 Najim Z. Alshahrani1*
Najim Z. Alshahrani1* Suzan M. Bukhari2
Suzan M. Bukhari2 Lujain M. Bukhari3
Lujain M. Bukhari3 Lama S. Alghamdi2
Lama S. Alghamdi2 Shouq R. Aljohani2
Shouq R. Aljohani2 Radwan A. Ghurab3
Radwan A. Ghurab3- 1Department of Family and Community Medicine, Faculty of Medicine, University of Jeddah, Jeddah, Saudi Arabia
- 2Faculty of Medicine, University of Jeddah, Jeddah, Saudi Arabia
- 3Department of Family Medicine, Ministry of Health, Jeddah, Saudi Arabia
Background: Recent HFMD cases have surged in Saudi Arabia, highlighting a literature gap on healthcare professionals’ understanding and attitudes towards HFMD. This study evaluates and compares knowledge and attitudes among medical students and physicians at the University of Jeddah.
Methods: An analytical cross-sectional study design was employed to survey medical students and physicians at the University of Jeddah from 1 November 2023 to 1 January 2024. Participants were assessed using multiple-item scales to measure their knowledge (max score: 23) and attitudes (max score: 32) towards HFMD. Logistic regression analysis was utilized to explore the association between various independent factors and the outcomes of interest (knowledge and attitude levels).
Results: A total of 317 responses (260 medical students and 57 physicians) were analyzed. Among medical students, the analysis of knowledge scores revealed a mean score of 6.36, with a standard deviation (SD) of 5.68, a median score of 6, and an interquartile range (IQR) of 0-10. About 31.6% of the students demonstrated adequate knowledge of HFMD. Notably, students who had received education on HFMD showed significantly higher levels of knowledge compared to those who had not. For student attitudes towards HFMD, the mean score in the attitude group was 20.1, with a SD of 4.2, a median of 20, and an IQR of 16 to 23. Among physicians, the mean knowledge score for those with adequate knowledge was 14.3, with a SD of 4.3 and a median of 15, and an IQR of 12-18. Furthermore, 54.4% of the physicians showed good knowledge, with being single significantly associated with this higher level of knowledge. In terms of attitudes among physicians, the mean score for the positive attitude group was 19.8, with a SD of 5.92, and a median score of 20, with an IQR of 16 to 25.
Conclusion: The study highlights a significant gap in knowledge and attitudes towards HFMD among healthcare professionals in Saudi Arabia.
1 Introduction
Hand, foot, and mouth disease (HFMD) is a prevalent viral infection in children, predominantly caused by enteroviruses (1, 2). This illness is characterized by a trio of symptoms: fever, oral enanthem, and lesions on the hands and feet, ranging from macular to vesicular eruptions (3). Typically affecting children under five years of age, HFMD has also been documented in older children, adolescents, and adults (4). The disease spreads through respiratory droplets, direct contact, and contaminated objects, maintaining its contagiousness even after symptom resolution. The incubation period varies between 3 to 10 days, with diagnosis primarily based on clinical symptoms such as a distinctive rash and painful oral ulcers, appearing after initial fever and respiratory symptoms (5). Atypical presentations, like isolated lesions, pose challenges in diagnosis, potentially leading to underdiagnosis in healthcare settings. Advanced diagnostic methods, including serology and PCR for enterovirus detection, are employed when the clinical diagnosis is uncertain (1). While HFMD is generally self-limiting, requiring symptomatic treatment, severe complications such as encephalitis, viral meningitis, and myocarditis can occur. Identified risk factors for adverse outcomes include young age, high fever, and signs of systemic involvement (5).
First identified in Toronto in 1957, HFMD has since emerged as a significant global health concern, leading to numerous outbreaks across diverse geographic regions (1). The disease’s virology has been extensively studied, revealing a variety of enterovirus subtypes responsible for its spread. Notably, EV-A71 and CV-A16 have been identified as primary agents in severe outbreaks, with CV-A6 and several echoviruses also playing significant roles in its epidemiology. These subtypes vary not only in their geographic distribution but also in the severity of the disease they cause, with EV-A71, for instance, being linked to more serious complications such as neurological disorders.
Recent advances in our understanding of HFMD have underscored the impact of external factors on its transmission dynamics. Climate change, for instance, has been shown to affect the seasonality and geographic spread of HFMD, with warmer temperatures and increased rainfall promoting virus survival and spread. Urbanization has been associated with larger and more frequent outbreaks, likely due to higher population densities and increased human-to-human contact. Furthermore, socioeconomic status has emerged as a key determinant of outbreak susceptibility, with lower socioeconomic groups facing higher risks due to factors such as crowded living conditions and limited access to healthcare services (6–8). In terms of management, prevention strategies have evolved significantly. The development and deployment of inactivated EV71 vaccines have marked a significant milestone, demonstrating high efficacy in phase 3 trials and offering a promising tool for controlling outbreaks (7). Moreover, public health measures such as hand hygiene and environmental disinfection remain foundational in preventing the spread of HFMD. These strategies underscore the importance of both individual and collective efforts in controlling the disease.
Despite HFMD’s global impact, there is a notable gap in specific literature concerning the disease in Saudi Arabia, especially regarding the knowledge and attitudes of healthcare workers towards HFMD as well as the epidemiology of the disease. This gap is particularly concerning given the recent surge in HFMD cases within the country. The absence of dedicated studies on this front highlights a critical need for research focused on understanding the awareness levels and perspectives of medical professionals in Saudi Arabia. Such research is essential for enhancing disease management and prevention efforts, tailoring strategies to the unique epidemiological and social context of the region. Given the evolving nature of HFMD outbreaks, influenced by factors such as climate change and urbanization, there is an urgent need to assess the current level of awareness and preparedness within the healthcare community in regions experiencing a surge in cases. The recent surge in HFMD cases in Saudi Arabia highlights the need for focused research in this area. Therefore, our study seeks to fill this gap by evaluating the awareness and perspectives of medical professionals in Saudi Arabia regarding HFMD, aiming to improve disease management and prevention efforts.
