 Dusan Kostic1*†
Dusan Kostic1*† André Henrique Teruaki Kato1‡
André Henrique Teruaki Kato1‡ Laila Lima2‡
Laila Lima2‡ Patricia Palmeira2‡
Patricia Palmeira2‡ Rossana Pulcineli Vieira Francisco3
Rossana Pulcineli Vieira Francisco3 Victor Bunduki3‡
Victor Bunduki3‡ Vera Hermina Kalika Koch1†
Vera Hermina Kalika Koch1†- 1Pediatric Nephrology Unit, Instituto da Criança, Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo, São Paulo, Brazil
- 2Laboratory of Medical Investigations [Laboratório de investigações médicas (LIM)-36] - Instituto da Criança, Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo, São Paulo, Brazil
- 3Department of Obstetrics and Gynecology, Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo, São Paulo, Brazil
Objective: To investigate a selection of renal injury biomarkers in fetal congenital lower urinary tract obstruction (LUTO) and their potential to identify renal damage in significant obstructive patterns, eventually to benefit fetal intervention and predict the outcome in terms of survival.
Study Design: Ten fetuses with congenital LUTO were submitted to fetal urine analysis that included six renal injury biomarkers: Neutrophil gelatinase-associated lipocalin (NGAL), kidney injury molecule-1 (KIM-1), transforming growth factor beta-1 (TGF-β1), retinol-binding protein (RBP), cystatin C (uCyC), and microalbuminuria (µALB). The results were compared with urinary parameters of patients born with LUTO and healthy newborns.
Result: The majority of fetal biomarker levels showed significantly higher values when compared to all groups at birth with exception of KIM-1 and μALB. RBP and uCyC performed with 100% accuracy to identify severe renal damage in fetal LUTO.
Conclusion: Urine CyC, NGAL, RBP, and TGF-ß1 demonstrated high capability of identifying significant renal impairment due to severe LUTO and may contribute to currently used fetal medicine diagnostic parameters.
Introduction
Congenital urinary tract obstruction is considered the most frequent fetal anomaly detected by prenatal ultrasound (US) and the leading cause of chronic renal disease (CKD) in children (1). Lower urinary tract obstruction (LUTO), with an incidence of 2.2 – 3.3 per 10,000 births (2), is associated with high fetal and neonatal mortality, mostly due to severe early- to mid-gestation oligohydramnios (3). In male fetuses, the typical and most frequent LUTO-related anatomical abnormality is posterior urethral valve (PUV), 63%, while in females LUTO is associated with more complex and rare abnormalities such as cloacal plate dysgenesis and megacystis micro-colon syndrome (2). These malformations may present a wide and extreme spectrum of outcomes, from prenatal death to slightly reduced renal mass with almost normal function. The screening US is capable of identifying enlarged fetal urinary bladder starting from the 10th gestational week (GW), although its reliability to discriminate obstructive from non-obstructive (transitional) forms, as well as to provide postnatal renal function prognosis, is not completely understood and depends on the underlying etiology and the presence of associated malformations (4, 5). A few studies have shown that the earlier the US finding of megacystis is made, the poorer the outcome (6). This is attributed to the higher prevalence of the most severe obstruction patterns (e.g., urethral atresia) and frequent chromosomal aberrations in the first trimester of gestation (6). On the other hand, for up to 90% of fetuses with normal karyotype and bladder length < 15 mm the megacystis will resolve spontaneously (4, 5). Obstruction that occurs after 22 GW is associated with chronic interstitial nephropathy and its severity correlates with the duration and degree of obstruction (4, 7). Serial US is frequently used in prenatal follow-up while fetal amniotic fluid analytes are sometimes obtained to determine the indication for fetal bladder decompression, although several studies have shown that neither of these is sufficiently reliable to predict the final renal function outcome (8). Currently, this intervention is considered when fetal amniotic fluid analytes are higher than usual (sodium > 100 mg/dL, chloride > 110 mg/dL, Osmolarity > 210 mOsm/L, ß-2 microglobulin > 6 mg/L) and accompanied by oligohydramnios. However, the results and prognosis continue to be reserved and without obvious benefit for the child (9). In the last few decades, there has been an increasing interest and development of biomarkers for early detection of renal impairment, including their possible application in patients with congenital LUTO in order to better predict the postnatal outcome and eventually to benefit early intervention. In this study six urinary biomarkers of renal injury, neutrophil gelatinase-associated lipocalin (NGAL), kidney injury molecule-1 (KIM-1), transforming growth factor beta-1 (TGF-β1), retinol-binding protein (RBP), cystatin C (CyC), and microalbuminuria (µALB), were measured in fetal urine to verify their potential to identify renal damage in fetuses with known LUTO, which may eventually benefit fetal intervention, as well as to predict the outcome in terms of survival. These potential and novel biomarkers of tubular damage or glomerular filtration have already been tested in different clinical settings, proving their efficiency with variable success (10–14). The studies on fetal congenital LUTO are scant, mainly due to ethical and practical concerns, although the few that were performed brought some promising preliminary results (15).
