 Humberto Ferraz1,2,3
Humberto Ferraz1,2,3 Kevan Akrami2,3,4
Kevan Akrami2,3,4 Laise de Moraes2,3Lais Cambuí Gusmão3Genevieve Coelho5Daniele Freitas5,6
Laise de Moraes2,3Lais Cambuí Gusmão3Genevieve Coelho5Daniele Freitas5,6 Manoel Barral-Netto3
Manoel Barral-Netto3 Aldina Barral3
Aldina Barral3 Viviane Boaventura2,3
Viviane Boaventura2,3 Luciane Amorim Santos2,3,6
Luciane Amorim Santos2,3,6 Ricardo Khouri2,3*
Ricardo Khouri2,3*- 1Departamento de Ciências da Vida, Curso de Medicina, Universidade do Estado da Bahia (UNEB), Salvador, BA, Brazil
- 2Departamento de Patologia e Medicina Legal, Faculdade de Medicina, Universidade Federal da Bahia (UFBA), Salvador, BA, Brazil
- 3Instituto Gonçalo Moniz (IGM), Fundação Oswaldo Cruz (FIOCRUZ), Salvador, BA, Brazil
- 4Department of Medicine, Faculty of Medicine, University of California, San Diego, San Diego, CA, United States
- 5Instituto Valenciano de Infertilidade (IVI), Salvador, BA, Brazil
- 6Departamento de Biomedicina, Escola Bahiana de Medicina e Saúde Pública (EBMSP), Salvador, BA, Brazil
Introduction: Zika virus (ZIKV) is primarily transmitted through mosquito bites though may act as a sexually transmitted infection. Men can shed the virus in their semen for extended periods, with reports indicating shedding for up to six months after the initial infection. This poses a concern for couples planning pregnancy, whether through natural or assisted methods due to the risk of congenital Zika disease. Human reproductive clinics typically perform serologic tests to screen for Zika infection.
Methods: In this study, we evaluated semen samples stored in a human reproduction clinic in Salvador, Brazil, during the Zika virus outbreak, using real-time quantitative reverse transcription polymerase chain reaction (RT-qPCR) technique.
Results: 36 sperm samples from 23 donors were analyzed, including 5 with positive IgG serology for ZIKV and all negative for IgM. Despite these serologic findings, all analyzed samples were negative by RT-qPCR ZIKV.
Discussion: Despite the limited number of samples, this study raises further concern that the use of serology may be an unreliable surrogate method to predict the presence of ZIKV in semen.
Introduction
Zika virus (ZIKV) is an RNA flavivirus with the first documented case of ZIKV infection reported in 1947 in the Zika Forest in Uganda. In 2013 an outbreak occurred in French Polynesia spreading widely throughout the world including South America (1).
While most infected people are asymptomatic, nearly 20-30% of patients may develop clinical symptoms, including fever, skin rash, arthralgia, arthritis, and conjunctivitis (1–5). Notably, neurological complications such as Guillain Barré Syndrome are life-threatening complications associated with acute infection (6). During the ZIKV outbreak in Brazil in 2015 (7), there were also numerous cases of Congenital Zika Syndrome, which is characterized by severe neurological conditions, particularly microcephaly (8).
Zika transmission typically occurs through the bite of the Aedes aegypti mosquito and through vertical transmission, though sexual transmission has been well documented. It primarily occurs from men to women with reports of infection in partners of travelers to ZIKV endemic areas (9–12). One important aspect of sexual transmission is the potential for ZIKV persistence in semen (13–15). The male genital tract provides a favorable microenvironment for viral persistence, particularly in the testis, where the blood-testis barrier confers immune privilege (15). Mathematical modeling suggests that 3-23% of Zika infections may occur through sexual transmission, even in areas with mosquito derived ZIKV infections (16–18).
