 André Ricardo Ribas Freitas1*
André Ricardo Ribas Freitas1* Antonio Silva Lima Neto2,3
Antonio Silva Lima Neto2,3 Rosana Rodrigues1
Rosana Rodrigues1 Erneson Alves de Oliveira4
Erneson Alves de Oliveira4 José S. Andrade Jr5
José S. Andrade Jr5 Luciano P. G. Cavalcanti6,7,8
Luciano P. G. Cavalcanti6,7,8- 1São Leopoldo Mandic School, Faculty of Medicine, Campinas, Brazil
- 2Center of Health Sciences, University of Fortaleza, Fortaleza, Ceará, Brazil
- 3Health Secretariat of Ceará State, Fortaleza, Ceará, Brazil
- 4Data Science and Artificial Intelligence Center, University of Fortaleza, Fortaleza, Ceará, Brazil
- 5Physics Department, Federal University of Ceará, Fortaleza, Ceará, Brazil
- 6Public Health Department, Federal University of Ceara, Fortaleza, Brazil
- 7School of Medicine, Christus University Center, Fortaleza, Brazil
- 8Ceara School of Public Health, Fortaleza, Brazil
The chikungunya virus (CHIKV) was first detected in Brazil in 2014 and has since caused major epidemics. In 2023, a major chikungunya epidemic occurred in Minas Gerais, one of the most populous states in the country. We analyzed the North and Northeast Health Macroregions of Minas Gerais, with 2.5 million inhabitants. The study used epidemiological data from the Ministry of Health’s laboratory surveillance, disease notification and mortality systems. A robust Poisson regression model was constructed to estimate expected monthly mortality. Excess deaths were calculated by comparing observed deaths with model estimates during the epidemic period. During the epidemic, there were 890 excess deaths attributed to chikungunya, translating into a mortality rate of 35.1/100,000 inhabitants. The excess mortality rate was significantly 60 times higher than the deaths reported by surveillance, with only 15 confirmed deaths. The correlation between excess deaths and laboratory-confirmed chikungunya cases was strong, while the correlation with dengue and COVID-19 was not statistically significant. The results highlighted the serious underestimation of chikungunya mortality by epidemiological surveillance. During the same year, only 420 chikungunya deaths were reported by all PAHO member countries. Routine epidemiological surveillance systems cannot capture the full impact of this disease. Excess mortality is a key measure for understanding the impact of epidemics, as demonstrated by COVID-19 and influenza pandemics. The study highlights the need for complementary tools to traditional surveillance to better assess impacts on morbidity and mortality and support priority setting in public health interventions.
Introduction
Chikungunya is an emerging acute viral disease transmitted by Aedes aegypti and Aedes albopictus mosquitoes, causing fever, joint pain, rashes and fatigue, and is often confused with dengue (1). It was first isolated in the 1950s in Tanzania and the first deaths were reported during the epidemics of the 1960s in India (2–4) and were consequences of neurological and cardiovascular complications, sepsis and decompensation of pre-existing diseases. Since 2004, chikungunya has emerged as a global threat to public health, causing extensive epidemics in several parts of the world, including the Americas, Africa, Asia and Islands in the Indian and Pacific Oceans (1).
The severity of cases may be associated with different genotypes, lineages and specific mutations. Host genetic characteristics and local availability of healthcare resources can also affect disease severity, resulting in wide variation in mortality across different epidemics and contexts (5, 6). Acute cases and, especially, deaths from chikungunya have been greatly underdiagnosed and underreported, especially in countries with less availability of resources (7, 8). Excess deaths have been a tool that contributes to the assessment in these situations. Excess mortality refers to the number of deaths that surpass expected levels based on historical trends, adjusted for seasonal and long-term fluctuations (9, 10). This measure is necessary for accurately assessing the impact of epidemics, especially in the context of diseases like chikungunya, where severe cases often go unrecognized by healthcare professionals due to limited clinical familiarity with the disease (11, 12). Chikungunya-associated mortality is frequently underreported because severe forms of the disease, such as those involving neurological or cardiovascular complications (13, 14), are misclassified or overlooked because these forms are poorly understood. Excess mortality allows for a more comprehensive evaluation of the true burden of chikungunya, particularly in areas with high transmission rates and limited healthcare capacity (7, 10, 15–18).
Until then free area, in Brazil in 2014 two lineages of the chikungunya virus (CHIKV) were detected, in the North, Asian lineage and in the Northeast, ECSA (East/Central/South Africa, CHIKV), with transmission sustained by Aedes aegypti. In the following years, only the ECSA lineage remained and caused several focal epidemics, mainly in the North and Northeast regions (19). In recent years there has been an increase in the number of cases with rapid territorial expansion, reaching densely populated areas in the South and Southeast regions (19). The co-circulation of dengue and chikungunya, associated with little clinical knowledge of the latter by health professionals, has made the diagnosis and treatment of the disease difficult, in addition to preventing a more reliable assessment of the impact of chikungunya in Brazil (12) and in other countries in the region (11).
In the year 2023, Minas Gerais, a state located in the Southeast Region of Brazil, was the state most affected by the chikungunya epidemic (12). Using a methodology adopted by the World Health Organization (10, 18), we assessed mortality associated with the chikungunya epidemic in the most affected areas.
Methods
Study location and characteristics
We conducted the study in the North and Northeast Health Macro-regions of Minas Gerais, Brazil (Figure 1). These regions were selected due to their high chikungunya incidence during the 2023 epidemic and their epidemiological similarity. The combined population of these regions is approximately 2.5 million people, distributed across urban and rural areas. Montes Claros, the largest city, has a population of 413,000, while the rest of the population is spread across low-density rural zones. The climate in these regions is tropical, with defined wet and dry seasons, and there were no extreme weather events during the study period, according to the National Institute of Meteorology (INMET, Supplementary Material). This lack of extreme climatic events ensured that mortality patterns were not influenced by environmental factors outside of the epidemic.
