 Jennifer Routh1*
Jennifer Routh1* Sharmini Julita Paramasivam1
Sharmini Julita Paramasivam1 Peter Cockcroft1Vishna Devi Nadarajah2
Peter Cockcroft1Vishna Devi Nadarajah2 Kamalan Jeevaratnam1*
Kamalan Jeevaratnam1*- 1School of Veterinary Medicine, University of Surrey, Guildford, United Kingdom
- 2Division of Human Biology, School of Medicine and IMU Centre for Education, International Medical University, Kuala Lumpur, Malaysia
Learning theories are abstract descriptions which help us make sense of educational practice. Multiple theories can inform our understanding of a single concept, in this case: veterinary workplace clinical training (WCT), which occurs just prior to students' graduation as competent veterinary surgeons. The competency movement has strongly influenced reforms in veterinary education and is considered important. In reflection of this, the term “preparedness” is operationalised here as a measure of the likelihood that the veterinary student is going to be a competent learner and participant during WCT. Preparedness itself is therefore important because it directly impacts performance. Workplace clinical training is explored through the lenses of cognitivist, social constructivist and socio-culturalist learning theories and used to inform student preparedness characteristics (“tools”) in terms of their behaviours, personal attributes, knowledge and skills, and awarenesses to optimise learning and participation. These form a new conceptual framework—the “Preparedness Toolkit.”
Introduction
Veterinary workplace clinical training (WCT) comprises an essential part of the veterinary curriculum and typically takes place in the final 12–24 months of the programme. A form of preceptorship (1), students learn through authentic but supervised participation in “real-world” veterinary practice. Workplace clinical training consists of experiential, informal and opportunistic teaching approaches, albeit guided by structured objective setting and assessment frameworks. It can be located in a number of different types of facilities including university-owned teaching hospitals and clinics, or private practice as part of a distributed curriculum. Often several different types of facility are used for WCT within a programme. Through the integration and application of knowledge, alongside the development of key skills, attributes and professional identity, students transition to competent veterinarians. The development of competency during WCT is critical given that veterinary graduates are licensed to practice unsupervised when they leave the programme, albeit with structured support. Veterinary institutions must therefore ensure that graduates gain the competences required to meet the standards of their statutory registration body to ensure they are able to practice safely and professionally.
Workplace-based medical education has been identified as a “black box” (2); the output is clear but the inner workings are difficult to understand. In a similar way and having developed haphazardly from apprenticeship principles, our direct understanding of how veterinary students learn during WCT is imperfect. In addition, there is limited use and application of learning theories in clinical veterinary education (3–8) which is not representative of their potential usefulness in understanding education practices (9). Indeed, Schoenfeld-Tacher and Baker (10) assess that it's no longer appropriate to expect a clinician to be an outstanding teacher without the appreciation of the underlying principles of learning. As such, theory and practice are linked in a bidirectional manner; theory has the potential to inform practice and to be informed by it (11).
Using learning theory to open the lid of the “black box” and understand the underlying pedagogy of WCT could help us to prepare students for their experiences. Improving preparedness, defined here as “are you going to be a competent learner and participant of WCT?” (12), should improve student competency and produce veterinarians better able to serve the needs of society.
Learning Theories
A theory is a set of interrelated propositions, concepts or definitions, which specifies the relationships between them, with the aim of explanation or making predictions (13). Learning theories are abstract descriptions which help us make sense of educational practice. More broadly, “conceptual frameworks represent ways of thinking about a problem… or ways of representing how complex things work the way they do” [(14), p. 313]. Different conceptual frameworks can be used to illuminate or magnify different aspects of a system, such as an education programme (14). However, no one conceptual framework can adequately explain or justify an entire system. It is therefore both “necessary and confusing” [(15), p. 70] to acknowledge that there will be many appropriate conceptual frameworks applicable to any topic of interest. The conceptual frameworks cognitivism, social constructivism and socio-culturalism encompass different learning theories and focus on different ways of understanding learning in the workplace. The ways in which a range of these learning theories align with WCT will be discussed in this paper and the aim is to produce a new conceptual framework to model how students might be prepared for veterinary WCT.
Cognitivist Theories
Cognitivism focuses on individual psychology and in the context of workplace learning is concerned with the epistemology of professional practice, in other words how do we know how to be a veterinary surgeon? As such, its explanatory power is limited to the individual student. Cognitivism endeavours to explain how knowledge and skills are acquired through transmission (with the input of another resource) and constructivism. Constructivism is important to consider in the context of WCT. It describes how knowledge, meaning or learning is “constructed” and integrated into an expanding but existing network with experience. Nothing is learned from scratch; knowledge is assimilated or reinterpreted in the light of the learner's existing understanding and ability (16). The influence of constructivist concepts such as andragogy (17) and reflective learning (18) is exemplified by the adoption of portfolios, personal development logs and learning objective planning in veterinary curricula.
Kolb's Learning Cycle
Kolb's learning cycle combines the models of learning developed by Dewey, Lewin and Piaget (16). The cycle describes how knowledge is continuously derived from and tested out in the experiences of the learner, and Kolb is credited with proposing that reflection is how learners abstract and transfer their learning to new contexts. In the constructivist style, Kolb states that all learning is re-learning; learners' minds are not blank sheets of paper. This aligns readily with veterinary students entering WCT, their sheet of paper already populated with some concepts (for example their knowledge of anatomy, pathology, microbiology). It is by their experiences in the workplace that students learn how to integrate and apply these subjects in the practice of veterinary medicine.
The learning that Kolb describes is more extensive than that which occurs in the confines of the lecture theatre; learning occurs in all settings (including the workplace) and is lifelong. Additionally, it encompasses not only knowledge acquisition, but the cycle can be applied to other cognitive concepts such as decision making and problem-solving. Learning is viewed by Kolb as a holistic process and involves thinking, feeling, perceiving, and behaving. All these facets of the theory make it attractive for application to veterinary WCT (Table 1).
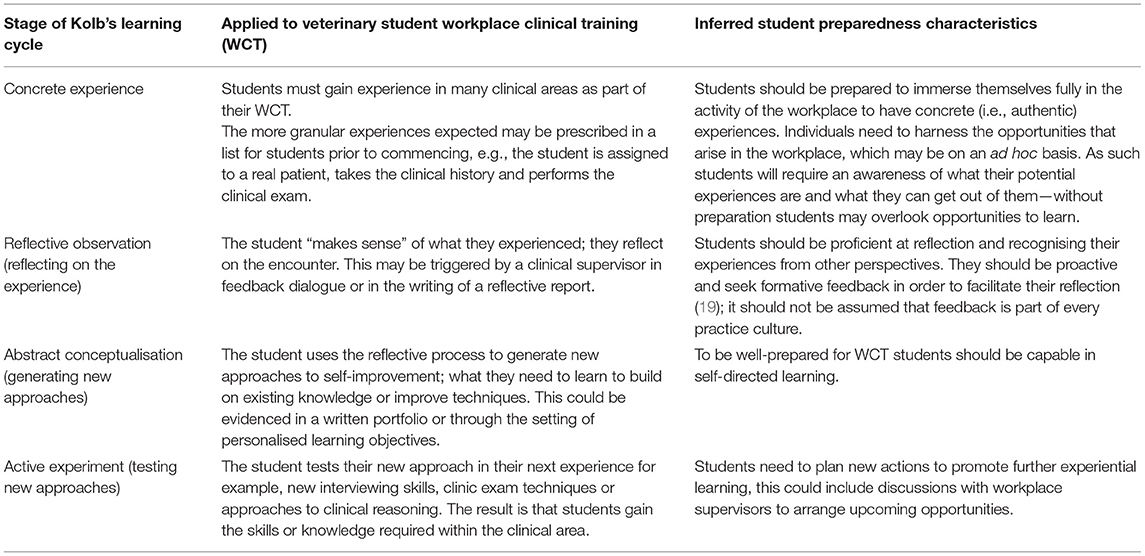
Table 1. The stages of Kolb's learning cycle, applied to veterinary workplace clinical training (WCT) and inferred student preparedness characteristics.
Greenberg and Blatt (20) provide a guide for medical students in negotiating their undergraduate WCT equivalent, based on Kolb's learning cycle. They propose a preparatory fifth stage suggesting that students should learn and be prepared to implement adult learning principles and Kolb's experiential learning cycle. They state that students should identify their roles and responsibilities prior to commencing training to give them confidence in seeking out concrete experiences. Students also need to understand that they must act within their boundaries and to be certain that clients understand their level of training; experiences must be appropriate for the training level.
