 Alfred Kwesi Manyeh1*
Alfred Kwesi Manyeh1* Rosemond Akpene Ekey2
Rosemond Akpene Ekey2 Rukaya Dongu Kamaldeen1
Rukaya Dongu Kamaldeen1 Dorothy Fosu1
Dorothy Fosu1 Saviour Edem Vidzro1
Saviour Edem Vidzro1 Maxwell Dalaba1
Maxwell Dalaba1- 1Institute of Health Research, University of Health and Allied Sciences, Ho, Volta Region, Ghana
- 2Shai Osudoku District Health Directorate, Ghana Health Service, Dodowa, Greater Accra Region, Ghana
Background: Female genital schistosomiasis (FGS) is among the most neglected of tropical diseases. FGS remains underreported, under and misdiagnosed and mostly untreated. This neglected epidemic disproportionately affects communities already burdened by HIV and cervical cancer. The study aims to assess FGS knowledge, attitude, and practices and associated factors in communities in the Shai-Osudoku District of Ghana.
Method: The study employed an analytical cross-sectional design, utilizing quantitative methods for data collection from 161 community members. Analysis was conducted using STATA 18, included both descriptive statistics and simple logistic regression.
Results: About half (50.31%) of the respondents demonstrated poor knowledge of FGS. Furthermore, 65.84% of the respondents exhibited a poor attitude towards FGS, Poor practice related to FGS were also observed in 60.25% of the respondents. Regression analysis showed significant associations between various factors and knowledge, attitudes, and practices regarding FGS. Specifically, married women were found to have 54% lower odds of possessing good knowledge about FGS compared single women. (AOR=0.46, 95%CI= 0.22-0.94). Respondents with poor socioeconomic status displayed 76% higher odds of engaging in good practices compared to respondents those in the poorest socioeconomic status. (AOR=0.24, 95%CI=0.06-0.96).
Conclusion: Comprehensive, context-specific interventions are necessary to address the multifaceted challenges associated with FGS. Targeted education and awareness campaigns are crucial to improve understanding of FGS, and addressing socio-economic factors that influence attitudes and practices related to the disease is essential.
Background
Female genital schistosomiasis (FGS) is a neglected tropical disease prevalent in sub-Saharan Africa, caused by the parasitic flatworm Schistosoma haematobium. FGS is characterized by the deposition of schistosome eggs in the genital tract, leading to a range of gynecological and reproductive health complications (1). The burden of FGS is exacerbated by its association with other major public health challenges such as HIV (2). Furthermore, the socio-economic impact of FGS is substantial, with implications for productivity, quality of life, and healthcare costs (3).
Despite the significant impact of FGS on the health and well-being of affected individuals, the disease remains underreported, underdiagnosed, and largely untreated, and there is a notable lack of awareness and understanding of FGS among both affected communities and healthcare providers (1, 3).
The Shai-Osudoku District, located in the Greater Accra Region of Ghana (4), represents a setting where FGS is prevalent, yet knowledge, attitudes, and practices related to the disease remain poorly understood. This study aims to address these knowledge gaps by conducting a comprehensive assessment of FGS knowledge, attitudes, and practices, as well as the socio-economic impact of the disease, within communities in the Shai-Osudoku District.
The findings of this study are expected to contribute to a deeper understanding of FGS and its socio-economic impact, and to inform the development of targeted education, awareness, and intervention programs that are context-specific and responsive to the needs of the affected communities in the Shai-Osudoku District.
Method
Study design
This study used a quantitative analytical cross-sectional design. The researchers used this study design to get comprehensive understanding of the FGS knowledge, attitude, and practices and associated factors in communities in the Shai-Osudoku District of Ghana to inform future studies, interventions, and public health strategies.
Sampling strategy
In the Shai Osudoku district of Ghana, four communities (Asutsuare, Domelam, Kadjanya and No-Smoking) with the highest prevalence of schistosomiasis were purposively selected for this study. Using the Expanded Program for Immunisation (EPI) cluster sampling technique, 40 clusters were systematically chosen (10 clusters per community) with at least 7 women or girls aged 18 years or older per cluster. Then, a simple random sampling method was applied to select 4 participants from each cluster. This was done by writing ‘Yes’ or ‘No’ on pieces of paper, folding them, and placing them in a container. The container was shaken, and the women and girls picked one paper at a time. Those who picked ‘Yes’ were included in the study.
The sample size was calculated using the formula n = Z2pq/d2, where n is the sample size, Z is the standard normal deviation at the desired confidence level (set at 1.96 for a 95% confidence level), p is the estimated prevalence of schistosomiasis in the district (set at 90%), q is 1-p, and d is the desired level of precision (set at 5%). The sample size was increased by 17% to compensate for nonresponse and missing data.
