
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Trop. Dis. , 18 February 2025
Sec. Neglected Tropical Diseases
Volume 5 - 2024 | https://doi.org/10.3389/fitd.2024.1469201
 Jurel Payii Mamur1†
Jurel Payii Mamur1† Gilles Van Cutsem2,3,4*†
Gilles Van Cutsem2,3,4*† Sekonjo Juliano Hamid Motto1
Sekonjo Juliano Hamid Motto1 Stephen Raimon Jada5Tatjana Gerber5Yak Yak Bol6
Stephen Raimon Jada5Tatjana Gerber5Yak Yak Bol6 Joseph Nelson Siewe Fodjo7
Joseph Nelson Siewe Fodjo7 Robert Colebunders7,8
Robert Colebunders7,8Background: High epilepsy prevalence and mortality has been reported in onchocerciasis-endemic areas with suboptimal elimination programs in South Sudan. In Deim Zubeir, an onchocerciasis-endemic area in Western Bahr El Ghazal state, demand for antiseizure medication is high, but epilepsy prevalence has never been investigated.
Methods: A two-step household survey was conducted in four locations in Deim Zubeir over two weeks in July 2023. Trained local community volunteers screened household members for epilepsy using four screening questions, assessed blindness, and inquired about family members’ deaths in the past three years. Participants with suspected epilepsy were referred to a medical doctor for confirmation of the diagnosis.
Results: A total of 7,807 individuals in 1,803 households participated in the survey; 180 (2.3%) had epilepsy and 146 (1.9%) were blind in at least one eye. The point prevalence of active epilepsy was 23.1 (95% confidence interval [CI] 20.0-26.6) per 1,000 persons. The median age of persons with epilepsy (PWE) was 25 (interquartile range [IQR] 20-31.5) years; median age at onset of seizures was 14 (IQR 9-19) years; 36.4% of PWE had siblings with a history of seizures; 5.3% were blind in at least one eye; 40.7% had burn lesions and 24.7% had skin lesions compatible with onchocerciasis; 55% met the criteria for onchocerciasis-associated epilepsy (OAE). The mortality rate of PWE was 182.4 per 100,000 person-years (95%CI 132.8-232.0) and the epilepsy case fatality rate was 64.1 (95% CI 47.2-80.9) per 1,000 PWE per year. PWE were six times more likely to die within one year than people without epilepsy. Their median age of death was 21.5 (IQR 16-34) years compared to 41 (IQR 7-60) years for people without epilepsy.
Conclusion: The prevalence of epilepsy and epilepsy-related mortality in Deim Zubeir is high, likely because of ongoing Onchocerca volvulus transmission. Strengthening the local onchocerciasis elimination program and ensuring consistent access to epilepsy care is urgently needed to prevent OAE and epilepsy-related mortality and morbidity. It is necessary to increase advocacy and funding to ensure early identification of epilepsy and uninterrupted, free access to antiseizure medication for PWE in this remote, impoverished area.
Epilepsy affects more than fifty million people globally. Nearly 80% of people with epilepsy (PWE) live in low- and middle-income countries, where rates of epilepsy prevalence and incidence are higher than in high-income countries (1) and less than one in four PWE has access to adequate care (1, 2). In Africa, the prevalence of epilepsy is estimated to be between 0.5 to 10%, with higher rates in rural areas compared to urban areas (1). There is an important epilepsy diagnosis and treatment gap, leading to a high mortality and case fatality rate (3). Disability-adjusted life years (DALYs) attributed to epilepsy in Africa were estimated at 3.9 million DALYs in 2017 (4).
The only published data on epilepsy in South Sudan are from onchocerciasis-endemic areas in the Western Equatoria state (5–12), and more recently from the Lakes state (13). A significant proportion of epilepsy in these states was found to be associated with onchocerciasis (5–10). There is no data on epilepsy in the area of Deim Zubeir in the Western Bahr El Ghazal state.
Onchocerciasis, a neglected tropical disease caused by the nematode Onchocerca volvulus, remains a major health burden worldwide (14). The Global Burden of Disease Study estimated that in 2017 at least 220 million people were in need of preventive chemotherapy against onchocerciasis, 14.6 million presented with skin disease, and 1.15 million with loss of vision (15). More than 99% of those infected live in African countries, including South Sudan (14). South Sudan is highly endemic with almost 49% of the country affected (16), mostly Western Equatoria, followed by Northern and Western Bahr El Ghazal. Deim Zubeir in Raga County is an onchocerciasis endemic area in Western Bahr El Ghazal State.
Onchocerciasis is known to induce skin and eye disease (17). Increasing epidemiological evidence suggests that onchocerciasis can also induce epilepsy (18–20). A high prevalence of epilepsy was observed in several onchocerciasis-endemic areas in South Sudan, e.g. in Maridi (6), Mundri East and West (21) and Mvolo (10). Many people with epilepsy in these areas present with the characteristics of onchocerciasis-associated epilepsy (OAE) (5, 22). The first seizures in persons with OAE usually occur in previously healthy children between the ages of 3-18 years with no other obvious cause of epilepsy (5, 22, 23). Onchocerciasis-associated epilepsy includes a wide spectrum of seizure types (24, 25). Nodding and Nakalanga syndromes are two phenotypic severe forms of OAE observed only in areas with very high ongoing or past O. volvulus transmission, and mainly in households living close to blackfly breeding sites (20, 26). Nodding syndrome is characterized by head nodding seizures often during periods of reduced consciousness and frequently accompanied by cognitive impairment (26–28). Nakalanga syndrome presents with growth retardation, delayed secondary sexual development, often with morphological deformities and seizures (25, 29).
Recent retrospective (30–32) and prospective (8, 9, 33) population-based studies showed that strengthening onchocerciasis elimination programs decreased the incidence of OAE. The main strategy for onchocerciasis elimination is Community-Directed Treatment with Ivermectin (CDTI) (34, 35). However, ivermectin only eliminates microfilaria in the skin and only temporarily sterilizes female adult worms without killing them (35). Consequently, to eliminate onchocerciasis, mass drug administration with ivermectin needs to be given for at least 15 years, the lifespan of the adult worms (14), and with a CDTI coverage of at least 80% of people in the targeted community (36). People who develop epilepsy (whether OAE or other forms of epilepsy) will often require lifelong treatment with antiseizure medications.
Deim Zubeir is known as an onchocerciasis-endemic area with a high number of PWE and blindness, but a prevalence survey had never been done1. During a health assessment by the Health Department of the Catholic Diocese of Wau in 2021, many parishes in Deim Zubeir reported a high number of PWE. During meetings with PWE, a high level of stigma and discrimination was reported; about half of the PWE had been chased away from their family homes due to the misconception that epilepsy is contagious, and some mentioned that they feared to go to public places, including attending health facilities, because of stigma. In 2017, the parish priest of Deim Zubeir convinced the Catholic health facilities to provide him with antiseizure medication and to give him guidance on the management of epilepsy. In 2017, the first 30 PWE received antiseizure medication in Deim Zubeir.
In this study, we describe the results of a population-based epilepsy prevalence survey conducted in Deim Zubeir in July 2023, in prelude to the implementation of preventive and treatment actions for PWE in that area.
Deim Zubeir and the nearby villages of Abul, Sopo, and Kuru are located within Raga (also known as Raja) County, 200 km West from Wau, the capital of Western Bahr el Ghazal. The study sites are close to the border with the Central African Republic, and near the Biri tributary of the River Chel (Figures 1, 2). This remote area has been plagued by conflicts, and access to healthcare, education, clean water, and infrastructure is limited. CDTI and bed nets are irregularly provided by the government.