Schön's Reflective Learning Theory
Schön's reflective learning theory (18) specifically addresses learning in contexts of uncertainty, working in the “swamp” with messy and confusing problems. The veterinary workplace is swamp-like, it can be unpredictable and difficult to see a clear path to take to solve patients' problems. Clinical cases presented are often not as the textbook would describe but are unique and might require improvisation. Schön theorises that practitioners work in the “indeterminate zones of practice,” characterised by this uncertainty, uniqueness, where values might conflict, and “technical rationality” can fall down. Schön developed the concept of the “reflective practitioner” to help students acquire the kind of artistry essential to professional competence in these indeterminate zones of practice.
Firstly, we consider “reflecting in action,” where, without interrupting action, thinking reshapes the action. “Reflecting in action” can be likened to trial and error, but successive trials have an immediate significance for the next action; they are iterative, and trials are not performed at random. A good example would be a veterinary student making attempts at venepuncture, redirecting the needle each time based upon their quick reflections in the action. Students will also need to be prepared for performing the on-the-spot experiments of “reflecting in action” in the workplace by putting their knowledge to the test in other contexts. An example would be the recognition of clinical signs or proposing treatment options for a disease known in one species to another.
Secondly, we consider “reflecting on action,” the “stop and think” phase, where practitioners reflect later, after an event. Schön explains that it is crucial that a learner thinks about the processes that they have used and the extent to which they were appropriate. In the veterinary workplace reflecting on action can be facilitated using reflective journals or portfolios in addition to feedback from supervisors.
Schön theorises that reflective practice (both in and on action) becomes a vehicle for learning effectively in the professional environment and may be integrated into future “knowing in action” or “professional artistry” (11). Students will need to graduate omnicompetent not omniscient, it is not possible to know everything (21), and reflection is key to managing this insurmountable challenge. In other words, without reflection contextual learning will be trapped in the precise context in which it was learnt. Reflection is evidently something that students must be prepared for.
Knowles' Andragogy
With roots in humanistic psychology, the foundation of Knowles' somewhat controversial andragogy was initially to distinguish between the ways in which children and adults learn (pedagogy vs. andragogy) (17). Many authors have argued that the dichotomisation of andragogy and pedagogy is unfounded, lacking a conceptual basis and empirical evidence; children and adults do not necessarily learn differently because of their age. Andragogy is presented as a series of assumptions about the adult learner (Table 2), and it is argued by some that it's neither a true learning theory nor a proven educational method (4, 22, 23). Nonetheless, andragogy is stated in terms of the learners' behaviour as opposed to teachers' actions, and therefore could be utilised to infer how students might be prepared for WCT.
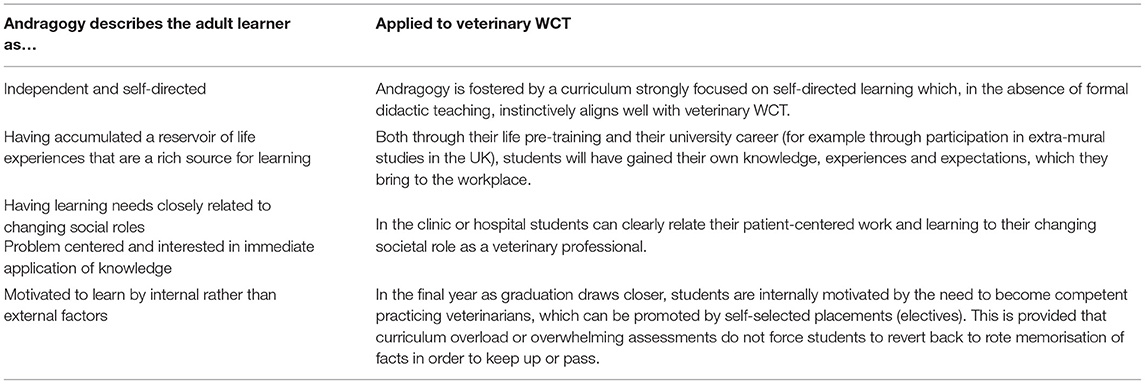
Table 2. The assumptions of andragogy applied to veterinary workplace clinical training (WCT).
In work by Matthew et al. (24, 25) a cohesive conception of WCT learning by veterinary students (learning the contextual variation that affects the management of cases in real-world veterinary practice) was associated with deep learning approaches. These approaches were strongly andragogical; they emphasised independent, reflective and self-directed learning alongside intrinsic motivation and satisfaction in progressing towards competency in practice. Veterinary students adopting such an approach performed better in assessments of WCT, which were an indicator of practice readiness. This provides evidence of the importance of these andragogical approaches, which students should be prepared with.
In an “adult” classroom, learners should feel accepted, respected and supported with a spirit of joint enquiry between teachers and students (17). Therefore, in addition to internal motivation and self-directed learning skills, students should be prepared for the dynamics of the relationship with their educators to change with the transition to WCT. Instead of being presented with information by lecturers, students should feel prepared to be part of the clinical team, solving problems alongside their teacher clinicians.
Threshold Concepts
When considering student preparedness for WCT, Meyer and Land's threshold concepts offer promise as a useful tool (26, 27). Likened to a portal, threshold concepts are ideas that are necessary for a student to possess in order to progress in their learning, and eventually enable them to think like a professional. They are transformational and change the way that the student thinks about a concept, not just what they know about it. Threshold concepts could be thought of as keys to preparedness for the next stage of learning, or which allow students to participate effectively in the workplace.
Attempts have been made to examine threshold concepts in veterinary education (28). Pharmacology and neurology areas were identified as the most challenging subjects across the entire curriculum in two separate schools, which is part-way towards classification as a threshold concept. However, the study was unable to determine any areas that once understood transformed students' way of thinking or professional development, and therefore could not identify any legitimate threshold concepts.
Threshold concepts have been assessed in human medicine (29–31). Bhat et al. (29) describe nine threshold concepts that junior trainees may encounter during an internal medicine rotation (Figure 1). Additionally, working with uncertainty, considering the bigger picture, not needing to know everything and professional culture have been identified as threshold concepts for professionalism learning in undergraduate medicine (31). These could be considered as candidate preparedness characteristics for veterinary WCT.
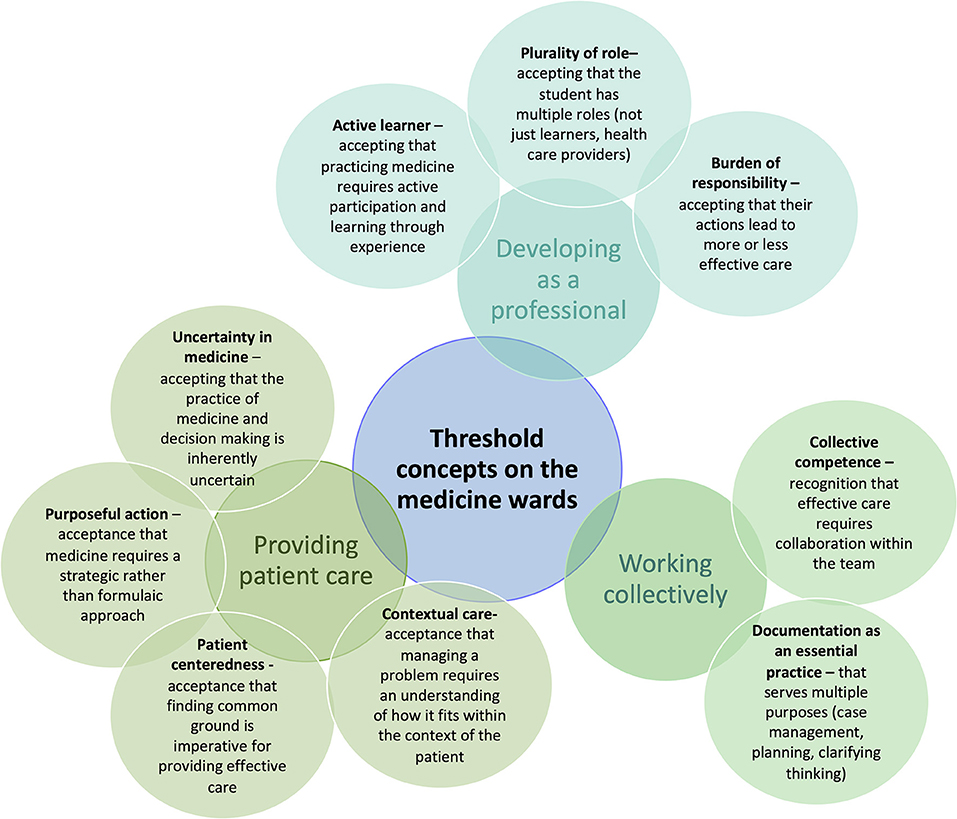
Figure 1. Threshold concepts encountered by junior trainees on an internal medicine rotation, content from Bhat et al. (29).
