 Cristina Possas
Cristina Possas João Baptista Risi
João Baptista Risi Akira Homma
Akira HommaIntroduction
The international initiatives for a global strategy to rapidly accelerate the development of new quality vaccines for a possible next Disease X pandemic contrast with the concerning sharp decline in immunization rates worldwide for many infectious diseases, including COVID-19 and influenza vaccines. Huge investments required for vaccine development and pandemic preparedness will only make sense if there is a simultaneous recovery of high vaccination coverage.
The debate on the determinants of the drastic global decline of vaccine coverage for many infectious diseases has been mostly focused so far on three main factors: the impacts of the COVID-19 pandemic resulting in the disruption of vaccination programs worldwide, unequal recovery in vaccination coverage across regions and income groups; and the impacts of vaccine hesitancy, a behavioral issue identified by WHO as one of the top 10 global threats (in 2019) to public health and that was aggravated in the pandemic (1).
Nevertheless, the global decline in immunization coverage, with the resurgence of vaccine-preventable diseases like measles started long before the COVID-19 pandemic. It started at the beginning of the last decade, affecting particularly developing countries, most of them located in the tropics.
Brazil illustrates this declining immunization scenario in the tropical region. A large country, with 5,570 municipalities and 208 million population, organized its internationally recognized National Immunization Program (NIP) in 1973, and which experienced a sharp decline in immunization rates starting 2012. Brazil is now among the countries with the lowest vaccination coverage in the world (Figure 1).
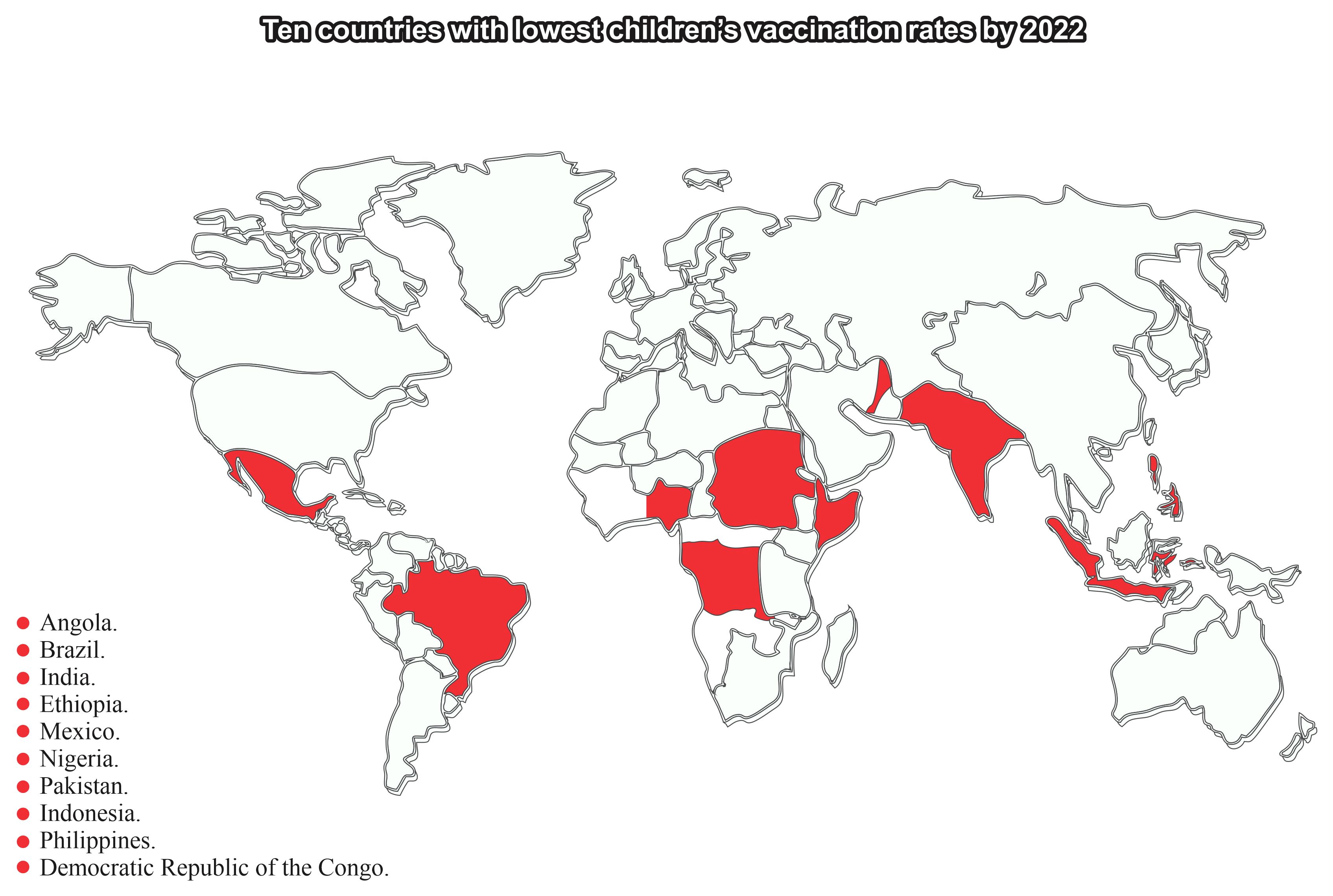
Figure 1 Ten countries with the lowest vaccination coverage for childhood vaccines in 2022. Source: Based on the data from WHO (2023) (2), elaborated by the authors.
