 Giuseppe Morgia1,2
Giuseppe Morgia1,2 Arturo Lo Giudice2
Arturo Lo Giudice2 Maria Giovanna Asmundo2Ilenia Rapallo2Maurizio Carrino3Francesco Persico3
Maria Giovanna Asmundo2Ilenia Rapallo2Maurizio Carrino3Francesco Persico3 Carlo Terrone4
Carlo Terrone4 Rafaela Malinaric4Alessandro Tedde5Massimo Madonia5Salvatore Voce6Giulio Reale6
Rafaela Malinaric4Alessandro Tedde5Massimo Madonia5Salvatore Voce6Giulio Reale6 Gaetano Larganà6
Gaetano Larganà6 Andrea Cocci7
Andrea Cocci7 Lorenzo Masieri7Francesca Zingone1Daniela Carcò8
Lorenzo Masieri7Francesca Zingone1Daniela Carcò8 Giorgio Ivan Russo2*
Giorgio Ivan Russo2*- 1Department of Urology, Mediterranean Institute of Oncology (IOM), Catania, Italy
- 2Urology Section, Department of Surgery, University of Catania, Catania, Italy
- 3Department of Urology, AORN Cardarelli, Naples, Italy
- 4Department of Urology, University of Genoa, Genova, Italy
- 5Department of Urology, University of Sassari, Sassari, Italy
- 6Department of Urology, S. M. Delle Croci, Ravenna, Italy
- 7Department of Urology, University of Florence, Florence, Italy
- 8Laboratory of Clinical Pathology, Mediterranean Institute of Oncology (IOM), Catania, Italy
Background: Due to the pandemic emergency caused by COVID-19, many countries were forced to apply a variety of measures such as quarantine and full national lockdown in order to contain the contagion. Medication adherence to chronic diseases may have been negatively influenced by restrictions due to the COVID-19 pandemic. The purpose of this study is to investigate adherence to urological therapies of patients with lower urinary tract symptoms (LUTSs) secondary to benign prostatic hyperplasia (BPH) during the COVID-19 lockdown period.
Methods: In this cohort study, we included a total of 151 male patients who were prescribed medications for LUTSs/benign prostatic enlargement (BPE) between January 2019 and December 2020. The prescriptive data of the following medications were collected: alpha-blockers (AB), 5-alpha reductase inhibitors (5-ARIs), 5-phosphodiesterase inhibitors (PDE5-i), antimuscarinics, and phytotherapy (i.e., Serenoa repens). According to adherence or discontinuation of therapy, patients were divided into two groups: those who took their medications for a minimum of 6 months during the index period were considered in the “Medication adherence group” and those whose treatment was considered “discontinued” if it was interrupted for a 1-month period.
Results: Overall, the median age was 69.0 (interquartile range [IQR]: 63.0–74.0), the median International Prostate Symptom Score (IPSS) before the lockdown was 15.0 (IQR: 11.0–18.0), and the median IPSS–quality of life (IPSS-QoL) before the lockdown was 2.0 (IQR: 2.0–3.0). During the lockdown, 19 patients (12.58%) stopped taking their medications due to the pandemic situation: six (31.58%) stopped phytotherapy, two stopped AB+phytotherapy (10.53%), five stopped AB (26.32%), three stopped 5-ARIs (15.79%), one stopped antimuscarinics (5.26%), and two stopped other combination therapies (p < 0.01). Among the patients who stopped therapy, five (26.31%) reported the presence of worsening symptoms (score ≥ 3), while 14 (73.69%) reported the absence of worsening symptoms (score < 3). During the lockdown, five (3.31%) patients required hospitalization: three (1.99%) for acute urinary retention and two (1.32%) for urinary tract infection.
Conclusions: The rate of medication adherence for LUTSs/BPE during COVID-19 was 86.75%, but 13.25% of the patients had their treatments interrupted due to the pandemic situation. This rate determined a slight increase in symptoms with a potential impact on hospitalization. These results should be taken into account in order to develop adequate strategies in telehealth to maintain medication adherence for chronic diseases.
Introduction
The novel severe acute respiratory syndrome caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) quickly spread throughout the whole world since its very first detection in Wuhan, China, on December 1, 2019 (1). COVID-19 was soon declared a pandemic, and on April 2, one million cases were confirmed (2).