Gaunt and Loffman (32) explain that medical students should be prepared to seek out opportunities to tackle threshold concepts. If students understand that by accomplishing threshold concepts, they will unlock new ways of thinking previously closed off to them, it will create more confident and curious learners with a professional mindset that can succeed in the workplace.
Social Constructivist Theories
Like cognitivism, in social constructivism focus remains on the individual's internal mind. However, social constructivism contrasts with the independent learning embedded in much of the cognitivist theories and formal, classroom based, veterinary education; these theories explore how learning can be shaped by the engagement of experience with others.
Vygotsky's Zone of Proximal Development
Through his work to describe the zone of proximal development (ZPD), Vygotsky is a key contributor to social constructivism (33). He depicts the ZPD as the gap between (1) a students' actual developmental level, which is their proven, independent mental function and (2) the level of potential development which can be established by problem-solving under the guidance of, or in collaboration with, more capable others (33).
There are three key features of the ZPD theory that can be taken forward into WCT (34). Firstly, the use of “tools” to “mediate” learning. Using patients as a scaffold for learning is the central tenet of WCT and they are fundamentally a teaching tool. Using diagnostic images, laboratory results or case notes would be other physical examples, but tools can also be symbolic such as mnemonics to help remember differential diagnoses. Secondly, identifying learners' actual developmental level and their learning potential. Students could prepare for their placements by considering and even communicating their actual developmental level, and identify gaps in their knowledge or skills, which is expected by veterinary clinical supervisors (35). Thirdly, students should prepare to learn from the entire clinical team. If one locates learning in the social arena of a workplace, a whole community (veterinary surgeons, nurses, receptionists) opens up to assisting with navigation across the ZPD. The value of near-peer education also aligns well with the social nature of Vygotsky's theory, particularly when considering preparing for transitions to new working environments. The “student grapevine” (acquiring information from students who have previously experienced that WCT environment) has been identified in both the medical (36, 37) and veterinary (35, 38) settings.
Socio-Culturalist Theories
Learning in complex and dynamic systems such as the veterinary workplace cannot be wholly explained by cognitive or constructivist theories alone and is perhaps best understood from a socio-cultural viewpoint. Socio-cultural learning theories underlie the learning-as-participation metaphor (as opposed to learning-as-acquisition) (39). The goal is the full, authentic participation in the work of a community, which has a striking resemblance to the aims of veterinary WCT.
Situated Learning Theory
Lave and Wenger (40) conceived situated learning theory which draws together the learner, their activity and their world as “mutually constitutive.” Learning is a process of participation in “communities of practice,” that is “legitimate” and at first “peripheral” but that gradually increases in engagement and complexity. The learning is embodied in the everyday activity of the community and knowledge is co-constructed through participation and social interaction. An expansion of these key terms in situated learning theory are presented in Supplementary Item One (40, 41).
Steven et al. (42) demonstrated that medical clerkship students learn from real patients by participating in patient care within an educational practice. The students participated in two communities of practice: education and patient care (Figure 2). In some cases, clinical care was provided but no teaching took place and students were unable to learn from the practice, in other cases, students learnt and/or were taught but patient care was not contributory. In education within patient care, students learnt from patient care without intentional teaching. This represents situated learning. In a similar way, undergraduate veterinary students are assigned to various teaching sites (and communities of practice) throughout their clinical training where they are immersed in the work of patient care, to a greater or lesser extent.
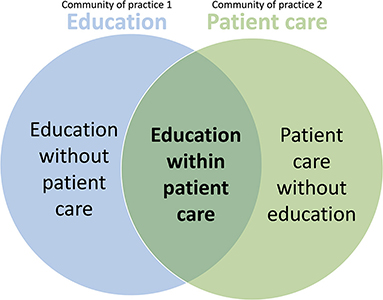
Figure 2. The two communities of practice that medical clerkship students participate in (education and patient care). Situated learning occurs when patient care created learning opportunities, which were enriched when practitioners intentionally supported participants' learning (42).
How clinical students learn from real patients in veterinary workplace settings has not been examined prospectively through the lens of situated learning theory but is discussed from a veterinary perspective by Scholz et al. (5). Despite the lack of research, there are facets of veterinary WCT which seem to align well with situated learning theory. First and foremost, veterinary students should broadly be legitimate peripheral participants in a community of practice during WCT (5). Secondly, it is recognised that veterinary students learn from the formal (intended and scheduled), informal (opportunistic) and hidden curricula of the veterinary workplace (43–47). The hidden curriculum is the “underbelly” of practice and training (47), the unwritten information that is tacitly absorbed by students from their environment, particularly what it's like to be a professional in the workplace (enculturation), which is a central tenet of situated learning. Thirdly, students do have increasing levels of responsibility in the workplace as learning occurs and trust develops within the community of practice and they should be genuinely regarded as part of the team. They demonstrate what they have learned through exhibiting competency, externalising rather than internalising knowledge. In an ideal world, veterinary schools would like students' participation to be authentic, and they should take part in all kinds of activity. They should not be “sequestered” away and left to learn abstract knowledge.
Steven et al. (42) describe how practitioners supported students' learning and verbal communication was identified as critical for this. The nature and quality of learning were dependent on clinicians entering a dialogue with students linked to patient care. Scholz et al. (5) and King et al. (48) also highlight the importance of language in veterinary WCT, which is fundamentally a social enterprise. Participants learn both the technical terminology of the sciences alongside the tacit tone and language required for communicating successfully with clients and colleagues in various contexts, for example on the farmyard, in the consultation room, in theatre or the staff room. The importance of language and the way in which WCT students use it is reflected in the emphasis now placed on communication skills in modern veterinary curricula (49–53).
Situated learning theory provides a detailed model for how students might learn during WCT and there are several facets from which suitable student preparation can be deduced, which are discussed in Table 3.
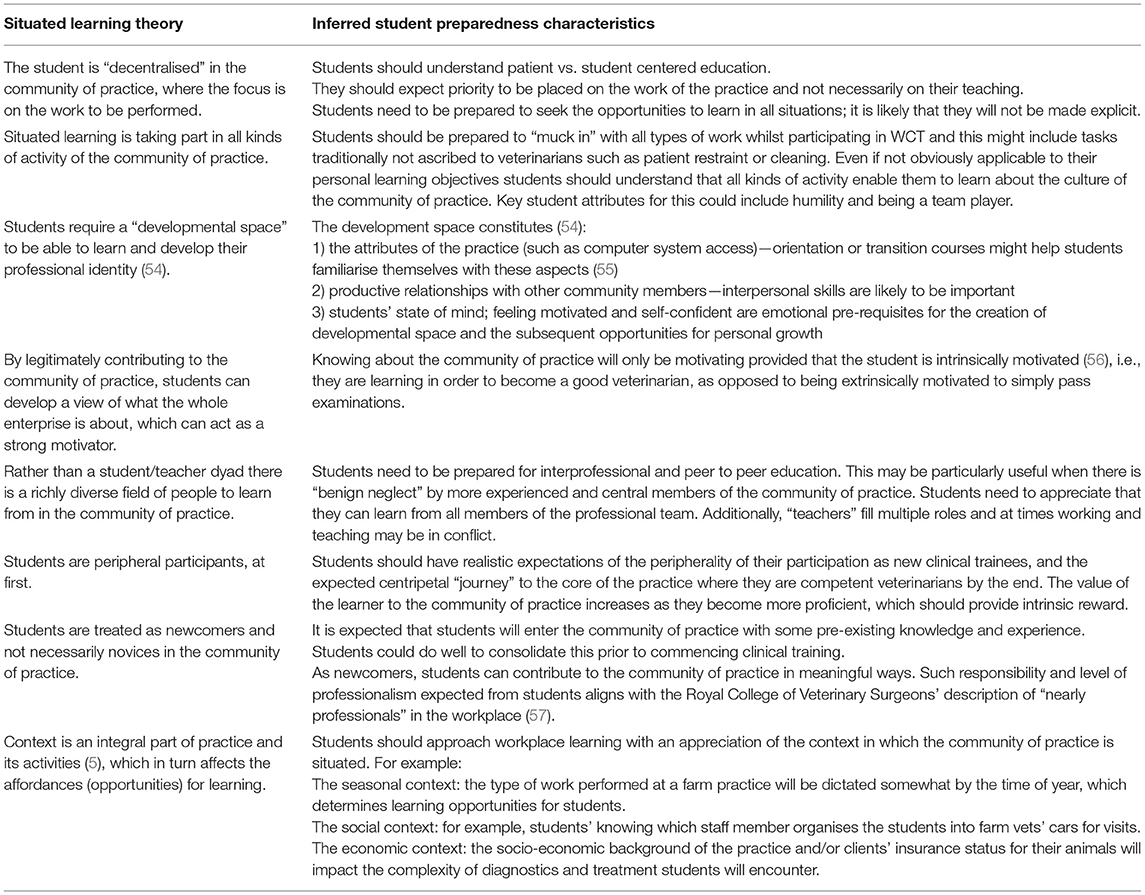
Table 3. How can we use situated learning theory to inform valuable student preparedness characteristics for workplace clinical training (WCT)?
