
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Urol., 08 November 2022
Sec. Pediatric, Adolescent and Developmental Urology
Volume 2 - 2022 | https://doi.org/10.3389/fruro.2022.1042689
 Giuseppe Aiello1†
Giuseppe Aiello1† Alessandro Morlacco1,2*†Marta Bianco1,2Matteo Soligo3
Alessandro Morlacco1,2*†Marta Bianco1,2Matteo Soligo3 Davide Meneghesso4
Davide Meneghesso4 Enrico Vidal4Waifro Rigamonti2
Enrico Vidal4Waifro Rigamonti2 Fabrizio Dal Moro1,2
Fabrizio Dal Moro1,2Purpose: Endoscopic treatment with high-pressure balloon dilatation (HPBD) has been proposed as a feasible, safe and minimally invasive procedure for primary obstructive megaureter, but the level of evidence is still low. This systematic review aims to evaluate the efficacy and safety of HPBD and its long-term results in paediatric population.
Methods: The review was conducted following the PRISMA guidelines. Systematic research of available literature in the English language from 1995 until June 2022 was conducted through EMBASE, MEDLINE, Cochrane Library and NIH Registry of Clinical Trials. For each relevant study, information was gathered regarding the study design, the inclusion/exclusion criteria, the indications for treatment, the success rate and the complications.
Results: The final set included 13 studies. Median age of the patients ranged from 4 months to 7 years (full range 15 days-15 years). The indications for HPBD varied in different studies, however most authors included patients with increasing dilation, obstructive patterns found at diuretic renogram scan, decreased renal function or symptoms. All the studies analysed reported a success rate ranging from 69 to 100% for the treatment of POM with HPBD. This approach may avoid surgery in up to 77% of cases and is thought to be a less invasive, definitive and safe treatment for this disorder. The complication rate ranged from 0 to 50% and it was mostly infectious or associated to the stent placement or both.
Conclusion: HPBD demonstrated to be safe for the treatment of POM in infants, with effective long-term results and can be a definitive treatment in a considerable subset of patients. Nevertheless, the overall level of evidence for HPBD is still low and further comparative studies or randomized clinical trials are needed.
Megaureter is defined as a congenital dilated ureter larger than 7 mm (1). A different classification was made by Smith, who identified four categories of megaureters: refluxing, obstructive, refluxing and obstructive, or non-refluxing and non-obstructive. King subdivided these categories into primary and secondary (2).
Primary obstructive megaureter (POM) is due to terminal ureter anomaly creating a functional obstruction (adynamic ureteral segment). This anomaly is thought to be caused by a delay in smooth muscle differentiation, and the process of differentiation may last up to a couple of years, explaining the possible spontaneous resolution of primary obstructive megaureter in approximately 80% of cases (3). For this reason, most of megaureters are treated conservatively, especially in children under one year of age. Indications for surgical management are: progressive increase in ureteral diameter, impairment of split renal function, or symptoms (recurrent UTIs, pain, stones or haematuria) (4).
The traditional surgical approach of POM consists of distal ureteral reimplantation with or without ureteral remodelling (tapering or tailoring), which is reported to have a success rate of 90–96%. However, it has high complication and morbidity rates, especially during the first year of life, when reimplantation of a dilated ureter in a tiny bladder can be technically challenging and may lead to several complications such as vesicoureteral reflux (VUR), secondary obstruction or bladder dysfunction (3, 5, 6).
POM treatment with HPBD was first described in 1998 by Angulo et al. (7). From then on, many authors have shown the feasibility and safety of this minimally invasive procedure, even for children under 1 year of age (6, 8–10). During the last years, authors have been focused their interest on long-term effectiveness of this procedure. However, its validity as a definitive treatment is uncertain, since only small case series have been reported.
This systematic review aims to evaluate the efficacy and safety of HPBD and its long-term results in paediatric population.
The review was conducted following the PRISMA guidelines. A comprehensive search of terms (megaureter, endoscopic dilation, endoscopic dilatation, balloon, high-pressure balloon, POM, primary megaureter, endourological treatment) was conducted through EMBASE, MEDLINE, Cochrane Library and NIH Registry of Clinical Trials in the English language from 1995 until June 2022. For each relevant study, information was gathered regarding the study design, the inclusion/exclusion criteria, the indications for treatment, the success rate and the complications. Two authors (AM and MB) undertook the study selection, screening the titles and abstracts of articles found in the search and discarding those which did not meet the eligibility criteria. Full text copies of the eligible articles were obtained.
Overall, after initial screening, 29 studies were retrieved, after removing duplicates and irrelevant findings 20 studies were eligible for full text evaluation. The final set included 13 studies. The complete process selection is shown in Figure 1.
