 Windtaré Roland Bougma1
Windtaré Roland Bougma1 Victorino Martinho Aiogalé2Bienvenu Yao Attoumbre3
Victorino Martinho Aiogalé2Bienvenu Yao Attoumbre3 Sarah Bartlett4Kouma Brahima5
Sarah Bartlett4Kouma Brahima5 Mamadou Coulibaly6
Mamadou Coulibaly6 Yaya Ibrahim Coulibaly7
Yaya Ibrahim Coulibaly7 Boubacar Morou Dicko6
Boubacar Morou Dicko6 Susan D’Souza4Salif Seriba Doumbia7Gar Mondyu Gargannah8Balla Musa8
Susan D’Souza4Salif Seriba Doumbia7Gar Mondyu Gargannah8Balla Musa8 Babacar Ngom9Dje N’Goran Norbert5
Babacar Ngom9Dje N’Goran Norbert5 Christian Nwosu10Alberto Luis Papique11
Christian Nwosu10Alberto Luis Papique11 Emerson J. Rogers12Astou Sarr3
Emerson J. Rogers12Astou Sarr3 Philip Downs13*
Philip Downs13*- 1Neglected Tropical Diseases Department, Sightsavers, Ouagadougou, Burkina Faso
- 2Programme for the Elimination of Onchocerciasis and Lymphatic Filariasis, Ministry of Public Health, Bissau, Guinea-Bissau
- 3Neglected Tropical Diseases Department, Sightsavers, Abidjan, Côte d'Ivoire
- 4Neglected Tropical Diseases Department, Sightsavers, Haywards Heath, United Kingdom
- 5National Programme for the Control of Neglected Tropical Diseases with Preventive Chemotherapy, Ministry of Health and Public Hygiene Abidjan, Abidjan, Côte d'Ivoire
- 6Neglected Tropical Diseases Department, Sightsavers, Bamako, Mali
- 7Filariasis Unit, Ministry of Health and Social development, Bamako, Mali
- 8Neglected Tropical Diseases Department, Sightsavers, Monrovia, Liberia
- 9Neglected Tropical Diseases Department, Sightsavers, Dakar, Senegal
- 10Neglected Tropical Diseases Department, Sightsavers, Kaduna, Nigeria
- 11Neglected Tropical Disease Programme, Ministry of Public Health, Bissau, Guinea-Bissau
- 12Neglected Tropical Diseases Programme, Ministry of Public Health and Social Welfare, Monrovia, Liberia
- 13Neglected Tropical Diseases Department, Sightsavers, Durham, NC, United States
Background: A country claiming to have achieved elimination of Lymphatic filariasis (LF) as a public health problem must undergo and document a quality assessment of the World Health Organization (WHO) recommended essential package of care for patients with lymphedema and hydrocele. This must be done in at least 10% of facilities offering services. In Liberia, Côte d’Ivoire, Mali and Guinea-Bissau the LF programmes used the Hydrocele Facility Assessment Tool (HFAT) and the Lymphedema Facility Assessment Tool (LFAT) to provide an objective assessment of facilities providing LF morbidity management services. Information gathered through these tools is used to improve service delivery and document the number of implementation units with at least one facility providing the essential package of care in the WHO epidemiological reporting form (EPIRF). The development of the HFAT and LFAT digital tools were informed by WHO’s direct inspection protocol (DIP) for lymphedema, WHO’s service availability and readiness assessment (SARA), and WHO’s situational analysis to assess emergency and essential surgical care.
Methods: Between May 2022 and January 2023, 33 hydrocele facility assessments and 102 lymphedema facility assessments were implemented in these four countries. Facility and indicator score benchmarks were set at 75%.
Results: The LFAT and HFAT indicator results were variable both within and between countries. 26 (79%) facilities scored 75% or better on the assessment for hydrocele surgery and 15 (15%) facilities scored 75% or better on the assessment for lymphedema. Examples of indicators with significant need for quality improvement actions were 1) LFAT indicator ‘Trained staff - Community Health Care Providers trained in lymphoedema management’ which did not achieve the 75% benchmark in any of the countries; 2) HFAT indicator on use of surgical safety checklist which only achieved the 75% benchmark in Liberia.
Discussion: The discussion highlights the current challenges faced by endemic countries to ensure that an essential package of care (of sufficient quality) for lymphedema management and hydrocele surgery is available.
Introduction
Lymphatic filariasis (LF) is a preventable neglected tropical disease (NTD) caused by infection with the filarial parasites Wuchereria bancrofti, Brugia malayi or B. timori (1). Infection is usually acquired in childhood and causes hidden damage to the lymphatic system.
Infected persons may be clinically asymptomatic or present visible clinical manifestations such as lymphedema (tissue swelling), advanced lymphedema with dermatosclerosis (elephantiasis) and hydrocele (scrotal swelling). These chronic manifestations are often associated with debilitating acute episodes (attacks) of local inflammation and physical impairments that can lead to disability, psychological harm and social exclusion. The acute attacks are caused by secondary bacterial skin infection or the body’s immune response to the parasite.
The global baseline estimate of people affected by lymphatic filariasis was 25 million men with hydrocele and over 15 million people with lymphoedema (2)1. In 2022, 794 million people living in 44 countries were living in areas that require mass drug administration (MDA) to stop the spread of infection (3).
In 1997, the World Health Assembly adopted resolution WHA50.29 on the elimination of lymphatic filariasis as a public health problem (4). The Global Programme to Eliminate Lymphatic Filariasis (GPELF) was launched by the WHO in 2000 with aims to: 1) Stop the spread of LF infection to prevent new cases through MDA, and 2) Alleviate suffering through morbidity management and disability prevention (MMDP) (5).
An essential (also known as minimum) package of care has been defined to alleviate suffering in people with acute attacks, lymphoedema and hydrocele and to improve their quality of life (5). This package of care includes:
● Treatment of adenolymphangitis episodes: treating acute episodes of adenolymphangitis (ADL) among people with lymphedema or advanced lymphedema with dermatosclerosis (elephantiasis);
● Management of lymphedema: preventing debilitating, painful episodes of acute attack and progression of lymphedema;
● Management of hydrocele: providing access to hydrocele surgery; and
● Provision of antifilarial medicines: to destroy any remaining worms and microfilariae by mass drug administration or individual treatment for LF infection.
The GPELF target of 100% geographical coverage of this essential package of care aims to ensure that endemic countries reach all areas with known patients.
Tools have been developed to assess the quality and readiness of morbidity management services in designated health facilities. WHO developed a direct inspection protocol (DIP) tool to assess the quality of services offered for lymphedema management (5, 6) and The Liverpool School of Tropical Medicine (LSTM) developed an equivalent tool, the Hydrocele Surgery Facility Assessment Tool (HSFAT) for hydrocele services (7). These tools incorporate elements from the WHO tool for Situational Analysis to Assess Emergency and Essential Surgical Care (8), the WHO Service Availability and Readiness Assessment tool (SARA) (9), and the WHO/UNICEF guide to monitor water, sanitation and hygiene in health care facilities (10). While quality assessments can be implemented at any time, WHO guidance recommends that 10% of the health facilities that provide care be evaluated at least once, preferably within two years of the submission of the LF elimination dossier (6).
