 Safiya-Hana Belbina
Safiya-Hana Belbina Mia Rose Schmolze
Mia Rose Schmolze Sofia Gereta
Sofia Gereta Aaron A. Laviana1,3*
Aaron A. Laviana1,3*- 1Dell Medical School at the University of Texas, Austin, TX, United States
- 2The University of Texas Rio Grande Valley School of Medicine, Edinburg, TX, United States
- 3Department of Surgery and Perioperative Care, University of Texas At Austin Dell Seton Medical Center, Austin, TX, United States
Objective: Prostate-specific membrane antigen (PSMA) is a cell-surface protein widely expressed on most prostate cancer cells that has rapidly emerging clinical utility in the realm of prostate cancer. This systematic review aims to evaluate the efficacy as well as cost-effectiveness of PSMA in the roles of diagnosis and treatment in prostate cancer management.
Background: The use of PSMA in the initial staging of patients, early detection of recurrence, and response monitoring are critical to improving prostate cancer treatment. We performed a systematic review of the role of Gallium-68 (68Ga)-PSMA in the initial detection of prostate cancer and detection of biochemical recurrence (BCR) as well as the role of Lutium-177 (177Lu)-PSMA in theranostics. We also investigated the cost-effectiveness of both ligands in comparison to the current standard of care.
Methods: In February 2022 we performed a systematic and comprehensive review of the existing literature. We identified and screened articles published from 1983 up to January 2022 through PubMed. Only 1 study was included prior to 2011. We included articles that investigated the efficacy or cost-effectiveness of PSMA in prostate cancer detection and therapy. Using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRSIMA) guidelines eligible articles were selected, and relevant information was extracted from the original articles.
Results: A total of 26 articles were included in the analysis of this systematic review. These studies were heterogeneous and were comprised of five prospective studies including 336 patients, three retrospective analyses including 540 patients, one phase III trial, one survival analysis, one randomized control trial, three systematic reviews, three meta-analyses, two in-vivo studies, three reviews, and four cost analyses.
Conclusion: The diagnostic and therapeutic role of PSMA appears more efficacious and potentially less expensive than the standard treatment for patients with BCR of prostate cancer. Current evidence suggests PSMA will also fill an unmet need in initial diagnostics of prostate cancer and ligand therapy. However, a consensus has not yet been reached on cost-effectiveness of PSMA and further prospective studies are needed.
Introduction
Prostate cancer is the second most common cause of cancer-related deaths in men in the United States. In 2021, prostate cancer accounted for 13.1% of all new cancer cases and 5.6% of all cancer-related deaths. Current treatments have proven to be highly effective resulting in a five-year relative survival rate of nearly 100% in localized disease. However, the five-year survival rate significantly decreases to 30.6% in those with metastatic disease (1). As such, accurate initial staging of patients, early detection of recurrence, and response monitoring are critical to improving prostate cancer treatment.
Current guidelines for assessing metastasis recommend a) skeletal scintigraphy (bone scan) and b) abdominal and pelvic computed tomography (CT), both of which have their limitations. Bone scintigraphy has a sensitivity of 79% and a specificity of 82% for metastatic lesions (2). Although CT has a high sensitivity for metastases to cortical bone, it is limited in its sensitivity to tumors restricted to the marrow space. CT also has a low sensitivity when screening for lymphatic disease (42%) and is fairly poor in detecting smaller volume and size metastases (3). As such, there is a substantial need to improve detection of metastatic prostate cancer with prostate-specific membrane antigen (PSMA) and its concomitant ligands, becoming a noteworthy research focus of late.
Prostate specific membrane antigen (PSMA) is a type II transmembrane antigen expressed in all forms of prostate tissue as well as other benign tissues such as salivary glands, duodenal mucosa, and neuroendocrine cells (4, 5). PSMA expression in these benign tissues is significantly lower than in prostate cancer lesions where PSMA expression is notably increased. In healthy prostate cells, PSMA is localized to the cytoplasm and apical side of the epithelium. During malignant transformation, PSMA is transferred to the luminal surface of the prostate ducts and presents a large extracellular domain to ligands.
It is important to note that PSMA differs from prostate-specific antigen (PSA) both biologically and in its clinical role. Unlike PSA, a glycoprotein enzyme detected in serum, PSMA is a transmembrane protein that is often used in conjunction with positron emission tomography (PET) to aid in its detection. Increased PSMA expression correlates with cancer aggressiveness and is an independent indicator of a poor prognosis (6). These properties of PSMA have made the protein a promising candidate for prostate cancer therapy research.
From a research perspective, PSMA studies have focused on three main avenues a) initial prostate cancer detection and staging, b) radioligand therapy, and c) prostate cancer recurrence monitoring. The potential role of PSMA in the detection and treatment of prostate cancer as well as its economic value are discussed below.
Methods
This systematic review aims to investigate the following question: In men initially diagnosed with prostate cancer and in men with recurrent disease (P), is the use of PSMA (I) in comparison with the current standard of care (C) potentially more precise and accurate in detecting diseases, more beneficial in reducing morbidity and mortality outcomes, and more cost-effective (O). We chose to follow the PRISMA guidelines. Bias in the literature selected was assessed using predefined criteria outlined below and the Cochrane Tool. Ethical approval and patient consent were not required because all analyses were based on previously published studies.
Literature Search And Eligibility Criteria
We systematically searched PubMed using relevant keywords in February 2022 for papers and reviews published from January 1983 to January of 2022. Retrieved studies and reviews were hand-searched and hand-selected. Inclusion criteria included (1) in-vitro studies published after 1982, (2) all other studies published after 2010, (3) full text only, (4) relevant data for extraction, (5) sufficient data for extraction.