2 Method
2.1 Study design and settings
This research was structured as an analytical cross-sectional study carried out among medical students and physicians within the Kingdom of Saudi Arabia from November 1, 2023, to January 1, 2024. The population of interest included medical students and practicing physicians affiliated with the University of Jeddah. The study meticulously excluded non-Saudi medical students, those not enrolled at the University of Jeddah, physicians not practicing in Saudi Arabia, and any individuals who refrained from providing informed consent. To ascertain an adequate sample size, we employed the Raosoft sample size calculator, utilizing data pertaining to the total enrollment of medical students across all academic levels at the University of Jeddah, which was estimated to be 770. Given the absence of prior research on the knowledge of HFMD among medical students in Saudi Arabia, we adopted a conservative response distribution of 50% for our calculations. This approach ensured that our study was sufficiently powered to detect differences or patterns within the data. To achieve a 95% confidence level and a margin of error of 5%, we determined that the minimum required sample size was 385 participants. This calculation was pivotal in guiding our recruitment efforts, ensuring the study’s findings would be representative and reliable within the specified confidence and precision parameters. For the physicians, we randomly reach out to them to fill out the survey via WhatsApp due to their busy schedules.
2.2 Data collection process
The recruitment of participants for this study was facilitated using a convenience sampling method, ensuring swift and efficient participant engagement without offering any monetary incentives. To extend our invitation for participation, we employed a Google Forms questionnaire, leveraging the widespread accessibility and ease of use of this platform. Our primary method of reaching potential respondents was through a targeted approach on a widely used social media platform, WhatsApp, allowing us to connect with our target demographic effectively. The link to the survey was randomly sent via WhatsApp to the class page for the medical students by the class representative. Similarly, physicians were also randomly reached out to fill the questionnaire.
Prior to their participation, each potential respondent was required to provide informed consent. This process was seamlessly integrated into the beginning of the online questionnaire, where participants were presented with a consent statement. This statement clearly outlined the study’s purpose and its objectives, ensuring that participants were well-informed about the nature of the research they were contributing to. Acknowledging this consent was mandatory, obtained through a click that signified their agreement to proceed. The survey was designed to be comprehensive yet user-friendly, prompting participants to answer all questions to ensure the validity and completeness of the data collected. Upon completion, respondents were instructed to submit their responses by clicking the “submit” button, which directly transmitted their data to our collection platform. This method not only streamlined the data collection process but also emphasized the importance of complete participation, as only fully answered questionnaires were accepted for submission, thereby enhancing the quality and reliability of the data gathered. We have only one incomplete response which was deleted before we commenced our final analysis.
2.3 Data collection tools
The data was gathered using a self-administered questionnaire, which was carefully crafted by adapting current guidelines from the Centers for Disease Control and Prevention (CDC) along with insights gleaned from previously published studies (1, 8). Detailed in the Supplementary Materials, the questionnaire is structured into four key sections. The first part introduces the study and includes the consent form, ensuring that participants are well-informed about the research objectives and agree to participate voluntarily. The second section collects comprehensive sociodemographic data, such as age, gender, marital status, education level, academic performance [Less than 3.75, 3.75 – 4.49 and 4.5 and above; 5-point scale] (Grade point Average [GPA]), family income, residence details, parents’ education levels, professional standing, place of employment and years of medical experience. This allows for a detailed demographic analysis of the respondents.
The third section assesses the participants’ knowledge of hand-foot-mouth disease through 23 multiple-choice questions, with correct answers scored as one point and incorrect answers as zero, leading to a possible score range of 0 to 23. Higher scores indicate greater knowledge of the disease. The questionnaire concludes with the fourth section, which measures attitudes towards HFMD via eight statements on a 5-point Likert scale, ranging from strongly agree to strongly disagree. These statements explore perceptions of global and Saudi Ministry of Health efforts to control the HFMD epidemic, the adequacy of preventive measures, and interest in further information about HFMD.
2.4 Knowledge and attitude scoring index
For the knowledge component, the assessment includes 23 questions, each with a binary scoring system: a correct answer earns 1 point, while an incorrect answer yields 0 points, making the highest possible score 23. The scoring criteria are differentiated between medical students and physicians to reflect their varying levels of expected knowledge. Medical students are considered to have adequate knowledge if they score 10 or above, recognizing the learning stage they are in. In contrast, for physicians, who are expected to have a more comprehensive understanding due to their advanced training and experience, the threshold for adequate knowledge is set higher. A score of 15 or above is required for physicians to be classified as having adequate knowledge and acknowledging their professional development and expertise in the field.
The attitude-scoring segment of the index is more nuanced, catering to both negatively and positively framed questions to capture a holistic view of the participants’ attitudes. This part consists of 8 questions, split between 3 negatively framed and 5 positively framed items. The scoring is inversely proportional for these sets: for negatively framed questions, the scale is 4 points for ‘strongly disagree’ to 0 points for ‘strongly agree’, while for positively framed questions, it is reversed, with 0 points for ‘strongly disagree’ and 4 points for ‘strongly agree’. This approach ensures that both types of questions are weighted equally, leading to a maximum attainable score of 32. A positive attitude is indicated by a score of 24 or above, aligning with responses that fall within the ‘agree’ to ‘strongly agree’ range for positively framed questions and ‘disagree’ to ‘strongly disagree’ for negatively framed questions. The same cut-off for a positive attitude is applied to both medical students and physicians, maintaining a consistent standard for evaluating the mindset and professional disposition in the medical community.
2.5 Statistical analysis
Descriptive statistics, such as percentages, were used to summarize categorical variables (e.g., demographic characteristics), while continuous variables (such as Age and Knowledge/Attitude Score) were summarized using mean, median, interquartile range, and standard deviations. The Chi-square test for independence was utilized to investigate the bivariate association between knowledge categories (adequate and inadequate knowledge) or attitude categories (positive and negative attitude) and demographic characteristics for both medical students and physicians. If the sample size in each cell is less than 5, Fisher’s Exact Test was used instead of Chi-square. However, the t-test was employed for analyzing the bivariate association between age and knowledge/attitude categories for medical students and physicians. If the bivariate association was statistically significant, multivariate logistic regression was used to further investigate the predictors of knowledge categories (adequate and inadequate knowledge) or attitude categories (positive and negative attitude). Bar charts were used to compare the mean scores for knowledge and attitude for medical students and physicians. To further ascertain the validity of the results, linear regression was conducted as a sensitivity analysis, where knowledge and attitude scores were treated as continuous outcomes, and the results were not different from those of the logistic regression. The p-value was set at 0.05 for statistical significance. All analyses were performed using STATA 18.