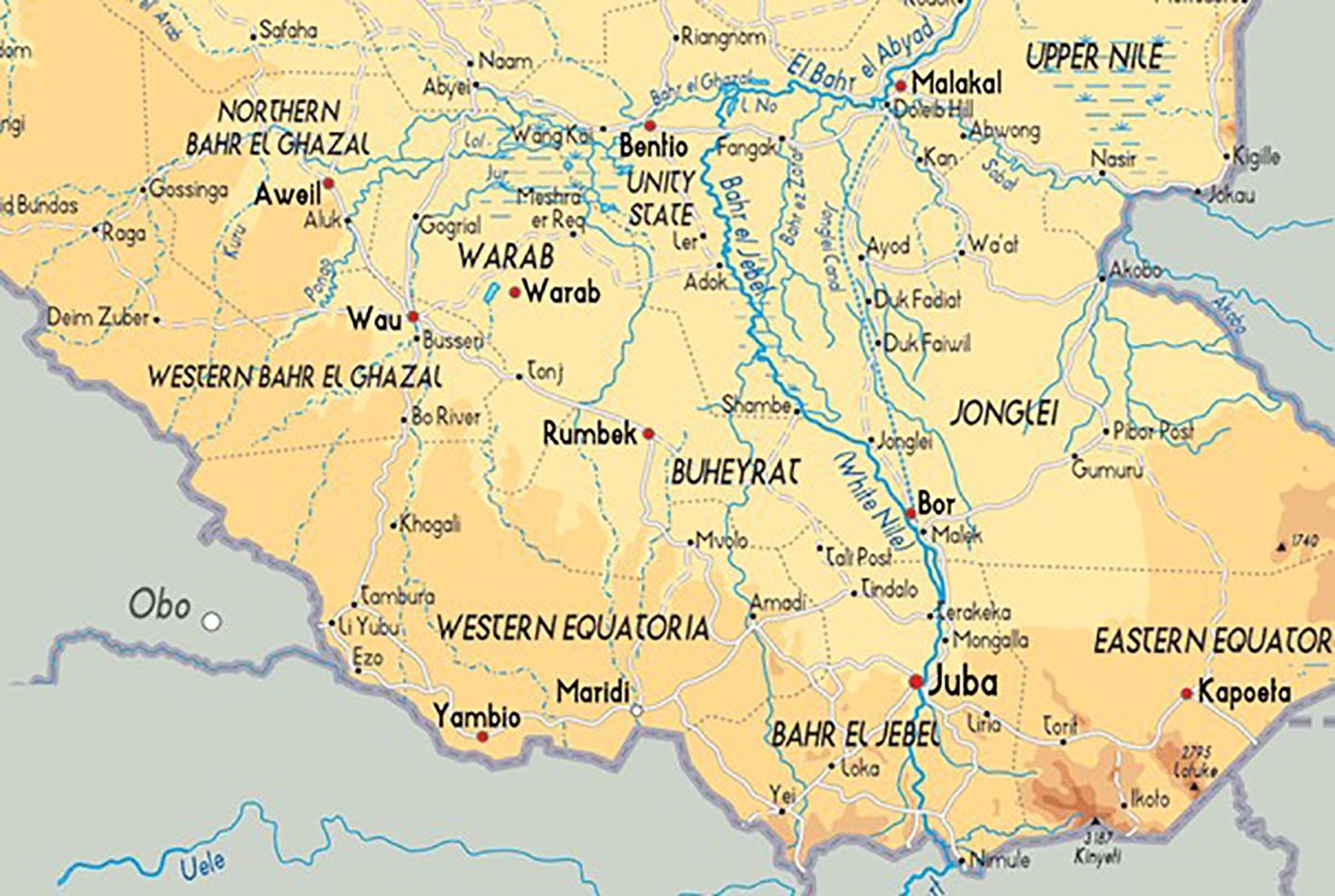
Figure 1. Map of South Sudan showing the location of Deim Zubeir.

Figure 2. Map of Deim Zubeir area.
Western Bahr el Ghazal is located at 626.9 meters above sea level and has a tropical savannah climate (37). The annual average temperature is 29 degrees Celsius and annual average precipitation is 105 millimeters, with 138 rainy days per year. Raga County had an estimated population of 59,638 in 2022, of which 34,200 had humanitarian needs (38). During the latest census in 2008, 42% of the population was 0-14 years, 55% was 15-64 and 2% was above 65 years (39). Primary economic activities include subsistence farming, hunting, and fishing, as well as firewood and charcoal making (40).
PWE relied solely on traditional medicine until 2017, when the parish priest started providing antiseizure medication. Between June 2022 and May 2023 an epilepsy health unit was established with a trained community registered nurse, and guidance of a medical officer. This survey was conducted as part of a project to provide better care and treatment for PWE.
We conducted a two-step, cross-sectional, population-based survey over a two-week period in July 2023 in Deim Zubeir, Abul, Sopo and Kuru, to estimate the prevalence of epilepsy. The first step was a door-to-door household survey by trained community volunteers to identify persons suspected to have epilepsy. All households in the study sites were visited for this screening phase. In a second step persons with suspected epilepsy were interviewed to obtain an in-depth medical history and underwent clinical examination by a clinician. A similar methodology has been used in other onchocerciasis-endemic areas in Western Equatoria, South Sudan (5–10).
To prepare the survey, meetings were held with local chiefs, traditional healers, and the local authorities in the four villages, in the presence of the Health Advisor of the Catholic Diocese of Wau, the Public Health Officer, and the parish priest. Epilepsy awareness sessions were organized in public places to sensitize local communities about epilepsy, and to explain the importance to obtain reliable data about the prevalence of epilepsy in their community.
For the household survey, volunteers recruited from the community were trained on epilepsy and its causes, signs, symptoms, treatment options, and how to administer the survey questionnaire (Supplementary Material 1). The volunteers undertook door-to-door screening for epilepsy in all the households of the four sites. Upon obtaining informed consent, all household members provided information on age, sex, household ethnicity, household occupation, household residency status, bed net use and household contact with animals. They then answered four epilepsy screening questions adapted from a questionnaire that was initially validated in Mauritania (41) and later used in many African countries, including South Sudan (6). Household members were also questioned about ivermectin intake during the most recent CDTI round in 2022. If a family member was unavailable during the interview, information pertaining to them was sought from another family member present. Suspected epilepsy was defined as a positive response to any of the four epilepsy screening questions. Participants were also screened for blindness and asked about family members who died during the last three years, and whether this deceased person had epilepsy. Data were collected on paper forms. Suspected cases were referred to the epilepsy health unit to be consulted by a medical doctor.
In the second step, a medical doctor reviewed the diagnosis of epilepsy of the individuals with suspected epilepsy by taking a detailed medical history and conducting a clinical examination, which included screening for onchocerciasis skin lesions and vision assessment. The clinician completed an “epilepsy confirmation questionnaire” (Supplementary Material 1) which contained additional questions on clinical signs of onchocerciasis, namely blindness and onchocerciasis-associated skin lesions, as well as potential causes of epilepsy, cognitive impairment, frequency, and types of seizures, Nakalanga features, and prior intake of ivermectin and antiseizure medication.
After the study, a community registered nurse continued to provide antiseizure medication and follow-up care for the identified PWE.
A case of confirmed epilepsy was defined according to the International League against Epilepsy as an individual with at least two unprovoked seizures with a minimum of 24 hours separating the two episodes (42).
A person was considered to meet the OAE criteria if the following six criteria were satisfied (23): 1. A history of two or more unprovoked epileptic seizures occurring at least 24 hours apart; 2. Living in an onchocerciasis-endemic region for at least three years; 3. Living in a village with a high prevalence of epilepsy and with families having more than one child with epilepsy; 4. No other obvious cause of epilepsy; 5. Onset of seizures in childhood or adolescence (between the ages of 3 to 18 years); 6. Normal neurological development before the onset of epilepsy.
The following skin lesions were considered compatible with onchocerciasis: nodules, itching, papular or nodular pruritic skin, leopard skin, and dry, thickened, wrinkled skin (lizard skin).
The following features were considered as part of the Nakalanga syndrome: growth retardation, thoracic or spinal abnormalities, and delay in sexual maturation.
Blindness was defined as the inability to discern the five fingers of a hand.
Mortality rate of PWE refers to the number of PWE who died from any cause within one year divided by the total person-years in the entire population. It is expressed as PWE deaths per 100,000 person-years.
Epilepsy case fatality rate refers to the proportion of PWE who died within one year. It is expressed as number of deaths per 1000 PWE per year.