Given the risk of Zika sexual transmission, guidelines have been developed for couples during reproductive planning. These recommendations include the use of condoms or abstaining from sexual activity for at least 3 months after traveling to an area with ongoing Zika virus circulation. In cases of confirmed infection or residence in a high-risk area, continuous condom use is advised for the duration of pregnancy (19, 20). In addition, ZIKV investigations in assisted fertilization clinics were implemented in endemic areas during the outbreak period (21), including testing of couples and semen donors.
The gold standard for diagnosing an ongoing ZIKV infection depends on the presence of viral RNA in blood or other body fluids (including urine, vaginal secretions, saliva, or semen) using RT-qPCR. However, serologic tests may be an alternative to molecular testing in certain situations, particularly in the later stages of infection or when there is a strong suspicion of Zika virus infection despite negative RT-PCR results (4, 19). In Brazil, only ZIKV serology tests (IgM and IgG) were incorporated into the infectious disease screening protocol for Cell and Germinative Tissue Banks, which includes testing for other infectious diseases such as HIV (Human Immunodeficiency Virus), Hepatitis B, and Hepatitis C (22).
It remains unknown whether immunoglobulin tests for ZIKV are sufficiently accurate to determine presence of prior infection and eligibility as a semen donor. The present study seeks to evaluate whether serologic tests are reliable for screening semen donors for ZIKV compared with virus screening using RT-qPCR.
Methodology
Study population
In 2019, we selected samples from a sperm bank at the Instituto Valenciano de Infertilidade (IVI), located in Salvador, Bahia, Brazil, which was the epicenter of the ZIKV outbreak in Brazil. These samples were chosen from aliquots designated for discard. 36 sperm samples were identified, originating from 23 donors. All donors resided within Bahia state. These samples were collected between 2013 and 2019, a time window that encompasses both the beginning of the epidemic period of ZIKV and the years following it in Brazil.
We analyzed socio-demographic data and serologic tests for ZIKV (IgM and IgG), performed at the time of each semen donation as part of standard screening. Cryopreserved semen samples were then tested for the presence of ZIKV using RT-qPCR. This study received approval from the ethics and research committee of the Faculdade de Medicina da Universidade Federal da Bahia, under approval number 4.409.879.
Real-time quantitative reverse transcription PCR
For the molecular diagnosis of ZIKV infection, sperm samples (200 µL) were tested. Viral RNA was initially extracted using a modified two-step protocol that involved TRIzol Reagent-based extraction, followed by a magnetic bead-based technology for further purification. Specifically, we combined 200 µL of sperm samples with 800 µL of TRIzol Reagent (Thermo Fisher Scientific, Cat. no. 15596026) and 160 µL of chloroform (Sigma-Aldrich, Cat. no. 516726), then centrifuged the mixture for 15 minutes at 12,000xg at 4°C. The resulting aqueous phase was subjected to additional purification using magnetic bead-based technology to ensure high-quality RNA extraction. This further purification was conducted using the MagMAX Viral/Pathogen II (MVP II) Nucleic Acid Isolation Kit (Thermo Fisher Scientific, Cat. no. A48383R) on the KingFisher Flex System (Thermo Fisher Scientific, Cat. no. 5400630), all according to the manufacturer’s instructions. ZIKV detection was carried out using the ZDC Molecular Kit (Instituto de Biologia Molecular do Paraná, ANVISA no. 80142170032) on a 7500 Real-Time PCR System (Applied Biosystems, Cat. no. 4351105), also following the manufacturer’s instructions.
Spiking of sperm samples for limit of detection calculations
To assess the feasibility of using RT-qPCR with sperm for ZIKV identification and to determine the minimum detectable concentration, we spiked certain semen samples with varying ZIKV dilutions. Briefly, three known ZIKV-negative sperm samples were spiked with Zika virus culture dilutions from 1:10 to 1:10,000. The virus stock solution was 3.1x108 PFU/mL and RT-qPCR was performed in all above-described dilutions, confirming the presence of ZIKV in those samples. The detection limit of the RT-qPCR test for ZIKV presence in sperm samples demonstrated the ability to detect up to a 6.2x102 PFU/extraction (Table 1).