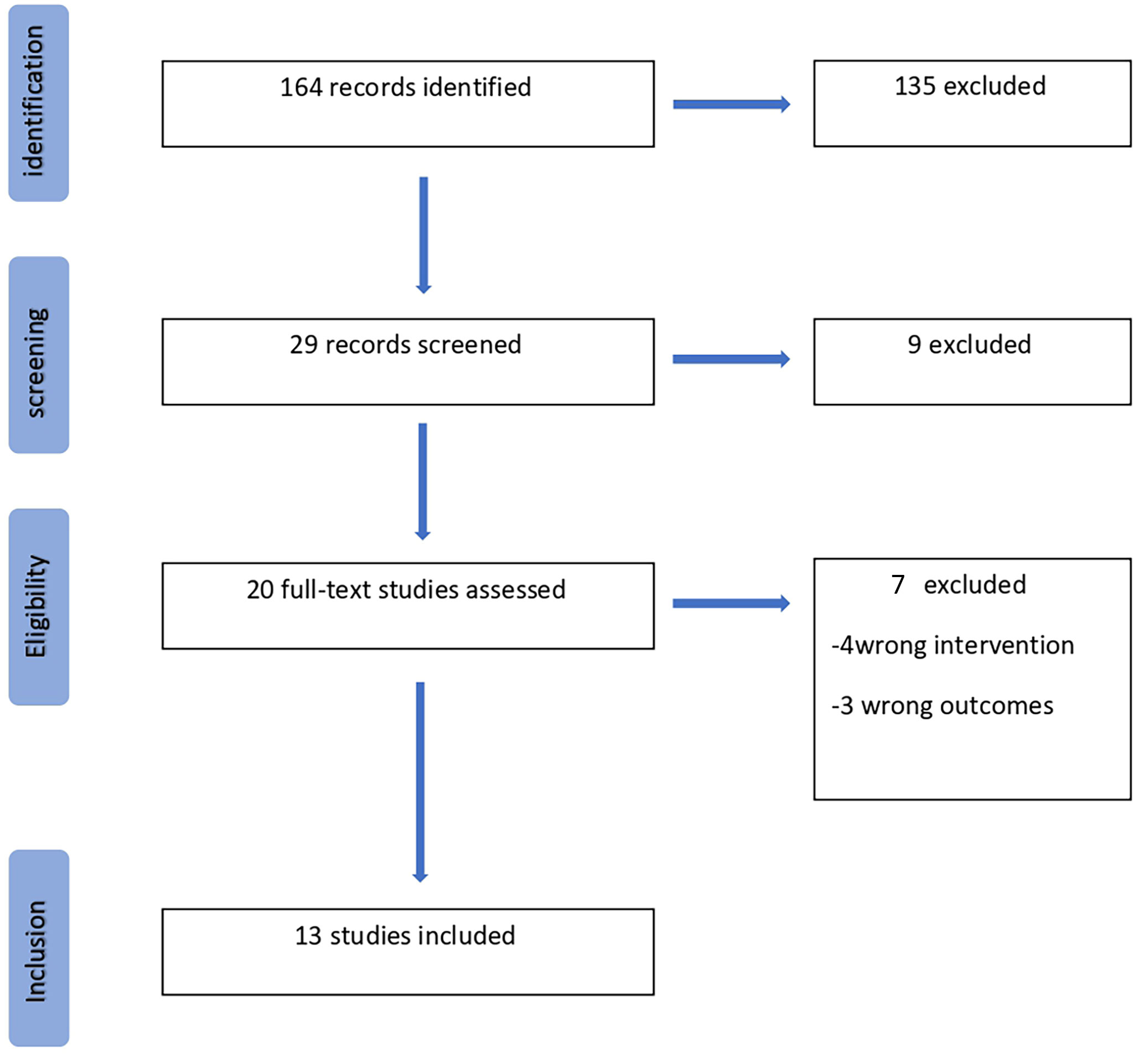
Figure 1 Flow diagram of the study.
Characteristics of the included studies are summarized in Table 1. All studies were retrospective, no RCTs nor prospective comparative studies were found.