Data collection
Data was collected using a structured questionnaire that was administered to selected adult community members (18 years and older) between November and December 2023. The questionnaire was developed based on a review of the literature on FGS knowledge (5, 6) attitudes (6, 7), and practices (5, 7), and was pretested in a sample of households in the district prior to the start of data collection. The questionnaire includes questions on socio-demographic characteristics, knowledge of FGS, attitudes towards FGS, and practices related to FGS prevention and treatment. The questionnaire also includes questions on the socio-economic impact of FGS, including its effect on productivity, quality of life, and healthcare costs. Five graduate level data collectors were recruited and trained for 3 days for the data collection.
Females aged 18 years and above in the selected communities who agreed to participate in the study were included.
Female Genital Schistosomiasis is defined in this study as an untreated and complicated Schistosoma infection in women, which has progressed to cause damage and complications in the female genital tract.
Data analysis
Data was entered into EpiData and exported to STATA 18 software for cleaning and analysis. Descriptive statistics were used to summarize the socio-demographic characteristics of the study population, as well as their knowledge, attitudes, and practices related to FGS. Univariable analysis was used to examine the association between socio-demographic factors and FGS knowledge, attitudes, and practices. Multivariate logistic regression analysis was used to identify factors associated with FGS knowledge, attitudes, and practices, while controlling for potential confounding variables. Only variables statistically significant at 95% confidence level at the univariable analysis level were included in the multivariable model.
Measurement of knowledge, attitude and practice variables
These variables were measured by correct answers to signs associated with FGS, FGS prevention methods, and how FGS is acquired.