Of 521 articles identified in the literature search, 419 were excluded due to ineligible year of publication, irrelevant title or abstract, or not a full paper. 102 reports were then assessed for eligibility, 74 of these were excluded due to duplicate results, irrelevant outcomes, or irrelevant interventions. 26 studied were then included in the review. This process is demonstrated in Figure 1.
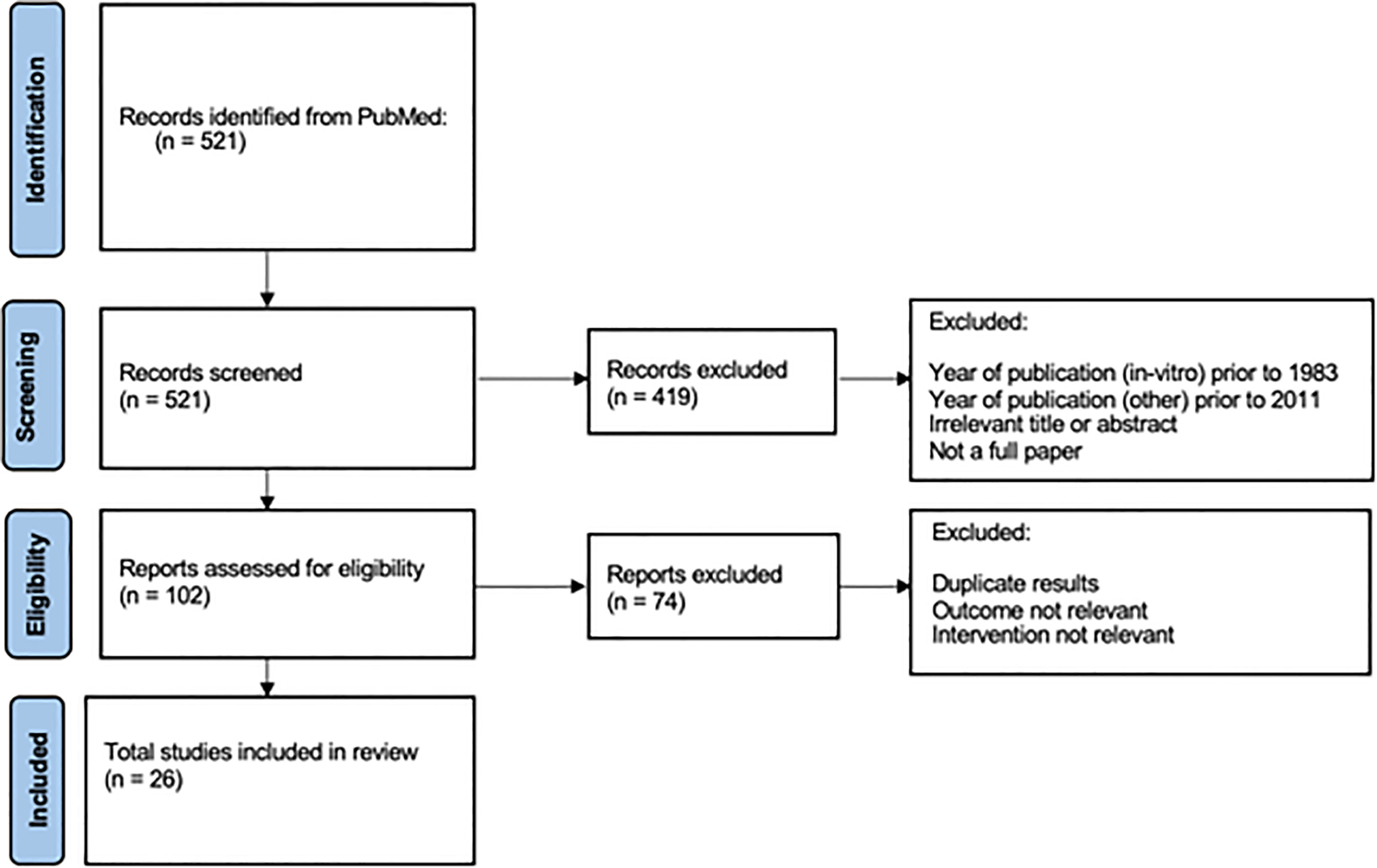
Figure 1 Literature search PRISMA flow diagram (1983-2022).
Included Studies
This systematic review includes a total of 26 articles: five prospective studies including 336 patients, three retrospective analyses including 540 patients, one phase III trial, one survival analysis, one randomized control trial, three systematic reviews, three meta-analyses, two in-vivo studies, three reviews, and four cost analyses. Baseline information extracted from these studies include: first author, published year, title, purpose, study design, number of samples, and results. These studies and characteristics (excluding results) are summarized in Table 1.