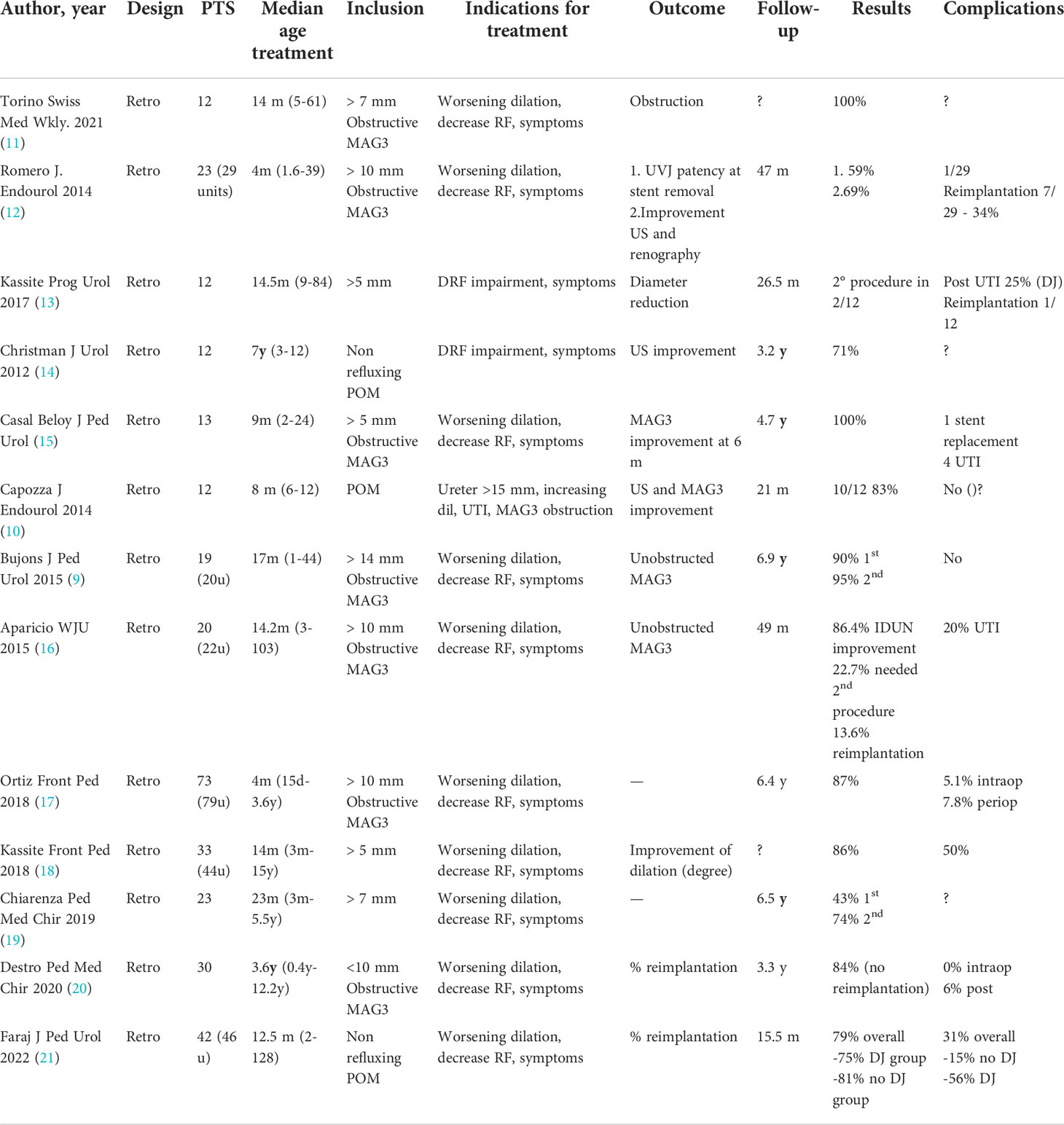
Table 1 Characteristics and outcomes of the included studies.
Median age of the patients ranged from 4 months to 7 years (full range 15 days-15 years). The indications for HPBD varied in different studies, however most authors included patients with increasing ureteral dilation, symptoms, and decreased split renal function or obstructive patterns found at diuretic renogram scan. Two studies (13, 14) included patients with differential renal function impairment and symptoms; one study (10) included patients with dilated ureter larger than 15 mm, increasing dilation, urinary tract infections or alterations at MAG-3 diuretic renogram scan, in particular an obstructive pattern.
HPBD was performed in all studies under general anaesthesia. In one study (10) a cutting balloon ureterotomy was performed in three patients when HPBD alone was not sufficient for the resolution of the stenosis. In Christman et al. study (14), if the narrowed segment was shorter than 20 mm, HPBD was performed, while if it was 20 to 30 mm in lenght, the authors performed a laser incision followed by HPBD. The laser incision was performed using a holmium:YAG laser at the 12 o’clock position within the ureter. A DJ stent was positioned after the balloon dilation and left in place for 6 to 8 weeks. In one study (21), the authors did not use the DJ stent at the end of the procedure and compared the results with the control group with the stent positioned after dilation.
Casal et al. (15) excluded all patients with ureter >25 mm, while Chiarenza et al. (19) identified patients with poor prognosis by evaluating their anatomical features,which include an ostium placed in a bladder diverticulum or with a very tight diameter, and a narrowed segment longer than 10 mm: these subgroups of patients were in fact excluded from endoscopic treatment and required an open surgical procedure. For short narrowed segments, HPBD proved to be more effective, with the chance of repeating the dilation in the group with intermediate narrow segment (5 mm - 10 mm).
