
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Urol., 04 February 2022
Sec. Urologic Oncology
Volume 2 - 2022 | https://doi.org/10.3389/fruro.2022.819433
This article is part of the Research TopicWomen in Urologic Oncology: 2022View all 4 articles
 Anne S. Valiquette1,2
Anne S. Valiquette1,2 Natalia Vidal Crespo3*
Natalia Vidal Crespo3* Augusto Wong1Juan M. Mascarós1
Augusto Wong1Juan M. Mascarós1 Álvaro Gómez-Ferrer1
Álvaro Gómez-Ferrer1 Argimiro Collado-Serra1Jose L. Marenco1Juan Casanova Ramón-Borja1José Rubio-Briones1
Argimiro Collado-Serra1Jose L. Marenco1Juan Casanova Ramón-Borja1José Rubio-Briones1 Miguel Ramirez-Backhaus1
Miguel Ramirez-Backhaus1Introduction and Objectives: We report our experience with salvage lymph node dissection (sLND) in oligorecurrent prostate cancer (PCa) post radical prostatectomy (RP).
Material and Methods: We retrospectively analyzed data of 24 patients who underwent sLND for biochemical recurrence (BCR) post RP, from July 2012 to February 2018. sLND was performed following an extended bilateral template. Clinical and pathological characteristics of primary RP and sLND were reported. Biochemical response and initiation of additional therapy post sLND were analyzed. Survival analysis was performed using KaplanMeier curves.
Results: 24 sLND were performed. RP specimens showed 58.3% of Gleason score 7 and 50% of locally advanced disease. Median time to BCR post RP was 24 months with a median PSA value of 1.4 ng/ml pre sLND. 75% of patients underwent imaging prior to sLND. sLND showed oligometastasis on the final pathology report in 54.2% of patients. Metastatic lymph nodes were mainly identified in the iliac artery territory (61.5%). Complete biochemical response (PSA < 0.2 ng/ml) was maintained throughout the first 12 months of follow-up in 20.83% of patients and 8.33% of patients at the end of the study (median follow-up 70 months). Survival rates free of additional therapy (ADT/RT) were 45.83% at one year and 25% at 5 years.
Conclusions: We observed a biochemical response post sLND in 20.83% of our patients, lasting throughout the first year of follow up, with survival rates free of ADT and/or RT of 45.83% at one year and 25% at 5 years.
In 2021, more than 35 000 new cases of prostate cancer (PCa) will be diagnosed in Spain, and approximately 5 800 patients will die from this disease (1, 2). Some theories suggest that PCa evolves from a localized disease to an oligometastatic spread, before turning into a disseminated disease leading to death (3, 4). Moreover, we know that the location of metastasis has prognostic value in PCa. In fact, lymph node progression portends a better prognosis than bone and visceral metastasis (5–7). Historically, treatment in the context of oligoprogression to lymph nodes following radical prostatectomy (RP) was limited to salvage radiation therapy (RT) and/or androgen deprivation therapy (ADT). However, we have observed a trend in recent years toward more invasive treatment such as salvage lymph node dissection (sLND). To date, sLND has not demonstrated survival benefit or potential for cure in patients with biochemical recurrence (BCR) post RP but has led to complete biochemical responses (PSA < 0.2 ng/ml) in some patients, in addition to delaying ADT initiation (8–10). In this article, we report results from our cohort of 24 patients with BCR after RP, in which we performed sLND.
In our center, from July 2012 to February 2018, we performed 24 consecutive sLND in patients with BCR following RP. We included all patients in which this surgery was performed. Selection criteria were the documentation of BCR in patients previously treated with RP with or without evidence of lymph node metastasis on imaging, and a life expectancy of more than 10 years. Exclusion criteria were patients previously treated with salvage or adjuvant radiotherapy to the whole pelvis, evidence of distant metastasis, patients under ADT and the presence of a positive margin in the RP specimen (as it may suggest that the BCR is secondary to local recurrence on the prostatic fossa).
Patients had to sign a surgical consent for this procedure, after being informed that sLND is an experimental treatment with an estimated biochemical complete response rate of about 30- 40%. The data was collected prospectively in our clinical database after each case. Imaging was not routinely performed in all patients prior to sLND. When performed, patients underwent either bone scan, abdominopelvic CT scan, MRI and/or PET-choline, depending on the clinician criteria.
The surgical approach for sLND was either open or laparoscopic. The sLND template included the pre-sacral area, obturator fossa and external, internal, and common artery regions. Retroperitoneal lymph nodes were resected only if imaging revealed the presence of metastasis in this area. In patients who had undergone primary pelvic lymph node dissection during initial RP, image suspicion of nodal recurrence was always present. In these cases sLND was limited only to the anatomical area in which suspicious nodes were identified on imaging.
We recorded clinical and pathological characteristics of the primary RP, use of therapeutic and imaging modalities prior to sLND, time to BCR and PSA measurements before surgery. We also reported the pathology results of sLND.
During follow-up, 30-days complications related to sLND were reported. Scheduled PSA measurements were recorded at six weeks and at three, six and twelve months following sLND. Initiation of additional therapy post sLND, being either ADT and/or RT, was observed, and the number of deaths related to PCa at the end of the study was reported.
