance through creation and persistence of immense phenotypic diversity, including metabolically inactive bacteria and subpopulations of “persisters” or phenotypically resistant bacteria (30–33). Debridement of necrotic bone should be thorough, with the goal of reaching healthy, viable tissue and removing sources of biofilm. This often includes removing implanted hardware (2, 5). While this approach sounds straightforward and reasonable to accomplish, there are many challenges in the treatment of osteomyelitis which often leave patients suffering relapses or struggling with chronic infections (11, 34–36). Particular challenges include inadequate debridement (2, 15, 19, 30), metabolically inactive bacteria or bacteria embedded in biofilm (2, 12, 30), inadequate antimicrobial penetration to infected tissues (37), antimicrobial resistant bacterial species (2, 25), and loss of tissue or organ function to the patient during treatment (12, 38). Challenges are augmented by the negative impact of treatment on patient quality of life (25), increased risk of bacterial infection upon hardware reimplantation (39), and the ability of S. aureus to evade the host immune system (30, 40).
Bacterial osteomyelitis has a progressively increasing incidence, and it is important to reduce morbidity and mortality to patients while concurrently reducing the burden on the healthcare system (11). Continued improvements in the understanding, diagnosis, and therapy of bacterial osteomyelitis are necessary to accomplish these goals. As a result of variable patient population, case presentation and disease management, clinical osteomyelitis research has proven difficult (38). A major step in achieving improved diagnostic and therapeutic methods lies within animal modeling of this disease. In vivo models facilitate groundbreaking research by allowing scientists to expand upon promising in vitro discoveries and utilize research findings to improve the lives of patients suffering from osteomyelitis. Ultimately, animal models promise to speed advances in modern medicine. The purpose of this review is to highlight a range of animal models used to study bacterial osteomyelitis. While it is not possible to present all of the features for each individual model, this review will emphasize the limitations and benefits of the most common animal models used to investigate the pathogenesis, diagnostic methods, and therapeutic strategies to better understand and combat bacterial osteomyelitis.
There are many approaches to inducing bacterial osteomyelitis in animal models. This review will focus on two main categories of bacterial osteomyelitis induction: surgical and hematogenous.
Authors have chosen to exclude detailed discussion of in vivo modeling of osteomyelitis secondary to DFU. There are reports of modeling bacterial infection with diabetic rodent strains, however, osteomyelitis resulting from DFU is a multifactorial, chronic condition and the complexity of modeling and translational healing differences raise concerns regarding reliable in vivo models (41–44). To surgically induce bacterial osteomyelitis in any species, there are a few necessary components. An injury to bone tissue (45) is required, and typically stems from mechanical trauma with or without the addition of a sclerosing agent (22, 46). A foreign body or medical device may be used to serve as a nidus for bacterial colonization (47). Bacterial inoculation is necessary and may be accomplished via direct administration of a bacterial inoculum (48), soaking of a foreign object or hardware in a bacterial suspension, creating a biofilm on a piece of hardware for implantation (49), or by intravenous (IV) administration of bacterial suspension (hematogenous seeding) (50). Many investigators choose to seal the bone defect, e.g. using sterile bone wax to ensure local containment of the bacteria and minimize undesired concomitant soft tissue infections (51). Induction of hematogenous bacterial osteomyelitis typically carries the advantage no required surgical manipulations or placement of foreign materials (52, 53). Hematogenous models are designed to closely mimic the acute hematogenous osteomyelitis that most commonly occurs in pediatric patients (52, 54).
Within these two categories, many differences exist in model design. Differences include the type of bone injury and surgical approach, bacterial strain and colony forming unit (CFU) count, administration vehicle and quantity of bacterial inoculum, as well as length of study and monitoring techniques. It is crucial to consider the bacterial species and strain that will be utilized in animal modeling. During initial model establishment, it is recommended to utilize a bacterial strain with well documented behavior within the chosen animal species. After confirming that osteomyelitis can be established in the selected model, the bacterial species, strain, dose, and even delivery vehicle may be altered to best accomplish the research objectives. On that token, investigators should consider the species-specificity, antimicrobial sensitivity profile, and clinical relevance of the chosen pathogen. These pillars of model development are highlighted by Laratta et al. (55) and commented on by Johansen et al. (56). Markers of success within model development typically include clinical manifestation of disease, evidence of osteomyelitis on histopathology, and positive bone cultures upon study completion. Most investigators elect to pulverize bone samples and perform bacterial culture from the pulverized samples. Confirmation of bacterial cultures using polymerase chain reaction (PCR) has become routine since the method was described in 1999 (54).
There are many surgical models of bacterial osteomyelitis performed in murine models. Models typically utilize long bones, although alternatives such as vertebral models are also reported (57). An extensive review of murine models, including the goal, method, and bacterial inoculum used in each study, was recently published by Guarch-Pérez et al. (58). One approach used by multiple investigators was described in 2008 as a model to assess intramedullary response to titanium particles (59). This surgical approach is accomplished by creating a medial parapatellar arthrotomy to access the femur. Once accessed, a defect extending to the medullary cavity of the femur is created. Kirschner wire (K-wire) is inserted into the femoral medullary canal and penetrated into the patellofemoral joint space. Bacterial inoculation occurs via direct application of a bacterial suspension and the surgical site is closed (48, 60, 61). This model was recently adapted and modified to model shoulder implant infections (62). In this study, investigators were able to reliably induce bacterial osteomyelitis using a bioluminescent strain of S. aureus and were able to track infection with radiographs and bioluminescent imaging (BLI). Another surgical approach that is utilized in various forms by many investigators is described well by Funao et al. (63). Much of this approach is similar to that described above; the distal portion of the femur is exposed surgically, and a 0.5 mm drill hole is created to expose the medullary canal of the femur. Rather than placing an implant, bioluminescent S. aureus is inoculated directly into the defect. The defect is then sealed with bone wax and the surgical site is closed. Another unique model of murine bacterial osteomyelitis is the hematogenous model described by Horst et al. (52). This model does not involve surgical manipulation or placement of foreign material. Instead, mice received one injection of S. aureus in phosphate-buffered saline (PBS) via the lateral tail vein. This model was created to closely mimic both acute and chronic hematogenous bacterial osteomyelitis and is unique in that it does not require additional bone injury. These approaches highlight the various methods available to induce bacterial osteomyelitis and the subtleties between the various models.
While arguably each investigation into bacterial osteomyelitis provides information on pathogenesis, there are experiments designed to evaluate specific questions regarding the pathogenesis of bacterial osteomyelitis (64). One such experiment, described by De Mesy Bentley et al. (65), utilized two murine long bone infection models and captured groundbreaking transmission electron microscopy (TEM) images of S. aureus invading and residing within the osteocyte lacuno-canalicular network (OLCN) of live bone. Staphylococcus aureus cells are thought to be protected while within the canaliculi system, as immune cells are likely too large to successfully access this area of the body. Therefore, these findings offer insight into the ability of S. aureus to evade the host immune system and cause latent and recurrent osteomyelitis. Zoller et al. (40), established and utilized a murine model of bulk allograft infection to expand upon the findings of de Mesy Bentley et al. by investigating the mechanisms of immune system evasion by S. aureus, specifically microarchitecture of implant surfaces as a potential factor in increased bacterial colonization. Staphylococcus aureus was discovered within allograft cortical haversian canals and submicron canaliculi within the native mouse femur. Results indicated that bulk allograft implant material was more susceptible to bacterial infection even at low bacterial inoculums compared to stainless steel implants. This finding suggests that implant microarchitecture is incredibly important and may offer bacteria a submicron reservoir to evade clearance by the immune system. The work of Masters et al. (66) expanded upon these findings by investigating the role of S. aureus cell wall synthesis machinery and surface adhesins in OLCN invasion. The authors established a model of bacterial osteomyelitis by placing stainless steel pins inoculated with various mutant strains of S. aureus into the medial tibia of mice. Results showed significant changes in OLCN invasion, abscess formation and pathogenic bone loss with the deletions of penicillin binding protein 3 and 4 (PBP3, PBP4) and autolysin (Atl), indicating that cell wall synthesis machinery can modulate S. aureus' pathogenesis in osteomyelitis.
While there are multiple reports of utilizing BLI and in vivo micro-CT in murine models (63, 67, 68), these reports are often geared toward improving the in vivo modeling system rather than improving diagnostic capabilities for clinical patients (63). Recently, however, Isogai et al. (69) performed plasma metabolome analysis in a model of murine osteomyelitis caused by S. aureus and identified 12 metabolites as candidate positive biomarkers and two candidate negative biomarkers for osteomyelitis. Novel plasma biomarkers are aimed to improve the early diagnosis of osteomyelitis. Improvement in the early diagnosis of osteomyelitis is of great interest, as there are currently many challenges in obtaining a swift and specific diagnosis in clinical patients.
A major goal of in vivo osteomyelitis work is to evaluate novel treatment strategies and investigate potential efficacy for clinical use. There are many investigations focused on various combinations or applications of antibiotics for clearance of osteomyelitis (48, 70–72). Jørgensen et al. modeled the particularly challenging situation of biofilm presence upon orthopedic implants. They investigated the efficacy of rifampicin-containing combinations of antimicrobials compared with non-rifampicin-containing combinations of antimicrobials in reducing bacterial counts or clearing infection. Results indicated that combinations of antimicrobials that included rifampicin, as well as the combination of daptomycin and linezolid, were more effective in reducing bacterial burden than combinations not containing rifampicin (70). There are also many investigations into novel therapeutics (73–75). Wang et al. utilized a model of S. aureus hematogenous orthopedic implant infection to identify specific virulence factors to be translated into therapeutic targets. This work identified two key pathogenic factors, anti-α-toxin (AT) and anti-clumping factor A (ClfA) and demonstrated markedly improved efficacy in infection treatment utilizing human anti-AT/anti-ClfA combination therapy (50). Similarly, Yokogawa et al. (76) created a novel murine one-stage revision model of methicillin-resistant S. aureus (MRSA) implant-associated osteomyelitis. This model facilitated discovery of synergistic activity of vancomycin and anti-glucosaminidase (Gmd). Identification of alternative therapeutics is important, as medical device implantation continues to increase and antimicrobial resistance (AMR) is becoming increasingly prevalent.
Murine models are particularly helpful to researchers investigating bacterial osteomyelitis. Main attractions of the mouse model include the small size, economics, and genetic and molecular tools that are available to tailor murine strains and facilitate a wide array of investigations. Indeed, mouse strain selection is of paramount importance as strains contain significant differences from one another. Investigators should consider the primary research objective of the model to guide strain selection and ensure research objectives can be accomplished appropriately. This pillar of model development is highlighted nicely by Dworsky et al. (57). These advantages make mice attractive for investigations into pathogenesis and proof of concept models (58, 72). Also, mice allow for certain longitudinal monitoring techniques, such as BLI and in vivo microCT. Longitudinal monitoring is an asset that adds strength and clarity to data collection as individuals can be compared to themselves over multiple timepoints. While mice can mimic the human inflammatory response of osteomyelitis (58), their bone structure and bone remodeling process is less similar to humans than other animal models provide (77). As a result of the mouse's small size, complex and multi-stage surgical procedures are not impossible, but are challenging to perform. This small size also prohibits the investigation and translation of implants intended for human use. Additionally, serial blood collection is limited by volume and frequency. When considering the benefits and limitations of murine models, it can be concluded that mice are an excellent tool for early investigations from in vitro to in vivo modeling and proof of concept work.