A great national effort has historically been made in Brazil for measles elimination (3, 4). Nevertheless, in 2019, Brazil lost its measles elimination certificate issued in 2016 by PAHO/WHO, consequent to low vaccine coverage for the disease and a peak of cases between 2017 and 2021. Measles outbreak reported more than 20,000 cases in 2019 and has been followed by an alarming decline in vaccine coverage to 74.9% in 2021. This scenario started to improve from 2022 and 2023, when vaccine coverage increased respectively to 80.7% and 85.6%. A great effort by the Brazilian Ministry of Health will be necessary to recover the previous measles vaccination rate of 95% sustained uninterruptedly with slight variations from 2002 to 2012, according to a 2022 document from the National Council of Health Secretaries (5). Progress has been made recently by the Brazilian government: No measles cases have been reported in more than 1 year, and the National Immunization Program and the Ministry of Health are collaborating with PAHO/WHO to recover its measles elimination certificate.
The Bio-Manguinhos/Oswaldo Cruz Foundation is also contributing to this effort, implementing the project, Recovering High Vaccinations Coverage, working with the Amapá State (with the lowest immunization coverage in Brazil) and some municipalities in Paraiba State, with focus on municipalities and communities, to understand the causes of low immunization coverage. It showed that the entire society must be involved to bring back high vaccinations coverage (6, 7).
It is important to note that the Brazilian National Immunization Program (NIP) offers for free to the entire population, all vaccines in the national vaccination calendar available in the universal national health system (known as Brazilian National Unified System (SUS)), which is not a reality in many countries, intensifying their capacity to respond to the decline in immunization coverage.
The severity of this epidemiological scenario is illustrated by the very high risk of polio reintroduction in the country and in the Latin American and Caribbean region (LAC) region (Figure 2) due to very low vaccine coverage.