We summarized continuous variables with medians and interquartile ranges (IQRs) and categorical variables with percentages (%) and 95% confidence intervals (CI). Crude estimates of the prevalence of lifetime epilepsy were calculated by dividing the total number of confirmed cases by the total population screened, reported as the number of PWE per 1,000 people screened. The crude annual mortality rate in the population and of PWE was estimated by dividing the number of deaths by the sum of all participants and deaths, divided by 3.5 years (January to July 2023 plus the three years before). This simplified calculation for mortality rate assumed a stable population size during the 3.5-year period being studied. The epilepsy case fatality rate was estimated by dividing the number of PWE who died by the sum of the participants with epilepsy (including those who died during the reported period); this was then divided by 3.5 years to obtain an annual rate. Annual CDTI coverage, was calculated by dividing the number of individuals who reported receiving ivermectin during the last CDTI round by the total population that was surveyed. Data were analyzed with Stata/MP version 17.0 (StataCorp LLC).
Ethical approval was obtained from the ethics committee of the Ministry of Health of South Sudan (January 2018, MOH/ERB50/2019) and from the ethics committee of the Antwerp University Hospital, Belgium (April 2019, B300201940004). Community engagement meetings were organized before the start of the survey. Written informed consents were obtained from the head of households and PWE and carers who participated in the study. For children up to 11 years of age, the parents/caretakers provided consent, while adolescents between the ages of 12-17 years provided assent before parental consent.
A total of 7,807 individuals in 1,803 households were included in the household survey; 3,981 (51%) were female; median age was 15 (IQR 6-30) years. Most (1,051, 58.3%) households were visited in the rural town of Deim Zubeir; the remainder in the nearby villages of Sopo (316, 17.5%), Kuru (275, 15.3%), and Abul (161, 8.9%). Households belonged to the following main ethnic groups: Balanda (464, 25.7%), Thuri (406, 22.5%), Chat (233, 12.9%), Banda (130, 7.2%), Kresh (90, 5%), Zande (67, 3.7%), and Dinka (27, 1.5%). Around one tenth of the households (183/1803) were not originally from the village where they were interviewed. Farming was the income generating activity of the large majority (1,788, 99.2%) of households. Most households (1,741, 96.6%) had poultry, and less than 1% had goats or cattle; none had pigs. Only 23.3% (420/1803) of homes had bed nets.
After detailed history taking and examination, a physician confirmed the diagnosis of epilepsy in 180 (2.3%) of the 7,807 surveyed participants. The point prevalence of active epilepsy was therefore 23.1 (95% CI 20.0-26.6) per 1,000 persons. The sex-specific epilepsy prevalence was similar in males and females (Table 1). The median age of PWE was 25 (IQR 20-31.5) years compared to 14.5 (IQR 6-30) years for those without epilepsy. The highest prevalence of epilepsy was among the 21-25 years age group (Figure 3).
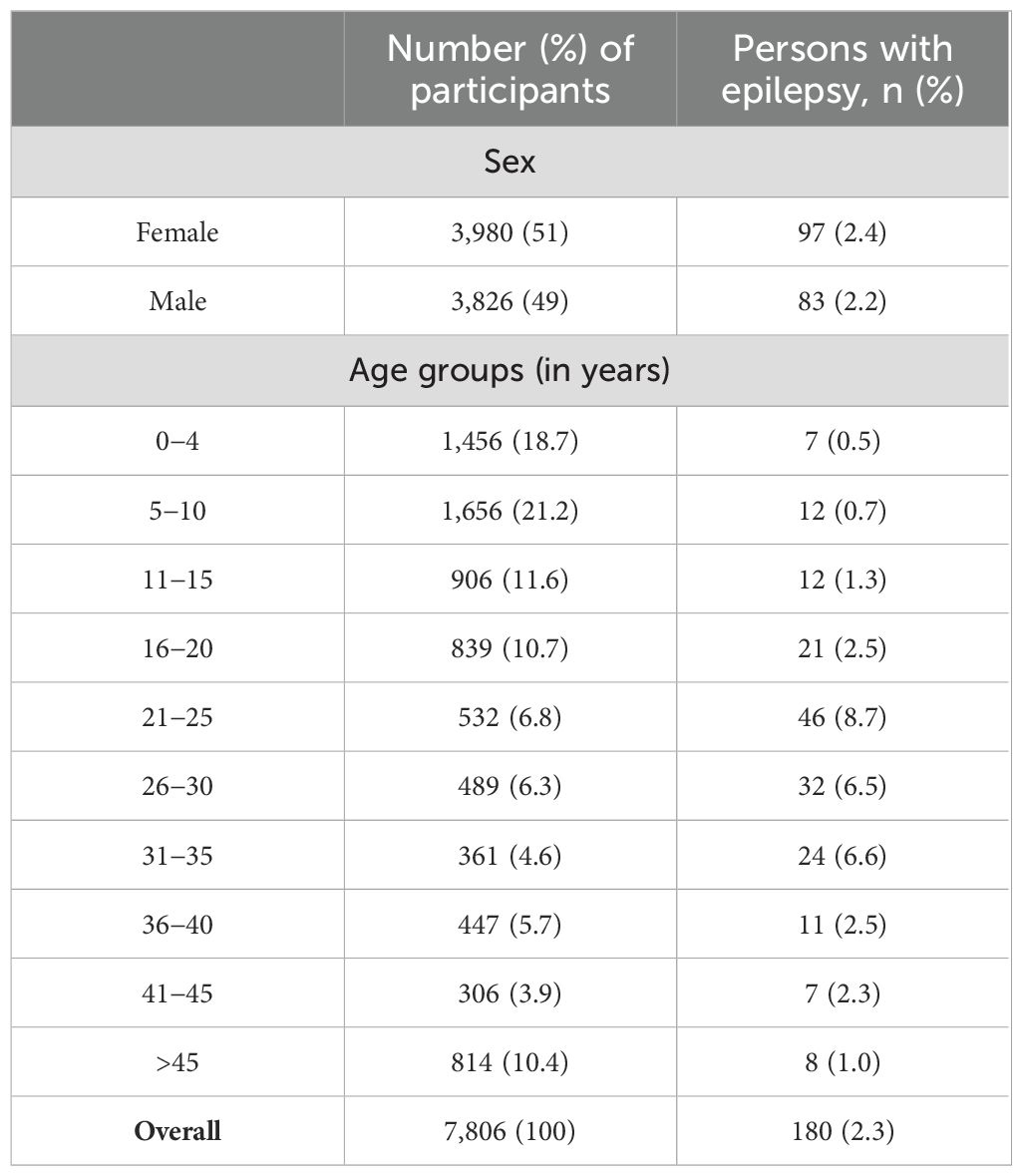
Table 1. Prevalence of epilepsy by sex and age group.