The variables used for the knowledge score include awareness of FGS, source of information, knowledge of transmission, causes, symptoms, and treatment. Variables for attitude includes history of testing, confidence in recognizing signs and symptoms, encountering cases in clinical practice, interest in participating in prevention and control programs and health seeking behavior.
Ethical considerations
The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. Ethical approval was obtained from the Ghana Health Service Ethic Review Committee (GHS-ERC 004/03/23). Informed consent was obtained from all study participants prior to their inclusion in the study. Participants were assured of their right to refuse participation or to withdraw from the study at any time without penalty. All data was kept confidential and anonymous and was used for the purposes of this study only.
Results
Socio-demographic characteristics of respondents
The study included 161 females from 4 communities in the Shai Osudoku District of the Greater Accra Region of Ghana. The mean age of the participants was approximately ±32.5, and the comparative majority (39.1%) were 26-39 years old. Most of the participants were married (50.9%) and had completed Junior High School (39.8%). The majority (61.5%) of the respondents belonged to the Dangme ethnic group and (94.4%) of them were Christians. Approximately 35.4% of the participants were traders (Table 1).
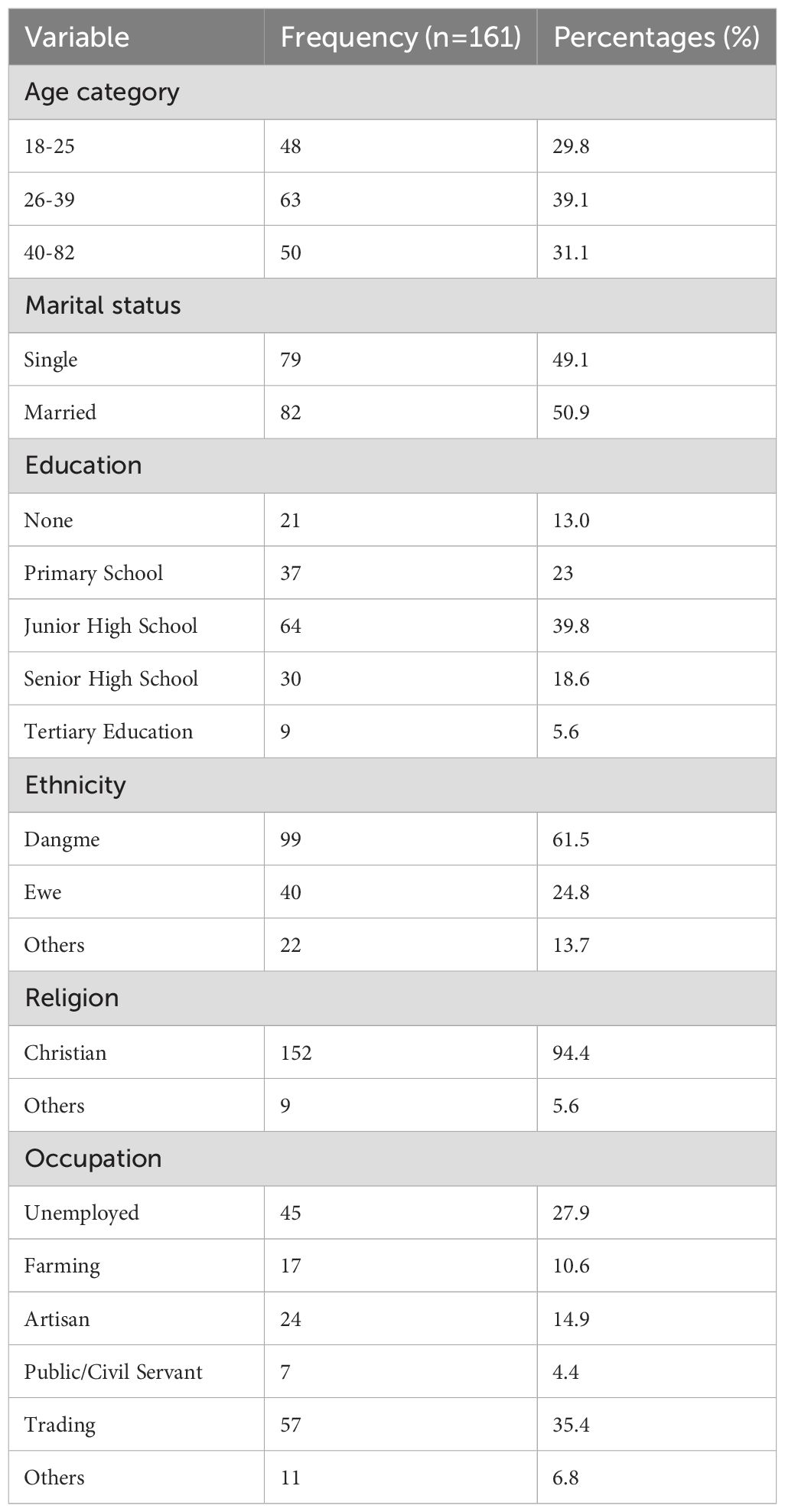
Table 1. Background characteristics.
Knowledge of FGS
Among the 161 participants in the study, (92.5%) said they had heard of urinating blood disease.
About 42.1% believe that FGS is caused by worms in streams, and most of them (61.6%) indicated blood in urine as a sign of FGS. A majority (54.9%) of them said that swimming in infested water is the most recognized mode of infection, while 43.1% recognized preventive measures as avoiding contact with infested water. Most of the participants (59.6%) said it could be treated with hospital medicine (praziquantel). The majority (66.2%) believe that FGS does not cause infertility in women (Table 2).
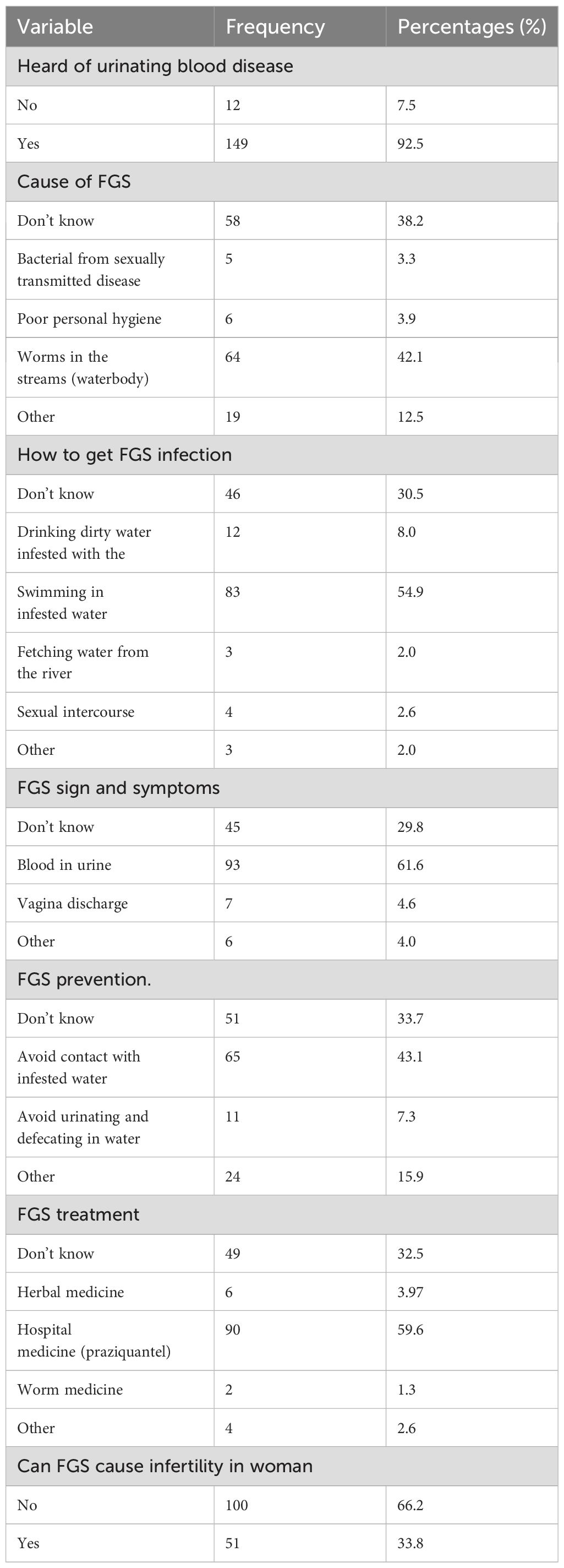
Table 2. Knowledge of FGS.