Success was defined in various manners, as resolution of the obstruction, ureterovesical junction (UVJ) patency at stent removal, improvement on ultrasound or renal scan at the follow up visit performed at 3, 6 and 12 months post-operative. A satisfactory follow-up was conducted in patients who underwent surgical correction in almost all studies. The median follow-up ranged between 21 months and 10.3 years.
All the studies reported a success rate ranging from 69 to 100% for the treatment of POM with HPBD. This approach is thought to be a definitive, less invasive, and safe treatment for this disorder that may avoid surgery in up to 77% of cases (22). Some authors also reported the definitive success rate after a second endoscopic dilation (9, 12, 13, 16, 19) when needed.
Angerri et al. (23), in 2007, reported their first experience with a small case series of 6 patients, who had resolution of the urinary obstruction without any complications with a mean follow-up of 31 months. Torino et al. (11) presented a series of 5 patients treated below 1 year of age with resolution of the obstruction and a median follow up of 23.8 months. In 2012, Christman et al. (14) reported their experience with 17 children and a follow-up of 3.2 years. These authors, in addition, a laser incision in cases of narrowed segment longer than 20 mm and placed two DJ stents together in the ureter, reporting good long-term outcomes with resolution of hydroureteronephrosis (HUN) in 71% of cases, while those with moderate improvement on ultrasound had no obstruction on MRI. The authors hypothesized that movement of the two DJs, combined with ureteral peristalsis, allows for a durable dilation of the adynamic segment at the UVJ and prevent scar tissue formation.
García-Aparicio et al. (24) reported their experience with 13 patients with resolution of the obstruction in 84.6% (11 out of 13) in the mid-term. In this series 3 patients required ureteral reimplantation(2 patients had persistence of HUN and 1 patient had a high-grade VUR). Casal et al. (15) presented good outcomes in a small series of 13 patients, with a consistent mean follow-up of 10.3 years [4.7–12.2], supporting the key role of HPBD as a definitive approach for primary obstructive megaureter. They registered a success rate of 100%, without re-interventions or secondary treatment. However, all patients with ureter >2,5 cm were excluded, and this can explain the high success rate. Capozza et al. (10) described the use of a cutting-balloon for dilation of VUJ in 3 patients in which persisted the stenotic ring during the previous HPBD. Using this technique they obtained a complete resolution of the stenosis and good mid-term outcomes. Overall, they reported a success rate of 83% and no complications were registered.
Other endourologic procedures proposed for POM included endoureterotomy with stenting. Kajbafzadeh et al. (25) described this approach in patients with ‘intravesical ureteral obstruction’ and a narrowed segment length less than 15 mm. Their case series of 47 patients included infants as young as 1.5 months, although the mean age at intervention was 3.7 years. The authors reported a 90% success rate with a median follow-up of 39 months, including 71% complete resolution of HUN, with self-limiting haematuria as the only complication. Romero et al. (12) reported in 2014 their experience with 23 patients (29 ureters) with a median age at surgery of 4 months and a mean follow-up of 47 months, treated until 2010 using a high-pressure balloon, followed by placement of a DJ stent. Their results suggested that patients with a favourable evolution at 18 months with resolution of the HUN and adequate renal drainage confirmed by MAG-3 renogram, remained stable and asymptomatic during the subsequent follow-up. Secondary VUR occurred in five patients and three of them were successfully treated endoscopically, while 1 patient required ureteral reimplantation. Overall, the endourological management of the POM, including HPBD of the VUJ and treatment of secondary VUR, reported a success rate of 86%. Bujons et al. (9) registered excellent results in 19 children, with a 90% long-term success rate after the initial dilation and a follow-up of 6.9 years. One patient required a second dilation due to re-stenosis, and another patient needed endoscopic treatment of secondary VUR, both with good outcomes.
Destro et al. (20) reported a success rate of 84% and compared results in patients under 1 year of age and in older children. The statistical analysis (p-value modified by Yates for small numbers) showed no significant difference between these two groups.