Rats provide a variety of models that produce well-characterized and reliable bacterial osteomyelitis. Significant historical developments have previously been described (36, 64, 78, 79). Currently, the most popular rat models are of long bone osteomyelitis and most often utilize the tibia (17, 22, 80–83) or femur (84–90). Long bone models rely on mechanical trauma, placement of foreign bodies, or creation of fractures, all typically with concurrent sealing of the defect area with bone wax to contain bacterial inoculums and prevent concomitant soft tissue infection. Alternative models include mandibular models (91), vertebral models (92), joint prosthesis models (93), and hematogenous models (94, 95). Hematogenous models required additional surgical manipulations to successfully establish osteomyelitis. This may be a result of the rat's ability to respond to acute infection, which can rapidly clear peripheral infection and may complicate infection models (78). Although reports of rat osteomyelitis models exist, a comprehensive review of these models is lacking. In this review, we present a detailed summary of rat osteomyelitis models that were utilized to inform this review (Table 1).
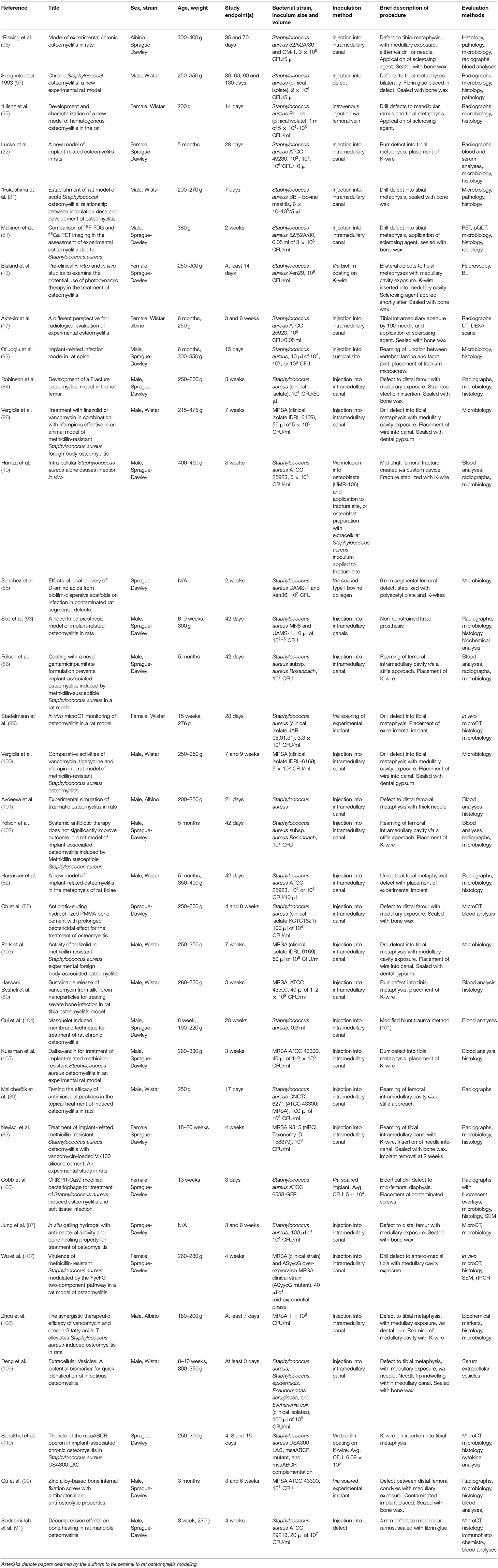
Table 1. Rat models of osteomyelitis.
Similar to murine models, rat models can be utilized for investigations into pathogenesis. Rat models have facilitated valuable discoveries, including investigations of virulence factors associated with S. aureus biofilms and the ability of S. aureus to function as an intracellular pathogen. Biofilms are well recognized as a source of recalcitrant bacteria that can impair antibiotic treatment of osteomyelitis and cause persistent or recurrent osteomyelitis, particularly when orthopedic implants are in place (13, 31, 111). Two studies that have pursued the in vivo investigation of biofilm virulence factors and genetic components in rats include the investigation by Wu et al. (107), which demonstrated that overexpression of ASyycG led to a reduction in biofilm formation and in vivo pathogenicity of MRSA in a model of rat tibial osteomyelitis; as well as the investigation by Sahukhal et al. (110) who utilized a model of implant-associated osteomyelitis. This investigation demonstrated that deletion of the msaABCR operon of S. aureus (USA300 LAC) resulted in defective biofilm production and reduced severity of bacterial osteomyelitis. The capability of S. aureus to function as an intracellular pathogen is considered to be a mechanism of immune system evasion and a source of recurrent, persistent osteomyelitis (31) and is supported by in vitro evidence (112, 113). Based on that in vitro evidence, Hamza et al. investigated and confirmed the ability of purely intracellular S. aureus to induce osteomyelitis in a rat model (10).
Similar to murine models, rat models have allowed for improvements in diagnostic or longitudinal monitoring capabilities in experimental models. Examples of these improvements include the findings of Stadelmann et al. (99), who demonstrated the use of in vivo microCT to longitudinally monitor bacterial osteomyelitis in a rat tibial model, thus offering a method to limit numbers of animals needed for experiments and to add strength to collected data. Also, Aktekin et al. evaluated the utility of available scoring systems for the radiographic evaluation of experimental osteomyelitis. Authors utilized a tibial model of osteomyelitis and evaluated serial radiographs throughout their study period, ultimately concluding that it is best to evaluate and report each radiograph individually, rather than appointing a numerical grade from a previously published grading scale (17). This is a valuable report for experimental studies, and with appropriate radiographic interpretation, is likely to add strength to radiograph assessments. An improvement to in vivo studies that holds potential to translate into human medicine is the investigation into various tracers for positron emission tomography (PET) to successfully image osteomyelitis and differentiate between bone infection and bone healing (51). The work investigating PET tracers indicated that Gallium-68 (68Ga), did not accumulate in healing bone, only infected bone. This work brings interest to the use of 68Ga and PET for clinical patients, although further work is needed to clarify use and safety concerns. Another interesting foray into improving diagnostics for clinical patients was completed by Deng et al. who described the potential use of extracellular vesicles (EVs) as a diagnostic marker for acute osteomyelitis (109).
Rats are recognized to be more resilient than mice and therefore are well suited to investigations into therapeutic strategies, such as antibiotic trials. Indeed, there are many investigations into antibiotic therapies. These include therapeutic efficacy assessments of systemic antibiotics administered solo or in combination (98, 100, 103, 105), investigations of local antibiotic delivery systems (80, 83, 88) and antibiotics in combination with alternative therapies such as omega-3 fatty acid supplementation (108). There also are investigations into novel therapeutic strategies such as the use of photodynamic therapy (PDT) to treat contaminated orthopedic implants and minimize reliance on antibiotic therapy to clear implant associated bacterial osteomyelitis (13). Recently, Cobb et al. (106) investigated the feasibility of utilizing a bacteriophage to mitigate bacterial osteomyelitis, biofilm, and soft tissue infection.
Rat models are a valuable animal resource in the study of osteomyelitis. They provide similar benefits to mice, including small size, economics, ease of housing and handling, and well-characterized strains that provide appropriate uniformity and enable study of disease pathophysiology relevant to that seen in people (97). Rats have the ability to tolerate sustained, high dose antibiotic therapy (97). While larger than mice, rats remain too small for assessment of orthopedic hardware for human use, and multi-step revision procedures, although not impossible, remain challenging. Uniquely, the rat is one of few ideal species for modeling of mandibular osteomyelitis (91, 95) because of their size, anatomy, and general hardiness. Therefore, the strength of rat models lies within the ability to investigate pathogenesis and pursue initial investigations into therapeutic strategies to further understand in vitro data and gain in vivo knowledge prior to utilizing a larger animal model.
Rabbits provide many useful and reliable models of bacterial osteomyelitis. The systematic review by Reizner et al. (78) details significant historical developments and the review by Bottagisio et al. provides a thorough overview of model development and utility (114). Historically and currently, the most utilized models are long bone models, including tibial (115–121), femoral (49, 122–124), and radial (125–129). Alternative models such as joint prostheses (130, 131), mandibular defects (132), vertebral models (133–136) and implant infection via hematogenous seeding (137) exist. Induction of osteomyelitis among these various models can be accomplished via mechanical trauma, either defect (117) or fracture (49) creation and bacterial contamination with or without application of a sclerosing agent or foreign body placement (115), or through placement of contaminated implants (49, 129). Bone wax may be used to seal defect areas and prevent bacterial leakage and concomitant soft tissue infection (116). A benefit of rabbits compared to smaller models such as mice and rats is the improved ability to model chronic osteomyelitis (138) and perform revision procedures such as debridement (23, 116), which improves the capabilities of modeling human osteomyelitis and therapy. Rabbits offer a distinct advantage in studying bone disease because full segmental defects of the radius can be created without the need to stabilize the bone using orthopedic implants.
Majority of reports into pathogenesis utilize well-characterized and reproducible rabbit models and are related to the capabilities of various bacterial species and strains (117, 121, 128) to induce osteomyelitis, as opposed to mechanistic work that more often is performed in murine and rat models. For example, Gahukamble et al. (117) describe an investigation into the abilities of Staphylococcus lugdunensis (S. lugdunensis) and Propionibacterium acnes (P. acnes) to establish osteomyelitis in a model that was previously characterized with a strain of S. aureus isolated from an infected human hip prosthesis (139). Results indicated that both organisms could induce osteomyelitis and described varying severity and clinical presentation. This work again emphasizes the importance of considering model development and bacterial strain selection during experimental design.
Similar to murine and rodent models, there are studies aimed to improve the longitudinal monitoring of experimental osteomyelitis in rabbit models (21, 115) to improve utility of animal modeling and reduce required animal numbers. Odekerken et al., demonstrated that 18F-FDG micro-PET is a sensitive diagnostic tool for detecting early bone pathology, including early osteomyelitis (21), even in the presence of titanium implants (118). This method of imaging could differentiate between aseptic and infected bone as early as three weeks post-operatively and post-infection. Authors suggest that 18F-FDG PET carries potential as an early detector of clinical osteomyelitis cases, which is further confirmed by a retrospective analysis of clinical osteomyelitis cases performed by Wenter et al. (140). An important investigation geared toward improving available diagnostics was performed in a rabbit model of chronic osteomyelitis. In this study, the capability of PCR to return positive results was compared with traditional osteomyelitis diagnosis via radiographs and bacterial cultures of bone biopsies taken via different methods. Results indicated that PCR was a sensitive diagnostic tool and described techniques to determine species identification (23). It deserves recognition that while PCR is a strong tool to detect low bacterial burdens or metabolically inactive bacteria that may not yield positive bacterial culture, PCR results will not provide antibiotic susceptibility data. The described PCR techniques are useful for experimental models and also offer utility for clinical cases.