Attitude and practices towards FGS
Off the 161 respondents in the study, 63.8% agreed that FGS is a serious disease that affects women and young girls of reproductive age. The majority (78.2%) disagrees that FGS is a disease that affects women who cheat on their husbands. Most of the participants (80.8%) disagree that FGS is a disease that is spiritual and caused by the gods. A substantial majority (72.7%) agree that FGS can be cured using a hospital drug, praziquantel. Almost 81% of them express a positive attitude, agreeing that they would tell their partner or relative if they suspected they had FGS symptoms (Table 3).
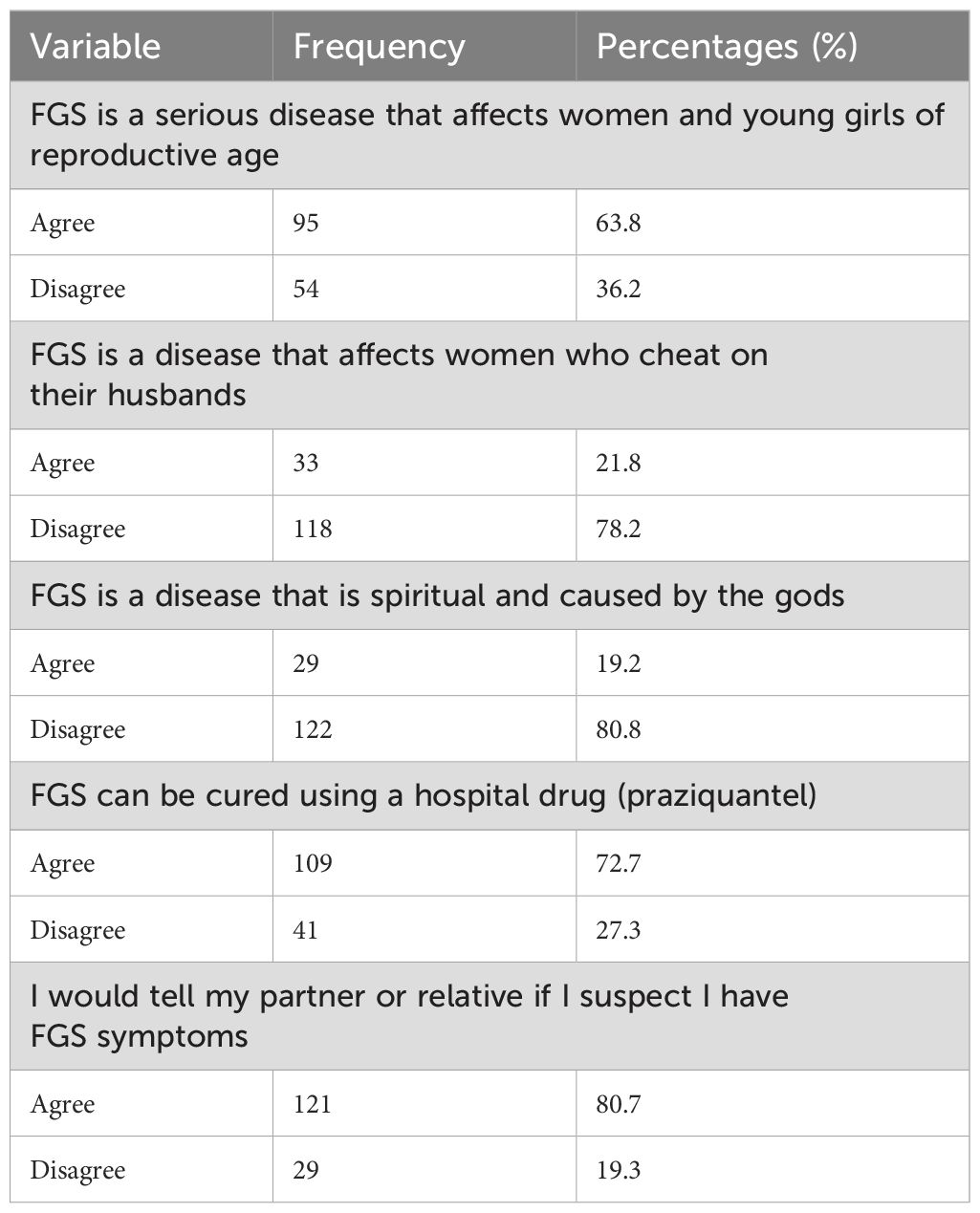
Table 3. Attitude towards FGS.
