 Yévèdo Borel Tossou1*Fifamin Noël Christelle Gbaguidi1Sonagnon Inès Elvire Agbo1Sètondji Diane Edwige Zanvo1Karine Lucrèce Marie Codjo-Seignon1Paule Héléna Biaka2Fernand Aimé Guedou1Kouakou Jerôme Kouadio2Sèdjro Gimatal Esaï Anagonou1Franck Zinsou Mignanwande1Parfait Djossou1Brunelle Vanessa Yemadje1Flora Sylvie Houndjrebo1Jeanne d’Arc Natacha Lessanh Arrawo1Yvette Faihoun1Harvey Johnson1Ghislain Emmanuel Sopoh3Jean Gabin Houezo4Mamadou Kaloga5Agui Sylvestre Dizoe6Mark Nichter7Cristina Juan Jimenez8Anna Gine-March8Roch Christian Johnson1,9
Yévèdo Borel Tossou1*Fifamin Noël Christelle Gbaguidi1Sonagnon Inès Elvire Agbo1Sètondji Diane Edwige Zanvo1Karine Lucrèce Marie Codjo-Seignon1Paule Héléna Biaka2Fernand Aimé Guedou1Kouakou Jerôme Kouadio2Sèdjro Gimatal Esaï Anagonou1Franck Zinsou Mignanwande1Parfait Djossou1Brunelle Vanessa Yemadje1Flora Sylvie Houndjrebo1Jeanne d’Arc Natacha Lessanh Arrawo1Yvette Faihoun1Harvey Johnson1Ghislain Emmanuel Sopoh3Jean Gabin Houezo4Mamadou Kaloga5Agui Sylvestre Dizoe6Mark Nichter7Cristina Juan Jimenez8Anna Gine-March8Roch Christian Johnson1,9- 1Département Environnement et Santé, Centre Interfacultaire de Formation et de Recherhe en Environnement pour le Développement Durable, Université d’Abomey-Calavi, Abomey-Calavi, Benin
- 2Département d'Anthropologie, Institut des Sciences Anthropologiques de Développement, Université Félix Houphouet Boigny de Cocody, Abidjan, Côte d’Ivoire
- 3Département d'Anthropologie, Institut Régional de Santé Publique de Ouidah, Université d’Abomey-Calavi, Abomey-Calavi, Benin
- 4Programme National de Lutte contre la Lèpre et l’Ulcère de Buruli, Cotonou, Benin
- 5Programme National de Lutte contre l’Ulcère de Buruli, Abidjan, Côte d’Ivoire
- 6Programme National d’Elimination de la Lèpre, Abidjan, Côte d’Ivoire
- 7School of Anthropology University of Arizona, Tucson, AZ, United States
- 8Anesvad Foundation, Bilbao, Spain
- 9Fondation Raoul Follereau, Paris, France
Introduction: Healthcare systems and social services in developing countries are often ill-equipped to provide comprehensive care for people with disabilities (PWDs). As a result, the quality of life for PWD frequently deteriorates. Comprehensive health care includes five key components: access to diagnosis, treatment, rehabilitation, psychosocial support, and prevention with follow-up. This study aimed to document those segments of the disabled population and factors most associated with inadequate care in regions of Benin and Côte d’Ivoire endemic to neglected tropical diseases (NTDs).
Methods: An exploratory cross-sectional study of PWD was conducted in 2022 in Benin and Côte d’Ivoire, using a combination of quantitative and qualitative approaches. The sample included 841 PWD, 29 caregivers, and 51 family members. Disability management was evaluated using a scoring system ranging from 0 to 5, classifying management into three categories: good management (scores of 4-5), inadequate management (scores of 1-3), and no management (score of 0). Quantitative data were analyzed using SPSS version 25.5, with a p-value of <5% considered statistically significant. Open-ended interviews were carried out with a subsample of PWD, family members, and caretakers to provide further insights into what forms of care were and were not being provided.
Results: Among PWD, 98 (11.6%) experienced disability associated with skin-related neglected tropical diseases skin-NTDs [apply throughout]. Of the total, 158 (18.8%) received good management, 532 (63.3%) inadequate management, and 151 (18.0%) no management at all. The median age of the sample was 38 years (22; 52), and the male-to-female sex ratio was 1.45. The key factors associated with the quality of disability management (expressed as odds ratios [OR] with 95% confidence intervals [CI] and p-values) were: age 30 to 44 years (OR 0.29 [0.16−0.54], p<0.000), occupation—saleswoman/housewife (OR 0.32 [0.12−0.81], p=0.017), farmer (OR 0.30 [0.16−0.59], p=0.000), other occupations (OR 0.42 [0.18−0.96]), monthly income over 76 euros (OR 0.41 [0.23−0.74], p=0.003), and cause of disability, specifically skin-NTDs (OR 2.15 [1.13−4.09], p=0.000). The interviews highlighted the need for medical interventions, social and economic support.
Conclusion: Comprehensive and sustainable interventions are needed to improve the well being of people affected by disabilities. These need to be built into public health programs for skin-NTDs.
1 Introduction
Disability is “any limitation of activity or restriction of participation in society experienced by a person in his or her environment due to a substantial, lasting or permanent impairment of one or more physical, sensory, mental, cognitive or psychic functions, multiple disabilities or a disabling health disorder” (1). According to the World Health Organization (WHO), disability represents a global health, human rights and development challenge (2). Access to health, rehabilitation, and related services is often hampered for PWD (PWDs), particularly children (3). Inadequate management of PWDs leads to difficulties in accessing education, employment, and remuneration, restricting social participation and contributing to poverty (4). In 2022, approximately 240 million children worldwide were disabled, and they were more likely than nondisabled children to have never attended school (5).
The causes of disabilities are diverse. In Africa, and particularly in Benin and Côte d’Ivoire, Skin-NTD are common causes of permanent disability when not diagnosed and treated early (6). Skin-NTDs are a diverse group of conditions caused by a variety of pathogens (including viruses, bacteria, parasites, fungi and toxins) and associated with skin manifestations such as ulcers, plaques, nodules, wounds, etc. For example, in 2022, Africa reported 20,000 new cases of leprosy, with 6–7% of cases involving irreversible disabilities affecting the eyes, hands, and feet (7). Between 2006 and 2018, 2,785 new cases of Skin-NTD were reported in Benin, with the proportion of new cases involving irreversible disabilities treated in Beninese hospitals ranging between 21.33% and 32% during this period.
A study conducted in Pobè, Benin, between 2005 and 2011 revealed that 66% of Buruli ulcer (BU) cases presented with ulcerative lesions, 36% of which were large (≥15 cm). The severity of the condition and delays in treatment likely resulted in permanent functional sequelae for many patients in treatment (7). In 2022, Côte d’Ivoire recorded 500 new cases of leprosy, 25% of which involved disabilities (8). That same year, 251 new cases of BU were reported in Côte d’Ivoire, with 65% of patients presenting severe disabilities (9). Lymphatic filariasis (LF), another disabling Skin-NTD, was endemic in 77 districts of Benin in 2023, while 93 districts in Côte d’Ivoire were suspected to be endemic that same year (10).
Early, comprehensive, and high-quality management is crucial for managing disabilities and reducing associated social stigma (11). Unfortunately, despite efforts by the governments of both countries, care management remains insufficient in both quality and quantity. This study aimed to identify segments of the disabled population and factors associated with inadequate disability management in communities endemic to neglected tropical diseases with cutaneous manifestations (Skin-NTD) in Benin and Côte d’Ivoire. Special attention was given to this segment of the PWD population.
2 Study framework and methods
2.1 Study setting
Data were collected from the localities of Ouidah, Lalo, Allada and Pobè in Benin (Figure 1_Benin), and from Divo, Yamoussoukro and Tiassalé in Cote d’Ivoire (Figure 2_Cote d’Ivoire). These localities were selected because they are endemic to Skin-NTD, and most of them have specialized centers dedicated to treatment. The main language spoken in these areas is Fon, and the religions present are Christian, Muslim and traditional. Wealth varies from place to place. Ouidah and Allada are the most developed towns. In Côte d’Ivoire, the main languages spoken in these areas are Baoulé, Bété and Dida, and as in Benin, different religions coexist and wealth varies from town to town. Of the three, Yamoussokro is the most developed.