The complication rate ranged from 0 to 50% and it was mostly infectious or associated to the stent placement or both (13, 18). Four studies registered no complications (9, 10, 15, 20). The use of a DJ stent has been reported to be associated with 70% morbidity (26): abdominal pain, haematuria, stent migration or encrustation, intracorporeal knotting, lower urinary tract symptoms, infections. Kassite et al. (13) focused their interest on the infectious morbidity of the DJ stenting in patients undergoing HPBD. They registered infectious stent-related complication rate of25%, despite antibiotic prophylaxis. In one study (13), infectious stent-related complications occurred in 50% of cases, despite antibiotic prophylaxis. This incidence was higher than other studies and may potentially be accounted for the longer duration of stenting in that series. No other risk factor for infection was identified. The high complication rate due to ureteral stenting raised the question of theactual need of ureteral stenting following HPBD. Stent placement after balloon dilation has been questioned for a long time (27). In general, the use of a stent is suggested only for a short period in order to drain the upper urinary tract preventing the possible obstruction due to oedema, epithelial hyperplasia, or inflammatory cell reaction and the subsequent renal failure. However, some authors suggested that the ureteral stent is not necessary at all in uncomplicated procedures (28, 29). For this reason, Kassite et al. (18) did not place any stent in the last 4 cases of their series after dilation and no complication occurred at follow-up. Faraj et al. (21) compared in their series the group with DJ stent positioned after the endoscopic procedure and the group without stent. They noted that there was a significantly higher rate of post-operative complications in the group with DJ stenting compared to the group without the stent, including all Clavien-Dindo grades (56% vs 15%, p Z 0.014) and Clavien-Dindo grade III alone (31% vs 0%, p Z 0,0051). The five Clavien-Dindo III complications in the “DJ group” were: one severe sepsis requiring urinary diversion (ureterostomy), two migrations of the DJ associated with pain, and two encrustations of the DJ stent needing early intervention to remove the stents using laser lithotripsy. Grade I Clavien-Dindo complications were painful episodes needing supplementary analgesics treatment. In the “no-DJ group”, there were one episode of acute urinary retention and one stone migration after the procedure. In the DJ group, three patients needed opioid treatment including one patient who had to be readmitted the week after surgery. Clavien-Dindo grade II complications were symptomatic and febrile urinary tract infections with prompt resolution under intravenous antibiotic treatment (2 in the no DJ group and 1 in the DJ group). Overall, success rate (defined by the absence of further ureteral reimplantation) was 79% with a median follow-up of 35.5 months [12–101]. The authors did not register any statistical difference between the success rate of the two groups: 75% with a double J stent in situ(median follow up: 70 months [13–101]) and 81% when no DJ stent was positioned after HPBD (median follow up: 26 months [12–95]) (13).
Another frequent complication was secondary VUR, with an incidence between 5% and 27% (9, 16), but it was endoscopically treated with high success rate (17). According to Garcia-Aparicio et al. (22) postoperative VUR after HPBD might be transient. In addition, they identified two elements related to postoperative VUR: the presence of periureteral diverticula in the preoperative VCUG and bilateral POM (P < 0.05). Most of the authors suggest not to perform systematic VCUG to assess VUR after surgery, and they recommend it only in case of UTIs (10, 12, 23). However, Aparicio et al. performed VCUG in all the patients of their study 6 months after balloon dilation to evaluate VUR. They reported a 27.2% postoperative VUR rate (6 of 22 ureters) (16)., which was higher than other series.However, only one patient with bilateral high-grade VUR needed endoscopic treatment. The other VURs spontaneously resolved during follow-up. Overall, they concluded that postoperative VUR was not clinically significant, but a transient condition after balloon dilation. For that reason, systematic VCUG after ureteral dilation is not necessary. Ortiz et al. (17) found post-operative secondary VUR during long-term follow-up in 17 patients (21.5%), being diagnosed in 12 cases after UTI and in 5 cases after a routine cystogram suggested for contralateral VUR previously diagnosed in the initial workup of the POM. Only 1 out of 11 patients who needed HPBD of the VUJ at time of stent removal, presented post-operative reflux. Endoscopical injection of subureteral Deflux™ (dextramer copolymer in hyaluronic acid) was successful in 13 children (76.4%), and failed in 4 (23.6%) who underwent to open ureteral reimplantation. In the same study long-term re-stenosis occurred in 9 cases (12.2%). A new HPBD was performed with good long-term outcome in 8 patients (88.9%). One patient developed recurrent re-stenosis and finally required ureteral reimplantation.
The management of POM is conservative in the majority of cases, particularly in the first year of life. The indications for active treatment include at least one of the following clinical conditions or instrumental findings: i) initial split renal function <40% with an obstructive excretion pattern at MAG-3 renogram or > 10% loss of differential renal function during follow-up; ii) progressive significant increase of HUN at ultrasound; iii) febrile UTIs not controlled by antibiotic prophylaxis. In these patients an operative treatment is required, even in the first months of life.