The facility assessments described in this paper are based on the WHO DIP for lymphedema and the HSFAT. The assessments took place in Côte d’Ivoire, Guinea-Bissau, Liberia and Mali between May 2022 and January 2023. This geography covers countries at various stages towards the elimination of LF as a public health problem and provision of morbidity management services. Notably, in the case of Côte d’Ivoire and Guinea-Bissau, the LFAT assessments described mark the start of support to lymphedema management in the country. By contrast, in Liberia and Mali, national level programme support for lymphedema management started in 2017 and 2012 respectively. In the case of Liberia, all the facilities implementing LFAT had prior experience in implementing lymphedema management. In the case of Mali, two of the ten districts covered by the LFAT assessments in this manuscript had prior experience.
In all four countries the assessments were carried out more than two years from the date that the countries were projected to submit elimination dossiers. However, the activity helps promote four essential elements of LF morbidity services: 1) provision of quality care to patients 2) identifying less efficient areas in order to take corrective actions before the evaluation for the elimination dossier 3) familiarising health personnel with the conduct of this protocol 4) contributing to the strengthening of the health system by strengthening the capacities of personnel and the acquisition of materials and equipment.
Additionally, results from the HFAT and LFAT assessments can be used to complete the ‘number of implementation units with at least one facility providing the essential package of care’ in the WHO epidemiological reporting form (EPIRF) (4, 11) and to inform the formulation of quality improvement recommendations by national LF programmes.
Materials and methods
Description of the tools
Structured questionnaires were developed using the Hydrocele Surgery Facility Assessment Tool (HSFAT) developed by LSTM (7) for hydrocele and a precursor to the WHO DIP for lymphedema (6).
The HFAT consists of the HSFAT facility-level questionnaire (7) and a newly developed patient level questionnaire (see Supplementary Material: Data sheet 1 for full tool). As described previously (7), the facility level questionnaire consists of questions and key (equally scored) indicators grouped across the following 10 domains: 1) background information, 2) essential amenities, 3) emergency patient transfer, 4) laboratory capacity, 5) surgical procedures and trained staff, 6) infection prevention, 7) non-disposable basic equipment, 8) disposable basic equipment, 9) essential medicines and 10) current hydrocoele practices (Table 1). The patient level questionnaire covers: knowledge to make an informed decision, changes in economic situation following surgery, changes in family life following surgery and suggestions for improvements.
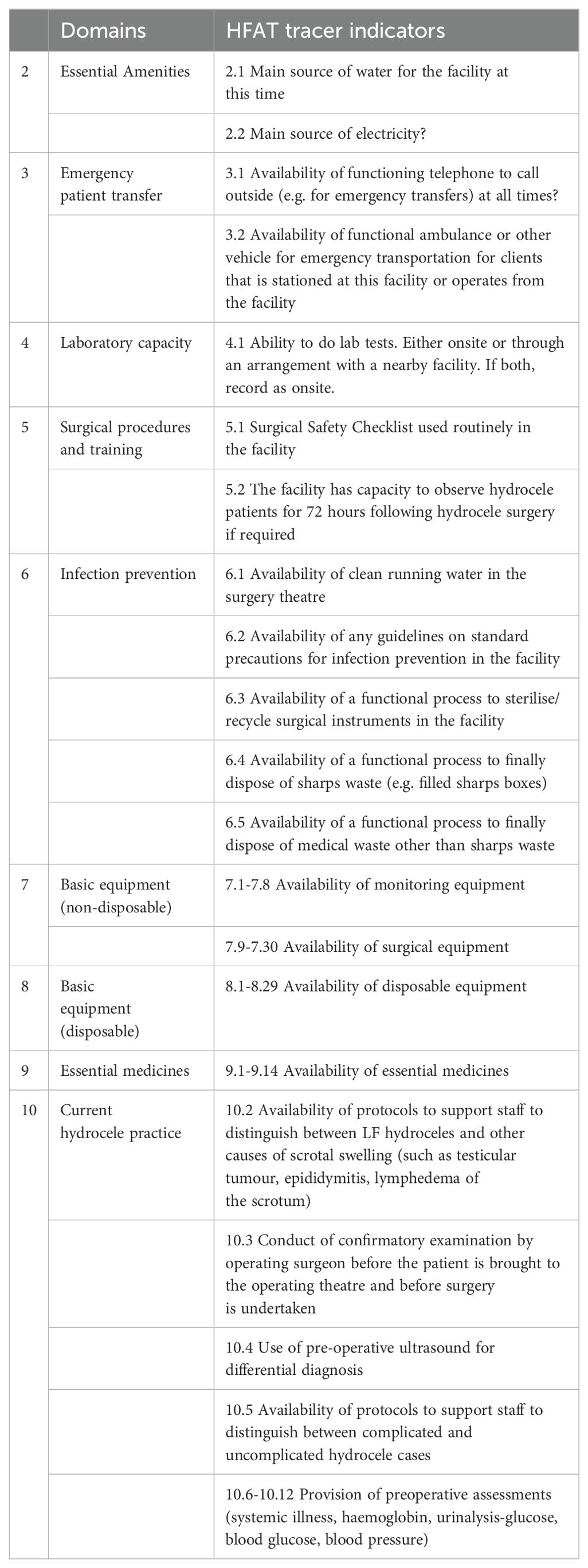
Table 1. HFAT domains and indicators.
The LFAT corresponds to the WHO DIP with questions relating to the facility level questionnaire and a patient interview (see Supplementary Material: Data sheet 2 for full tool). The facility level questionnaire consists of questions and key (scored/tracer) indicators grouped across the following domains: 1) background information (not scored), 2) trained staff, 3) case management and education materials, 4) infrastructure, 5) medications and commodities, 6) patient tracking system, 7) staff knowledge, 8) challenges and feedback (not scored), 9) staff demonstration (not scored). Table 2 highlights some minor differences between the WHO DIP and the LFAT with indicator wording and scoring of indicators under domains 5 and 7. As much as possible, the format of the results presented in this paper is aligned with the WHO protocol. The patient interview assesses knowledge of strategies for preventing acute attacks and the progression of lymphedema, and collects patient feedback and suggestions on service improvement.