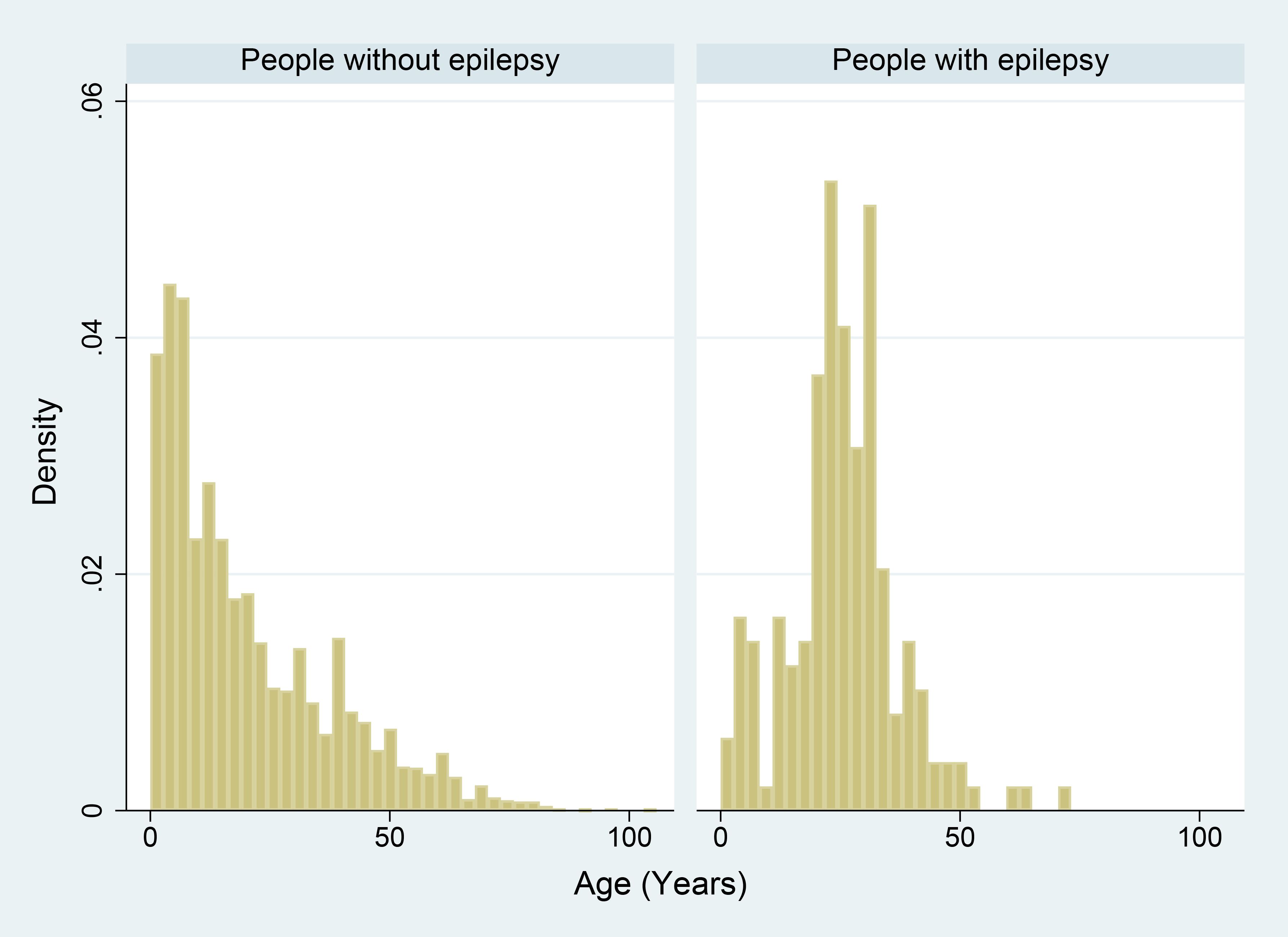
Figure 3. Age distribution among people without and with epilepsy.
The prevalence of epilepsy was the highest (3.0%) in Deim Zubeir, while the prevalence of blindness was highest in Abul village (Table 2). Overall, blindness was reported by 1.9% (146/7,807) of participants; 61 (1.5%) women and 85 (2.2%) men; 44 (0.6%) were blind in one eye and 102 (1.3%) in both eyes.
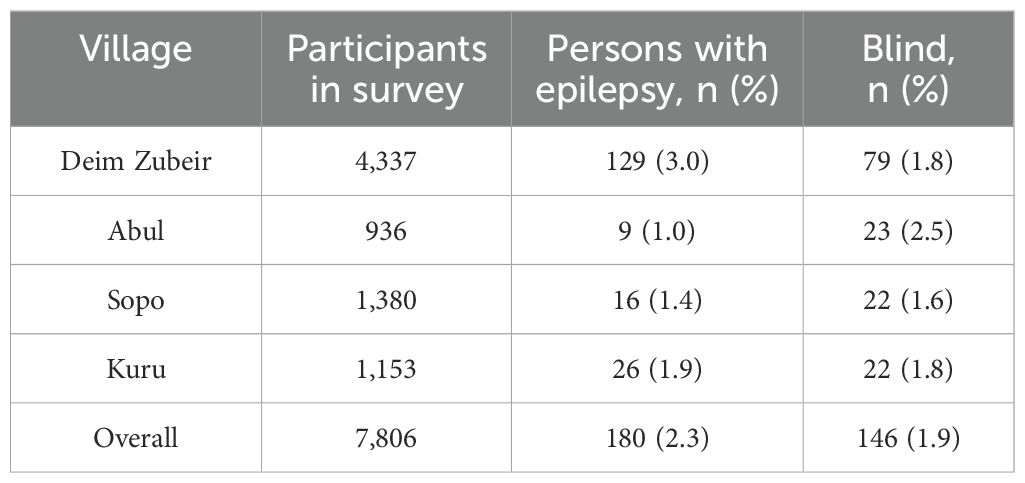
Table 2. Prevalence of epilepsy and blindness by village.
The characteristics of 169 PWE for whom a detailed clinical questionnaire was available are summarized in Tables 3, 4. The median age was 27 years (IQR 20.5-34) and the median age at onset of seizures was 14 (IQR 9-19) years. A wide range of seizure-related symptoms was reported. Most PWE reported loss of bladder control, foaming at the mouth, loss of consciousness and/or generalized seizures, and/or head movements during seizures. Episodes of loss of contact for a few minutes was reported in 53.0% (89/168), behavioural changes in 95.8% (161/168), hallucinations in 73.4% (124/169) and unilateral tingling in 25.8% (43/167). Almost half of the PWE had a family history of seizures, and more than one third had a sibling with seizures. The majority exhibited normal growth (91.1%) and normal learning (82.0%) prior to seizure onset. Severe disease preceding seizures was reported by 6.5% (11/169) of participants. On physical examination, 5.3% were blind in at least one eye (compared to 1.9% in all participants), almost 15% had one or more characteristics of Nakalanga syndrome (growth retardation, delayed sexual maturation, and/or thoracic abnormalities), 40.7% (68/167) had burn lesions and 24.7% (41/166) had skin lesions compatible with onchocerciasis. Nearly all (99.4%) PWE had taken carbamazepine intermittently, provided through the parish priest. Lifetime exposure to ivermectin was 88.2% (149/169), and 84.0% (142/169) had received ivermectin in 2022, the year preceding the survey.
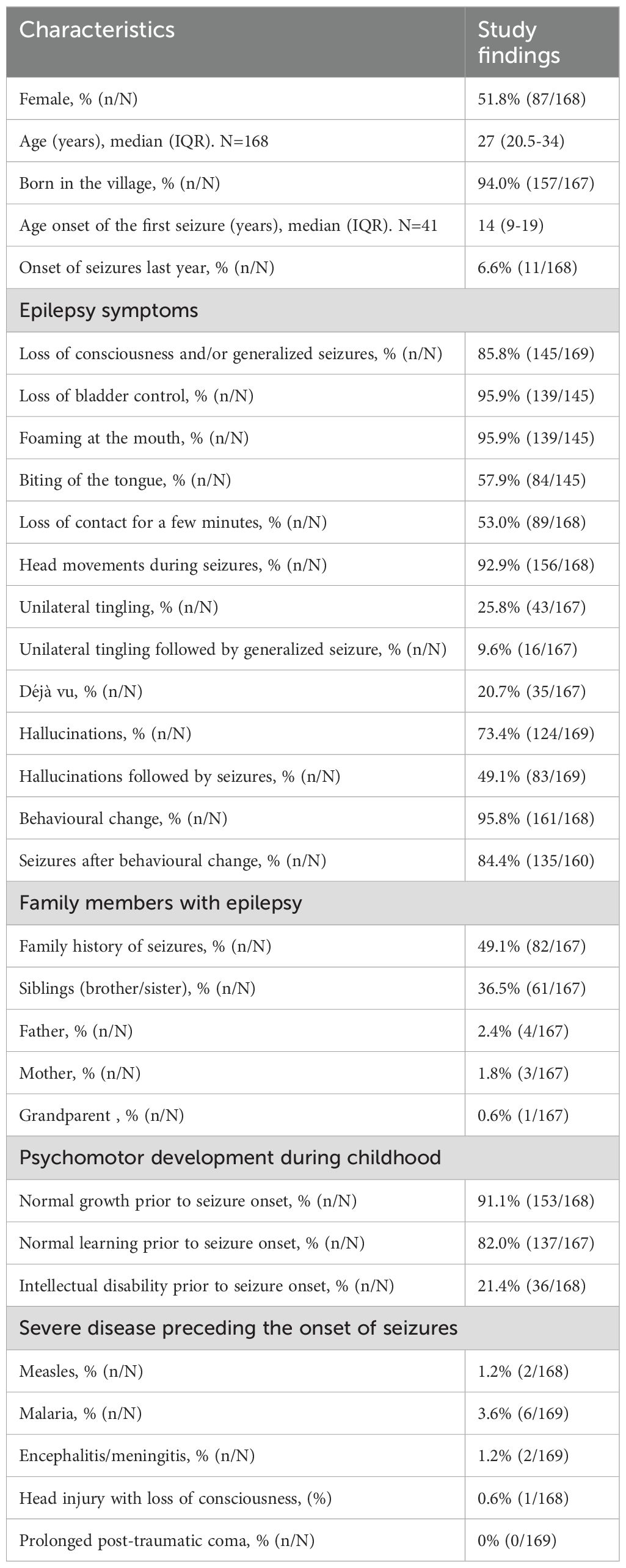
Table 3. Characteristics of persons with epilepsy.