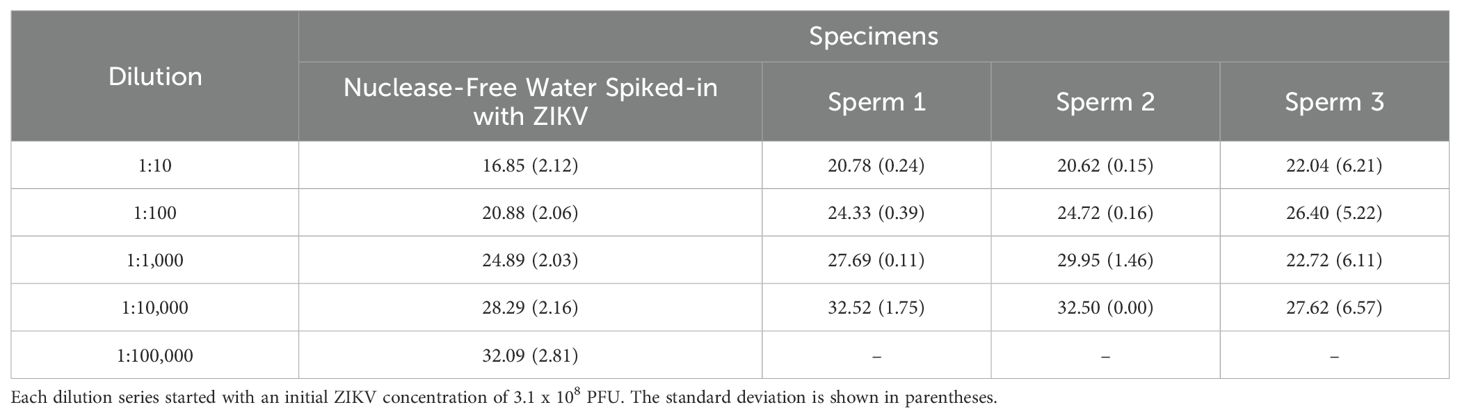
Table 1. Cq values to determine sensitivity for ZIKV detection in sperm samples.
Results
A total of 36 samples from 23 healthy donors with no arboviral-like symptoms and a median age of 31 years (IQR: 26-39), were evaluated using RT-qPCR. Four donors provided more than one sample, each collected at distinct time points (Figure 1). Ten donors were tested for both IgM and IgG antibodies against ZIKV. Among these, five tested positive and one was inconclusive for IgG anti-ZIKV. Two IgG-positive donors made four and five semen donations, respectively, during the study period. One of these donors was tested for IgG at three different time points during semen donation, yielding positive IgG results in all