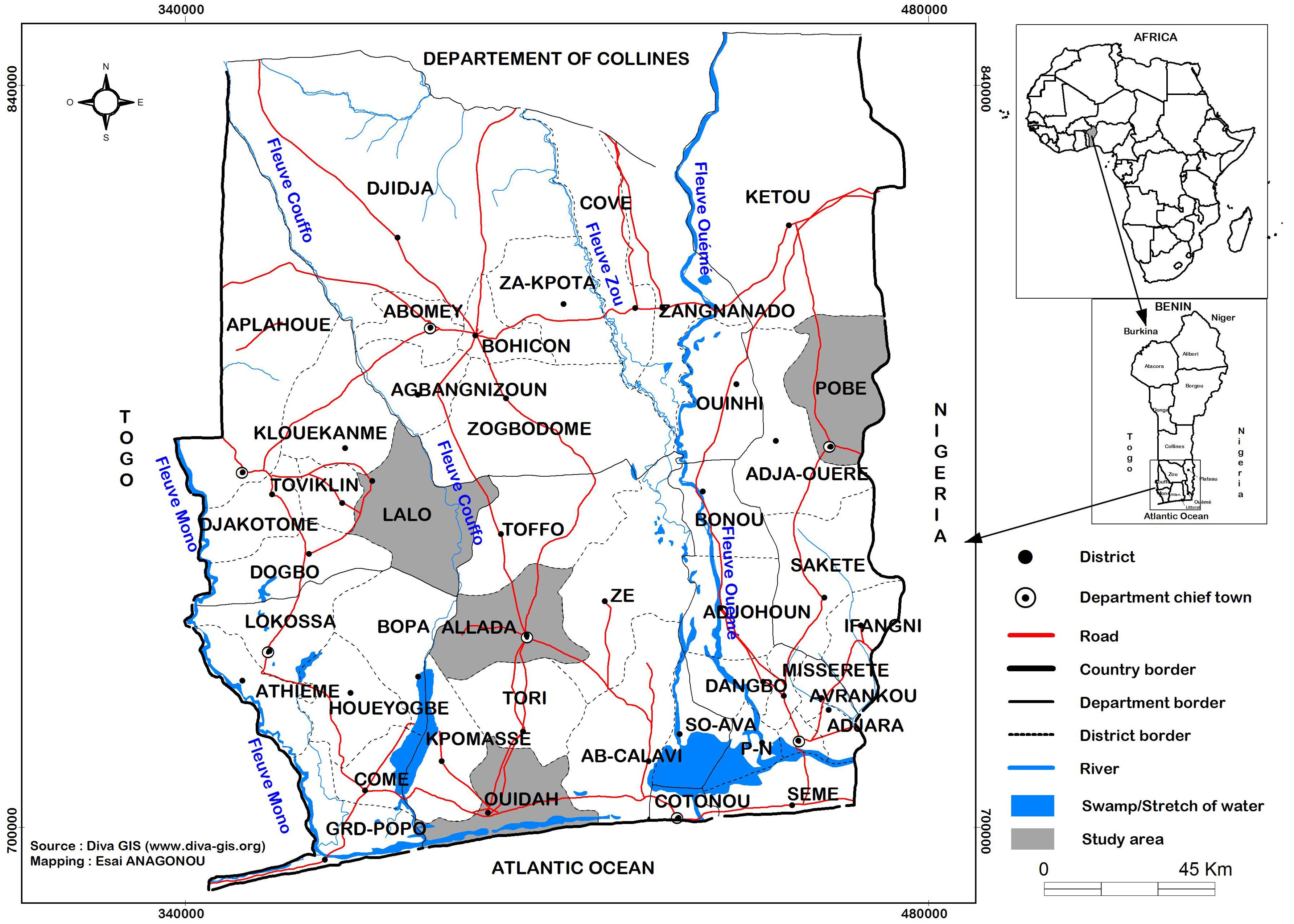
Figure 1. Map showing study sites in Benin.
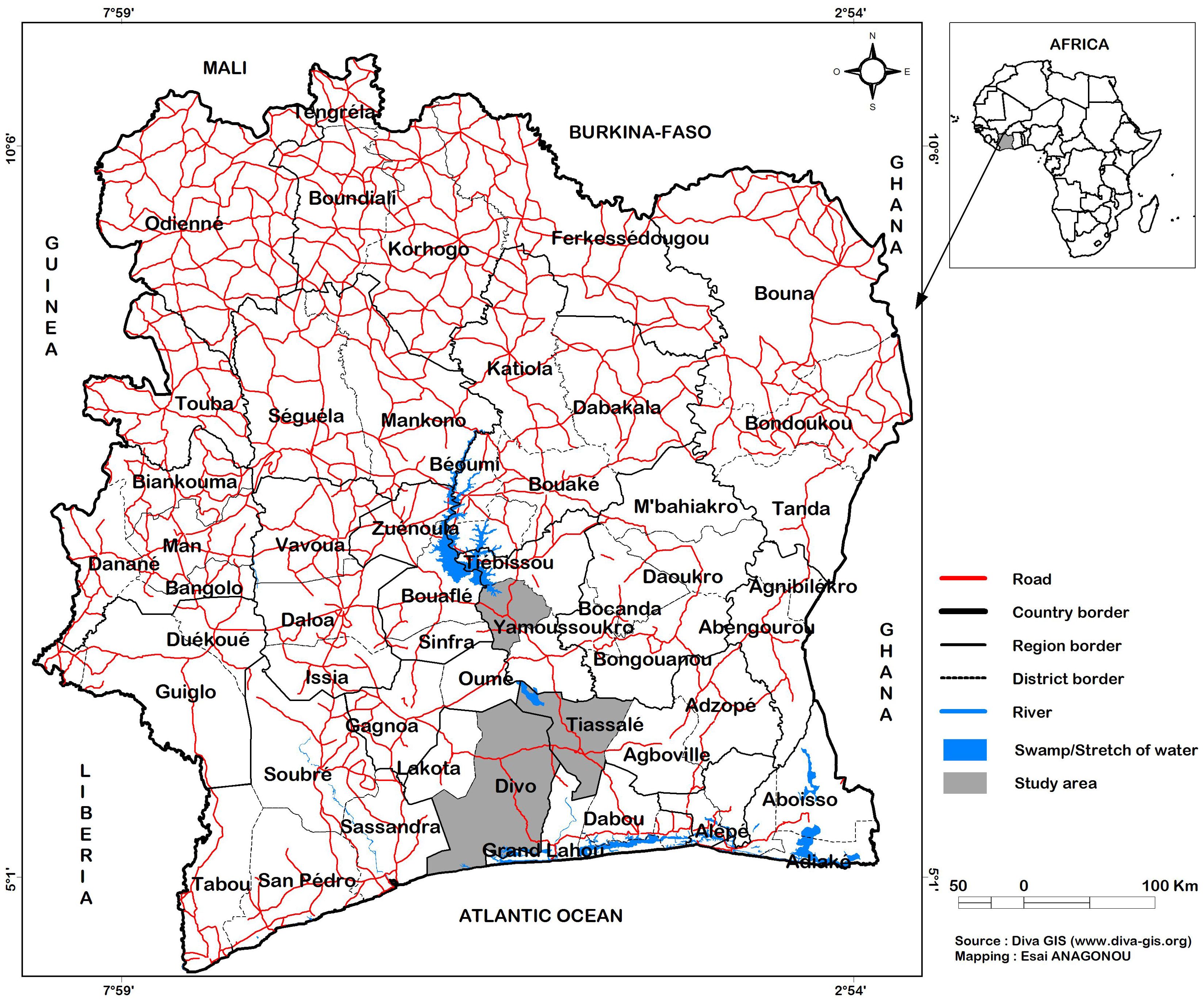
Figure 2. Map showing study sites in Côte d’Ivoire.
2.2 Study design
This was a descriptive cross-sectional study with an analytical focus, using a mixed-method approach, which took place from September 2022 to October 2023. in Benin and Côte d’Ivoire.
A preparatory phase preceded data collection in Benin and Côte d’Ivoire, during which data collection tools were developed and validated, and interviewers were recruited and trained.
2.3 Target populations and selection criteria
2.3.1 Target populations
This study targeted communities in which PWD due to Skin-NTD resided. All PWD in these communities were surveyed regardless of the cause of their disability. A subsample of family members and caretakers were also interviewed.
2.3.2 Selection of participants
2.3.2.1 PWD
2.3.2.1.1 Sample size justification
The sample size of 841 people with disabilities was determined based on the Schwartz formula to ensure sufficient statistical power to detect meaningful differences in disability management across the study sites.
In the study literature, we have few recent studies on disability related to neglected tropical diseases. We have therefore used a prevalence estimate of 0.5. The application of Schwartz’s formula in this study is as follows:
n = sample size; i = 5% (desired precision); p= 50%; q = 1-p=50; Zα = 1.96 (value of reduced deviation at risk α equal to 5%); Hence n = 384.
The minimum size obtained will be 384. This number will be increased by 5%, giving 403 people with disabilities to include in the study in each target country. In both countries, the size will be 806 people with disabilities. In both countries, the size will be 806 people with disabilities.
2.3.2.1.2 Selection of PWD
The patient registers of specialized centers dedicated to Skin-NTD treatment were reviewed. All individuals with disabilities due to Skin-NTD who had been treated in these centers over the past five years were listed, and their localities of origin were carefully documented. The research team then traveled to the recorded villages to locate and interview these individuals and all other individuals with disabilities residing in and around the target localities. A total of 841 PWD were included in the study, 418 from Benin and 421 from Côte d’Ivoire.
Based on the list of people with disabilities received from the health centers, the interviewers went out to the corresponding localities to look for them. Once the information had been collected from these people, a snowball method was used to find the disabled people present in these areas but not present on the starting site.
2.3.2.2 Community members and caregivers
Thirty-five family members in Benin and 16 family members in Côte d’Ivoire were also interviewed. Additionally, 18 healthcare providers in Benin and 11 in Côte d’Ivoire were interviewed including social workers, nurses, doctors, and physiotherapists.
As for family members, those available and willing to take part in the survey were included. As for health professionals, those available and present at the time of the survey were interviewed.
2.4 Variables
Management of PWD is a composite variable. This composite variable is based on the patient’s access to five different services, whose absence is rated 0 and access is rated 1. These five services are access to diagnosis, treatment, rehabilitation, psychosocial support, and prevention and follow-up. When all these five services are available and the patient has access to them, the sum of the total score is 5 (Table 1).

Table 1. Levels of disability management.
The following are the specific services queried:
● Diagnosis: whether or not for the PWD health has been diagnosed by a professional.
● Treatment: access or not to treatment (in case of disease) for PWD.
● Rehabilitation: whether or not for the PWD is followed by a healthcare professional whose aim is to restore the disabled person to a more normal lifestyle.
● Psychosocial support: whether or not the individual is followed up by a psychologist.
● Prevention and follow-up: whether or not the individual is followed up by a healthcare professional (such as a physiotherapist, to prevent possible complications).
The other variables assessed in the study were:
● Sociodemographic and socioeconomic factors: age, sex, level of education, marital status, occupation, monthly income, and income-generating activity (IGA).
● Clinical factors: type and cause of disability.
● Health system-related factors: availability of health services and organization of the health system.
2.5 Data collection tools
Data were collected through structured questionnaires and interview guides administered to participants with disabilities, their family members/caregivers, and healthcare providers. The questionnaires and interview guides included questions on socio-demographic characteristics, disability type, access to healthcare services (diagnosis, treatment, rehabilitation, psychosocial support, prevention/follow-up), and perceived barriers to accessing these services.
A detailed observation grid was developed to assess interactions between people with disabilities and their community members, focusing on focus on their daily lifestyle and how they interact with their environment to accomplish daily tasks.