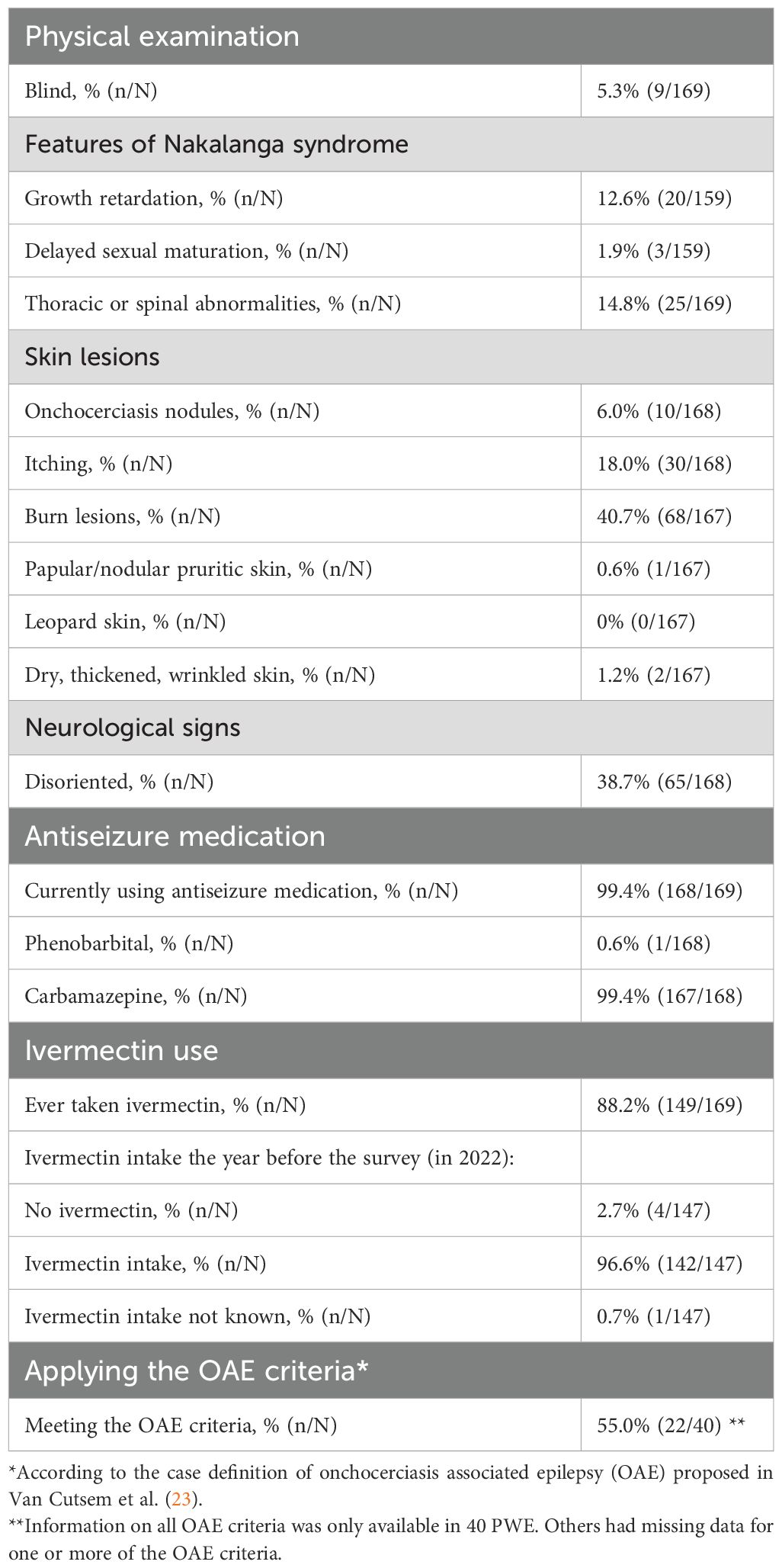
Table 4. Clinical examination and medication use of persons with epilepsy.
Surveyed households reported 338 deaths in the last 42 months, of which 52 (15.4%) were known to have epilepsy.
The crude annual mortality rate (for persons with and without epilepsy) was 11.9 per 1,000 persons per year (95% CI 10.6-13.1). Out of an estimated 232 PWE (180 PWE found during the survey + 52 who died with epilepsy during the 3.5 years before), 52 (22.4%) died during the 3.5 years preceding the household visit. The mortality rate of PWE was 182.4 per 100,000 person-years (95%CI 132.8-232.0). The epilepsy case fatality rate was 64.1 deaths per 1,000 PWE per year (95% CI 47.2-80.9), compared to a mortality rate of 10.3 (95% CI 9.1-11.5) deaths per 1,000 person-years among persons without epilepsy. PWE were more than six times more likely to die within one year than people without epilepsy (relative mortality risk among PWE = 6.2).
The overall median age of death was 38 years (IQR 11-60): 21.5 years (IQR 16-34) for PWE and 41 years (IQR 7-60) for people without epilepsy.
The proportion of deceased persons who were reported to have epilepsy was 51.3% (20/39) in Sopo, 16.1% (5/31) in Abul, 10.6% (22/207) in Deim Zubeir, and 8.2% (5/61) in Kuru.
Slightly more than half of the survey population (52.1%, 4069/7807) had received ivermectin in 2022, compared to 84.0% (142/169) of PWE (p<0.001).
While current estimates suggest an important burden of OAE in many South Sudanese villages, a prevalence survey had never been conducted in Deim Zubeir, a remote, onchocerciasis-endemic area of South Sudan where a high number of patients with epilepsy has been reported. This paper presents the results of the first epilepsy household survey conducted in Deim Zubeir to the best of our knowledge, with the aim to estimate the prevalence of epilepsy in that area.
This household survey documents the very important burden of epilepsy in Deim Zubeir and surrounding villages. A high prevalence of epilepsy and blindness, a high epilepsy mortality rate, and a high epilepsy case-fatality rate were documented. The crude mortality rate for the entire population was 11.9 per 1,000 persons per year, very similar to the World Bank estimate of 11.05 for South Sudan in 2021 (43). PWE were more than six times more likely to die and did so at a much younger age (21 vs 41 years) compared to those without epilepsy. The prevalence of epilepsy was highest among young adults, blindness was three times higher among PWE compared to people without epilepsy; more than one third of PWE had siblings with epilepsy, and a quarter had skin lesions compatible with onchocerciasis, a pattern that is typical of OAE (21).
Our study confirms the strong epidemiological link between onchocerciasis and epilepsy. However, the pathogenesis of OAE still remains to be elucidated. Several pathophysiological mechanisms were proposed but remain unproven (20). Before the widespread use of ivermectin, microfilariae have been identified in the cerebrospinal fluid (CSF) of persons with onchocerciasis without epilepsy (44). In more recent studies, neither microfilariae nor O. volvulus DNA was detected in CSF but CSF was obtained many years after the onset of seizures (45–47). Therefore, it is possible that parasites had already been eliminated by the central nervous system immune system. One of the hypotheses for OAE-inducing mechanisms is immune mediated inflammation (46). Parasitic tolerance in children exposed to filariae in utero is another potential co-factor (48). Recently, a virus associated with O. volvulus, Onchocerca volvulus RNA virus 1 (OVRV1), was found to elicit antibody responses from infected or exposed humans (49). However, it is not known whether OVRV1 plays a role in the pathophysiology of OAE.