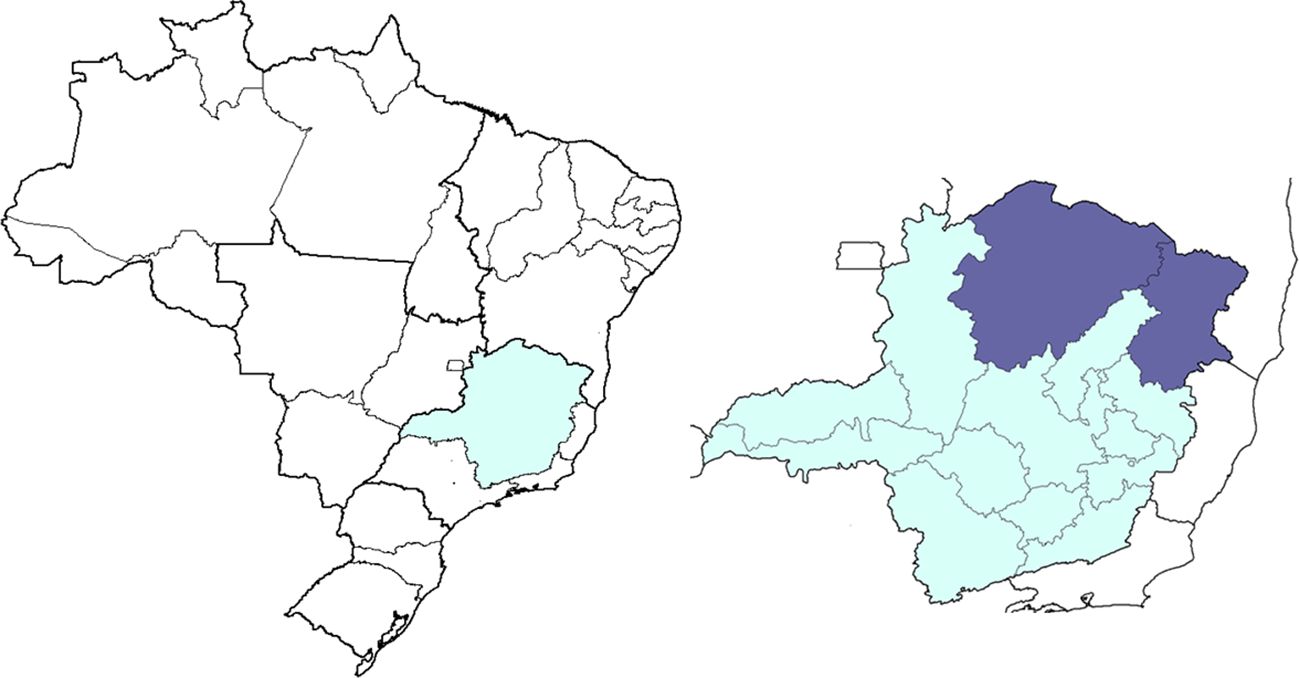
Figure 1. Map of Brazil highlighting the State of Minas Gerais and the North and Northeast Health Macro-regions.
Data collection procedure
We obtained epidemiological data from three key systems maintained by the Brazilian Ministry of Health: the laboratory surveillance system (GAL, acronymous in Portuguese), the disease notification system (SINAN, acronymous in Portuguese), and the mortality system (SIM, acronymous in Portuguese). The laboratory surveillance system provided investigated cases of chikungunya, dengue, and COVID-19 (Severe Acute Respiratory Infection cases) based on RT-qPCR testing, while the disease notification system provided reported cases, and the mortality system recorded all-cause mortality data (excluding external causes of death, such as accidents, homicides, and suicides). We calculated incidence rates and test positivity for chikungunya, dengue, and COVID-19 based on laboratory surveillance system (Table 1).
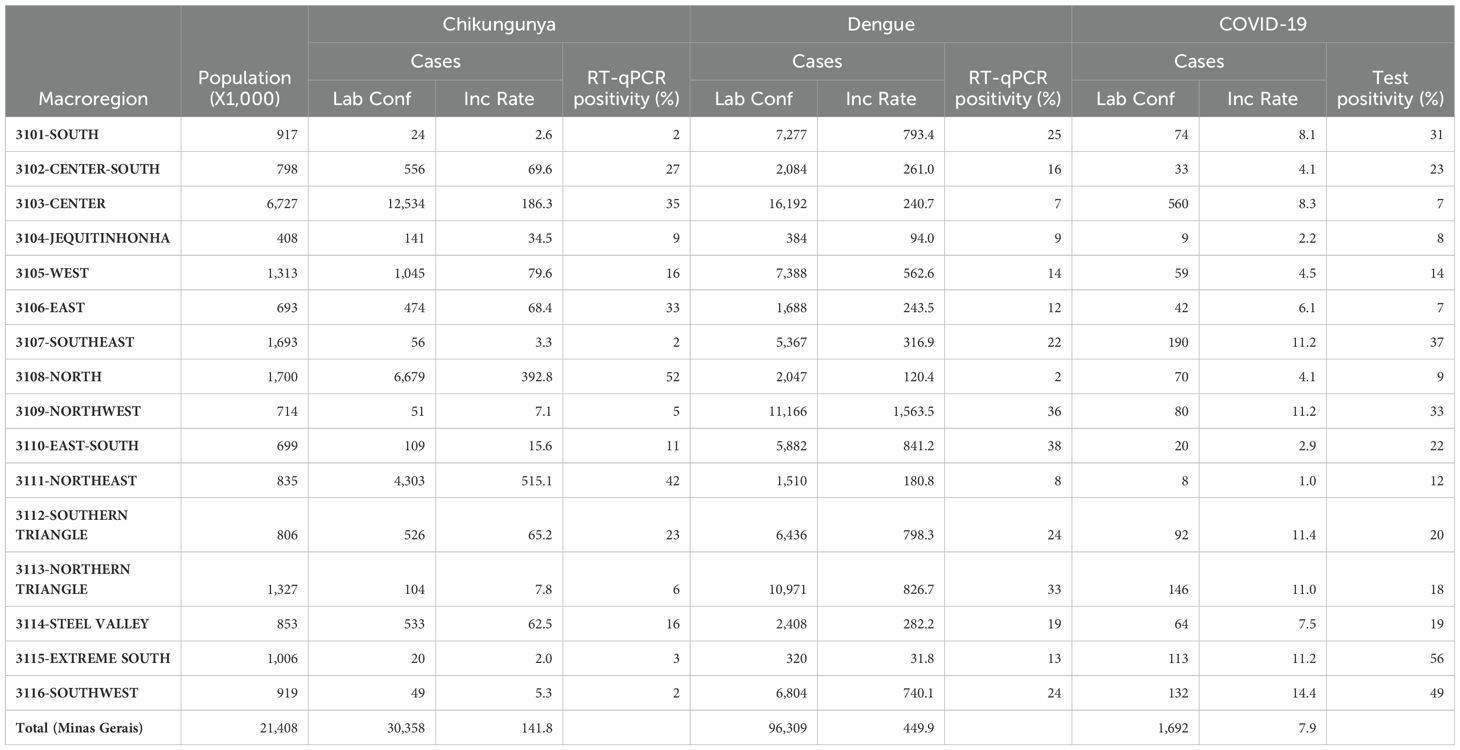
Table 1. Population, laboratory confirmed cases, incidence rate and test positivity in the Health Macro-regions of Minas Gerais (chikungunya, dengue and covid-19, Dec 2022-May 2023, Brazil).