Situated learning in communities of practice has developed greatly since its conception (58). This occurs frequently with learning theories, which aren't static, but are tested, refined and evolve. As an example, Wenger-Trayner et al. (59) introduced the concept of a “landscape of practice” as a system of communities of practice. An example would be the veterinary profession with its constituent communities of practice (veterinary practices, regulatory bodies, veterinary schools, research communities). Professional “knowledgeability” has been introduced as the ability of a practitioner to transform what they know about all the different communities of practice to produce meaningful action (for example the delivery of veterinary care) in their own community of practice. If knowledgeability is valued in our landscape of practice, this could have implications for inter-professional education (60), professional identity formation and evidence-based veterinary medicine. Although this development in situated learning theory doesn't intuitively inform preparedness for WCT, it does highlight the requirement for educators to be alert to these developments and their implications for their practice.
Cultural Historical Activity Theory
Cultural Historical Activity Theory, which is also referred to as activity theory or CHAT, focuses on goal-directed joint activity (22). In this context, activity is not only what and how the subject is performing, but why (termed the object). A key way in which it is different to the other socio-cultural theories is that the intended goal of learning does not align well with Sfard's learning-as-participation, nor learning-as-acquisition metaphors (39, 61). Instead, the goal is the expansive transformation of systems; deliberate change that results from tensions arising within a system.
Activity theory takes root in Vygotsky's triad of human-mediated activity in which “activity” represents the basic unit of analysis (33). The triad consists of a subject (the student, the veterinary surgeon), mediating tools (e.g., patients, diagnostic images) and an object (e.g., preparing future veterinarians, treating patients). In its second-generation form, Engeström describes activity theory as a conceptual framework for describing the interactions of people, the tools that they use and the rules within complex “activity systems” (62–64). The key terms of activity theory are expanded in Supplementary Item Two (62–64).
The third generation of activity theory exists where multiple activity systems interact and compete (62, 65, 66) (Figure 5). An example would be the activity systems of the classroom-based veterinary school and the clinical teaching facilities that host students. Whilst participants have a shared outcome (veterinary education), the ways in which they mediate their activity and the communities in which they occur are different. Preparedness for the transition from one activity system to the other (“boundary crossing”) should consider to what extent students can make sense of the teaching practices used in each system, and identify and react to the changing cultures and rules in their new environment (68). We can consider boundary-crossing artefacts, e.g., communication skills practice using actors in the classroom, or clinical skill simulation in the workplace, as potentially useful in preparing for this transition (68).
Another relevant example of two activity systems in competition would be “student as learner” and “student as veterinary care provider” systems. When veterinary students are both working and learning in the workplace these activity systems have overlapping but not fully aligned outcomes (Figure 3). An instance of tension would be when a student has the desire to develop a specific skill (object) in order to become a competent veterinarian (outcome), but they do not want to cause the patient or client undue inconvenience by practising with them (a competing object in a different activity system, with the outcome of patient care) (35, 66). Simultaneously the student may feel pressure to display their competence in the skill to the clinical supervisor to achieve a good assessment result (another outcome).
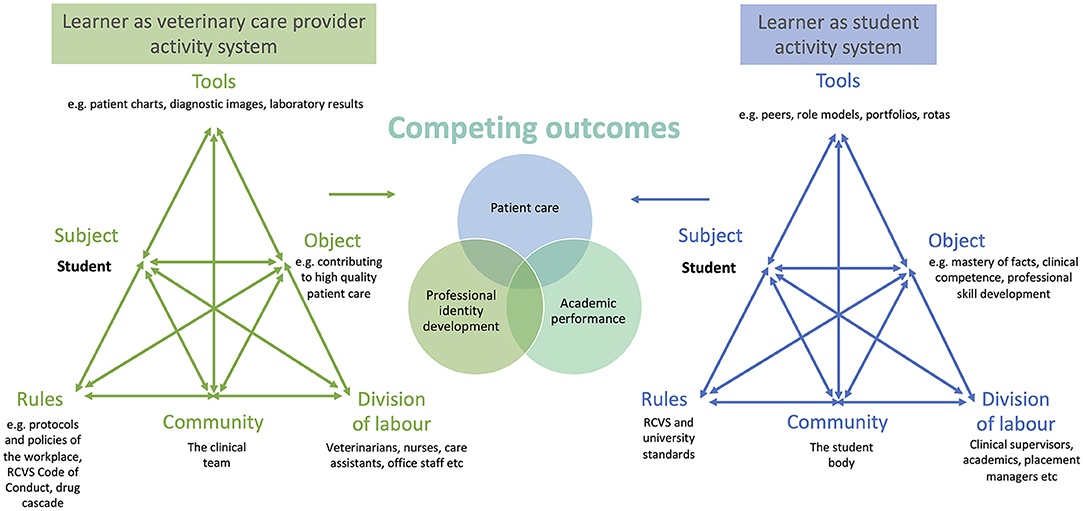
Figure 3. Adapted with permission from Larsen et al. (65) for the veterinary WCT context. The clinical veterinary student in the workplace is part of several activity systems, between which there may be interaction or tensions and competing outcomes. RCVS, Royal College of Veterinary Surgeons.
However, these tensions are creative forces for change (69). To overcome them, new ways of acting or new objects can be developed in the workplace and this process is termed expansive learning (70). In the above example, the clinical supervisor could help the student to identify amenable patients to practice with and facilitate getting consent.
Using written learning goals for clinical workplace training has been described as a tool to overcome tensions in the medical workplace (65, 66) and several desirable preparedness characteristics could be assumed from this work. Larsen et al. identified that student engagement with and commitment to goals were important and that students should understand that they can use learning goals to negotiate the demands faced in the workplace. This may include prioritising who or what they observe and take part in, reflecting on how their time is best used and acknowledgement that a degree of proactivity is required to create opportunities for participation. However, the vicissitude of daily practice needs to be acknowledged and a realisation that the learning goals of the student will not necessarily match the needs of the patients that walk in through the door. Some supervisors identified broader goals to be useful; these were seen as tools for leveraging greater learning opportunities because as they fit many more scenarios.
Experience Based Learning
Dornan et al. explored the pedagogic principles that underlie rotation based medical clerkships (analogous to veterinary WCT), and from it developed Experience Based Learning (ExBL) theory (Figure 4) (71, 72). The theory clearly draws on the higher communities of practice theory from Lave and Wenger (40) but is applied to the clinical setting resulting in a middle-range theory grounded in empirical findings.

Figure 4. Experience based learning theory adapted with permission from Dornan et al. (71).
The theory states that medical students learn during clerkships as a result of “supported participation in practice” (71, 73). Participation is embedded within triadic relationships between the student, clinical supervisors, and their patients in authentic workplaces. Within the triad, the student can have an observatory (passive or active) or actor-like (in rehearsal or in performance) role (Figure 4). Unlike in Lave and Wenger's (40) communities of practice, teaching is observable and does contribute to ExBL, however, it is not a central or defining feature. Participation is always supported, and it is provided in three ways: pedagogic, affective, and organisational support (Figure 4). Participation is rooted in “real patient learning,” a critical process that results in both practical (proficiency) and affective outcomes, but it is also a learning outcome in itself. These outcomes contribute to professional identity development. How these outcomes can be used to inform the preparation of veterinary students for “supported participation in practice” is discussed in Table 4.