Practices of female genital schistosomiasis
The majority (58.7%) of the respondents said they do not have contact with water. Among those who reported having contact with a water body, the majority (31.3%) stated that they have contact every day (Table 4).
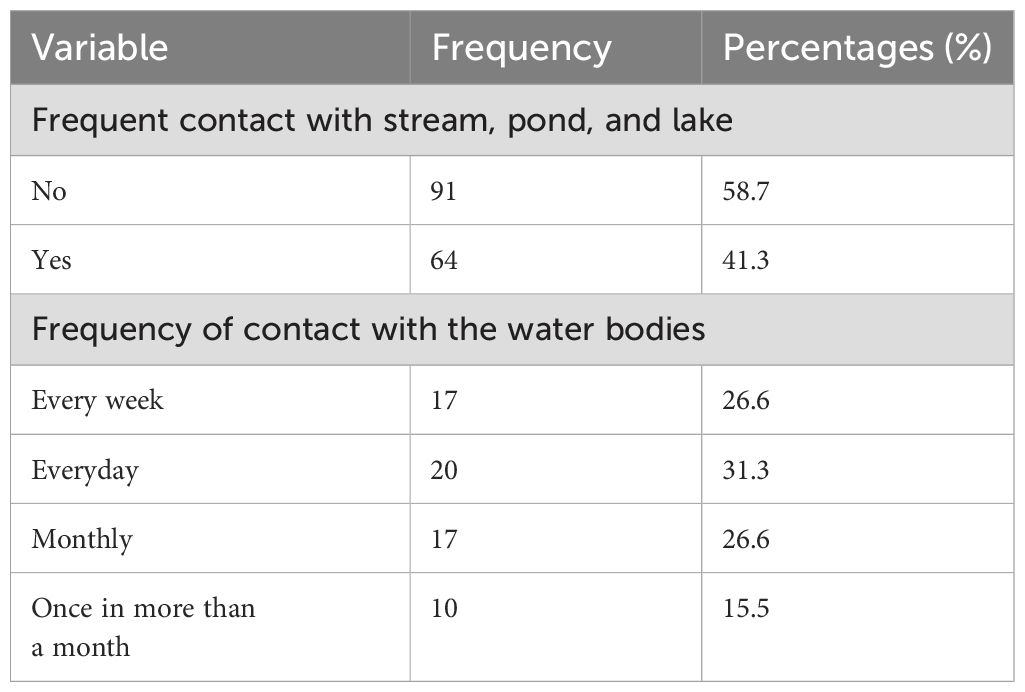
Table 4. Practices towards FGS.
Socio-economic impact
Of the 161 participants, 87% of them do not have a fixed amount of income while 38.5% of them have their primary source of income from government or private jobs. In addition, 38.5% of respondents have their total combined income for 12 months to be >4500 Ghana cedi (338USD). Most (67.1%) of the respondents pay for their healthcare expenses using both insurance and out-of-pocket.
Nearly half (46.0%) of respondents reported living with 2-3 females, and the majority (95.0%) of them indicated that one (1) female had ever had FGS. The majority (67.1%) of the respondents reported that their main source of water for washing/bathing/cooking and drinking (62.1%) was pipe water.
Nearly all (90.7%) of all the respondents have metal as their primary roof material. A larger proportion (49.7%) of the respondents belonged to the middle wealth category and none belonged to the rich category (Table 5).