3 Results
In our study, we received a total of 317 valid responses, comprising 260 students and 57 physicians. Table 1 illustrates the demographic profiles of student respondents based on their HFMD knowledge levels, highlighting key differences. Among the participants, 31.9% (n=83) demonstrated adequate knowledge, while 68.1% (n=177) showed inadequate knowledge. Age differences were notable, with the adequately informed students being older on average (mean age of 22.1 years, SD = 1.6) compared to their less informed counterparts (mean age of 21.4 years, SD = 1.8) (P = 0.001). Gender disparities also emerged, with females constituting 72.3% of the adequately knowledgeable group versus 54.2% in the less knowledgeable group (P = 0.006). No significant variance was seen in marital status (P = 0.194). Educational progression revealed that fifth-year students were predominant in the adequately knowledgeable group (34.9%), against second-year students leading the inadequate knowledge group (23.2%) (P = 0.022). GPA also significantly influenced knowledge levels (P = 0.044), where students with GPAs between 3.75 and 4.49 were more likely to have adequate knowledge (65.1%) compared to those with inadequate knowledge (53.1%). Furthermore, exposure to HFMD education markedly differed, with 68.7% of adequately informed students having received HFMD education, versus only 29.4% in the less informed group (P < 0.001).
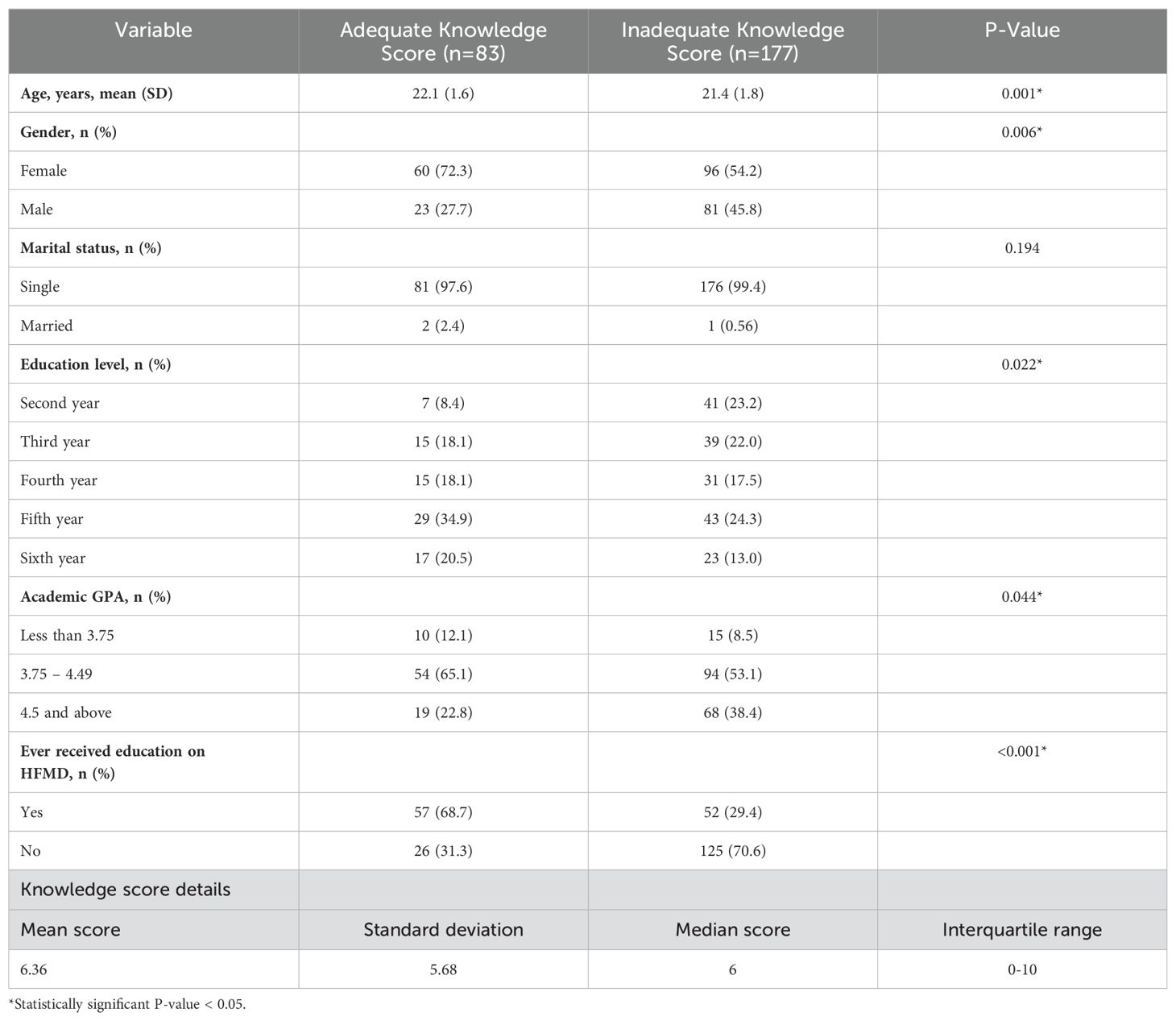
Table 1. Demographic characteristics of student respondents by their knowledge status.
Table 2 presents a multivariate logistic regression analysis assessing the impact of various demographic factors on students’ HFMD knowledge levels. Age was not a significant predictor of adequate HFMD knowledge (AOR = 1.05, 95% CI: 0.81-1.36, P=0.698). Gender differences suggested males were slightly less likely than females to have adequate knowledge, though the result was not statistically significant (AOR = 0.56, 95% CI: 0.30-1.04, P=0.066). Education level did not significantly alter the likelihood of possessing adequate knowledge across different academic years, with adjusted odds ratios ranging from 1.24 for the third year to 2.42 for the sixth year, all showing no statistical significance. Similarly, GPA levels—both 3.75-4.49 (AOR = 0.82, 95% CI: 0.31-2.16, P=0.686) and above 4.5 (AOR = 0.67, 95% CI: 0.21-2.13, P=0.501)—did not significantly influence knowledge adequacy compared to those with a GPA below 3.75. However, prior education on HFMD showed a significant positive impact, with students who had received HFMD education being significantly more likely to have adequate knowledge (AOR = 4.40, 95% CI: 2.41-8.01, P<0.001).