A grid for observing interactions between PWD and their community was also employed to assess these people in their social context (Example: washing, shampooing, eating meals, moving around outdoors). To capture the experiences and interrelations of PWD with their families and communities, the interviewers spent 24− to 48 hours with the individuals selected for this in-depth study (Observation grid and Interview guide details are presented in Supplementary Material).
2.6 Data processing and analysis
Quantitative data from the 841 PWD were collected using the KoboCollect digital tool, exported to Excel, and then checked for completeness and accuracy. Data analysis was performed using the Statistical Package for Social Science (SPSS version 25). Quantitative variables are expressed as the means with standard deviations, whereas qualitative variables were summarized as frequencies. Means were compared with the Student’s t-test, and frequencies were compared with Pearson’s chi2 test or Fisher’s exact test, as appropriate. Variables with a p-value of less than 20% in the bivariate analysis were retained for multivariable analysis to account for potential confounders and to ensure a comprehensive exploration of factors associated with inadequate disability management. The multivariable analysis was conducted using a stepwise iterative logistic regression model (Wald top-down). This multivariable analysis was performed for all PWDs and then stratified according to gender. For all comparisons, the difference was considered significant for p values less than 5%. At the end of the variable selection procedure in the final model, the adequacy of the model was verified using the Hosmer and Lemeshow test. Finally, the results are presented in the form of text and tables.
For the qualitative data, the interview recordings were fully transcribed in French and coded. This allowed for a comprehensive, interpretative description of the interviewees’ discourse, using a method that ensured the information was preserved “in legible terms” (12). The data input process facilitated categorization, cross-referencing, and thematic synthesis. On the basis of the triangulation of the different points of view emerging from the interviews, the data analysis was structured around the main lines retained after analysis of the verbatim content.
2.7 Ethical aspects
The study was approved by the research ethics committee of the University of Parakou (CLERB-UP) in Benin under authorization N°0492/CLERB-UP/P/SP/R/SA of 19/11/2021 and by the National Life and Health Sciences Ethics Committee (CNESVS) of Côte d’Ivoire under authorization N/Réf: 076-22/MSHPCMU/CNESVS-kp of 28/07/2022. Written informed consent was obtained from all participants, with an emphasis on the voluntary nature of participation. It was made clear that there would be no consequences for those who chose not to participate.
3 Results
3.1 Sociodemographic and socioeconomic characteristics of PWD
The distribution of disabled people according to the different variables is summarized in Table 2.
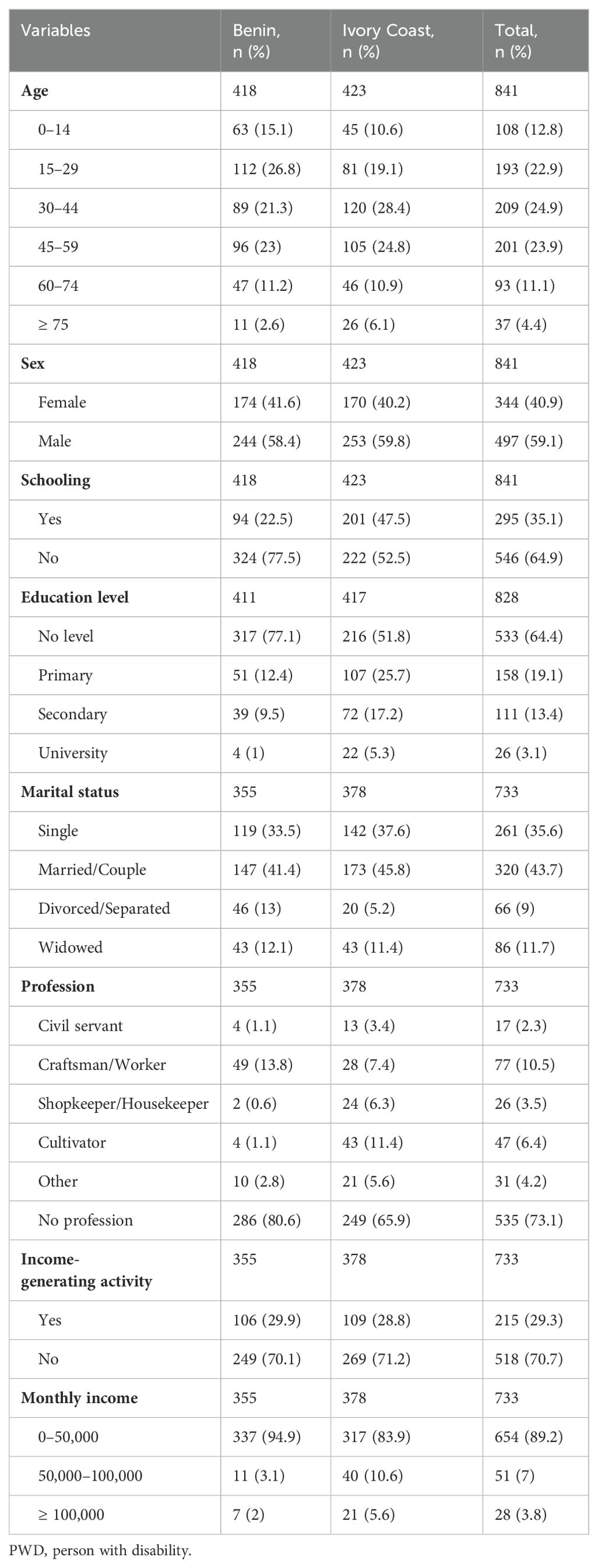
Table 2. Distribution of PWD linked to Skin-NTD according to sociodemographic and economic variables in Benin and Côte d’Ivoire (n = 841).
• Median age: The median age of study participants (Q1; Q3) was 38 (22; 52) years, ranging from 1− to 115 years. In Benin, the ages ranged from 1.5− to 90 years, with a median age (Q1; Q3) of 35 (20; 52). In Côte d’Ivoire, the ages ranged from 1− to 115, with a median age (Q1; Q3) of 40 (26; 54) years.
• Among PWD, 497 (59.1%) were men and 344 (40.9%) were women (sex ratio=1.45). In Benin, 244 (58.4%) men and 174 (41.6%) women (sex ratio=1.40) were included, while in Côte d’Ivoire, 253 (59.8%) men and 170 (40.2%) women (sex ratio=1.48) were included.
• Education: We have only taken into account individuals aged 5 years and over (school starting age). Of the 828 subjects meeting this criterion, 295 (35.6%) had attended school: 158 (18.0%) at the primary level, 111 (03.4%) at the secondary level and 26 (03.1%) at the tertiary level. The remaining 533 or 64.4% had not attended school (311 (62.2%) men and 104 (61.2%) women). In Benin, 324 (77.5%) PWD had not attended school. Of these, 193 (79.1%) were men and 131 (75.3%) were women. In Côte d’Ivoire, 222 (52.5%) had not attended school, including 118 (46.6%) men and 104 (61.2%) women.
• Marital status: Marital status was assessed among 733 eligible subjects (aged 15 years and older). In this group, married individuals accounted for 43.7%, followed by single individuals at 35.6%. In Benin, 147 (41.4%) participants were married, comprising 89 (44.1%) men and 58 (37.9%) women. In Côte d’Ivoire, 173 (45.8%) participants were married, including 125 (54.3%) men and 48 (32.4%) women.
• Occupation: With respect to occupation, 535 (73.1%) of the sample reported having no occupation, and 198 (27.0%) an occupation. Among those with an occupation, 77 (38.9%) were craftsmen/workers, 47 (23.7%) were farmers/peasants, and 17 (08.6%) were civil servants. In Benin, 286 (80.6%) had no profession including 149 (73.8%) men and 137 (89.5%) women). In Côte d’Ivoire, 249 (65.9%) had no profession consisting of 123 (53.5%) men and 126 (85.1%) women).
• Income-generating activities: Among the PWD, 215 (29.3%) had income-generating activity (IGA). In Benin, 106 (29.9%) had an IGA (41 (20.3%) men and 65 (42.5%) women). In Côte d’Ivoire, 109 (28.8%) had an IGA (62 (27.0%) men and 47 (31.8%) women).
• Monthly income: Monthly income varied between €0 and €762. Among the respondents, 654 (89.2%) reported a monthly income of less than €76. In Benin, 337 respondents (94.9%) had an income below €76, which is the minimum wage. Of these, 189 (93.6%) were men and 148 (96.7%) were women. In Côte d’Ivoire, the proportion of individuals earning less than €76 was 317 (83.9%), consisting of 173 men (75.2%) and 144 women (97.3%), with a minimum wage of €114.
3.2 Disability management and clinical features
● Among the 841 individuals with disabilities included in this study, 151 (18%) reported having no management services at all, with variations between the two countries: 23.2% in Benin and 12.8% in Côte d’Ivoire. In Benin, 97 individuals (23.2%) received no management-related services from healthcare providers, while 237 (56.7%) had insufficient management, and 84 (20.1%) received good management. In Côte d’Ivoire, 54 individuals (12.8%) reported no management services, 295 (69.7%) had insufficient management, and 74 (17.5%) received good management.
● In terms of the type of disability, 772 (91.8%) experienced a single disability, the remaining 69 (08.2%) had multiple disabilities. Among those with a single disability, 554 patients (65.8%) had a motor disability. Isolated sensory disabilities (visual, auditory, olfactory, and tactile) were reported by 173 individuals (20.6%), and isolated cerebral palsy (CP) was found in 45 individuals (5.4%) of the surveyed population. In Benin, 393 individuals with disabilities (94.0%) had a single disability, comprising 230 men (94.3%) and 163 women (93.7%). Conversely, 25 individuals (6.0%) had multiple disabilities, including 14 men (5.7%) and 11 women (6.3%). In Côte d’Ivoire, 379 individuals (90.0%) had a single disability, with 229 men (90.5%) and 150 women (88.2%). A total of 44 individuals (10.4%) were multi-disabled, consisting of 24 men (9.5%) and 20 women (11.8%).