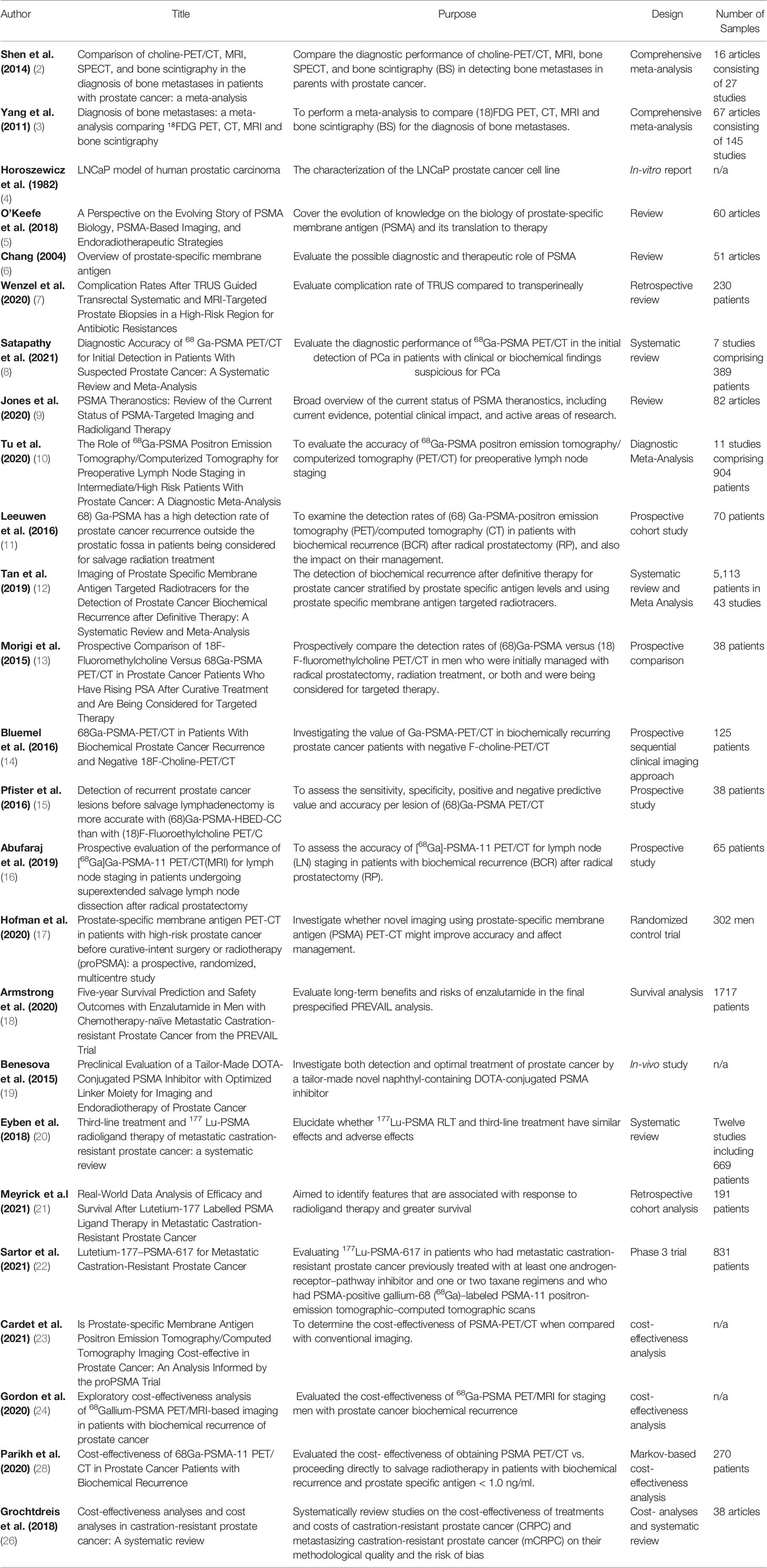
Table 1 Summary of included studies and study characteristics.
Methodological quality assessment
Articles were selected by title and abstract by 1 methodologist, and full articles were reviewed by the other authors. All studies were evaluated for bias and generalizability by a predefined set of criteria. The included studies were required to provide (1) appropriate study methodology, (2) appropriate sample size and follow-up, (3) relevant study objectives, (4) comprehensive and objective reporting of findings (5) discussion on the limitation and generalizability of findings, (6) detail on source of funding. The validity of the one randomized control trial included in this review were assessed using the Cochrane tool for assessing risk of bias in randomized trials (Table 2). Hofman et al. had 4 participants lost to follow up or withdrawal, however this was a small loss and balanced. As such, we evaluated this study as low risk for bias.

Table 2 Cochrane Tool for Assessing Risk of Bias in Included Randomized Control Trials.
Results
PSMA in Prostate Cancer Detection
The current standards for the initial diagnosis and staging of prostate cancer include a transrectal or transperineal ultra-sound (TRUS) guided biopsy often with magnetic resonance imaging (MRI) fusion when appropriate. Although biopsy is an effective screening tool, it is an invasive procedure with the potential morbidity of hematuria, hematochezia, hematospermia, and urosepsis (the latter when done via a transrectal approach) and may contribute to over-treatment (7). MRI, meanwhile, is non-invasive and considered an effective screening tool for clinically significant cancer due to its high sensitivity. Nevertheless, it is limited by its relatively low specificity and high range of negative predictive values (NPVs), thus necessitating a biopsy to confirm diagnosis (8). These limitations result in an unmet need for alternative, non-invasive diagnostic and staging modalities.
The first synthesized PSMA ligands, such as J591, aimed to fill this need but were restricted by their limited ability to penetrate tumors. These antibodies also had long half-lives, which resulted in an extended delay between time of injection and imaging. Furthermore, this resulted in high antibody accumulation before decay, which prolonged patient radiation exposure.
More recently, small-molecule PSMA inhibitors have been developed, further advancing PSMA therapy. These small molecule inhibitors are highly accurate in localizing prostate cancer lesions, have fast tumor uptake, and are rapidly excreted to minimize radiation exposure (9). Gallium-68 (68Ga)-PSMA has become one of the primary small-molecule tracers used in both the staging of de novo and recurrent disease.