Rabbits are widely utilized to test therapeutic strategies for the clearance of bacterial osteomyelitis. Rabbits are hindgut fermenters, which means that they may process oral antibiotics differently than humans (64). Nonetheless, rabbits have been widely utilized for evaluation of systemic and locally delivered antibiotic therapies (114, 123, 141). Rabbits also are a useful modeling system for evaluation of antibacterial coatings upon implants and local drug delivery systems (114, 129), as demonstrated by the use of silver ion doped calcium phosphate beads (120). There have also been investigations into alternative therapies for osteomyelitis, including the work performed by Kishor et al., investigating the use of bacteriophages to clear chronic osteomyelitis (142). In this study, S. aureus specific phages were purified, characterized, and utilized as a therapeutic in a model of acute and chronic femoral osteomyelitis. High doses of phage cocktail were found to be effective to clear S. aureus infection. This work presents an intriguing consideration for specific therapy of bacterial osteomyelitis. Another interesting study investigated the use of locally applied ozonated oxygen in a rabbit femoral model. While this treatment did not eliminate osteomyelitis, it did seem to lessen the clinical and radiographic markers of disease (122).
Rabbits fill a unique niche in in vivo osteomyelitis research. They are often utilized when the research goal involves assessment of orthopedic hardware or locally applied therapeutics and a small animal is needed, whether that need is dictated by animal housing limitations or by stage of research development. Rabbits provide a more relevant size to evaluate some human orthopedic implants, as well as an appropriate size to be maintained long-term so that revision procedures can be performed. Rabbits also provide a more similar immune system and long bone density to humans than mice and rats provide (143, 144). Despite these benefits, rabbit models are accompanied by more complex challenges including respiratory depression under anesthesia, hindgut fermentation, which impacts the ability to assess oral antibiotic therapies, and variation in bone healing response of young rabbits compared to humans. Most rabbit modeling should be performed in mature rabbits to maximize translation of results to clinical patients.
Pigs are not as widely utilized to model bacterial osteomyelitis, but the models that are available are effective, well-characterized, and have seen logical progression. Studies may utilize either mini-pigs or commercial pigs. Perhaps the most widely utilized model of porcine osteomyelitis is a hematogenous model (56, 145–149). Alternative models include mandibular osteomyelitis (46, 150), tibial implant-related osteomyelitis (151–154), and traumatic tibial osteomyelitis (155). When the hematogenous model of osteomyelitis was initially introduced, an inoculum of S. aureus (S54F9) was administered IV through a lateral ear vein without any additional trauma. This IV inoculation resulted in acute, suppurative pneumonic and osteomyelitic lesions. Lesions of osteomyelitis were found primarily in the long bones, but also in the costochondral junctions of ribs (147). This model has been modified and is most frequently used by administering bacterial inoculums into the femoral artery (145, 146, 148, 149). Femoral artery inoculation is reliable in inducing osteomyelitis localized to the injected limb. This technique may produce concurrent soft tissue infections, injection site abscesses, and the degree of disease during the study may be variable (148, 156). However, this remains a strong technique for modeling acute hematogenous (juvenile) osteomyelitis.
Pigs have not been utilized as widely as mice and rats to investigate pathogenesis of osteomyelitis, but there are a few interesting reports. One such study was carried out in a hematogenous model of osteomyelitis to determine the infection potential and disease characterization of three different strains of S. aureus (56). This work compared the typically utilized strain of porcine S. aureus (SF549) with two human strains of S. aureus (UAMS-1 and NCTC-8325-4). Results indicated that UAMS-1 and NCTC-8325-4 were less successful in establishing osteomyelitis than the porcine specific strain. Authors hypothesize that this may be due to increased host specificity, in contrast to rodent models, and that inoculation dose may play a role, which again brings attention to the importance of model and bacterial strain selection during experimental design. Additionally, an interesting discovery of biofilm within bone lesions shortly after infection was made and raises the concern that biofilms may form quite early on in disease. Jødal et al. investigated blood perfusion using [15O]water PET, and confirmed their hypothesis that blood perfusion would be increased in osteomyelitis-diseased bone as compared to healthy bone. While blood perfusion was increased in diseased bone as compared to healthy bone, blood perfusion was four-fold greater in areas of soft tissue infection than diseased bone (156).
Afzelius et al. (149, 157) have made multiple investigations involving ideal tracing agents for diagnosing osteomyelitis. They investigated the use of more specific radiotracers, including: 68Ga-labeled DOTA-K-A9, DOTA-GSGK-A11, [18F]NaF, [68Ga]Ga Ubiquicidin, and [68Ga]Ga-DOTA-Siglec-9, and compared them to the use of [18F]FDG. This study demonstrated no accumulation of the more specific radiotracers, but positive accumulation of [18F]FDG (149). Investigators also compared [99mTc]Interleukin-8 (IL-8) scintigraphy with [18F]FDG PET/CT in a hematogenous porcine model of osteomyelitis and found that [99mTc]IL-8 was simple to prepare and use, and that it was capable of detecting 70% of lesions compared with 100% sensitivity of [18F]FDG PET/CT. This makes [99mTc]IL-8 scintigraphy a promising candidate for further investigation for use in children, to decrease the radiation exposure, as compared to utilizing [18F]FDG PET/CT (157). Another interesting study was performed by Lüthje et al., who investigated the regulation of various acute phase proteins during osteomyelitis and found a significant pro-inflammatory local response to osteomyelitis, with limited systemic response. These findings confirm that osteomyelitis remains challenging to diagnose based on systemic findings and adds to the understanding that local investigation is necessary (153).
Most porcine studies thus far have been accomplishing model development, pharmacokinetic work (152) and diagnostic methods. There is even one investigation into bone regeneration techniques in the face of osteomyelitis (46). Hill et al. (155) completed a study utilizing tibial implant-associated osteomyelitis and found that they could prevent osteomyelitis by administering combination antibiotic therapy every 6 h for 7 days. Jensen et al. (154) comment that pigs provide an ideal model for investigation into implant surface coatings, medical and surgical treatment regimes, and vaccination against S. aureus.
Pigs, particularly mini-pigs, offer many benefits, including size that is appropriate for complex or multi-stage procedures and for assessments of orthopedic hardware for human use. Porcine bone possesses similar fracture stress to human bone (158), hematogenous modeling creates a very similar situation to juvenile hematogenous osteomyelitis, and the gastrointestinal system of pigs is appropriate to receive oral antibiotics. There are many challenges when using pig models, including rapid growth and excessive mature body weight when utilizing commercial pigs (159), shorter long bones than found in people (154), the greater expense associated with a large animal model, variation in degree of disease manifestation, as well as a generally fractious demeanor. Porcine models are not currently as widely utilized as small animal models of osteomyelitis but provide an ideal model for the study of hematogenous osteomyelitis, offer great capabilities into investigation of imaging techniques, and are an area of interest for further development in the modeling of osteomyelitis. In general, commercial pigs are suitable for proof of concept and model development work, as they are less expensive than mini-pigs, but for longer-term studies and more appropriate translational work, mini-pigs should be utilized.
Kaarsemaker et al. (160) initiated development of ovine models of osteomyelitis via creation of a tibial defect and subsequent bacterial inoculum injection into the medullary cavity of adult sheep. This study provided valuable information, including the ability to establish osteomyelitis in sheep and also the requirement for peri-operative systemic antibiotics to lessen the risk of fatal sepsis. Since then, a variety of long bone models have been developed, focused on the tibia (161, 162) or the femur (163), and often involving hardware infected with biofilm or planktonic bacteria (164) with or without revision procedures (162, 165). There remain a variety of techniques of creating bone injury, from unicortical defects and medullary canal inoculation (165) to osteotomies stabilized with experimental hardware (166). Recently, Moriarty et al. (162) established a model to replicate a failed two-stage revision procedure utilizing a MRSA infected intramedullary nail. This will likely be a valuable model to evaluate therapeutic strategies moving forward.
Most investigations into therapeutics in ovine models have been centered upon experimental implants, systemic or local antibiotic therapies, and the ability to replicate the multi-stage revision procedures utilized in human medicine. There have been multiple investigations into local drug delivery devices to clear osteomyelitis. Boot et al. performed a multi-stage revision procedure and compared an injectable hydrogel impregnated with gentamicin and vancomycin to an antibiotic-loaded bone cement impregnated with gentamicin and vancomycin. Investigators were able to clear significantly more cases of osteomyelitis in the experimental hydrogel group, compared to the bone cement group, thereby presenting this material as a promising candidate for further exploration (165). Stewart et al. investigated another concept in local drug delivery by creating a vancomycin-modified titanium plate that demonstrated decreased clinical signs of infection, prevented biofilm formation and promoted bone healing in an infected tibial osteotomy model (166).
Currently, sheep are most often utilized for investigations into therapeutics utilizing long bone models. As such, sections regarding pathogenesis and diagnostic innovations were not included. Regardless, sheep are a valuable animal resource for the modeling of bacterial osteomyelitis, particularly focused on long bones. Sheep provide an ideal long bone size to perform complex procedures, replicate the treatment strategies utilized in clinical cases such as multiple revision procedures, and assess orthopedic hardware and devices for human use. Many characteristics of ovine bone are similar to that of humans, including torsional stiffness and osteogenesis (64), which adds to the strength of ovine modeling. Challenges associated with ovine modeling include the risk of sepsis, which may require peri-operative antibiotics, as well as the cost of housing and maintaining a large animal.
Most caprine models of osteomyelitis utilize the tibia, although models have variable approaches. Salgado et al. described a unicortical tibial defect with concurrent application of a sclerosing agent. Staphylococcus aureus was inoculated into the medullary canal and the defect was sealed with bone wax. In this model, goats received a perioperative dose of IV antibiotics. Induction of osteomyelitis was successful and no goats suffered from fatal sepsis (167). In an adaptation of this model, the sclerosing agent and perioperative antibiotics were omitted, and osteomyelitis was successfully induced, again with no reported sepsis (168). Other tibial models include the internal fixation of a tibial osteotomy (169) and percutaneous pin placement throughout the tibia (170). Through these investigations, researchers have also proposed histology scoring systems, to aid in the evaluation of model development (169).
Similar to sheep, goats serve as viable translational models for investigations into therapeutic strategies. Wenke et al. utilized a similar model to that of Salgado et al. to investigate the efficacy of tobramycin-loaded calcium sulfate pellets compared to the efficacy of tobramycin-loaded antibiotic beads to treat bacterial osteomyelitis. Calcium sulfate and bone cement formulations loaded with tobramycin performed well, raising interest into the use of calcium sulfates for local drug delivery, as they do not require an additional procedure for removal (168). Tran et al. (169) investigated a silver-based antibacterial coating on intramedullary nails. In an experiment utilizing two goats, the goat that received the experimental implant displayed less severe signs of osteomyelitis than the control goat. An interesting experiment was performed to investigate the utility of a directly applied electric current to eliminate osteomyelitis over the course of 3 weeks. Authors found that electric currents were able to prevent signs of infection and suggest that this would be effective in clinical situations (170). Salgado et al. also reported an investigation of muscle vs. non-muscle flaps for reconstruction of defects and effective clearance of osteomyelitis. This study was designed as a result of discrepancies in the literature, with some reports of muscle flaps being superior and vice versa. This study found no difference between muscle and non-muscle flaps and re-emphasized that the most critical factor in treatment of bacterial osteomyelitis is thorough debridement (38).