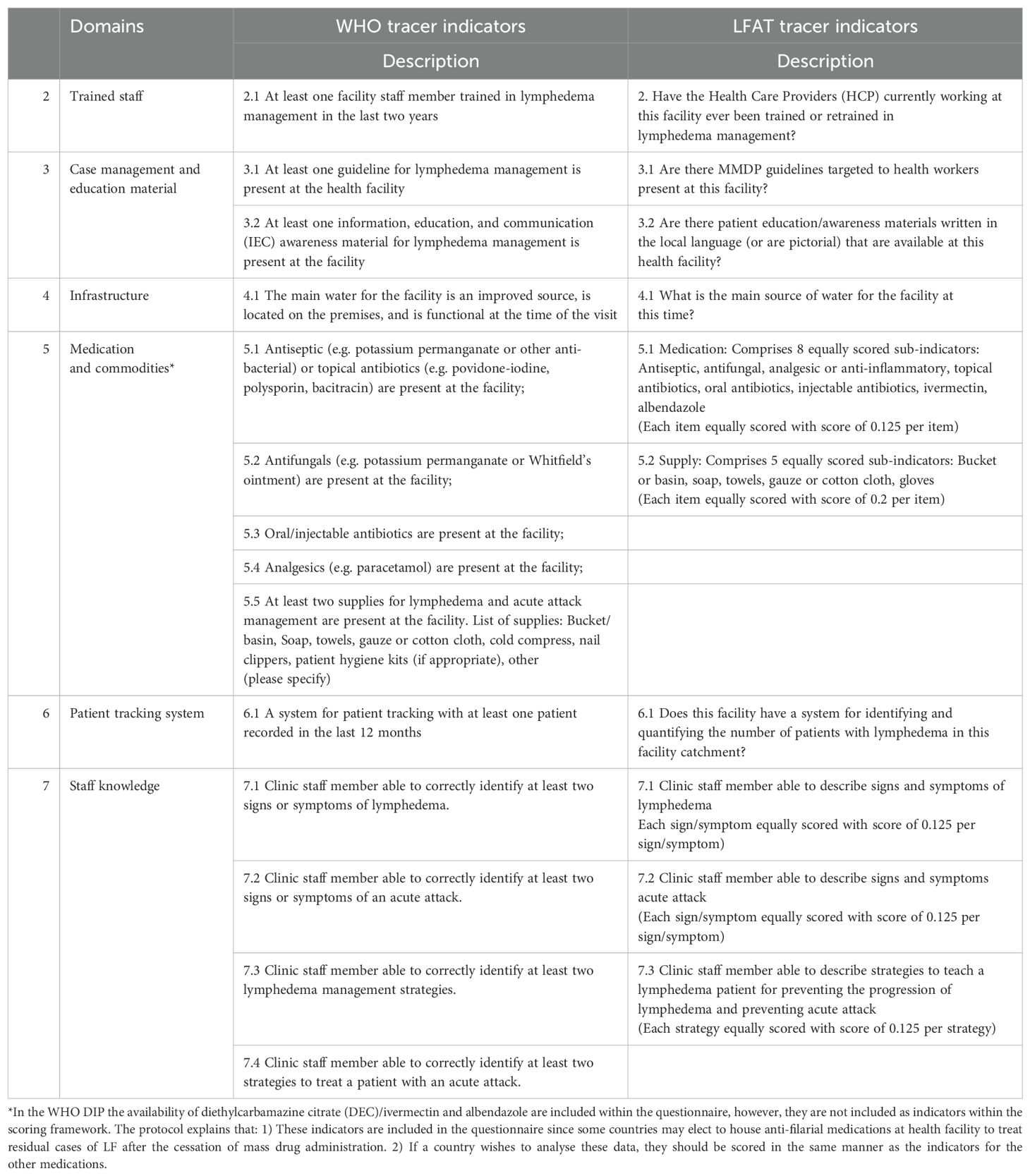
Table 2. LFAT scored domains and tracer indicators, highlighting differences in wording and scoring system between WHO 2021 DIP and LFAT.
The scoring of the indicators in the HFAT and LFAT provided national, facility and indicator level scores. A score of 75% was set as a benchmark for health facilities and indicators as a minimum standard to achieve. The analysis herein presented focuses on the indicator level scores.
Intervention area
The assessments described in this manuscript were implemented between May 2022 and January 2023 in Côte d’Ivoire, Guinea-Bissau, Liberia and Mali. All the assessments took place in intervention areas supported by Sightsavers. In the case of the LFAT, 10% of health facilities in the targeted areas (in each country) were randomly selected. In the case of the HFAT, all hospitals declared able (by health authorities) to provide hydrocele surgery were assessed.
Tables 3, 4 provide summary information on the facilities assessed in each country. For the purpose of this paper, health care facilities were categorised using standard health care facility classification in developing countries, including four distinct tiers: local health posts (tier 1), district health centres (tier 2), province- and regional-level hospitals (tier 3), and national and central hospitals (tier 4) (12).
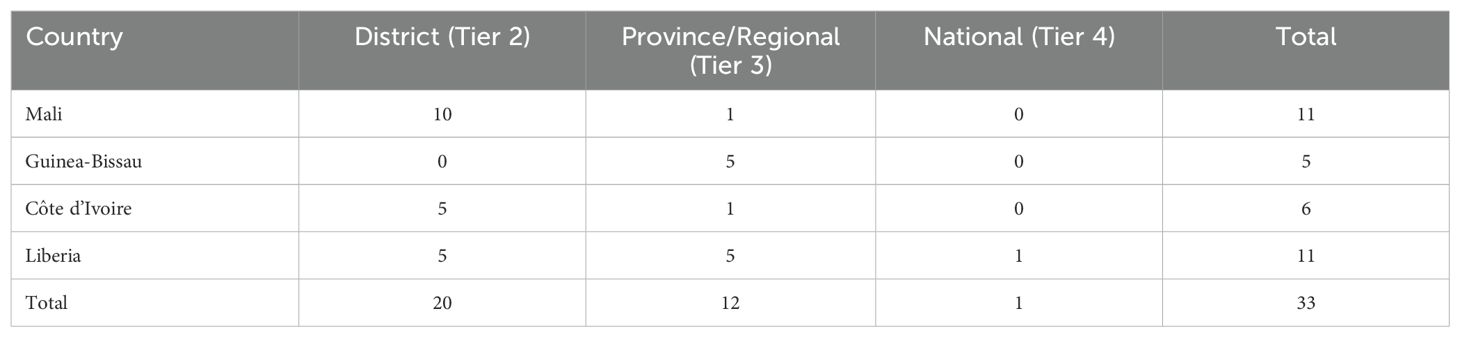
Table 3. Summary of facilities assessed by country – HFAT.
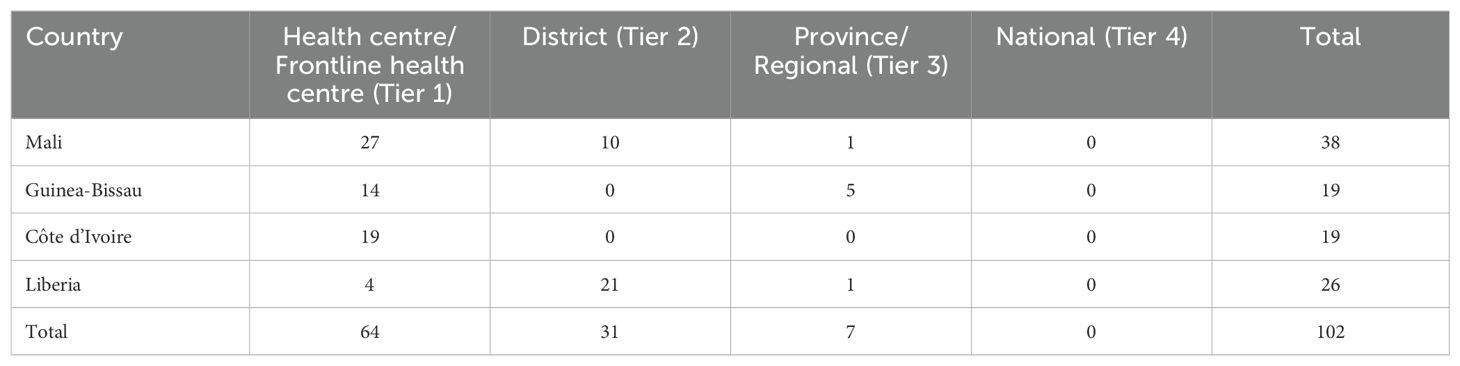
Table 4. Summary of facilities assessed by country – LFAT.