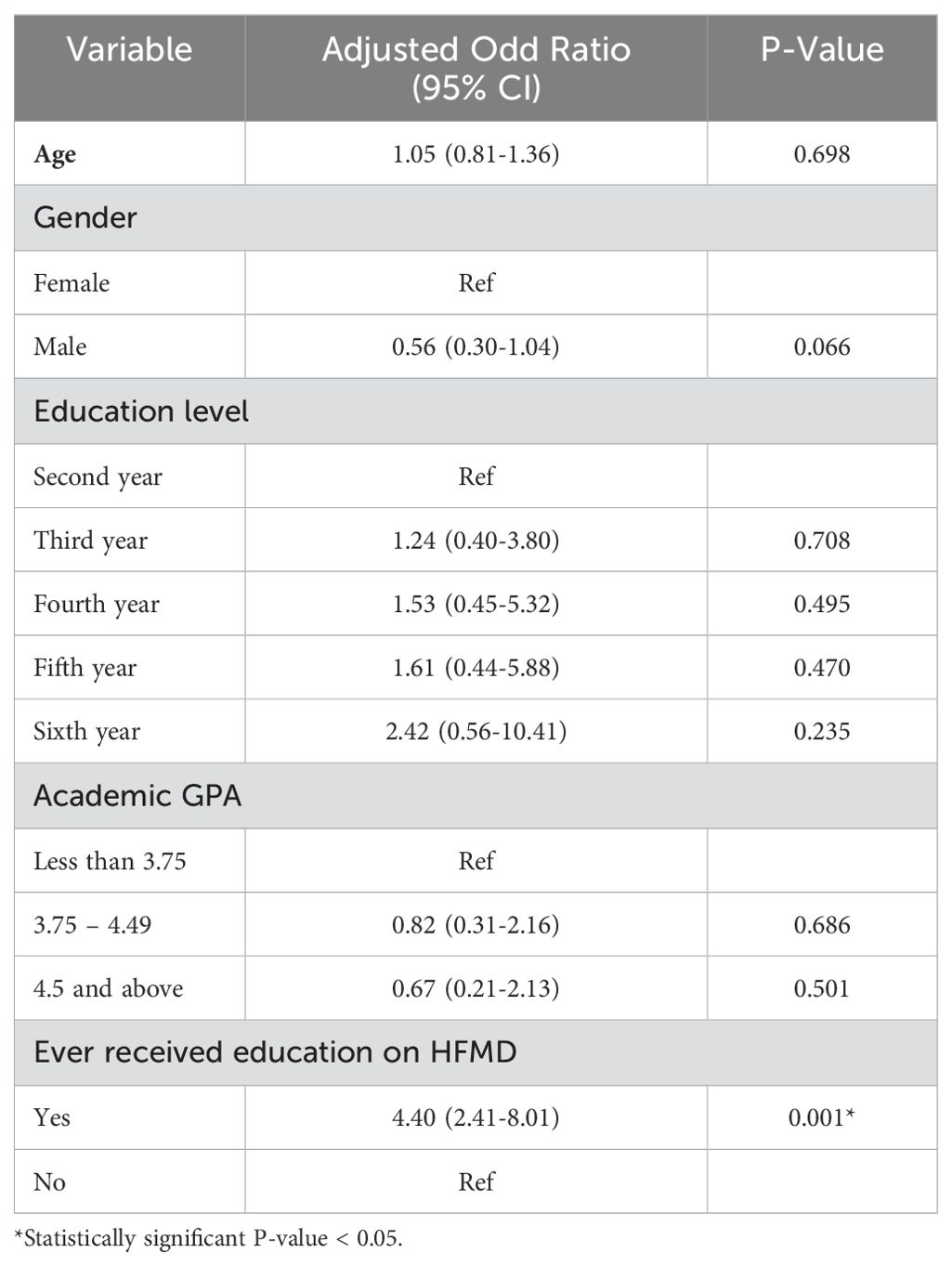
Table 2. Multivariate logistic regression of the association between knowledge status and students’ sociodemographic factors.
Table 3 outlines the demographic characteristics of students based on their attitudes towards HFMD, dividing them into positive (23.5%, n=61) and negative (76.5%, n=199) attitude groups. The average age was nearly identical for both groups, at 21.7 years (SD = 1.8) for the positive attitude group and 21.6 years (SD = 1.8) for the negative attitude group, with no significant age difference (P=0.701). The gender composition slightly favored females in the negative attitude group (62.8%) over the positive attitude group (50.8%), though the difference was not statistically meaningful (P=0.094). Marital status was overwhelmingly single across both groups, showing no significant impact on attitude (P=0.335). Educational levels and academic year representation did not show significant differences between groups (P=0.160), with the fifth year slightly more prevalent in both. GPA levels were also similar across groups, predominantly ranging from 3.75 to 4.49, without a significant difference (P=0.977). The rate of prior education on HFMD was slightly higher in the positive attitude group (45.9%) compared to the negative attitude group (40.7%), yet this difference did not reach statistical significance (P=0.472).
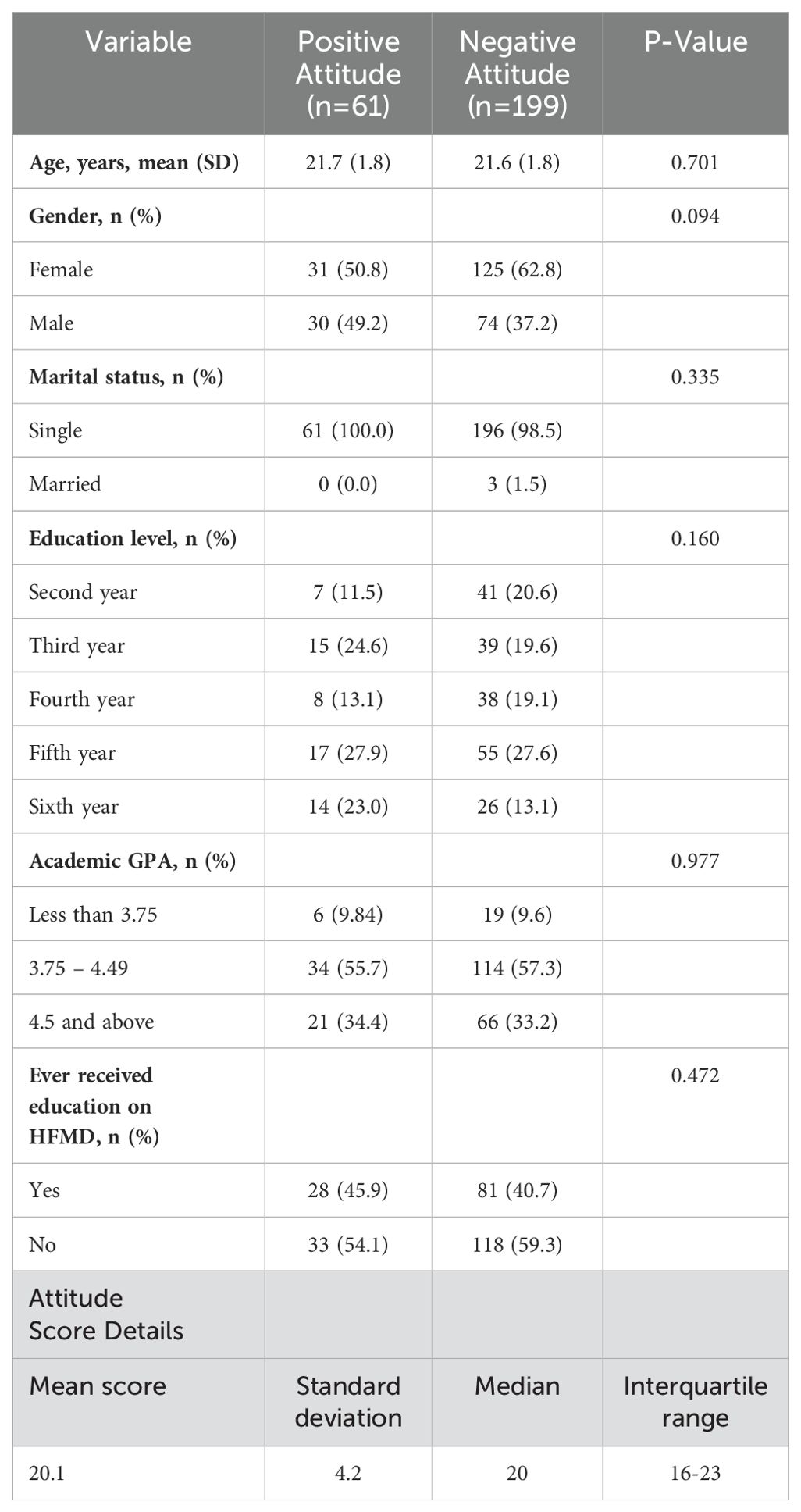
Table 3. Demographic characteristics of student respondents by attitude status.