Methods
This study is part of a larger and recently published longitudinal and prospective study on renal biomarkers in infants with LUTO in comparison to gestational age-matched healthy newborns with follow-up from birth to the end of the first year of life (16). The study protocol was approved by the institution’s Ethics Committee (Reg. N° 0383/11, CAPPesq—HCFMUSP), supported by São Paulo Research Foundation—FAPESP Grant (Reg. N° 2012/50337-9), and was carried out in accordance with the Declaration of Helsinki. Each participant signed an informed parental consent form. The study participants were recruited between June 2012 and June 2016 at the Fetal Medicine Unit, during prenatal US visits, between 16 and 32 GW. The LUTO inclusion criteria were based on the diagnosis of antenatal hydronephrosis with minimal grade III anterior-posterior renal pelvic diameter (by Grignon et al.), defined according to fetal US parameters (17) and LUTO (with or without hydronephrosis) with reduced amniotic fluid volume, renal cortex, increased or abnormal thickness of bladder wall or its volume (megacystis), fusiform dilatation of urethra (keyhole sign), etc. (18). The fetuses with severe congenital LUTO with the indication of invasive tests that excluded fetal chromosomal and genetic defects were submitted for fetal urine analysis which included six renal injury biomarkers: neutrophil gelatinase-associated lipocalin (NGAL), kidney injury molecule-1 (KIM-1), transforming growth factor beta-1 (TGF-β1), retinol-binding protein (RBP), cystatin C (CyC), and microalbuminuria (µALB). In addition, when indicated by a fetal medicine specialist, and exclusively in cases of an isolated LUTO with eventual unilateral or bilateral hydronephrosis, vesicoamniotic or bilateral pyeloamniotic shunting was also performed. The exclusion criteria for these procedures were: multi-fetal pregnancies, chromosomal anomalies, structural anomalies unrelated to LUTO, normal amniotic fluid volume or analytes, and maternal contraindications.
Fetal urine was obtained between the 16th and 32nd GW when deemed necessary and exclusively by fetal medicine specialists, using 18-22G needle bladder puncture, under local anesthesia and fetal US guidance. The results were compared with urine biomarker parameters of newborns with LUTO and healthy infants matched by gestational age, obtained between the 3rd and 7th day from birth and at 12 months of age (16). Postnatal urine was collected using collecting bags and the US was performed between the 3rd and 7th day of life and at 12 months of age. Infants with confirmed genetic diseases or other congenital anomalies, systemic diseases (e.g., necrotizing enterocolitis, respiratory distress syndrome, sepsis, and neonatal asphyxia), hyperbilirubinemia > 10 mg/dL at 7th day of life or after, hemolytic anemia, uncontrolled gestational hypertension and/or diabetes, severe chronic medical conditions, incomplete family history and/or clinical follow-up were excluded from the study. The urine samples were immediately centrifuged, and the supernatant stored at −70°C. Postnatal renal function was estimated by measuring levels of serum CyC and creatinine (sCr) to calculate glomerular filtration rate and by renal US that was performed in the first week of life and at 12 months of age. Urine NGAL, KIM-1, RBP, TGF-ß1, CyC, and serum CyC were measured using commercially available Quantikine® (R&D Systems, Inc., Minneapolis, MN, USA) kits and Multiskan MS® (Labsystems, Helsinki, Finland) microplate reader, strictly following manufacturer instructions. All obtained values were in the range of the standard curve provided by the manufacturer. Creatinine and μALB were processed on a Cobas C501® Chemistry Analyzer (Roche, Rotkreuz, Switzerland) and analyzed by modified Jaffé and nephelometric methods, respectively. All the biomarker samples were run in duplicate and normalized by uCr.