Inclusion and exclusion criteria
We included all laboratory confirmed chikungunya cases reported between January 2017 and December 2023 from the North and Northeast Health Macro-regions of Minas Gerais State. For mortality analysis, we included all-cause mortality (excluding external causes of death) data. The most critical period of the COVID-19 pandemic (January 2020 to July 2022) was excluded from the mortality analysis. To calibrate the model and estimate expected deaths, we excluded the peak period of the chikungunya epidemic (December 2022 to May 2023), which was defined as the months with incidence coefficients above the 95% percentile of the period analyzed.
Sample size and selection
The study sample size consisted of all residents of the North and Northeast Health Macro-regions of Minas Gerais, totaling 2.5 million people. This large population base ensured a robust sample for the analysis of both incidence rates and excess mortality. The inclusion large populations allowed for a comprehensive analysis across different socio-economic and geographic contexts. The sample selection was justified by the fact that these regions had the highest chikungunya positivity rates and incidence during the 2023 epidemic in Minas Gerais, making them ideal for assessing the impact of the epidemic.
Statistical analysis
To estimate the excess mortality associated with chikungunya, we constructed a robust Poisson regression model based on a time series of monthly deaths. The choice of the Poisson model was justified by its flexibility in modeling count data and its widespread use in epidemiological studies to estimate expected mortality (10, 20). The regression model included time variables (in months) as linear, quadratic, and cubic terms to correct for long-term secular trends. We also included month-specific nominal variables to adjust for seasonal variations, which are critical in the analysis of infectious diseases like chikungunya that exhibit strong seasonal patterns (10, 17).
where: represented the number of deaths in a particular month i, are time in months as a linear, quadratic and cubic to correct for secular fluctuations and are the nominal variables associated with the months, to correct seasonal fluctuations and ϵi is the error term.