The oncological outcomes that we examined were biochemical response following sLND, timing and need for additional therapy (RT/ADT) and survival free of additional therapy. Complete biochemical response after sLND was defined as PSA < 0.2 ng/ml 6 weeks post sLND. Partial biochemical response was defined as a reduction in PSA values of more than 50% after sLND. Biochemical progression was defined as PSA ≥ 0.2 ng/ml after sLND, confirmed by two PSA measurements performed at least two weeks apart. Patients who received concurrent ADT post sLND or whose testosterone levels were in the castration range were excluded from the endpoint related to biochemical response post sLND. Means and medians were calculated. Survival analysis was performed with Kaplan-Meier curves. Data analysis was carried out using R language programming v. 3.6.3 (The R Foundation for statistical computing, Vienna, Austria). The study was approved by the ethics committee of our institution.
From July 2012 to February 2018, 24 sLND were performed in our center in the context of BCR post RP.
Table 1 shows the clinical characteristics of patients and pathological features at the time of the initial RP. Pathological analysis post RP revealed Gleason score 6 in 25.00% of patients, Gleason score 7 in 58.30% and Gleason scores from 8 to 10 in 16.70% of patients. Locally advanced disease (pT3a/b) was reported in 12 patients (50.00%). Positive surgical margins were observed in 9 patients (37.50%). Primary pelvic lymph node dissection was performed in only 7 patients (29.17%). The indication for LND at the initial RP was based on nomograms. Specifically, we use the Briganti nomogram (11) for selecting candidates to initial LND. Of these seven patients, two had pathologically confirmed lymph node metastasis (anatomical area of lymph nodes not specified).
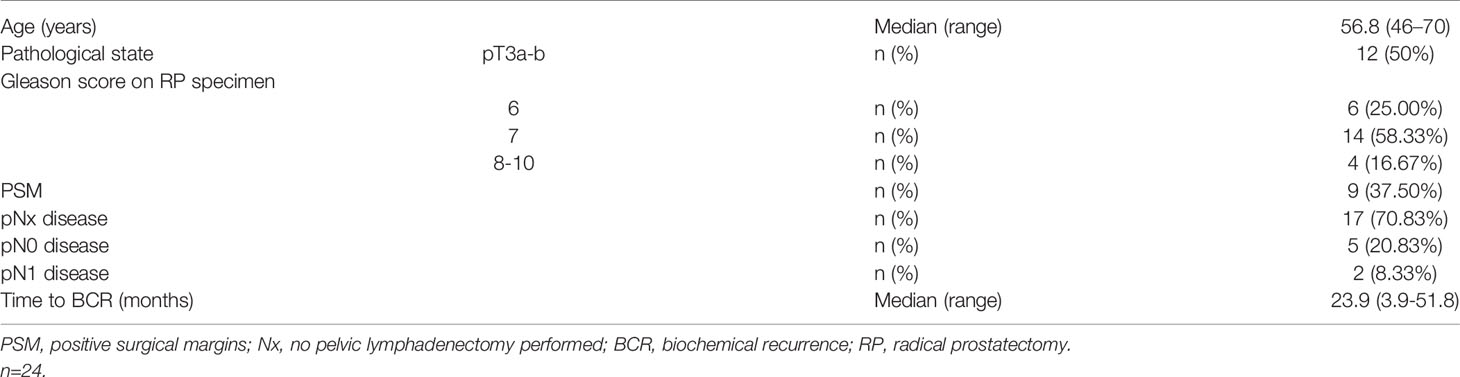
Table 1 Clinical and pathological characteristics of initial radical prostatectomy (RP).
All but one patient (who was pN1) achieved undetectable PSA post RP. 12 patients (50.00%) underwent adjuvant or salvage treatment post RP and before sLND. Eleven patients (45.83%) underwent adjuvant/salvage radiotherapy (RT) to the prostatic fossa with or without ADT and one patient was treated with ADT alone. The median time from RP to BCR was 24 months.
As shown in Table 2, the median PSA value prior to sLND was 1.4 ng/ml (range 0.2-8.3 ng/ml), and the median PSA doubling time was 5.4 months. Imaging studies were performed in 19 patients (79,17%) prior to sLND and revealed suspicious lymph nodes in 11 of these patients (45.83%). PET-choline, either alone or in combination with other imaging techniques, was used for detection of lymph node metastasis in a total of 13 patients (54.17%).
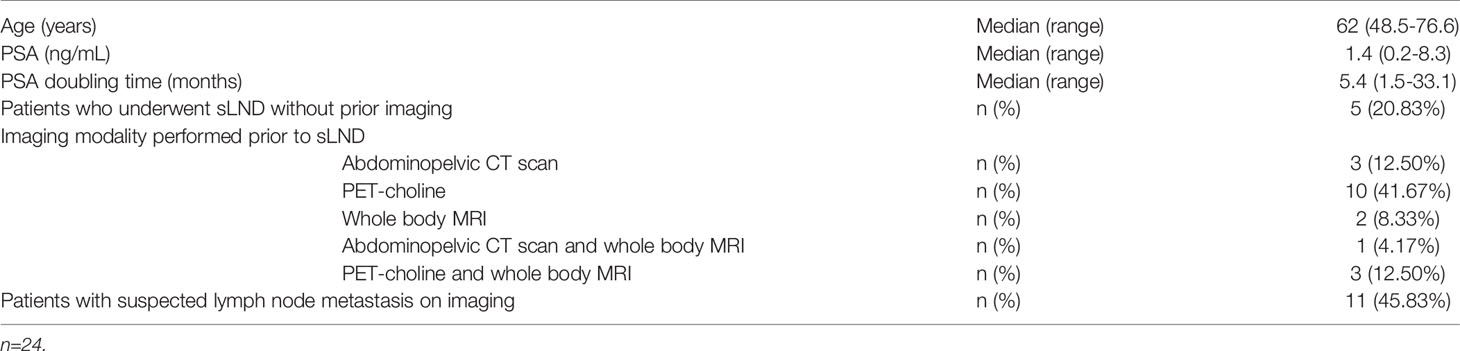
Table 2 Clinical characteristics prior to salvage lymph node dissection (sLND).