Statistical Analysis
Numerical variables were expressed as statistical measures: mean, standard deviation, median, and percentiles. Pearson’s chi-square test was used for the comparison between the groups in relation to the categorical variables. Student’s t-test was used for numerical variables with equal and unequal variances or the Mann-Whitney test for the comparison between groups. To evaluate the degree of discrimination of the outcomes, ROC curves and area under the curves (AUC) were obtained with respective confidence intervals for the aforementioned parameter and cutoff points that maximize sensitivity and specificity sum values. The margin of error used in statistical test decisions was 5%, and the intervals were obtained with 95% confidence. The Statistical Package for Social Sciences (IBM® SPSS® version 24 for IOS®, USA), MEDCALC® (version 14.8.1), and GraphPad Prism® (version 9) were used to perform statistical analyses.
Results
Ten fetuses with confirmed severe congenital LUTO with indication of invasive tests for fetal diagnosis of malformations and genetic conditions were included in the study (Figure 1). The mean gestational age at the time of inclusion was 26.8 ± 3.6 weeks. In terms of outcome, 5/10 fetuses were submitted to the legal termination of pregnancy, 2/10 were stillborn, and 3/10 were born full-term. The three surviving fetuses were submitted to fetal interventions between 31 and 32 GW, which included insertion of vesico-amniotic shunting (one case of anterior urethral valve, megapenis, and megaurethra) and bilateral pyelo-amniotic shunting (one case of bilateral hydronephrosis and one PUV case). They were followed for at least 1 year with the pediatric nephrology and urology teams. The comparison between the sub-groups of