Similar to sheep, goats possess great utility in modeling bacterial osteomyelitis, and this utility lies primarily within the size and composition of the caprine long bones, specifically the tibia. Long bone size and composition makes goats ideal for complex procedures and multi-stage surgeries. Goats provide an excellent model for assessment of orthopedic hardware intended for human use, as well as examination of local drug delivery devices and experimental coatings. Goats have not suffered from the reported sepsis that affected sheep when receiving intramedullary bacterial inoculation, which may aid researchers when selecting either sheep or goats as a model. Similar to any large animal model, goats are accompanied by greater costs than small animal models. As the majority of caprine modeling has been performed to either establish a reliable model or assess treatment options, the sections for pathogenesis and diagnostic investigations were omitted.
Canine models have been used in the past to model osteomyelitis, although today they are not widely utilized. Similar to caprine and ovine models, canine models have primarily utilized long bones, specifically the tibia (53, 171, 172) and the femur (47, 173, 174), although a vertebral model has also been described (175). Models vary in approach. Deysine et al. described an injection of bacterial inoculum into the tibial nutrient artery without any additional trauma. This approach was effective in establishing osteomyelitis, but also resulted in the loss of three dogs from septicemia (53). Most other models report bone trauma and bacterial inoculation of the medullary canal, whether that is by direct inoculation or placement of an infected implant (47, 171, 174). Khodaparast et al. had success in establishing osteomyelitis via application of a penetrating captive bolt device to the tibia of dogs to create an open fracture. This approach was selected in order to mimic traumatic osteomyelitis. This model involved the placement of microdialysis probes for sample collection, which is a valuable tool (172) when investigating the dynamics of local environments, whether that is physiologic dynamics or drug delivery profiles.
As described above, Khodaparast et al. (172) established a tibial fracture model of canine osteomyelitis and placed microdialysis probes with the goal of exploring the role of vascular endothelial growth factor (VEGF) as a rate-limiting step in wound healing. This was investigated by measuring VEGF mRNA levels in response to S. aureus osteomyelitis and S. aureus osteomyelitis treated with a rotational gastrocnemius muscle flap. The muscle flap was investigated because wound healing is accelerated in the presence of well-vascularized tissue. VEGF mRNA levels were found to be greater in the animals with osteomyelitis that received the rotational muscle flap as compared to those who did not. This finding suggests that type of surgical closure impacts specific biological signals and cellular pathways, and may add strength to the recommendation for utilizing muscle flaps for improved wound healing in reconstructive surgeries. Another investigation into pathogenesis was performed by Chen et al. (175) who aimed to investigate the presence, type, and origin of bacteria adjacent to metal implants utilized in the surgical management of pyogenic vertebral osteomyelitis. Investigators found that bacteria were retrieved not only from metal implants, but also from surrounding bone, despite the lack of radiographic signs of infection. These findings suggest that metallic implants are not necessarily the source of persistent or recurrent bacterial infection in vertebral osteomyelitis.
Despite there being few reports, there are canine models of osteomyelitis that investigate treatment strategies. Two models focused on the prevention of osteomyelitis, and found that the placement of gentamicin impregnated bone cement could prevent the development of osteomyelitis in the experimental models (171, 173). Similarly, Huneault et al. (174) investigated the ability of cross-linked high amylose starch (CLHAS) implants loaded with ciprofloxacin to prevent and cure chronic femoral osteomyelitis. This study demonstrated strong preventative efficacy of the ciprofloxacin loaded implants, and also showed that ciprofloxacin loaded implants and oral ciprofloxacin had similar efficacy in clearing bacterial osteomyelitis.
Dogs provide strong models for long bone osteomyelitis. Benefits include appropriate size to perform complex and multi-stage procedures, bone composition and density that is most similar to humans out of the available species (158), temperament that is amenable to handling, as well as well-characterized anesthetic and imaging protocols. Despite these strengths, canine models are no longer frequently utilized for osteomyelitis research. Osteomyelitis research is terminal, and ethical concerns are raised when considering these companion animals as research models. Therefore, despite the provided benefits, it is unlikely that dogs will have a resurgence in popularity for osteomyelitis modeling.
Through the currently available reports of advancements in the management and understanding of osteomyelitis that animal models have facilitated, it is clear that animal models are vital in osteomyelitis research. With the plethora of available species and approaches to model bacterial osteomyelitis, it is also clear that each species provides specific strengths and certain shortcomings, as is highlighted in this review. Based on current information, we suggest an approach where proof of concept work is performed in small mammal models, either a mouse or a rat model. Advanced pathogenesis investigations can also be carried out in small mammal models, either a mouse, rat, or rabbit model. Complex treatment strategies, whether local or systemic, are best suited for large animal models, either mini-pigs, sheep, or goats, to mimic the human response as closely as possible. Improvements to diagnostic procedures may be performed in a variety of models; initial investigations, especially into novel imaging techniques, are best suited for rodent models. Ideally, imaging techniques would be validated in large animal models before preclinical testing. Regardless of the specific indication and utility, the knowledge we gain from animal models of osteomyelitis is an essential asset to the understanding, diagnosis and treatment of bacterial osteomyelitis, and animal modeling is a crucial step toward improving the lives of patients suffering from this life-altering disease.
CB: conceptualization, writing, and editing. DA: conceptualization, editing, and supervision. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Kavanagh N, Ryan E, Widaa A. Staphylococcal osteomyelitis: disease progression, treatment, challenges and future directions. Clin Microbiol Rev. (2018) 31. doi: 10.1128/CMR.00084-17
2. Conterno LO, Turchi MD. Antibiotics for treating chronic osteomyelitis in adults. Cochrane Database Syst Rev. (2013) CD004439. doi: 10.1002/14651858.CD004439.pub3
3. Garcia Del Pozo E, Collazos J, Carton JA, Camporro D, Asensi V. Factors predictive of relapse in adult bacterial osteomyelitis of long bones. BMC Infect Dis. (2018) 18. doi: 10.1186/s12879-018-3550-6
4. Dinh P, Hutchinson BK, Zalavras C, Stevanovic MV. Reconstruction of osteomyelitis defects. Semin Plast Surg. (2009) 23:108–18. doi: 10.1055/s-0029-1214163
5. Fritz JM, McDonald JR. Osteomyelitis: approach to diagnosis and treatment. Phys Sportsmed. (2008) 36:nihpa116823. doi: 10.3810/psm.2008.12.11
6. Lew DP, Waldvogel FA. Osteomyelitis. Lancet. (2004) 364:369–79. doi: 10.1016/S0140-6736(04)16727-5
7. Calhoun JH, Manring MM, Shirtliff M. Osteomyelitis of the long bones. Semin Plast Surg. (2009) 23:59–72. doi: 10.1055/s-0029-1214158
8. Kremers HM, Nwojo ME, Ransom JE, Wood-Wentz CM, Melton LJ, Huddleston PM. Trends in the epidemiology of osteomyelitis. J Bone Joint Surg. (2015) 97:837–45. doi: 10.2106/JBJS.N.01350
9. Rubin RJ, Harrington CA, Poon A, Dietrich K, Greene JA, Moiduddin A. The economic impact of Staphylococcus aureus infection in new york city hospitals. Emerg Infect Dis. (1999) 5:9–17. doi: 10.3201/eid0501.990102
10. Hamza T, Dietz M, Pham D, Clovis N, Danley S, Li B. Intra-cellular Staphylococcus aureus alone causes infection in vivo. Eur Cell Mater. (2013) 25:341–50. Discussion: 50. doi: 10.22203/eCM.v025a24
11. Panteli M, Giannoudis PV. Chronic osteomyelitis: what the surgeon needs to know. EFORT Open Rev. (2016) 1:128–35. doi: 10.1302/2058-5241.1.000017
12. Zimmerli W. Clinical presentation and treatment of orthopaedic implant-associated infection. J Intern Med. (2014) 276:111–9. doi: 10.1111/joim.12233
13. Bisland SK, Chien C, Wilson BC, Burch S. Pre-clinical in vitro and in vivo studies to examine the potential use of photodynamic therapy in the treatment of osteomyelitis. Photochem Photobiol Sci. (2006) 5:31–8. doi: 10.1039/B507082A
14. Urish KL, Cassat JE. Staphylococcus aureus osteomyelitis: bone, bugs, and surgery. Infect Immun. (2020) 88:e00932-19. doi: 10.1128/IAI.00932-19
15. Gallie WE. First recurrence of osteomyelitis eighty years after infection. J Bone Joint Surg Br. (1951) 33:110–1. doi: 10.1302/0301-620X.33B1.110
16. Tiemann A, Hofmann GO, Krukemeyer MG, Krenn V, Langwald S. Histopathological Osteomyelitis Evaluation Score (HOES) – an innovative approach to histopathological diagnostics and scoring of osteomyelitis. GMS Interdiscip Plast Reconstr Surg DGPW. (2014) 3:Doc08. doi: 10.3205/iprs000049
17. Aktekin CN, Ozturk AM, Tabak AY, Altay M, Korkusuz F. A Different perspective for radiological evaluation of experimental osteomyelitis. Skeletal Radiol. (2007) 36:945–50. doi: 10.1007/s00256-007-0342-2
