 Watton Rodrigue Diao
Watton Rodrigue Diao Abel Bicaba
Abel Bicaba Aboubacar Sanou
Aboubacar Sanou Lissy Eric Parfait Ouattara
Lissy Eric Parfait Ouattara
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Trop. Dis., 07 March 2025
Sec. Neglected Tropical Diseases
Volume 6 - 2025 | https://doi.org/10.3389/fitd.2025.1516101
This article is part of the Research TopicEnhancing Global Access to Diagnostic Tools for Emerging Tropical Diseases in Resource-Limited SettingsView all articles
Objectives: This study intends to learn lessons quickly from the dengue epidemic of 2023 in Burkina Faso for better preparation for future health emergencies.
Methods: A cross-sectional study was conducted from April to May 2024. The technical functions to be explored were coordination, case management, epidemiological surveillance, risk communication and community engagement, vector management, laboratory and logistics. The members of the after action review were selected according to a reasoned process to document best practice and gaps, and to formulate key recommendations.
Results: The workshops reported that the level of preparedness was good and the response was adequate compared with epidemics in previous years. Gaps were observed mainly in terms of leadership in planning and resource mobilization. All the recommendations arising from this review were discussed and the main ones retained in order to strengthen the system’s response capacity.
Conclusion: As this study is an internal evaluation, it would be interesting to combine it with an external evaluation to analyze the structuring of the response mechanism, its operation and the effectiveness of interventions.
Dengue is an arbovirosis whose virus is transmitted to humans by the bite of the infecting female Aedes mosquito. Serotypes 1, 2, 3, and 4 circulate worldwide (1). The number of incident cases of dengue fever has risen alarmingly worldwide in recent decades (2).
The West African region was not spared from dengue fever in 2023. Out of a population of 456 million (3), 171,991 suspected cases of dengue fever, including 70,223 confirmed cases and 753 deaths, were reported in 15 West African countries. Burkina Faso was the country most affected by dengue fever (4). The epidemiological situation in Burkina Faso was particularly marked by the dengue epidemic in 2023. According to the Laboratoire National de Référence des Fièvres Hémorragiques Virales (LNR- FHV), 79% of dengue cases were due to the DENV-3 serotype. Aedes aegypti was the main vector involved in dengue transmission. The Centre region was particularly hard hit, with 89,799 suspected cases of dengue, including 43,946 probable cases and 351 deaths. At the end of 2023, the incidence of dengue fever in this region was 1,268 cases per 100,000 inhabitants (5).
In the absence of antiviral drugs and effective vaccines, the fight against dengue is essentially based on epidemiological surveillance, mapping of cases, communication and awareness raising, strengthening management skill and vector management. A number of actions were carried out as part of the management of this epidemic.
As for epidemiological surveillance, monitoring to improve data quality were carried out in the health districts. Case maps were drawn up for targeted action. Clinical audits of deaths was carried out to improve the management of serious cases. Samples were collected and forwarded to the LNR-FHV for case confirmation. As a result, three virus serotypes (DENV1, DENV2 and DENV3) were identified in 2023 in the Centre region. In terms of communication, awareness-raising and mobilization messages were broadcast on radio and television. Target groups such as nurserymen, market gardeners and teachers have been sensitized. In terms of strengthening management skills, training has also been provided for those involved. At coordination level, these included training to strengthen management skills, meetings with municipal authorities and technical and financial partners (TFPs) to mobilize funds, and regular meetings of the national epidemic management committee. Vector management activities focused on destroying larval breeding sites and spraying in and around homes.
It should be noted that in the national health context, despite the recurrence of epidemics of various kinds, very few post-epidemic assessments are carried out. Analyses are generally quantitative, based on data collected during epidemics. At the end of the 2023 dengue epidemic, the aim was to evaluate, using the After Action Review (AAR) approach (6) to identify the capacities in place prior to the intervention, any difficulties encountered during the intervention, lessons learned, and best practices observed during the intervention, including the development of new capacities. This is one of the recommendations of the World Health Organization (WHO) following a public health emergency response (6).
The AAR was applied in this study. This is a qualitative approach based on structured stakeholder discussions on experience sharing for analyzing the chronology of previous interventions, identifying successes and failures in order to project into the future for better action (7, 8). The study was carried out from April to May 2024 and concerns the Centre region. This administrative region is home to the country’s largest urban city. Epidemiologically, it has suffered repeated outbreaks of dengue fever in 2013, 2016 and 2017 (5). In 2023, all health districts were affected by dengue epidemics.