● Of the entire population of PWD identified in study locales, 98 individuals (11.7%) were disabled as a result of NTDs. In Benin, this included 49 men (11.7%) and 23 women (13.2%). In Côte d’Ivoire, the proportion was similar, with 49 individuals (11.6%), comprising 30 men (11.9%) and 19 women (11.2%) (Table 3).
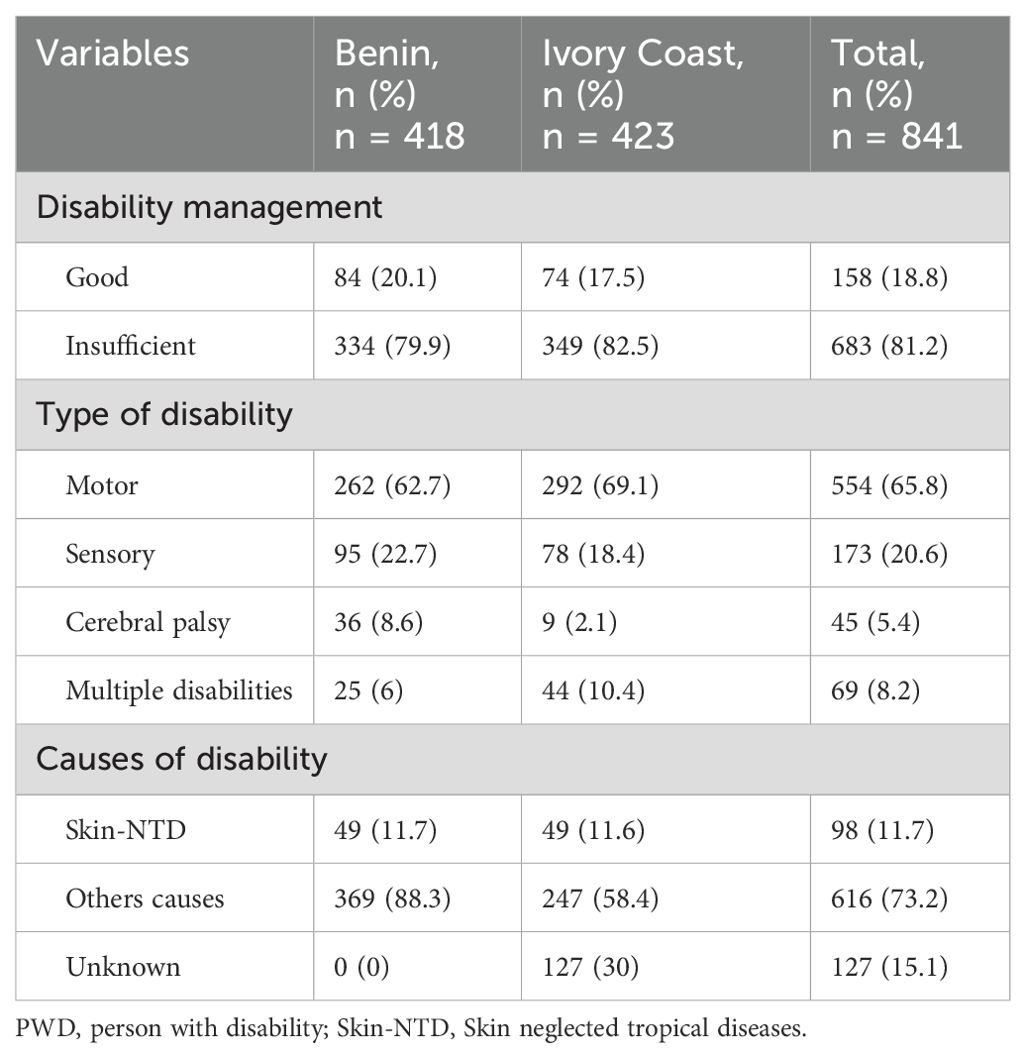
Table 3. Distribution of PWD linked to Skin-NTD according to clinical variables in Benin and Côte d’Ivoire (n = 841).
3.3 Family members and caregivers
● Among the 51 family members interviewed, 38 (74.5%) were aged between 30 and 59 years. This population comprised 25 men (49.0%) and 26 women (51.0%), with a sex ratio of 1. In terms of educational level, 25 (49.0%) had attended school, of whom 12 (23.5%) had a primary education, 12 (23.5%) had a secondary education, and 1 (2.0%) had a higher education. The remaining 26 (51.0%) had no schooling. In terms of marital status, married people predominated, accounting for 37 (72.5%) of the total cohort.
● Among the 29 caregivers interviewed, 22 (75.9%) were aged between 30 and 59 years. Among this population, 14 (48.3%) were men and 15 (51.7%) were women, with a sex ratio of 0.9. Almost all 22 individuals (93.1%) had a university-level education. Married people predominated at 19 (65.5%). In terms of professions, 3 (10.3%) were doctors, 7 (24.1%) nurses and midwives, 4 (13.8%) physiotherapists, 5 (17.2%) social workers, and 3 (10.3%) traditional therapists and others (religious leaders and management assistants) (Table 4).
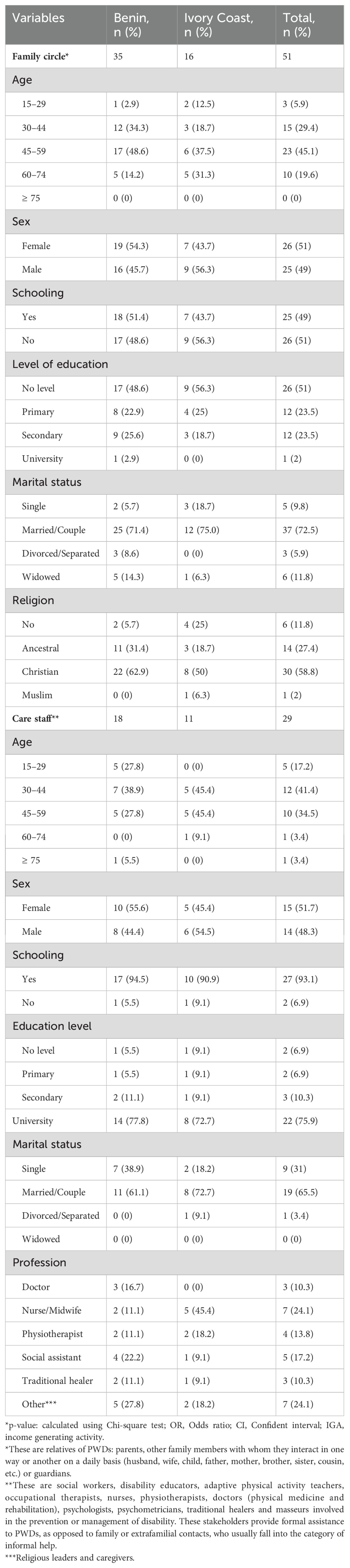
Table 4. Distribution of families and caregivers according to sociodemographic variables in Benin and Côte d’Ivoire.
3.4 Factors associated with disability management
● In the univariate analysis (Table 5), variables such as age, marital status, occupation, income, type of disability, and causes of disability were significantly associated with disability management in our study. When stratified by sex, only variables such as the IGA and level of education were significantly associated with inadequate disability management.
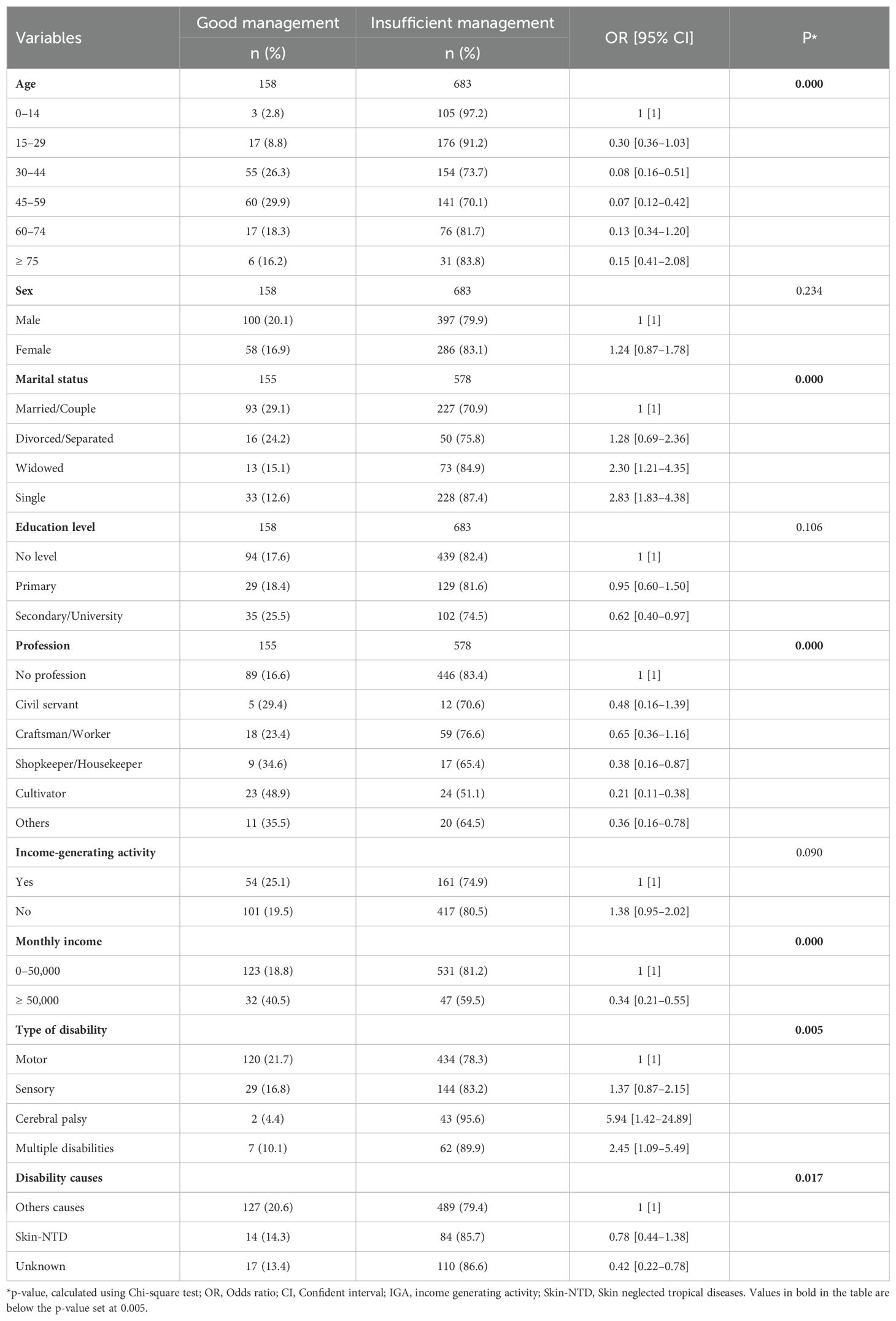
Table 5. Breakdown of sociodemographic to clinical variables in relation to inadequate management of disability.