As demonstrated in Table 3, 75% of sLND surgeries were performed laparoscopically in our center. The median number of lymph nodes removed in each procedure was 20. 13 of the 24 patients (54.17%) who underwent sLND had lymph node metastasis on final pathological analysis. Concerning imaging studies prior to sLND in these 13 patients, 7 (53.85%) had evidence of suspicious lymph nodes, 4 (30.76%) had a negative radiologic workup and 2 (15.38%) did not undergo any kind of imaging study. Nodal metastasis in the iliac territory were found in 61.54% of the 13 cases with pathologically proven lymph nodes. Similarly, nodes in the obturator fossa were found in 53.85% of cases. Retroperitoneal and presacral positive lymph nodes were found in 1 and 2 patients respectively.
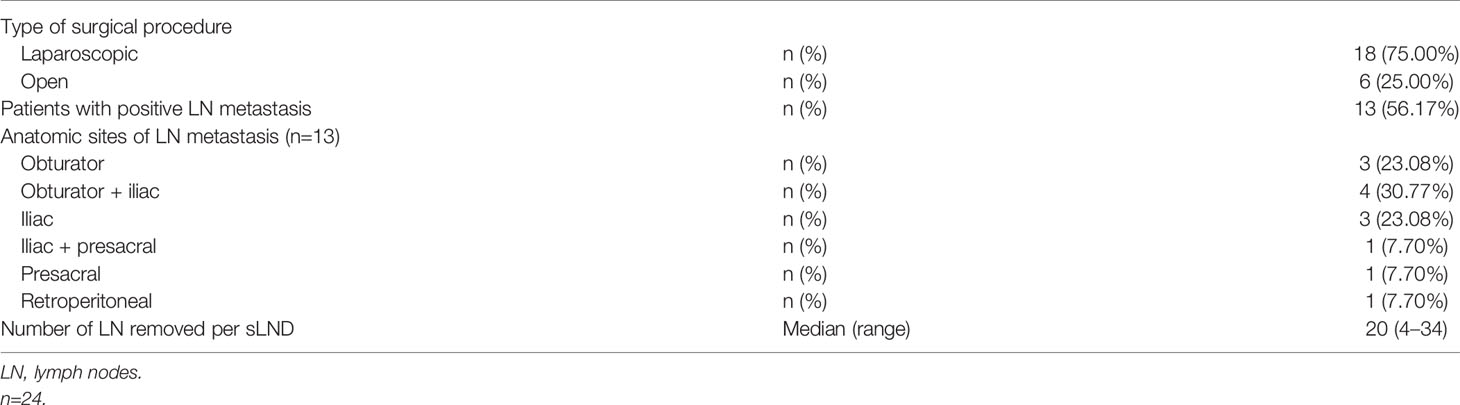
Table 3 Characteristics of salvage lymph node dissection (sLND).
Intra-operative and 30-day complications post sLND were reported. One patient underwent a complete ureteral transection during sLND, which required an intra-operative ureteral reimplantation. Concerning post-operative follow-up, grade IIIb complications, according to the Clavien-Dindo classification, were observed in 2 patients. A ureteral injury was reported, which required post-operative ureteral stenting. A second patient required an exploratory laparotomy with blood transfusion, in the context of post-operative blood loss and hemoperitoneum. Minor complications (Grade I) were also observed. 3 patients complained of post-operative paresthesias, related to iatrogenic trauma of the genitofemoral nerve and 2 patients required prolonged urethral catheterization, due to post-operative urinary retention. Table 4 shows the biochemical response of patients, during their scheduled follow-ups post sLND. 6 weeks post-surgery, 5 patients (20.83%) demonstrated a complete biochemical response (PSA < 0.2 ng/ml), which was maintained during the first year of follow-up. A persistent complete biochemical response was observed in 3 of these 5 patients during a follow-up period of 2 years. Patients who experienced a biochemical failure post sLND were either managed conservatively or treated with ADT and/or RT. Additional treatment free survival is shown in Figure 1. At 3 months, 5 patients (20.83%) received ADT either alone or combined with RT, compared to a total of 15 patients (62.50%) after 2 years of follow-up. At the end of the study, for a median follow-up of 70 months, 6 patients (25.00%) remained free of any additional therapy, and a total of 18 patients (75.00%) were treated with ADT and/or RT. A persistent complete biochemical response was observed in 2 patients (8.33%) at the end of the study period. Cancer-specific and overall survival were 95.83%, as only one patient died of PCa during the follow-up period (see Table 5).