In Côte d’Ivoire, the assessment area covered six health districts (Tiassale, Tiebissou, Divo, Yakasse Attobrou, Lokota, Bongouanou) across five regions (Agneby-Tiassa, Belier, Loh Djiboua, Me, Moronou), (Figure 1). The HFAT was implemented in six hospitals (tiers 2-3) and the LFAT in 19 front line health facilities (tiers 1). Assessments were done from 18 to 23 October, 2022.
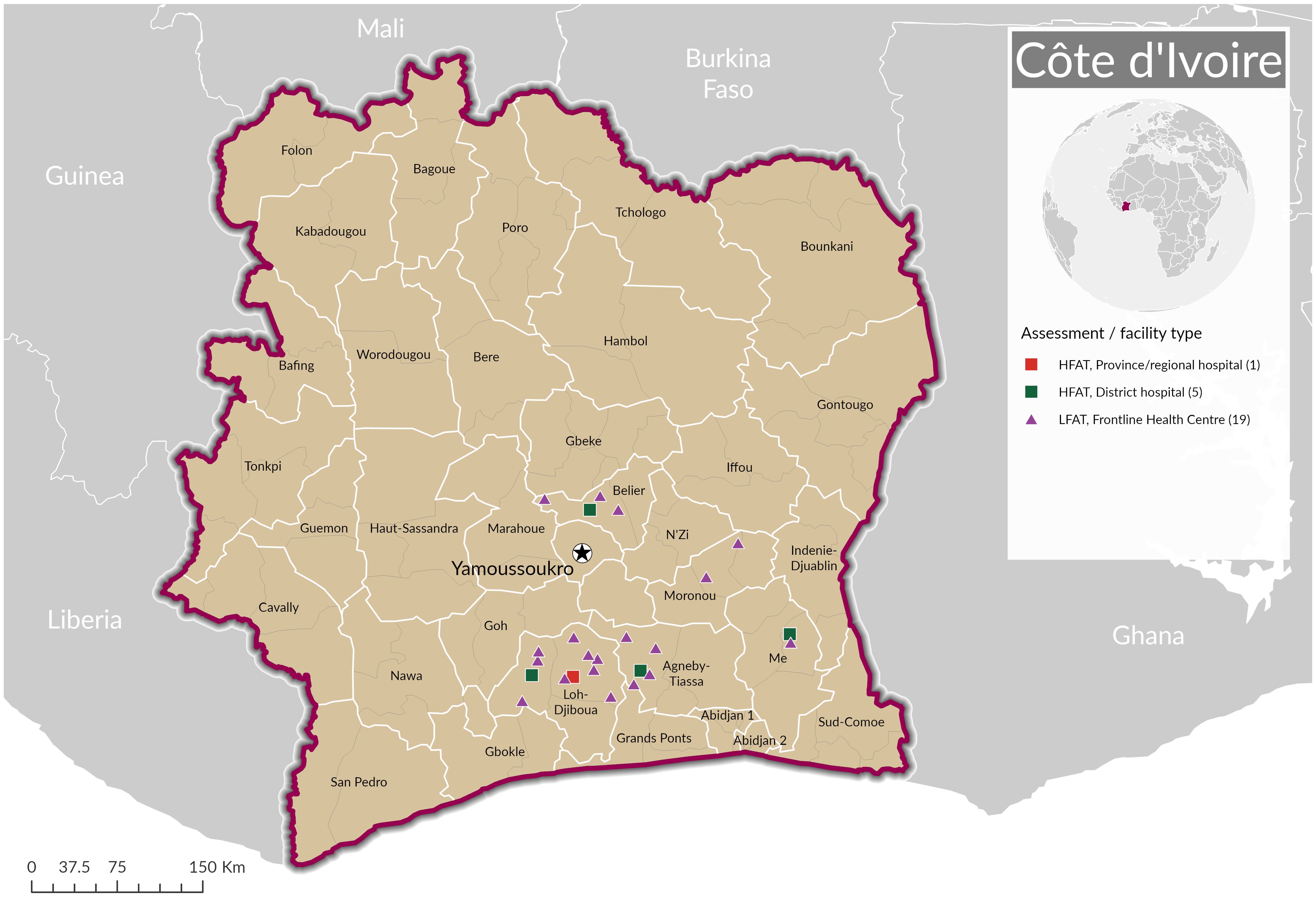
Figure 1. Location of Hydrocele Facility Assessments and Lymphedema Facility Assessments in Côte d'Ivoire.
In Guinea-Bissau, the study targeted five regions (Bafata, Bijagos, Cacheu, Gabu, Quinara), 19 health areas (Bafata, Bambadinca, Contuboel, Sare Bacar, Bubaque, Caravela, Formosa, Uno, Barro, Canchungo, Carenque, Sao Domingos, Canjadude, Gabu, Pirada, Tumana, Brandao, Buba, Empada) (Figure 2). The HFAT was implemented in five regional hospitals (tier 3) and the LFAT in 19 health facilities (tier 1 and tier 3). Assessments were done from 15 December, 2022 to 15 January, 2023.