Due to the pandemic emergency, many countries were forced to apply a variety of measures such as quarantine and full national lockdown in order to contain the contagion. In fact, on March 9, the Italian government imposed a stay-at-home order that moved toward a full lockdown, with workplaces, schools, shops, and bars closed and the application of smart-working systems. The interruption of the lockdown statement on May 1, 2020, determined the start of “phase 2” of the pandemic (3).
Hospitals and health authorities took unprecedented stringent measures to curb the wave of COVID-19 patients; in fact, many hospitals were converted into dedicated facilities that had the specific task to manage these patients. However, despite that preventive measures were applied, it was unavoidable that doctors and nurses who assisted patients affected by COVID-19 were infected by the virus too. This moment became critical, as it imposed enormous difficulties and challenges on urology health professionals globally.
The global pandemic led many urologists to make unprecedented decisions to strike a balance between providing optimal and high-quality urological care to their patients and mitigating the risk of infection.
The European Association of Urology (EAU) provided an update of its guidelines with the aim to reduce the risk of contagion and optimize the resources during pandemic emergencies (4).
In this context, medication adherence to chronic diseases may have been negatively influenced by restrictions due to the COVID-19 pandemic. In particular, it was reported that approximately 51% of the patients reported a medication-related problem, with 19.6% reporting problems in obtaining medications and 31.7% reporting forgetting or not taking their medications (5).
Among chronic urological diseases, lower urinary tract symptoms (LUTSs) secondary to benign prostatic enlargement (BPE) are very common in adult men, and they are related to age as well as genetic factors and family history (6). LUTSs/BPE is defined as a variety of storage, voiding, and post-voiding urination symptoms (7).
A study conducted by McNicholas et al. reported that α1-blockers are the most frequently prescribed medications in men who suffer from LUTSs/BPE (8); however, phytotherapy surprisingly accounted for 27% of all monotherapies and 54% of all combination therapies. A similar prescription profile was reported between general practitioners and urologists who represent 92% and 3.7% of total prescribers, respectively. In 95.4% of cases, the first approach is a medical treatment consisting mainly of α1-blockers (AB) (60.3%), phytotherapy (31.8%), or 5 alpha-reductase inhibitors (5-ARIs) (7.9%), although modification of treatments within 12 months from the beginning may occur at an extremely high rate (8.7%, 14.6%, and 12.9%, respectively) (9).
The purpose of this study is to investigate LUTS/BPE patients’ adherence to urological therapies during the COVID-19 lockdown period.
Materials and Methods
In this cohort study, we included a total of 151 male patients who were prescribed medications for LUTSs/BPE between January 2019 and December 2020. Data were collected through Google form sent by email using hospital records.
The prescriptive data of the following medications were collected: AB, 5-ARIs, 5-phosphodiesterase inhibitors (PDE5-i), antimuscarinics, and phytotherapy (i.e., Serenoa repens).
According to adherence or discontinuation of therapy, patients were divided into two groups: those who took their medications for a minimum of 6 months during the index period were considered in the “Medication adherence group” and those whose treatment was considered “discontinued” if it was interrupted for a 1-month period. The presence or absence of worsening symptoms was considered only in patients who discontinued their therapy.
Data collection forms included baseline data, consisting of the International Prostate Symptom Score (IPSS) questionnaire, which referred to the period before and after lockdown.
The second part of the form included questions regarding the interruption of LUTS/BPE therapy: which main or association medications were discontinued, the reason the therapy was abandoned, if after discontinued therapy any worsening of urinary symptoms occurred, and a potential hospitalization for urological LUTS/BPE-related condition. Finally, the reasons for medical therapy discontinuation were categorized into “reasons related to pandemic and lockdown” and “other reasons”. Moreover, any self-reported worsening of urological symptoms was objectified by a numerical scale graduated from 0 to 5, where “0” means “absence of worsening” and “5” means “very high worsening”. Patients were divided into two groups according to continuation or interruption of LUTS/BPE treatment.