Detection for Prostate Cancer Recurrence
Biochemical recurrence (BCR) following radical prostatectomy is conventionally defined as a PSA value greater than 0.2ng/mL on two separate occasions. However, the sensitivity of conventional imaging is poor, especially for PSA values this low (10). One of the first clinical roles of PSMA was for better detection of metastatic disease within this space. Figure 2 shows a PSMA PET/CT for detection of metastatic disease from a patient with BCR following radical prostatectomy treated by the Department of Surgery and Perioperative Care University of Texas at Austin Dell Seton Medical Center. The scan was performed with Piflufolastat F-18, a newly approved F-18-labeled PSMA-targeted PET imaging agent. The scan revealed metastatic disease in multiple lymph nodes, identified in the right pelvic sidewall that are metabolically active.
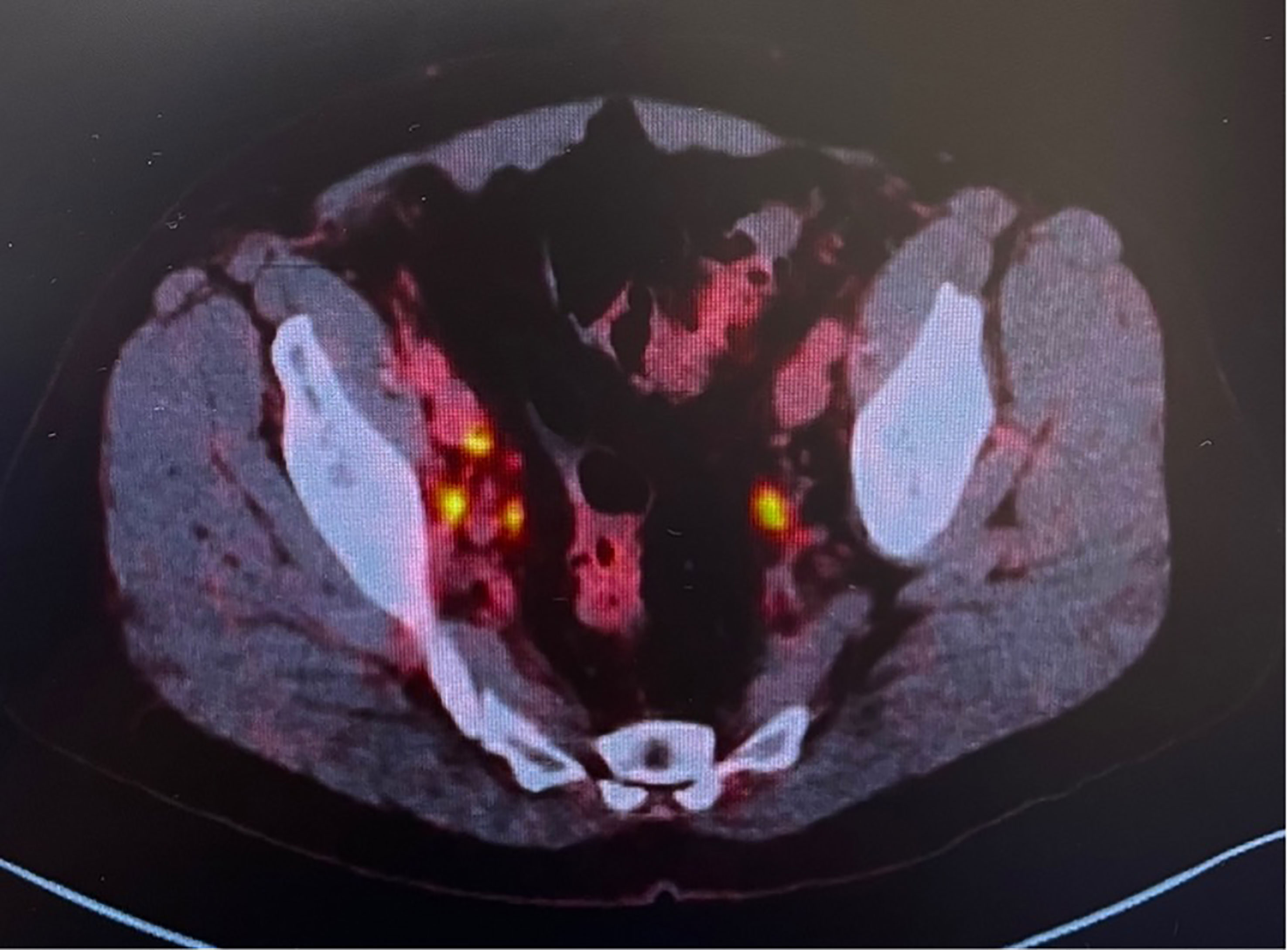
Figure 2 68Ga-PSMA PET/CT with intense tracer bilateral nodal uptake from Department of Surgery and Perioperative Care University of Texas at Dell Seton Medical Center.
A prospective study by Van Leeuwen et al. analyzed 300 patients with BCR following radical prostatectomy who underwent 68Ga-PSMA PET/CT. They found pathologic uptake in 54% of the cohort that resulted in significant management change in 28.6%. The management changes included enlarging the volume of the radiation template, shrinking the radiation field, adding adjuvant androgen deprivation therapy, or converting to a salvage lymph node dissection (11).
A systematic review by Tan et al. compared the detection rates of conventional imaging versus PMSA PET/CT based on 43 studies and 5113 patients with BCR prostate cancer and no known metastatic disease. For PSMA tracers, the detection rates were 45% for patients with PSA levels < 0.5 ng/mL, 61% for patients with PSA level 0.5-0.9 ng/mL, 78% for patients with PSA level 1.0-1.9 ng/mL, and 94% for patients with PSA level >2 ng/mL. Importantly, the rate of detection at PSA values of less than 0.5ng/mL were reported to be significantly higher than that of conventional imaging (12). Along these lines, a 2015 study by Morigi et al. prospectively compared detection capabilities of 68Ga-PSMA-11 versus conventional imaging using 18F-fluromethylcholine in 38 patients with recurrent prostate cancer. They found that in patients with biochemical failure and low PSA levels, PSMA had a significantly higher detection rate and a higher overall impact on management. When PSA was 0.5-2.0ng/mL the detection rate was 69% for 68Ga-PSMA versus 31% using 18F-fluromethylcholine. When PSA was above 2.0 the detection rate was 86% for 68Ga-PSMA versus 57% using 18F-fluromethylcholine. In addition, there was a 54% management impact due to 68Ga-PSMA imagine alone (13). Another study which only performed 68Ga-PSMA PET/CT in patients with negative 18F-fluromethylcholine PET/CT scans found that 68Ga-PSMA identified areas of recurrent disease in 43.8% of patients with negative 18F -fluromethylcholine scans (14).