samples. All semen samples, whether from IgG-positive or IgG-negative donors, tested negative for ZIKV via RT-qPCR (Table 2).
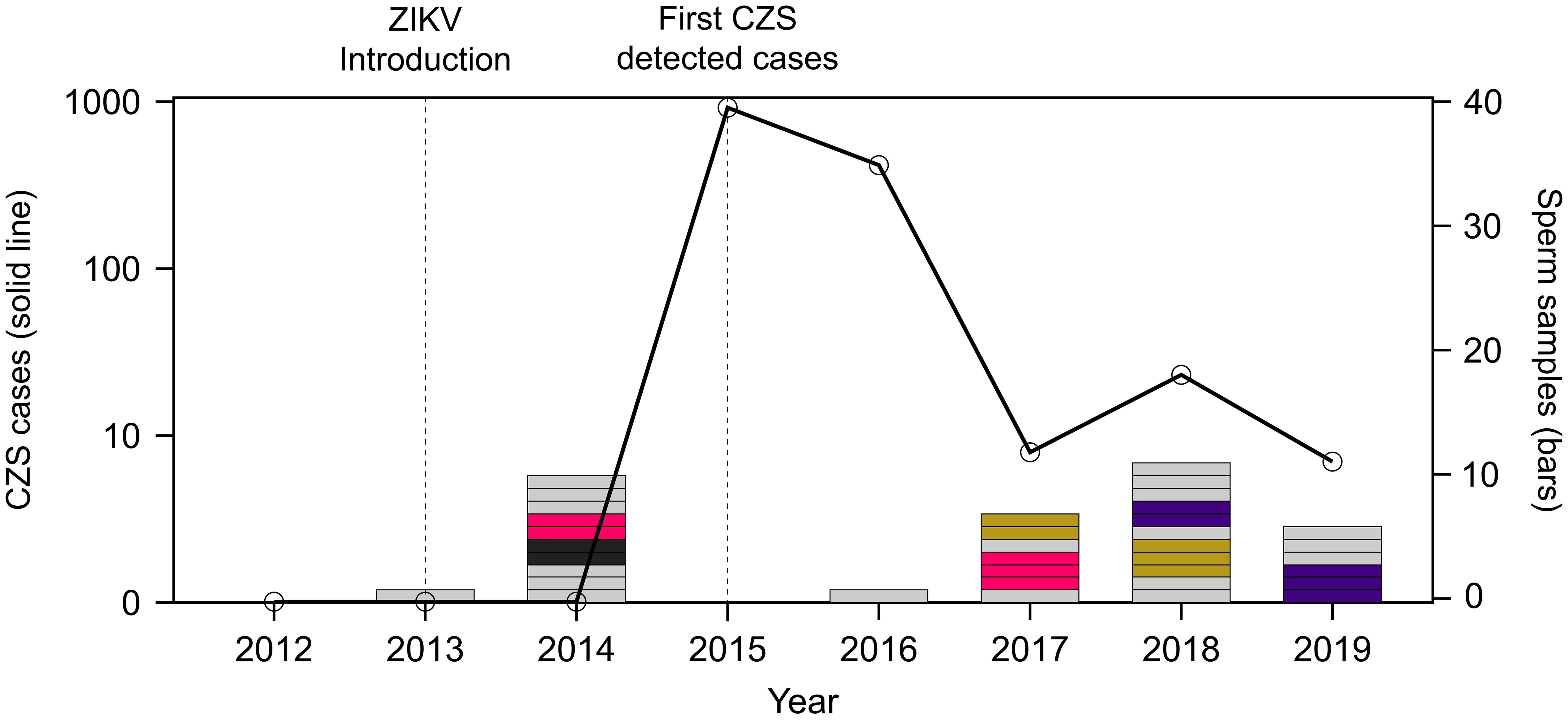
Figure 1. Semen samples distribution during the Congenital Zika Virus Syndrome (CZS) Epidemic in Northeast Brazil. The right Y-axis represents the number of confirmed CZS cases in the Northeast from 2015 to 2019 (Epidemiological Bulletin 35, Cgiae/Daent/SVS/MS). The left Y-axis shows the selected sperm samples: grey represents single samples, while pink, black, green, and purple represent serial samples from the same subjects. The introduction of ZIKV was determined by molecular dating analyses, which revealed that the virus likely entered Brazil in the second half of 2013 (7).