severely obstructed fetuses, 10 LUTO patients, and 24 healthy newborns (control group) in terms of demographic characteristics, such as gender (masculine: feminine = 2:1), ethnicity (African Brazilian: Caucasian = 1:1), maternal and final gestational age showed no statistical difference (p ≥ 0,18). Comparative analysis of urine biomarkers’ values in all groups is presented in Figure 2. Statistical significance of p < 0.001 was observed for RBP, NGAL, and uCyC when fetal values were compared with controls’ values at birth and at the age of 12 months. Fetal RBP, NGAL, TGF-ß1, and uCyC levels were significantly higher when compared to corresponding values from the subgroup of survivors with LUTO (p ≤ 0.01). The values of the same biomarkers observed in both subgroups, fetal and LUTO, were significantly elevated in comparison to their levels in the control group at birth (Figure 2).
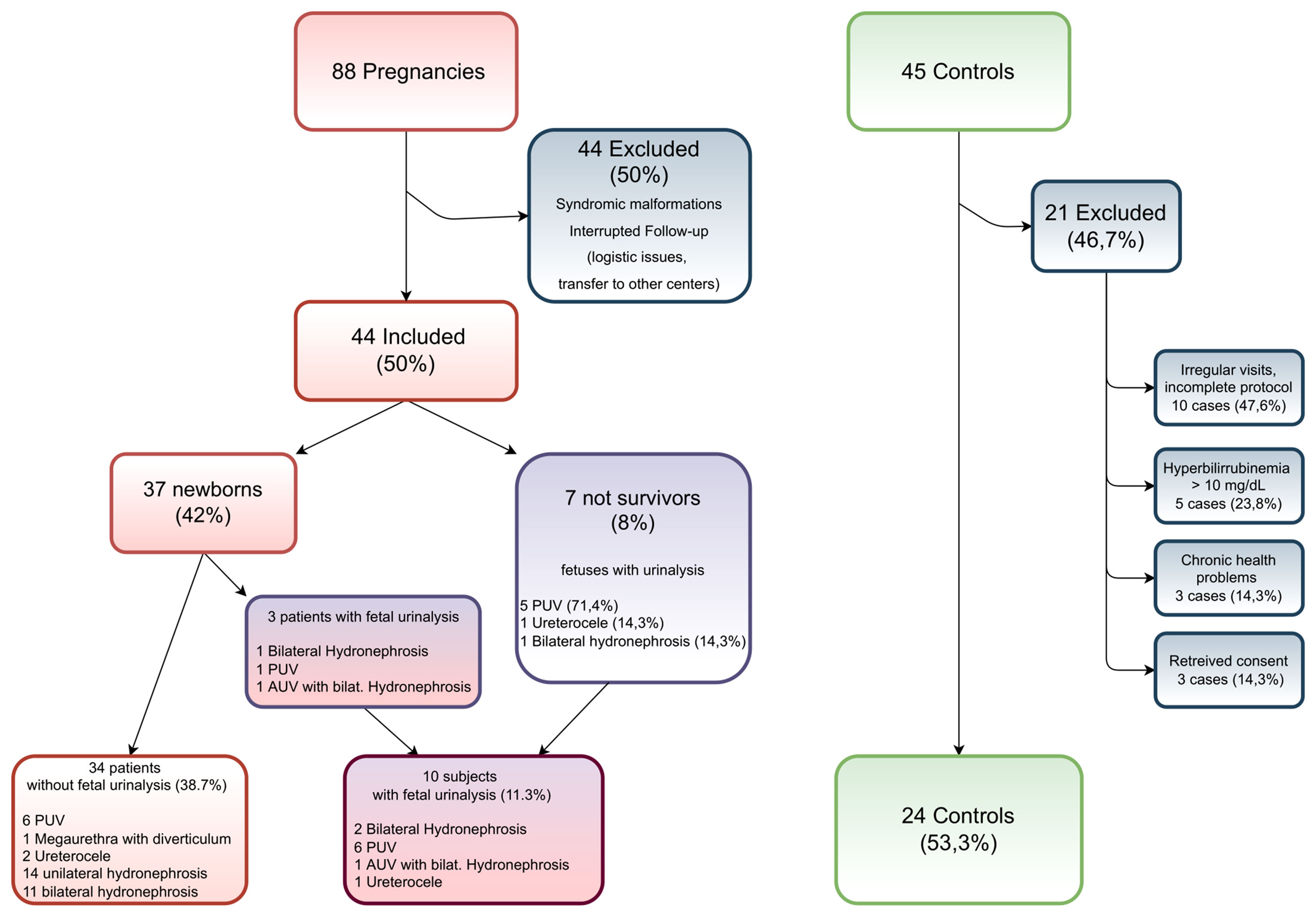
Figure 1 Recruitment dynamics in the period from June 2012 to June 2016. PUV, posterior urethral valve; AUV, anterior urethral valve.

Figure 2 Comparative analysis of urine biomarkers in fetuses, infants born with low urinary tract obstruction (LUTO), and healthy infant controls. RBP, retinol-binding protein; NGAL, neutrophil gelatinase-associated lipocalin; KIM-1, kidney injury molecule; TGF-ß1, transforming growth factor beta-1; uCyC, urine cystatin C; MALB, microalbuminuria; uCr, urine creatinine; LUTO, low urinary tract obstruction; statistical significance at p < 0.05, *) Mann-Whitney Test only.
Diagnostic performance of single renal biomarkers regarding identification of renal damage in fetal congenital LUTO (ROC curve, Figure 3) was considered excellent for RBP (cut-off value 727.3 ng/g), NGAL (cut-off value 2.88 ng/g), uCyC (cut-off value 11.37 ng/g), and TGF-ß1 (cut-off value of 6.17 pg/g). KIM-1 and µALB didn’t perform well at all (cut-off 0.67 ng/g, 58.3% specificity and 50% sensitivity; cut-off 20 mg/g, 20.8% specificity and 75% sensitivity, respectively).