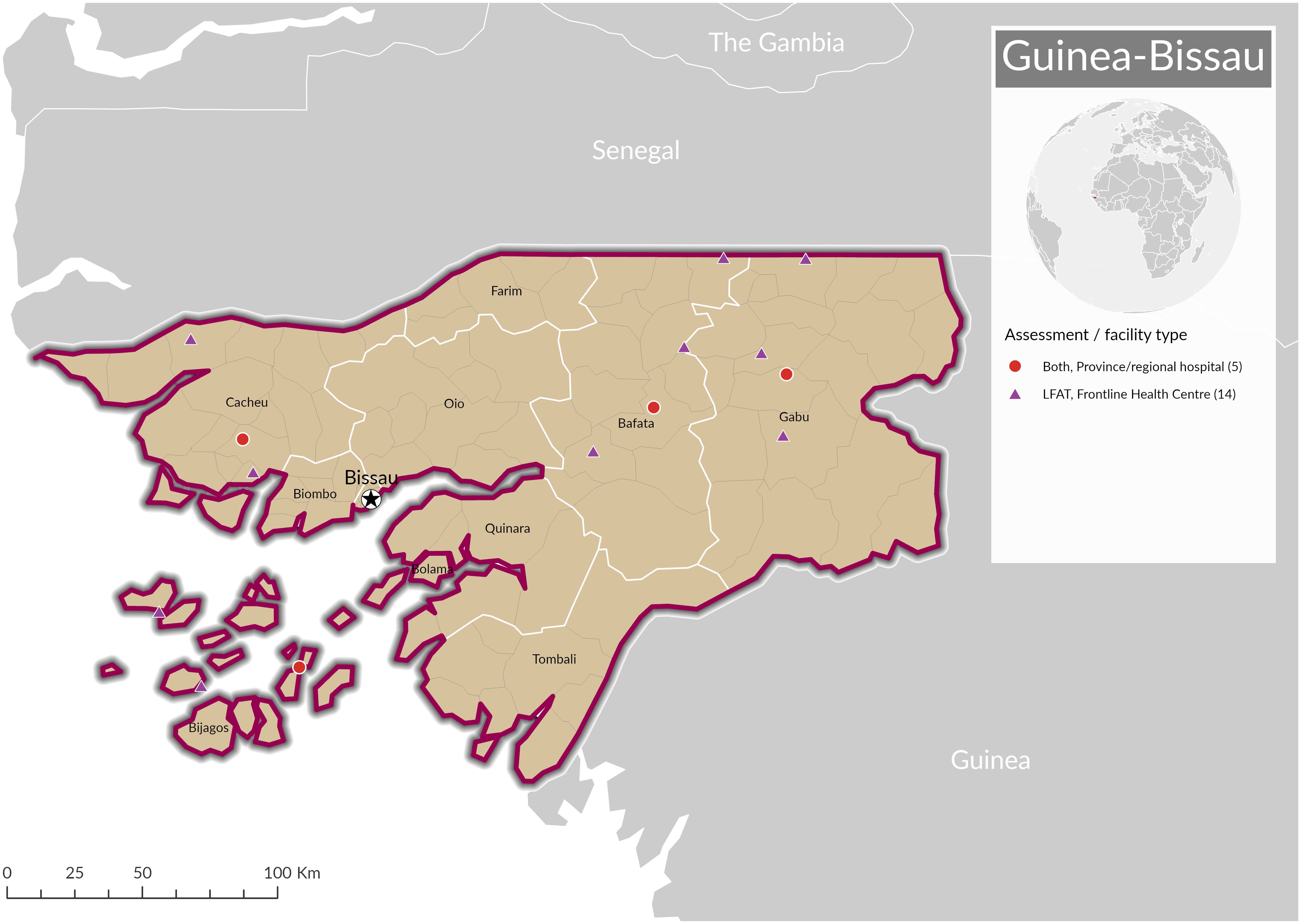
Figure 2. Location of Hydrocele Facility Assessments and Lymphedema Facility Assessments in Guinea-Bissau.
In Liberia, the assessment was conducted in five counties (Bomi, Bong, Lota, Maryland, Nimba), 14 districts (Clay, Sinji, Jorquelleh, Suakoko, Foyah, Kolahun, Salayea, Voinjama, Zorzor, Harper, Karluway 2, Plebo, Saclepea Mahn, Tapeta) (Figure 3). The HFAT was implemented in 11 hospitals (tiers 2-4). The LFAT assessed 26 health facilities (tiers 1 –3). Assessments were done from 14 to 21 July, 2022.
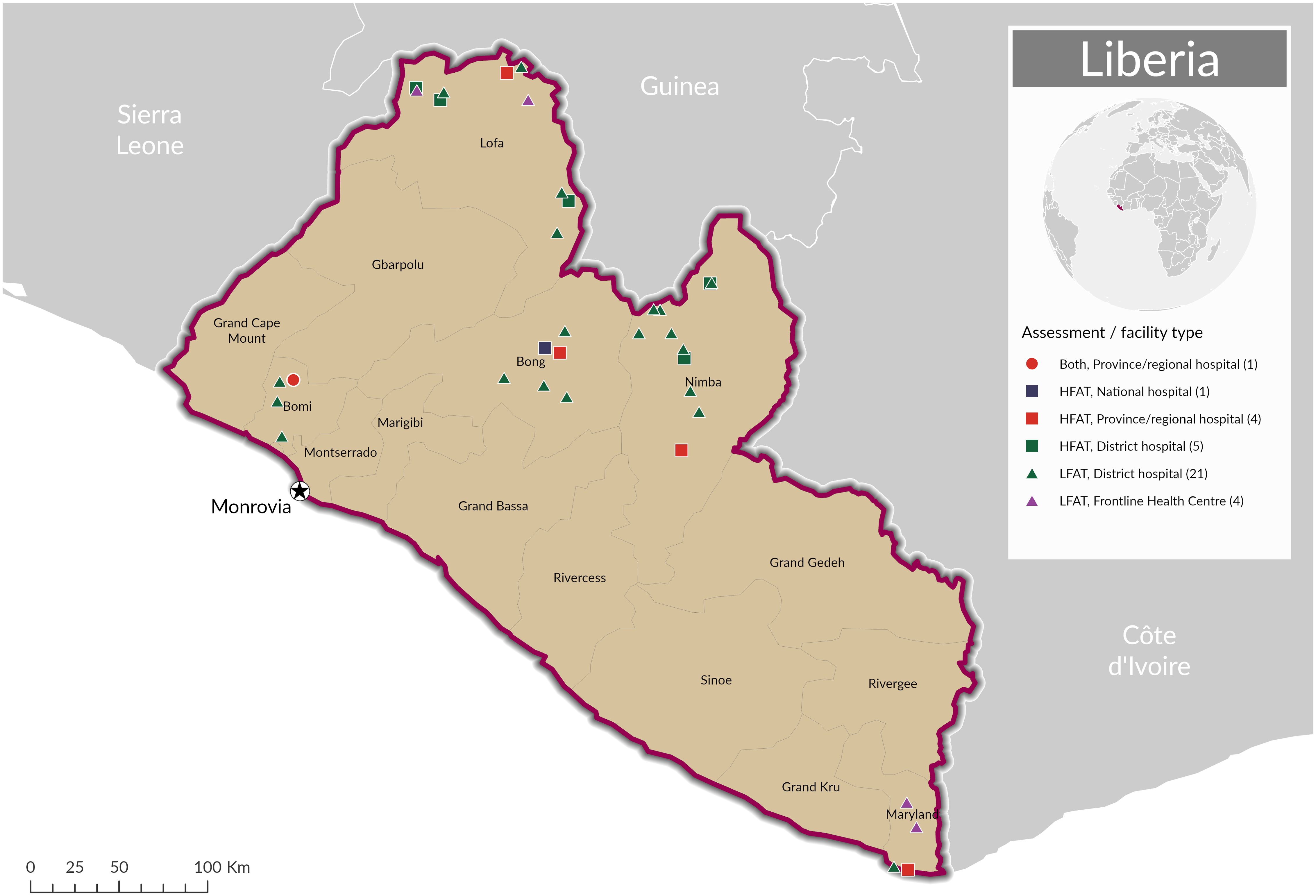
Figure 3. Location of Hydrocele Facility Assessments and Lymphedema Facility Assessments in Liberia.
In Mali, the assessment targeted one region (Sikasso), ten districts (Bougouni, Kadiolo, Kignan, Kolondieba, Koutiala, Niena, Selingue, Sikasso, Yanfolila, Yorosso) (Figure 4). The HFAT was implemented in one regional hospital (tier 3) and 10 referral health centres (tier 2). The LFAT assessed the regional hospital and 10 referral health centres (tiers 2-3) as well as 27 community health centres (tier 1). Assessments were done from 9 to 16 May, 2022.