18. Hatzenbuehler J, Pulling TJ. Diagnosis and management of osteomyelitis. Am Fam Physician. (2011) 84:1027–33.
19. Lima AL, Oliveira PR, Carvalho VC, Cimerman S, Savio E, Diretrizes Panamericanas para el Tratamiento de las Osteomielitis e Infecciones de Tejidos Blandos Group. Recommendations for the treatment of osteomyelitis. Braz J Infect Dis. (2014) 18:526–34. doi: 10.1016/j.bjid.2013.12.005
20. Trampuz A, Zimmerli W. Diagnosis and treatment of infections associated with fracture-fixation devices. Injury. (2006) 37(Suppl 2):S59–66. doi: 10.1016/j.injury.2006.04.010
21. Odekerken JC, Walenkamp GH, Brans BT, Welting TJ, Arts JJ. The longitudinal assessment of osteomyelitis development by molecular imaging in a rabbit model. Biomed Res Int. (2014) 2014:424652. doi: 10.1155/2014/424652
22. Lucke M, Schmidmaier G, Sadoni S, Wildemann B, Schiller R, Stemberger A, et al. A new model of implant-related osteomyelitis in rats. J Biomed Mater Res B Appl Biomater. (2003) 67:593–602. doi: 10.1002/jbm.b.10051
23. Mariani BD, Martin DS, Chen AF, Yagi H, Lin SS, Tuan RS. Polymerase chain reaction molecular diagnostic technology for monitoring chronic osteomyelitis. J Exp Orthop. (2014) 1:9. doi: 10.1186/s40634-014-0009-6
24. Darouiche R. Treatment of infections associated with surgical implants. N Engl J Med. (2004) 350:1422–9. doi: 10.1056/NEJMra035415
25. Ellington JK, Harris M, Hudson MC, Vishin S, Webb LX, Sherertz R. Intracellular Staphylococcus aureus and antibiotic resistance: implications for treatment of Staphylococcal osteomyelitis. J Orthop Res. (2006) 24:87–93. doi: 10.1002/jor.20003
26. Roblot F, Besnier JM, Juhel L, Vidal C, Ragot S, Bastides F, et al. Optimal duration of antibiotic therapy in vertebral osteomyelitis. Semin Arthritis Rheum. (2007) 36:269–77. doi: 10.1016/j.semarthrit.2006.09.004
27. Gomes D, Pereira M, Bettencourt AF. Osteomyelitis: an overview of antimicrobial therapy. Braz J Pharm Sci. (2013) 49:13–27. doi: 10.1590/S1984-82502013000100003
28. Cobb LH, McCabe EM, Priddy LB. Therapeutics and delivery vehicles for local treatment of osteomyelitis. J Orthop Res. (2020) 38:2091–103. doi: 10.1002/jor.24689
29. Sankaran J, Tan NJHJ, But KP, Cohen Y, Rice SA, Wohland T. Single microcolony diffusion analysis in Pseudomonas aeruginosa biofilms. NPJ Biofilms Microbiomes. (2019) 5:35. doi: 10.1038/s41522-019-0107-4
30. Masters EA, Trombetta RP, de Mesy Bentley KL, Boyce BF, Gill AL, Gill SR, et al. Evolving concepts in bone infection: redefining “biofilm”, “acute vs. chronic osteomyelitis”, “the immune proteome” and “local antibiotic therapy”. Bone Res. (2019) 7:20. doi: 10.1038/s41413-019-0061-z
31. Muthukrishnan G, Masters EA, Daiss JL, Schwarz EM. Mechanisms of immune evasion and bone tissue colonization that make Staphylococcus aureus the primary pathogen in osteomyelitis. Curr Osteoporos Rep. (2019) 17:395–404. doi: 10.1007/s11914-019-00548-4
32. Savage VJ, Chopra I, O'Neill AJ. Staphylococcus aureus biofilms promote horizontal transfer of antibiotic resistance. Antimicrob Agents Chemother. (2013) 57:1968–70. doi: 10.1128/AAC.02008-12
33. Hall-Stoodley L, Costerton JW, Stoodley P. Bacterial biofilms: from the natural environment to infectious diseases. Nat Rev Microbiol. (2004) 2:95–108. doi: 10.1038/nrmicro821
34. Al-Mayahi M, Hemmady MV, Shoaib A, Morgan-Jones RL. Recurrence of chronic osteomyelitis in a regenerated fibula after 65 years. Orthopedics. (2007) 30:403–4. doi: 10.3928/01477447-20070501-12
35. Libraty DH, Patkar C, Torres B. Staphylococcus aureus reactivation osteomyelitis after 75 years. N Engl J Med. (2012) 366:481–2. doi: 10.1056/NEJMc1111493
36. O'Reilly T, Mader JT. Rat model of bacterial osteomyelitis of the tibia. In: Zak O, Sande MA, editors. Handbook of Animal Models of Infection: Experimental Models in Antimicrobial Chemotherapy. San Diego, CA: Academic Press. (1999), p. 561–75. doi: 10.1016/B978-012775390-4/50205-0
37. Ford CA, Cassat JE. Advances in the local and targeted delivery of anti-infective agents for management of osteomyelitis. Expert Rev Anti Infect Ther. (2017) 15:851–60. doi: 10.1080/14787210.2017.1372192
38. Salgado CJ, Mardini S, Jamali AA, Ortiz J, Gonzales R, Chen HC. Muscle versus nonmuscle flaps in the reconstruction of chronic osteomyelitis defects. Plast Reconstr Surg. (2006) 118:1401–11. doi: 10.1097/01.prs.0000239579.37760.92
39. Darouiche R. Device-associated infections: a macroproblem that starts with microadherence. Healthc Epidemiol. (2001) 33:1567–72. doi: 10.1086/323130
40. Zoller SD, Hegde V, Burke ZDC, Park HY, Ishmael CR, Blumstein GW, et al. Evading the host response: Staphylococcus “Hiding” in cortical bone canalicular system causes increased bacterial burden. Bone Res. (2020) 8:43. doi: 10.1038/s41413-020-00118-w
41. Zomer HD, Trentin AG. Skin wound healing in humans and mice: challenges in translational research. J Dermatol Sci. (2018) 90:3–12. doi: 10.1016/j.jdermsci.2017.12.009
42. Phang SJ, Arumugam B, Kuppusamy UR, Fauzi MB, Looi ML. A review of diabetic wound models-novel insights into diabetic foot ulcer. J Tissue Eng Regen Med. (2021) 15:1051–68. doi: 10.1002/term.3246
43. Mendes JJ, Leandro CI, Bonaparte DP, Pinto AL. A rat model of diabetic wound infection for the evaluation of topical antimicrobial therapies. Comp Med. (2012) 62:37–48.
44. Ortines RV, Liu H, Cheng LI, Cohen TS, Lawlor H, Gami A, et al. Neutralizing alpha-toxin accelerates healing of Staphylococcus aureus-infected wounds in nondiabetic and diabetic mice. Antimicrob Agents Chemother. (2018) 62:e02288-17. doi: 10.1128/AAC.02288-17
45. Mader JT. Animal models of osteomyelitis. Am J Med. (1985) 78:213–7. doi: 10.1016/0002-9343(85)90387-0
46. Hwang SC, Hwang DS, Kim HY, Kim MJ, Kang YH, Byun SH, et al. Development of bone regeneration strategies using human periosteum-derived osteoblasts and oxygen-releasing microparticles in mandibular osteomyelitis model of miniature pig. J Biomed Mater Res A. (2019) 107:2183–94. doi: 10.1002/jbm.a.36728
47. Petty W, Spanier S, Shuster J, Silverthorne C. The influence of skeletal implants on incidence of infection experiments in a canine model. J Bone Joint Surg. (1985) 67:1236–44. doi: 10.2106/00004623-198567080-00015
48. Niska JA, Shahbazian JH, Ramos RI, Francis KP, Bernthal NM, Miller LS. Vancomycin-rifampin combination therapy has enhanced efficacy against an experimental Staphylococcus aureus prosthetic joint infection. Antimicrob Agents Chemother. (2013) 57:5080–6. doi: 10.1128/AAC.00702-13
49. Zhang X, Ma YF, Wang L, Jiang N, Qin CH, Hu YJ, et al. A rabbit model of implant-related osteomyelitis inoculated with biofilm after open femoral fracture. Exp Ther Med. (2017) 14:4995–5001. doi: 10.3892/etm.2017.5138
50. Wang Y, Cheng LI, Helfer DR, Ashbaugh AG, Miller RJ, Tzomides AJ, et al. Mouse model of hematogenous implant-related Staphylococcus aureus biofilm infection reveals therapeutic targets. Proc Natl Acad Sci USA. (2017) 114:E5094–102. doi: 10.1073/pnas.1703427114
51. Makinen TJ, Lankinen P, Poyhonen T, Jalava J, Aro HT, Roivainen A. Comparison of 18f-Fdg and 68ga pet imaging in the assessment of experimental osteomyelitis due to Staphylococcus aureus. Eur J Nucl Med Mol Imaging. (2005) 32:1259–68. doi: 10.1007/s00259-005-1841-9
52. Horst SA, Hoerr V, Beineke A, Kreis C, Tuchscherr L, Kalinka J, et al. A novel mouse model of Staphylococcus aureus chronic osteomyelitis that closely mimics the human infection: an integrated view of disease pathogenesis. Am J Pathol. (2012) 181:1206–14. doi: 10.1016/j.ajpath.2012.07.005
53. Deysine M, Isenberg H, Steiner G. Chronic haematogenous osteomyelitis; studies on an experimental model. Int Orthop. (1983) 7:69–78. doi: 10.1007/BF00266454
54. Chadha HS, Fitzgerald RH, Wiater P, Sud S, Nasser S, Wooley PH. Experimental acute hematogenous osteomyelitis in mice I histopathological and immunological findings. J Orthop Res. (1999) 17:376–81. doi: 10.1002/jor.1100170312
55. Laratta JL, Shillingford JN, Hardy N, Lehman RA, Lenke LG, Riew KD. A dose-response curve for a gram-negative spinal implant infection model in rabbits. Spine. (2017) 42:E1225–30. doi: 10.1097/BRS.0000000000002205
56. Johansen LK, Koch J, Frees D, Aalbæk B, Nielsen OL, Leifsson PS, et al. Pathology and biofilm formation in a porcine model of Staphylococcal osteomyelitis. J Comp Path. (2012) 147:343–53. doi: 10.1016/j.jcpa.2012.01.018
57. Dworsky EM, Hegde V, Loftin AH, Richman S, Hu Y, Lord E, et al. Novel in vivo mouse model of implant related spine infection. J Orthop Res. (2017) 35:193–9. doi: 10.1002/jor.23273
58. Guarch-Pérez C, Riool M, Zaat S. Current osteomyelitis mouse models, a systematic review. Eur Cells Mater. (2021) 42:334–74. doi: 10.22203/eCM.v042a22
59. Bragg B, Epstein NJ, Ma T, Goodman S, Smith RL. Histomorphometric analysis of the intramedullary bone response to titanium particles in wild-type and Il-1r1 Knock-out mice: a preliminary study. J Biomed Mater Res B Appl Biomater. (2008) 84:559–70. doi: 10.1002/jbm.b.30904
60. Pribaz JR, Bernthal NM, Billi F, Cho JS, Ramos RI, Guo Y, et al. Mouse model of chronic post-arthroplasty infection: noninvasive in vivo bioluminescence imaging to monitor bacterial burden for long-term study. J Orthop Res. (2012) 30:335–40. doi: 10.1002/jor.21519
61. Bernthal NM, Stavrakis AI, Billi F, Cho JS, Kremen TJ, Simon SI, et al. A Mouse model of post-arthroplasty Staphylococcus aureus joint infection to evaluate in vivo the efficacy of antimicrobial implant coatings. PLoS ONE. (2010) 5:e12580. doi: 10.1371/journal.pone.0012580
62. Sheppard WL, Mosich GM, Smith RA, Hamad CD, Park HY, Zoller SD, et al. Novel in vivo mouse model of shoulder implant infection. J Shoulder Elb Surg. (2020) 29:1412–24. doi: 10.1016/j.jse.2019.10.032
63. Funao H, Ishii K, Nagai S, Sasaki A, Hoshikawa T, Aizawa M, et al. Establishment of a real-time, quantitative, and reproducible mouse model of Staphylococcus osteomyelitis using bioluminescence imaging. Infect Immun. (2012) 80:733–41. doi: 10.1128/IAI.06166-11