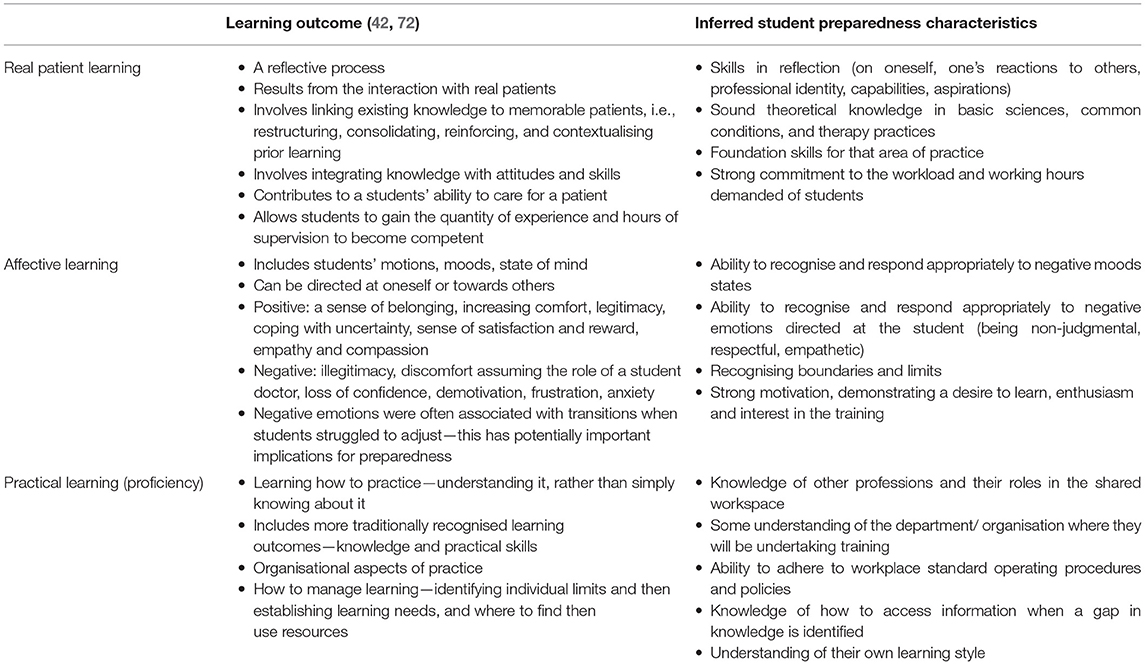
Table 4. How can experience based learning (ExBL) theory outcomes be used to inform valuable preparedness characteristics for veterinary workplace clinical training (WCT)?
Organisational Socialisation Theory
Organisational socialisation theory describes the way in which newcomers move from being organisational outsiders to organisational insiders (67). It incorporates the process by which new members learn the knowledge, skills and behaviours they need to succeed in their new environment. It is distinct from the process of occupational socialisation which describes professional identity formation. Organisational socialisation theory is important to consider because students are embedded in social organisations during WCT and the transition into it reflects the effectiveness of the programme in preparing students.
Organisational socialisation theory has been utilised by Atherley et al. (37) to explore how medical students transition within their rotational clinical training, additionally it has been applied to nursing graduates entering the clinical workplace (74). The first phase of the theory has three components (67): newcomer characteristics, newcomer behaviours and organisational efforts. This is followed by an adjustment phase, leading to newcomer outcomes (Figure 5).
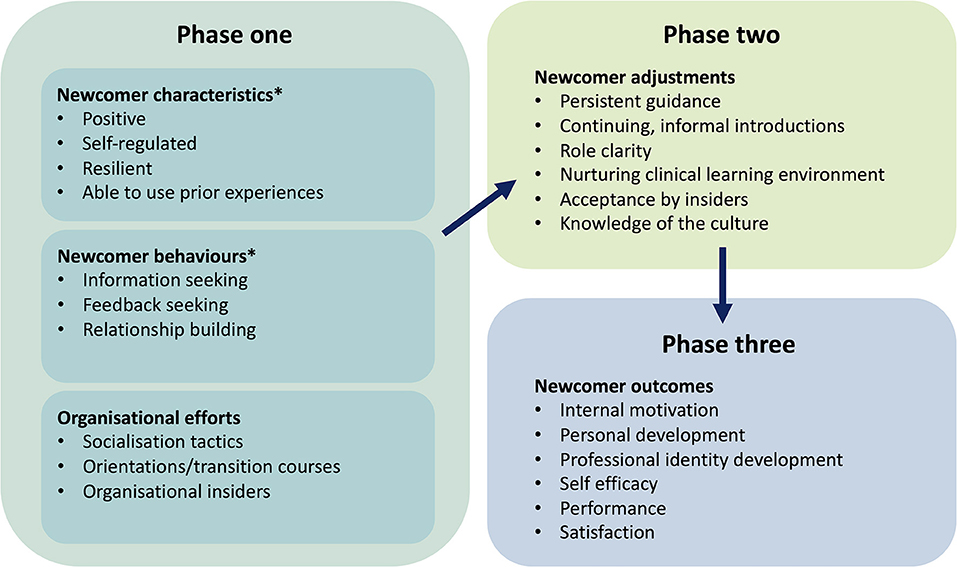
Figure 5. Organisational socialisation theory. Adapted from Atherley et al. (37) and Bauer & Erdogan (67). *Newcomer characteristics and behaviours align particularly well to preparedness for workplace clinical training (WCT).
Newcomer characteristics and behaviours directly align with preparedness for entering the workplace. Through student focus groups and open-ended written questions, Atherley et al. (37) found that students recognised the need to commence a placement with proactivity, positivity and the ability to build productive relationships. Students were required to ignore the reputation that preceded the rotation [via the “student grapevine” (36)] to achieve this, or risk anxiety prohibiting learning. Peer-to-peer preparation for veterinary WCT has also been identified as conceivably problematic given the potential for the transmission of misconceptions (35). Many students were concerned about their role as part of the medical team and clarification would have been useful in preparation. Only a few students looked forward to feedback-seeking but those that did thought it would be useful in the transition. It was also suggested that targeting skills such as self-regulated learning [goal-setting, self-monitoring and self-reflection (75)] and resilience in the pre-clinical phase may prove useful in developing proactivity and feedback-seeking behaviour.
Billet's Theory of Workplace Affordances and Individual Engagements
Billet's theory of workplace affordances and individual engagements identifies the factors that shape learning in workplaces (76–78). It is centered on co-participation, and the duality of how the workplace invites access to activities and guidance (workplace affordances) but also how individuals elect to participate in what the workplace affords (individual engagements).
King et al. (48) developed a constructivist grounded theory to understand how veterinary students interact in the workplace and Billet's workplace affordances and individual engagements provided a conceptual orientation for the work. The resulting theory “Learning to Interact and Interacting to Learn” (LIIL) has a central concept of harnessing dialogue. Students came to understand that the way in which they engaged in dialogue influenced three inter-related processes (1) contributing to the daily functioning of the workplace, (2) the impressions that others had of them and (3) learning in the moment, acquiring specific skills or knowledge whilst working. They established that some students had to learn to interact more effectively, to be able to learn from interactions. Preparation of veterinary students for learning in the workplace could therefore include building social discourse awareness to enable students to perceive how best to find learning opportunities through interaction.
The work by King et al. shines a light on the importance of learner agency; how veterinary students elect to engage with workplace activities. Billet explains that learning new knowledge is an active, demanding process; individuals must be prepared to engage actively and deliberately seek to improve performance. This process includes self-directed learning, interacting with others, objects, and artefacts, and perceptively seeking clues from the social and physical environment for arising opportunities, and then monitoring progress during task completion.
Additionally, veterinary students might elect to engage actively in some components of activities but less actively (and even resentfully) in others, often simultaneously. It is also likely that individuals' interests and priorities will mediate their participation in work. This is perhaps enhanced by the fact that veterinary students, at the time of WCT, are likely to have species-specific career aspirations, which according to Billet's theory may influence the effort they expend on each rotation. Given that full-bodied engagement by individuals is likely to be required to develop robust vocational practices, we can infer that veterinary students should engage with all opportunities with equal enthusiasm and endeavour, despite any influence of their individual interests.