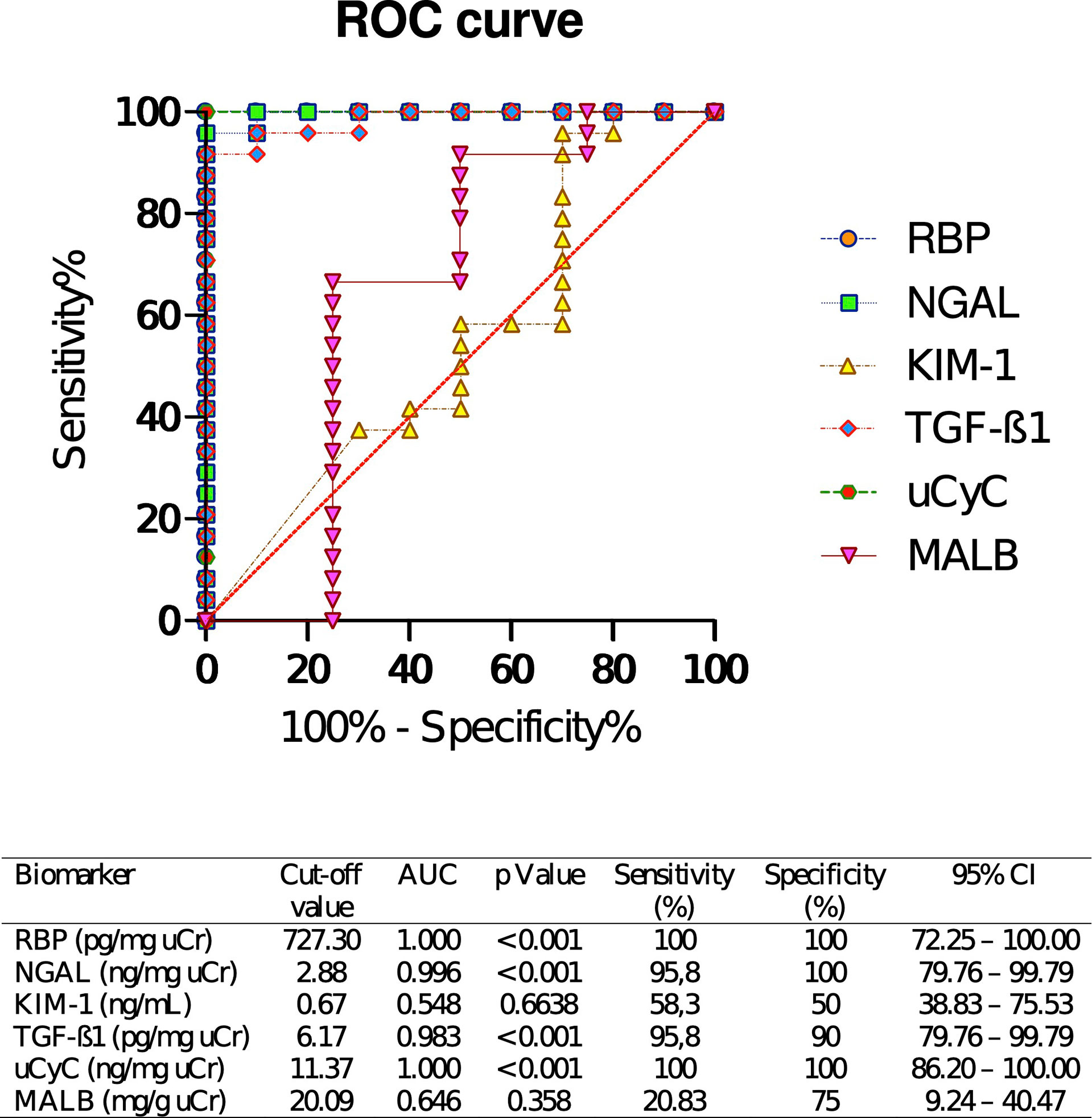
Figure 3 Diagnostic performance of renal injury biomarkers regarding the identification of renal damage due to fetal urinary tract obstruction. ROC, receiver operating characteristic curve; AUC, area under the curve (95% confidence interval); RBP, retinol-binding protein; NGAL, neutrophil gelatinase-associated lipocalin; MALB, microalbuminuria; uCyC, urine cystatin C; KIM-1, kidney injury molecule-1; TGF-ß1, transforming growth factor beta 1; uCr, urine creatinine.
At birth, the three surviving infants from the fetal group presented lower levels of urinary biomarkers in terms of absolute values when compared to non-survivors (80% lower in case of NGAL and RBP and 50% lower in case of uCyC, approximately), but still significantly above the control group range (Figure 4). Two of these patients were submitted to bilateral pyelo-amniotic shunting in the fetal period with KIM-1, TGF-ß1, and uCyC levels in the range of controls at 12 months of age. In all three patients, NGAL and MALB values remained higher when compared to controls’ values, mostly during the whole observational period while RBP and CyC levels were very high in the perinatal period and decreased with age, meeting the normal values throughout most of the observed period. However, the three survivors evolved to CKD stage 2, based on serum cystatin and serum creatinine values. During follow-up, they were maintained on alkali supplementation, on account of renal tubular acidosis, with satisfactory growth and development.