64. Roux KM, Cobb LH, Seitz MA, Priddy LB. Innovations in osteomyelitis research: a review of animal models. Animal Model Exp Med. (2021) 4:59–70. doi: 10.1002/ame2.12149
65. De Mesy Bentley KL, Trombetta R, Nishitani K, Bello-Irizarry SN, Ninomiya M, Zhang L, et al. Evidence of Staphylococcus aureus deformation, proliferation, and migration in canaliculi of live cortical bone in murine models of osteomyelitis. J Bone Miner Res. (2017) 32:985–90. doi: 10.1002/jbmr.3055
66. Masters EA, Muthukrishnan G, Ho L, Gill AL, de Mesy Bentley KL, Galloway CA, et al. Staphylococcus aureus cell wall biosynthesis modulates bone invasion and osteomyelitis pathogenesis. Front Microbiol. (2021) 12:723498. doi: 10.3389/fmicb.2021.723498
67. Bernthal NM, Taylor BN, Meganck JA, Wang Y, Shahbazian JH, Niska JA, et al. Combined in vivo optical and microct imaging to monitor infection, inflammation, and bone anatomy in an orthopaedic implant infection in mice. J Vis Exp. (2014) doi: 10.3791/51612
68. Avci P, Karimi M, Sadasivam M, Antunes-Melo WC, Carrasco E, Hamblin MR. In-vivo monitoring of infectious diseases in living animals using bioluminescence imaging. Virulence. (2018) 9:28–63. doi: 10.1080/21505594.2017.1371897
69. Isogai N, Shiono Y, Kuramoto T, Yoshioka K, Ishihama H, Funao H, et al. Potential osteomyelitis biomarkers identified by plasma metabolome analysis in mice. Sci Rep. (2020) 10:839. doi: 10.1038/s41598-020-57619-1
70. Jørgensen NP, Skovdal SM, Meyer RL, Dagnæs-Hansen F, Fuursted K, Petersen E. Rifampicin-containing combinations are superior to combinations of vancomycin, linezolid and daptomycin against Staphylococcus aureus biofilm infectionin vivoandin vitro. Pathog Dis. (2016) 74:ftw019. doi: 10.1093/femspd/ftw019
71. Inzana J, Trombetta R, Schwarz E, Kates S, Awad H. 3D printed bioceramics for dual antibiotic delivery to treat implant-associated bone infection. Eur Cells Mater. (2015) 30:232–47. doi: 10.22203/eCM.v030a16
72. Trombetta R, Ninomiya M, El-Atawneh I, Knapp E, De Mesy Bentley K, Dunman P, et al. Calcium phosphate spacers for the local delivery of sitafloxacin and rifampin to treat orthopedic infections: efficacy and proof of concept in a mouse model of single-stage revision of device-associated osteomyelitis. Pharmaceutics. (2019) 11:94. doi: 10.3390/pharmaceutics11020094
73. Lindsay SE, Lindsay HG, Kallet J, Weaver MR, Curran-Everett D, Crapo JD, et al. Mnte-2-pyp disrupts Staphylococcus aureus biofilms in a novel fracture model. J Orthop Res. (2021) 39:2439–45. doi: 10.1002/jor.24967
74. Büren C, Lögters T, Oezel L, Rommelfanger G, Scholz AO, Windolf J, et al. Effect of hyperbaric oxygen therapy (Hbo) on implant-associated osteitis in a femur fracture model in mice. PLoS ONE. (2018) 13:e0191594. doi: 10.1371/journal.pone.0191594
75. Johnson CT, Sok MCP, Martin KE, Kalelkar PP, Caplin JD, Botchwey EA. Lysostaphin and Bmp-2 co-delivery reduces S. aureus infection and regenerates critical-sized segmental bone defects. Sci Adv. (2019) 5: eaaw1228. doi: 10.1126/sciadv.aaw1228
76. Yokogawa N, Ishikawa M, Nishitani K, Beck CA, Tsuchiya H, Mesfin A, et al. Immunotherapy synergizes with debridement and antibiotic therapy in a murine 1-stage exchange model of MRSA implant-associated osteomyelitis. J Orthop Res. (2018) 36:1590–8. doi: 10.1002/jor.23801
77. Muschler GF, Raut VP, Patterson TE, Wenke JC, Hollinger JO. The design and use of animal models for translational research in bone tissue engineering and regenerative medicine. Tissue Eng Part B Rev. (2010) 16:123–45. doi: 10.1089/ten.teb.2009.0658
78. Reizner W, Hunter JG, O'Malley NT, Southgate RD, Schwarz EM, Kates SL, et al. Systematic review of animal models for Staphylococcus aureus osteomyelitis. Eur Cell Mater. (2015) 27:196–212. doi: 10.22203/eCM.v027a15
79. An YH, Kang QK, Arciola CR. Animal models of osteomyelitis. Int J Artif Organs. (2006) 29:407–20. doi: 10.1177/039139880602900411
80. Hassani Besheli N, Mottaghitalab F, Eslami M, Gholami M, Kundu SC, Kaplan DL, et al. Sustainable release of vancomycin from silk fibroin nanoparticles for treating severe bone infection in rat tibia osteomyelitis model. ACS Appl Mater Interfaces. (2017) 9:5128–38. doi: 10.1021/acsami.6b14912
81. Fukushima N, Yokoyama K, Sasahara T, Dobashi Y, Itoman M. Establishment of rat model of acute Staphylococcal osteomyelitis: relationship between inoculation dose and development of osteomyelitis. Arch Orthop Trauma Surg. (2005) 125:169–76. doi: 10.1007/s00402-004-0785-z
82. Harrasser N, Gorkotte J, Obermeier A, Feihl S, Straub M, Slotta-Huspenina J, et al. A new model of implant-related osteomyelitis in the metaphysis of rat tibiae. BMC Musculoskelet Disord. (2016) 17:152. doi: 10.1186/s12891-016-1005-z
83. Neyisci C, Erdem Y, Bilekli AB, Demiralp B, Kose O, Bek D, et al. Treatment of implant-related methicillin-resistant Staphylococcus aureus osteomyelitis with vancomycin-loaded Vk100 silicone cement: an experimental study in rats. J Orthop Surg. (2018) 26:2309499017754093. doi: 10.1177/2309499017754093
84. Robinson DA, Bechtold JE, Carlson CS, Evans RB, Conzemius MG. Development of a fracture osteomyelitis model in the rat femur. J Orthop Res. (2011) 29:131–7. doi: 10.1002/jor.21188
85. Sanchez CJ Jr., Prieto EM, Krueger CA, Zienkiewicz KJ, Romano DR, Ward CL, et al. Effects of local delivery of D-amino acids from biofilm-dispersive scaffolds on infection in contaminated rat segmental defects. Biomaterials. (2013) 34:7533–43. doi: 10.1016/j.biomaterials.2013.06.026
86. Fölsch C, Federmann M, Kuehn KD, Kittinger C, Kogler S, Zarfel G, et al. Coating with a novel gentamicinpalmitate formulation prevents implant-associated osteomyelitis induced by methicillin-susceptible Staphylococcus aureus in a rat model. Int Orthop. (2015) 39:981–8. doi: 10.1007/s00264-014-2582-9
87. Jung SW, Oh SH, Lee IS, Byun JH, Lee JH. In situ gelling hydrogel with anti-bacterial activity and bone healing property for treatment of osteomyelitis. Tissue Eng Regen Med. (2019) 16:479–90. doi: 10.1007/s13770-019-00206-x
88. Oh EJ, Oh SH, Lee IS, Kwon OS, Lee JH. Antibiotic-eluting hydrophilized PMMA bone cement with prolonged bactericidal effect for the treatment of osteomyelitis. J Biomater Appl. (2016) 30:1534–44. doi: 10.1177/0885328216629823
89. Melicherčík P, Cerovský V, Nešuta O, Jahoda D, Landor I, Ballay R, et al. Testing the efficacy of antimicrobial peptides in the topical treatment of induced osteomyelitis in rats. Folia Microbiol. (2018) 63:97–104. doi: 10.1007/s12223-017-0540-9
90. Qu X, Yang H, Jia B, Wang M, Yue B, Zheng Y, et al. Zinc alloy-based bone internal fixation screw with antibacterial and anti-osteolytic properties. Bioact Mater. (2021) 6:4607–24. doi: 10.1016/j.bioactmat.2021.05.023
91. Sodnom-Ish B, Eo MY, Oh JH, Seo MH, Yang HJ, Lee JH, et al. Decompression effects on bone healing in rat mandible osteomyelitis. Sci Rep. (2021) 11:11673. doi: 10.1038/s41598-021-91104-7
92. Ofluoglu EA, Zileli M, Aydin D, Baris YS, Kuçukbasmaci O, Gonullu N, et al. Implant-related infection model in rat spine. Arch Orthop Trauma Surg. (2007) 127:391–6. doi: 10.1007/s00402-007-0365-0
93. Søe NH, Jensen NV, Nürnberg BM, Jensen AL, Koch J, Poulsen SS, et al. A novel knee prosthesis model of implant-related osteo- myelitis in rats. Acta Orthop. (2013) 84:92–7. doi: 10.3109/17453674.2013.773121
94. Shiels SM, Bedigrew KM, Wenke JC. Development of a hematogenous implant-related infection in a rat model. BMC Musculoskelet Disord. (2015) 16. doi: 10.1186/s12891-015-0699-7
95. Hienz SA, Sakamoto H, Flock JI, Mörner AC, Reinholt FP, Heimdahl A, et al. Development and characterization of a new model of hematogenous osteomyelitis in the rat. J Infect Dis. (1995) 171:1230–6. doi: 10.1093/infdis/171.5.1230
96. Rissing JP, Buxton TB, Weinstein RS, Shockley RK. Model of experimental chronic osteomyelitis in rats. Infect Immun. (1985) 47:581–6. doi: 10.1128/iai.47.3.581-586.1985
97. Spagnolo N, Greco F, Rossi A, Ciolli L, Teti A, Posteraro P. Chronic Staphylococcal osteomyelitis: a new experimental rat model. Infect Immun. (1993) 61:5225–30. doi: 10.1128/iai.61.12.5225-5230.1993
98. Vergidis P, Rouse MS, Euba G, Karau MJ, Schmidt SM, Mandrekar JN, et al. Treatment with linezolid or vancomycin in combination with rifampin is effective in an animal model of methicillin-resistant Staphylococcus aureus foreign body osteomyelitis. Antimicrob Agents Chemother. (2011) 55:1182–6. doi: 10.1128/AAC.00740-10
99. Stadelmann VA, Potapova I, Camenisch K, Nehrbass D, Richards RG, Moriarty TF. In vivo microct monitoring of osteomyelitis in a rat model. Biomed Res Int. (2015) 2015:1–12. doi: 10.1155/2015/587857
100. Vergidis P, Schmidt-Malan SM, Mandrekar JN, Steckelberg JM, Patel R. Comparative activities of vancomycin, tigecycline and rifampin in a rat model of methicillin-resistant Staphylococcus aureus osteomyelitis. J Infect. (2015) 70:609–15. doi: 10.1016/j.jinf.2014.12.016
101. Avdeeva EY, Slizovsky GV, Skorokhodova MG, Fomina TI, Zorkaltsev MA, Zavadovskaya VD, et al. Experimental simulation of traumatic osteomyelitis in rats. Bull Exp Biol Med. (2016) 161:137–40. doi: 10.1007/s10517-016-3364-8
102. Fölsch C, Federmann M, Lakemeier S, Kuehn KD, Kittinger C, Kerwat M, et al. Systemic antibiotic therapy does not significantly improve outcome in a rat model of implant-associated osteomyelitis induced by methicillin susceptible Staphylococcus aureus. Arch Orthop Trauma Surg. (2016) 136:585–92. doi: 10.1007/s00402-016-2419-7
103. Park KH, Greenwood-Quaintance KE, Mandrekar J, Patel R. Activity of tedizolid in methicillin-resistant Staphylococcus aureus experimental foreign body-associated osteomyelitis. Antimicrob Agents Chemother. (2016) 60:6568–72. doi: 10.1128/AAC.01248-16
104. Cui T, Li J, Zhen P, Gao Q, Fan X, Li C. Masquelet induced membrane technique for treatment of rat chronic osteomyelitis. Exp Ther Med. (2018) doi: 10.3892/etm.2018.6573