Table 4 delineates the demographic attributes of physician respondents based on their HFMD knowledge levels, contrasting those with adequate knowledge (54.4%, n=31) against those with inadequate knowledge (45.6%, n=26). The analysis found no significant age difference between the groups, with the adequate knowledge group averaging 29.5 years (SD = 4.8) and the inadequate knowledge group at 27.6 years (SD = 6.1) (P=0.184). Gender distribution was almost even, with 74.2% females in the adequate knowledge group and 73.1% in the inadequate knowledge group, leading to a non-significant difference (P=0.924). However, marital status differed significantly, with 51.6% single in the adequate knowledge group versus 80.8% single in the inadequate knowledge group (P=0.028). Work categories and institution types showed no significant variance between residents and others (P=0.652) or governmental versus private institutions (P=0.651). Experience levels were comparable across both groups, predominantly featuring physicians with up to 5 years of experience, without significant influence on knowledge levels (P=0.160). Interestingly, prior education on HFMD was similarly high in both groups, with 77.4% in the adequate knowledge group and 80.8% in the inadequate group, showing no significant difference (P=1.000).
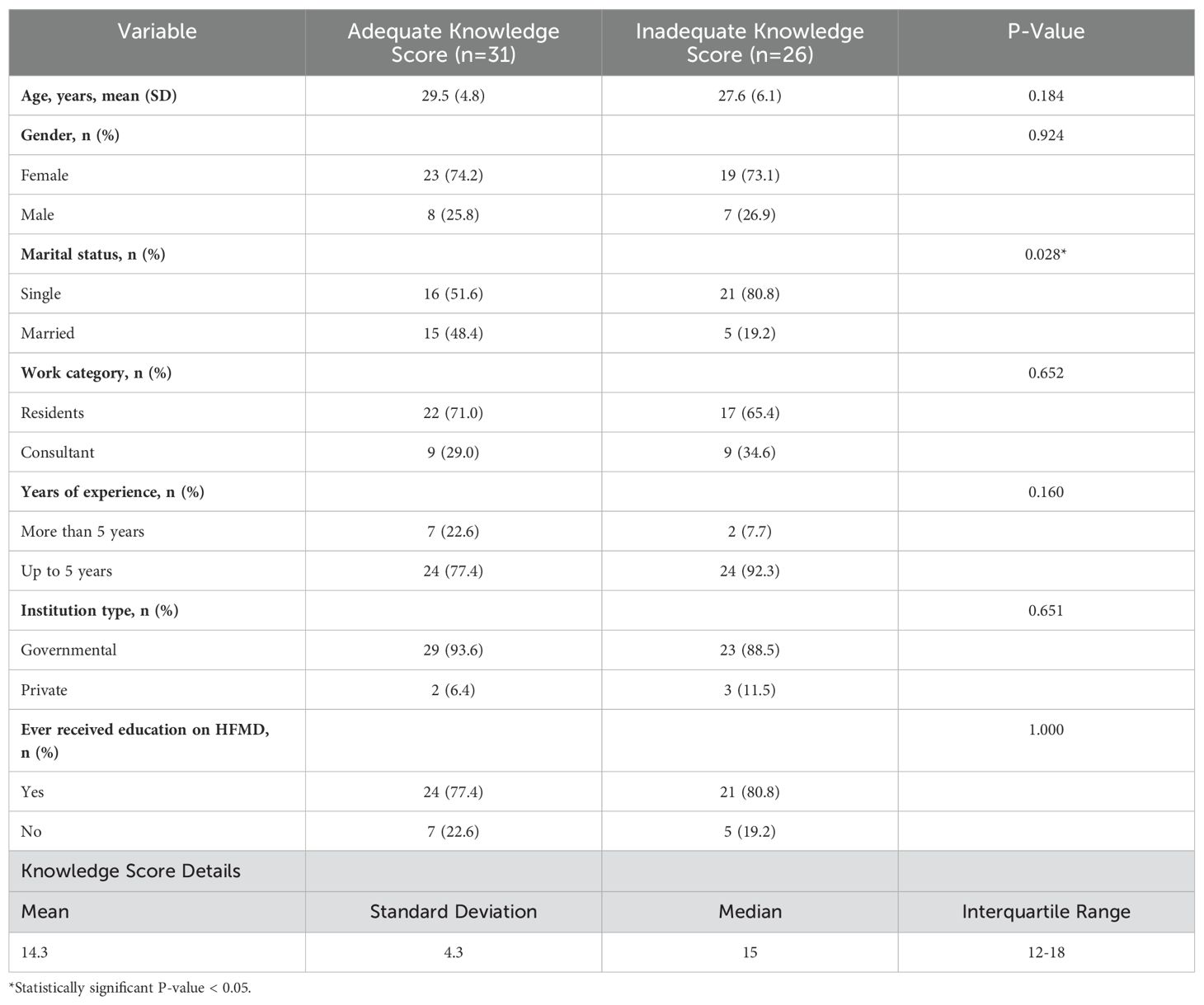
Table 4. Demographic characteristics of physician respondents by knowledge status.
