
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Vet. Sci. , 23 September 2021
Sec. Veterinary Regenerative Medicine
Volume 8 - 2021 | https://doi.org/10.3389/fvets.2021.732073
This article is part of the Research Topic Mesenchymal Stromal- and Stem Cell-Based Applications in Livestock Species View all 7 articles
 Janko Mrkovački1†
Janko Mrkovački1† Sanja Srzentić Dražilov2†
Sanja Srzentić Dražilov2† Vesna Spasovski2
Vesna Spasovski2 Amira Fazlagić3
Amira Fazlagić3 Sonja Pavlović2
Sonja Pavlović2 Gordana Nikčević2*
Gordana Nikčević2*The management of degenerative lumbosacral stenosis (DLSS) in dogs usually requires aggressive, costly surgical treatments that may themselves present complications, while do not fully resolve the symptoms of the disease. In this study, the dog diagnosed with severe DLSS, with hind limb paresis, was treated using a new and least invasive treatment. Cultured autologous adipose tissue-derived mesenchymal stem cells (AT-MSCs) were injected bilaterally at the level of L7-S1, in the vicinity of the external aperture of the intervertebral foramen of DLSS patient. In the previously described treatments of spontaneous intervertebral disc degeneration in dogs, intradiscal injections of MSCs did not lead to positive effects. Here, we report a marked improvement in clinical outcome measures related to the ability of a dog to walk and trot, which were expressed by a numeric rating scale based on a veterinary assessment questionnaire. The improved status persisted throughout the observed time course of 4.5 years after the AT-MSC transplantation. To the best of our knowledge, this is the first case of successful therapy, with long-term positive effect, of spontaneously occurring canine DLSS using presented treatment that, we believe, represents a contribution to current knowledge in this field and may shape both animal and human DLSS treatment options.
Canine degenerative lumbosacral stenosis (DLSS) is a syndrome of low back pain that includes various levels of neurologic dysfunction, and it has been defined as an acquired narrowing of the vertebral duct, the vertebral aperture, or both, resulting in compressive radiculopathy of cauda equina (1, 2). The degeneration of the intervertebral disc (IVD) L7-S1 is thought to be the cause of DLSS that occurs as a result of prolonged stress, along with the activity and age of the animal. Namely, when the elastic and fibrous annulus fibrosus weakens, and the central, gelatinous nucleus pulposus loses its hydration, the Hansen type II protrusion of the disc occurs that leads to the loss of the intervertebral spacing (3). The loss of normal biomechanical properties of the disc and the resulting degenerative changes in the supporting soft tissue and bony structures at the lumbosacral junction are the main contributors to the compression of sacral and caudal nerve roots (3). It is important to note that dogs with a transitional vertebra have an increased risk of DLSS due to increased rotational force caused by a poor position and poor articulation of the asymmetric lumbosacral junction (3).
Current management of DLSS in dogs comprise either conservative pharmacological treatments that frequently lead to a poor response, or aggressive and expensive surgical strategies that may themselves present complications, while do not fully resolve the symptoms (3). Recently, intradiscal injections of mesenchymal stem cells (MSCs) have been investigated in naturally developed DLSS in dogs, but this therapeutic approach did not lead to improvement of the disease (4, 5). This report proposes a novel and least invasive strategy, the transplantation of autologous adipose tissue-derived MSCs (AT-MSCs) in the vicinity of the external aperture of the intervertebral foramen of DLSS patient instead of intradiscally. Our aim was to avoid the harsh microenvironment within the IVD, assuming that the proposed route of application would allow AT-MSCs to exhibit their most important characteristics—trophic and homing effects at their full potential.
A client-owned 12-year-old female blend dog was presented with a several-month history of walk with flexed knees and hips, reduced activity with pronounced abstaining from climbing and descending the stairs, and with occasional urine incontinence. The dog weighed 19 kg (4–5 kg more than average) and had not received any medication beforehand.
During general examination, the dog was found to be conscious, oriented in space, with a normal posture of the head. The dog repeatedly supported body with forelegs, while hind legs were kept down, on the side. The perineal region was wet, most likely from urine.
On orthopedic and neurological examinations (Table 1), hind limb paresis with a mild drift of lumbosacral part, which was in a slight kyphosis, was noted. When the animal was placed to stand up on the hind legs, disturbed proprioception was observed, and quickly the dog rested again. Deep and superficial sensibility, retrieval reflex, and patellar reflex were preserved, while the crossed extensor reflex was slightly reduced. The stiffness was detected during each knee flexion with audible crepitation, which indicated osteoarthritis (OA) of both knees. Regarding hip flexion and extension, nothing abnormal was detected. During palpation of the lumbosacral region, the dog expressed discomfort and pain. The lordosis test (performed in a lying position) was positive; the animal felt pain. The enlarged urinary bladder was detected by palpation, which was released by pressure. Perineal reflex was preserved. The tone of the tail was decreased. Since the dog had no pain except the one that was elicited during physical examination (PE), and since she had had several episodes of gastritis in the past, no analgesic therapy was prescribed. A short video from that period was provided by the owner (Supplementary Video S1).