Discussion: Inferences About Student Preparedness
No single theory of learning can adequately explain the process of WCT in its entirety or in all its detail, each one magnifies certain aspects of the world, and possibly distorts or hides other aspects. However, by considering a number of theories, principles and models a framework of learning can be constructed, which can be used to inform different components of WCT preparedness and as a reference for discussion. It is important to acknowledge that although the authors have attempted to be wide-ranging in their selection of learning theories to review, it is not complete, and there are other relevant learning theories that one might consider with respect to clinical education (such as Zimmerman's Self-regulated Learning Theory). We should also recognise that these theories describe what should or could happen in ideal circumstances, and it cannot be assumed that every clinical training experience will be like this. Extensive research using objectivist deductivist approaches will be required to confirm how well, or how poorly, the learning theories approximate veterinary WCT in reality (13).
All learning theories have been subjected to critique by the research community, but cognitivism and social constructivism, in particular, have some limitations in providing an adequate account of workplace learning that are worthy of acknowledgement. If only examined through the lens of cognitivism, learning in the workplace would be understood as concerned with only the individual, as an essentially unmediated activity (learners engaging with their own experience with little input from others), independent of context, unproblematic, and with learning treated as a “thing” (which lends itself to the knowledge acquisition and transfer metaphors). Additionally, from the perspective of cognitivism, the performance of work consists of thinking and then the application of this thinking and the role of social or cultural factors are, at best, a background feature of workplace learning, and are underestimated. Similarly, social constructivism still ignores the context in which learning takes place, which we believe to be important. The ZPD ascribes a label to something clinical educators are probably already aware of: that students know what they know and, with their help, can progress to a more advanced level. However, the theory doesn't add detail about how this might be achieved. Additionally, like cognitivism, the ZPD remains individualistic and describes teaching on a one-to-one basis and so fails to account for group learning which occurs in the workplace.
It is intuitive that WCT is best understood from a socio-cultural perspective. However, there is very little published putting these theories to work in veterinary education and much of the content discussed here draws on observations and analysis of medical clerkships. It is reasonable to deduce that similarly veterinary WCT is shaped by experience as a peripheral participant within a community of practice. Students can be seen as boundary crossers who are engaged with the objects of two activity systems (student-as-learner and student-as-worker). Through observing, rehearsing and performing students achieve affective and practical learning outcomes alongside real patient learning. Organisational socialisation theory suggests that newcomer characteristics, behaviours and adjustments could help students to transition to workplace learning proficiently. Some aspects of cognitivism are also instinctively important for veterinary clinical trainees: grasping threshold concepts such as patient-centeredness and uncertainty and risk in decision making, reflecting in and on action and conducting their training in an andragogical manner.
Being prepared for WCT and the student's ability to learn is not limited by their actual development level (33); students can possess sufficient prior knowledge but fail to learn in workplaces (79). This is because competence in WCT is likely to be highly contextualised (80); it is fundamentally affected by the activity, organisational practices and culture of that particular workplace (81). In other words, some responsibility for students' competence must be placed on the workplace itself and other members of the community of practice. Preparedness is also individualised and fluctuates over time (82). For these reasons, it is not possible to be fully prepared for a transition into WCT, and it should be viewed as a “critically intensive learning period” instead (81). However, by understanding how students learn from WCT using learning theory, we can deduce how students could be placed in the best position to learn from those experiences, i.e., what tools can they possess to be best prepared?
“A conceptual framework is the end result of bringing together a number of related concepts to explain or predict a given event, or give a broader understanding of the phenomenon of interest” [(83), p. 189]. Using this narrative review we have developed a new conceptual framework, the “Preparedness Toolkit” as a useful way to think about our phenomenon of interest: preparedness for WCT (Figure 6). The “Preparedness Toolkit” contains “tools” derived from the learning theories explored in this paper (as detailed by the colour key). We propose that if possessed and put to work by the veterinary student, these “tools” will assist them in learning and working at the expected level during WCT, whilst negotiating the critically intensive learning period. In other words, it will facilitate their competency (actual performance).
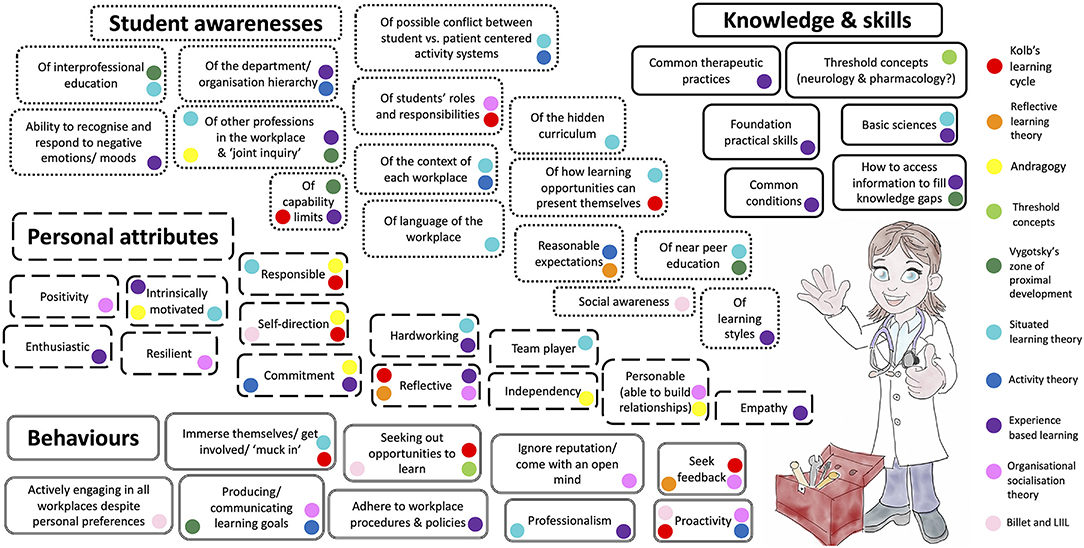
Figure 6. The veterinary clinical trainee preparedness toolbox contains the preparedness characteristics, derived from an understanding of relevant learning theory, which could be utilised to engage with, and learn from, the veterinary workplace by undergraduate veterinary students (LIIL, Learning to Interact, Interacting to Learn).
This conceptual framework is only the start of a scholarly conversation; it can be used in future research to support data collection and analysis about student preparedness for WCT. This research will be theoretically grounded in a novel way; drawing on many theories to produce a conceptual framework of preparedness for WCT de novo. It is only after this validity evidence has been gathered to support its existence should the “Preparedness Toolkit” be considered for implementation in the preparation of students for WCT. A further extension of the conceptual framework would be to generate “tools” for the other members of the community of practice (for example clinical supervisors), and the workplace environment itself, to facilitate students' WCT experience.
Author Contributions
JR, SP, PC, VN, and KJ contributed to the conception of the manuscript. JR wrote the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
Funding
JR's doctoral studies, to which this work contributes, is sponsored by the Longhurst Legacy (University of Surrey).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fvets.2022.833034/full#supplementary-material
References
1. Billay D, Myrick F. Preceptorship: An integrative review of the literature. Nurse Educ Pract. (2008) 8:258–66. doi: 10.1016/j.nepr.2007.09.005
2. Shipengrover JA, James PA. Measuring instructional quality in community-orientated medical education: looking into the black box. Med Educ. (1999) 33:846–53. doi: 10.1046/j.1365-2923.1999.00480.x
3. Dale VHM, Sullivan M, May SA. Adult learning in veterinary education: Theory to practice. J Vet Med Educ. (2008) 35:581–8. doi: 10.3138/jvme.35.4.581
4. Parkinson TJ. George AM. Are the concepts of andragogy and pedagogy relevant to veterinary undergraduate teaching? J Vet Med Educ. (2003) 30:247–53. doi: 10.3138/jvme.30.3.247
5. Scholz E, Trede F, Raidal SL. Workplace learning in veterinary education: a sociocultural perspective. J Vet Med Educ. (2013) 40:355–62. doi: 10.3138/jvme.0113-015R
6. Meehan MP, Menniti MF. Final-year veterinary students' perceptions of their communication competencies and a communication skills training program delivered in a primary care setting and based on Kolb's Experiential Learning Theory. J Vet Med Educ. (2014) 41:371–83. doi: 10.3138/jvme.1213-162R1
7. Barron D, Khosa D, Jones-Bitton A. Experiential learning in primary care: impact on veterinary students' communication confidence. J Experi Educ. (2017) 40:349–65. doi: 10.1177/1053825917710038
8. King E. Learning to Interact and Interacting to Learn: A Grounded Theory of Clinical Workplace Learning for Diverse Cohorts. Brisbane, QLD: The University of Queensland (2020).