PSMA has also shown utility when specific to identifying lymph node metastases. A study of 38 patients planning to undergo salvage lymphadenectomy found that 68Ga-PSMA PET/CT had better performance than 18F-fluromethylcholine PET/CT as the PSMA tracer had a significantly higher NPV (88.8% 18F-fluromethylcholine versus 96.6% 68Ga-PSMA) and higher accuracy to detect metastatic lesions (82.5% 18F-fluromethylcholine versus 91.9% 68Ga-PSMA) (15). Another prospective study of 65 patients with biochemical recurrence who underwent 68Ga-PSMA PET/CT prior to salvage lymph node dissection reported sensitivity ranging from 72%-100% and specificity ranging from 96%-100% (16).
Initial Prostate Cancer Detection
Until recently, few studies have considered the role of68Ga-PSMA PET/CT in the initial diagnosis of prostate cancer. A recent meta-analysis of seven studies compromising 389 patients evaluated 68Ga-PSMA PET/CT in initial prostate cancer diagnosis and found that the therapy had an excellent sensitivity of 97% and negative likelihood ratio of 5%. The researchers concluded that 68Ga-PSMA PET/CT has a high diagnostic accuracy for the initial detection of prostate cancer and has great potential as a rule-out test (8).
ProPSMA is a recent prospective randomized, multicentered study of 339 patients with high-risk, localized prostate cancer that investigated the accuracy of 68Ga-PSMA PET/CT versus conventional imaging. The primary outcomes were accuracy of first-line imaging for identifying pelvic nodal or distant-metastatic disease. The authors found that PSMA PET/CT had 27% greater accuracy than conventional imaging and outperformed conventional imaging in the detection of both pelvic nodal disease and distant metastases. The study also demonstrated that PSMA PET/CT resulted in less equivocal imaging and less radiation exposure, as well as greater sensitivity (85% vs 38%) and specificity (98% vs. 91%) (17). Altogether, 68Ga-PSMA PET/CT has superior diagnostic accuracy versus conventional imaging and may be a viable replacement. The 2021 National Comprehensive Cancer Network (NCCN) guidelines have been updated to reflect these changes as stated: “The NCCN panel has recognized the increased sensitivity and specificity of PSMA-PET tracers, compared to conventional imaging (CT, MRI) for detecting micrometastatic disease, at both initial staging and biochemical recurrence. The updated guidelines state that the NCCN Panel does not feel that conventional imaging is a necessary prerequisite to PSMA-PET and that PSMA-PET/CT or PSMA-PET/MRI can serve as equally effective, if not more effective front-line imaging tools for these patients” (27).
PSMA Theranostics
PSMA also appears to have a profound role in theranostics. Although there are an increasing number of medications and therapies approved for metastatic castration-resistant prostate cancer (mCRPC), median survival for chemotherapy-naïve patients remains only approximately 31-35 months (18). As such, there is a clinical need for therapies with an increased response. Recent developments of PSMA radioligands, specifically the small-molecule PSMA inhibitor 177Lu-PSMA, have demonstrated the potential to fill this need. Although multiple radioligands exist, 177Lu-PSMA has the preferred pharmacokinetic profile due to its reduced kidney uptake and low toxicity (19). 177Lu-PSMA is a macromolecular radiolabeled humanized monoclonal antibody that targets the extracellular region of PSA. Patients with a positive 68Ga-PSMA PET/CT are candidates for treatment with 177Lu-PSMA radioligand therapy (RLT), which targets the lesions revealed by 68Ga-PSMA PET/CT. Current data suggests that RLT decreases PSA in mCRPC, although its improvement with regard to overall survival is less certain. More data into its theranostics benefit are below.
A recent systematic review and meta-analysis found that 177Lu-PSMA RLT is particularly effective against advanced stage mCRPC refractory to standard therapeutic options such as enzalutamide and carbazitaxel. This study found patients with mCRPC treated with 177Lu-PSMA RLT had better treatment effects and fewer adverse effects versus third-line treatment agents. 177Lu-PSMA RLT resulted in a PSA decline ≥50% more often than the third line treatment (44% versus 22%, p=0.0002). They also report that adverse effects of third-line treatment caused discontinuation of treatment more often than for 177Lu-PSMA (22 of 66 patients versus 0 of 469 patents, p<0.001) (20). With regard to overall survival, initial studies reported rates comparable to the currently available third-line therapies (9).
A recent retrospective study of 191 patients with mCRPC treated with 177Lu-PSMA RLT found a low toxicity profile and a durable overall survival with median values (interquartile ranges) of 12 (5-18) months, PSA progression-free survival of 4 (3-8) months, and PET/CT progression-free survival of 6 (3-10) months. Most of the included patients (89.5%) had previously received first and second line systemic therapies. However, important factors associated with increased survival included having predominantly lymph node metastatic disease, chemotherapy-naïve status, and lower baseline PSA levels (21). These findings suggest 177Lu-PSMA RLT may provide some efficacy in mCRPC treatment and that 177Lu-PSMA is a promising candidate for therapy. Nevertheless, these findings are somewhat limited due to the lack of a comparative group.