105. Kussmann M, Obermueller M, Berndl F, Reischer V, Veletzky L, Burgmann H, et al. Dalbavancin for treatment of implant-related methicillin-resistant Staphylococcus aureus osteomyelitis in an experimental rat model. Sci Rep. (2018) 8:9661. doi: 10.1038/s41598-018-28006-8
106. Cobb LH, Park J, Swanson EA, Beard MC, McCabe EM, Rourke AS, et al. Crispr-Cas9 modified bacteriophage for treatment of Staphylococcus aureus induced osteomyelitis and soft tissue infection. PLoS ONE. (2019) 14:e0220421. doi: 10.1371/journal.pone.0220421
107. Wu S, Liu Y, Lei L, Zhang H. Virulence of methicillin-resistant Staphylococcus aureus modulated by the YycFG two-component pathway in a rat model of osteomyelitis. J Orthop Surg Res. (2019) 14:433. doi: 10.1186/s13018-019-1508-z
108. Zhou P, Wu J, Wang Y, Zhang H, Xia Y, Zhang Y, et al. The synergistic therapeutic efficacy of vancomycin and omega-3 fatty acids alleviates Staphylococcus aureus-induced osteomyelitis in rats. Biomed Pharmacother. (2019) 111:1228–33. doi: 10.1016/j.biopha.2018.12.125
109. Deng S, Wang Y, Liu S, Chen T, Hu Y, Zhang G, et al. Extracellular vesicles: a potential biomarker for quick identification of infectious osteomyelitis. Front Cell Infect Microbiol. (2020) 10:323. doi: 10.3389/fcimb.2020.00323
110. Sahukhal GS, Tucci M, Benghuzzi H, Wilson G, Elasri MO. The role of the msaabcr operon in implant-associated chronic osteomyelitis in Staphylococcus aureus Usa300 Lac. BMC Microbiol. (2020) 20:324. doi: 10.1186/s12866-020-01964-8
111. Schierholz JM, Beuth J. Implant infections: a haven for opportunistic bacteria. J Hosp Infect. (2001) 49:87–93. doi: 10.1053/jhin.2001.1052
112. Hudson MC, Ramp WK, Nicholson NC, Williams AS, Nousiainen MT. Internalization of Staphylococcus aureus by cultured osteoblasts. Microb Pathog. (1995) 19:409–19. doi: 10.1006/mpat.1995.0075
113. Tucker KA, Reilly SS, Leslie CS, Hudson MC. Intracellular Staphylococcus aureus induces apoptosis in mouse osteoblasts. FEMS Microbiol Lett. (2000) 186:151–6. doi: 10.1111/j.1574-6968.2000.tb09096.x
114. Bottagisio M, Coman C, Lovati AB. Animal models of orthopaedic infections. A review of rabbit models used to induce long bone bacterial infections. J Med Microbiol. (2019) 68:506–37. doi: 10.1099/jmm.0.000952
115. Odekerken JC, Arts JJ, Surtel DA, Walenkamp GH, Welting TJ, et al. A rabbit osteomyelitis model for the longitudinal assessment of early post-operative implant infections. J Orthop Surg Res. (2013) 8:38. doi: 10.1186/1749-799X-8-38
116. Yan L, Wu J, Jiang D, Wu J, Wang X, Wang Z-L, et al. Treatment of Staphylococcus aureus-induced chronic osteomyelitis with bone-like hydroxyapatite/poly amino acid loaded with rifapentine microspheres. Drug Des Devel Ther. (2015) 9:3665–76. doi: 10.2147/DDDT.S84486
117. Gahukamble AD, McDowell A, Post V, Salavarrieta Varela J, Rochford ET, Richards RG, et al. Propionibacterium acnes and Staphylococcus lugdunensis cause pyogenic osteomyelitis in an intramedullary nail model in rabbits. J Clin Microbiol. (2014) 52:1595–606. doi: 10.1128/JCM.03197-13
118. Odekerken JC, Brans BT, Welting TJ, Walenkamp GH. (18)F-Fdg micropet imaging differentiates between septic and aseptic wound healing after orthopedic implant placement: a longitudinal study of an implant osteomyelitis in the rabbit tibia. Acta Orthop. (2014) 85:305–13. doi: 10.3109/17453674.2014.900894
119. Zahar A, Kocsis G, Citak M, Puskás G, Domahidy M, Hajdú M, et al. Use of antibiotic-impregnated bone grafts in a rabbit osteomeylitis model. Technol Health Care. (2017) 25:929–38. doi: 10.3233/THC-170869
120. Kose N, Asfuroglu ZM, Kose A, Sahinturk V, Gurbuz M, Dogan A. Silver ion-doped calcium phosphate-based bone-graft substitute eliminates chronic osteomyelitis: an experimental study in animals. J Orthop Res. (2021) 39:1390–401. doi: 10.1002/jor.24946
121. Yin L-Y, Manring MM, Calhoun JH. A Rabbit osteomyelitis model to simulate multibacterial war wound infections. Mil Med. (2013) 178:696–700. doi: 10.7205/MILMED-D-12-00550
122. Steinhart H, Schulz S, Mutters R. Evaluation of ozonated oxygen in an experimental animal model of osteomyelitis as a further treatment option for skull-base osteomyelitis. Eur Arch Otorhinolaryngol. (1999) 256:153–7. doi: 10.1007/s004050050130
123. Moskowitz JS, Blaisse MR, Samuel RE, Hsu H-P, Harris MB, Martin SD, et al. The effectiveness of the controlled release of gentamicin from polyelectrolyte multilayers in the treatment of Staphylococcus aureus infection in a rabbit bone model. Biomaterials. (2010) 31:6019–30. doi: 10.1016/j.biomaterials.2010.04.011
124. Inceoglu S, Botimer G, Maskiewicz VK. Novel microcomposite implant for the controlled delivery of antibiotics in the treatment of osteomyelitis following total joint replacement. J Orthop Res. (2021) 39:365–75. doi: 10.1002/jor.24919
125. Jones-Jackson L, Walker R, Purnell G, McLaren SG, Skinner RA, Thomas JR, et al. Early detection of bone infection and differentiation from post-surgical inflammation using 2-deoxy-2-[18F]-fluoro-D-glucose positron emission tomography (FDG-PET) in an animal model. J Orthop Res. (2005) 23:1484–9. doi: 10.1016/j.orthres.2005.03.010.1100230635
126. Overstreet D, McLaren A, Calara F, Vernon B, McLemore R. Local gentamicin delivery from resorbable viscous hydrogels is therapeutically effective. Clin Orthop Relat Res. (2015) 473:337–47. doi: 10.1007/s11999-014-3935-9
127. Munoz NM, Minhaj AA, Dupuis CJ, Ensor JE, Golardi N, Jaso JM, et al. What are the effects of irreversible electroporation on a Staphylococcus aureus rabbit model of osteomyelitis? Clin Orthop Relat Res. (2019) 477:2367–77. doi: 10.1097/CORR.0000000000000882
128. Smeltzer MS, Thomas JR, Hickmon SG, Skinner RA, Nelson CL, Griffith D, et al. Characterization of a rabbit model of Staphylococcal osteomyelitis. J Orthop Res. (1997) 15:414–21. doi: 10.1002/jor.1100150314
129. Ambrose CG, Clyburn TA, Mika J, Gogola GR, Kaplan HB, Wanger A, et al. Evaluation of antibiotic-impregnated microspheres for the prevention of implant-associated orthopaedic infections. J Bone Joint Surg Am. (2014) 96:128–34. doi: 10.2106/JBJS.L.01750
130. Saleh-Mghir A, Muller-Serieys C, Dinh A, Massias L, Cremieux AC. Adjunctive rifampin is crucial to optimizing daptomycin efficacy against rabbit prosthetic joint infection due to methicillin-resistant Staphylococcus aureus. Antimicrob Agents Chemother. (2011) 55:4589–93. doi: 10.1128/AAC.00675-11
131. Nielsen NHS, Renneberg J, Nürnberg BM, Torholm C. Experimental implant-related osteomyelitis induced with Staphylococcus aureus. Eur J Orthop Surg Traumatol. (1996) 6:97–100. doi: 10.1007/BF00568321
132. Lan Y, Xie H, Shi Y, Jin Q, Zhang X, Wang Y, et al. Nemobinding domain peptide ameliorates inflammatory bone destruction in a Staphylococcus aureus induced chronic osteomyelitis model. Mol Med Rep. (2019) 19:3291–7. doi: 10.3892/mmr.2019.9975
133. Liu G, Chen S, Fang J, Xu B, Li S, Hao Y, et al. Vancomycin microspheres reduce postoperative spine infection in an in vivo rabbit model. BMC Pharmacol Toxicol. (2016) 17:61. doi: 10.1186/s40360-016-0105-6
134. Elgazzar AH, Dannoon S, Sarikaya I, Farghali M, Junaid TA. Scintigraphic patterns of indium-111 oxine-labeled white blood cell imaging of gram-negative versus gram-positive vertebral osteomyelitis. Med Princ Pract. (2017) 26:415–20. doi: 10.1159/000480083
135. Shiels SM, Raut VP, Patterson PB, Barnes BR, Wenke JC. Antibiotic-loaded bone graft for reduction of surgical site infection in spinal fusion. Spine J. (2017) 17:1917–25. doi: 10.1016/j.spinee.2017.06.039
136. Bierry G, Jehl F, Boehm N, Robert P, Dietemann J-L, Kremer S. Macrophage imaging by USPIO-enhanced MR for the differentiation of infectious osteomyelitis and aseptic vertebral inflammation. Eur Radiol. (2009) 19:1604–11. doi: 10.1007/s00330-009-1319-4
137. Poultsides LA, Papatheodorou LK, Karachalios TS, Khaldi L, Maniatis A, Petinaki E, et al. Novel model for studying hematogenous infection in an experimental setting of implant-related infection by a community-acquired methicillin-resistant S. aureus strain. J Orthop Res. (2008) 26:1355–62. doi: 10.1002/jor.20608
138. Schulz S, Steinhart H, Mutters R. Chronic osteomyelitis in a new rabbit model. J Invest Surg. (2001) 14:121–31. doi: 10.1080/08941930152024246
139. Moriarty TF, Campoccia D, Nees SK, Boure LP, Richards RG. In vivo evaluation of the effect of intramedullary nail microtopography on the development of local infection in rabbits. Int J Artif Organs. (2010) 33:667–75. doi: 10.1177/039139881003300913
140. Wenter V, Müller J-P, Albert NL, Lehner S, Fendler WP, Bartenstein P, et al. The diagnostic value of [18f]Fdg pet for the detection of chronic osteomyelitis and implant-associated infection. Eur J Nucl Med Mol Imaging. (2016) 43:749–61. doi: 10.1007/s00259-015-3221-4
141. Lazzarini L, Overgaard KA, Conti E, Shirtliff ME. Experimental osteomyelitis: what have we learned from animal studies about the systemic treatment of osteomyelitis? J Chemother. (2006) 18:451–60. doi: 10.1179/joc.2006.18.5.451
142. Kishor C, Mishra RR, Saraf SK, Kumar M, Srivastav AK, Nath G. Phage therapy of Staphylococcal chronic osteomyelitis in experimental animal model. Indian J Med Res. (2016) 143:87–94. doi: 10.4103/0971-5916.178615
143. Graur D, Duret L, Gouy M. Phylogenetic position of the order lagomorpha (rabbits, hares and allies). Nature. (1996) 379:333–5. doi: 10.1038/379333a0
144. Mäkitaipale J, Sievänen H, Laitinen-Vapaavuori O. Tibial bone density, cross-sectional geometry and strength in finnish pet rabbits: a peripheral quantitative computed tomography study. Vet Rec. (2018) 183:382. doi: 10.1136/vr.104419
145. Nielsen OL, Afzelius P, Bender D, Schønheyder HC, Leifsson PS, Nielsen KM, et al. Comparison of autologous (111)In-leukocytes, (18)F-FDG, (11)C-methionine, (11)C-PK11195 and (68)Ga-citrate for diagnostic nuclear imaging in a juvenile porcine haematogenous Staphylococcus aureus osteomyelitis model. Am J Nucl Med Mol Imaging. (2015) 5:169–82.