9. Moore DA, Leamon MH, Cox PD, Servis ME. Teaching implications of different educational theories and approaches. J Vet Med Educ. (2002) 29:117–23. doi: 10.3138/jvme.29.2.117
10. Schoenfeld-Tacher R, Baker HJ. Educational theory and practice. J Vet Med Educ. (2013) 40:94–5. doi: 10.3138/jvme.0313-051
11. Kaufman DM. Teaching and learning in medical education: how theory can inform practice. In: Swanwick T, Forrest K, O'Brien B, editors. Understanding Medical Education: Evidence, Theory and Practice. Third ed. Hoboken, NJ: Wiley-Blackwell. (2019) p. 37–69. doi: 10.1002/9781119373780.ch4
12. Burford B, Vance G. When I say … preparedness. Med Educ. (2014) 48:849–50. doi: 10.1111/medu.12427
13. Varpio L, Paradis E, Uijtdehaage S, Young M. The distinctions between theory, theoretical framework, and conceptual framework. Acad Med. (2020) 95:989–94. doi: 10.1097/ACM.0000000000003075
14. Bordage G. Conceptual frameworks to illuminate and magnify. Med Educ. (2009) 43:312–9. doi: 10.1111/j.1365-2923.2009.03295.x
15. Teunissen PW. Trust your struggle. Perspect Med Educ. (2016) 5:69–70. doi: 10.1007/s40037-016-0259-3
16. Kolb DA. Experiential Learning: Experience as the Source of Learning and Development. Englewood Cliffs, NJ: Prentice Hall (1984).
17. Knowles MS. The Modern Practice of Adult Education: From Pedagogy to Andragogy. Rev. &Updated. ed. Englewood Cliffs, NJ: Cambridge Adult Education (1980).
18. Schön DA. Educating the Reflective Practitioner: [Toward a New Design for Teaching and Learning in the Professions]. San Francisco: Jossey-Bass (1987).
19. Warman SM, Laws EJ, Crowther E, Baillie S. Initiatives to improve feedback culture in the final year of a veterinary program. J Vet Med Educ. (2014) 41:162–71. doi: 10.3138/jvme.1013-142R
20. Greenberg L, Blatt B. Perspective: successfully negotiating the clerkship years of medical school: a guide for medical students, implications for residents and faculty. Acad Med. (2010) 85:706–9. doi: 10.1097/ACM.0b013e3181d2aaf2
21. Pew National Veterinary Education Program. Future directions for veterinary medicine: The Pew report Pew National Veterinary Education Program. Canad Vet J. (1989) 30:472–6.
22. Yardley S, Teunissen PW, Dornan T. Experiential learning: AMEE Guide No. 63. Med Teach. (2012) 34:e102–15. doi: 10.3109/0142159X.2012.650741
23. Merriam SB. Andragogy and self-directed learning: pillars of adult learning theory. New Direct Adult Continuing Educ. (2001) 2001:3–14. doi: 10.1002/ace.3
24. Matthew SM, Taylor RM, Ellis RA. Students' experiences of clinic-based learning during a final year veterinary internship programme. Higher Educ Res Dev. (2010) 29:389–404. doi: 10.1080/07294361003717903
25. Matthew SM, Ellis RA, Taylor RM. Evaluating the quality of veterinary students' experiences of learning in clinics. J Vet Med Educ. (2017) 44:369–80. doi: 10.3138/jvme.0516-094R
26. Meyer J, Land R. Threshold concepts and troublesome knowledge (2): epistemological considerations and a conceptual framework for teaching and learning. Higher Educ. (2005) 49:373–88. doi: 10.1007/s10734-004-6779-5
27. Meyer J, Land R. Threshold concepts and troublesome knowledge: Linkages to ways of thinking and practising within the disciplines. In: Rust C, editor. Improving Student Learning: Improving Student Learning Theory and Practice - Ten Years On. Oxford: Oxford Centre for Staff and Learning Development. (2003).
28. Rhind SM, Warman S, Paterson J, Hughes KJ, Hammond J. Short Communication: An Exploration of Threshold Concepts in the Veterinary Curriculum. Bristol: VetEd Symposium (2014).
29. Bhat C, Burm S, Mohan T, Chahine S, Goldszmidt M. What trainees grapple with: a study of threshold concepts on the medicine ward. Med Educ. (2018) 52:620–31. doi: 10.1111/medu.13526
30. Neve H, Wearn A, Collett T. What are threshold concepts and how can they inform medical education? Med Teach. (2016) 38:850–3. doi: 10.3109/0142159X.2015.1112889
31. Neve H, Lloyd H, Collett T. Understanding students' experiences of professionalism learning: a ‘threshold' approach. Teach Higher Educ. (2017) 22:92–108. doi: 10.1080/13562517.2016.1221810
32. Gaunt T, Loffman C. When I say… threshold concepts. Med Educ. (2018) 52:789–90. doi: 10.1111/medu.13537
33. Vygotsky LS. Mind in Society: The Development of Higher Psychological Processes. Cambridge, MA: Harvard university press (1978). doi: 10.2307/j.ctvjf9vz4
34. Morris C. Work-based learning. In: Swanwick T, Forrest K, O'Brien B, editors. Understanding Medical Education: Evidence, Theory and Practice. Third ed. Hoboken, NJ: Wiley-Blackwell. (2019) p. 163–77. doi: 10.1002/9781119373780.ch12
35. Magnier K, Wang R, Dale VHM, Murphy R, Hammond RA, Mossop L, et al. Enhancing clinical learning in the workplace: a qualitative study. Vet Rec. (2011) 169:682. doi: 10.1136/vr.100297
36. Masters DE, O'Brien BC, Chou CL. The third-year medical student “grapevine”: managing transitions between third-year clerkships using peer-to-peer handoffs. Acad Med. (2013) 88:1534–8. doi: 10.1097/ACM.0b013e3182a36c26
37. Atherley AE, Hambleton IR, Unwin N, George C, Lashley PM, Taylor CG. Exploring the transition of undergraduate medical students into a clinical clerkship using organizational socialization theory. Perspect Med Educ. (2016) 5:78–87. doi: 10.1007/s40037-015-0241-5
38. Royal Veterinary College,. Online Induction Video Educational Resource (OLIVER). (2011). Available from: https://oliver.live.ac.uk (accessed January 15, 2021).
39. Sfard A. On two metaphors for learning and the dangers of choosing just one. Educ Res. (1998) 27:4–13. doi: 10.3102/0013189X027002004
40. Lave J, Wenger E. Situated Learning: Legitimate Peripheral Participation. Cambridge: Cambridge University Press (1991). doi: 10.1017/CBO9780511815355
41. Wenger E. Communities of Practice: Learning, Meaning, and Identity. Cambridge: Cambridge University Press (1998). doi: 10.1017/CBO9780511803932
42. Steven K, Wenger E, Boshuizen H, Scherpbier A, Dornan T. How clerkship students learn from real patients in practice settings. Acad Med. (2014) 89:469–76. doi: 10.1097/ACM.0000000000000129
43. Mossop L, Dennick R, Hammond R, Robbé I. Analysing the hidden curriculum: use of a cultural web. Med Educ. (2013) 47:134–43. doi: 10.1111/medu.12072
44. Gaufberg EH, Batalden M, Sands R, Bell SK. The hidden curriculum: what can we learn from third-year medical student narrative reflections? Acad Med. (2010) 85:1709–16. doi: 10.1097/ACM.0b013e3181f57899
45. Roder CA, May SA. The hidden curriculum of veterinary education: mediators and moderators of its effects. J Vet Med Educ. (2017) 44:542–51. doi: 10.3138/jvme.0416-082
46. Whitcomb TL. Raising awareness of the hidden curriculum in veterinary medical education: a review and call for research. J Vet Med Educ. (2014) 41:344–9. doi: 10.3138/jvme.0314-032R1
47. Hafferty FW. Beyond curriculum reform: confronting medicine's hidden curriculum. Acad Med. (1998) 73:403–7. doi: 10.1097/00001888-199804000-00013
48. King E, Turpin M, Green W, Schull D. Learning to interact and interacting to learn: a substantive theory of clinical workplace learning for diverse cohorts. Adv Health Sci Educ. (2019) 24:691–706. doi: 10.1007/s10459-019-09891-8
49. Shaw JR. Evaluation of communication skills training programs at North American veterinary medical training institutions. J Am Vet Med Assoc. (2019) 255:722–33. doi: 10.2460/javma.255.6.722
50. Englar RE. A novel approach to simulation-based education for veterinary medical communication training over eight consecutive pre-clinical quarters. J Vet Med Educ. (2017) 44:502–22. doi: 10.3138/jvme.0716-118R1
51. Englar RE. Tracking veterinary students' acquisition of communication skills and clinical communication confidence by comparing student performance in the first and twenty-seventh standardized client encounters. J Vet Med Educ. (2019) 46:235–57. doi: 10.3138/jvme.0917-117r1
52. Stevens BJ, Kedrowicz AA. Evaluation of fourth-year veterinary students' client communication skills: Recommendations for scaffolded instruction and practice. J Vet Med Educ. (2018) 45:85–90. doi: 10.3138/jvme.0816-129r1
53. Sheats MK, Hammond S, Kedrowicz AA. Analysis of final year veterinary students' telephone communication skills at a veterinary teaching hospital. Vet Sci. (2018) 5:99. doi: 10.3390/vetsci5040099
54. Van der Zwet J, Zwietering P, Teunissen P, Van der Vleuten C, Scherpbier A. Workplace learning from a socio-cultural perspective: creating developmental space during the general practice clerkship. Adv Health Sci Educ. (2011) 16:359–73. doi: 10.1007/s10459-010-9268-x
55. O'Brien BC, Poncelet AN. Transition to clerkship courses: preparing students to enter the workplace. Acad Med. (2010) 85:1862–9. doi: 10.1097/ACM.0b013e3181fa2353
56. Ryan RM, Deci EL. Intrinsic and extrinsic motivations: classic definitions and new directions. Contemp Educ Psychol. (2000) 25:54–67. doi: 10.1006/ceps.1999.1020
57. Royal College of Veterinary Surgeons. Consultation on Extra-Mural Studies in the Veterinary Undergraduate Curriculum. (2009). Available online at: https://www.rcvs.org.uk/document-library/ems-consultation-paper/ (accessed October 1, 2020).