The AAR process was developed in line with WHO recommendations, using the “debriefing workshop” format. It is an approach based on retrospective review with ten (10) facilitators from Centre des Opérations de Réponse aux Urgences Sanitaires (CORUS), other central departments of the Ministry of Health and TFPs. They had received prior training in the AAR methodology. They are responsible for organizing exchanges, retaining the best ideas and converging them towards the objective set by the RAA. The AAR stakeholders (key informants) were selected on the basis of two criteria: their commitment to the fight against the dengue epidemic in 2023, and their experience in conducting AAR. They include national experts from the Ministries of Health, Territorial Administration, Higher Education and Scientific Research, Defense, civil society, and technical and financial partners. To facilitate sub- committee work, interventions have been grouped into eight (8) pillars or functions: coordination; case management and prevention; epidemiological surveillance; Risk communication and community engagement (RCCE); vector management; laboratory and logistics. One or more neutral facilitators (depending on the level of progress) help stakeholders to reflect on their shared experiences. An introductory presentation was made on the AAR method, the incident action plan for the Centre region, and a review of preparedness and response documents to enable stakeholders to make a critical diagnosis based on their informed experience and knowledge of interventions during the dengue epidemic in 2023. These presentations helped participants to familiarize themselves with analysis, the sharing of good practices and the identification of challenges. Participants were organized into five sub-committees or teams and tasked with exploring all the functions or seven pillars (6). To achieve this, five workshop sessions were held: session one on “setting the scene”; session two on “what happened during the response”; session three on “what worked well? what didn’t work so well”; session four on “what can be done to improve the response next time”; and session five on “moving forward”. All facilitators and stakeholders were present at all workshop sessions.
After the committee work, the results were presented in plenary followed by discussion. Post-it notes in different colors were used to facilitate the reporting of group work to the plenary. The results of the plenary sessions were structured in two main parts: what was in place before the response and what happened during the response. Analysis of the results focused on assessing the level of preparedness of the response, best practices and gaps. The activities that received the highest scores over the five sessions were considered and the subject of key recommendations for countering future dengue epidemics.
Long before the activation of the regional CORUS, there was a coordinating body for the response to health emergencies. This coordination had standards and guidelines in terms of control policy and strategy. There was a support mechanism in place, focusing on the availability of documents and guidelines, health infrastructures, human resources and logistics. Support from partners to improve healthcare provision was already in place. The main activities underway were training in integrated disease surveillance and response, briefing private-sector health workers on diseases with epidemic potential, and pre-positioning of inputs.
In terms of epidemiological surveillance, all existing documentation was mobilized to ensure proper monitoring of the epidemic’s dynamics. This made it possible to identify existing resources in terms of human resources, logistics, support and financial resources through the mobilization of the epidemic management fund.
As part of our response preparedness, stakeholders have been trained in RCCE and the incident management system. Resources have been mobilized, and awareness-raising messages should be developed and broadcast on radio, television and other communication platforms identified for this purpose.
Given the rapid spread of this disease in the community, vector management was a key aspect of our preparations. The first step was to gather together all existing documentation and information on the vector, its aggressiveness, bio-ecology and level of insecticide resistance. Medical entomologists were to train community relays mobilized to carry out distribution activities for Long-lasting insecticidal nets. Coordination was provided by CORUS.
Finally, logistics were mobilized around a dozen preparation activities. Resources were focused primarily on the purchase and supply of equipment, materials and inputs. Documentation on emergency response was well supplied.
The Centre region reported 120 suspected cases of dengue in the first week of 2023. The outbreak began in week 28 with 128 cases, peaking in week 43 with 10,152 cases. Interventions intensified in early November as the attack rate rose to 672 cases per 100,000 inhabitants. Tables 1, 2 show the best practices and key gaps in the different response functions.