We excluded months impacted by COVID-19 and the peak of the chikungunya epidemic from the model calibration to avoid overestimating the baseline mortality. The final model was used to predict expected deaths, and excess mortality was calculated as the difference between observed and predicted deaths during the chikungunya epidemic period. Excess deaths were considered significant when observed deaths exceeded the upper limit of the 99% confidence interval of the predicted values (Figure 2). All analyses were performed using SPSS version 24.
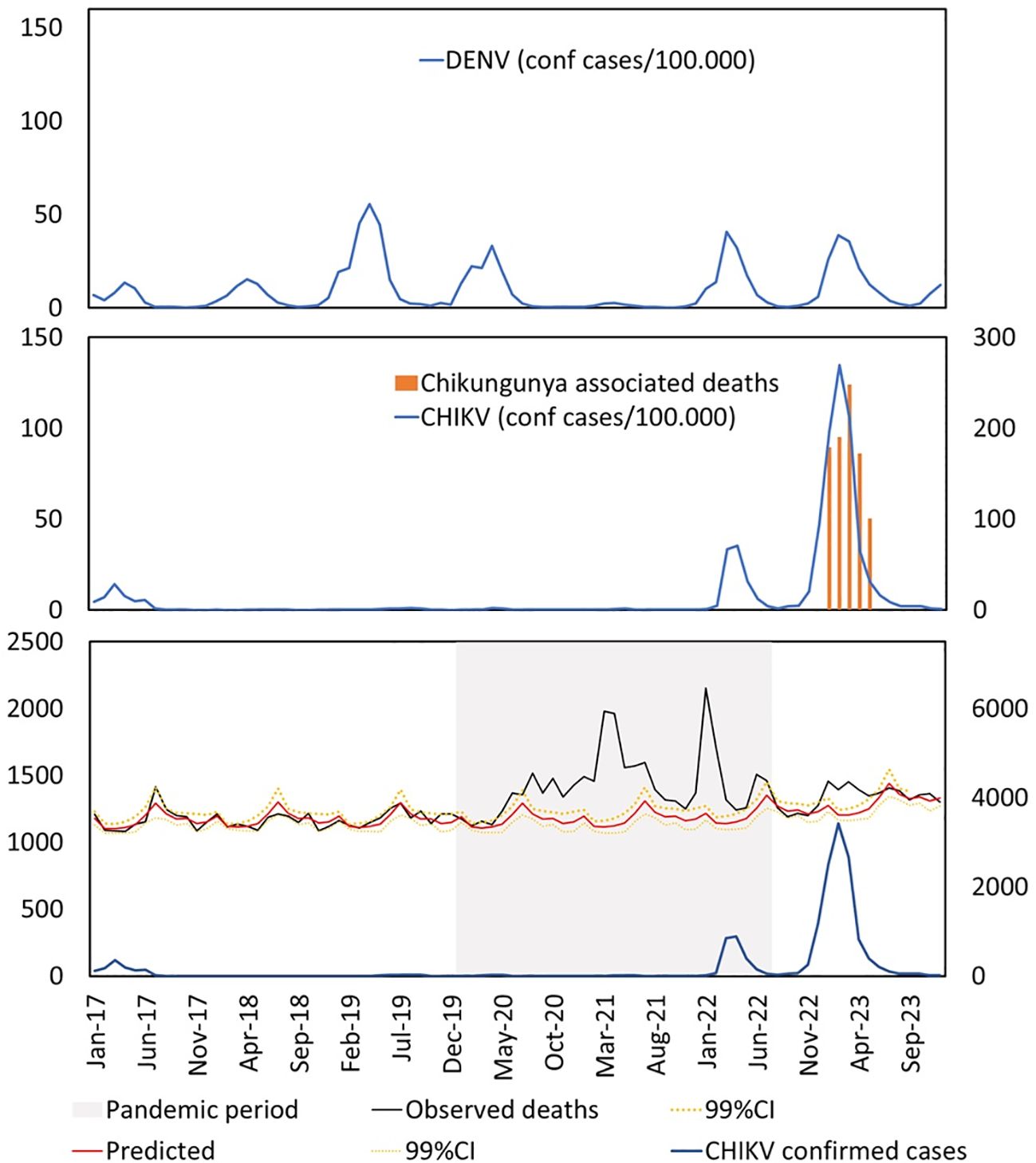
Figure 2. Bottom: absolute number of monthly cases of chikungunya (blue line, right scale), number of observed monthly deaths (black line, left scale), number of monthly deaths predicted by the model (solid red line, left scale) and upper and lower limits of the 99% confidence interval (dotted and solid yellow lines respectively, left scale). In the middle: monthly incidence coefficient of chikungunya per 100,000 inhabitants (blue line, left scale), monthly number of excess deaths (red columns, right scale). Above: dengue incidence coefficient per 100,000 inhabitants (blue line, left scale). All data refer to the North and Northeast Health Macro-regions of Minas Gerais.
Ethical aspects
Since the data used in this study are publicly available and do not include any identifiable personal information, there was no need for submission to an ethics committee for this research.
Results
The results indicate a positive and significant correlation between monthly excess mortality and laboratory-confirmed chikungunya cases, with a Kendall’s tau-b of 0.706 (p=0.003). This data is presented in Table 2, which details the correlation coefficients for chikungunya, dengue, and COVID-19. As expected, due to the seasonal overlap, there was a correlation between excess mortality and the number of dengue cases, although the correlation with the positivity of laboratory tests (RT-qPCR) for dengue was negative and non-significant (Kendall’s tau-b = -0.277, p=0.191) (Table 2).
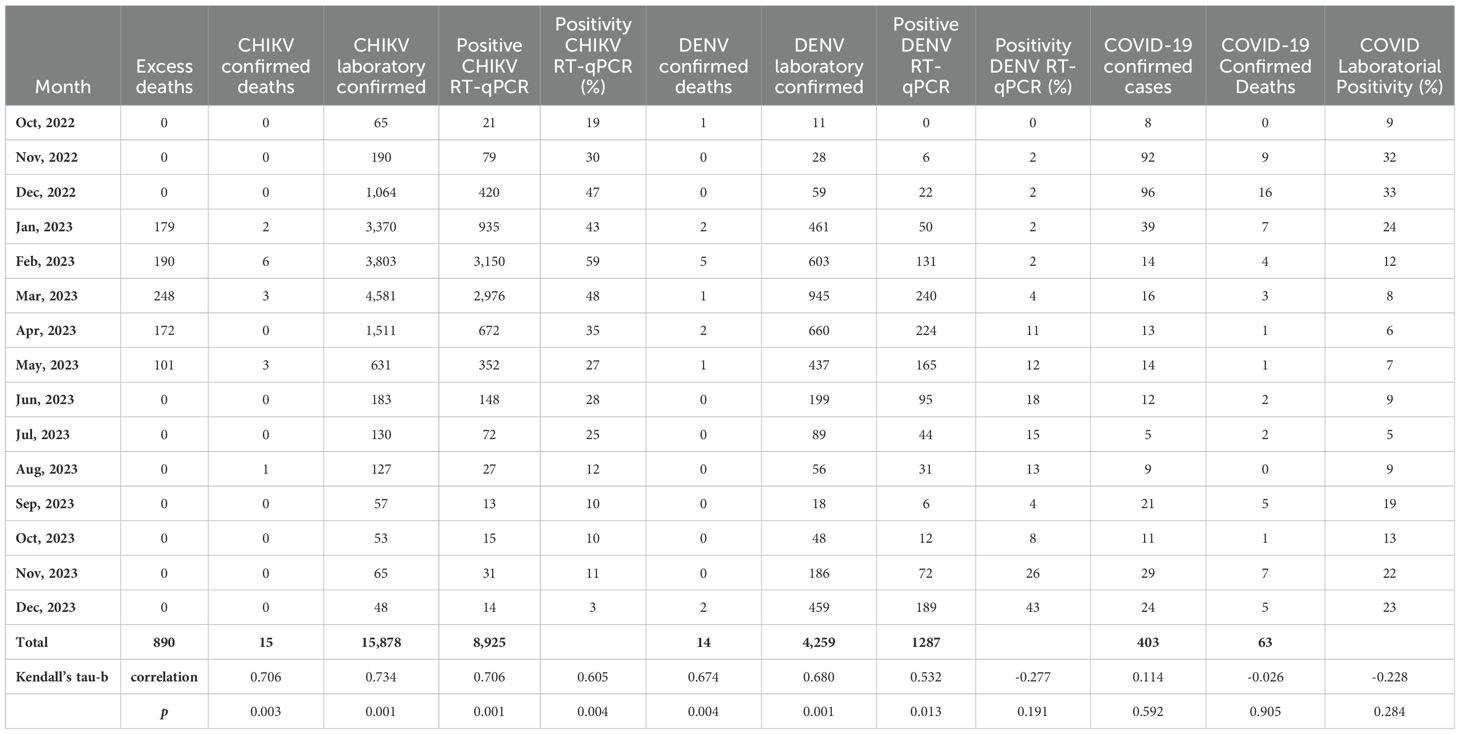
Table 2. Excess deaths, laboratory-confirmed cases and deaths, incidence rate and test positivity per month North and Northeast Health Macro-regions of Minas Gerais (chikungunya, dengue and covid-19, Oct, 2022 - Dec, 2023, Brazil).