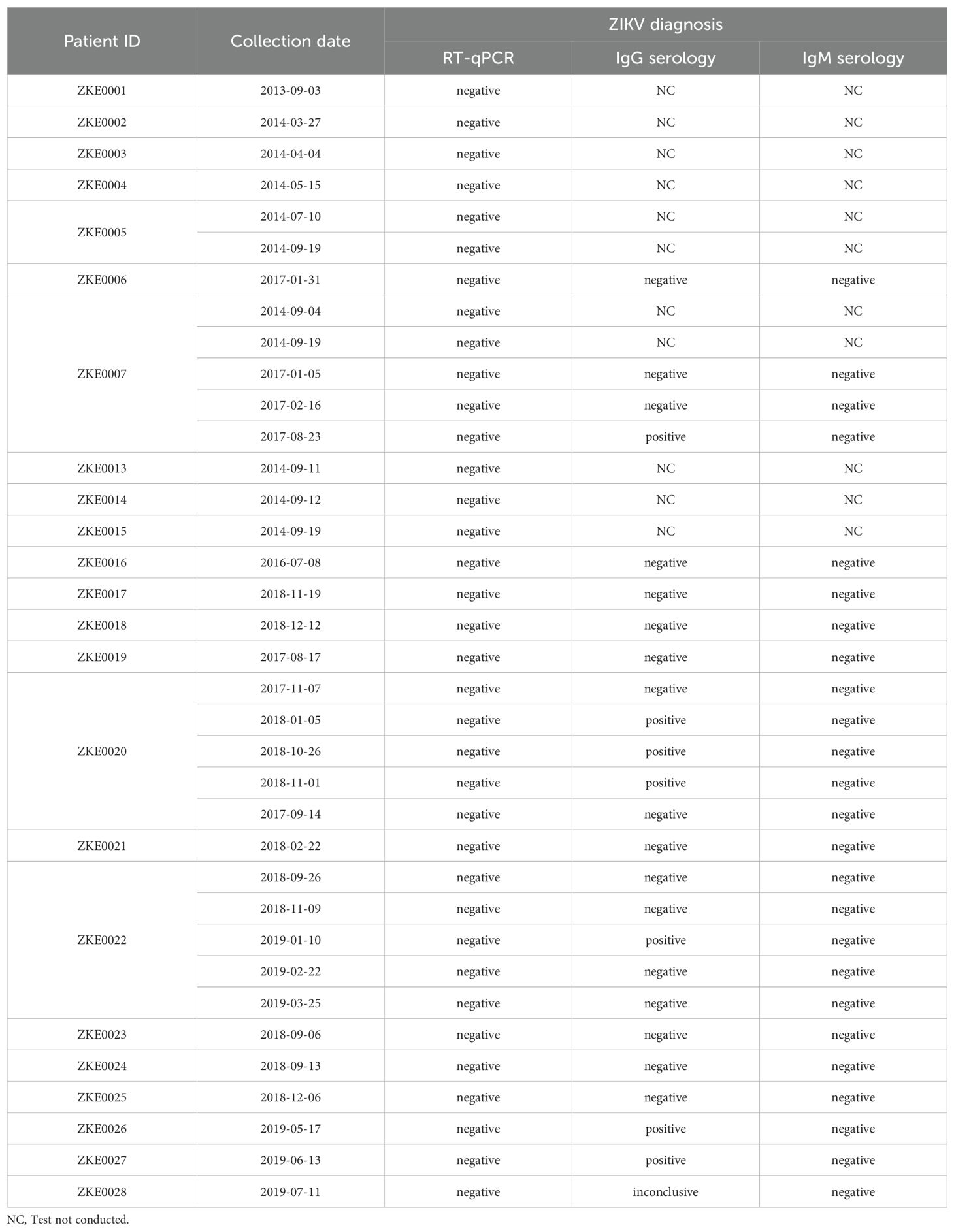
Table 2. RT-qPCR semen samples and IgG serology results of the participants.
Discussion
In this study, no positive results were observed for ZIKV through RT-qPCR in 8 semen samples from 5 individuals with IgG positive serology for ZIKV. Therefore, despite the small sample size, these findings provide additional evidence that IgG serologic testing for ZIKV may be unreliable to determine risk of sexual transmission of ZIKV, particularly within the immunological window. With confirmation of ZIKV sexual transmission through semen, protocols have been established for human reproduction clinics that rely on serologic testing for ZIKV (20, 21). In addition to the recommendations for travelers and couples of childbearing age, accurate testing is required to exclude infection and allow use of semen samples (19). Typically, candidates for assisted fertilization undergo serological testing, specifically IgM and IgG tests. RT-qPCR testing of the collected semen samples is not commonly performed, raising two important points. First, serological testing may result in false positive testing of ongoing ZIKV infection, particularly in areas with other endemic arboviruses (Dengue in particular) that may have demonstrate cross-reactivity serologically. Second, the duration and viability of ZIKV in samples from various body fluids may not correlate with serological test results.