In a large, recent meta-analysis, the prevalence of active epilepsy in Africa was estimated at 9 per 1,000 persons (95% CI 8.0-9.9 per 1,000 persons) with wide regional variations, peaking at 30.2 per 1,000 persons (95%CI 6.2 to 66.7) in the Central Africa subregion (50). Our estimate of 23.1 per 1,000 persons is in line with this figure.
In another systematic review, the epilepsy mortality rate and case fatality rate in Africa were estimated at 342.9 per 100,000 person-years and 57.0 per 1,000 PWE in onchocerciasis high-risk sites, compared to 10.0 per 100,000 person-years and 26.6 per 1,000 PWE in non-onchocerciasis endemic sites (3). The estimated mortality rate in Deim Zubeir of 182.4 per 100,000 person-years and epilepsy case fatality rate of 64.1 deaths per 1,000 PWE are comparable with mortality rates observed in other onchocerciasis endemic areas.
Only about half of the study population took ivermectin during the last CDTI round in 2022, a proportion that is insufficient to control ongoing O. volvulus transmission (51). However, significantly more PWE took ivermectin treatment compared to the general population, with over 80% coverage in this group. This could be related to the fact that ivermectin treatment has been associated with fewer seizures (52–54); hence PWE may be more likely to take ivermectin to reduce their seizure frequency and not necessarily for onchocerciasis elimination purposes.
Similar high prevalence and mortality of epilepsy were observed in other onchocerciasis-endemic areas in Western Equatoria, South Sudan. In two large surveys in Mvolo, the prevalence of epilepsy was 51.4 per 1,000 persons in 2020 and 44.5 per 1,000 persons in 2022; 3% were blind; the median age of those with epilepsy was 20 years; 82.8% met the criteria for OAE in 2022; less than one third had taken ivermectin the year before, and only 23% were receiving antiseizure medication (9). In Maridi, the prevalence of epilepsy was 44 per 1,000 persons (6) and 85% fulfilled the OAE criteria (5); median age of PWE was 18 years; 40.8% took ivermectin the year before (5). Our study also documented a very high epilepsy case fatality rate of 64.1 per 1,000 PWE per year. This is comparable with the 62.9 per 1,000 mortality among PWE documented in Maridi (6). Slightly higher epilepsy fatality rates was found in the Wulu County (Lakes State), where it was estimated at 70.3 per 1000 PWE (13). The high epilepsy related mortality in our study and other onchocerciasis-endemic areas in South Sudan is explained by the high epilepsy prevalence and the lack of access to uninterrupted antiseizure medication in the area. The relatively low epilepsy prevalence in Deim Zubeir contrasts with this high epilepsy related mortality. Most likely because of epilepsy-related stigma, epilepsy-related symptoms were not reported in certain households and therefore the epilepsy prevalence has been underestimated. The high epilepsy mortality in onchocerciasis endemic regions with high O. volvulus transmission compared to the epilepsy mortality in most non-onchocerciasis endemic areas in Africa (3) is explained, at least in part, by the lack of access to adequate epilepsy care in these remote poor onchocerciasis endemic areas without health infrastructure, often affected by insecurity. Additionally, It was observed that persons with OAE and notably the nodding syndrome, are prone to more severe forms of epilepsy which may also worsen their prognosis (26).
Our study has several limitations, in addition to the potential for misclassification and recall bias, which are inherent to questionnaire-based household surveys. First, the diagnosis of epilepsy was not confirmed by a neurologist. The prevalence of nodding syndrome could not be determined. Head movements during seizures were described by 92.8% of family members. However, to consider these movements as head nodding seizures they should be between 5-20 head movements per minute (23). Most likely many of these head movements were part of generalized seizures. We did not perform any laboratory/imaging analysis to confirm onchocerciasis, nor an entomological study with PCR testing of blackflies to document the level of onchocerciasis transmission in the area. Moreover, we did not investigate the exact cause of death in PWE. However, given the difficulty to obtain antiseizure medication in the area, it is most likely that the PWE died of causes directly or indirectly related to seizures, as was observed in a recent clinical trial among PWE in Uganda (55).
In conclusion, the prevalence of epilepsy and the epilepsy case-fatality rate was high in the region of Deim Zubeir. More than half of the persons with epilepsy met the definition of onchocerciasis-associated epilepsy. The high prevalence of epilepsy, blindness, and skin lesions consistent with onchocerciasis, coupled with the low coverage of CDTI, suggest high ongoing O. volvulus transmission Based on study findings in onchocerciasis-endemic areas in the Western Equatoria state in 2021, the South Sudanese Neglected Tropical Disease program decided recently to switch from annual to semi-annual CDTI (19, 56). Hopefully, this will result in increased ivermectin coverage (19, 20). Strengthening the onchocerciasis elimination program in Deim Zubeir is urgently needed. To prevent children from developing OAE, it will be important that they take ivermectin at least once but ideally twice a year (19, 57).
In 2023, the Catholic diocese of Wau started an epilepsy treatment program in Deim Zubeir that included the provision of free antiseizure medication. It is expected that this will improve the health seeking behaviour of PWE and their families and, together with OAE awareness campaigns, will reduce epilepsy related stigma and discrimination (19, 20). Hopefully this program will be sustainable and curb the epilepsy-related mortality. However, more advocacy is needed to ensure the provision of uninterrupted free access to antiseizure medication to PWE in these remote impoverished areas (20).
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Oral consent in the presence of an independent witness was obtained from the head of households and people with epilepsy and carers who participated in the study. For children up to 11 years of age, the parents/caretakers provided consent, while adolescents between the ages of 12-17 years provided assent before parental consent.
JM: Writing – original draft, Writing – review & editing, Conceptualization, Investigation. GVC: Writing – original draft, Writing – review & editing, Data curation, Formal analysis, Software, Validation, Visualization. SM: Investigation, Writing – review & editing. SJ: Funding acquisition, Software, Writing – review & editing. TG: Funding acquisition, Investigation, Writing – review & editing. YB: Writing – review & editing. JS: Funding acquisition, Methodology, Writing – original draft, Writing – review & editing. RC: Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The study was funded by the Catholic Diocese of Wau and an R2HC grant of Amref Health Africa, South Sudan (Project ID: 78719). RC and JS received funding from the Research Foundation – Flanders (FWO), grant number G0A0522N and 1296723N, respectively. The study sponsors had no role in the design, execution, interpretation, or writing of the study.
We thank the Catholic Diocese of Wau, the parishes of Deim Zubeir and the administrators of Deim Zubeir for their support. We also thank all the families who participated in the study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fitd.2024.1469201/full#supplementary-material
CDTI, Community directed treatment with ivermectin; CI, confidence interval; IQR, Interquartile range; OAE, onchocerciasis-associated epilepsy; O. volvulus, Onchocerca volvulus; PWE, persons with epilepsy.
1. World Health Organisation. Epilepsy: a public health imperative (2019). Geneva: World Health Organization. Available online at: https://www.who.int/publications/i/item/epilepsy-a-public-health-imperative (Accessed 14 September 2024). Licence: CC BY-NC-SA 3.0 IGO.