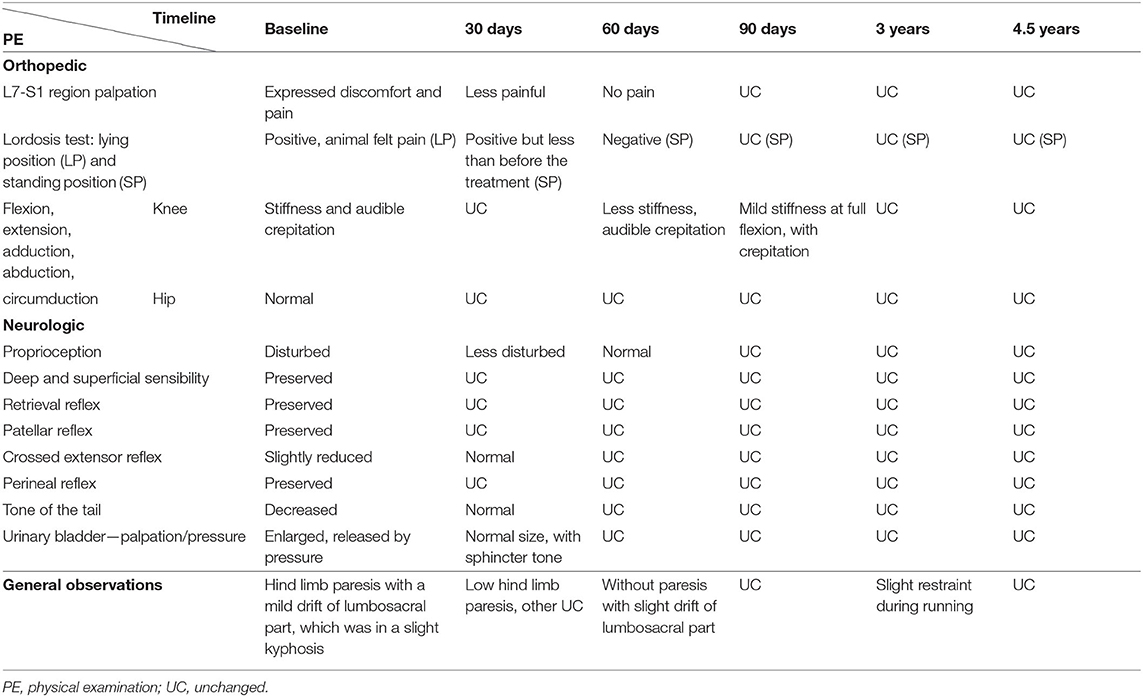
Table 1. Comprehensive information on the results of physical examination at each indicated patient's visit.
Following described assessments, an X-ray and magnetic resonance imaging (MRI) were performed. The animal was anesthetized only during MRI due to her age and our technical limitation to complete these examinations consecutively. That is why the animal was poorly positioned on the radiograph image (Figure 1), but nevertheless, an asymmetric lumbosacral transitional vertebra with ossification on the left side was clearly seen (indicated by an oblique arrow), as well as a reduced intervertebral space L7-S1 (indicated by a horizontal arrow). On the sagittal MRI of the lumbosacral region (Figure 2A), the IVD L7-S1 was seen as protruded and hypointense compared with the bright signal from normally hydrated discs. The disc protrusion was also seen on the transversal MRI section (Figure 2B). Based on these results, as well as on orthopedic and neurological findings, this case was diagnosed as DLSS, accompanied with OA of both knees.
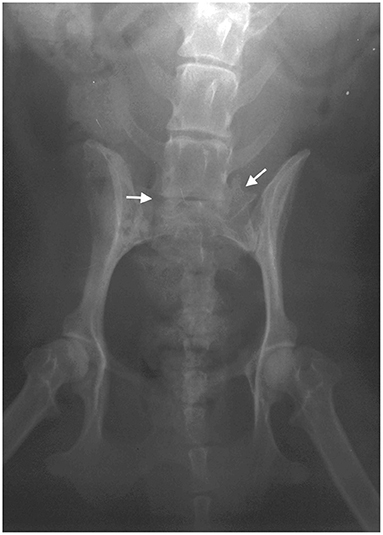
Figure 1. Radiograph image (X-ray) of the lumbosacral region. The image was taken in the ventrodorsal projection using the Atomscope radiograph machine (model 100pr type B, Auckland, New Zealand), with a collimator-to-film distance of 70 cm, exposure of 80 ms, and penetration power of 80 kV.