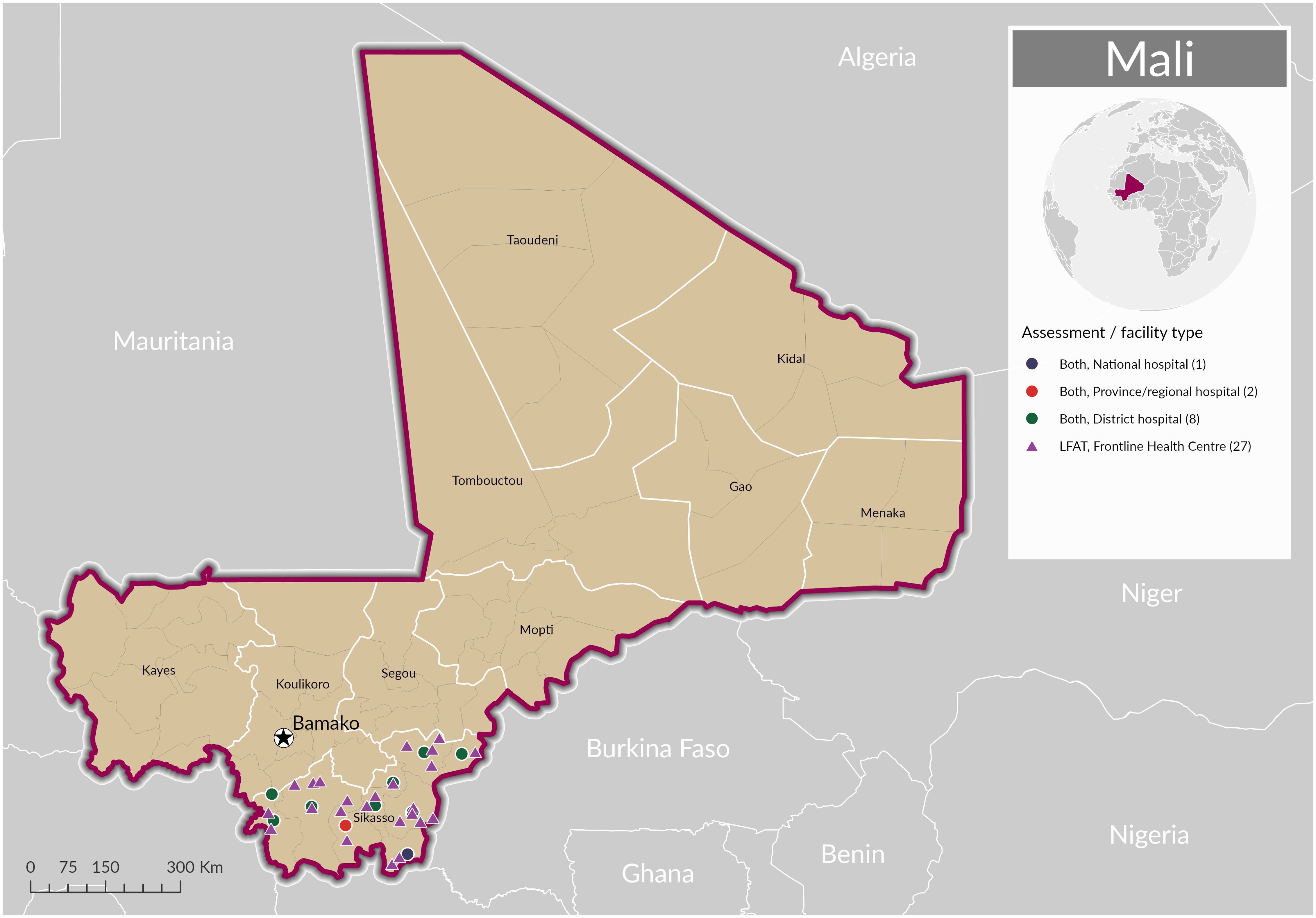
Figure 4. Location of Hydrocele Facility Assessments and Lymphedema Facility Assessments in Mali.
Digital tools and data management
The structured questionnaires were uploaded on the CommCare platform2 so that field teams could digitally collect data on structured, error-detecting forms; that data was immediately sent into protected cloud storage. A dashboard using Metabase3 and a set of automated reports, accessible to designated health staff involved in the activity, were also developed to monitor the progress of the assessment and make reporting easier. They include the final score obtained by each health facility and for each indicator. The data was cleaned during data review meetings organised in each country at the end of the assessment period. To do so, data was downloaded from CommCare in the Excel format then cleaned and updated based on feedback provided by country teams. It was then reintegrated and used for scoring.
Training and rollout of LFAT and HFAT
Training for all enumerators, LF programme supervisors, additional Ministry of Health staff, and Sightsavers country office staff was rigorously conducted to ensure all personnel had sufficient skills and experience. Training topics covered included the protocol, the CommCare application and data collection procedures, the evaluation instruments (questionnaire using CommCare), quality control methods and the online dashboard. Due to their length, the questionnaires and protocols were sent to all designated enumerators prior to the training to ensure that they were familiar with the tools.
Prior to implementing any assessments, authorisation to collect data in the area (region and/or district, depending on the country) was obtained. National LF programme coordinators then wrote letters to each health facility which would be assessed; the letters were presented to the health facility lead upon arrival. Assessments took anywhere between a half to a full day in each facility.
Process of administering questionnaires
The structured questionnaires were administered by asking questions one after the next. One enumerator asked the questions while the second recorded the answers on the smartphone or tablet. Where demonstrations of certain activities were part of the assessment, the enumerators observed and noted the performed gestures and attitudes.
In the case of the LFAT, staff of medical wards/dermatology departments and front-line health facility doctors, nurses and other health personnel provided the answers. For the HFAT, surgeons and their staff are targeted to answer questions but if the surgical team could not answer a question support also came from hospital administration, laboratory, or pharmacy staff. Information on the number of beds and the availability of fuel could also be provided by the staff of the finance department; information on personnel could be provided by human resources managers or the director of the facility. In the operating theatres, depending on the availability of the staff at the time of the interview, the surgeon answered alone or was assisted by assistant surgeons and anaesthetists.
Results
Lymphedema facility assessment tool
The facility benchmark of 75% was attained by 32% of the facilities assessed in Mali, 12% of the facilities assessed in Liberia and 0% of the facilities assessed in Cote D’Ivoire and Guinea Bissau. Across countries 15% of the facilities assessed attained the 75% benchmark.
Summary indicator results from the LFAT assessments are presented in Table 5 (‘Mean number of key indicators marked positively for each facility and overall percentage of positively scoring indicators by domain’). Figure 5 graphically represents the percentage of facilities that achieved quality indicator criteria for domains 2 to 7. A full breakdown of LFAT indicator results is provided in Supplementary Material: Table 1.