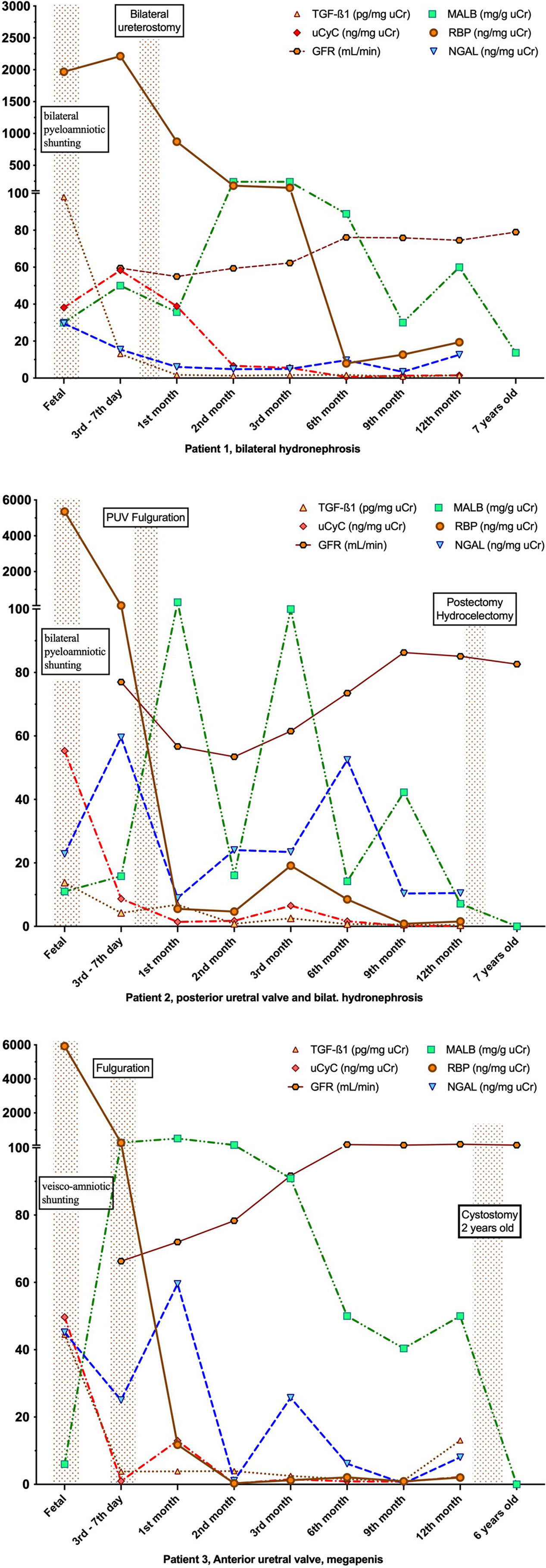
Figure 4 The first-year renal biomarkers profile of the infants submitted to fetal interventions and fetal urinalysis who survived and continued follow-up. RBP, retinol-binding protein; NGAL, neutrophil gelatinase-associated lipocalin; KIM-1, kidney injury molecule; TGF-ß1, transforming growth factor beta-1; uCyC, urine cystatin C; MALB, microalbuminuria; uCr, urine creatinine; GFR, glomerular filtration rate; PUV, posterior urethral valve.
Discussion
There are more than 4000 peptides in fetal urine, which may represent an important pool of potential biomarkers for the various developmental diseases in which early prediction could affect treatment and clinical decision-making. All currently available diagnostic methods are unsatisfactory in predicting postnatal renal function and may lead to unjustified offering of termination or continuation of the pregnancy resulting in early (in utero, at birth, or within the first months) end-stage CKD (8). This is the first study that evaluated the diagnostic performance of six urine biomarkers (RBP, NGAL, KIM-1, TGF-ß1, uCyC, and µALB) in the setting of fetal LUTO, compared to LUTO and healthy newborns matched by gestational age, with insight on postnatal renal function prediction. The present results show remarkably high fetal urine values for RBP, uCyC, and NGAL when compared to the control group, especially in non-survivors with 100% sensitivity and specificity for renal damage in severe LUTO. Relatively high RBP values in all the subgroups, in the fetal period and at birth, can be explained by its reduced excretion due to immaturity of the proximal convoluted tubule. In healthy individuals, the process of tubular maturation can extend until complete at 2 years of life, when the RBP excretion levels become stable and independent of age (19, 20).
The three survivors’ fetal values for RBP and uCyC were very high when compared to normal range but 80% and 50% lower, respectively, when compared to non-survivors. This finding is promising in terms of potential prediction of advanced stage CKD and lesser chance of survival, thus facilitating the decision for termination of pregnancy (when this option is legally available) or indication of fetal intervention in carefully selected cases. RBP, uCyC, NGAL, and TGF-ß1 seem to be better predictors of poor renal function and poor outcome, individually, when compared to the currently used urine parameters (8, 21, 22). Fetal uCyC was demonstrated to be superior to US and fetal urinary sodium to discriminate postnatal renal disease from preserved renal function (23). As soon as fetuses (especially with PUV) reach the 22nd GW, they may express elevated urine levels of several inflammatory biomarkers, including TGF-ß1, as a response to LUTO (24). The most important limitation of this study is the very low number of participants. This is principally due to rigorous legal and ethical policies involved in this type of investigation. The study was performed in a single center with a considerable loss of potential participants due to logistical issues, mainly because of frequent transfers to other centers or personal migrations to distant regions of the country. Regardless of these challenges, the verified fetal values were extremely high and doubtlessly merit consideration.