A significant association was found between age and monthly income for both sexes. The risk of insufficient management decreases as age increases, except for women aged 75 and above (Table 6).
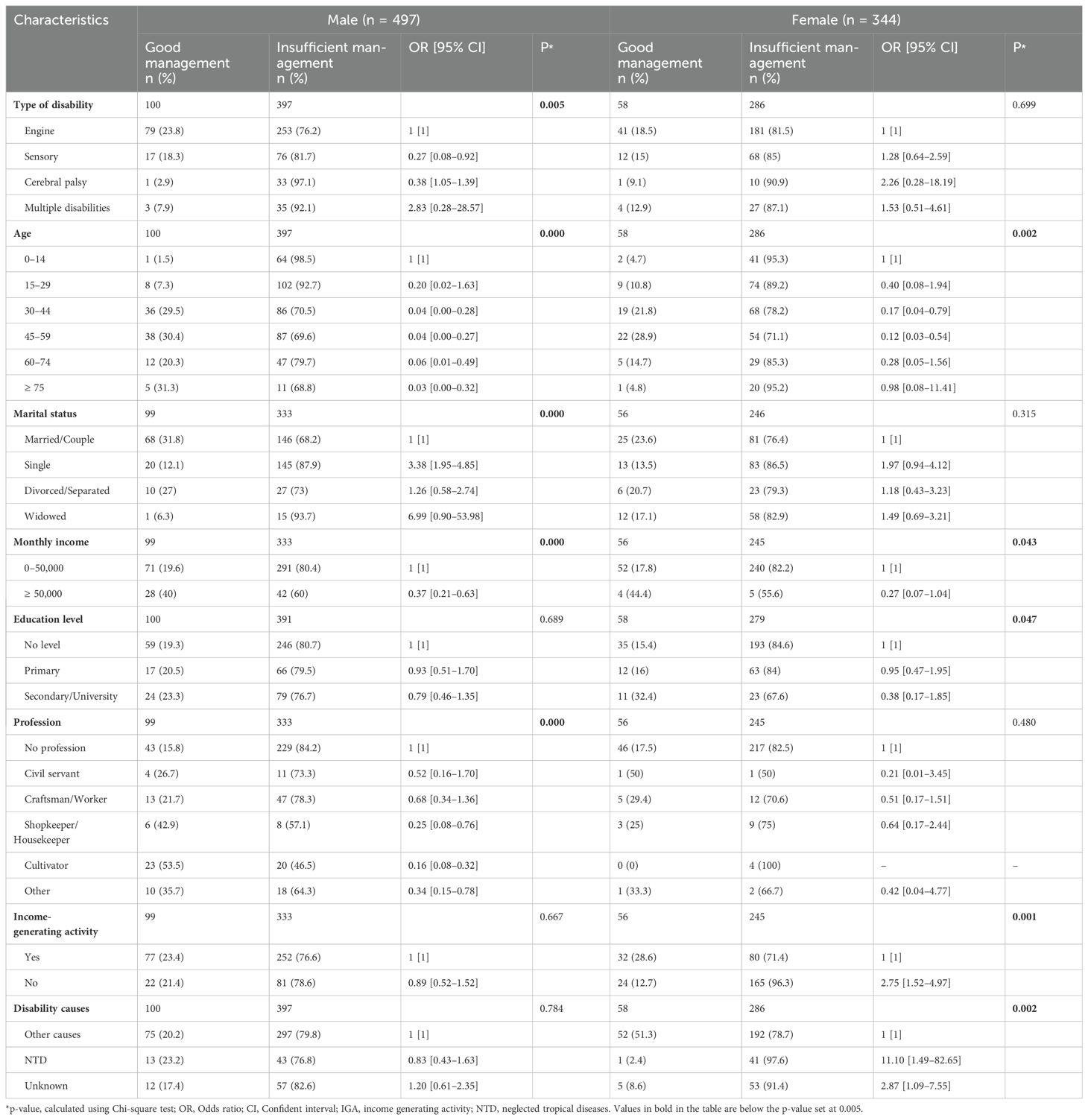
Table 6. Study of the associations between management and sex and a number of demographics, economic and medico-social characteristics among PWD (whether or not related to NTDs) in Benin and the Ivory Coast.
In men, significant associations were observed with marital status (p = 0.000), profession (p = 0.000), and type of disability (p = 0.005) in men. Being single, not having a profession, and having multiple disabilities increased the risk of receiving inadequate treatment (Table 6).
A significant association was also found between level of education (p = 0.047) and IGAs in women. Having some education and engaging in IGAs reduced the risk of experiencing insufficient management (Table 6).
● Multivariable analysis: multivariable analysis revealed four factors that were significantly associated with disability management: age (p=0.000), occupation (p=0.001), income (p=0.003), and causes of disability (p=0.000). These results are presented in Table 7.
● The factors ultimately associated with inadequate management by sex were as follows (Tables 8, 9):
- for men, young age, a monthly income of less than 76 euros and not exercising a profession;
- for women, not practicing an IGA and causes of disability due to NTDs.
● For men, the analysis revealed the following: age 30− to 44 years (OR=0.26 [95% CI=0.11−0.60]), age 45− to 59 years (OR=0.25 [95% CI=0.11−0.58]), age 75 years (OR=0.21 [95% CI=0.05−0.82]), monthly income greater than 76 euros (OR=0.47 [95% CI=0.25−0.89]) and occupation as farmer (OR=0.25 [95% CI=0.11−1.16]). For women, results were obtained for IGA (OR=3.04 [95% CI=1.64−5.61]) and NTD-related causes of disability (OR=12.61 [95% CI=1.67−95.31]).
● In others to explore the differences between both sexes regarding disability management and its associations with all variables (socio-demographic and socio-economic), an analysis was conducted, represented in Table 5.
● When stratified by sex, only variables such as the IGA and level of education were significantly associated with insufficient disability management.
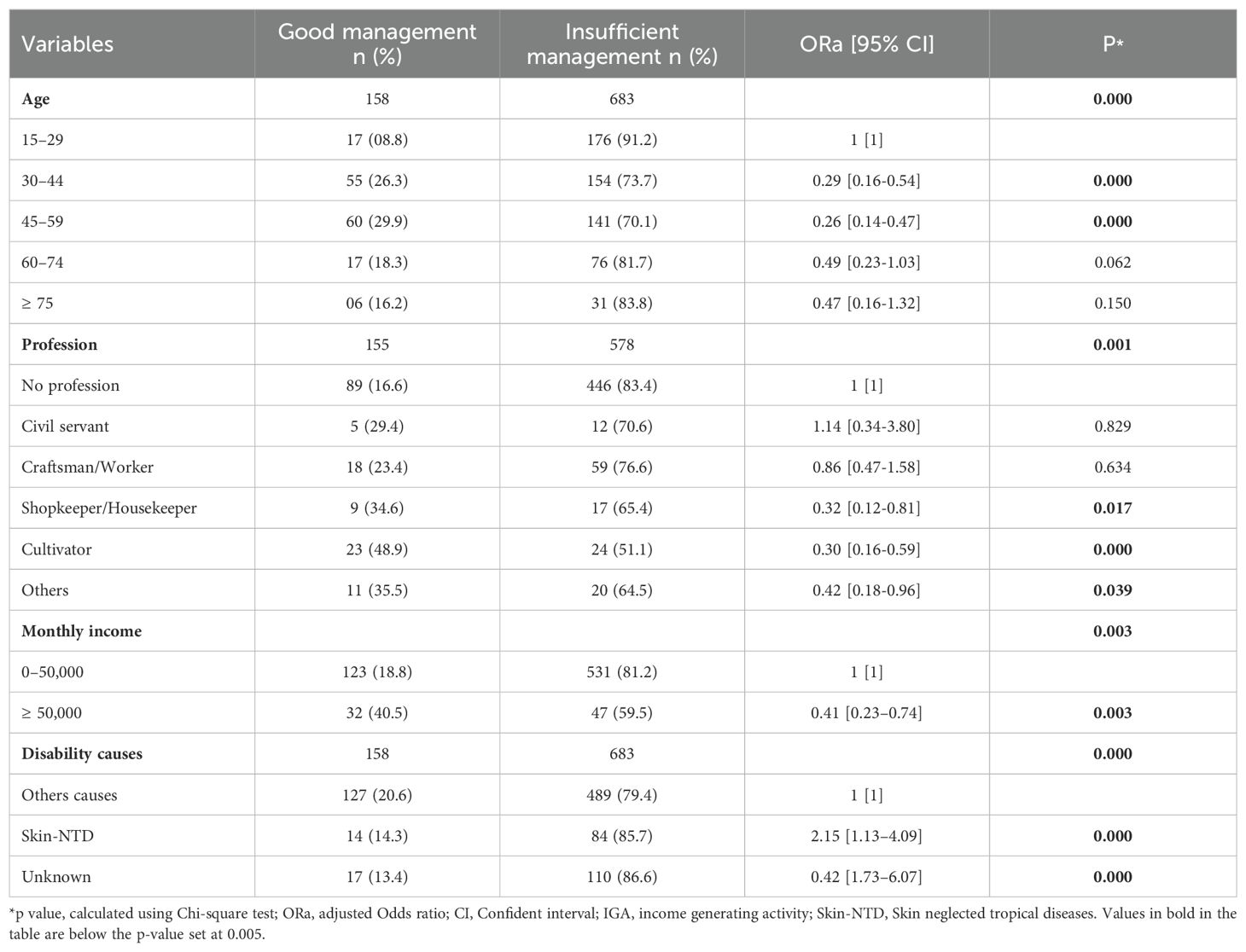
Table 7. Distribution of PWD linked to NTD or not, according to multivariable analysis with inadequate management in Benin and Côte d’Ivoire.