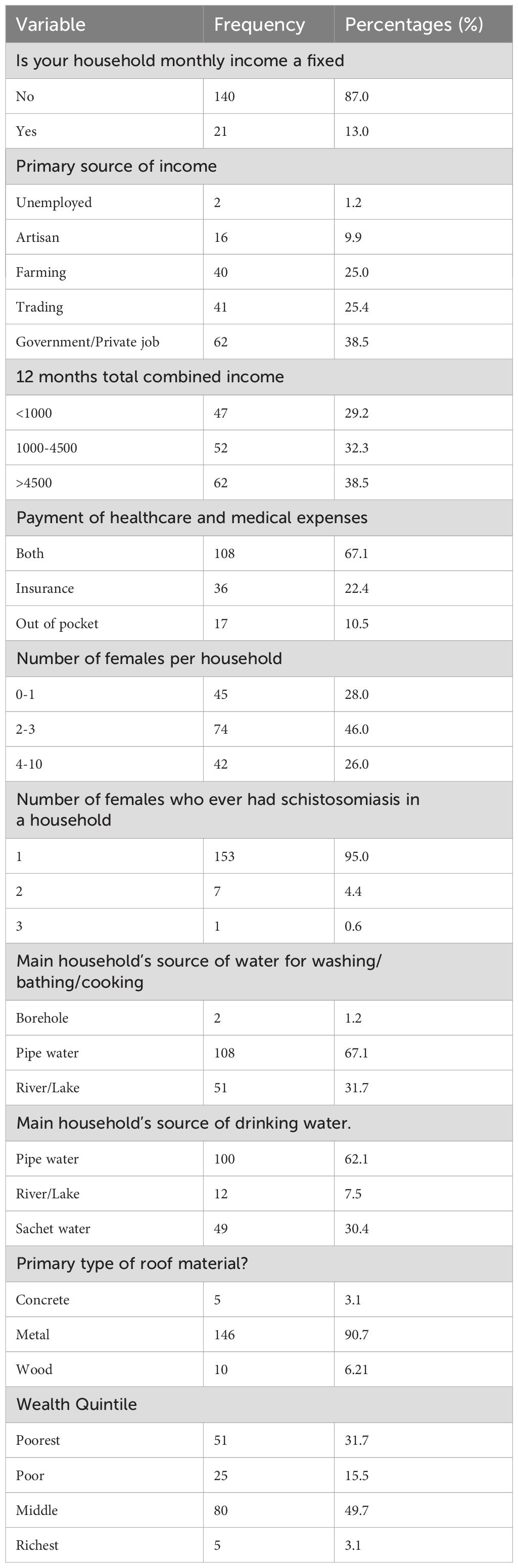
Table 5. Socio-economic impact.
Association between knowledge and socio-demographic variables
The regression analysis revealed significant associations between various factors and knowledge/practices related to FGS (Table 6). Specifically, married respondents had 54% lower odds of knowledge on FGS compared to single participants (AOR=0.46, 95%CI=0.22-0.94). In contrast, those with primary level education were over three times more likely to have knowledge of FGS compared to those with no formal education (AOR: 3.43, 95%CI=1.05-11.43). Additionally, poor participants were 77% less likely to have good practices compared to the poorest participants (AOR: 0.33, 95%CI=0.11-0.96). Notably, frequent contact with water was associated with poor knowledge, with participants being 1.90 times more likely to have poor knowledge compared to those without frequent contact (COR=1.90, 95%CI=0.99-3.64).

Table 6. Association between knowledge and socio-demographic variables.
Discussion
Schistosomiasis, a neglected tropical disease caused by parasitic worms, persists as a significant public health challenge in Ghana, particularly in the Shai-Osudoku District. This study investigated the knowledge, attitudes, and practices (KAP) surrounding Female Genital Schistosomiasis (FGS), as well as the socioeconomic impact of the disease in local communities. The findings offer valuable insights into the understanding of schistosomiasis, revealing that a high percentage of participants were familiar with the disease, mostly associating it with specific symptoms and modes of transmission, thereby shedding light on the factors influencing its prevalence and impact in the region.
Furthermore, Kjetland et al. (2012) conducted a study in Zimbabwe and South Africa, highlighting the importance of addressing socio-economic factors and cultural beliefs in improving knowledge and practices related to FGS. Their findings revealed that cultural taboos and stigmatization were significant barriers to seeking care for FGS (1).
A systematic review revealed that there is a lack of awareness and knowledge about FGS among affected communities (1). This lack of knowledge often results in misconceptions and stigmatization, impacting the attitudes towards the disease. Additionally, the study found that the practices related to FGS, such as seeking treatment and preventive measures, were influenced by the level of knowledge and the prevailing attitudes towards the disease (1).
Efforts to raise awareness and improve knowledge of FGS are essential for addressing the impact of the disease on women’s health. This includes integrating FGS screening and treatment into existing reproductive health programs, as well as providing education and training for healthcare providers on the diagnosis and management of FGS as suggested elsewhere (8).
The study’s findings reveal a mix of positive and negative attitudes and practices regarding FGS within the study population. While most participants acknowledged the disease’s severity and expressed willingness to seek treatment, a significant proportion held poor attitudes and practices, highlighting the need to address misconceptions and promote positive health-seeking behaviors. This aligns with previous research by Kjetland et al. (2012), which found that women with FGS symptoms often sought treatment from traditional healers due to cultural beliefs and stigma surrounding the disease (1). To combat this, community-based education and awareness campaigns, coupled with increased access to diagnosis and treatment, are essential to improve attitudes and practices related to FGS, ultimately reducing the disease’s burden and promoting better health outcomes.