Table 5 shows a breakdown of the demographic characteristics of physician respondents, categorized by their attitude status toward HFMD. The table compares physicians with a positive attitude (n=17; 29.8%) to those with a negative attitude (n=40; 70.2%). Age differences between the two groups were not statistically significant, with the positive attitude group having a mean age of 29.8 years (SD = 7.2) and the negative attitude group 28.1 years (SD = 4.5) (P=0.287). In terms of gender, 70.6% of the positive attitude group were female, compared to 75.0% in the negative attitude group. This difference was not significant (P=0.751). Marital status showed no significant difference between single and married physicians in relation to attitude status (P=0.217), with 52.9% single in the positive attitude group and 70.0% in the negative attitude group. The work category, divided between residents and consultants, showed no significant difference in attitude status (P=1.000). The same was true for the type of institution they worked for, whether governmental or private (P=0.308). Years of experience approached significance (P=0.109), with a higher percentage of those with more than 5 years of experience in the positive attitude group (29.4%) compared to the negative attitude group (10.0%). Education on HFMD showed no significant difference in terms of shaping attitude status (P=0.478), with 70.6% of the positive attitude group and 82.5% of the negative attitude group having received education on HFMD.
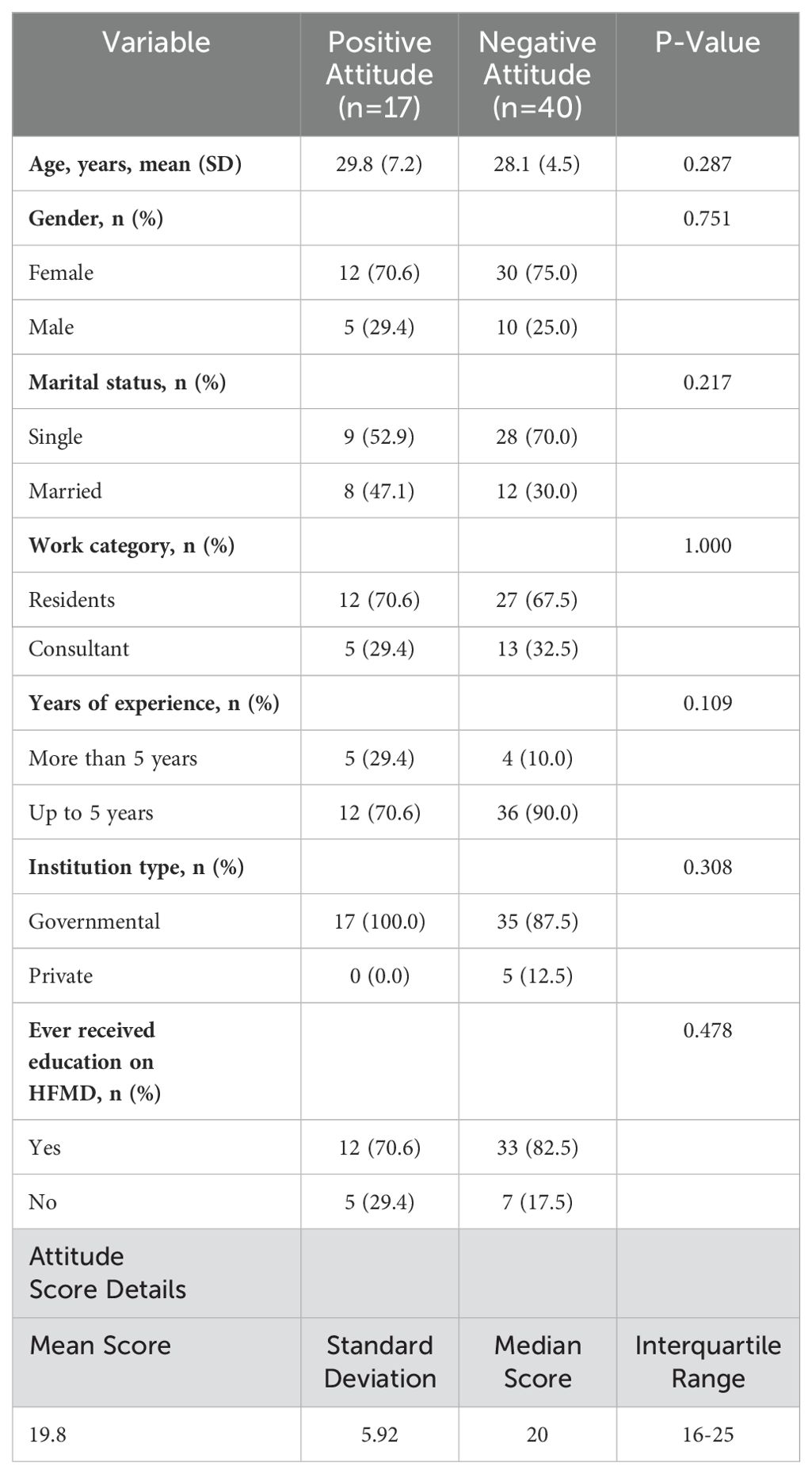
Table 5. Demographic characteristics of physician respondents by attitude status.
Figure 1 illustrates a comparative analysis of mean knowledge and attitude scores between medical students and physicians. The left side of the figure shows the mean knowledge scores on a scale up to 23, where physicians demonstrate a higher mean score, indicating more substantial knowledge of Hand, Foot, and Mouth Disease (HFMD). On the right side, the mean attitude scores, on a scale up to 32, reveal that medical students have a marginally higher score than physicians, suggesting a slightly more positive attitude towards HFMD. The scores for attitude between the two groups are closely aligned, indicating that both medical students and physicians possess comparable positivity in their attitudes toward HFMD, despite differences in their levels of knowledge.