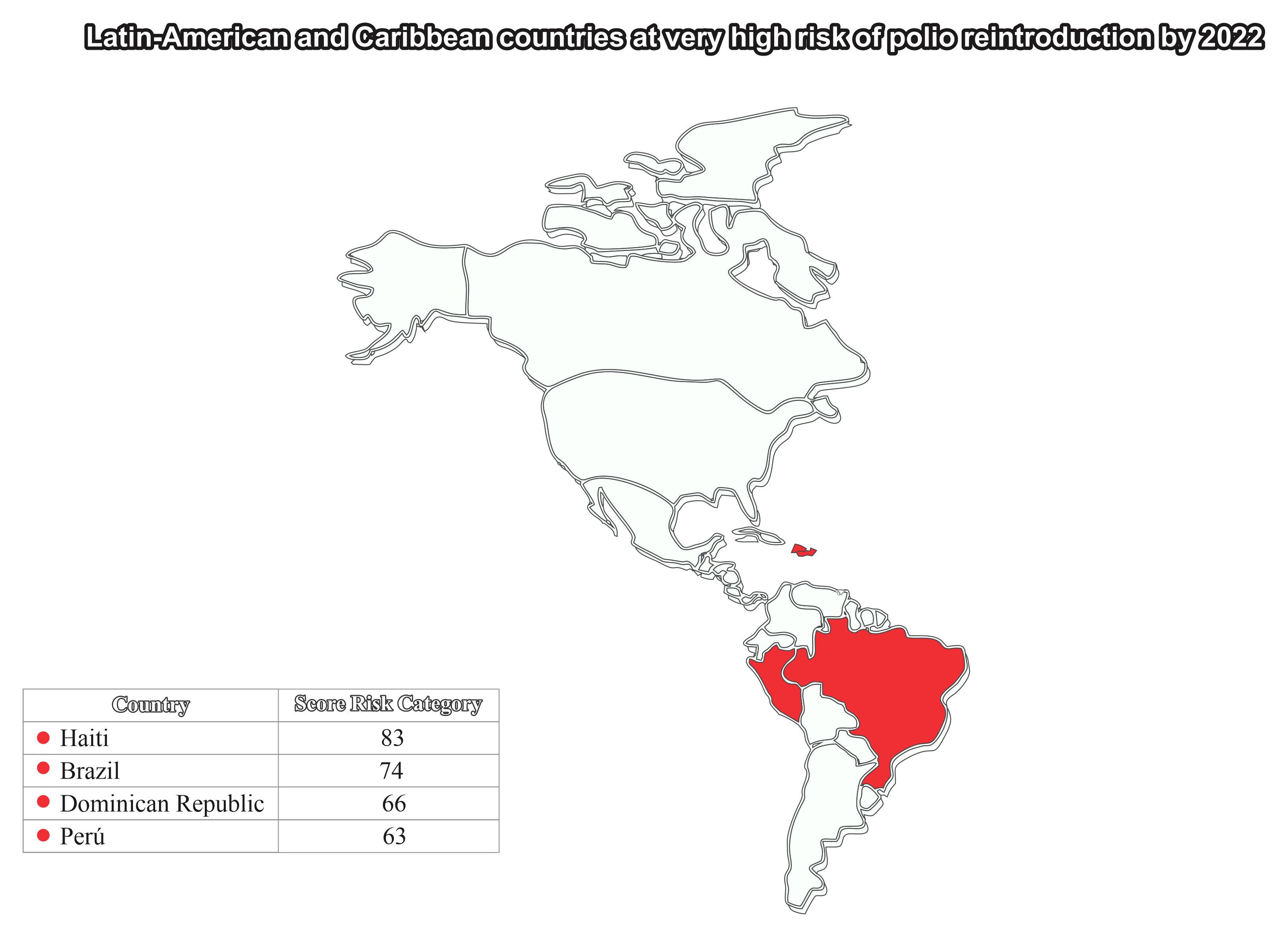
Figure 2 High risk of polio reintroduction in Brazil and the LAC region in 2022. Source: Based on the data from PAHO/WHO (2022) (8), elaborated by the authors.
Understanding the reasons for this scenario of sharp decline in immunization coverage, particularly in the most vulnerable developing countries, is a critical issue for Disease X preparedness and requires addressing the main barriers to vaccination, considering the complex interaction of cultural, behavioral, administrative, and socio-economic factors.
However, reversing this scenario under current circumstances implies setting goals that will be difficult to achieve and evaluate if general attention remains on simplistic explanations and solutions.
Many causes have been suggested. Among them is the assumption that people refuse vaccination for fear of adverse events, within what has been called “vaccine hesitancy” due to misinformation or the spread of fake news. Another cause would be a sense of collective security due to the virtual absence of diseases and epidemic outbreaks. Finally, mandatory vaccination has been pointed out as a possible solution to vaccine refusal, but so far, there is no evidence supporting this assumption.