2. Winter SF, Walsh D, Amos A, Secco M, Sofia F, Baker GA. The WHO intersectoral global action plan and epilepsy cascade target: Towards a roadmap for implementation. Seizure. (2022) 103:148–50. doi: 10.1016/j.seizure.2022.09.022
3. Siewe Fodjo JN, Van Cutsem G, Amaral LJ, Colebunders R. Mortality among persons with epilepsy in onchocerciasis-endemic and non-endemic areas of sub-Saharan Africa: A systematic review and meta-analysis. Seizure. (2023) 110:253–61. doi: 10.1016/j.seizure.2023.07.006
4. Gouda HN, Charlson F, Sorsdahl K, Ahmadzada S, Ferrari AJ, Erskine H, et al. Burden of non-communicable diseases in sub-Saharan Africa, 1990-2017: results from the Global Burden of Disease Study 2017. Lancet Glob Health. (2019) 7:e1375–e87. doi: 10.1016/S2214-109X(19)30374-2
5. Colebunders R, Abd-Elfarag G, Carter JY, Olore PC, Puok K, Menon S, et al. Clinical characteristics of onchocerciasis-associated epilepsy in villages in Maridi County, Republic of South Sudan. Seizure. (2018) 62:108–15. doi: 10.1016/j.seizure.2018.10.004
6. Colebunders R, YC J, Olore PC, Puok K, Bhattacharyya S, Menon S, et al. High prevalence of onchocerciasis-associated epilepsy in villages in Maridi County, Republic of South Sudan: A community-based survey. Seizure. (2018) 63:93–101. doi: 10.1016/j.seizure.2018.11.004
7. Bhattacharyya S, Vinkeles Melchers NVS, Siewe Fodjo JN, Vutha A, Coffeng LE, Logora MY, et al. Onchocerciasis-associated epilepsy in Maridi, South Sudan: Modelling and exploring the impact of control measures against river blindness. PLoS Negl Trop Dis. (2023) 17:e0011320. doi: 10.1371/journal.pntd.0011320
8. Jada SR, Amaral LJ, Lakwo T, Carter JY, Rovarini J, Bol YY, et al. Effect of onchocerciasis elimination measures on the incidence of epilepsy in Maridi, South Sudan: a 3-year longitudinal, prospective, population-based study. Lancet Glob Health. (2023) 11:e1260–e8. doi: 10.1016/S2214-109X(23)00248-6
9. Amaral LJ, Jada SR, Ndjanfa AK, Carter JY, Abd-Elfarag G, Okaro S, et al. Impact of annual community-directed treatment with ivermectin on the incidence of epilepsy in Mvolo, a two-year prospective study. PLoS Negl Trop Dis. (2024) 18:e0012059. doi: 10.1371/journal.pntd.0012059
10. Raimon S, Dusabimana A, Abd-Elfarag G, Okaro S, Carter JY, Newton CR, et al. High prevalence of epilepsy in an onchocerciasis-endemic area in Mvolo county, South Sudan: A door-to-door survey. Pathog. (2021) 10(5):599. doi: 10.3390/pathogens10050599
11. Abd-Elfarag GOE, Emmanuel L, Edridge AWD, van Beers S, Sebit MB, van Hensbroek MB, et al. Epidemiology of nodding syndrome in the Greater Mundri area, South Sudan: Prevalence, spatial pattern and environmental risk factors. PLoS Negl Trop Dis. (2022) 16:e0010630. doi: 10.1371/journal.pntd.0010630
12. Tumwine JK, Vandemaele K, Chungong S, Richer M, Anker M, Ayana Y, et al. Clinical and epidemiologic characteristics of nodding syndrome in Mundri County, southern Sudan. Afr Health Sci. (2012) 12:242–8. doi: 10.4314/ahs.v12i3.1
13. Siewe Fodjo JS JS, Taban A, Bebe J, Bol YY, Carter JY, Colebunders R. Epidemiology of epilepsy in Wulu County, an onchocerciasis-endemic area in South Sudan. Helyion. (2024) 10:e37537. doi: 10.1016/j.heliyon.2024.e37537
14. Brattig NW, Cheke RA, Garms R. Onchocerciasis (river blindness) - more than a century of research and control. Acta Trop. (2021) 218:105677. doi: 10.1016/j.actatropica.2020.105677
15. World Health Organisation. Onchocerciasis (2022). Available online at: https://www.who.int/news-room/fact-sheets/detail/onchocerciasis (Accessed 14 September 2024).
16. Noma M, Zoure HG, Tekle AH, Enyong PA, Nwoke BE, Remme JH. The geographic distribution of onchocerciasis in the 20 participating countries of the African Programme for Onchocerciasis Control: (1) priority areas for ivermectin treatment. Parasit Vectors. (2014) 7:325. doi: 10.1186/1756-3305-7-325
18. Colebunders R, Njamnshi AK, Menon S, Newton CR, Hotterbeekx A, Preux PM, et al. Onchocerca volvulus and epilepsy: A comprehensive review using the Bradford Hill criteria for causation. PLoS Negl Trop Dis. (2021) 15:e0008965. doi: 10.1371/journal.pntd.0008965
19. Colebunders R, Siewe Fodjo JN, Kamoen O, Amaral LJ, Hadermann A, Trevisan C, et al. Treatment and prevention of epilepsy in onchocerciasis-endemic areas is urgently needed. Infect Dis Poverty. (2024) 13:5. doi: 10.1186/s40249-024-01174-8
20. Van Cutsem G, Siewe Fodjo JN, Hadermann A, Amaral LJ, Trevisan C, Pion S, et al. Onchocerciasis-associated epilepsy: Charting a path forward. Seizure. (2024), S1059-1311(24)00123-7. doi: 10.1016/j.seizure.2024.04.018
21. Jada SR, Dusabimana A, Abd-Elfarag G, Okaro S, Brusselaers N, Carter JY, et al. The prevalence of onchocerciasis-associated epilepsy in mundri west and east counties, South Sudan: A door-to-door survey. Pathog. (2022) 11(4):396. doi: 10.3390/pathogens11040396
22. Hadermann A, Amaral LJ, Van Cutsem G, Siewe Fodjo JN, Colebunders R. Onchocerciasis-associated epilepsy: an update and future perspectives. Trends Parasitol. (2022) 39(2):126–38. doi: 10.1016/j.pt.2022.11.010
23. Van Cutsem G, Siewe Fodjo JN, Dekker MCJ, Amaral LJ, Njamnshi AK, Colebunders R. Case definitions for onchocerciasis-associated epilepsy and nodding syndrome: A focused review. Seizure. (2023) 107:132–5. doi: 10.1016/j.seizure.2023.03.024
24. Siewe JFN, Ngarka L, Tatah G, Mengnjo MK, Nfor LN, Chokote ES, et al. Clinical presentations of onchocerciasis-associated epilepsy (OAE) in Cameroon. Epilepsy Behav. (2019) 90:70–8. doi: 10.1016/j.yebeh.2018.11.008
25. Siewe Fodjo JN, Mandro M, Mukendi D, Tepage F, Menon S, Nakato S, et al. Onchocerciasis-associated epilepsy in the Democratic Republic of Congo: Clinical description and relationship with microfilarial density. PLoS Negl Trop Dis. (2019) 13:e0007300. doi: 10.1016/j.ibror.2019.07.1581
26. Abd-Elfarag G, Carter JY, Raimon S, Sebit W, Suliman A, Fodjo JNS, et al. Persons with onchocerciasis-associated epilepsy and nodding seizures have a more severe form of epilepsy with more cognitive impairment and higher levels of Onchocerca volvulus infection. Epileptic Disord. (2020) 22:301–8. doi: 10.1684/epd.2020.1164
27. Sejvar JJ, Kakooza AM, Foltz JL, Makumbi I, Atai-Omoruto AD, Malimbo M, et al. Clinical, neurological, and electrophysiological features of nodding syndrome in Kitgum, Uganda: an observational case series. Lancet Neurol. (2013) 12:166–74. doi: 10.1016/S1474-4422(12)70321-6
28. Idro R, Opoka RO, Aanyu HT, Kakooza-Mwesige A, Piloya-Were T, Namusoke H, et al. Nodding syndrome in Ugandan children–clinical features, brain imaging and complications: a case series. BMJ Open. (2013) 3(5):e002540. doi: 10.1136/bmjopen-2012-002540
29. Foger K, Gora-Stahlberg G, Sejvar J, Ovuga E, Jilek-Aall L, Schmutzhard E, et al. Nakalanga syndrome: clinical characteristics, potential causes, and its relationship with recently described nodding syndrome. PLoS Negl Trop Dis. (2017) 11:e0005201. doi: 10.1371/journal.pntd.0005201
30. Siewe Fodjo JN, Tatah G, Tabah EN, Ngarka L, Nfor LN, Chokote SE, et al. Epidemiology of onchocerciasis-associated epilepsy in the Mbam and Sanaga river valleys of Cameroon: impact of more than 13 years of ivermectin. Infect Dis Poverty. (2018) 7:114. doi: 10.1186/s40249-018-0497-1
31. Gumisiriza N, Kaiser C, Asaba G, Onen H, Mubiru F, Kisembo D, et al. Changes in epilepsy burden after onchocerciasis elimination in a hyperendemic focus of western Uganda: a comparison of two population-based, cross-sectional studies. Lancet Infect Dis. (2020) 20:1315–23. doi: 10.1016/S1473-3099(20)30122-5
32. Gumisiriza N, Mubiru F, Siewe Fodjo JN, Mbonye Kayitale M, Hotterbeekx A, Idro R, et al. Prevalence and incidence of nodding syndrome and other forms of epilepsy in onchocerciasis-endemic areas in northern Uganda after the implementation of onchocerciasis control measures. Infect Dis Poverty. (2020) 9:12. doi: 10.1186/s40249-020-0628-3
33. Bhwana D, Amaral LJ, Mhina A, Hayuma PM, Francis F, Siewe Fodjo JN, et al. Impact of a bi-annual community-directed treatment with ivermectin programme on the incidence of epilepsy in an onchocerciasis-endemic area of Mahenge, Tanzania: A population-based prospective study. PLoS Negl Trop Dis. (2023) 17:e0011178. doi: 10.1371/journal.pntd.0011178
35. Dadzie Y, Amazigo UV, Boatin BA, Seketeli A. Is onchocerciasis elimination in Africa feasible by 2025: a perspective based on lessons learnt from the African control programmes. Infect Dis Poverty. (2018) 7:63. doi: 10.1186/s40249-018-0446-z
36. World Health Organization. Guidelines for Stopping Mass Drug Administration and Verifying Elimination of Human Onchocerciasis (2006). Available online at: https://apps.who.int/iris/handle/10665/204180 (Accessed 14 September 2024).