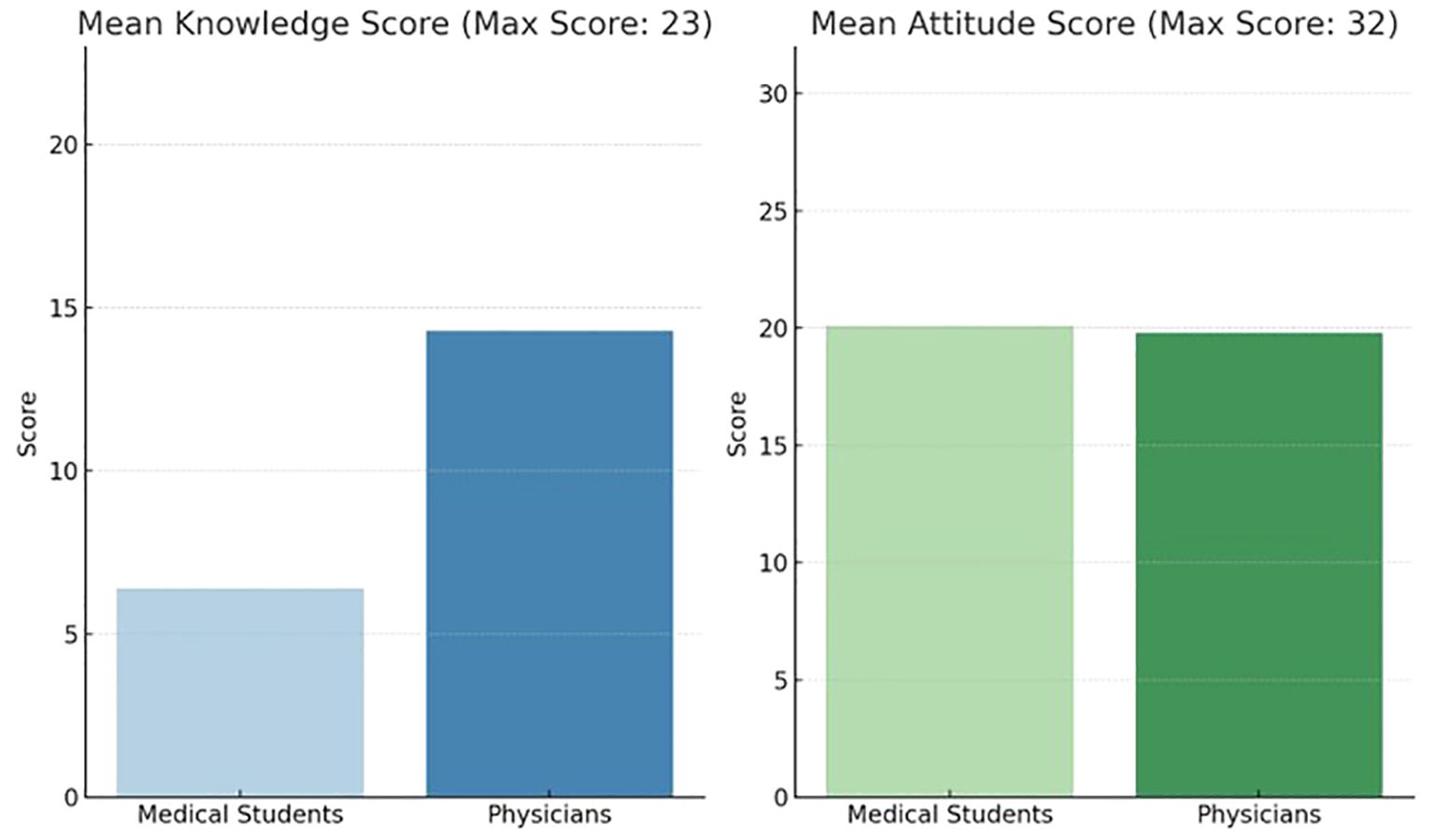
Figure 1. Comparative analysis of mean knowledge and attitude scores among medical students and physicians.
4 Discussion
The findings of this pioneering study in Saudi Arabia, focusing on the knowledge and attitudes towards HFMD among medical students and physicians, underscore a crucial gap in the healthcare education system with significant public health implications. Notably, the study revealed a general lack of adequate knowledge about HFMD among both medical students and physicians, with 67.5% of students and 45.6% of physicians demonstrating insufficient understanding of the disease. This gap in knowledge is critical, as it directly impacts the ability of future and current healthcare providers to accurately diagnose, manage, and prevent the spread of HFMD. Comparatively, literature from other regions has shown similar trends, where healthcare professionals’ knowledge gaps about specific infectious diseases correlate with less effective disease management and prevention strategies (9–11).
The negative attitudes towards HFMD identified in 76.5% of medical students and 70.2% of physicians further compound the challenge, potentially affecting patient care and engagement in preventive practices. This aligns with findings from other studies indicating that healthcare professionals’ attitudes towards diseases can significantly influence their clinical practices and patient interactions (12, 13). The detailed examination of demographic factors such as age, gender, education level, and academic performance sheds light on the complex interplay between these variables and knowledge levels among medical students. The observation that older students and those with higher academic performance tend to have better knowledge of HFMD suggests that both age-related experience and academic success are important determinants of disease-specific knowledge. This finding is consistent with literature indicating that increased exposure to medical education and clinical experiences can enhance knowledge of specific diseases (14).
The findings from this study have profound implications for healthcare policy and practice, particularly in the context of Saudi Arabia’s response to HFMD. The identified knowledge gap among both medical students and physicians necessitates immediate action to incorporate HFMD-specific education into medical curricula and continuing education programs. This education should not only cover the clinical aspects of HFMD but also emphasize the importance of positive attitudes towards patients and disease management. Policymakers and healthcare institutions should consider these findings as a call to action to develop targeted educational interventions that can effectively address these gaps. Furthermore, the association between demographic factors and knowledge levels suggests the need for tailored educational strategies that consider the diverse backgrounds of medical students and practitioners. Enhancing the knowledge and attitudes of healthcare providers towards HFMD will directly contribute to improved diagnostic, management, and prevention practices, ultimately leading to better patient outcomes and a more effective public health response to outbreaks. This study serves as a crucial baseline for future research and policy development aimed at strengthening the healthcare workforce’s preparedness and response to infectious diseases like HFMD.
This study, being the first of its kind in Saudi Arabia to assess knowledge and attitudes towards HFMD among medical students and physicians, stands out for its timely and relevant insights amidst an HFMD outbreak, marking a significant strength. It addresses a critical gap in the existing literature, providing a foundational baseline for future research and policy development to enhance healthcare professionals’ preparedness and response to infectious diseases. The targeted focus on both students and practicing physicians allows for a nuanced understanding of educational needs, highlighting the importance of integrating HFMD-specific content into medical education. However, the study is not without limitations. Its small sample size and confinement to a single educational institution may not fully capture the diversity of experiences and knowledge levels across the broader medical community in Saudi Arabia. Additionally, the reliance on self-reported data through online questionnaires introduces the potential for response bias, which could influence the accuracy of reported knowledge and attitudes. Despite these challenges, the study’s pioneering approach and its implications for healthcare policy and practice represent a vital step forward in addressing HFMD in the region.