Statistical Analysis
Continuous variables are presented as the median and interquartile range (IQR) and were compared by Student’s independent t-test or the Mann–Whitney U test based on their normal or non‐normal distribution, respectively (normality of variables’ distribution was tested by the Kolmogorov–Smirnov test). Categorical variables were tested with the χ2 test. Data analysis was performed under the guidance of our statistics expert, using SPSS version 17 (Statistical Package for the Social Sciences, SPSS Inc., released 2008; SPSS Statistics for Windows, Version 17.0) (SPSS Inc.).
Results
Overall, the median age was 69.0 (IQR: 63.0–74.0), median IPSS before the lockdown was 15.0 (IQR: 11.0–18.0), and median IPSS–quality of life (IPSS-QoL) before the lockdown was 2.0 (IQR: 2.0–3.0). Figure 1 shows the type of medications taken by our cohort before the pandemic. During the lockdown, 19 patients (12.58%) stopped taking their medications due to the pandemic situation: six (31.58%) stopped phytotherapy, two stopped AB+phytotherapy (10.53%), five stopped AB (26.32%), three stopped 5-ARIs (15.79%), one stopped antimuscarinics (5.26%), and two stopped other combination therapies (p < 0.01) (Figure 1). Among the patients who stopped therapy, five (26.31%) reported the presence of worsening symptoms (score ≥ 3), while 14 (73.69%) reported the absence of worsening symptoms (score < 3).
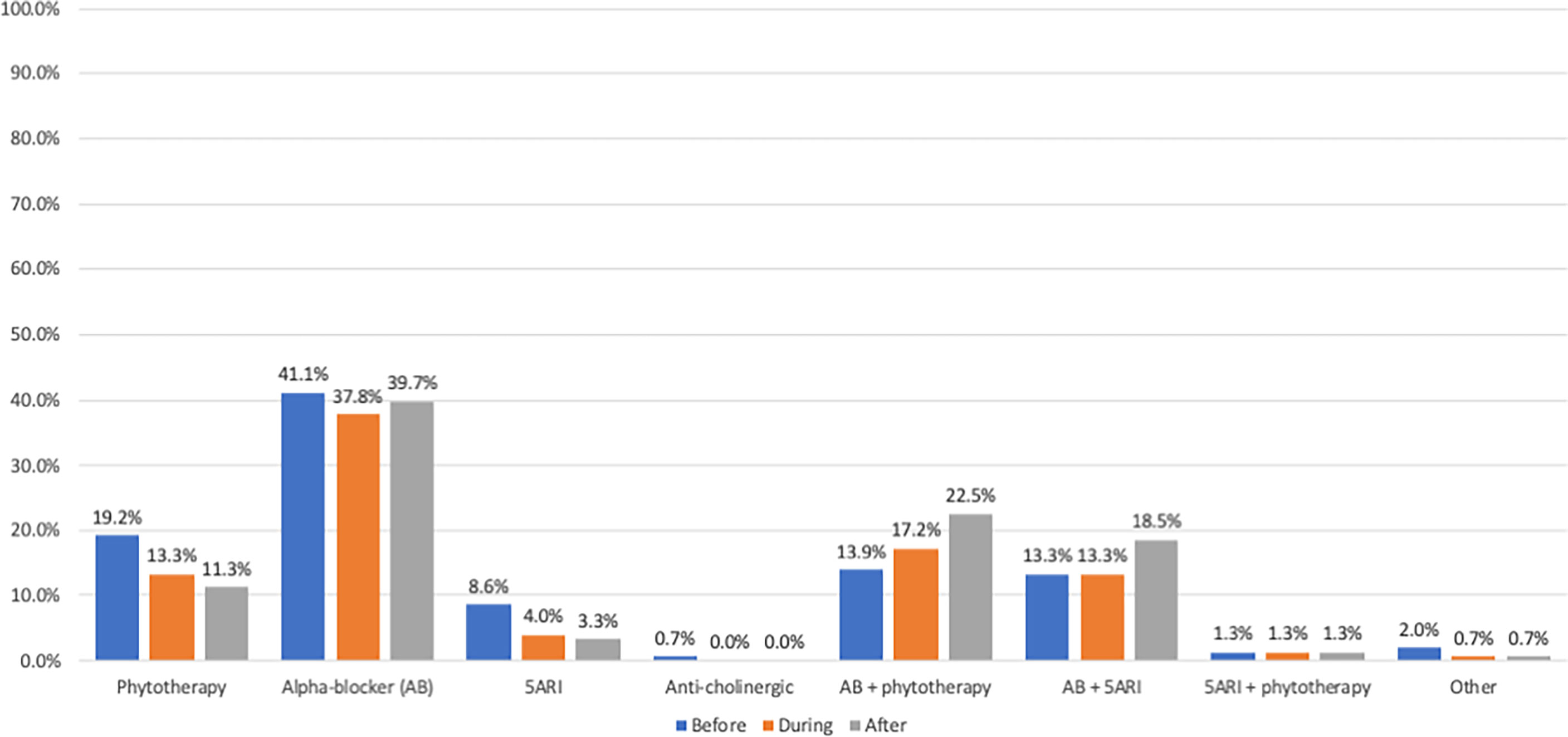
Figure 1 Distribution of taken medications before, during, and after COVID-19 pandemic. AB, alpha-blockers; 5-ARIs, 5-alpha reductase inhibitors.