A positive serological test for ZIKV can occur due to cross-reactivity with other flaviviruses, including Dengue virus (DENV) (23, 24). IgM typically becomes positive within two weeks after infection and persists for up to 12 weeks (about 3 months), while IgG antibodies can persist for an extended period (24). Plaque Reduction Neutralization Test (PRNT) detects IgM and IgG broad neutralizing action though may have significant cross-reactivity among viruses from same family. Both IgG and PRNT can remain positive for several years suggesting that IgM may be a better diagnostic alternative to assess risk during the ZIKV sexual transmissible window. However, many IgM tests are either highly specific with low sensitivity or highly sensitive with low specificity limiting their diagnostic accuracy. An alternative method to assess ZIKV infection in travelers that is viable would be the CDC Zika IgM MAC ELISA test (24). This test demonstrates excellent specificity and sensitivity for Zika virus diagnosis, without the risk of cross-reactivity with other arboviruses, as seen in traditional serology utilized in the current study. Nevertheless, it is a labor-intensive test requiring several days with a limited number of samples able to be tested simultaneously.
ZIKV may persist up to 6 months in the male reproductive tract and semen after serological conversion (14, 23), leading to prolonged shedding of viral particles in sperm. However, in a study by Paz-Bailey et al. (2017) (25), RT-qPCR positive results in sperm from ZIKV infected men reaches 55% in the first month, gradually decreasing thereafter with an average time for semen to test negative between 40 to 54 days (about 2 months), similar to the testing window of IgM serology. Moreover, in a study attempting to culture ZIKV in Vero cells from 78 ZIKV positive semen samples, only three samples had a positive culture. A higher likelihood of culture positivity occurred in samples collected closer to the acute stage of infection, with a higher viral load, and in individuals over 50 years of age, implying that sexual transmission might occur only during the first month (23). Additionally, further studies investigating the correlation between virus persistence in semen and IgM titers are required to evaluate the utility of IgM as a biomarker of ZIKV in semen.
The current study has several limitations, including a small sample size of semen samples analyzed, which were obtained through convenience sampling, and retrospective design. Moreover, positive IgM or IgG identified in our study by standard serology may be false positive for ZIKV given cross-reactivity with DENV and may limit interpretation of discordant serologic positive and negative RT-qPCR results. With a new outbreak of Zika infection in the future, a prospective study may determine the accuracy of different diagnostic tests (serologic PRNT and MAC-ELISA and nucleic acid testing) over a specified timeline during and after infection. This approach would aid in the development of diagnostic algorithms and evaluate their real-world reliability and cost-effectiveness for individuals of reproductive age and assisted reproduction clinics.
Several unresolved questions linger: Is it necessary to test semen samples using the RT-qPCR technique? Would serological testing alone be sufficient for a couple in which one partner has traveled to the ZIKV endemic zone? Does a positive RT-qPCR in the semen correspond to viable viruses with the potential for infection? An approach based on available data may include condom use for the first 30 days (about 4 and a half weeks) following possible ZIKV exposure. Following this period, if available, the next recommended test would be the ZIKV IgM MAC-ELISA, which can indicate a probable recent infection. If this test is positive, RT-qPCR testing of semen would be advised. Once the RT-qPCR results are negative, it would be considered safe for spontaneous or assisted contraception. For populations residing in endemic areas, where infection can be transmitted by mosquitoes at any time, routine precautions against mosquito bites must be maintained.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Faculdade de Medicina da Universidade Federal da Bahia, under approval number 4.409.879. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