5 Conclusion
The findings from our research highlight a noteworthy knowledge gap and prevalent negative attitudes towards HFMD among both medical students and physicians in Saudi Arabia. This underscores a critical need for comprehensive educational programs and initiatives to enhance understanding and improve perceptions of HFMD within the healthcare community. The significant proportion of participants with inadequate knowledge about HFMD, coupled with their generally negative attitudes towards the disease, indicates a potential barrier to effective disease management and prevention strategies. To address these challenges, healthcare educational curricula in Saudi Arabia must integrate targeted, disease-specific information and training on HFMD. This should not only focus on the clinical aspects of the disease but also on effective communication strategies to foster positive attitudes towards patients and disease management. Furthermore, continuing medical education programs for practicing physicians should include updates on the latest research, treatment protocols, and prevention strategies for HFMD, ensuring that healthcare providers are well-equipped to manage outbreaks and educate the public effectively.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics statement
The study protocol underwent review and approval by the Bioethics Committee of Scientific and Medical Research at the University of Jeddah, with the reference number HAP-02-J-094 and application number UJ-REC-192. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
NA: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. SB: Data curation, Methodology, Writing – original draft, Writing – review & editing. LB: Data curation, Methodology, Writing – original draft, Writing – review & editing. LA: Data curation, Methodology, Writing – original draft, Writing – review & editing. SA: Data curation, Methodology, Writing – original draft, Writing – review & editing. RG: Data curation, Methodology, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We thank all physicians and medical students for supporting and participating in this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fitd.2024.1383211/full#supplementary-material
References
1. Zhu P, Ji W, Li D, Li Z, Chen Y, Dai B, et al. Current status of hand-foot-and-mouth disease. J Biomed Sci. (2023) 30:1-23. doi: 10.1186/s12929-023-00908-4
2. Esposito S, Principi N. Hand, foot and mouth disease: Current knowledge on clinical manifestations, epidemiology, aetiology and prevention. Eur J Clin Microbiol Infect Dis. (2018) 37:391–8. doi: 10.1007/s10096-018-3206-x
3. Alshahrani NZ, Algethami MR, Alarifi AM, Alzahrani F, Alshehri EA, Alshehri AM, et al. Knowledge and attitude regarding monkeypox virus among physicians in Saudi Arabia: A cross-sectional study. Vaccines. (2022) 10:2099. doi: 10.3390/vaccines10122099
4. Liu SL, Pan H, Liu P, Amer S, Chan TC, Zhan J, et al. Comparative epidemiology and virology of fatal and nonfatal cases of hand, foot and mouth disease in mainland China from 2008 to 2014. Rev Med Virol. (2015) 25:115–28. doi: 10.1002/rmv.v25.2
5. Ventarola D, Bordone L, Silverberg N. Update on hand-foot-and-mouth disease. Clin Dermatol. (2015) 33:340–6. doi: 10.1016/j.clindermatol.2014.12.011
6. Li R, Liu L, Mo Z, Wang X, Xia J, Liang Z, et al. An inactivated enterovirus 71 vaccine in healthy children. New Engl J Med. (2014) 370:829–37. doi: 10.1056/NEJMoa1303224
7. Guo N, Ma H, Deng J, Ma Y, Huang L, Guo R, et al. Effect of hand washing and personal hygiene on hand food mouth disease: A community intervention study. Med (United States). (2018) 97:1-7. doi: 10.1097/MD.0000000000013144
8. Prevention of Hand, Foot, and Mouth Disease | CDC (2023). Available online at: https://www.cdc.gov/hand-foot-mouth/about/prevention.html.
9. Sotomayor-Castillo C, Nahidi S, Li C, Macbeth D, Russo PL, Mitchell BG, et al. Infection control professionals’ and infectious diseases physicians’ knowledge, preparedness, and experiences of managing COVID-19 in Australian healthcare settings. Infect Dis Health. (2021) 26:249–57. doi: 10.1016/j.idh.2021.05.002
10. Algunmeeyn A, El-Dahiyat F, Altakhineh MM, Azab M, Babar ZU. Understanding the factors influencing healthcare providers’ burnout during the outbreak of COVID-19 in Jordanian hospitals. J Pharm Policy Pract. (2020) 13:53. doi: 10.1186/s40545-020-00262-y
11. Zahn M, Adalja AA, Auwaerter PG, Edelson PJ, Hansen GR, Hynes NA, et al. Infectious diseases physicians: improving and protecting the public’s health: why equitable compensation is critical. Clin Infect Dis. (2019) 69:352–6. doi: 10.1093/cid/ciy888
12. Kennedy BM, Rehman M, Johnson WD, Magee MB, Leonard R, Katzmarzyk PT. Healthcare providers versus patients’ Understanding of health beliefs and values. Patient Exp J. (2017) 4:29–37. doi: 10.35680/2372-0247.1237
13. Godin G, Bélanger-Gravel A, Eccles M, Grimshaw J. Healthcare professionals’ intentions and behaviours: a systematic review of studies based on social cognitive theories. Implement Sci. (2008) 3:36. doi: 10.1186/1748-5908-3-36
Keywords: attitude, hand foot mouth disease, knowledge, medical students, physician, HFMD, infection, Saudi Arabia
Citation: Alshahrani NZ, Bukhari SM, Bukhari LM, Alghamdi LS, Aljohani SR and Ghurab RA (2024) Knowledge and attitudes of hand, foot, and mouth disease infection among medical students and physicians at the University of Jeddah. Front. Trop. Dis 5:1383211. doi: 10.3389/fitd.2024.1383211
Received: 07 February 2024; Accepted: 23 September 2024;
Published: 21 October 2024.
Edited by:
Alfonso J. Rodriguez-Morales, Fundacion Universitaria Autónoma de las Américas, ColombiaReviewed by:
Hugo Carrillo-Ng, Northwestern University, United StatesJuan Pablo Escalera-Antezana, Secretaria Municipal de Salud, Bolivia
Sultan M. Alshahrani, King Khalid University, Saudi Arabia
Copyright © 2024 Alshahrani, Bukhari, Bukhari, Alghamdi, Aljohani and Ghurab. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Najim Z. Alshahrani, bmFsc2hhaHJhbmlAdWouZWR1LnNh