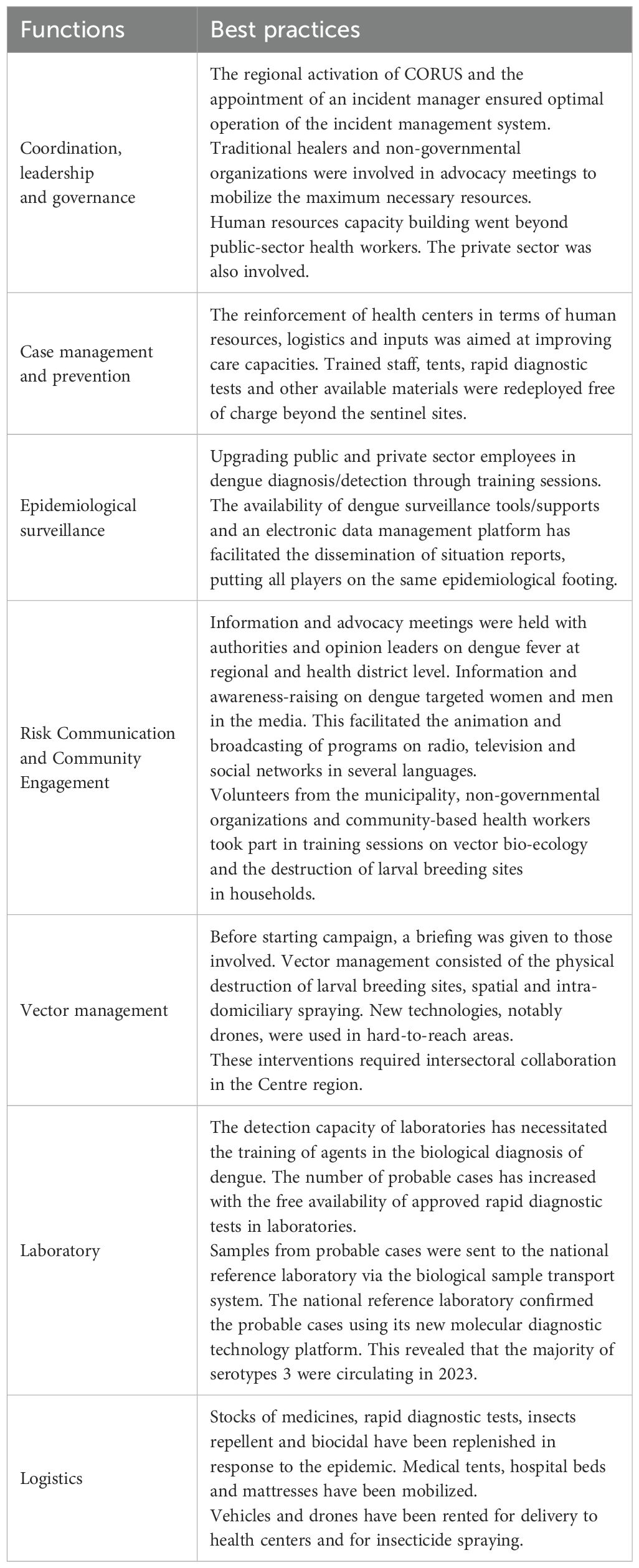
Table 1. Best practices by function observed during the dengue epidemic in the Centre region, Burkina Faso in 2023.

Table 2. Main gaps identified by function during the dengue epidemic in the Centre region, Burkina Faso in 2023.
Our study showed that the response functions had normative documents already drawn up, a minimum of their own resources mobilized, coordination mechanisms in place and epidemic-related activities in progress. In 2017, the dengue epidemic response system had not reached this level of preparedness. Laboratory and logistics functions did not exist (9). Prior to the 2023 epidemic, working documents were updated and new normative documents such as hospital white plans, guidelines for the management of diseases with epidemic potential, the plan to control arbovirosis in Burkina Faso, and standard operating procedures on the coordination/mobilization of resources were drawn up. Existing human resources were strengthened with the planned training of national volunteers/community-based health agents and, above all, the creation of a rapid response team whose personnel should receive training in incident management systems. The teams already had manual sprayers and vehicles.
During the response to the 2023 dengue epidemic, we note that coordination in the management of this epidemic was better structured than in 2017. We note a clear improvement in the performance of the regional incident system thanks to resource-building activities, namely organized training and simulation exercises. Coordination played a key role, providing guidance throughout the incident management process. Efficient use of human resources was limited by a failure to plan for the skills needed to manage the incident, and by a financial deficit. Virtuous governance of endogenous financial resources and knowledge of the management standards of financial partners should offset delays linked to disbursement requirements (10, 11). Free health care led to an influx of dengue-infected patients, but did not hinder the provision of routine inpatient and outpatient care in health centers. Continuity of care was facilitated by the provision of rapid diagnostic tests (RDTs) to health facilities.
Epidemiological surveillance had seen a clear improvement over previous health emergency in 2017 (9). This surveillance enabled CORUS to be alerted and act in time: targeting of an area, intensification of activities, generalization of the intervention and normalization of the situation.
During health emergencies, there is a large amount of information and messages circulating, and this can lead to negative perceptions that limit the system’s ability to respond. It is important to develop accurate risk communication (12). During the dengue epidemic, the RCCE was of strategic importance, with a communication and media plan focused on the community. An option was made for top-down communication, despite the existence of theoretical models developed for emergency and disaster management (7, 8, 13–15). However, the engagement of community leaders and the use of information and communication technologies helped to channel the flow of information, raise awareness and provide an effective response.