Table 4 Biochemical response post sLND and need for additional therapy.
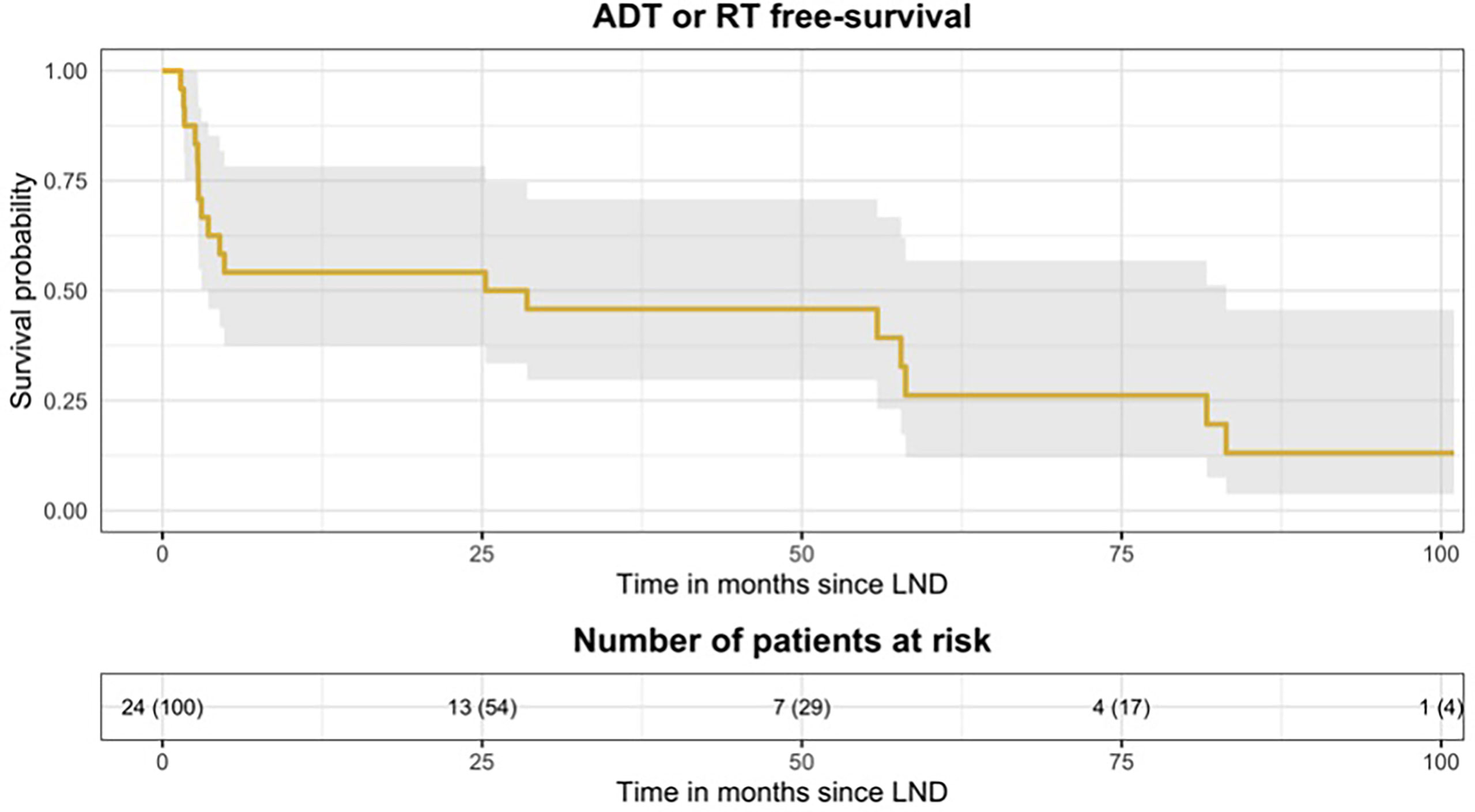
Figure 1 Kaplan Meier curve, representing survival free of additional therapy throughout the study period. At one year post sLND, survival rates free of any therapy (RT and/or ADT) were 45.83% compared to 25.00% at 5 years. sLND, salvage lymph node dissection; RT, Radio theraphy; ADT, Androgen deprivation theraphy.

Table 5 Oncological outcomes at the end of the study.
In our cohort, we reported a complete biochemical response (PSA 2ng/mL) post sLND in 20.83% of patients at one year post surgery and in 8.33% at the end of the study, with a median follow-up of 70 months. ADT/RT-free survival rates following sLND were 45.83% at one year and 25.00% at 5 years.
sLND is considered to be an experimental treatment alternative in patients with biochemical recurrence post RP, since most recurrences are initially observed in pelvic lymph nodes (3, 12). Available data shows that biochemical recurrence precedes the detection of metastatic lesions through conventional imaging by approximately 8-9 years (13, 14). The detection of metastasis depends largely on the sensitivity of imaging studies, but also on PSA values (absolute PSA and PSA kinetics) and pathological characteristics of the primary PCa.