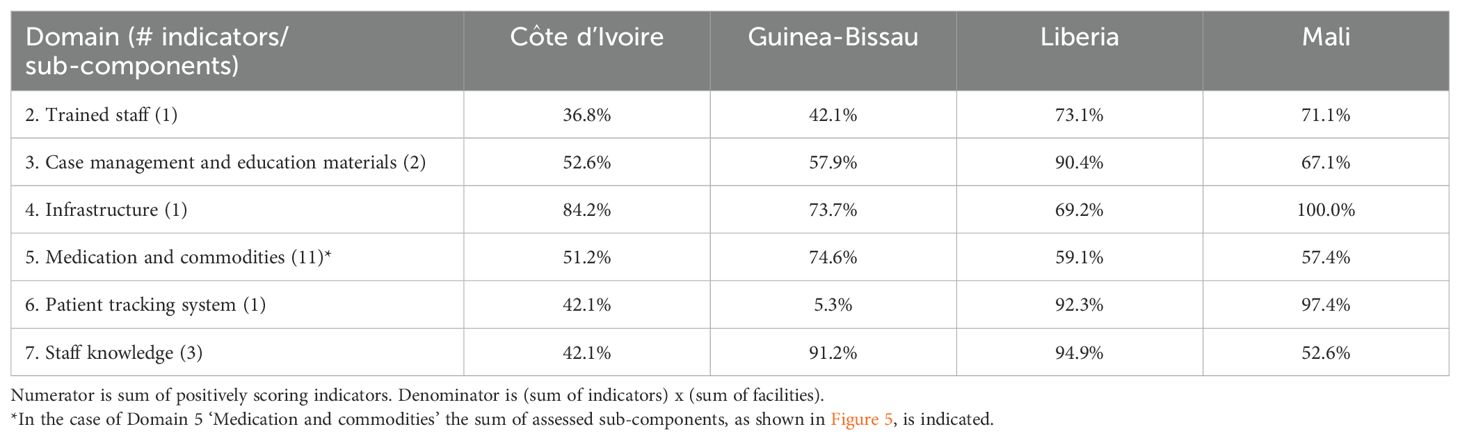
Table 5. Overall percentage of positively scoring indicators by LFAT domain.
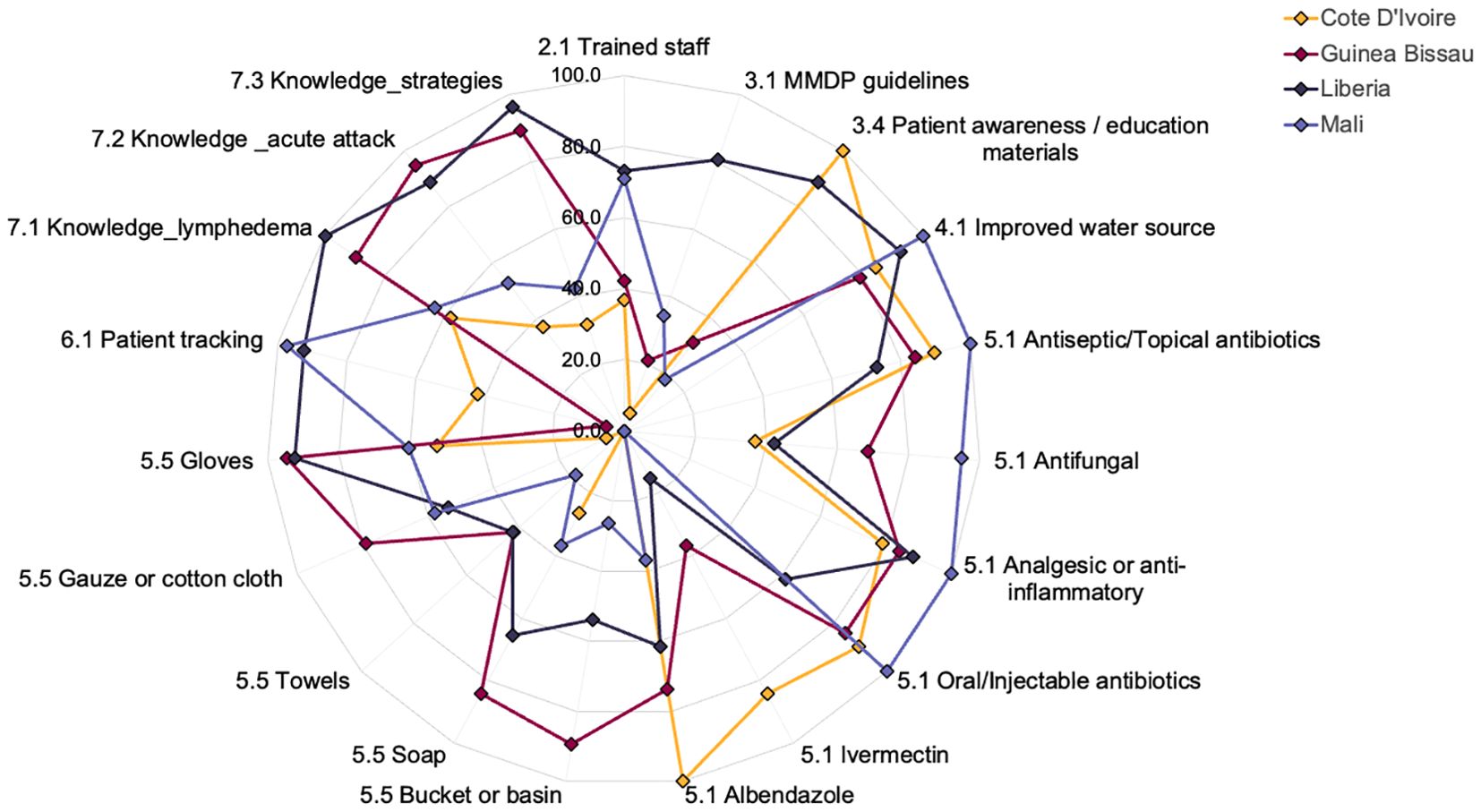
Figure 5. % Facilities achieving LFAT quality indicator criteria (domains 2-7).
Key findings by domain
Trained staff (domain 2)
The percentage of facilities reporting to have Community Health Care Providers trained in lymphoedema management was (in descending order): Liberia – 73.1%, Mali – 71.1%, Guinea-Bissau – 42.1%, Côte d’Ivoire – 36.8%.
MMDP guidelines (domain 3)
The percentage of facilities with MMDP guidelines targeted to health workers present at the facility was high in Liberia (80.8%) though low in the other countries (Mali 34.2%, Guinea-Bissau 21.1%, Côte d’Ivoire 5.3%).
Patients awareness/education materials (domain 3)
The percentage of facilities with patient education/awareness materials available in the local language (or pictorial) was in descending order Côte d’Ivoire (100%), Liberia (88.5%) Guinea-Bissau (31.6%) and Mali (18.4%).
Improved water source (domain 4)
The percentage of facilities with an improved water source was in descending order: Mali (100%), Liberia (92.3%), Côte d’Ivoire (84.2%) and Guinea-Bissau (78.9%).
Medications (domain 5)
Antiseptics/topical antibiotics: The percentage of facilities with antiseptics/topical antibiotics was in descending order: Mali (100.0%), Côte d’Ivoire (89.5%), Guinea-Bissau (84.2%), Liberia (73.0%).
Antifungals: The percentage of facilities with antifungals was high in Mali (94.7%) though less than 75% in Guinea-Bissau (68.4%), Liberia (42.3%) and Côte d’Ivoire (36.8%).
Oral/injectable antibiotics: The percentage of facilities with oral/injectable antibiotics was in descending order: Mali (100.0%), Côte d’Ivoire (89.5%), Guinea-Bissau (84.2%), Liberia (61.5%).