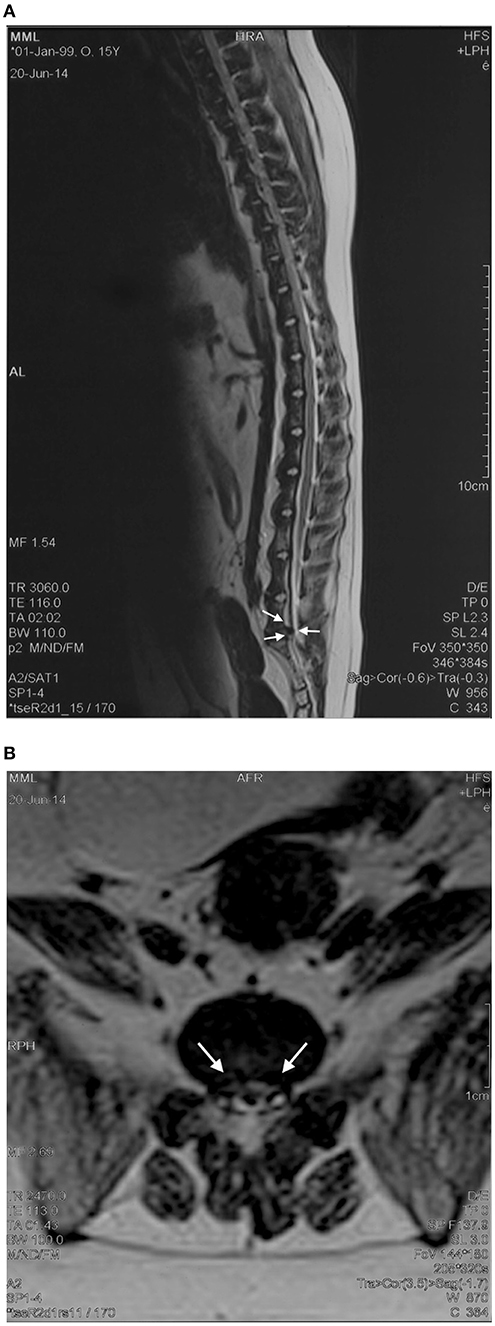
Figure 2. Representative magnetic resonance imaging (MRI) scans of the lumbosacral region. The T2-weighted sagittal (A) and transversal (B) images of the lumbosacral region are shown, and the intervertebral disc L7-S1 herniation is indicated by arrows.
There is currently no consensus on treatment selection for dogs with DLSS, and available options most often involve aggressive surgical techniques (3). We decided to try a new and least invasive procedure, using cultured autologous adipose tissue-derived mesenchymal stem cells (AT-MSCs). These cells hold enormous potential as therapeutic agents in vivo, especially for regenerating damaged tissues in diseases of the locomotor system (6, 7).
The adipose tissue collection and AT-MSC therapy were approved and certified by the dog owner with signed informed consent. The AT collection was performed using anesthetics, and AT-MSC therapy was performed using sedatives, which excluded the pain, suffering, fear, and stress of the animal, following the standards of good veterinary practice, the guidelines of good laboratory practice, the European Parliament Directive, the Council of 22 September 2009 (2010/63/EU), and the European Convention for the protection of vertebrates intended for experimental and other scientific purposes (ETS 170).
Around 10 g of subcutaneous adipose tissue from the paralumbar region (on the borderline of the middle and caudal lateral abdominal region) was collected through the 5-cm-long incision while patient was under general anesthesia using medetomidine hydrochloride (Domitor, Orion Pharma, Espoo, Finland; 10 μg/kg IM) and Propofol (Diprivan, Astra Zeneca, Macclesfield, UK; 1.5 mg/kg IV).
The isolation, culture of AT-MSCs for the treatment, and differentiation of cells for control of the stemness were performed as previously described (8). A total of 91.8 × 106 cells resuspended in 3 ml of PBS were transplanted as follows: paravertebrally at the level L7-S1, a 30.6 × 106 cells were injected into each, left and right side with a 0.8 × 40-mm needle; while intraarticularly into each knee, a 15.3 × 106 cells were injected with a 0.6 × 30-mm needle. During this procedure, the animal was sedated with medetomidine hydrochloride (Domitor, Orion Pharma, Espoo, Finland; 20 μg/kg IM). Following the application of AT-MSCs, the dog was not subjected to any physiotherapy treatment. Until the next PE, rest and restraint from physical activity under the owner's supervision were the only recommendations.