New imaging modalities have emerged for earlier detection of PCa metastasis in the context of BCR, 68Ga-PSMA PET/CT being the most widely used. A large prospective study by Caroli et al. showed a 68Ga-PSMA PET/CT detection rate for metastasis of 27.3% for PSA 2ng/mL in recurrent PCa (15). Another recent meta-analysis by Perera et al. showed a detection rate of 45% for PSA between 0.2-0.5 ng/ml in recurrent PCa (16). Thus, 68Ga-PSMA PET/CT allows detection of metastasis at lower PSA measurements than conventional imaging, hence allowing earlier targeted therapy for oligorecurrence in lymph nodes. Specifically in this clinical scenario, a meta-analysis performed by Kimura et al. showed a higher accuracy of 68Ga-PSMA PET/CT to identify suspicious lymph nodes prior to sLND in patients with BCR, compared to more conventional imaging modalities (PET choline, standard abdominopelvic CT scans) (17). The pooled sensitivity using lesion-based analyses was 84%, with a positive predictive value ranging from 70-93%, for mean PSA values of 1.31 to 5.3 ng/mL. As a comparison, a review by Evangelista et al., examining the accuracy of PET choline prior to sLND, demonstrated a lesion-based pooled sensitivity of 56.2%, with a pooled positive predictive value of 81.2% (18). By better identifying the site of recurrence, 68Ga-PSMA PET/CT helps establish the appropriate management in BCR post RP, guiding toward either a local targeted therapy or a more systemic treatment. In fact, the impact of 68Ga-PSMA PET/CT on management of recurrent PCa has been examined in various studies (19–21). It was shown that choice of treatment was modified in up to 62% of cases following 68Ga-PSMA PET/CT. Sadly, 68Ga-PSMA PET/CT is not available in many centers in Spain and was not available in our center during our study period. 75% of our patients still underwent radiological staging with conventional imaging prior to sLND.
With sensitivity ranging between 64-85% in recurrent PCa, 68Ga-PSMA PET/CT clearly has a higher diagnostic accuracy than conventional imaging. However, general consensus still stipulates that with this reported sensitivity, it is not safe to perform a sLND only in the areas where suspicious nodes have been identified on 68Ga-PSMA PET/CT (22–24). In a study by Siriwardana et al, complete biochemical response at 6 weeks was observed in 90% of patients who underwent a bilateral extended template sLND, while only 21.4% of patients had a complete response following a targeted sLND, based on 68Ga-PSMA PET/CT identified lesions (22). Hence 68Ga-PSMA PET/CT is useful to guide therapeutic decision making, but for now, bilateral extended template dissection, alike the template used in our study, should remain the standard of care in sLND.One of the main benefits of performing sLND is to delay metastatic progression and initiation of additional therapy, either ADT and/or RT. A prospective, randomized, multicenter study by Ost et al. showed an increased length of ADT-free survival in patients undergoing sLND (21 months) compared to a control group undergoing surveillance only (13 months) (9). In a systematic review by Ploussard et al., following sLND, mean complete biochemical response rates of 44% (ranging from 13.0% to 79.5%) were observed in the first 2 months of follow-up. 64% of patients were ADT free at one year post sLND compared to 23% of patients at five years (10). In another recent large study by Bravi et al., they reported a 10y-BCR-free survival of 11%. Their ADT-free survival was 62% and 44% at 1 and 5 years, respectively (25).
Some retrospective studies have also compared treatment options for these lymphatic only recurrent patients (26–28). While it seems clear in all of them that sLND is a better option for these patients than just ADT, results from the SBRT/EBRT cohorts showed no difference between surgery and RT in this clinical setting (28). With the improved accuracy obtained with the previously mentioned new imaging tools, there is a certain security that recurrence is limited to what we see in the tests. Therefore, it seems logical that the directed treatment of such recurrence should obtain good outcomes. Whether the directed treatment should be performed with sLND or salvage RT remains to be answered.
In our study, we reported complete biochemical response rates of 20.83% at 3 months. Our ADT-free survivals of 54.17% at one year post sLND and 25% at 5 years are similar to some of those reported in Ploussard’s systematic review, for a comparable number of lymph nodes resected per sLND (20 vs 19.8 nodes). It is important to report that some series mentioned in this systematic review based their biochemical response analysis on patients who received either adjuvant ADT or RT post sLND, which could have favorably biased the results and overestimate the real complete response rate (10). This may be one reason to explain the discrepancy between their rates and those reported in our study. Another reason for such differences could be the positivity rate in final pathology. While in our cohort, pN1 after sLND patients represented 54.17%, large published series of sLND report rates that vary around 70%-83.2% (25, 29, 30). It must be pointed that, in most series, patient selection was based on PET/CT, which could be why they have a higher positivity rate than ours.
The backbone of sLND is to select the appropriate candidates who will benefit from this procedure. As discussed previously,68Ga-PSMA PET/CT pre sLND plays an important role in selection, but various other factors have been identified as predictive variables of oncological and clinical outcomes (29–34). In a large, multi-institutional study including 654 patients who underwent sLND for BCR post RP, Fossati et al. established a predictive model to help identify the optimal candidate that would benefit from the surgery. They reported various predictors of clinical recurrence post sLND: Gleason grade group 5, time from RP to PSA rise, use of salvage ADT pre sLND, characteristics of PET/CT scan uptake (retroperitoneal uptake and/or 3 or more positive spots on pre-op staging) and PSA level at sLND (33). Concerning PSA level at sLND, a cut-off of <4ng/mL has been reported in various studies as an indicator of good response post sLND (10, 29, 35). Many of the favorable variables mentioned were identified in our patients, reinforcing the idea that even if we didn’t benefit form pre-op PSMA, our choice of sLND candidates was appropriate.