58. Farnsworth V, Kleanthous I, Wenger-Trayner E. Communities of practice as a social theory of learning: a conversation with etienne wenger. Br J Educ Stud. (2016) 64:139–60. doi: 10.1080/00071005.2015.1133799
59. Wenger-Trayner E, Fenton-O'Creevy M, Hutchinson S, Kubiak C, Wenger-Trayner B. Learning in Landscapes of Practice: Boundaries, Identity, and Knowledgeability in Practice-Based Learning. London: Taylor & Francis Group (2014). doi: 10.4324/9781315777122
60. de Nooijer J, Dolmans DHJM, Stalmeijer RE. Applying landscapes of practice principles to the design of interprofessional education. Teach Learn Med. (2021) 2016:1–6. doi: 10.1080/10401334.2021.1904937
61. Morris C. From Time-Served Apprenticeship to Time-Measured Training: New Challenges for Postgraduate Medical Education. London: University of London (2011).
62. Engeström Y. Expansive learning at work: toward an activity theoretical reconceptualization. J Educ Work. (2001) 14:133–56. doi: 10.1080/13639080020028747
63. Engeström Y. Learning by Expanding: An activity. Theoretical Approach to Develomental Research. Helsinki: Orienta–Konsultit (1987).
64. Engeström Y. Innovative learning in work teams: Analyzing cycles of knowledge creation in practice. In: Engeström Y, Miettinen R, Punamäki R-L, editors. Perspectives on Activity Theory. First ed. Cambridge: Cambridge University Press (1999) p. 377–404. doi: 10.1017/CBO9780511812774.025
65. Larsen DP, Nimmon L, Varpio L. Cultural historical activity theory: the role of tools and tensions in medical education. Acad Med. (2019) 94:1255. doi: 10.1097/ACM.0000000000002736
66. Larsen DP, Wesevich A, Lichtenfeld J, Artino Jr AR, Brydges R, Varpio L. Tying knots: an activity theory analysis of student learning goals in clinical education. Med Educ. (2017) 51:687–98. doi: 10.1111/medu.13295
67. Bauer TN, Erdogan B. Organizational Socialization: The Effective Onboarding of New Employees. APA Handbook of Industrial and Organizational Psychology, Vol 3: Maintaining, Expanding, and Contracting the Organization. APA Handbooks in Psychology®. Washington, DC: American Psychological Association (2011) p. 51–64. doi: 10.1037/12171-002
68. Morris C. From classroom to clinic: an activity theory perspective. In: Cook V, Daly C, Newman M, editors. Work-based Learning in Clinical Settings: Insights from Socio-cultural Perspectives. First ed. London, UK: Radcliffe Publishing Ltd. (2012) p. 85–102.
69. Morris C, Reid A-M, Ledger A, Teodorczuk A. Expansive learning in medical education: putting change laboratory to work. Med Teach. (2020) 2020:1–6. doi: 10.1080/0142159X.2020.1796948
70. Engeström Y, Sannino A. Studies of expansive learning: Foundations, findings and future challenges. Educ Res Rev. (2010) 5:1–24. doi: 10.1016/j.edurev.2009.12.002
71. Dornan T, Tan N, Boshuizen H, Gick R, Isba R, Mann K, et al. How and what do medical students learn in clerkships? Experience based learning (ExBL). Adv Health Sci Educ. (2014) 19:721–49. doi: 10.1007/s10459-014-9501-0
72. Dornan T, Conn R, Monaghan H, Kearney G, Gillespie H, Bennett D. Experience Based Learning (ExBL): clinical teaching for the twenty-first century. Med Teach. (2019) 41:1098–105. doi: 10.1080/0142159X.2019.1630730
73. Dornan T, Boshuizen H, King N, Scherpbier A. Experience-based learning: a model linking the processes and outcomes of medical students' workplace learning. Med Educ. (2007) 41:84–91. doi: 10.1111/j.1365-2929.2006.02652.x
74. Phillips C, Esterman A, Kenny A. The theory of organisational socialisation and its potential for improving transition experiences for new graduate nurses. Nurse Educ Today. (2015) 35:118–24. doi: 10.1016/j.nedt.2014.07.011
75. Sandars J, Cleary TJ. Self-regulation theory: applications to medical education: AMEE Guide No. 58. Med Teach. (2011) 33:875–86. doi: 10.3109/0142159X.2011.595434
76. Billett S. Learning through work: workplace affordances and individual engagement. J Workplace Learn. (2001) 13:209–14. doi: 10.1108/EUM0000000005548
77. Billett S. Toward a workplace pedagogy: guidance, participation, and engagement. Adult Educ Quart. (2002) 53:27–43. doi: 10.1177/074171302237202
78. Billett S. Learning through health care work: premises, contributions and practices. Med Educ. (2016) 50:124–31. doi: 10.1111/medu.12848
79. Schaap H, Baartman L, de Bruijn E. Students' Learning Processes During School-Based Learning And Workplace Learning In Vocational Education: A Review. Vocations Learn. (2012) 5:99–117. doi: 10.1007/s12186-011-9069-2
80. Hager P, Hodkinson P. Moving beyond the metaphor of transfer of learning. Br Educ Res J. (2009) 35:619–38. doi: 10.1080/01411920802642371
81. Kilminster S, Zukas M, Quinton N, Roberts T. Preparedness is not enough: understanding transitions as critically intensive learning periods. Med Educ. (2011) 45:1006–15. doi: 10.1111/j.1365-2923.2011.04048.x
82. Chaou CH, Yu SR, Chang YC, Ma SD, Tseng HM, Hsieh MJ, et al. The evolution of medical students' preparedness for clinical practice during the transition of graduation: a longitudinal study from the undergraduate to postgraduate periods. BMC Med Educ. (2021) 21:260. doi: 10.1186/s12909-021-02679-8
Keywords: learning theory, preparedness, preceptorship, veterinary education, workplace learning, clinical rotations
Citation: Routh J, Paramasivam SJ, Cockcroft P, Nadarajah VD and Jeevaratnam K (2022) Using Learning Theories to Develop a Veterinary Student Preparedness Toolkit for Workplace Clinical Training. Front. Vet. Sci. 9:833034. doi: 10.3389/fvets.2022.833034
Received: 10 December 2021; Accepted: 14 February 2022;
Published: 07 April 2022.
Edited by:
Deirdre P. Campion, University College Dublin, IrelandReviewed by:
Eva King, The University of Queensland, AustraliaJennifer Hammond, University of Glasgow, United Kingdom
Copyright © 2022 Routh, Paramasivam, Cockcroft, Nadarajah and Jeevaratnam. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jennifer Routh, ai5yb3V0aEBzdXJyZXkuYWMudWs=; Kamalan Jeevaratnam, ZHJrYW1hbGFuamVldmFAZ21haWwuY29t