Clinical evaluation consisted of PE of the patient (Table 1). Also, the assessment for lameness at walk and trot, using a numeric rating scale, has been performed as previously described (8). Briefly, the clinical outcome measures were expressed by a numeric rating scale based on a veterinary assessment questionnaire. The scale ranged from 1 to 6, where 1 was marked as the best, normal condition (without the lameness) and 6 as the most severe (the animal cannot walk or trot). The evaluation was performed initially, upon admission of the patient (baseline) and at specified intervals after the treatment with AT-MSCs, supplemented with assessments of the owner (Figure 3). There were no detected adverse reactions to the described treatment.
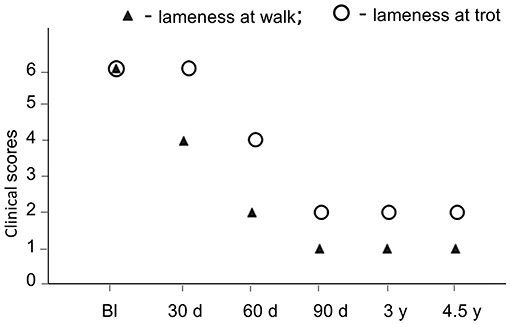
Figure 3. Timeline of the clinical course and effects of AT-MSC treatment on lameness of a dog at walk and trot during long-term follow-up. Bl, baseline; d, days; y, years. The numeric rating scale applied to evaluate clinical outcome in lameness at walk was as follows: 1, normal; 2, mild, sporadic; 3, persistent, weight bearing; 4, severe, occasionally weight bearing; 5, severe, non-weight bearing; 6, cannot walk without assistance; while for the lameness at trot was as follows: 1, normal; 2, mild, sporadic; 3, persistent, weight bearing; 4, severe, non-weight bearing; 5, cannot trot without stimulation; 6, cannot trot.
As it is presented in Table 1, at first check-up performed 30 days after the treatment, the dog walked with stiff hind legs, occasionally weight bearing. Palpation of the lumbosacral region was less painful. The lordosis test (performed in a standing position) was positive but less than before the treatment. Stiffness during the flexion of both knees still existed, with audible crackling. The urinary bladder was of normal size and did not leak under the pressure. The tail had a normal tone. According to the owner, the dog was walking but with difficulties, could not run, turning was performed with an effort to maintain the balance of the backside, had problems when trying to get up and lie down, and it was difficult for the animal to take a position to urinate.
After 60 days of AT-MSC injection, the animal moved normally without the stiffness of the hind limbs. The knee stiffness was lesser than during previous examination. According to the owner, getting up and lying down was easier for the dog, and the position to urinate was almost normal.
Ninety days post-AT-MSC treatment, the animal functioned normally, with a desire to run and play, albeit cautiously. The mild stiffness of both knees remained at full flexion, with crepitation.
Once a year, the owner informed the veterinarian about the condition of the dog, which was unchanged compared with the examination that was performed on the 90th day after the AT-MSC treatment.
After 3 years posttreatment, the animal was re-examined. It was found that the dog still felt well, without any problems during the movement or with the balance, and without pain throughout the lordosis test. Slight restraint was observed during running. At full flexion, the mild stiffness of both knees was still present but painless. Videos from that period were provided by the veterinarian (Supplementary Videos S2, S3).
The final follow-up was performed 4.5 years after the treatment. The dog was still feeling well, with signs of slightly slower walking and turning and a bit less willingness to climb the stairs. Video from that period was provided by the veterinarian (Supplementary Video S4). Eight days after this examination, the dog died of old age.
In animals diagnosed with DLSS, the basic treatment consists of abstinence from all physical activities, with the administration of SAID and nonsteroidal anti-inflammatory drugs (NSAID). The application of methylprednisolone epidurally gave good results; it was reported that 53% of animals was totally cured during the follow-up of 1 week to 46 months (9). Also, it was reported that NSAID application for 6 weeks lead to improvement in 50% of treated dogs, which lasted up to 14.5 weeks (10). For dogs that do not respond to this medical treatment, particularly for dogs which are required to work, surgical intervention may be indicated. The surgical management of DLSS includes strategies that are employed with the goal to decompress cauda equina and/or root nerves and/or to stabilize the lumbosacral junction (3).