The need for increased awareness and education to address FGS in vulnerable population has been emphasized (9). Community-based interventions like health education programs and mass drug administration campaigns can improve attitudes and practices related to FGS. Similarly, a comprehensive review of neglected tropical diseases in sub-Saharan Africa highlights the importance of addressing attitudes and practices related to FGS through increased awareness and education, as well as improved access to diagnosis and treatment (10). By implementing community-based education and awareness campaigns, and increasing access to diagnosis and treatment, attitudes and practices related to FGS can be improved, ultimately reducing the disease’s burden on affected communities and enhancing overall health outcomes.
FGS has a profound socio-economic impact on affected individuals, families, and communities, as evident in the current study’s findings on income, healthcare expenses, living conditions, and access to basic amenities. The high reliance on out-of-pocket healthcare expenses and prevalence of low-income households highlight the need for targeted interventions to address socio-economic barriers to schistosomiasis prevention and treatment (11). The socio-economic impact of FGS is further exacerbated by increased healthcare costs, reduced productivity, and the burden of managing FGS and HIV co-infection (2), emphasizing the need for integrated approaches to address both diseases and their consequences. Studies in Zimbabwe, Zambia (12), and sub-Saharan Africa (10) have consistently shown the significant socio-economic implications of FGS on women and girls, including impacts on reproductive health, quality of life, and productivity, underscoring the need for increased control measures, awareness, and holistic approaches to mitigate the socio-economic burden of FGS and other neglected tropical diseases on affected communities.
The socio-economic impact of FGS, including its association with increased healthcare costs, reduced productivity, and implications for reproductive health and overall well-being cannot be overemphasized. Addressing the socio-economic burden of FGS requires integrated control measures, awareness campaigns, and targeted interventions to improve the quality of life and economic prospects for affected individuals and communities.
The study’s regression analysis revealed significant associations between knowledge, attitudes, practices, and socio-demographic factors, including lower odds of knowledge on FGS among married participants and a link between practices and socio-economic status. These findings align with Mazigo et al.’s (2010) study, which showed that marital status and socio-economic status influenced knowledge and practices related to schistosomiasis/FGS (13). The current study highlights the need for targeted educational interventions for married individuals and addressing economic barriers to accessing preventive and treatment measures. It also underscores the importance of tailored interventions considering the specific socio-demographic characteristics of the target population, and comprehensive educational campaigns and community-based interventions to improve awareness, change attitudes, and promote appropriate practices for FGS prevention and management in affected populations, particularly in rural Sub-Saharan African communities.
The study has limitations, including a small sample size from a specific geographic area, which may not be representative of the broader population. The methodology may not fully capture the socio-economic impact of FGS, and potential confounding variables may not have been accounted for. These limitations should be considered when interpreting the findings and highlight opportunities for further research to address these gaps.
Conclusion
The study revealed that there is a significant lack of knowledge, poor attitudes, and practices related to female genital schistosomiasis among the participants in the Shai-Osudoku District of Ghana. The findings underscore the urgent need for comprehensive, context-specific interventions to address the multifaceted challenges associated with FGS. Additionally, targeted education and awareness campaigns are crucial to improve understanding of FGS, while addressing socio-economic and cultural factors that influence attitudes and practices related to the disease is essential. The study’s results highlight the importance of tailored public health efforts to effectively combat FGS and improve the overall well-being of the communities in the region.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The human study was approved by Ghana Health Service Ethic Review Committee. The study was conducted in accordance with the local legislation and institutional requirements. Study participants provided their written informed consent to participate in this study.
Author contributions
AM: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. RE: Conceptualization, Formal analysis, Investigation, Visualization, Writing – original draft, Writing – review & editing. RK: Data curation, Formal analysis, Investigation, Methodology, Project administration, Visualization, Writing – review & editing. DF: Conceptualization, Data curation, Formal analysis, Investigation, Project administration, Writing – review & editing. SV: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Validation, Writing – original draft, Writing – review & editing. MD: Conceptualization, Formal analysis, Investigation, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The study was funded by Royal Society of Tropical Medicine and Hygiene Small Grant Scheme. The funders did not participate in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Acknowledgments
The authors express their appreciation to all stakeholders who participated in the study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer MA declared a shared parent affiliation with the author(s) to the handling editor at the time of review.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
FGS, Female Genital Schistosomiasis; MDA, Mass drug administration; NTD, Neglected tropical diseases; HIV, human immunodeficiency virus.