Another recent international open-label, phase 3 randomized trial evaluating 177Lu-PSMA-617 RLT reported prolonged imaging-based progression-free survival and overall survival when RLT was added to standard care in patients with advanced, PSMA positive mCRPC (22). This study randomized 831 patients to either receive 177Lu-PSMA-617 RLT plus standard care or standard care alone. The standard care excluded chemotherapy, immunotherapy, 223Ra, and investigational drugs. The investigation found that 177Lu-PSMA-617 RLT significantly prolonged imaging-based progression-free survival (median 8.7 versus 3.4 months) and overall survival (median 15.3 months versus 11.3 months). It is important to note that the incidence of 30-day adverse events (Clavien-Dindo grade 3 or above) was higher with 177Lu-PSMA-617 RLT than without (52.7% versus 38%). However, quality of life was not affected, and the authors reported the adverse events may have been overestimated relative to control since the treatment duration varied among patients treated with 177Lu-PSMA-617. This trial was also limited as it was not double blinded and lacked a placebo group. While the theranostic potential of 177Lu-PSMA-617 is promising, these conclusions remain limited with randomized control trials still pending.
PSMA: Cost-Effective or Cost-Prohibitive?
Although the diagnostic and therapeutic potential of PSMA is promising, especially as its clinical applications continue to grow, the cost of treatment must also be factored in when considering applicability. Cardet et al. performed a cost-effectiveness analysis for PSMA as a diagnostic tool utilizing data from the proPSMA study and prospectively defined key inputs to compare the costs of patients with high-risk prostate cancer who underwent conventional imaging versus 68Ga-PSMA PET/CT. The analysis reports that the frank cost of PSMA PET/CT is essentially cost equivocal for metastatic disease detection versus conventional imaging ($1,140 AUD versus $1,181 AUD). For the cost-analysis, the authors adopted a societal perspective by assigning a monetary value to the cost associated with image delivery time to recognize the time-costs associated with the new imaging modality. From this perspective, overall scan costs increased but PSMA PET/CT cost remained lower with a cost of $1,203 AUD versus $1,412 AUD for conventional imaging. When the cost per scan was combined with the overall accuracy of detection, PSMA PET/CT remained most cost-effective as it was less costly and more accurate. The authors also analyzed PSMA PET/CT cost in relation to the accuracy of detection for each metastasis type (nodal and distant metastasis) separately. They found that PSMA PET/CT detection of nodal disease compared to conventional imaging resulted in a cost saving of $959 AUD per additional accurate detection, and PSMA PET/CT detection of distant metastasis resulted in a cost saving of $1,412 AUD per additional accurate detection (23). When this cost-saving was weighted against the probability of accurate metastasis detection observed from the proPSMA trial, PSMA PET/CT remained superior with a cost saving of $428 AUD per additional accurate diagnosis. This societal perspective cost-analysis importantly demonstrates that PSMA PET/CT is more cost-effective than conventional imaging for both metastasis types.
Another cost-effectiveness analysis of 68Ga-PSMA PET/CT as a modality to detect prostate cancer recurrence was performed by Gordon et al. using a decision-analytic model with Markov modelling chains. The primary measured outcomes were health system costs and years of survival over 10 years. The cost model was sensitive to the percentage of patients whose 68Ga-PSMA prostate cancer lesions were successfully detected, the cost of usual care, and 68Ga-PSMA follow-up investigations. In this study, utilizing 68Ga-PSMA cost $39,426 USD versus $44,667 USD with standard therapy. 68Ga-PSMA was found to be slightly more effective at 0.07 life years gained. The likelihood that 68Ga-PSMA was cost-effective at acceptable thresholds was 87% at the threshold of $34,626 USD. In all values tested, 68Ga-PSMA remained superior in cost-savings and higher life years. As such, the authors concluded that 68Ga-PSMA PET/CT, as a modality to detect prostate cancer recurrence, was cost-effective relative to usual care (24).
Parikh et al. also performed a Markov-based cost-effectiveness analysis focused on patients with metastatic M1 disease using 68Ga-PSMA PET/CT. They explored the cost-effectiveness of obtaining 68Ga-PSMA PET/CT versus proceeding directly to salvage radiotherapy for patients with BCR and a PSA < 1.0ng/mL. This differs from the previously discussed analysis which compared 68Ga-PSMA against the standard imaging modalities. Their analysis derived costs from Medicare fee schedules and the Veteran Affairs oral drug pricing list. Utilizing a life-long time horizon and willingness to pay threshold of $100,000/quality adjusted life years (QALY), 68Ga-PSMA PET/CT ($2,647 USD) was found to have a higher cost of $17,300 USD and a higher effectiveness of 0.29 QALYs versus no 68Ga-PSMA PET/CT. This translated to an incremental cost-effectiveness ratio of $60.4K/QALY below the pre-determined threshold. For their threshold analysis, PSMA PET/CT needed to be equal to or greater than $14,004 USD to no longer remain cost effective. With costs currently well below that, the authors concluded that 68Ga-PSMA is cost-effective (28).
With the above studies suggesting that 68Ga-PSMA is cost-effective or, at least, cost-neutral, adopting 68Ga-PSMA as the standard of care for the detection of recurrent prostate cancer deserves merit. With regard to initial prostate cancer detection, cost analysis studies still need to be performed. Nevertheless, given its diagnostic accuracy, it will also likely be cost-effective as well.