The most commonly used surgical treatment of decompression is dorsal laminectomy L7 and S1, with dorsal annulectomy, in which the prolonged portion of annulus fibrosus is cut. In studies in which this approach has been applied, different success rate has been reported. In particular, it was shown that the pain relief was detected within 6 weeks in 81% of animals, while positive neurological outcomes were observed in 62.5% of treated dogs within the follow-up of 30 weeks (10); recovery has been reported for 33% of dogs after 2 months following the treatment, with follow-up period of up to 4 years (11); clinical improvement has been reported for 76.8% animals during the follow-up period of 9–41 months (12); and the 53% of dogs were totally cured during the mean follow-up of 30 months (13). This approach, however, often results in a limited decompression effect. Lateral foraminotomy and dorsal decompression technique is also available, although it may increase the instability of L7-S1, as it was shown in 45% of treated patients, during the mean follow-up of 15.2 months (14).
Approaches that aim to stabilize the lumbosacral junction include application of various implants, such as, bone grafting implants of the facets (with or without laminectomy), screw implants (instead of bone grafts), a combination of multiple screw and graft implants that are dorsally connected to each other with bone cement, pedicle screw rod fixation, and transilial bar, for which 53–79% of positive outcomes have been reported during the follow-up period of 6 months to 4 years (3). However, none of these treatments enables optimal stabilization, while, to a greater or lesser extent, all lead to certain complications.
The application of MSCs has emerged as a promising alternative approach to those invasive surgical strategies. Due to the unique properties of MSCs, their application for treating different diseases of the locomotor system, including disc degeneration, has been extensively examined in vitro and in vivo (6, 15). These cells could be isolated from various tissues, while bone marrow and adipose tissue are most commonly used. The advantage of the latter is easy accessibility of subcutaneous adipose tissue as well as relatively large number of MSCs that it contains (16). It is well known that MSCs can differentiate into various cell types, including chondrocyte lineages, and some studies have shown their capability to differentiate into nucleus pulposus-like cells (17). Other important properties of MSCs include trophic effects that lead to local reduction of inflammation and apoptosis, prevention of fibrosis, stimulation of endogenous regenerative programs, and neovascularization (18). Also, it is important to point out that MSCs can migrate to the point of damage via signals sent by tissues affected by ischemia, inflammation, or are otherwise damaged, which is referred to as MSC homing (18–20).
The successful use of AT-MSCs as a regenerative therapy in dogs has mainly been reported for bone and cartilage defects with inflammatory component, such as OA (8, 21–24). Namely, it has been shown that the treatment of canine OA with AT-MSCs leads to a reduction in local inflammation level, and it enables slowdown of degenerative processes and regeneration of damaged articular cartilage (25). Since the similarity between articular cartilage and IVD has been recognized at the morphological, functional, and physiological/pathophysiological levels (26–29), we hypothesized that the positive effects of AT-MSC application, observed in the treatment of canine OA, could also be expected in the treatment of the presented DLSS patient.
Furthermore, we have assumed that autologous AT-MSC transplantation in our DLSS patient near the foramen can lead to a reduction in soft tissue hypertrophy that compresses the root of the nerve. Although soft tissue hypertrophy has been regarded as secondary (30), it is responsible for the appearance of DLSS symptoms and represents a sign of chronic inflammation accompanied with pathological, degenerative processes. Therefore, our assumption was that AT-MSC treatment could facilitate a reduction in the level of local soft tissue chronic inflammation, which would then lead to a decompression of the intervertebral foramen L7-S1.
Positive effects of therapeutic applications of MSCs have been observed in the majority of experimentally induced intervertebral disc degeneration models in small (mouse, rat, rabbit) and large (sheep, dog, minipig) animals (7, 15, 17, 31). In most of these studies, bone marrow MSCs were used, as described for beagle dogs (32). Adipose-MSC transplantation into discs following their nucleotomy has been described for the rat (33) and the dog (34) models.
Even though described in vivo studies on induced intervertebral disc degeneration models showed positive effects of MSC application, this therapeutic approach did not lead to improvement when it was used to treat spontaneously occurring IVD degeneration in dogs (4, 5). In these studies, intradiscal injections of 3 × 106 bone marrow-derived MSCs, with or without microcarriers, were used. It was hypothesized that the harsh microenvironment within the IVD, which includes constant loading and low nutrient, oxygen and pH levels, is the reason why MSCs failed to divide and regenerate the damaged structure of IVD (35, 36).
In our case of spontaneous canine IVD degeneration, a different approach of MSC therapy was applied, which proved to be very successful. Namely, we used around 20 times higher number of AT-MSCs (61.2 × 106), which were injected bilaterally in the vicinity of the external aperture of the intervertebral foramen instead of intradiscally. We assumed that this route of application would allow AT-MSCs to exhibit their most important characteristics—trophic and homing effects on all inflamed/edematous/hypertrophied soft intervertebral foramen structures that exert pressure on the nerve root, which would then lead to a decompression of the intervertebral foramen L7-S1 along with the regeneration of the damaged tissues.