Although “vaccine hesitancy” is a behavioral issue, it is an important global reality, and as underlined by WHO, it should be noted that Brazil had, for decades, a strong and long-standing culture of adherence to vaccination, responding very quickly to national campaigns and other immunization initiatives by local health services. Despite occasional regulations that made vaccination mandatory in Brazil, the success historically achieved in immunization practices has never been attributed to mandatory measures. On the contrary, the best results achieved were due to the persistence of efforts to convince the population to get vaccinated.
The main causes of the decline in immunization in Brazil are related to difficulties in sustaining the NIP as a federal program, responsible for promoting, financing, and managing activities carried out by state and municipal governments. This issue is quite critical due to the country’s geography and its socioeconomic and political-administrative diversity. It is noteworthy that other federal initiatives within the national health system (SUS) compete with NIP in promoting decentralized efforts at state level.
The very high risk of polio reintroduction in Brazil illustrates this scenario well, as indicated in Figure 2. Brazil historically had a strong participation in global efforts to eradicate polio (9, 10).
Brazil sustained very high vaccination coverage for all vaccines in the national calendar for decades and the reasons for this decline starting in 2012 must be examined carefully. A document published by CONASS (the Brazilian National Council of Health Secretaries) on October 2012 confirmed the history of success in immunization and declared that Brazil had sustained 95% of vaccination coverage in the last 10 years for most of the vaccines in the children’s calendar and vaccination campaigns.
Nevertheless, this successful scenario has been dramatically reversed from 2012. A good example is the polio national immunization coverage: from 95%–100% in the early 2010s, it continuously declined to unacceptable rates of 71% in 2021 and 77% in 2022, according to the Brazilian NIP and WHO (2).
The reasons for the sharp drop in vaccination coverage must be analyzed in the scope of a historical process in which two main vectors can be identified. The first refers to the accelerated expansion of the NIP in recent years, which required greater effort from the program’s management structure at the federal level. New vaccines were incorporated into the vaccination calendar, with specific indications and procedures that are more difficult for the public to understand and that required better training of health professionals. The detrimental effects of these factors on the operationalization, management, and evaluation of the NIP need to be better understood at the level of basic health units responsible for vaccination.
The Brazilian 1988 Constitution establishes federative principles for the national health system (SUS), which provides for coordinated actions between the federal, state, and municipal governments, with the latter being responsible for carrying out immunization activities.
However, the NIP has become increasingly dependent on federal support from the Ministry of Health for technical and programmatic guidelines, as well as budgetary resources to ensure a regular supply of more technologically advanced and expensive vaccines. Furthermore, the expansion of NIP’s responsibilities was not accompanied by corresponding funding.
The performance of NIP was affected over time by budgetary and managerial restrictions at state and municipal levels, which made it difficult to comply with new operational requirements. In this context, there was a progressive decline in vaccination coverage, which could not be accurately measured by continuous data recording systems at the local level.
Around the year of 2010, an in-depth assessment of NIP in Brazil was needed to recommend strategic interventions aiming to re-establish harmony at all levels, between the network of services, health professionals, and society’s perception of the program.
However, historical events moved in another direction. From 2012 onward, a sequence of political and administrative crises affected the stability of the federal government, and as a result, the scheduling of vaccination activities was also affected. At the beginning of 2020, the COVID-19 pandemic broke out and caused serious damage on global health, the economy, and social order, strongly impacting the provision of health services. Extreme control measures were recommended internationally at the time, such as the extemporaneous administration of vaccines in the process of technological development, which undermined the structural basis and protagonism of the NIP.
Possible solutions to ensure the full operations of Brazil’s NIP depend on directly addressing all these issues, and it is not enough for them to be addressed punctually or tangentially. There should be a serious attempt to address the problem, avoid politically motivated debate, and be open to expert criticisms and suggestions that can benefit the program. Vaccination efforts must return to the SUS agenda, benefiting the entire Brazilian society.
Finally, the proposal for a strategy to develop new vaccines in Brazil depends on a strong national initiative to revitalize the NIP and the governmental ability to recognize the most important causes of the PNI’s programmatic failure, and to overcome the distortions caused by the COVID-19 pandemic and its deleterious effects associated with the international challenges brought about by COVID-19 that also directly and adversely affected Brazil.