Table 1 shows the characteristics of patients according to discontinuation of therapy.
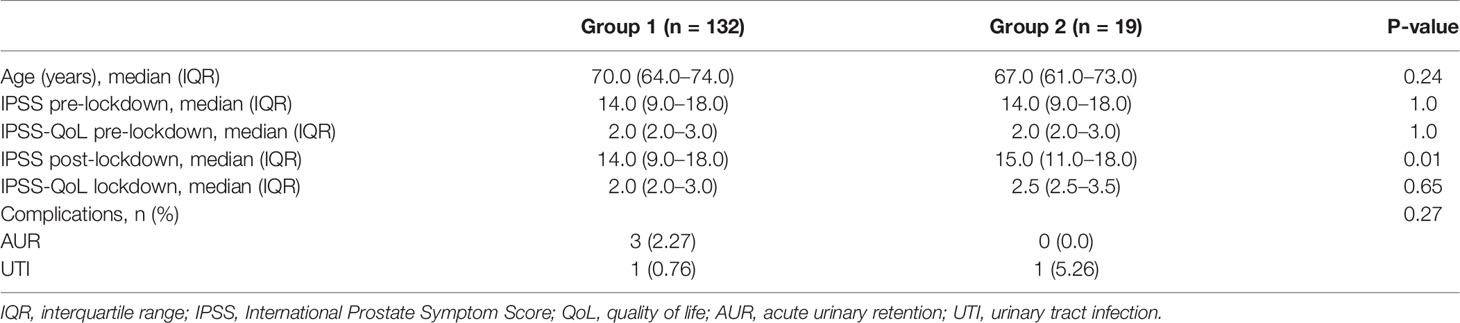
Table 1 Characteristics of patients according to the discontinuation of therapy.
During the lockdown, five (3.31%) patients required hospitalization: three (1.99%) for acute urinary retention (AUR) and two (1.32%) for urinary tract infection (UTI). Among these patients, two (40.0%) were under AB+phytotherapy, two (40.0%) were under AB+5-ARIs, and one (20.0%) stopped therapy (p = 0.38).
After lockdown, 147 patients (97.35%) continued to take their medication for LUTSs/BPE, while only four (2.65%) stopped taking their medication. Figure 1 shows the type of medications taken by our cohort after the pandemic.
The median IPSS after lockdown was 14.0 (IQR: 9.0–18.0) (p < 0.01), while the median IPSS-QoL was 2.0 (IQR: 2.0–3.0) (p = 0.12). Only one patient (0.66%) was hospitalized for AUR after the lockdown.
Discussion
Herein we demonstrated that the medication adherence for LUTSs/BPE during the COVID-19 pandemic was 86.75%, but 13.25% interrupted their medications due to lockdown. Although the rate of hospitalization was low due to the short period of observation, we observed a statistically significant reduction of IPSS after lockdown.