In conclusion, uCyC, NGAL, RBP, and TGF-ß1 demonstrated high capability in identifying significant renal impairment due to severe in utero LUTO, with the potential to discriminate between postnatal outcomes and perspective to contribute to currently used fetal medicine parameters.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Comissão de Ética para Análise de Projetos de Pesquisa da Faculdade de Medicina da Universidade de São Paulo, CAPPesq – HCFMUSP, Reg. N° 0383/11. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin. Written informed consent was obtained from the minor(s)’ legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article.
Author Contributions
All authors listed have made a substantial, direct, and intellectualcontribution to the work, and approved it for publication.
Funding
This research was funded by São Paulo Research Foundation - FAPESP Grant (Reg. N° 2012/50337-9).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Harambat J, van Stralen KJ, Kim JJ, Tizard EJ. Epidemiology of Chronic Kidney Disease in Children. Pediatr Nephrol (2012) 27:363–73. doi: 10.1007/s00467-011-1939-1
2. Malin G, Tonks AM, Morris RK, Gardosi J, Kilby MD. Congenital Lower Urinary Tract Obstruction:a Population-Based Epidemiological Study. BJOG (2012) 119:1455–64. doi: 10.1111/j.1471-0528.2012.03476.x
3. Freedman AL, Johnson MP, Gonzalez R. Fetal Therapy for Obstructive Uropathy: Past, Present, Future? Pediatr Nephrol (2000) 14:167–76. doi: 10.1007/s004670050035
4. Cheung KW, Morris RK, Kilby MD. Congenital Urinary Tract Obstruction. Best Pract Res Clin Obstet Gynaecol (2019) 58):78–92. doi: 10.1016/j.bpobgyn.2019.01.003
5. Liao AW, Sebire NJ, Geerts L, Cicero S, Nicolaides KH. Megacystis at 10-14 Weeks of Gestation: Chromosomal Defects and Outcome According to Bladder Length. Ultrasound Obstet Gynecol (2004) 21(4):338–41. doi: 10.1002/uog.81
6. Bornes M, Spaggiari E, Schmitz T, Dreux S, Czerkiewicz I, Delezoide AL, et al. Outcome and Etiologies of Fetal Megacystis According to the Gestational Age at Diagnosis. Prenat Diagn (2013) 33(12):1162–6. doi: 10.1002/pd.4215
7. Chevalier RL. Pathogenesis of Renal Injury in Obstructive Uropathy. Curr Opin Pediatr (2006) 18(2):153–60. doi: 10.1097/01.mop.0000193287.56528.a4
8. Klein J, Lacroix C, Caubet C, Siwy J, Zürbig P, Dakna M, et al. Fetal Urinary Peptides to Predict Postnatal Outcome of Renal Disease in Fetuses With Posterior Urethral Valves (PUV). Sci Transl Med (2013) 5(198):198ra106. doi: 10.1126/scitranslmed.3005807
9. Freedman AL, Bukowski TP, Smith CA, Evans MI, Berry SM, Gonzalez R. Use of Urinary Beta-2-Microglobulin to Predic Severe Renal Damage in Fetal Obstructive Uropathy. Fetal Dagn Ther (1997) 12(1):1–6. doi: 10.1159/000264415
11. Gerber C, Harel M, Lynch ML, Herbst KW, Ferrer FA, Shapiro LH. Proximal Tubule Proteins are Significantly Elevated in Bladder Urine of Patients With Ureteropelvic Junction Obstruction and may Represent Novel Biomarkers: A Pilot Study. J Pediatr Urol (2016) 12(2):e1–7. doi: 10.1016/j.jpurol.2015.10.008
12. Karakus S, Oktar O, Kucukgergin C, Kalelioglu I, Seckin S, Atar A, et al. Urinary IP-10, MCP-1, NGAL, Cystatin-C, and KIM-1 Levels in Prenatally Diagnosed Unilateral Hydronephrosis: The Search for an Ideal Biomarker. Urology (2016) 87:185–92. doi: 10.1016/j.urology.2015.09.007
13. Noyan A, Parmaksiz G, Dursun H, Ezer SS, Anarat R, Cengiz N. Urinary NGAL, KIM-1 and L-FABP Concentrations in Antenatal Hydronephrosis. J Pediatr Urol (2015) 11(5):249.e1–6. doi: 10.1016/j.jpurol.2015.02.021