From an international perspective, a correct analysis of the reasons for the deteriorating vaccine coverage, affecting particularly the poorest and more vulnerable populations in developing countries is needed. Lessons from the Brazilian experience can help these countries in understanding the determinants of the sharp decline in immunization coverage in developing countries, affected by social exclusion and extreme poverty, that go far beyond the simplistic generalization of the “vaccine hesitancy” assumption. These lessons can contribute to supporting them to strengthen their national immunization programs and prepare for a possible Disease X pandemic, and in the process, help achieve the sustainable development goals of the UN’s 2030 Agenda.
Author contributions
CP: Writing – original draft, Writing – review & editing. JR: Writing – original draft, Writing – review & editing. AH: Writing – original draft, Writing – review & editing.
Funding
The authors declare financial support was received for the research of this article and thank Bio-Manguinhos, Oswaldo Cruz Foundation, for the support to this research. Thanks to Frontiers for funding the APC for this article.
Acknowledgments
The authors thank José Viña for the design of figures.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. WHO. Ten threats to global health in 2019. Geneva: WHO News Room (2019). Available at: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019.
2. WHO. immunization coverage, fact sheet. Geneva: WHO News Room (2023). Available at: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage.
3. Homma A, Possas C, Menezes R, Risi JB. Eradication of Smallpox and Prospects for Measles eradication: lessons from the Brazilian experience. J Vaccines Vaccin S. (2012) 3:2.
4. Possas C, Homma A, Risi JB Jr., Ho PL, Camacho LAB, Freire MS, et al. Vacinas e vacinações no Brasil: Agenda 2030 na perspectiva do desenvolvimento sustentável. In: Homma A, Possas CA, Noronha J, Gadelha P, editors. Vacinas e vacinação no Brasil: horizontes para os próximos 20 anos. Edições Livres, Rio de Janeiro (2020). p. 250.
5. CONASS – National Council of Health Secretaries. Brazil has maintained 95% vaccine coverage in the last 10 years, 2012. In: O Brasil manteve 95% da sua cobertura vacinal nos últimos 10 anos (2012). Brasilia, DF, Brazil: CONASS. Available at: https://www.conass.org.br/brasil-mantem-95-de-cobertura-vacinal-nos-ultimos-10-anos/.
6. Bio-Manguinhos, Oswaldo Cruz Foundation. Pela reconquista das altas coberturas vacinais. Relatório final do Projeto 2021-293. In: For recovering high vaccination coverage. Final Project Report 2021-2023. Rio de Janeiro, RJ, Brazil: Manole Editor and Fiocruz (2024).
7. Homma A, Maia MD, Azevedo IC, Figueiredo IL, Gomes LB, Pereira CV, et al. Pela reconquista das altas coberturas vacinais. In: Cadernos de Saúde Pública, vol. 39. Rio de Janeiro: National School of Public Health, Oswaldo Cruz Foundation (2023) 39. doi: 10.1590/0102-311xpt240022
8. PAHO/WHO. Analysis of regional risk for polio reintroduction in the Americas. Washington DC, US: RCC (2022).
9. Risi JB. The control of poliomyelitis in Brazil. Rev Infect Dis. (1984). doi: 10.1093/clinids/6.Supplement_2.S400
Keywords: vaccine coverage, immunization, disease X, preparedness, emerging diseases
Citation: Possas C, Risi JB and Homma A (2024) Vaccine coverage in the tropics: sharp decline in immunization and implications for Disease X preparedness and the UN 2030 agenda. Front. Trop. Dis 5:1441970. doi: 10.3389/fitd.2024.1441970
Received: 31 May 2024; Accepted: 01 July 2024;
Published: 06 August 2024.
Edited by:
Malcolm Scott Duthie, HDT Biotech Corporation, United StatesReviewed by:
Isabela Gobbo Ferreira, University of São Paulo, BrazilCopyright © 2024 Possas, Risi and Homma. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cristina Possas, Y3Jpc3RpbmEucG9zc2FzQGJpby5maW9jcnV6LmJy