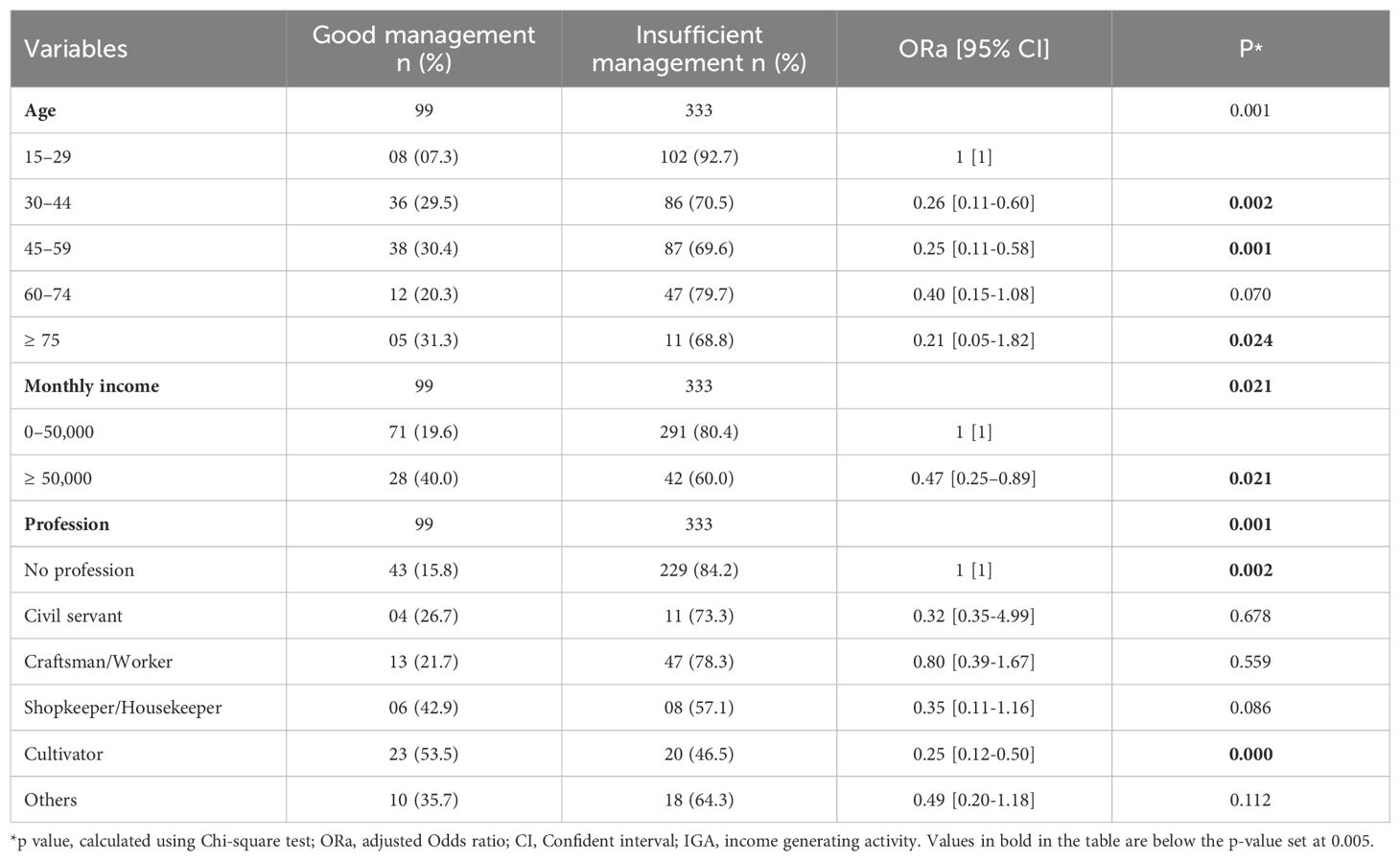
Table 8. Study of the association between management, male sex and some demographic, economic and medico-social characteristics among PWD (whether or not related to NTD) in Benin and Côte d’Ivoire.
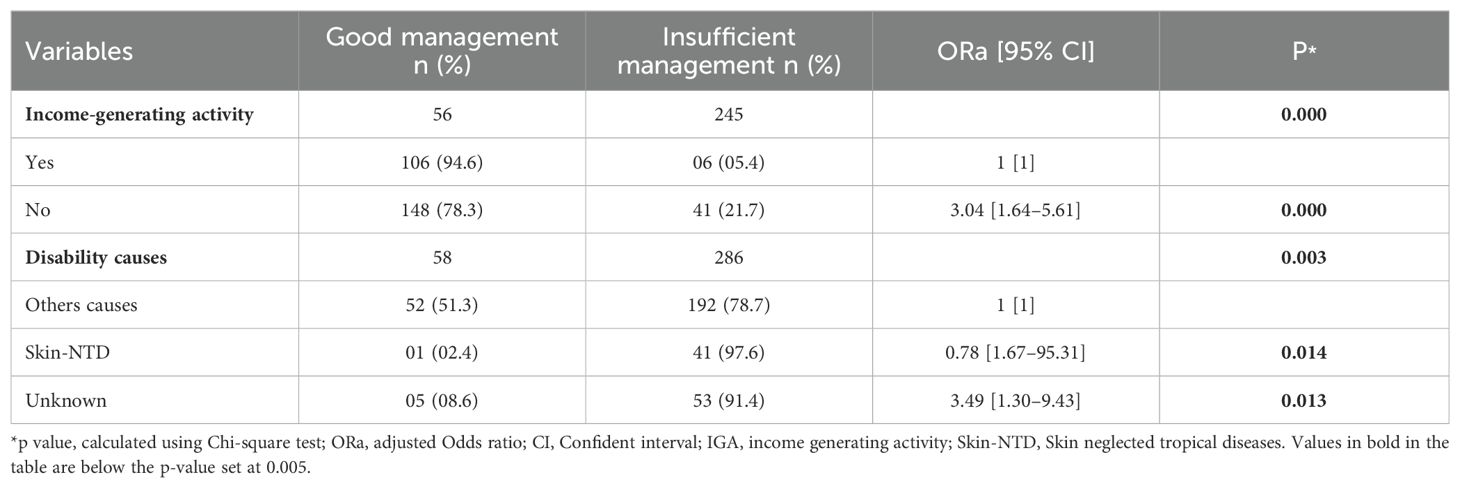
Table 9. Study of the association between management, female sex and some demographic, economic and medico-social characteristics among PWD (whether or not related to NTD) in Benin and Côte d’Ivoire.
A significant association was found between age and monthly income for both sexes. The risk of insufficient management decreases as age increases, except for women aged 75 and above. In the case of low incomes, the vulnerability to insufficient treatment increases.
In men, significant associations were observed with marital status (p = 0.000), profession (p = 0.000), and type of disability (p = 0.005) in men. Being single, not having a profession, and having multiple disabilities increased the risk of receiving inadequate treatment.
A significant association was also found between level of education (p = 0.047) and IGAs in women. Having some education and engaging in IGAs reduced the risk of experiencing insufficient management.
3.5 Problems encountered by PWD
In all of the interviews with PWD, the causes of their disabilities were shown to have profound economic, emotional, and social consequences. The deep interconnection of these factors highlights the need for not only medical interventions, but also social and economic support.
Data from in-depth interviews with a subsample of PWD affected by NTD illustrate how unemployment, lack of income, stigma, and isolation are interrelated and severely impact their lives. The narrative of Mrs. “AM” illustrates these challenges.
“I am disabled as a result of BU contracted at the age of 8 years. That is when Dr. Annick from the Tatonnoukon Health Center examined me and sent me to the Pobè leprosy and BU screening and treatment center. In my family, all I had was my mother’s support. Today, I have the support of my husband alone. I have lost three of my children due to lack of resources. What I’m most happy about today is that Dr. Annick enrolled me in school and put me through training. Then, I bought a sewing machine. My wish is that God will give me good health so that I can go about my business and open a store. I do not like stories, for fear of being insulted because of my handicap. I tell myself that by God’s grace, I will be able to join the community one day; only I will not be open to anyone. I also tell myself that others live worse lives than I do, so I keep hoping because tomorrow will be better.” (Mrs AM, 29, seamstress, Bonou-Benin).
Interviews like this highlighted a need for comprehensive interventions to help PWD regain a sense of self-worth and build meaningful social relationships.
3.6 Specific obstacles to care for PWD
3.6.1 Cultural perceptions of disabilities
Access to care is hindered by several obstacles, including the belief in the supernatural origin of disabilities, and a lack of knowledge about available disability management resources. In some cases, such as that of this 36-year-old man from Benin, disability is perceived to be a curse or the result of witchcraft. Notably, this belief has limited his pursuit of appropriate health care resources.
He explains:
“In my village, we do not know anything about the possibility of managing my disability in a health center. In addition, for me, this is a definitive situation, especially as it was not a natural illness. According to my understanding, the illness that led to my disability was considered to be a curse, the result of witchcraft, often referred to as “ayigbanou” disease (…….). For me, nothing is possible anymore. I was treated free of charge at the Lalo screening and treatment center (CDT)But now, where am I going to find the money to pay for additional treatment given my situation?” (Mr. DJ, 36, Tire repairer, Lalo-Benin).