The gold-standard procedure for these patients has been, so far, ureteral reimplantation with or without ureteral tapering, with a success rate between 90 and 95%. However, reimplantation of a grossly dilated ureter in a small infantile bladder could be challenging and may lead to potential complications such as VUR, secondary obstruction and bladder dysfunction (4, 30, 31). In some studies morbidity rate ranging from 4 to 25% and reoperation rate of 12% have been registered (30, 32). For such reasons, temporary urinary diversions could be suggested during the first months of life, but they are not exempt of complications. External ureterostomies may present problems such as infections, skin irritations, and stenosis. The placement of a DJ ureteral stent as a temporary solution for the initial treatment of POM has been described by many authors. Castagnetti et al. (26) registered efficient ureteral drainage after DJ stent placement, avoiding further treatments. However, they recurred to open surgery for the 50% of double-J stent placements, and more than half of the patients required ureteral reimplantation.
Unlike open surgery, HPBD avoids traumatizing the bladder and the distal ureteral blood supply is left intact (14). There is also no violation of the bladder or abdomen, and no urinary catheter is required postoperatively. Moreover, reimplantation can still be performed in case of failure of the endoscopic treatment. Since the first descriptions, several publications with limited numbers of patients and variable follow-up periods suggested that HPBD is a feasible, safe, and minimallyinvasive procedure for the initial management of POM with surgical criteria even for very young patients.
Several aspects deserve further discussion. Christman et al. (14) is innovative for two reasons: the adjunct of laser incision in cases stenotic tracts of 20 to 30 mm long and the use of double stenting. However, in the absence of comparative data the role of each of these interventions on the final success of treatment remains unclear. Kassite et al. (13) reported that the morbidity of this approach is mostly infectious and exclusively related to the use of a DJ stent. Faraj et al. (21) compared the “DJ group” (75%, follow-up of 70 months) and the “no DJ group” (81%, follow-up of 26 months), supporting the hypothesis that DJ stenting is not necessary after HPBD for POM, with no influence on the success rate of the procedure. No statistical difference was registered.
The presence of a pseudo-ureterocele at the orifice or long ureteral stenosis may interfere with the ureteral stenting and seems to be associated with worse outcomes (20). Casal Beloy et al. (15) considered a ureter diameter >25 mm one of the main contraindications for HPBD. In these cases, and according with the current literature, an open approach with ureteral tapering should be performed to improve peristalsis and achieve better outcomes. Some authors recommended an open reimplantation in cases of ureteral diameter >15 mm identified during endoscopic procedure (33).
A great concern is the associated to the ionizing radiation used during this technique, since the risk of radio-induced secondary effects is particularly relevant in the paediatric age. Despite the radiation dose administered during HPBD of POM is very low, some authors (17) did not use fluoroscopic guidance except in selected cases.
Success of the procedure was defined during follow up in case of improvement or stabilization of renal function, elimination of the UTIs episodes, and reduction of the degree of HUN and was mainly based on US findings at 3, 6, and 12 months post-operative. VCUG was performed only in cases of UTIs.
The present study is not without limitations. The nature of the studies (mainly retrospective case series, without comparative studies or RCTs) constitutes an important drawback. Moreover, the lack of homogeneity in the indication for HPBD between different studies is certainly one of the main limitations of the present review. This hinders any generalizable and definitive conclusion about the efficacy of the procedure. Since it is known that most POMs resolve spontaneously, it is possible that missing inclusion criteria may have influenced the results in some studies. The large differences in median age between studies (and the wide age ranges within each study) are another source of bias, potentially interfering with the comparison of homogeneous populations. Finally, the definition of success and the follow-up modalities showed considerable discrepancies in the included series, thus limiting the possibility of meaningful comparison between different experiences.
The results of this systematic review show that HPBD may be a safe and effective long-term option for the treatment of POM in infants and can be a definitive treatment in a considerable subset of patients. Nevertheless, the overall level of evidence for HPBD is still low and further comparative studies or randomized clinical trials with standardized inclusion criteria and sound follow-up would be useful to confirm these findings.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Conceptualization: AM, MB, GA, WR, and FM Literature search and data collection: GA, AM, and MB. Manuscript writing: GA, AM, MS; writing—review and editing: all authors, supervision: AM and FM. All authors contributed to the article and approved the submitted version.