HF: Conceptualization, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing, Project administration. KA: Validation, Visualization, Writing – review & editing. LdM: Data curation, Formal analysis, Methodology, Writing – original draft. LCG: Data curation, Investigation, Methodology, Writing – original draft. GC: Conceptualization, Data curation, Investigation, Writing – review & editing. DF: Data curation, Investigation, Writing – review & editing. MB: Resources, Supervision, Validation, Writing – review & editing. AB: Funding acquisition, Resources, Supervision, Visualization, Writing – review & editing. VB: Supervision, Visualization, Writing – review & editing. LAS: Formal analysis, Investigation, Validation, Visualization, Writing – review & editing. RK: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was funded by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES) [Finance Code 001], Conselho Nacional de Desenvolvimento Cientfico e Tecnológico [439967/2016-3], Programa de Excelência em Pesquisa [420765/2017-4] and Financiadora de Estudos e Projetos [MCTIC/FINEP/FNDCT 01/2016 ZIKA—0416006000]. LM received a Ph.D. scholarship from CAPES. RK, VB, AB, and MB-N are CNPq fellows. The funding organizations had no role in the study design, data collection, data interpretation, or writing of this report.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Kurscheidt FA, Mesquita CSS, Damke GMZF, Damke E, Carvalho ARB d. A, Suehiro TT, et al. Persistence and clinical relevance of Zika virus in the male genital tract. Nat Rev Urol. (2019) 16:211–30. doi: 10.1038/s41585-019-0149-7
2. Aubry M, Teissier A, Huart M, Merceron S, Vanhomwegen J, Roche C, et al. Zika virus seroprevalence, French Polynesia, 2014–2015. Emerg Infect Dis. (2017) 23:669–72. doi: 10.3201/eid2304.161549
3. Lozier MJ, Burke RM, Lopez J, Acevedo V, Amador M, Read JS, et al. Differences in prevalence of symptomatic zika virus infection, by age and sex—Puerto Rico, 2016. J Infect Dis. (2018) 217:1678–89. doi: 10.1093/infdis/jix630
5. Mansuy JM, Dutertre M, Mengelle C, Fourcade C, Marchou B, Delobel P, et al. Zika virus: High infectious viral load in semen, a new sexually transmitted pathogen? Lancet Infect Dis. (2016) 16:405. doi: 10.1016/S1473-3099(16)00138-9
6. Akrami KM, De Nogueira BMF, Do Rosário MS, De Moraes L, Cordeiro MT, Haddad R, et al. The re-emergence of Zika in Brazil in 2020: A case of Guillain Barré Syndrome during the low season for arboviral infections. J Travel Med. (2021) 27:1–2. doi: 10.1093/jtm/taaa165
7. Faria NR, Azevedo R do S da S, Kraemer MUG, Souza R, Cunha MS, Hill SC, et al. Zika virus in the Americas: Early epidemiological and genetic findings. Sci (80-). (2016) 352:345–9. doi: 10.1126/science.aaf5036
8. Moore CA, Staples JE, Dobyns WB, Pessoa A, Ventura CV, Da Fonseca EB, et al. Characterizing the pattern of anomalies in congenital zika syndrome for pediatric clinicians. JAMA Pediatr. (2017) 171:288–95. doi: 10.1001/jamapediatrics.2016.3982
9. Musso D, Roche C, Robin E, Nhan T, Teissier A, Cao-Lormeau VM. Potential sexual transmission of zika virus. Emerg Infect Dis. (2015) 21:359–61. doi: 10.3201/eid2102.141363
10. Davidson A, Slavinski S, Komoto K, Rakeman J, Weiss D. Suspected female-to-male sexual transmission of Zika virus — New York City, 2016. MMWR Morb Mortal Wkly Rep. (2016) 65:716–7. doi: 10.15585/mmwr.mm6528e2