It is important to point out that after the application of AT-MSCs, the dog was not subjected to any physiotherapy treatment, as well as that a gradual improvement in clinical outcome measures related to the ability of the dog to walk and trot started to be detected relatively rapidly (30–60 days posttreatment), reaching a marked improvement that was maintained during long-term (4.5 years) follow-up.
To the best of our knowledge, this is the first case of successful therapy of spontaneously occurring canine DLSS using autologous AT-MSCs that were injected bilaterally in the vicinity of the external aperture of the intervertebral foramen. We believe that the described therapeutic approach represents a contribution to current studies in this field, in both veterinary and human regenerative medicine. Namely, since dogs have been recognized as a superior model compared with other commonly used species for studies of degenerative spinal diseases, DLSS in particular (37, 38), the presented data of safe, minimally invasive AT-MSC treatment with long-lasting positive effects, may shape not only animal but also human DLSS treatment options. The quality of regenerative effect, demonstrated for this DLSS case, should be confirmed in the future by larger, prospective studies that would involve selected canine subjects with spontaneously occurring DLSS.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
The adipose tissue collection and AT-MSC therapy were approved and certified by the dog owner with signed informed consent. The AT collection was performed using anesthetics, and AT-MSC therapy was performed using sedatives, which excluded the pain, suffering, fear, and stress of the animal, following the standards of good veterinary practice, the guidelines of good laboratory practice, the European Parliament Directive, the Council of 22 September 2009 (2010/63/EU), and the European Convention for the protection of vertebrates intended for experimental and other scientific purposes (ETS 170).
JM, AF, SP, and GN: conception of the case report. JM: clinical management of the case. VS: AT-MSC isolation and cultivation. JM, SSD, and GN: analysis and interpretation of results. JM, SSD, SP, and GN: writing and editing the manuscript. All authors contributed to the article and approved the submitted version.
This work was supported by the Ministry of Education, Science and Technological Development, Republic of Serbia (Grant No. III41004 and 451-03-68/2020-14/ 200042).
JM was employed by Stem Art Ltd., Belgrade, Serbia.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fvets.2021.732073/full#supplementary-material
Supplementary Video S1. A short video from the period just before the initial veterinary evaluation (baseline)—provided by the owner of the dog.
Supplementary Video S2. Video from the period 3 years post-AT-MSC treatment—provided by the veterinarian.
Supplementary Video S3. Video from the period 3 years post-AT-MSC treatmentprovided by the veterinarian.
Supplementary Video S4. Video from the period 4.5 years post-AT-MSC treatment—provided by the veterinarian.
AT, adipose tissue; DLSS, degenerative lumbosacral stenosis; IVD, intervertebral disc; MRI, magnetic resonance imaging; MSCs, mesenchymal stem cells; OA, osteoarthritis; PE, physical examination.
1. De Risio L, Thomas WB, Sharp NJ. Degenerative lumbosacral stenosis. Vet Clin North Am Small Anim Pract. (2000) 30:111–32. doi: 10.1016/s0195-5616(00)50005-9
2. Worth AJ, Thompson DJ, Hartman AC. Degenerative lumbosacral stenosis in working dogs: current concepts and review. N Z Vet J. (2009) 57:319–30. doi: 10.1080/00480169.2009.64719
3. Worth A, Meij B, Jeffery N. Canine degenerative lumbosacral stenosis: prevalence, impact and management strategies. Vet Med (Auckl). (2019) 10:169–83. doi: 10.2147/VMRR.S180448
4. Steffen F, Smolders LA, Roentgen AM, Bertolo A, Stoyanov J. Bone marrow-derived mesenchymal stem cells as autologous therapy in dogs with naturally occurring intervertebral disc disease: feasibility, safety, and preliminary results. Tissue Eng Part C Methods. (2017) 23:643–51. doi: 10.1089/ten.TEC.2017.0033