A study by Assenza et al. about the impact of COVID-19 lockdown on the treatment of patients with epilepsy demonstrated that during the COVID-19 pandemic, 32 (7%) people who reported inadequate adherence to therapy attributed it primarily to forgetfulness (70%), demotivation (15%), and adverse events (10%) (10). Further, Midao et al. reported that during the pandemic, 8.2% of participants reported that their adherence improved, 5.9% had worsened adherence results, widowers were 3 times more prone to be less adherent, and comorbid patients were 1.8 times more prone to be less adherent (11).
Literature data demonstrated that more prescriptions were filled in March 2020 than in any prior month, followed by a significant drop in monthly dispensing (12). A patient’s likelihood of discontinuing some medications increased after the spread of COVID compared to the pre-COVID era (12).
A study by Cindolo et al. was conducted in 2015 on 1.5 million men aged ≥40 years treated with alpha-blockers (ABs) and 5-alpha reductase inhibitors (5-ARIs) alone or in combination (CT) for their LUTSs/BPE. The authors reported that the 1-year adherence was 29% in patients exposed to at least 6-month therapy and that patients on CT had a higher discontinuation rate in the first 2 years as compared to those on monotherapy (p < 0.0001). Interestingly, the overall hospitalization rates for BPE and BPE surgery were 9.04 and 12.6 per 1,000 patient-years, respectively. Finally, discontinuation of medication treatment was an independent risk factor for hospitalization for benign prostatic hyperplasia (BPH) and BPH surgery (HR 1.65 and 2.80; p < 0.0001) regardless of the therapeutic group (13).
These findings highlight the importance of medication adherence for LUTSs/BPE in order to reduce the rate of hospitalization and disease progression in these patients.
Based on these premises, telehealth could be an important tool in caring services while keeping patients and health providers safe during the COVID-19 outbreak (14). In particular, phone calls and electronic health records can be used for screening or treating patients without the need for in-person visits and can be helpful in case of urgent care (15). Furthermore, elderly people can access health services using electronic devices (16).
Before concluding, we would like to underline some limitations. Firstly, we did not include a great number of patients. Secondly, the short follow-up of the lockdown could have limited the rate of complications and hospitalization in patients with a lack of adherence to medical therapy. Finally, we did not consider the potential influence of COVID-19 infection in our cohort.
Conclusions
The rate of medication adherence for LUTSs/BPE during COVID-19 was 86.75%, but 13.25% of the patients interrupted medications due to the pandemic situation. This rate determined a slight increase in symptoms with a potential impact on hospitalization.
These results should be taken into account in order to develop adequate strategies in telehealth to maintain medication adherence for chronic diseases.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved in October 2021 by the Polyclinic Hospital of Catania. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
GM and GIR designed the study. ALG, MC, FP, CT, RM, AT, MM, SV, GR, GL, AC, LM, FZ, and DC collected the data. AL, MA, and GIR drafted the manuscript. All authors approved the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical Features of Patients Infected With 2019 Novel Coronavirus in Wuhan, China. Lancet (London England) (2020) 395:497–506. doi: 10.1016/S0140-6736(20)30183-5
2. Sharma A, Ahmad Farouk I, Lal SK. COVID-19: A Review on the Novel Coronavirus Disease Evolution, Transmission, Detection, Control and Prevention. Viruses (2021) 13:202. doi: 10.3390/v13020202
3. Signorelli C, Scognamiglio T, Odone A. COVID-19 in Italy: Impact of Containment Measures and Prevalence Estimates of Infection in the General Population. Acta BioMed (2020) 91:175–9. doi: 10.23750/abm.v91i3-S.9511
4. Ribal MJ, Cornford P, Briganti A, Knoll T, Gravas S, Babjuk M, et al. An Organisation-Wide Collaborative Effort to Adapt the European Association of Urology Guidelines Recommendations to the Coronavirus Disease 2019 Era. Eur Urol (2020) 78:21–8. doi: 10.1016/j.eururo.2020.04.056
5. Ismail H, Marshall VD, Patel M, Tariq M, Mohammad RA. The Impact of the COVID-19 Pandemic on Medical Conditions and Medication Adherence in People With Chronic Diseases. J Am Pharm Assoc (2003) 62(3):834-9. doi: 10.1016/j.japh.2021.11.013
6. Langan RC. Benign Prostatic Hyperplasia. Prim Care Clin Off Pract (2019) 46:223–32. doi: 10.1016/j.pop.2019.02.003
7. Abrams P, Cardozo L, Fall M, Griffiths D, Rosier P, Ulmsten U, et al. The Standardisation of Terminology in Lower Urinary Tract Function: Report From the Standardisation Sub-Committee of the International Continence Society. Urology (2003) 61(1):37–49. doi: 10.1016/S0090-4295(02)02243-4
8. McNicholas T, Kirby R. Benign Prostatic Hyperplasia and Male Lower Urinary Tract Symptoms (LUTS). BMJ Clin Evid (2011) 86(4):359-60.