Our study is not devoid of limitations. First, the retrospective and descriptive nature of our study, and the heterogeneity and small number of patients included should be considered as limitations. It is difficult to accurately evaluate the clinical benefit of performing sLND in the context of BCR, considering the heterogeneity of cases to which it applies. There is heterogeneity in the severity of initial disease, adjuvant therapies received, concomitant use of ADT, techniques and templates of sLND, imaging modalities used to detect lesions, etc. Moreover, we used biochemical response as a clinical endpoint in our study, which is not a proxy of survival. We think that the use of a control group in our study could have helped shed better light on the real clinical benefits of sLND in BCR post PR. As previously mentioned, we performed 5 sLND without prior imaging, and we didn’t have access to 68Ga-PSMA PET/CT prior to sLND in our study. It is precisely because of this reason that we performed some of the sLND without prior imaging or with a negative study. We considered that waiting for PSA values at which conventional imaging studies have a better sensitivity, it would lead to treatment delay. There is no doubt that imaging guided treatment is preferable. However, other treatment modalities such as adjuvant or salvage RT have been historically performed without prior imaging, with good results regarding progression free survival or metastasis free survival. We still believe that our data is important, especially considering the fact that 68Ga-PSMA PET/CT is not available in the majority of centers in Spain. Our data demonstrates that even without this diagnostic tool, patients can be selected to undergo sLND, with adequate complete response and ADT free survival rates.
In our study, we reported a complete biochemical response rate of 20.83% 6 weeks post sLND, lasting throughout the first year of follow-up with ADT/RT free survival rates of 25% at the end of the study, for a median follow-up of 70 months. We believe that with the use of 68Ga-PSMA PET/CT pre sLND, even higher complete response rates and ADT/RT free survival could be expected.
The raw data supporting the conclusions of this article will be made available by the authors upon request, without undue reservation.
The studies involving human participants were reviewed and approved by CEI (Comité de Ética Asistencial) of Instituto Valenciano de Oncología. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
AV had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: AW and MR. Acquisition of data: AV and AW. Analysis and interpretation of data: JM, AV, and MR. Drafting of the manuscript: AV and NV. Critical revision of the manuscript for important intellectual content: AW, AG-F, and AC, JM, JC, JR, and MR. Statistical analysis: JM. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Fitzmaurice C, Abate D, Abbasi N, Abbastabar H, Abd-Allah F, Abdel-Rahman O, et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2017: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol (2019) 5:1749–68. doi: 10.1001/jamaoncol.2019.2996
2. Sociedad Española de Oncología Médica. Cifras Del Cancer En España. (2021). Available at: https://seom.org/images/Cifras_del_cancer_en_Espnaha_2021.pdf
3. Mottet N, van Der Berg RCN, Briers E, van der Broeck T, Cumberbatch MG, De Santis M, et al. EAU - EANM - ESTRO - ESUR - SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur Urol (2021) 79(2):243–62. doi: 10.1016/j.eururo.2020.09.042
4. Brown M, Assen FP, Leithner A, Abe J, Schachner H, Asfour G, et al. Lymph Node Blood Vessels Provide Exit Routes for Metastatic Tumor Cell Dissemination in Mice. Science (2018) 359:1408–11. doi: 10.1126/science.aal3662
5. Guijarro A, Hernández V, de la Morena JM, Jiménez-Valladolid I, Pérez-Fernández E, de la Peña E, et al. Influencia De La Localización Y Del Número De Metástasis En La Supervivencia De Los Pacientes Con Cáncer De Próstata Metastásico. Actas Urol Esp (2017) 41:221–33. doi: 10.1016/j.acuro.2016.09.004
6. Weichselbaum RR, Hellman S. Oligometastases Revisited. Nat Rev Clin Oncol (2011) 8:378– 382. doi: 10.1038/nrclinonc.2011.44
7. Halabi S, Kelly WK, Ma H, Zhou H, Solomon NC, Fizazi K, et al. Meta-Analysis Evaluating the Impact of Site of Metastasis on Overall Survival in Men With Castration-Resistant Prostate Cancer. J Clin Oncol (2016) 34:1652–9. doi: 10.1200/JCO.2015.65.7270