37. Weather and Climate South Sudan (2024). Western Bahr el Ghazal: SS Climate Zone, Monthly Weather Averages and Historical Data (weatherandclimate.com. Available online at: https://weatherandclimate.com/south-Sudan/western-bahr-el-ghazalgoogle_vignette (Accessed 14 September 2024).
38. Conflict Sensitivity Resource Facility South Sudan. Raja County, Western Bahr el-Ghazal State (2024). Available at: https://www.csrf-southSudan.org/. Raja - csrf-southSudan.
39. City population. Western Bahr el Ghazal (State, South Sudan) - Population Statistics, Charts, Map and Location (citypopulation.de) (2024). Available online at: https://www.citypopulation.de/en/southSudan/admin/83:western_bahr_el_ghazal/ (Accessed 14 September 2024).
40. World Food Programme. World Food Programme and REACH (2020). Raja Market Assessment 2020. Available online at: https://reliefweb.int/sites/reliefweb.int/files/resources/REACH_SSD_Raja_Rapid-Market-Assessment_Aug2021_final.pdf (Accessed 14 September 2024).
41. Diagana M PP, Tuillas M, Ould Hamady A, Druet-Cabanac M. Dépistage de l'épilepsie en zones tropicales: validation d'un questionnaire en Mauritanie. Bull Soc Pathol Exot. (2006) 99:103–7.
42. Fisher RS, Acevedo C, Arzimanoglou A, Bogacz A, Cross JH, Elger CE, et al. ILAE official report: a practical clinical definition of epilepsy. Epilepsia. (2014) 55:475–82. doi: 10.1111/epi.2014.55.issue-4
43. United Nations Populations Divisions. World Population Prospects: 2022. South Sudan. Available online at: https://liveprod.worldbank.org/en/indicator/sp-dyn-cdrt-in (Accessed 14 September 2024). Revision. Death rate, crude (per 1,000 people).
44. Duke BO, Vincelette J, Moore PJ. Microfilariae in the cerebrospinal fluid, and neurological complications, during treatment of onchocerciasis with diethylcarbamazine. Tropenmed Parasitol. (1976) 27:123–32.
45. Hotterbeekx A, Raimon S, Abd-Elfarag G, Carter JY, Sebit W, Suliman A, et al. Onchocerca volvulus is not detected in the cerebrospinal fluid of persons with onchocerciasis-associated epilepsy. Int J Infect Dis. (2020) 91:119–23. doi: 10.1016/j.ijid.2019.11.029
46. Hotterbeekx A, Namale Ssonko V, Oyet W, Lakwo T, Idro R. Neurological manifestations in Onchocerca volvulus infection: A review. Brain Res Bull. (2019) 145:39–44. doi: 10.1016/j.brainresbull.2018.08.024
47. Winkler AS, Friedrich K, Velicheti S, Dharsee J, Konig R, Nassri A, et al. MRI findings in people with epilepsy and nodding syndrome in an area endemic for onchocerciasis: an observational study. Afr Health Sci. (2013) 13:529–40. doi: 10.4314/ahs.v13i2.51
48. Gumisiriza N, Kugler M, Brusselaers N, Mubiru F, Anguzu R, Ningwa A, et al. Risk factors for nodding syndrome and other forms of epilepsy in northern Uganda: A case-control study. Pathog. (2021) 10(11):1451. doi: 10.3390/pathogens10111451
49. Quek S, Hadermann A, Wu Y, De Coninck L, Hegde S, Boucher JR, et al. Diverse RNA viruses of parasitic nematodes can elicit antibody responses in vertebrate hosts. Nat Microbiol. (2024) 9(10):2488–505. doi: 10.1038/s41564-024-01796-6
50. Owolabi LF, Adamu B, Jibo AM, Owolabi SD, Isa AI, Alhaji ID, et al. Prevalence of active epilepsy, lifetime epilepsy prevalence, and burden of epilepsy in Sub-Saharan Africa from meta-analysis of door-to-door population-based surveys. Epilepsy Behav. (2020) 103:106846. doi: 10.1016/j.yebeh.2019.106846
51. WHO Africa. Expanded Special Project for Elimination of Neglected Tropical Diseases: South Sudan—Onchocerciasis 2022 (2022). Available online at: https://espen.afro.who.int/countries/south-Sudan (Accessed 14 September 2024).
52. Kipp W, Burnham G, Kamugisha J. Improvement in seizures after ivermectin. Lancet. (1992) 340:789–90. doi: 10.1016/0140-6736(92)92329-E
53. Mandro M, Siewe Fodjo JN, Mukendi D, Dusabimana A, Menon S, Haesendonckx S, et al. Ivermectin as an adjuvant to anti-epileptic treatment in persons with onchocerciasis-associated epilepsy: A randomized proof-of-concept clinical trial. PLoS Negl Trop Dis. (2020) 14:e0007966. doi: 10.1371/journal.pntd.0007966
54. Mandro M, Siewe Fodjo JN, Dusabimana A, Mukendi D, Haesendonckx S, Lokonda R, et al. Single versus multiple dose ivermectin regimen in onchocerciasis-infected persons with epilepsy treated with phenobarbital: A randomized clinical trial in the Democratic Republic of Congo. Pathog. (2020) 9(3):205. doi: 10.20944/preprints202001.0259.v1
55. Idro R, Ogwang R, Anguzu R, Akun P, Ningwa A, Abbo C, et al. Doxycycline for the treatment of nodding syndrome: a randomised, placebo-controlled, phase 2 trial. Lancet Glob Health. (2024) 12:e1149–e58. doi: 10.1016/S2214-109X(24)00102-5
56. Siewe Fodjo JN JS, Rovarini J, Bol YY, Carter JY, Hadermann A, Lakwo T, et al. Accelerating onchocerciasis elimination in humanitarian settings: lessons from South Sudan. Int Health. (2024), ihae051. doi: 10.1093/inthealth/ihae051
Keywords: onchocerciasis-associated epilepsy, epilepsy, onchocerciasis, South Sudan, nodding syndrome, prevalence, mortality
Citation: Mamur JP, Van Cutsem G, Motto SJH, Jada SR, Gerber T, Bol YY, Siewe Fodjo JN and Colebunders R (2025) Epilepsy in the onchocerciasis endemic area of Deim Zubeir, South Sudan: a household survey. Front. Trop. Dis 5:1469201. doi: 10.3389/fitd.2024.1469201
Received: 23 July 2024; Accepted: 30 September 2024;
Published: 18 February 2025.
Edited by:
Roberta Iatta, University of Bari Aldo Moro, ItalyReviewed by:
Robert Adamu Shey, University of Buea, CameroonCopyright © 2025 Mamur, Van Cutsem, Motto, Jada, Gerber, Bol, Siewe Fodjo and Colebunders. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gilles Van Cutsem, Z2lsbGVzdmFuY3V0c2VtQGdtYWlsLmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.