This double barrier of the perceived supernatural origin of disability and financial constraints creates a vicious cycle that compromises access to disability management resources for PWD exacerbating their vulnerability.
3.6.2 Economic obstacles
In the context of caring for PWD, it is imperative to consider the profound impact of social and economic determinants on their well-being.
Unfortunately, the precarious socioeconomic conditions in which many PWD live exacerbate the complex challenges they face. One mother shared her experience with her daughter, who became disabled at the age of 13 years:
“After our daughter’s accidental fall, we underwent several types of treatment. She was first treated in the hospital, and as her disability persisted, we also tried traditional treatment without success. Friends referred us to a specialized hospital where she was operated on. The results were not satisfactory so, we had to perform further operations. Today, given the household financial situation, we no longer have the means to meet other expenses…” (Mother of Annick, motor-impaired, Taabo-Côte d’Ivoire).
The need for financial autonomy is crucial for the well-being of persons with disabilities (PWDs). While both governments recognize the need to offer support aimed at empowering PWDs, the assistance provided often falls short and remains inadequate due to a paucity of resources. As noted by Ms. KA from Côte d’Ivoire:
“For Ivorian society, PWDs are integrated into the system and benefit from the support of the Ministry of Employment and Social Protection. Institutions have been established to include them in education and employment. However, financial support is limited, and the actions undertaken often depend on available resources. Despite financial difficulties, initiatives such as financial support for PWD and their families or home visits show a commitment to these people. Financial challenges persist, but efforts are being made to provide ongoing support” (Ms. KA, 42, social worker and director of the social center, Yamoussoukro-Côte d’Ivoire).
3.6.3 Rehabilitation services are limited
Rehabilitation services available in each country are generally limited to referral centers typically financed by charitable organizations or regional hospitals. As Mr. GA, 33, a senior nurse and Mrs. YA, a 40-year-old physiotherapist from Divo, Côte d’Ivoire explain:
In terms of disability management, we do not have the resources or facilities to provide onsite rehabilitation, for example. We therefore refer patients to Taabo General Hospital. The costs of rehabilitation services vary, but can start at 500 francs (1 euro per session), with possible adjustments depending on the patient’s social situation. We do not offer direct disability management, but sometimes we organize home visits, if necessary, especially for patients who are unable to move. (Mr. GA, 33, senior nurse, CS Kouamékro-Côte d’Ivoire).
The physiotherapy department supports both outpatients and those at the Raoul Follereau hospital. The equipment includes two rehabilitation bikes, parallel bars, and other tools tailored to each condition. Patients are seen based on the severity and urgency of their situation. Services are free for those funded by the Raoul Follereau Foundation, while others have to pay for their care. Some patients with complications require surgery, which is often unavailable and financially out of reach for PWD. (Mrs. YA, 40 years old, physiotherapist, Divo-Côte d’Ivoire).
At referral centers where visits to former patients are offered, the role of these visits varies depending on the case and the stage of the disease. But the main concern is wound management, and sometimes it is to teach the disabled person how to take care of themselves on a daily basis.
4 Discussion
This study adopted an inclusive approach by considering the individual PWDs holistically and addressing both their medical and social support. Five factors were considered in the assessment of the management of disabilities: access to diagnosis, treatment, rehabilitation, psychosocial support, prevention, and follow-up services. The results demonstrate that out of a total of 841 PWD, 63.3% had support that was considered insufficient. Very few studies have been conducted on this subject, most of which have focused only on the qualitative aspect. Some of these studies have examined disability management, which is defined as an active process aimed at minimizing the impact of an impairment (resulting from an injury, illness or condition) on an individual’s ability to participate competitively in the work environment (12).
Hannah Kuper reported that disability management associated with neglected tropical diseases (NTDs) is often overlooked by programs focused on infectious disease control. To be more effective, these programs need to broaden their focus to include the provision of rehabilitation and mental health support services, as well as initiatives to combat stigma by eliminating NTDs (13). These efforts will contribute to the inclusion and well-being of people living with NTDs, demonstrating the current inadequacy of disability management (14).
In addition, Buruli ulcer and leprosy are closely linked, as shown by a study conducted in Liberia on the integrated management of these two neglected tropical skin diseases. This study reveals that another form of management should be considered. Thus, Mateo Prochazka et al. presented the results in three sections corresponding to patients’ experiences along three dimensions of management: (1) health education, disease identities, and interdisease stigma; (2) experiences of pain and healing through wound management and medication; and (3) rehabilitation experiences to address stigma and disability (15). It is therefore essential to consider these three dimensions and develop integrated management strategies that address not only the medical but also the psychosocial aspects of patients (16).
In addition, a 2012 study on the measurement of disability in patients with lymphatic filariasis examined generic tools used in morbidity management programs. The results of Lynne Zeldenryk et al. showed that the generic disability tools currently used by programs fail to measure the majority of known impacts of disability related to this disease. Therefore, the results of this review support the development of a lymphatic filariasis-specific disability measurement tool and raise doubts about the relevance of generic disability tools for assessing disability related to neglected tropical diseases (NTDs) globally (17, 18).
The median age of the PWD included in this study was 38 years. Thus, the PWD population is predominantly young. Badu et al., in a study that focused on barriers to access to health management for people with disabilities in the Kumasi metropolis in Ghana, reported that the average age of the respondents was 38 years (19).
Munthali et al. researched barriers to accessing health services for people with disabilities in Malawi and reported that the average age was greater than that reported in this study (47.02 years) (20).
The differences in the mean age of PWD between the different studies could be explained by the distinct socioeconomic and cultural contexts of the countries studied, which can influence the characteristics of the PWD population. For example, disparities in life expectancy, socioeconomic conditions and cultural attitudes toward disability may contribute to these variations in mean age (21). In addition, this study is distinguished by its comprehensive approach to management, encompassing not only medical aspects but also social, economic and cultural factors. By taking these different aspects into account, the present study offers a more complete understanding of the situation of PWD, which could influence the composition of the sample according to age (22). Thus, this results provide more detailed information on the challenges and needs of PWD, thus providing a solid basis for the development of policies and interventions aimed at improving their quality of life (23).
In this study, we had a predominance of PWD with no profession. This finding has been reported by several authors. Indeed, Badu et al. reported that 28.6% of PWD had no profession (19). Similarly, Koumbouna Coulibaly conducted a study on the disability and management of people with disabilities in the Banconi district of Mali. Based on their findings, it appeared that women with disabilities are particularly represented in this population. This finding highlights the specific position of women with disabilities in society (24). Women with disabilities may face unique challenges due to their dual sex and disability identities, which can increase their vulnerability to social exclusion and inequality (25).
There was a significant relationship between PWD income and undermanagement in the present study, which was consistent with several other studies, such as the study conducted by Yen et al. on factors associated with the use of free preventive health management for adults among people with physical disabilities in Taiwan: a nationwide population-based study. In that study, the results of the study showed that people with insured monthly payrolls of over NT$15,840 (excluding NT$48,200 to NT$57,800) have a higher utilization rate than those earning less than NT$15,840, which is consistent with the results of previous studies (26). These results highlight the importance of considering income and family burdens when health insurance policies are designed. They highlight socioeconomic disparities in access to health management and underscore the need for measures to ensure adequate coverage for all categories of the population, regardless of their income level or family situation (27).
In this study, causes of disability other than neglected tropical diseases were more predominant (79.4%). In contrast, in the study conducted by Koumbouna Coulibaly, disease-related disabilities were the majority, representing 36.9% of the cases (24). This difference may be explained by the different populations studied. Another possible contributing factor could be the methodology used in each study, including participant selection criteria, data collection tools, and samples studied.
At the end of the present study, it was found that disabilities related to these diseases were not more common than those attributable to other causes. However, the majority of PWD received insufficient management. This insufficiency was manifested in particular by a lack of adequate support in several aspects of their lives. The factors associated with the management of people with disabilities in the present study were age, occupation, income, and causes of disability. In addition, it would be relevant to explore the mechanisms by which socioeconomic factors influence access to management to propose appropriate interventions. Finally, it is essential to conduct key experiments, such as the evaluation of pilot programs that integrate solutions on the basis of these factors, such as expanding the resources allocated to the management of PWD in endemic areas and raising awareness among vulnerable populations about the importance of early detection of Skin-NTD.
However, some limitations must be considered. The reliance on self-reported data may have introduced bias due to recall bias, social desirability bias, and potential differences in understanding and interpreting questions. The use of simultaneous translation during interviews could have introduced the potential for information bias, although efforts were made to minimize this through rigorous interviewer training and pre-testing of the translated questionnaires.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The study was approved by the research ethics committee of the University of Parakou (CLERB-UP) in Benin under authorization N°0492/CLERB-UP/P/SP/R/SA of 19/11/2021 and by the National Life and Health Sciences Ethics Committee (CNESVS) of Côte d’Ivoire under authorization N/Réf: 076-22/MSHPCMU/CNESVSkp of 28/07/2022. Written informed consent was obtained from all participants, with an emphasis on the voluntary nature of participation. It was made clear that there would be no consequences for those who chose not to participate.
Author contributions
YT: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Writing – original draft, Writing – review & editing. FNG: Conceptualization, Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. SIA: Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. SZ: Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. KC-S: Data curation, Formal analysis, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. PB: Conceptualization, Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. FAG: Data curation, Formal analysis, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. KK: Data curation, Formal analysis, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. SGA: Writing – original draft, Writing – review & editing. FZM: Writing – original draft, Writing – review & editing. PD: Writing – original draft, Writing – review & editing. BY: Writing – original draft, Writing – review & editing. FH: Writing – original draft, Writing – review & editing. JA: Writing – original draft, Writing – review & editing. YF: Writing – original draft, Writing – review & editing. HJ: Writing – original draft, Writing – review & editing. GS: Methodology, Writing – original draft, Writing – review & editing. JH: Conceptualization, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MK: Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AD: Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MN: Conceptualization, Data curation, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. CJ: Conceptualization, Funding acquisition, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AG-M: Conceptualization, Funding acquisition, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. RJ: Conceptualization, Data curation, Formal analysis, Funding acquisition, Methodology, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The data contained in this article are part of a research project titled “Rational approach for effective management of disabilities related to Skin- NTD in Benin and Cote d’Ivoire”. It is funded by the ANESVAD Foundation and the RAOUL FOLLEREAU Foundation with the grant number REG-3621/21.