9. Lukacs B, Cornu J-N, Aout M, Tessier N, Hodée C, Haab F, et al. Management of Lower Urinary Tract Symptoms Related to Benign Prostatic Hyperplasia in Real-Life Practice in France: A Comprehensive Population Study. Eur Urol (2013) 64:493–501. doi: 10.1016/j.eururo.2013.02.026
10. Assenza G, Lanzone J, Brigo F, Coppola A, Di Gennaro G, Di Lazzaro V, et al. Epilepsy Care in the Time of COVID-19 Pandemic in Italy: Risk Factors for Seizure Worsening. Front Neurol (2020) 11:737. doi: 10.3389/fneur.2020.00737
11. Midão L, Almada M, Carrilho J, Sampaio R, Costa E. Pharmacological Adherence Behavior Changes During COVID-19 Outbreak in a Portugal Patient Cohort. Int J Environ Res Public Health (2022) 19:1135. doi: 10.3390/ijerph19031135
12. Clement J, Jacobi M, Greenwood BN. Patient Access to Chronic Medications During the Covid-19 Pandemic: Evidence From a Comprehensive Dataset of US Insurance Claims. PloS One (2021) 16:e0249453. doi: 10.1371/journal.pone.0249453
13. Cindolo L, Pirozzi L, Fanizza C, Romero M, Tubaro A, Autorino R, et al. Drug Adherence and Clinical Outcomes for Patients Under Pharmacological Therapy for Lower Urinary Tract Symptoms Related to Benign Prostatic Hyperplasia: Population-Based Cohort Study. Eur Urol (2015) 68:418–25. doi: 10.1016/j.eururo.2014.11.006
14. Portnoy J, Waller M, Elliott T. Telemedicine in the Era of COVID-19. J Allergy Clin Immunol Pract (2020) 8:1489–91. doi: 10.1016/j.jaip.2020.03.008
15. Reeves JJ, Hollandsworth HM, Torriani FJ, Taplitz R, Abeles S, Tai-Seale M, et al. Rapid Response to COVID-19: Health Informatics Support for Outbreak Management in an Academic Health System. J Am Med Inf Assoc (2020) 27:853–9. doi: 10.1093/jamia/ocaa037
Keywords: COVID-19, BPH (benign prostatic hyperplasia), drug, therapy, adherence, compliance, persistence
Citation: Morgia G, Lo Giudice A, Asmundo MG, Rapallo I, Carrino M, Persico F, Terrone C, Malinaric R, Tedde A, Madonia M, Voce S, Reale G, Larganà G, Cocci A, Masieri L, Zingone F, Carcò D and Russo GI (2022) Adherence to Urological Therapies for Lower Urinary Tract Symptoms Due to Benign Prostatic Enlargement During COVID-19 Lockdown. Front. Urol. 2:925575. doi: 10.3389/fruro.2022.925575
Received: 21 April 2022; Accepted: 10 May 2022;
Published: 06 June 2022.
Edited by:
Afonso Morgado, Centro Hospitalar Universitário de São João (CHUSJ), PortugalReviewed by:
Pedro Abreu-Mendes, Centro Hospitalar Universitário de São João, PortugalMurat Gul, University of Copenhagen, Denmark
Luca Boeri, University of Milan, Italy
Copyright © 2022 Morgia, Lo Giudice, Asmundo, Rapallo, Carrino, Persico, Terrone, Malinaric, Tedde, Madonia, Voce, Reale, Larganà, Cocci, Masieri, Zingone, Carcò and Russo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Giorgio Ivan Russo, Z2lvcmdpb2l2YW4ucnVzc29AdW5pY3QuaXQ=