The cost-effectiveness of 177Lu-PSMA-617 in theranositcs needs to be determined, as the price of lutetium is still being finalized. Given the need for multiple treatments, it is reasonable to assume that the therapy will be costly. Nevertheless, treatment of metastatic prostate cancer is already associated with high personal and economic burden. Mean annual costs per patient with prostate cancer in the USA is estimated at $10,612 in initial phase after diagnosis, $2,134 for continuing care, and $33,691 in the last year of life. The total economic expenditure cost was estimated at $9.8 billion in 2006 (25). Grochtdreis et al. recently performed a systematic review of the cost-effectiveness of mCRPC treatments. They identified 38 articles on various mCRPC treatments and found that the cost-effectiveness of mCRPC is heavily dependent on the willingness to pay per quality adjusted life year gained (26). As such, high QALYs based on randomized control trials are needed to make informed decisions on the management of mCRPC and the financial impact it has on patients and the healthcare system. How lutetium falls into this, especially with a potentially very steep price tag, remains to be determined.
Conclusion
The diagnostic and therapeutic role of PSMA is an active and evolving area of research. This new advanced molecular imaging appears more efficacious and potentially cheaper than the standard treatment for patients with BCR of prostate cancer. High quality data and well performed cost-analysis have strengthened the enthusiasm for this new medical technology. Although a consensus has not yet been reached on its role as an initial diagnostic tool or ligand therapy, current evidence demonstrates that it will likely fill these unmet needs in prostate cancer management with the NCCN already incorporating it into its prostate cancer guidelines.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Author Contributions
The authors confirm contribution to the paper as follows: study conception: AL; study design: AL and S-HB; data collection: AL and S-HB; analysis and interpretation of results: AL, S-HB, MS, and SG; draft manuscript preparation AL, S-HB, MS, and SG. All authors reviewed the results and approved the final version of the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Cancer of the Prostate - Cancer Stat Facts. NIH: SEER (2021). Available at: https://seer.cancer.gov/statfacts/html/prost.html.
2. Shen G, Deng H, Hu S, Jia Z. Comparison of Choline-PET/ct, MRI, SPECT, and Bone Scintigraphy in the Diagnosis of Bone Metastases in Patients With Prostate Cancer: A Meta-Analysis. Skeletal Radiol (2014) 43(11):1503–13. doi: 10.1007/s00256-014-1903-9
3. Yang H-L, Liu T, Wang X-M, Xu Y, Deng S-M. Diagnosis of Bone Metastases: A Meta-Analysis Comparing 18fdg Pet, CT, MRI and Bone Scintigraphy. Eur Radiol (2011) 21(12):2604–17. doi: 10.1007/s00330-011-2221-4
4. Horoszewicz JS, Leong SS, Kawinski E. LNCaP Model of Human Prostatic Carcinoma. Cancer Res (1983) 43(4):1809–18.
5. O’Keefe DS, Bacich DJ, Huang SS, Heston WD. A Perspective on the Evolving Story of PSMA Biology, PSMA-Based Imaging, and Endoradiotherapeutic Strategies. J Nucl Med (2018) 59(7):1007–13. doi: 10.2967/jnumed.117.203877
7. Wenzel M, Theissen L, Preisser F, Lauer B, Wittler C, Humke C, et al. Complication Rates After Trus Guided Transrectal Systematic and MRI-Targeted Prostate Biopsies in a High-Risk Region for Antibiotic Resistances. Front Surg (2020) 7.
8. Surasi DS. Editorial Comment on “Diagnostic Accuracy of 68GA-PSMA PET/CT for Initial Detection in Patients With Suspected Prostate Cancer: A Systematic Review and Meta-Analysis.”. Am J Roentgenol (2021) 216(3):607.
9. Jones W, Griffiths K, Barata PC, Paller CJ. PSMA Theranostics: Review of the Current Status of PSMA-Targeted Imaging and Radioligand Therapy. Cancers (2020) 12(6):1367. doi: 10.3390/cancers12061367
10. Tu X, Zhang C, Liu Z, Shen G, Wu X, Nie L, et al. The Role of 68ga-PSMA Positron Emission Tomography/Computerized Tomography for Preoperative Lymph Node Staging in Intermediate/High Risk Patients With Prostate Cancer: A Diagnostic Meta-Analysis. Front Oncol (2020) 10.