Regarding COVID-19, the results show a negative and non-significant correlation between excess monthly mortality and confirmed COVID-19 cases and positive RT-qPCR tests, with Kendall’s tau-b = -0.026 (p=0.905) for confirmed cases and Kendall’s tau-b = -0.228 (p=0.284) for test positivity (Table 2). As presented in the number of excess deaths associated with the chikungunya epidemic in Minas Gerais (2023) was significantly higher than the officially reported numbers. In total, there were 890 excess deaths, while only 15 deaths were officially confirmed as chikungunya-related, suggesting significant underreporting (Table 2).
The parameters and quality of fit for the final Poisson regression model are detailed in the Appendix. The results from an alternative model analysis, which included seasonal components (sine and cosine), did not significantly differ from the main model results (p=0.8). Based on the principle of parsimony and the simplicity of the model, we opted for the final model that uses discrete monthly seasonal variables.) (21), Detailed results of this supplementary analysis are also provided in the Appendix.
Discussion
The number of deaths (890 deaths) attributable to the chikungunya epidemic is almost 60 times greater than the number of deaths (15 deaths) identified by epidemiological surveillance in the two Macro-regions studied. Despite representing a small fraction of the Brazilian territory, this excess of deaths observed is almost 8 times greater than the total number of deaths from chikungunya identified by epidemiological surveillance throughout Brazil in the year 2023 (106 deaths). The negative and non-significant correlation between excess mortality and monthly COVID-19 confirmed cases, as well as dengue RT-qPCR positivity, suggests that these two diseases did not significantly contribute to the excess deaths observed during the study period. In contrast, there was a positive correlation between monthly excess mortality and CHIKV confirmed deaths, CHIKV laboratory-confirmed cases, positive CHIKV RT-qPCR results, and the percentage of CHIKV RT-qPCR positivity. This reinforces the conclusion that chikungunya was the primary driver of the observed excess mortality.
In Pernambuco (2016, Brazil) there were 4,505 excess deaths during the chikungunya epidemic period, but surveillance confirmed only 94 deaths. In Puerto Rico in the 2014 epidemic, only 31 deaths from chikungunya were confirmed, but there were 1,310 deaths higher than expected for the period (22, 23). In these examples, the underestimation of the number of deaths by the official surveillance system was 98%, the same value found in the present study (Table 3). These findings highlight the underestimation of chikungunya-associated mortality by routine epidemiological surveillance systems, a pattern also observed in other chikungunya epidemics. In these cases, excess mortality far exceeded the number of confirmed deaths, reinforcing the need for more comprehensive surveillance methods that extend beyond laboratory-confirmed cases. Many deaths attributed to chikungunya remain unrecognized due to the lack of clinical suspicion and the co-circulation of other arboviruses like dengue.
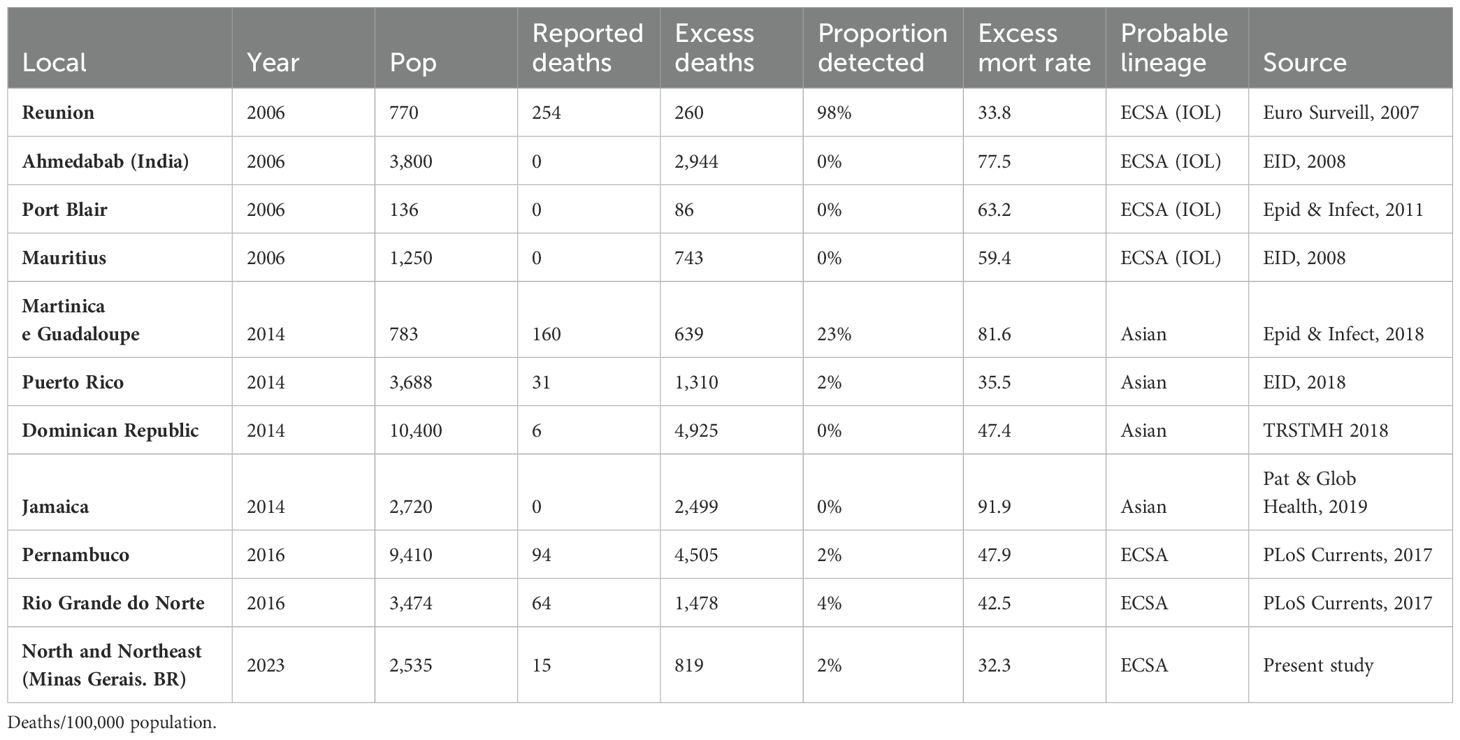
Table 3. Mortality associated with chikungunya epidemics: reported deaths, excess deaths, and excess mortality rates in various regions and countries during different epidemic periods.