11. Deckard DT, Chung WM, Brooks JT, Smith JC, Woldai S, Hennessey M, et al. Male-to-male sexual transmission of Zika virus — Texas, January 2016. MMWR Morb Mortal Wkly Rep. (2016) 65:372–4. doi: 10.15585/mmwr.mm6514a3
13. Nicastri E, Castilletti C, Liuzzi G, Iannetta M, Capobianchi MR, Ippolito G. Persistent detection of Zika virus RNA in semen for six months after symptom onset in a traveller returning from Haiti to Italy, February 2016. Eurosurveillance. (2016) 21:1–4. doi: 10.2807/1560-7917.ES.2016.21.32.30314
14. Joguet G, Mansuy JM, Matusali G, Hamdi S, Walschaerts M, Pavili L, et al. Effect of acute Zika virus infection on sperm and virus clearance in body fluids: a prospective observational study. Lancet Infect Dis. (2017) 17:1200–8. doi: 10.1016/S1473-3099(17)30444-9
15. Oliveira D, Durigon G, Mendes É, Ladner J, Andreata-Santos R, Araujo D, et al. Persistence and intra-host genetic evolution of Zika virus infection in symptomatic adults: A special view in the male reproductive system. Viruses. (2018) 10:615. doi: 10.3390/v10110615
16. Towers S, Brauer F, Castillo-Chavez C, Falconar AKI, Mubayi A, Romero-Vivas CME. Estimate of the reproduction number of the 2015 Zika virus outbreak in Barranquilla, Colombia, and estimation of the relative role of sexual transmission. Epidemics. (2016) 17:50–5. doi: 10.1016/j.epidem.2016.10.003
17. Gao D, Lou Y, He D, Porco TC, Kuang Y, Chowell G, et al. Prevention and control of zika as a mosquito-borne and sexually transmitted disease: a mathematical modeling analysis. Sci Rep. (2016) 6:4–13. doi: 10.1038/srep28070
18. Counotte MJ, Kim CR, Wang J, Bernstein K, Deal CD, Broutet NJN, et al. Sexual transmission of Zika virus and other flaviviruses: A living systematic review. PloS Med. (2018) 15:30–49. doi: 10.1371/journal.pmed.1002611
19. WHO. WHO guidelines for the prevention of sexual transmission of Zika virus. World Health Organization (2020). p. 84. World Health Organization, editor.
20. Polen KD, Gilboa SM, Hills S, Oduyebo T, Kohl KS, Brooks JT, et al. Update: interim guidance for preconception counseling and prevention of sexual transmission of zika virus for men with possible Zika virus exposure — United States, August 2018. MMWR Morb Mortal Wkly Rep. (2018) 67:1077–81. doi: 10.15585/mmwr.mm6731e2
21. Borges ED, Vireque AA, Berteli TS, Ferreira CR, Silva AS, Navarro PA. An update on the aspects of Zika virus infection on male reproductive system. J Assist Reprod Genet. (2019) 36:1339–49. doi: 10.1007/s10815-019-01493-y
23. Mead PS, Duggal NK, Hook SA, Delorey M, Fischer M, Olzenak McGuire D, et al. Zika virus shedding in semen of symptomatic infected men. N Engl J Med. (2018) 378:1377–85. doi: 10.1056/NEJMoa1711038
24. MaChado Portilho M, de Moraes L, Kikuti M, Jacob Nascimento LC, Galvão Reis M, Sampaio Boaventura V, et al. Accuracy of the Zika IgM antibody capture enzyme-linked immunosorbent assay from the centers for disease control and prevention (CDC Zika MAC-ELISA) for diagnosis of Zika virus infection. Diagnostics. (2020) 10:835. doi: 10.3390/diagnostics10100835
Keywords: Zika virus, semen, genital tract, sexual transmission, diagnosis
Citation: Ferraz H, Akrami K, de Moraes L, Gusmão LC, Coelho G, Freitas D, Barral-Netto M, Barral A, Boaventura V, Santos LA and Khouri R (2025) Screening semen samples for Zika virus infection: role for serologic and RT-PCR testing. Front. Trop. Dis. 5:1489647. doi: 10.3389/fitd.2024.1489647
Received: 02 September 2024; Accepted: 23 December 2024;
Published: 29 January 2025.
Edited by:
Ramesh C. Dhiman, National Institute of Malaria Research (ICMR), IndiaReviewed by:
Andréa Nazaré Monteiro Rangel Da Silva, Federal University of Pará, BrazilMadhuri Namekar, University of Hawaii at Manoa, United States
Copyright © 2025 Ferraz, Akrami, de Moraes, Gusmão, Coelho, Freitas, Barral-Netto, Barral, Boaventura, Santos and Khouri. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ricardo Khouri, cmljYXJkby5raG91cmlAZmlvY3J1ei5icg==