The present publications have been supported by the research funding of the Department of Surgical, Oncological and GE sciences, Padova University.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Hellstrom M, Hjalmas K, Jacobsson B, Jodal U, Odén A. Normal ureteral diameter in infancy and childhood. Acta Radiol Diagn (Stockh) (1985) 26:433–9. doi: 10.1177/028418518502600412
2. King LR. Megaloureter: Definition, diagnosis and management. J Urol (1980) 123:222–3. doi: 10.1016/S0022-5347(17)55867-X
3. Baskin LS, Zderic SA, Snyder HM, Duckett JW. Primary dilated megaureter: long-term followup. J Urol (1994) 152:618–21. doi: 10.1016/S0022-5347(17)32665-4
4. Farrugia MK, Hitchcock R, Radford A, Burki T, Robb A, Murphy F. British Association of paediatric urologists consensus statement on the management of the primary obstructive megaureter. J Pediatr Urol (2014) 10:26–33. doi: 10.1016/J.JPUROL.2013.09.018
5. Hendren WH. Operative repair of megaureter in children. J Urol (1969) 101:491–507. doi: 10.1016/S0022-5347(17)62370-X
6. Upadhyay J, Shekarriz B, Fleming P, González R, Barthold JS. Ureteral reimplantation in infancy: Evaluation of long-term voiding function. J Urol (1999) 162:1209–12. doi: 10.1016/S0022-5347(01)68135-7
7. Angulo JM, Arteaga R, Rodríguez Alarcón J, Calvo MJ. Role of retrograde endoscopic dilatation with balloon and derivation using double pig-tail catheter as an initial treatment for vesico-ureteral junction stenosis in children. Cir Pediatr (1998) 11(1):15–8.
8. Torino G, Collura G, Mele E, Garganese MC, Capozza N. Severe primary obstructive megaureter in the first year of life: Preliminary experience with endoscopic balloon dilation. J Endourol (2012) 26:325–9. doi: 10.1089/END.2011.0399
9. Bujons A, Saldaña L, Caffaratti J, Garat JM, Angerri O, Villavicencio H. Can endoscopic balloon dilation for primary obstructive megaureter be effective in a long-term follow-up? J Pediatr Urol (2015) 11:37.e1–6. doi: 10.1016/j.jpurol.2014.09.005
10. Capozza N, Torino G, Nappo S, Collura G, Mele E. Primary obstructive megaureter in infants: Our experience with endoscopic balloon dilation and cutting balloon ureterotomy. J Endourol (2015) 29:1–5. doi: 10.1089/end.2013.0665
11. Torino G, Roberti A, Brandigi E, Turrà F, Fonzone A, Di Iorio G. High-pressure balloon dilatation for the treatment of primary obstructive megaureter: Is it the first line of treatment in children and infants? Swiss Med Wkly (2021) 151:8–17. doi: 10.4414/SMW.2021.20513
12. Romero RM, Angulo JM, Parente A, Rivas S, Tardáguila AR. Primary obstructive megaureter: The role of high pressure balloon dilation. J Endourol (2014) 28:517–23. doi: 10.1089/END.2013.0210
13. Kassite I, Braïk K, Morel B, Villemagne T, Szwarc C, Maakaroun Z, et al. High pressure balloon dilatation of the ureterovesical junction in primary obstructive megaureter: Infectious morbidity. Prog Urol (2017) 27:507–12. doi: 10.1016/J.PUROL.2017.07.005
14. Christman MS, Kasturi S, Lambert SM, Kovell RC, Casale P. Endoscopic management and the role of double stenting for primary obstructive megaureters. J Urol (2012) 187:1018–23. doi: 10.1016/j.juro.2011.10.168
15. Casal Beloy I, Somoza Argibay I, García González M, García Novoa MA, Míguez Fortes LM, Dargallo Carbonell T. Endoscopic balloon dilatation in primary obstructive megaureter: Long-term results. J Pediatr Urol (2018) 14:167.e1–5. doi: 10.1016/j.jpurol.2017.10.016
16. García-Aparicio L, Blázquez-Gómez E, de Haro I, Garcia-Smith N, Bejarano M, Martin O, et al. Postoperative vesicoureteral reflux after high-pressure balloon dilation of the ureterovesical junction in primary obstructive megaureter. Incidence, management and predisposing factors. World J Urol (2015) 33:2103–6. doi: 10.1007/s00345-015-1565-9
17. Ortiz R, Parente A, Perez-Egido L, Burgos L, Angulo JM. Long-term outcomes in primary obstructive megaureter treated by endoscopic balloon dilation. experience after 100 cases. Front Pediatr (2018) 6:275. doi: 10.3389/FPED.2018.00275
18. Kassite I, Petel MR, Chaussy Y, Eyssartier E, Alzahrani K, Sczwarc C, et al. High pressure balloon dilatation of primary obstructive megaureter in children: A multicenter study. Front Pediatr (2018) 6:329. doi: 10.3389/fped.2018.00329