References
1. Kjetland EF, Ndhlovu PD, Gomo E, Mduluza T, Midzi N, Gwanzura L, et al. Female genital schistosomiasis: a systematic review of the literature from sub-Saharan Africa. Lancet Infect Dis. (2012) 12:733–41.
2. Kjetland EF, Ndhlovu PD, Gomo E, Mduluza T, Midzi N, Gwanzura L, et al. Association between genital schistosomiasis and HIV in rural Zimbabwean women. AIDS. (2006) 20:593–600. doi: 10.1097/01.aids.0000210614.45212.0a
3. Hotez PJ, Alvarado M, Basáñez M-G, Bolliger I, Bourne R, Boussinesq M, et al. The global burden of disease study 2010: interpretation and implications for the neglected tropical diseases. PLoS Negl Trop Dis. (2014) 8:e2865. doi: 10.1371/journal.pntd.0002865
4. Ghana Statistical Service (GSS). ICF: Ghana Demographic and Health Survey 2022: Summary Report. Accra, Ghana: Rockville, Maryland, USA: GSS and ICF (2023).
5. Kukula VA, MacPherson EE, Tsey IH, Stothard JR, Theobald S, Gyapong M. A major hurdle in the elimination of urogenital schistosomiasis revealed: Identifying key gaps in knowledge and understanding of female genital schistosomiasis within communities and local health workers. PloS Negl Trop Dis. (2019) 13:e0007207. doi: 10.1371/journal.pntd.0007207
6. Yirenya-Tawiah DR, Ackumey MM, Bosompem KM. Knowledge and awareness of genital involvement and reproductive health consequences of urogenital schistosomiasis in endemic communities in Ghana: a cross-sectional study. Reprod Health. (2016) 13:117. doi: 10.1186/s12978-016-0238-5
7. Yirenya-Tawiah D, Amoah C, Apea-Kubi KA, Dade M, Ackumey M, Annang T, et al. A survey of female genital schistosomiasis of the lower reproductive tract in the volta basin of Ghana. Ghana Med J. (2011) 45:16–21. doi: 10.4314/gmj.v45i1.68917
8. Kjetland EF, Kurewa EN, Ndhlovu PD, Midzi N, Gomo E, Mduluza T, et al. Female genital schistosomiasis—a differential diagnosis to sexually transmitted disease: genital itch and vaginal discharge as indicators of genital Schistosoma haematobium morbidity in a cross-sectional study in endemic rural Zimbabwe. Trop Med Int Health. (2021) 17:380–9.
9. Stothard JR, Sousa-Figueiredo JC, Betson M, Bustinduy A, Reinhard-Rupp J. Schistosomiasis in African infants and preschool children: let them now be treated! Trends Parasitol. (2013) 29:197–205.
10. Hotez PJ, Kamath A. Neglected tropical diseases in sub-Saharan Africa: review of their prevalence, distribution, and disease burden. PLoS Negl Trop Dis. (2009) 3:e412. doi: 10.1371/journal.pntd.0000412
11. Lo NC, Bezerra FS, Colley DG, Fleming FM, Homeida M, Kabatereine N, et al. Review of 2022 WHO guidelines on the control and elimination of schistosomiasis. Lancet Infect Dis. (2022) 22(11):e327–e335. doi: 10.1016/S1473-3099(22)00221-3
12. Kjetland EF, Kurewa EN, Ndhlovu PD, Midzi N, Gomo E, Mduluza T, et al. Female genital schistosomiasis in Zimbabwe and Zambia: a call for control and awareness. Reprod Health Matters. (2010) 18:18–26.
Keywords: female genital schistosomiasis, knowledge, attitude, practice, Ghana, neglected tropical diseases
Citation: Manyeh AK, Ekey RA, Kamaldeen RD, Fosu D, Vidzro SE and Dalaba M (2024) The hidden burden of female genital schistosomiasis: a cross-sectional study of knowledge, attitudes, and practices in Ghanaian communities. Front. Trop. Dis 5:1427402. doi: 10.3389/fitd.2024.1427402
Received: 03 May 2024; Accepted: 20 August 2024;
Published: 12 September 2024.
Edited by:
Amy S. Sturt, University of London, United KingdomReviewed by:
Hlengiwe Gwebu, University of Fort Hare, South AfricaYabo Josiane Honkpehedji, Centre de Recherche Médicales de Lambaréné, Gabon
Michael Amoh, University of Health and Allied Sciences, Ghana
Copyright © 2024 Manyeh, Ekey, Kamaldeen, Fosu, Vidzro and Dalaba. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alfred Kwesi Manyeh, YWttYW55ZWhAdWhhcy5lZHUuZ2g=