5. Steffen F, Bertolo A, Affentranger R, Ferguson SJ, Stoyanov J. Treatment of naturally degenerated canine lumbosacral intervertebral discs with autologous mesenchymal stromal cells and collagen microcarriers: a prospective clinical study. Cell Transplant. (2019) 28:201–11. doi: 10.1177/0963689718815459
6. Lavoie JR, Rosu-Myles M. Uncovering the secretes of mesenchymal stem cells. Biochimie. (2013) 95:2212–21. doi: 10.1016/j.biochi.2013.06.017
7. de Bakker E, Van Ryssen B, De Schauwer C, Meyer E. Canine mesenchymal stem cells: state of the art, perspectives as therapy for dogs and as a model for man. Vet Q. (2013) 33:225–33. doi: 10.1080/01652176.2013.873963
8. Srzentic Drazilov S, Mrkovacki J, Spasovski V, Fazlagic A, Pavlovic S, Nikcevic G. The use of canine mesenchymal stem cells for the autologous treatment of osteoarthritis. Acta Vet Hung. (2018) 66:376–89. doi: 10.1556/004.2018.034
9. Janssens L, Beosier Y, Daems R. Lumbosacral degenerative stenosis in the dog. The results of epidural infiltration with methylprednisolone acetate: a retrospective study. Vet Comp Orthop Traumatol. (2009) 22:486–91. doi: 10.3415/VCOT-08-07-0055
10. Ness MG. Degenerative lumbosacral stenosis in the dog: A review of 30 cases. J Small Anim Pract. (1994) 35:185–90. doi: 10.1111/j.1748-5827.1994.tb01683
11. Denny HR, Gibbs C, Holt PE. The diagnosis and treatment of cauda equina lesions in the dog. J Small Anim Pract. (1982) 23:425–43. doi: 10.1111/j.1748-5827.1982.tb03772
12. Danielsson F, Sjostrom L. Surgical treatment of degenerative lumbosacral stenosis in dogs. Vet Surg. (1999) 28:91–8. doi: 10.1053/jvet.1999.0091
13. Janssens LAA, Moens Y, Coppens P, Peremans K, Vinck H. Lumbosacral degenerative stenosis in the dog: the results of dorsal decompression with dorsal anulectomy and nuclectomy. Vet Comp Orthop Traumatol. (2000) 13:97–103. doi: 10.1055/s-0038-1632638
14. Godde T, Steffen F. Surgical treatment of lumbosacral foraminal stenosis using a lateral approach in twenty dogs with degenerative lumbosacral stenosis. Vet Surg. (2007) 36:705–13. doi: 10.1111/j.1532-950X.2007.00324.x
15. Zeckser J, Wolff M, Tucker J, Goodwin J. Multipotent mesenchymal stem cell treatment for discogenic low back pain and disc degeneration. Stem Cells Int. (2016) 2016:3908389. doi: 10.1155/2016/3908389
16. Arnhold S, Wenisch S. Adipose tissue derived mesenchymal stem cells for musculoskeletal repair in veterinary medicine. Am J Stem Cells. (2015) 4:1–12.
17. Wei A, Shen B, Williams L, Diwan A. Mesenchymal stem cells: potential application in intervertebral disc regeneration. Transl Pediatr. (2014) 3:71–90. doi: 10.3978/j.issn.2224-4336.2014.03.05
18. van Poll D, Parekkadan B, Borel Rinkes IHM, Tilles AW, Yarmush ML. Mesenchymal stem cell therapy for protection and repair of injured vital organs. Cel Mol Bioeng. (2008) 1:42–50. doi: 10.1007/s12195-008-0001-2
19. Lin W, Xu L, Zwingenberger S, Gibon E, Goodman SB, Li G. Mesenchymal stem cells homing to improve bone healing. J Orthop Translat. (2017) 9:19–27. doi: 10.1016/j.jot.2017.03.002
20. Wangler S, Peroglio M, Menzel U, Benneker LM, Haglund L, Sakai D, et al. Mesenchymal stem cell homing into intervertebral discs enhances the Tie2-positive progenitor cell population, prevents cell death, and induces a proliferative response. Spine (Phila Pa 1976). (2019) 44:1613–22. doi: 10.1097/BRS.0000000000003150
21. Black LL, Gaynor J, Gahring D, Adams C, Aron D, Harman S, et al. Effect of adipose-derived mesenchymal stem and regenerative cells on lameness in dogs with chronic osteoarthritis of the coxofemoral joints: a randomized, double-blinded, multicenter, controlled trial. Vet Ther. (2007) 8:272–84.
22. Black LL, Gaynor J, Adams C, Dhupa S, Sams AE, Taylor R, et al. Effect of intraarticular injection of autologous adipose-derived mesenchymal stem and regenerative cells on clinical signs of chronic osteoarthritis of the elbow joint in dogs. Vet Ther. (2008) 9:192–200.