A study by Cerqueira-Silva et al. (24) demonstrated that chikungunya virus infection is associated with an increased risk of death for up to 84 days after the onset of symptoms. This includes deaths resulting from neurological diseases, heart disease, and diabetes, which may be related to direct viral damage or the inflammatory response triggered by CHIKV infection. Supporting these findings, a study with data from Puerto Rico identified that the excess mortality observed during the chikungunya epidemic was concentrated precisely in these disease categories, with a 1-month lag between the peak of symptom onset and the peak of mortality (23). This extended time between infection and death from chikungunya likely contributes to the underreporting of chikungunya-related mortality (25). One factor that may help explain the differences in underreporting of deaths in other epidemics, such as COVID-19 and dengue, lies in the mechanisms of mortality and the challenges in accurately diagnosing and reporting chikungunya-associated deaths. While COVID-19 is primarily known for its impact on respiratory failure, and dengue is a disease with well-known complications that has recurred annually for decades, chikungunya-related deaths are usually due to circulatory, inflammatory, cardiovascular, neurological, and respiratory complications, or the decompensation of underlying conditions, which are less likely to be immediately attributed to the virus (6, 25).
The excess mortality rate in the period was calculated at 35.1/100,000 inhabitants. This value is a little more than half the global average excess mortality rate from Covid-19 estimated by WHO for the first year of the pandemic (60/100,000) (18), it is seven times greater than the excess rate estimated global average mortality rate for the 2009 influenza pandemic (5/100,000 inhabitants) and is close to the excess mortality rate for the 1967 influenza pandemic (40/100,000) (26). In a similar study we found that in the 2016 chikungunya epidemic in Pernambuco there was an excess death rate of 47.9 and in the 2014 epidemic on the islands of Guadalupe and Martinique the excess deaths were 81.6 per 100,000 inhabitants (22, 27). Mavalankar and colleagues calculated the excess mortality rate in Ahmedabab(India) during the 2006 chikungunya epidemic at 77.5 deaths per 100,000(3,800 deaths) (7) while no deaths have been officially confirmed in the country (Table 3) (8, 16, 28–30).
Covid-19 pandemic brought great interest to the topic of monitoring excess mortality as a fundamental tool for assessing the impact of emerging viruses, as it is applicable in different contexts and is less dependent on laboratory resources (18, 26). Given the significant increase in the number of chikungunya cases in endemic areas and the expansion of this and other arboviruses to free areas, tools complementary to traditional epidemiological surveillance need to be added to better assess the impact in terms of morbidity and mortality.
Excess mortality is a measure that contributes to building solid evidence of the impact of epidemics and pandemics. Influenza is a classic example of the use of this tool to more adequately measure the number of deaths, as a significant part of deaths occur due to bacterial complications, decompensation of pre-existing diseases, among others (26, 31). Adequately quantifying the number of deaths caused by emerging viruses is a fundamental need so that risk assessment and priority-setting systems can direct resources to address epidemiological challenges.
In recent years, necropsy studies have demonstrated viral antigens and genetic material in tissues of important organs such as the CNS, heart, lung and liver (6, 25, 32, 33). The fact that the worsening of chikungunya is caused by a severe systemic infection, immunological and hemodynamic dysfunction, associated with the dysfunction of multiple distinct organs makes it difficult to define a single clinical syndrome that characterizes the worsening, which makes clinical suspicion very difficult, especially as it is a disease emerging (6, 25, 32, 33).
Limitations, internal and external validity
A major limitation of this study is its ecological design, which uses aggregated population-level data rather than individual-level information, making it impossible to establish direct causal relationships. Additionally, although the health system was prepared for previous COVID-19 and dengue epidemics, the strain on the system during the chikungunya epidemic may have contributed to some excess deaths, either due to delays in treatment or limited access to care. Underreporting of confirmed cases is another potential issue, as chikungunya symptoms can easily be confused with other circulating arboviruses, such as dengue, and the limited availability of laboratory testing during epidemics may lead to inaccuracies in case reporting and investigation (12). Disparities in access to healthcare, particularly in regions with limited infrastructure, may exacerbate the outcomes of chikungunya infection. Socioeconomic status also plays a crucial role, as populations with lower income may experience delays in seeking care, increasing the likelihood of fatal complications. These factors should be considered when interpreting the mortality burden of chikungunya.
The internal validity of this study is supported by the use of robust Poisson regression modeling, which accounts for both secular and seasonal fluctuations in mortality over a multi-year period. By excluding the most critical periods of the COVID-19 pandemic and the peak months of the chikungunya epidemic from the model calibration, we minimized the risk of bias in the estimated baseline mortality. Furthermore, the inclusion of comprehensive data from official epidemiological and laboratory surveillance systems for other seasonal viruses, such as SARS-COV-2 and dengue, reinforces the reliability of the results.