8. Heidenreich A, Moul JW, Shariat S, Jeffrey Karnes R. Role of Salvage Lymph Node Dissection in Prostate Cancer. Curr Opin Urol (2016) 26:581–9. doi: 10.1097/MOU.0000000000000343
9. Ost P, Reynders D, Decaestecker K, Fonteyne V, Lumen N, DeBruycker A, et al. Surveillance or Metastasis-Directed Therapy for Oligometastatic Prostate Cancer Recurrence: A Prospective, Randomized, Multicenter Phase II Trial. J Clin Oncol (2018) 36:446–53. doi: 10.1200/JCO.2017.75.4853
10. Ploussard G, Gandaglia G, Borgmann H, de Visschere P, Heidegger I, Kretschmer A, et al. Salvage Lymph Node Dissection for Nodal Recurrent Prostate Cancer: A Systematic Review. Eur Urol (2019) 76:493–504. doi: 10.1016/j.eururo.2018.10.041
11. Gandaglia G, Fossati N, Zaffuto E, Bandini M, Dell’Oglio P, Bravi CA, et al. Development and Internal Validation of a Novel Model to Identify the Candidates for Extended Pelvic Lymph Node Dissection in Prostate Cancer. Eur Urol (2017) 72(4):632–40. doi: 10.1016/j.eururo.2017.03.049
12. Farolfi A, Gafita A, Calais J, Eiber M, Afshar-Oromieh A, Spohn F, et al. 68Ga-PSMA-11 Positron Emission Tomography Detects Residual Prostate Cancer After Prostatectomy in a Multicenter Retrospective Study. J Urol (2019) 202:1174–81. doi: 10.1097/JU.0000000000000417
13. Van den Broeck T, van den Bergh RCN, Arfi N, Gross T, Moris L, Briers E, et al. Prognostic Value of Biochemical Recurrence Following Treatment With Curative Intent for Prostate Cancer: A Systematic Review. Eur Urol (2019) 75:967–87. doi: 10.1016/j.eururo.2018.10.011
14. Gandaglia G, Abdollah F, Schiffmann J, Trudeau V, Shariat SF, Kim SP, et al. Distribution of Metastatic Sites in Patients With Prostate Cancer: A Population-Based Analysis. Prostate (2014) 74:210–6. doi: 10.1002/pros.22742
15. Caroli P, Sandler I, Matteucci F, De Giorgi U, Uccelli L, Celli M, et al. 68 Ga-PSMA PET/CT in Patients With Recurrent Prostate Cancer After Radical Treatment: Prospective Results in 314 Patients. Eur J Nucl Med Mol Imaging (2018) 45:2035–44. doi: 10.1007/s00259-018-4067-3
16. Perera M, Papa N, Roberts M, Williams M, Udovicich C, Vela I, et al. Gallium-68 Prostate-Specific Membrane Antigen Positron Emission Tomography in Advanced Prostate Cancer—Updated Diagnostic Utility, Sensitivity, Specificity, and Distribution of Prostate-Specific Membrane Antigen-Avid Lesions: A Systematic Review and Meta-Analysis. Eur Urol (2020) 77:403–17. doi: 10.1016/j.eururo.2019.01.049
17. Kimura S, Abufaraj M, Janisch F, Iwata T, Parizi MK, Foerster B, et al. Performance of [68Ga] Ga-PSMA 11 PET for Detecting Prostate Cancer in the Lymph Nodes Before Salvage Lymph Node Dissection: A Systematic Review and Meta-Analysis. Prostate Cancer Prostatic Dis (2020) 23:1–10. doi: 10.1038/s41391-019-0156-z
18. Evangelista L, Guttilla A, Zattoni F, Muzzio PC, Zattoni F. Utility of Choline Positron Emission Tomography/Computed Tomography for Lymph Node Involvement Identification in Intermediate- to High-Risk Prostate Cancer: A Systematic Literature Review and Meta-Analysis. Eur Urol (2013) 63(6):1040–8. doi: 10.1016/j.eururo.2012.09.039
19. Hoffmann MA, Wieler HJ, Baues C, Kuntz NJ, Richardsen I, Schreckenberger M. The Impact of 68Ga-PSMA PET/CT and PET/MRI on the Management of Prostate Cancer. Urology (2019) 130:1–12. doi: 10.1016/j.urology.2019.04.004
20. Roach PJ, Francis R, Emmett L, Hsiao E, Kneebone A, Hruby G, et al. The Impact of 68 Ga-PSMA PET/CT on Management Intent in Prostate Cancer: Results of an Australian Prospective Multicenter Study. J Nucl Med (2018) 59:82–8. doi: 10.2967/jnumed.117.197160
21. Hope TA, Aggarwal R, Chee B, Tao D, Greene KL, Cooperberg MR, et al. Impact of 68Ga-PSMA-11 PET on Management in Patients With Biochemically Recurrent Prostate Cancer. J Nucl Med (2017) 58:1956–61. doi: 10.2967/jnumed.117.192476
22. Siriwardana A, Thompson J, van Leeuwen PJ, Doig S, Kalsbeek A, Emmett L, et al. Initial Multicentre Experience of 68gallium-PSMA PET/CT Guided Robot-Assisted Salvage Lymphadenectomy: Acceptable Safety Profile But Oncological Benefit Appears Limited. BJU Int (2017) 120:673–81. doi: 10.1111/bju.13919
23. Mandel P, Tilki D, Chun FK, Pristupa E, Graefen M, Klutmann S, et al. Accuracy of 68Ga-Prostate-Specific Membrane Antigen Positron Emission Tomography for the Detection of Lymph Node Metastases Before Salvage Lymphadenectomy. Eur Urol Focus (2020) 6:71–3. doi: 10.1016/j.euf.2018.07.025