11. van Leeuwen PJ, Stricker P, Hruby G, Kneebone A, Ting F, Thompson B, et al. 68ga-PSMA has a High Detection Rate of Prostate Cancer Recurrence Outside the Prostatic Fossa in Patients Being Considered for Salvage Radiation Treatment. BJU Int (2016) 117(5):732–9. doi: 10.1111/bju.13397
12. Tan N, Bavadian N, Calais J, Oyoyo U, Kim J, Turkbey IB. Imaging of Prostate Specific Membrane Antigen Targeted Radiotracers for the Detection of Prostate Cancer Biochemical Recurrence After Definitive Therapy: A Systematic Review and Meta-Analysis. J Urol (2019) 2(2):231–40. doi: 10.1097/JU.0000000000000198
13. Morigi JJ, Stricker PD, van Leeuwen PJ, Tang R, Ho B, Nguyen Q, et al. Prospective Comparison of 18F-Fluoromethylcholine Versus 68ga-PSMA Pet/CT in Prostate Cancer Patients Who Have Rising PSA After Curative Treatment and are Being Considered for Targeted Therapy. J Nucl Med (2015) 56(8):1185–90. doi: 10.2967/jnumed.115.160382
14. Bluemel C, Krebs M, Polat B, Linke F, Eiber M, Samnick S, et al. 68ga-PSMA-PET/CT in Patients With Biochemical Prostate Cancer Recurrence and Negative 18F-Choline-PET/CT. Clin Nucl Med (2016) 41(7):515–21. doi: 10.1097/RLU.0000000000001197
15. Pfister D, Porres D, Heidenreich A, Heidegger I, Knuechel R, Steib F, et al. Detection of Recurrent Prostate Cancer Lesions Before Salvage Lymphadenectomy is More Accurate With 68ga-PSMA-HBED-Cc Than With 18F-Fluoroethylcholine PET/CT.0. Eur J Nucl Med Mol Imaging (2016) 43(8):1410–7. doi: 10.1007/s00259-016-3366-9
16. Abufaraj M, Grubmüller B, Zeitlinger M, Kramer G, Seitz C, Haitel A, et al. Prospective Evaluation of the Performance of [68ga]Ga-PSMA-11 Pet/CT(MRI) for Lymph Node Staging in Patients Undergoing Superextended Salvage Lymph Node Dissection After Radical Prostatectomy. Eur J Nucl Med Mol Imaging (2019) 46(10):2169–77. doi: 10.1007/s00259-019-04361-0
17. Hofman MS, Lawrentschuk N, Francis RJ, Tang C, Vela I, Thomas P, et al. Prostate-Specific Membrane Antigen Pet-CT in Patients With High-Risk Prostate Cancer Before Curative-Intent Surgery or Radiotherapy (Propsma): A Prospective, Randomized, Multicentre Study. Lancet (2020) 395(10231):1208–16. doi: 10.1016/S0140-6736(20)30314-7
18. Armstrong AJ, Lin P, Tombal B, Saad F, Higano CS, Joshua A, et al. Five-Year Survival Prediction and Safety Outcomes With Enzalutamide in Men With Chemotherapy-Naïve Metastatic Castration-Resistant Prostate Cancer From the Prevail Trial. Eur Urol (2020) 78(3):347–57.
19. Benešová M, Schäfer M, Bauder-Wüst U, Afshar-Oromieh A, Kratochwil C, Mier W, et al. Preclinical Evaluation of a Tailor-Made DOTA-Conjugated PSMA Inhibitor With Optimized Linker Moiety for Imaging and Endoradiotherapy of Prostate Cancer. J Nucl Med (2015) 56(6):914–20. doi: 10.2967/jnumed.114.147413
20. von Eyben FE, Roviello G, Kiljunen T, Uprimny C, Virgolini I, Kairemo K, et al. Third-Line Treatment and 177LU-PSMA Radioligand Therapy of Metastatic Castration-Resistant Prostate Cancer: A Systematic Review. Eur J Nucl Med Mol Imaging (2018) 45(3):496–508. doi: 10.1007/s00259-017-3895-x
21. Meyrick D, Gallyamov M, Sabarimurugan S, Falzone N, Lenzo N. Real-World Data Analysis of Efficacy and Survival After Lutetium-177 Labelled PSMA Ligand Therapy in Metastatic Castration-Resistant Prostate Cancer. Target Oncol (2021) 16(3):369–80. doi: 10.1007/s11523-021-00801-w
22. Sartor O, de Bono J, Chi KN, Fizazi K, Herrmann K, Rahbar K, et al. Lutetium-177–PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. New Engl J Med (2021) 385(12):1091–103. doi: 10.1007/s10585-020-10027-1
23. de Feria Cardet RE, Hofman MS, Segard T, Yim J, Williams S, Francis RJ, et al. Is Prostate-Specific Membrane Antigen Positron Emission Tomography/Computed Tomography Imaging Cost-Effective in Prostate Cancer: An Analysis Informed by the PROPSMA Trial. Eur Urol (2021) 79(3):413–8. doi: 10.1016/j.eururo.2020.11.043
24. Gordon LG, Elliott TM, Joshi A, Williams ED, Vellla I. Exploratory Cost-Effectiveness Analysis of 68gallium-PSMA PET/MRI-Based Imaging in Patients With Biochemical Recurrence of Prostate Cancer. Clin Exp Metastasis (2020) 37(2):305–12.
25. Roehrborn CG, Black LK. The Economic Burden of Prostate Cancer. BJU Int (2011) 108(6):806–13. doi: 10.1111/j.1464-410X.2011.10365.x
26. Grochtdreis T, König H-H, Dobruschkin A, von Amsberg G, Dams J. Cost-Effectiveness Analyses and Cost Analyses in Castration-Resistant Prostate Cancer: A Systematic Review. PloS One (2018) 13(12). doi: 10.1371/journal.pone.0208063
27. GlobeNewswire News Room. NCCN Guidelines Updated to Include PSMA-Pet Imaging (2021). Available at: https://www.globenewswire.com/news-release/2021/09/14/2296247/0/en/NCCN-Guidelines-Updated-to-Include-PSMA-PET-Imaging.html.
Keywords: radioligand, prostate cancer, 177Lu-PSMA, 68Ga-PSMA, mCRPC, PSMA cost analysis, PSMA - prostate specific membrane antigen, PSMA
Citation: Belbina S-H, Schmolze MR, Gereta S and Laviana AA (2022) PSMA as a Target for Advanced Prostate Cancer: A Systematic Review. Front. Urol. 2:912558. doi: 10.3389/fruro.2022.912558
Received: 05 April 2022; Accepted: 23 June 2022;
Published: 18 July 2022.
Edited by:
Trushar Patel, University of South Florida, United StatesReviewed by:
Reza Sari Motlagh, Medical University of Vienna, AustriaEnrico Checcucci, Candiolo Cancer Institute (IRCCS), Italy
Copyright © 2022 Belbina, Schmolze, Gereta and Laviana. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Aaron A. Laviana, QWFyb24ubGF2aWFuYUBhdXN0aW4udXRleGFzLmVkdQ==