Regarding external validity, this study’s methodology has been successfully applied in chikungunya studies not only in other regions of Brazil but also in countries such as India (7, 15), Mauritius (8, 16), Puerto Rico (23), Dominican Republic (34), Jamaica, and the overseas departments and regions of France, including Guadeloupe (27), Martinique (27), and Réunion (29), each with distinct epidemiological and healthcare contexts. This demonstrates the flexibility and robustness of the method in diverse settings. Furthermore, it is a methodology endorsed by major public health organizations such as the World Health Organization (WHO) (10), the European Centre for Disease Prevention and Control (ECDC) (21), and the Centers for Disease Control and Prevention (CDC) (31) for evaluating the impact of pandemics like influenza and COVID-19, as well as for monitoring annual influenza seasons. This widespread use underscores its reliability for assessing excess mortality in the context of arbovirus epidemics and other public health crises.
Recommendations for future studies
Future studies should consider incorporating more detailed clinical data, such as autopsy findings and hospital records, to improve the accuracy of death classification in chikungunya epidemics. In addition, expanding laboratory testing during epidemics could help differentiate between chikungunya and co-circulating arboviruses, such as dengue and Zika, leading to more accurate case counts and mortality estimates. We also recommend using excess mortality as a complementary tool to traditional surveillance, as it provides a broader understanding of the true mortality burden in regions where health systems are often overburdened during epidemics.
The first warning sign about the importance of severe forms of chikungunya was given in 2006 on the island of Reunion (13), the issue of underreporting of deaths was subsequently demonstrated in India (7). Since then, evidence of these warnings has been confirmed through different study designs, in different regions of the world, however, several researchers and even official documents still classify chikungunya disease as having a low risk of death.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author contributions
AR: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. AL: Conceptualization, Writing – original draft, Writing – review & editing. RR: Project administration, Writing – original draft, Writing – review & editing. EA: Conceptualization, Writing – original draft, Writing – review & editing. JA: Conceptualization, Writing – original draft, Writing – review & editing. LC: Conceptualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. JSA gratefully acknowledges the FUNCAP Award 06849573/2023, the CNPq Award 303765/2017-8 (Bolsa PQ), and the CAPES Award 88887.311932/2018-00 (CAPES/PRINT) for financial support. LPGC gratefully acknowledges the CNPq Award 310579/2022-8 (Bolsa PQ).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fitd.2024.1466207/full#supplementary-material
References
1. de Lima Cavalcanti TYV, Pereira MR, de Paula SO, de Franca RFO. A review on chikungunya virus epidemiology, pathogenesis and current vaccine development. Viruses. (2022) 14:969. doi: 10.3390/v14050969
2. Chakravarty SK, Sarkar JK. Attempt to isolate virus from mosquitoes during hemorrhagic fever in Calcutta. Bull Calcutta School Trop Med. (1967) 15:56–7.
3. Sarkar JK, Chatterjee SN, Chakravarty SK, Mitra AC. The causative agent of Calcutta haemorrhagic fever: chikungunya or dengue. Bull Calcutta School Trop Med. (1965) 13:53–4.
4. Sarkar JK, Chatterjee SN, Chakravarty SK, Mitra AC. Virological studies in nine fatal cases of fever with haemorrhagic manifestation in Calcutta. Indian J Pathol Bacteriology. (1966) 9:123–7.
5. Montalvo Zurbia-Flores G, Reyes-Sandoval A, Kim YC. Chikungunya virus: priority pathogen or passing trend? Vaccines. (2023) 11:568. doi: 10.3390/vaccines11030568
6. de Souza WM, Fumagalli MJ, de Lima STS, Parise PL, Carvalho DCM, Hernandez C, et al. Pathophysiology of chikungunya virus infection associated with fatal outcomes. Cell Host Microbe. (2024) 32:606–622.e8. doi: 10.1016/j.chom.2024.02.011
7. Mavalankar D, Shastri P, Bandyopadhyay T, Parmar J, Ramani KV. Increased mortality rate associated with chikungunya epidemic, Ahmedabad, India. Emerging Infect Dis. (2008) 14:412–5. doi: 10.3201/eid1403.070720
8. Beesoon S, Funkhouser E, Kotea N, Spielman A, Robich RM. Chikungunya fever, Mauritius, 2006. Emerging Infect Dis. (2008) 14:337–8. doi: 10.3201/eid1402.071024
9. Lima Neto AS, Sousa GS, Nascimento OJ, Castro MC. Chikungunya-attributable deaths: A neglected outcome of a neglected disease. PLoS Negl Trop Dis. (2019) 13:e0007575. doi: 10.1371/journal.pntd.0007575
10. World Health Organisation. Methods for estimating the excess mortality associated with the COVID-19 pandemic (2023). Available online at: https://www.who.int/publications/m/item/methods-for-estimating-the-excess-mortality-associatedwith-the-covid-19-pandemic (Accessed June 3, 2024).
11. Nunez-Avellaneda D, Tangudu C, Barrios-Palacios J, MaI S, Machain-Williams C, Cisneros-Pano J, et al. Chikungunya in Guerrero, Mexico, 2019 and evidence of gross underreporting in the region. Am J Trop Med Hygiene. (2021) 105:1281–4. doi: 10.4269/ajtmh.21-0431
12. Freitas ARR, Pinheiro Chagas AA, Siqueira AM, Pamplona de Góes Cavalcanti L. How much of the current serious arbovirus epidemic in Brazil is dengue and how much is chikungunya? Lancet Regional Health – Americas. (2024) 34. doi: 10.1016/j.lana.2024.100753
13. Economopoulou A, Dominguez M, Helynck B, Sissoko D, Wichmann O, Quenel P, et al. Atypical Chikungunya virus infections: clinical manifestations, mortality and risk factors for severe disease during the 2005-2006 outbreak on Réunion. Epidemiol Infection. (2009) 137:534–41. doi: 10.1017/S0950268808001167
14. Gupta A, Juneja D, Singh O, Garg SK, Arora V, Deepak D. Clinical profile, intensive care unit course, and outcome of patients admitted in intensive care unit with chikungunya. Indian J Crit Care Med. (2018) 22:5–9. doi: 10.4103/ijccm.IJCCM_336_17
15. Manimunda SP, Mavalankar D, Bandyopadhyay T, Sugunan AP. Chikungunya epidemic-related mortality. Epidemiol Infection. (2011) 139:1410–2. doi: 10.1017/S0950268810002542
16. Ramchurn SK, SSDGΨ M, Makhan M. An analysis of the excess mortality profile during the 2006 Chikungunya Fever epidemic in Mauritius. Internet J Med Update. (2010) 5:3–7.