24. Krimphove MJ, Theissen LH, Cole AP, Preisser F, Mandel PC, Chun FKH. Performance and Impact of Prostate Specific Membrane Antigen-Based Diagnostics in the Management of Men With Biochemical Recurrence of Prostate Cancer and its Role in Salvage Lymph Node Dissection. World J Men’s Health (2020) 38:32–47. doi: 10.5534/wjmh.180133
25. Bravi CA, Fossati N, Gandaglia G, Suardi N, Mazzone E, Robesti D, et al. Long-Term Outcomes of Salvage Lymph Node Dissection for Nodal Recurrence of Prostate Cancer After Radical Prostatectomy: Not as Good as Previously Thought. Eur Urol (2020) 78(5):661–9. doi: 10.1016/j.eururo.2020.06.043
26. Steuber T, Jilg C, Tennstedt P, De Bruycker A, Tilki D, Decaestecker K, et al. Standard of Care Versus Metastases-Directed Therapy for PET-Detected Nodal Oligorecurrent Prostate Cancer Following Multimodality Treatment: A Multi-Institutional Case-Control Study. Eur Urol Focus (2019) 5(6):1007–13. doi: 10.1016/j.euf.2018.02.015
27. Boeri L, Sharma V, Nehra A, Kwon E, Karnes RJ. The Role of Salvage Lymph Node Dissection in Nonmetastatic Castration-Resistant Prostate Cancer: A Single Center Experience. Urol Oncol Semin Orig Investig (2020) 38(2):38. doi: 10.1016/j.urolonc.2019.09.016
28. Boeri L, Sharma V, Kwon E, Stish BJ, Davis BJ, Karnes RJ. Oligorecurrent Prostate Cancer Treated With Metastases-Directed Therapy or Standard of Care: A Single-Center Experience. Prostate Cancer Prostatic Dis (2021) 24:514–23. doi: 10.1038/s41391-020-00307-y
29. Rigatti P, Suardi N, Briganti A, Da Pozzo LF, Tutolo M, Villa L, et al. Pelvic/retroperitoneal Salvage Lymph Node Dissection for Patients Treated With Radical Prostatectomy With Biochemical Recurrence and Nodal Recurrence Detected by [11C]Choline Positron Emission Tomography/Computed Tomography. Eur Urol (2011) 60:935–43. doi: 10.1016/j.eururo.2011.07.060
30. Porres D, Pfister D, Thissen A, Kuru TH, Zugor V, Buettner R, et al. The Role of Salvage Extended Lymph Node Dissection in Patients With Rising PSA and PET/CT Scan Detected Nodal Recurrence of Prostate Cancer. Prostate Cancer Prostatic Dis (2017) 20:85–92. doi: 10.1038/pcan.2016.54
31. Zattoni F, Nehra A, Murphy CR, Rangel L, Mynderse L, Lowe V, et al. Mid-Term Outcomes Following Salvage Lymph Node Dissection for Prostate Cancer Nodal Recurrence Status Post–radical Prostatectomy. Eur Urol Focus (2016) 2:522–31. doi: 10.1016/j.euf.2016.01.008
32. Jilg CA, Rischke HC, Reske SN, Henne K, Grosu AL, Weber W, et al. Salvage Lymph Node Dissection With Adjuvant Radiotherapy for Nodal Recurrence of Prostate Cancer. J Urol (2012) 188:2190–7. doi: 10.1016/j.juro.2012.08.041
33. Fossati N, Trinh QD, Sammon J, Sood A, Larcher A, Sun M, et al. Identifying Optimal Candidates for Local Treatment of the Primary Tumor Among Patients Diagnosed With Metastatic Prostate Cancer: A SEER-Based Study. Eur Urol (2015) 67:3–6. doi: 10.1016/j.eururo.2014.08.056
34. Suardi N, Gandaglia G, Gallina A, Di Trapani E, Scattoni V, Vizziello D, et al. Long-Term Outcomes of Salvage Lymph Node Dissection for Clinically Recurrent Prostate Cancer: Results of a Single-Institution Series With a Minimum Follow-Up of 5 Years. Eur Urol (2015) 67:299–309. doi: 10.1016/j.eururo.2014.02.011
Keywords: prostate cancer, oligorecurrence, biochemical recurrence, salvage lymph node dissection, radical prostatectomy
Citation: Valiquette AS, Vidal Crespo N, Wong A, Mascarós JM, Gómez-Ferrer Á, Collado-Serra A, Marenco JL, Casanova Ramón-Borja J, Rubio-Briones J and Ramirez-Backhaus M (2022) Outcomes of Salvage Lymph Node Dissection in Oligorecurrent Prostate Cancer Post Radical Prostatectomy: Experience of an Oncologic Center in Spain. Front. Urol. 2:819433. doi: 10.3389/fruro.2022.819433
Received: 21 November 2021; Accepted: 07 January 2022;
Published: 04 February 2022.
Edited by:
Gian Maria Busetto, University of Foggia, ItalyReviewed by:
Giovanni Battista Di Pierro, Sapienza University of Rome, ItalyCopyright © 2022 Valiquette, Vidal Crespo, Wong, Mascarós, Gómez-Ferrer, Collado-Serra, Marenco, Casanova Ramón-Borja, Rubio-Briones and Ramirez-Backhaus. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Natalia Vidal Crespo, bmF0YWxpYS52aS5jcmVAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.