14. Trnka P, Hiatt MJ, Tarantal AF, Matsell DG. Congenital Urinary Tract Obstruction: Defining Markers of Developmental Kidney Injury. Pediatr Res (2012) 72(5):446–54. doi: 10.1038/pr.2012.113
15. Buffin-Meyer B, Tkaczyk M, Stańczyk M, Breuil B, Siwy J, Szaflik K, et al. A Single-Center Study to Evaluate the Efficacy of a Fetal Urine Peptide Signature Predicting Postnatal Renal Outcome in Fetuses With Posterior Urethral Valves. Pediatr Nephrol (2020) 35:469–75. doi: 10.1007/s00467-019-04390-9
16. Kostic D, Beozzo G, do Couto S, Kato A, Lima L, Palmeira P, et al. The Role of Renal Biomarkers to Predict the Need of Surgery in Congenital Urinary Tract Obstruction in Infants. J Pediatr Urol (2019) 15(3):242.e1–9. doi: 10.1016/j.jpurol.2019.03.009
17. Grignon A, Filion R, Filiatrault D, Robitaille P, Homsy Y, Boutin H, et al. Urinary Tract Dilatation In Utero: Classification and Clinical Applications. Radiology (1986) 160(3):645–7. doi: 10.1148/radiology.160.3.3526402
18. Nguyen HT, Herndon CDA, Cooper C, Gatti J, Kirsch A, Kokorowski P, et al. The Society for Fetal Urology Consensus Statement on the Evaluation and Management of Antenatal Hydronephrosis. Jpurol (2010) 6:212–31. doi: 10.1016/j.jpurol.2010.02.205
19. Hua MJ, Kun HY, Jie CS, Yun NZ, De WQ, Yang Z. Urinary Microalbumin and Retinol-Binding Protein Assay for Verifying Children’s Nephron Development and Maturation. Clin Chim Acta (1997) 264(1):127–32. doi: 10.1016/s0009-8981(97)00086-7
20. Smith GC, Winterborn MH, Taylor CM, Lawson N, Guy M. Assessment of Retinol- Binding Protein Excretion in Normal Children. Pediatr Nephrol (1993) 8(8):148–50.. doi: 10.1007/BF00865463
21. Abdennadher W, Chalouhi G, Dreux S, Rosenblatt J, Favre R, Guimiot F, et al. Fetal Urine Biochemistry at 13–23 Weeks of Gestation in Lower Urinary Tract Obstruction: Criteria for in-Utero Treatment. Ultrasound Obstet Gynecol (2015) 46:306–11. doi: 10.1002/uog.14734
22. Dreux S, Rosenblatt J, Moussy-Durandy A, Patin F, Favre R, Lortat-Jacob S, et al. Urine Biochemistry to Predict Long-Term Outcomes in Fetuses With Posterior Urethral Valves. Prenatal Diagnosis (2018) 38:964–70. doi: 10.1002/pd.5359
23. Muller F, Bernard MA, Benkirane A, Ngo S, Lortat-Jacob S, JF O, et al. Fetal Urine Cystatin C as a Predictor of Postnatal Renal Function in Bilateral Uropathies. Clin Chem (1999) 45(12):2292–3. doi: 10.1093/clinchem/45.12.2292
Keywords: congenital urinary tract obstruction, hydronephrosis, renal biomarkers, fetus, kidney injury
Citation: Kostic D, Kato AHT, Lima L, Palmeira P, Francisco RPV, Bunduki V and Koch VHK (2022) Biomarkers for Early Detection of Renal Injury in Fetuses With Congenital Urinary Tract Obstruction. Front. Urol. 2:883903. doi: 10.3389/fruro.2022.883903
Received: 25 February 2022; Accepted: 11 May 2022;
Published: 15 June 2022.
Edited by:
Sachit Anand, Kokilaben Dhirubhai Ambani Hospital and Medical Research Institute, IndiaReviewed by:
Alessandro Boscarelli, Institute for Maternal and Child Health Burlo Garofolo (IRCCS), ItalyMarie-Klaire Farrugia, Chelsea and Westminster Hospital NHS Foundation Trust, United Kingdom
Copyright © 2022 Kostic, Kato, Lima, Palmeira, Francisco, Bunduki and Koch. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dusan Kostic, ZHVzYW4ua29zdGljQGhjLmZtLnVzcC5icg==
†These authors have contributed equally to this work and share first authorship
‡These authors have contributed equally to this work