23. Vilar JM, Morales M, Santana A, Spinella G, Rubio M, Cuervo B, et al. Controlled, blinded force platform analysis of the effect of intraarticular injection of autologous adipose-derived mesenchymal stem cells associated to PRGF-Endoret in osteoarthritic dogs. BMC Vet Res. (2013) 9:131. doi: 10.1186/1746-6148-9-131
24. Cuervo B, Rubio M, Sopena J, Dominguez JM, Vilar J, Morales M, et al. Hip osteoarthritis in dogs: a randomized study using mesenchymal stem cells from adipose tissue and plasma rich in growth factors. Int J Mol Sci. (2014) 15:13437–60. doi: 10.3390/ijms150813437
25. Sasaki A, Mizuno M, Mochizuki M, Sekiya I. Mesenchymal stem cells for cartilage regeneration in dogs. World J Stem Cells. (2019) 11:254–69. doi: 10.4252/wjsc.v11.i5.254
26. Willems N, Kersten R, van Gaalen SM, Oner FC, Strijkers GJ, Veraa S, et al. Temporary segmental distraction in a dog with degenerative lumbosacral stenosis. Vet Comp Orthop Traumatol. (2018) 31:298–303. doi: 10.1055/s-0038-1639599
27. Sharifi S, Bulstra SK, Grijpma DW, Kuijer R. Treatment of the degenerated intervertebral disc; closure, repair and regeneration of the annulus fibrosus. J Tissue Eng Regen Med. (2015) 9:1120–32. doi: 10.1002/term.1866
28. Longo UG, Papapietro N, Petrillo S, Franceschetti E, Maffulli N, Denaro V. Mesenchymal stem cell for prevention and management of intervertebral disc degeneration. Stem Cells Int. (2012) 2012:921053. doi: 10.1155/2012/921053
29. Bach FC, Willems N, Penning LC, Ito K, Meij BP, Tryfonidou MA. Potential regenerative treatment strategies for intervertebral disc degeneration in dogs. BMC Vet Res. (2014) 10:3. doi: 10.1186/1746-6148-10-3
30. Slocum B, Devine T. L7-S1 fixation-fusion for treatment of cauda equina compression in the dog. J Am Vet Med Assoc. (1986) 188:31–5.
31. Yim RL, Lee JT, Bow CH, Meij B, Leung V, Cheung KM, et al. A systematic review of the safety and efficacy of mesenchymal stem cells for disc degeneration: insights and future directions for regenerative therapeutics. Stem Cells Dev. (2014) 23:2553–67. doi: 10.1089/scd.2014.0203
32. Hiyama A, Mochida J, Iwashina T, Omi H, Watanabe T, Serigano K, et al. Transplantation of mesenchymal stem cells in a canine disc degeneration model. J Orthop Res. (2008) 26:589–600. doi: 10.1002/jor.20584
33. Jeong JH, Lee JH, Jin ES, Min JK, Jeon SR, Choi KH. Regeneration of intervertebral discs in a rat disc degeneration model by implanted adipose-tissue-derived stromal cells. Acta Neurochir (Wien). (2010) 152:1771–7. doi: 10.1007/s00701-010-0698-2
34. Ganey T, Hutton WC, Moseley T, Hedrick M, Meisel HJ. Intervertebral disc repair using adipose tissue-derived stem and regenerative cells: experiments in a canine model. Spine (Phila Pa 1976). (2009) 34:2297–304. doi: 10.1097/BRS.0b013e3181a54157
35. Adams MA, Roughley PJ. What is intervertebral disc degeneration, and what causes it? Spine (Phila Pa 1976). (2006) 31:2151–61. doi: 10.1097/01.brs.0000231761.73859.2c
36. Krock E, Rosenzweig DH, Haglund L. The inflammatory milieu of the degenerate disc: is mesenchymal stem cell-based therapy for intervertebral disc repair a feasible approach? Curr Stem Cell Res Ther. (2015) 10:317–28. doi: 10.2174/1574888x10666150211161956
37. Bergknut N, Rutges JP, Kranenburg HJ, Smolders LA, Hagman R, Smidt HJ, et al. The dog as an animal model for intervertebral disc degeneration? Spine (Phila Pa 1976). (2012) 37:351–8. doi: 10.1097/BRS.0b013e31821e5665
Keywords: canine (dog), degenerative lumbosacral stenosis, autologous AT-MSCs, minimally invasive treatment, regenerative medicine, case report
Citation: Mrkovački J, Srzentić Dražilov S, Spasovski V, Fazlagić A, Pavlović S and Nikčević G (2021) Case Report: Successful Therapy of Spontaneously Occurring Canine Degenerative Lumbosacral Stenosis Using Autologous Adipose Tissue-Derived Mesenchymal Stem Cells. Front. Vet. Sci. 8:732073. doi: 10.3389/fvets.2021.732073
Received: 28 June 2021; Accepted: 20 August 2021;
Published: 23 September 2021.
Edited by:
Anna Lange-Consiglio, University of Milan, ItalyReviewed by:
Takashi Taguchi, Western University of Health Sciences, United StatesCopyright © 2021 Mrkovački, Srzentić Dražilov, Spasovski, Fazlagić, Pavlović and Nikčević. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gordana Nikčević, Z29yZG5pa0BpbWdnZS5iZy5hYy5ycw==; Z29yZG5pazdAZ21haWwuY29t
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.