The response to dengue fever was essentially focused on interventions against Aedes aegypti, in the absence of vaccines and drugs targeting the virus. The regional CORUS relied on local authorities, TFPs and other sectors to mobilize key players, train them and provide them with the resources to carry out operations to physically destroy breeding sites and spray insecticides. In 2023, we note a clear improvement in the response to the disease compared with previous epidemics. In fact, past vector management initiatives and CORUS’ level of preparedness have strengthened the response in 2023. The major obstacle here is the low level of engagement of community-based implementing organizations in vector management, due to a lack of communication.
Despite efforts to strengthen the diagnostic capacity of laboratories (staff training and provision of molecular biology reagents), the supply of RDTs and polymerase chain reaction (PCR) reagents remains below epidemic levels. This has limited access to the test. This situation can be explained by inadequate planning, a shortage of local suppliers, the absence of optimized in-house PCR protocols and a delay in the disbursement of funds. Studies have shown that the diagnosis of a case of dengue fever, combined with the physical elimination of larval breeding sites by the community in the vicinity of sufferers, can significantly reduce the risk of dengue spreading (16).
The logistics chain during the 2023 epidemic appears to have been more appropriate than previous experience, in that it enabled better management of patient flows and biological samples. As part of the preparedness plan, a minimum stock of inputs was pre-positioned for dengue case management and vector management. Although this system received substantial support from partners, it should be noted that the continued availability of equipment, materials, reagents and consumables depended more on the quality of planning, mastery of emergency purchasing procedures and knowledge of financial partners’ disbursement mechanisms. The various procedures need to be standardized and tested well in advance of the epidemic.
The AAR method is a holistic, interdisciplinary approach to internal assessment. The analyses of certain participants can have a group effect. The training of participants in the AAR approach and its appropriation by them were part of a participatory approach. This minimized the influence of the group. AAR should take place at the right time, no more than three months after the health emergency. In our case, the AAR took place three months after the CORUS activation was lifted. To minimize recall bias, the introductory talk, the presentation of the incident action plan and the review of a few documents were of considerable help.
A regional dengue response plan must be drawn up annually. This plan must include training in emergency/epidemic management. This will make it possible to set up a directory of trained agents. Funding sessions will be organized and stakeholders will be asked to contribute.
For efficient case management, referral and counter-referral must be known and applied by health workers. The regional dengue response plan provides an opportunity to strengthen the skills of health workers. To cope with the massive influx of patients to public health centers, we need to strengthen collaboration with the private sector.
The recommendations are more focused on strengthening the system’s capacities: training some 50 agents in dengue surveillance for each health district and each Centres Hospitaliers Universitaires; permanent availability of collection tools/supports; specific supervision of case management staff in the use of RDTs; and recruitment of five operators to enter notification data for Centres Hospitaliers Universitaires.
The regional dengue response plan should include the training of some 30 volunteers in the development of the RCCE plan. Door-to-door awareness-raising activities on dengue prevention measures are to be implemented. These awareness-raising activities will be reinforced by the production of around twenty radio broadcasts on dengue in the main spoken languages. A rapid survey is to be carried out among the population to gather their perception of the messages broadcast.
The main recommendations focus on pleas to stakeholders for their financial contribution and on the engagement of community leaders in vector management activities.
This study shows the importance of effective preparedness and response in managing a dengue epidemic. After this study, it appears that interventions are consistent with previous years. In fact, the quality of interventions was linked to an increase in the level of preparedness for the response, and above all to system’s appropriation of experiences inherited from previous epidemics. Best practices and shortcomings were reported. Finally, key recommendations were made to improve future response capacities to other infectious diseases threatening the country.
The data that support the findings of this AAR are available on request from the head of CORUS. The data are not ready available due to information on the contribution of ARR members who took part in this study. This may violate the principle of confidentiality. Requests to access the datasets should be directed to Watton Rodrigue Diao, cm9kcmlndWVkaWFvQGdtYWlsLmNvbQ==.
WD: Conceptualization, Data curation, Investigation, Project administration, Resources, Writing – review & editing. AB: Conceptualization, Formal Analysis, Methodology, Validation, Writing – review & editing. AS: Formal Analysis, Methodology, Visualization, Writing – review & editing. LO: Conceptualization, Formal Analysis, Methodology, Project administration, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors would like to thank all those who helped to make this study possible. We thank the Minister of Health and the Regional Director of Health for the Centre for facilitating access to resource persons and documents. Finally, we would also like to thank SERSAP for sharing its experience in exploiting AAR data.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. OMS, Médias C des. Dengue et dengue sévère(2016). Available online at: http://www.who.int/mediacentre/factsheets/fs117/fr/ (Accessed February 17, 2017).