19. Chiarenza SF, Bleve C, Zolpi E, Battaglino F, Fasoli L, Bucci V. Endoscopic balloon dilatation of primary obstructive megaureter: Method standardization and predictive prognostic factors. Pediatr Med Chir (2019) 41:1–7. doi: 10.4081/PMC.2019.219
20. Destro F, Selvaggio G, Marinoni F, Pansini A, Riccipetitoni G. High-pressure balloon dilatation in children: Our results in 30 patients with pom and the implications of the cystoscopic evaluation. Pediatr Med e Chir (2020) 42:1–5. doi: 10.4081/pmc.2020.214
21. Faraj S, Loubersac T, Graveleau A, Alliot H, Camby C, Leclair MD. Postoperative JJ stent is not necessary after balloon high-pressure endoscopic dilatation of primary obstructive megaureter. J Pediatr Urol (2022) 18:369.e1–7. doi: 10.1016/J.JPUROL.2022.03.028
22. García-Aparicio L, Blázquez-Gómez E, Martin O, Palazón P, Manzanares A, García-Smith N, et al. Use of high-pressure balloon dilatation of the ureterovesical junction instead of ureteral reimplantation to treat primary obstructive megaureter: is it justified? J Pediatr Urol (2013) 9:1229–33. doi: 10.1016/J.JPUROL.2013.05.019
23. Angerri O, Caffaratti J, Garat JM, Villavicencio H. Primary obstructive megaureter: Initial experience with endoscopic dilatation. J Endourol (2007) 21:999–1004. doi: 10.1089/END.2006.0122
24. Garca-Aparicio L, Rodo J, Krauel L, Palazon P, Martin O, Ribó JM. High pressure balloon dilation of the ureterovesical junction–first line approach to treat primary obstructive megaureter? J Urol (2012) 187:1834–8. doi: 10.1016/J.JURO.2011.12.098
25. Kajbafzadeh AM, Payabvash S, Salmasi AH, Arshadi H, Hashemi SM, Arabian S, et al. Endoureterotomy for treatment of primary obstructive megaureter in children. J Endourol (2007) 21:743–9. doi: 10.1089/END.2006.0330
26. Castagnetti M, Cimador M, Sergio M, De Grazia E. Double-J stent insertion across vesicoureteral junction–is it a valuable initial approach in neonates and infants with severe primary nonrefluxing megaureter? Urology (2006) 68:870–5. doi: 10.1016/J.UROLOGY.2006.05.052
27. Başeskioğlu B, Sofikerim M, Demirtaş A, Yenilmez A, Kaya C, Can C. Is ureteral stenting really necessary after ureteroscopic lithotripsy with balloon dilatation of ureteral orifice? A multi-institutional randomized controlled study. World J Urol (2011) 29:731–6. doi: 10.1007/S00345-011-0697-9
28. Borboroglu PG, Amling CL, Schenkman NS, Monga M, Ward JF, Piper NY, et al. Ureteral stenting after ureteroscopy for distal ureteral calculi: A multi-institutional prospective randomized controlled study assessing pain, outcomes and complications. J Urol (2001) 166:1651–7. doi: 10.1016/S0022-5347(05)65646-7
29. Byrne RR, Auge BK, Kourambas J, Munver R, Delvecchio F, Preminger GM. Routine ureteral stenting is not necessary after ureteroscopy and ureteropyeloscopy: A randomized trial. J Endourol (2002) 16:9–13. doi: 10.1089/089277902753483646
30. Peters CA, Mandell J, Lebowitz RL, Colodny AH, Bauer SB, Hendren WH, et al. Congenital obstructed megaureters in early infancy: Diagnosis and treatment. J Urol (1989) 142:641–5. doi: 10.1016/S0022-5347(17)38842-0
31. Perdzyński W, Kaliciński ZH. Long-term results after megaureter folding in children. J Pediatr Surg (1996) 31:1211–7. doi: 10.1016/S0022-3468(96)90234-1
32. DeFoor W, Minevich E, Reddy P, Polsky E, McGregor A, Wacksman J, et al. Results of tapered ureteral reimplantation for primary megaureter: Extravesical versus intravesical approach. J Urol (2004) 172:1640–3. doi: 10.1097/01.JU.0000138529.43179.DD
Keywords: obstructive megaureter, POM, balloon dilatation, endoscopic treatment, pediatric urology
Citation: Aiello G, Morlacco A, Bianco M, Soligo M, Meneghesso D, Vidal E, Rigamonti W and Dal Moro F (2022) Efficacy and safety of high-pressure balloon dilatation for primary obstructive megaureter in children: A systematic review. Front. Urol. 2:1042689. doi: 10.3389/fruro.2022.1042689
Received: 12 September 2022; Accepted: 20 October 2022;
Published: 08 November 2022.
Edited by:
Sherry Ross, University of North Carolina at Chapel Hill, United StatesReviewed by:
Alberto Parente, Consultant, Madrid, SpainCopyright © 2022 Aiello, Morlacco, Bianco, Soligo, Meneghesso, Vidal, Rigamonti and Dal Moro. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alessandro Morlacco, YWxlc3NhbmRyby5tb3JsYWNjb0B1bmlwZC5pdA==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.