146. Johansen LK, Svalastoga EL, Frees D, Aalbaek B, Koch J, Iburg TM, et al. A new technique for modeling of hematogenous osteomyelitis in pigs: inoculation into femoral artery. J Invest Surg. (2013) 26:149–53. doi: 10.3109/08941939.2012.718043
147. Jensen EH, Nielsen OL, Agerholm JS, Iburg T, Johansen LK, Johannesson E, et al. A non-traumatic Staphylococcus aureus osteomyelitis model in pigs. In Vivo. (2010) 24:257–64.
148. Jødal L, Roivainen A, Oikonen V, Jalkanen S, Hansen SB, Afzelius P, et al. Kinetic modelling of [68ga]Ga-dota-siglec-9 in porcine osteomyelitis and soft tissue infections. Molecules. (2019) 24:4094. doi: 10.3390/molecules24224094
149. Afzelius P, Alstrup A, Nielsen O, Nielsen K, Jensen S. Attempts to target Staphylococcus aureus induced osteomyelitis bone lesions in a juvenile pig model by using radiotracers. Molecules. (2020) 25:4329. doi: 10.3390/molecules25184329
150. Patterson AL, Galloway RH, Baumgartner JC, Barsoum IS. Development of chronic mandibular osteomyelitis in a miniswine model. J Oral Maxillofac Surg. (1993) 51:1358–62. doi: 10.1016/S0278-2391(10)80142-9
151. Jensen LK, Koch J, Aalbaek B, Moodley A, Bjarnsholt T, Kragh KN, et al. Early implant-associated osteomyelitis results in a peri-implanted bacterial reservoir. APMIS. (2017) 125:38–45. doi: 10.1111/apm.12597
152. Bue M, Hanberg P, Koch J, Jensen LK, Lundorff M, Aalbaek B, et al. Single-dose bone pharmacokinetics of vancomycin in a porcine implant-associated osteomyelitis model. J Orthop Res. (2017) 36:1093–8. doi: 10.1002/jor.23776
153. Lüthje FL, Blirup-Plum SA, Moller NS, Heegaard PMH, Jensen HE, Kirketerp-Moller K, et al. The host response to bacterial bone infection involves a local upregulation of several acute phase proteins. Immunobiology. (2020) 225:151914. doi: 10.1016/j.imbio.2020.151914
154. Jensen LK, Koch J, Dich-Jorgensen K, Aalbaek B, Petersen A, Fuursted K, et al. Novel porcine model of implant-associated osteomyelitis: a comprehensive analysis of local, regional, and systemic response. J Orthop Res. (2017) 35:2211–21. doi: 10.1002/jor.23505
155. Hill PF, Watkins PE. The prevention of experimental osteomyelitis in a model of gunshot fracture in the pig. Eur J Orthop Surg Traumatol. (2001) 11:237–41. doi: 10.1007/BF01686897
156. Jødal L, Nielsen OL, Afzelius P, Alstrup AKO, Hansen SB. Blood perfusion in osteomyelitis studied with [15o]water pet in a juvenile porcine model. EJNMMI Research. (2017) 7:4. doi: 10.1186/s13550-016-0251-2
157. Afzelius P, Heegaard PM, Jensen SB, Alstrup AKO, Schønheyder HC, Eek A, et al. [99m Tc]-labelled interleukin-8 as a diagnostic tool compared to [18 F]FDG and CT in an experimental porcine osteomyelitis model. Am J Nucl Med Mol Imaging. (2020) 10:32–46.
158. Aerssens J, Boonen S, Lowet G, Dequeker J. Interspecies differences in bone composition, density, and quality: potential implications for in vivo bone research*. Endocrinology. (1998) 139:663–70. doi: 10.1210/endo.139.2.5751
159. Mullender MG, Huiskes R, Versleyen H, Buma P. Osteocyte density and histomorphometric parameters in cancellous bone of the proximal femur in five mammalian species. J Orthop Res. (1996) 14:972–9. doi: 10.1002/jor.1100140618
160. Kaarsemaker S, Walenkamp GH, Bogaard AE. New model for chronic osteomyelitis with Staphylococcus aureus in sheep. Clin Orthop Relat Res. (1997) 339:246–52. doi: 10.1097/00003086-199706000-00033
161. Klein K, Schweizer TA, Siwy K, Lechmann B, Karol A, von Rechenberg B, et al. Establishment of a localized acute implant-associated Staphylococcus aureus bone infection model in sheep. Pathog Dis. (2021) 79:ftab032. doi: 10.1093/femspd/ftab032
162. Moriarty TF, Schmid T, Post V, Samara E, Kates S, Schwarz EM, et al. A large animal model for a failed two-stage revision of intramedullary nail-related infection by methicillin-resistant Staphylococcus aureus. Eur Cell Mater. (2017) 34:83–98. doi: 10.22203/eCM.v034a06
163. McLaren JS, White LJ, Cox HC, Ashraf W, Rahman CV, Blunn GW, et al. A biodegradable antibiotic-impregnated scaffold to prevent osteomyelitis in a contaminated in vivo bone defect model. Eur Cell Mater. (2014) 27:332–49. doi: 10.22203/eCM.v027a24
164. Williams DL, Haymond BS, Woodbury KL, Beck JP, Moore DE, Epperson RT, et al. Experimental model of biofilm implant-related osteomyelitis to test combination biomaterials using biofilms as initial inocula. J Biomed Mater Res A. (2012) 100A:1888–900. doi: 10.1002/jbm.a.34123
165. Boot W, Schmid T, D'Este M, Guillaume O, Foster A, Decosterd L, et al. A hyaluronic acid hydrogel loaded with gentamicin and vancomycin successfully eradicates chronic methicillin- resistant Staphylococcus aureus orthopedic infection in a sheep model. Antimicrob Agents Chemother. (2021) 65:e01840-20. doi: 10.1128/AAC.01840-20
166. Stewart S, Barr S, Engiles J, Hickok NJ, Shapiro IM, Richardson DW, et al. Vancomycin-modified implant surface inhibits biofilm formation and supports bone-healing in an infected osteotomy model in sheep. J Bone Joint Surg. (2012) 94:1406–15. doi: 10.2106/JBJS.K.00886
167. Salgado CJ, Jamali AA, Mardini S, Buchanan K, Veit B. A Model for chronic osteomyelitis using Staphylococcus aureus in goats. Clin Orthop Relat Res. (2005) (436):246–50. doi: 10.1097/01.blo.0000159154.17131.bf
168. Wenke JC, Owens BD, Svoboda SJ, Brooks DE. Effectiveness of commercially-available antibiotic-impregnated implants. J Bone Joint Surg Br. (2006) 88:1102–4. doi: 10.1302/0301-620X.88B8.17368
169. Tran N, Tran PA, Jarrell JD, Engiles JB, Thomas NP, Young MD, et al. In vivo caprine model for osteomyelitis and evaluation of biofilm-resistant intramedullary nails. Biomed Res Int. (2013) 2013:674378. doi: 10.1155/2013/674378
170. van der Borden AJ, Maathuis PG, Engels E, Rakhorst G, van der Mei HC, Busscher HJ, et al. Prevention of pin tract infection in external stainless steel fixator frames using electric current in a goat model. Biomaterials. (2007) 28:2122–6. doi: 10.1016/j.biomaterials.2007.01.001
171. Fitzgerald RH. Experimental osteomyelitis: description of a canine model and the role of depot administration of antibiotics in the prevention and treatment of sepsis. J Bone Joint Surg. (1983) 65:371–80. doi: 10.2106/00004623-198365030-00013
172. Khodaparast O, Coberly DM, Mathey J, Rohrich RJ, Levin LS, Brown SA. Effect of a transpositional muscle flap on VEGF mRNA expression in a canine fracture model. Plast Reconstr Surg. (2003) 112:171–6. doi: 10.1097/01.PRS.0000066170.56389.27
173. Petty W, Spanier S, Shuster J. Prevention of infection after total joint replacement. J Bone Joint Surg. (1988) 70:536–9. doi: 10.2106/00004623-198870040-00009
174. Huneault LM, Lussier B, Dubreuil P, Chouinard L, Désévaux C. Prevention and treatment of experimental osteomyelitis in dogs with ciprofloxacin-loaded crosslinked high amylose starch implants. J Orthop Res. (2004) 22:1351–7. doi: 10.1016/j.orthres.2004.04.007
Keywords: osteomyelitis, bone, in vivo, animal model, Staphylococcus aureus
Citation: Billings C and Anderson DE (2022) Role of Animal Models to Advance Research of Bacterial Osteomyelitis. Front. Vet. Sci. 9:879630. doi: 10.3389/fvets.2022.879630
Received: 20 February 2022; Accepted: 05 April 2022;
Published: 26 April 2022.
Edited by:
Mark Gray, University of Edinburgh, United KingdomReviewed by:
Chao Xie, University of Rochester, United StatesCopyright © 2022 Billings and Anderson. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Caroline Billings, Y2JpbGxpMTBAdm9scy51dGsuZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.