2. WHO. Dengue and severe dengue. Who, Geneva (2024). Available at: https://www.who.int/news-room/fact-sheets/detail/dengue-and-severe-dengue (Accessed July 6, 2024).
3. Nations Unies/Commission économique pour l’Afrique. Profil socioéconomique de l’Afrique de l’Ouest, 2024 : une sous-région résiliente qui subit les effets socioéconomiques négatifs de crises multiples. Rabat (Maroc). (2024), 17.
4. World Health Organization. Dengue in the WHO African region, in: Situation report 01: 19 December 2023 (2023). Available online at: https://www.afro.who.int/countries/burkina-faso/publication/dengue-who-african-region-situation-report-01-19-december-2023 (Accessed June 23, 2024).
7. Taylor F, Dickmann P, McClelland A, Gamhewage GM, Portela de Souza Fa. P. Making sense of communication interventions in public health emergencies–an evaluation framework for risk communication. J Commun Heal 2015. (2015) 8:233–40. doi: 10.1080/17538068.2015.1101962. Taylor Fr Dickmann, A McClelland, GM Gamhewage, P Portela Souza, F Apfel.
8. Finucane ML, Holup JL. Risk as value: Combining affect and analysis in risk judgments. J Risk Res. (2006) 9:141–64. doi: 10.1080/13669870500166930
9. Ministère de la santé. Revue Après Action Épidémie de Dengue au Burkina Faso. Ouagadougou, Burkina Faso (2018). p. 64.
10. Godshall CE, Banach DB. Pandemic preparedness. Infect Dis Clin North Am. (2021) 35:1077–89. doi: 10.1016/J.IDC.2021.07.008
11. Chawla M, Schmunis R. pandemic preparedness. J Glob Health. (2024) 14:3026. doi: 10.7189/JOGH.14.03026
12. Khan S, Mishra J, Ahmed N, Onyige CD, Lin KE, Siew R, et al. Risk communication and community engagement during COVID-19. Int J Disaster Risk Reduct. (2022) 74:102903. doi: 10.1016/J.IJDRR.2022.102903
13. Sellnow-Richmond D. An IDEA model analysis of instructional risk communication in the time of Ebola. jicrcr.com. J Int Cris Risk Commun Res. (2018) 1:135–66. doi: 10.30658/jicrcr.1.1.7. AG-J of I, 2018 Undefined2018•jicrcr.com.
14. Janoske M, Brooke L, Ben S. Understanding risk communication theory: a guide for emergency managers and communicators. Maryland. (2012), 36.
15. Atman CJ, Bostrom A, Fischhoff B, Morgan MG. Designing risk communications: completing and correcting mental models of hazardous processes, Part I. Risk Anal. (1994) 14:779–88. doi: 10.1111/J.1539-6924.1994.TB00289.X
16. Kumar Paul K, Dhar-Chowdhury P, Emdad Haque C, Mohammad-Al-Amin H, Rani Goswami D, Abdullah Heel Kafi M, et al. Risk factors for the presence of dengue vector mosquitoes, and determinants of their prevalence and larval site selection in Dhaka, Bangladesh. journals.plos.org. PloS One. (2018) 13:19. doi: 10.1371/journal.pone.0199457. KK Paul, P Dhar-Chowdhury, CE Haque, HM Al-Amin, DR Goswami, MAH Kafi, MA Drebot2018•journals.plos.org.
Keywords: after action review, dengue epidemic, preparedness, response, Burkina Faso
Citation: Diao WR, Bicaba A, Sanou A and Ouattara LEP (2025) After action review: preparedness and response to the dengue epidemic in 2023 in the Centre region, Burkina Faso. Front. Trop. Dis. 6:1516101. doi: 10.3389/fitd.2025.1516101
Received: 23 October 2024; Accepted: 18 February 2025;
Published: 07 March 2025.
Edited by:
Falgunee K Parekh, EpiPointe LLC, United StatesReviewed by:
Krishnamoorthy Kaliannagounder, Vector Control Research Centre (ICMR), IndiaCopyright © 2025 Diao, Bicaba, Sanou and Ouattara. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lissy Eric Parfait Ouattara, b3VhdHRhcmFlcmljcGFyZmFpdEB5YWhvby5mcg==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.