17. WHO. Regional Office for the Western Pacific. A practical guide for designing and conducting influenza disease burden studies. WHO Regional Office for the Western Pacific. (2009) p. 41 Available at: https://iris.who.int/handle/10665/208104 (Accessed September 5, 2024).
18. Msemburi W, Karlinsky A, Knutson V, Aleshin-Guendel S, Chatterji S, Wakefield J. The WHO estimates of excess mortality associated with the COVID-19 pandemic. Nature. (2023) 613:130–7. doi: 10.1038/s41586-022-05522-2
19. de Souza WM, de Lima STS, Simões Mello LM, Candido DS, Buss L, Whittaker C, et al. Spatiotemporal dynamics and recurrence of chikungunya virus in Brazil: an epidemiological study. Lancet Microbe. (2023) 4(5):e319–29. doi: 10.1016/S2666-5247(23)00033-2
20. The true death toll of COVID-19 estimating global excess mortality. Available online at: https://www.who.int/data/stories/the-true-death-toll-of-covid-19-estimating-global-excess-mortality (Accessed September 5, 2024).
21. European Centre for Disease Prevention and Control. Trend analysis guidance for surveillance data. Stockholm: European Centre for Disease Prevention and Control (2024). doi: 10.2900/294038
22. Freitas ARR, Cavalcanti L, Zuben APV, Donalisio MR. Excess mortality related to chikungunya epidemics in the context of co-circulation of other arboviruses in Brazil. PLoS Currents Outbreaks. (2017), 140491. doi: 10.1371/currents.outbreaks.14608e586cd321d8d5088652d7a0d884
23. Freitas ARR, Donalisio MR, Alarcón-Elbal PM. Excess mortality and causes associated with Chikungunya, Puerto Rico, 2014–2015. Emerging Infect Dis. (2018) 24:2352–5. doi: 10.3201/eid2412.170639
24. Cerqueira-Silva T, Pescarini JM, Cardim LL, Leyrat C, Whitaker H, Antunes de Brito CA, et al. Risk of death following chikungunya virus disease in the 100 Million Brazilian Cohort, 2015-18: a matched cohort study and self-controlled case series. Lancet Infect Dis. (2024) 24:504–13. doi: 10.1016/S1473-3099(23)00739-9
25. de Lima STS, de Souza WM, Cavalcante JW, da Silva Candido D, Fumagalli MJ, Carrera J-P, et al. Fatal outcome of chikungunya virus infection in Brazil. Clin Infect Dis. (2021) 73:e2436–43. doi: 10.1093/cid/ciaa1038
26. Simonsen L, Viboud C. A comprehensive look at the COVID-19 pandemic death toll. eLife. (2021) 10. doi: 10.7554/eLife.71974
27. Freitas ARR, Alarcón-Elbal PM, Donalisio MR. Excess mortality in Guadeloupe and Martinique, islands of the French West Indies, during the chikungunya epidemic of 2014. Epidemiol Infection. (2018) 146(16):2059–65. doi: 10.1017/S0950268818002315
28. Ledrans M, Quatresous I, Renault P, Pierre V. Outbreak of chikungunya in the French Territories, 2006: lessons learned. Euro Surveil. (2007) 12. doi: 10.2807/esw.12.36.03262-en
29. Josseran L, Paquet C, Zehgnoun A, Caillere N, Tertre AL, Solet J-L, et al. Chikungunya disease outbreak , reunion island. Emerging Infect Dis. (2006) 12:1994–5. doi: 10.3201/eid1212.060710
30. Freitas ARR, Gérardin P, Kassar L, Donalisio MR. Excess deaths associated with the 2014 chikungunya epidemic in Jamaica. Pathog Global Health. (2019) 00:1–5. doi: 10.1080/20477724.2019.1574111
31. Centers for Disease Control and Prevention, National Center for Immunization and Respiratory Diseases (NCIRD), USA. Estimating Seasonal Influenza-Associated Deaths in the United States (2022). CDC. Available online at: https://www.cdc.gov/flu/about/disease/us_flu-related_deaths.htm (Accessed September 5, 2024).
32. Paz-Bailey G, Rosenberg ES, Doyle K, Munoz-Jordan J, Santiago GA, Klein L, et al. Persistence of zika virus in body fluids — Preliminary report. N Engl J Med. (2017), NEJMoa1613108. doi: 10.1056/NEJMoa1613108
33. Sharp TM, Keating MK, Shieh W-J, Bhatnagar J, Bollweg BC, Levine R, et al. Clinical characteristics, histopathology, and tissue immunolocalization of chikungunya virus antigen in fatal cases. Clin Infect Dis. (2021) 73:e345–54. doi: 10.1093/cid/ciaa837
Keywords: chikungunya, arbovirus, mortality, emerging disease, pandemics, tropical diseases, excess deaths
Citation: Ribas Freitas AR, Lima Neto AS, Rodrigues R, Alves de Oliveira E, Andrade JS Jr and Cavalcanti LPG (2024) Excess mortality associated with chikungunya epidemic in Southeast Brazil, 2023. Front. Trop. Dis 5:1466207. doi: 10.3389/fitd.2024.1466207
Received: 17 July 2024; Accepted: 17 September 2024;
Published: 29 October 2024.
Edited by:
Cristina Possas, Oswaldo Cruz Foundation (Fiocruz), BrazilReviewed by:
Lara Ferrero Gómez, Universidade Jean Piaget de Cabo, Cabo VerdeHugo Carrillo-Ng, Northwestern University, United States
Copyright © 2024 Ribas Freitas, Lima Neto, Rodrigues, Alves de Oliveira, Andrade and Cavalcanti. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: André Ricardo Ribas Freitas, YW5kcmUuZnJlaXRhc0BzbG1hbmRpYy5lZHUuYnI=