Acknowledgments
We would like to thank all the members of the disability project team, the staff of the BU Screening and Treatment Center and Leprosy Treatment Center, and the National Program for the Fight against Leprosy and Buruli Ulcer in Benin. We would also like to thank the National Program for the Control of Leprosy and Buruli Ulcer in Benin, the National Program for the Control of Buruli Ulcer in Benin, the National Program for the Control of Buruli Ulcer in Côte d’Ivoire and the National Program for the Elimination of Leprosy in Côte d’Ivoire for their administrative and technical support in carrying out this study for their administrative and technical support. We would also like to thank the RAOUL FOLLEREAU Benin Foundation, the RAOUL FOLLEREAU Ivory Coast Foundation and the ANESVAD Foundation.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fitd.2025.1522660/full#supplementary-material
Abbreviations
BU, Buruli ulcer; CP, Cerebral Palsy; IGA, Income-Generating Activity; LF, Lymphatic Filariasis; LMICs, Low-and Middle-Income Countries; NGO, Nongovernmental Organization; Skin-NTD, Skin neglected tropical diseases; NTDs, Neglected Tropical Diseases; PWDs, People with Disabilities; WHO, World Health Organization.
References
1. Organisation mondiale de la Santé. Projet de plan d’action mondial de l’OMS relatif au handicap 2014-2021 : un meilleur état de santé pour toutes les personnes handicapées. (2014) 1–34.
2. World health statistics 2024: monitoring health for the SDGs, sustainable development goals . Available online at: https://www.who.int/publications/i/item/9789240094703 (Accessed January 20, 2025).
3. Mac-Seing M, Zarowsky C. Une méta-synthèse sur le genre, le handicap et la santé reproductive en Afrique subsaharienne. Santé Publique. (2017) 29 (6), 909–919. doi: 10.3917/spub.176.0909
4. Strub-Wourgaft N. Les maladies tropicales négligées : un modèle collaboratif au service de l’innovation scientifique et médicale. Dans Armand J., Brun M., Cossy J., Doré J., Duchateau P., Guillamot G., et al (dir.), Chimie et Nouvelles Thérapies. (p. 85-104). EDP Sciences. Available at: https://stm.cairn.info/chimie-et-nouvelles-therapies--9782759824786-page-85?lang=fr.
5. INEE. Opportunities and Challenges for Disability-Inclusive Early Childhood Development in Emergencies . INEE. Available online at: https://inee.org/resources/opportunities-and-challenges-disability-inclusive-early-childhood-development-emergencies (Accessed January 20, 2025).
6. Organisation mondiale de la Santé. Intégrer les maladies tropicales négligées dans l’action pour la santé mondiale et le développement : quatrième rapport de l’OMS sur les maladies tropicales négligées. Organisation mondiale de la Santé (2018), 1-271.
7. Global leprosy (Hansen disease) update, 2022: new paradigm – control to elimination (2022). Available online at: https://www.who.int/publications/i/item/who-wer9837-409-430 (Accessed January 20, 2025).
8. Plan zéro-lèpre en Côte d’Ivoire à l’horizon 2030 : Le Gouvernement annonce la mobilisation 90% du budget et demande l’engagement de tous les acteurs (2022). OMS | Bureau régional pour l’Afrique. Available online at: https://www.afro.who.int/fr/countries/cote-divoire/news/plan-zero-lepre-en-cote-divoire-lhorizon-2030-le-gouvernement-annonce-la-mobilisation-90-du-budget (Accessed January 20, 2025).
9. OMS. Rapport de situation 2022 – Résumé d’orientation (2022). Available online at: https://www.who.int/fr/publications/m/item/2022-progress-report-executive-summary (Accessed January 20, 2025).
10. Ministère de la santé et du développement social. Plan stratégique intégré de lutte contre les Maladies tropicales Négligées (MTN). (2022).
11. La stigmatisation et les discriminations - Psycom - Santé Mentale Info . Available online at: https://www.psycom.org/comprendre/la-stigmatisation-et-les-discriminations/ (Accessed July 23, 2024).
12. Boseman J. Disability management. Application of a nurse based model in a large corporation. AAOHN J. (2001) 49:176–86. doi: 10.1177/216507990104900406
13. Kuper H. Disability, mental health, stigma and discrimination and neglected tropical diseases. Trans R Soc Trop Med Hyg. (2021) 115:145–6. doi: 10.1093/trstmh/traa160
14. Après le trachome, les acteurs s’engagent à redoubler d’efforts afin d’éliminer les autres MTN au Bénin (2024). OMS | Bureau régional pour l’Afrique. Available online at: https://www.afro.who.int/fr/countries/Benin/news/apres-le-trachome-les-acteurs-sengagent-redoubler-defforts-afin-deliminer-les-autres-mtn-au-Benin (Accessed January 20, 2025).
15. Prochazka M, Timothy J, Pullan R, Kollie K, Rogers E, Wright A, et al. Buruli ulcer and leprosy, they are intertwined”: Patient experiences of integrated case management of skin neglected tropical diseases in Liberia. PloS Negl Trop Dis. (2020) 14:e0008030. doi: 10.1371/journal.pntd.0008030
16. OMS, BM. La qualité des services de santé : Un impératif mondial en vue de la couverture santé universelle (2019). OCDE. Available online at: https://www.oecd.org/fr/publications/la-qualite-des-services-de-sante-un-imperatif-mondial-en-vue-de-la-couverture-sante-universelle_62f287af-fr.html (Accessed January 20, 2025).
17. Zeldenryk L, Gordon S, Gray M, Speare R, Melrose W. Disability measurement for lymphatic filariasis: A review of generic tools used within morbidity management programs. PloS Negl Trop Dis. (2012) 6:e1768. doi: 10.1371/journal.pntd.0001768
18. Filariose lymphatique (2024). Available online at: https://www.who.int/fr/news-room/fact-sheets/detail/lymphatic-filariasis (Accessed January 20, 2025).
19. Badu E, Agyei-Baffour P, Opoku MP. Access barriers to health care among people with disabilities in the Kumasi metropolis of Ghana. Can J Disabil Stud. (2016) 5:131–51. doi: 10.15353/cjds.v5i2.275
20. Munthali AC, Swartz L, Mannan H, MacLachlan M, Chilimampunga C, Makupe C. This one will delay us”: barriers to accessing health care services among persons with disabilities in Malawi. Disabil Rehabil. (2019) 41:683–90. doi: 10.1080/09638288.2017.1404148
21. Être handicapé dans les pays arabes: état des lieux et perspectives (2007). Available online at: https://www.dvv-international.de/fr/education-des-adultes-et-developpement/numeros/ead-682007/education-des-adultes-pour-les-personnes-handicapees/etre-handicape-dans-les-pays-arabes-etat-des-lieux-et-perspectives (Accessed January 20, 2025).
22. UN Enable - Promoting the rights of Persons with Disabilities - Statement by H.E. Mr. Jan Kavan, in: President of the 57th Session of the United Nations General Assembly 2004. Available at: https://www.un.org/esa/socdev/enable/rights/contrib-jk.htm.
23. Bakhshi P, Trani J-F. La conduite d’enquête auprès des personnes handicapées en Afghanistan : défis d’un terrain et réponses méthodologiques. STATECO (2007) p. 1–18.
24. Coulibaly D. Etude de la prévalence du handicap et prise en charge des personnes handicapées dans la commune VI du district de Bamako. (2013).
25. Les inégalités en matière de santé entraînent de nombreux décès prématurés chez les personnes handicapées (2022). Available online at: https://www.who.int/fr/news/item/02-12-2022-health-inequities-lead-to-early-death-in-many-persons-with-disabilities (Accessed January 20, 2025).
26. Yen S-M, Kung P-T, Tsai W-C. Factors associated with free adult preventive health care utilization among physically disabled people in Taiwan: nationwide population-based study. BMC Health Serv Res. (2014) 14:610. doi: 10.1186/s12913-014-0610-5
27. Couverture sanitaire universelle (CSU). (2023). Available online at: https://www.who.int/fr/news-room/fact-sheets/detail/universal-health-coverage-(uhc) (Accessed January 20, 2025).
Keywords: people with disabilities, infectious tropical diseases, management, Benin, Côte d’Ivoire west Africa
Citation: Tossou YB, Gbaguidi FNC, Agbo SIE, Zanvo SDE, Codjo-Seignon KLM, Biaka PH, Guedou FA, Kouadio KJ, Anagonou SGE, Mignanwande FZ, Djossou P, Yemadje BV, Houndjrebo FS, Arrawo JdNL, Faihoun Y, Johnson H, Sopoh GE, Houezo JG, Kaloga M, Dizoe AS, Nichter M, Juan Jimenez C, Gine-March A and Johnson RC (2025) Factors associated with the management of people affected by disabilities in communities endemic to skin-related neglected tropical diseases in Benin and Côte d’Ivoire. Front. Trop. Dis. 6:1522660. doi: 10.3389/fitd.2025.1522660
Received: 04 November 2024; Accepted: 07 February 2025;
Published: 06 March 2025.
Edited by:
Vito Colella, The University of Melbourne, AustraliaReviewed by:
Leticia Gomes De Pontes, Departamento de Bioquímica e Imunologia da Universidade de Minas Gerais, BrazilAbayeneh Girma, Mekdela Amba University, Ethiopia
Copyright © 2025 Tossou, Gbaguidi, Agbo, Zanvo, Codjo-Seignon, Biaka, Guedou, Kouadio, Anagonou, Mignanwande, Djossou, Yemadje, Houndjrebo, Arrawo, Faihoun, Johnson, Sopoh, Houezo, Kaloga, Dizoe, Nichter, Juan Jimenez, Gine-March and Johnson. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yévèdo Borel Tossou, tossouborel@yahoo.fr