Analgesic or anti-inflammatory medication: The percentage of facilities with analgesic or anti-inflammatory medication was greater than 75% in all countries.
Ivermectin and albendazole: The percentage of facilities with ivermectin available was high in Côte d’Ivoire (84.2%) though low in the other countries (Guinea-Bissau – 36.8%, Liberia – 15.4%, Mali – 0%). The percentage of facilities with albendazole varied from 100% in Côte d’Ivoire to 36.8% in Mali.
Commodities/components of washing kit (domain 5)
In descending order, average percentage scores by country are: Guinea-Bissau (77.9%), Liberia (61.5%), Mali (40.0%) and Côte d’Ivoire (16.8%). In Côte d’Ivoire, the presence of the components of the washing kit was low, ranging from 0% for buckets or basin and towels to 52.6% for gloves. In Mali, the presence of these components varied from 18.4% for towels to 60.5% for gloves. In Guinea-Bissau and Liberia, the presence of the components of the washing kit varied from 42% to more than 90% for gloves.
Patient tracking system (domain 6)
The percentage of facilities with a system for identifying and quantifying the number of patients with lymphoedema was over 90% in Mali and Liberia though only 42.1% and 5.3% in Côte d’Ivoire and Guinea-Bissau, respectively.
Staff knowledge (domain 7)
The percentages of facilities with staff demonstrating knowledge of at least two of the listed signs/symptoms for lymphedema (7.1), signs/symptoms for an acute attack (7.2) and strategies to teach a patient (7.3) was >75% in Guinea Bissau and Liberia only.
The percentage of facilities with staff demonstrating knowledge of the following signs of lymphedema (7.1) was less than 50% in all countries: knobs on skin, mossy lesion, inability to perform daily activities or care for self, wounds/entry lesions. Additionally in Côte d’Ivoire 26.3% of respondents replied that they didn’t know the signs and symptoms of lymphedema. The percentage of facilities with staff demonstrating knowledge of the following signs and symptoms of an acute attack (7.2) was ≤50% in all countries: warmth of limb, fever, headache, chills and nausea/vomiting. The response was given as ‘don’t know’ by 52.6% and 36.8% of respondents from Côte d’Ivoire and Mali, respectively. The percentage of facilities with staff demonstrating knowledge of the following strategies to teach for preventing progression of lymphedema and preventing acute attacks (7.3) was ≤50% in all countries: cool leg, rest, provide elevation and avoid exercise. The response to 7.3 was given as ‘don’t know’ by 57.9% and 34.2% of respondents from Côte d’Ivoire and Mali, respectively.
MMDP challenges and feedback (domain 8, not scored)
Challenges in providing high quality lymphedema care to patients were identified by 63% (Guinea-Bissau and Mali) to 79% (Côte d’Ivoire) of facilities in the four countries. Across countries the two most cited challenges (8.2), were lack of medication/supplies (cited by 36.8% to 61.5% of facilities) and lack of training (cited by 26.9% to 47.4% of facilities). In all four countries the most common suggestion (at more than 70%) as to how services could be improved was to improve training for personnel.
Specific feedback included the need for: 1) at least two health workers in each health facility need to be trained on lymphedema case management; 2) advocacy with the WASH sector to improve water supply health facilities; 3) support groups for patients in endemic communities; 4) collaboration with nutrition support groups to improve the identification of lymphedema cases.
Staff demonstration of lymphedema management (domain 9, not scored)
In each health facility, staff were asked to demonstrate all the strategies they know for ongoing lymphedema management. In Côte d’Ivoire, only one (5.3%) facility out of the 19 evaluated was able to demonstrate any of the 11 listed strategies. In Guinea-Bissau, the proportion of health facilities that completely or partially demonstrated the 11 strategies ranged from 31.6% for instructed on proper use of antibiotic ointment/potassium permanganate to 42.1% for look for entry lesions. In Liberia, the proportion of health facilities that completely or partially demonstrated the 11 strategies ranged from 69.2% for ‘instructed patient on the management of an acute attack’ to 88.5% for ‘counselled patients on shoes use’. In Mali the proportion of health facilities that completely or partially demonstrated the strategies varied from 47.4% for counselled of shoes use to 68.4% for washed or instructed patient to wash affected leg.
Patients interview (domain 10, not scored)
Patients were interviewed from Mali (n=31), Liberia (n=5) and Côte d’Ivoire (n=3). The ages of the patients interviewed ranged from 29 to 89 years. 61.5% were female. Full results from domain 10 may be found in Supplementary Material: Table 2.
Knowledge of strategies to prevent acute attacks and progress of lymphedema (10.4)
Across countries, the strategy with the highest percent of total responses was hygiene/washing and drying of affected limb (27.6%) while the strategies with the lowest percent of total responses were prophylactic creams and prophylactic systemic antibiotics (both 2.3% of total responses). The response ‘don’t know’ was given by 18 respondents (corresponding to 10% of the total number of responses). Traditional remedies corresponded to 5.7% of total responses.
Strategies known for treating acute attacks (10.5)
Across countries, the most commonly cited strategy was to visit the health facility (27.4% of total responses). Elevation, avoiding exercise and cooling the leg were the next most cited strategies (11.0%, 9.6% and 8.2% of total responses, respectively). There was little to no knowledge about antibiotics (antibiotics for the skin and mouth had 2.7% of total responses while injectable antibiotics were never mentioned).
Washing of legs in a specific manner with soap and water either independently or with the assistance of someone (10.6)
Across countries, 79.5% of patients responded positively to this question. Among these patients, 83.3% washed his/her leg more than once a day (10.7)
Experience of pain, warmth, redness or swelling of the legs over the last 30 days (10.9)
Overall, 79.5% of the patients interviewed had never experienced pain, warmth, swelling and redness of either of his/her legs (10.8). Among those that responded positively to this question, the frequency of the aforementioned ‘sensation’ was reported as more than four days over the past 30 days for 6.5% of the patients interviewed.
Feelings about lymphedema in the past 30 days (10.10)
38.5% of patients responded very good while 25.6% and 5.1% responded bad and very bad respectively.
Satisfaction with services provided at the facility (10.11) and suggestions on how to improve services (10.12)
Overall, 51.3% if the patients interviewed were pleased with the lymphedema services provided at their facility (10.11). Across countries the three most common responses to the question asking how services can be improved at the facility to improve your satisfaction were: more supplies for patients (34.6%), improve training for staff (20.5%) and reduce cost of treatment (19.2%).
Hydrocele facility assessment tool
The facility benchmark of 75% was attained by 100% of the facilities assessed in Liberia, 91% of the facilities assessed in Mali, 50% of the facilities assessed in Cote D’Ivoire and 40% of the facilities assessed in Guinea Bissau. Across countries 79% of the facilities assessed attained the 75% benchmark.
Summary indicator results from the HFAT assessments are presented in Table 6 (‘Overall percentage of positively scoring indicators by domain’). Figure 6 graphically represents the percentage of facilities that were marked positively on HFAT indicators under domains 2, 3, 4, 5, 6 and 10. The full table can be found in Supplementary Material: Table 3.
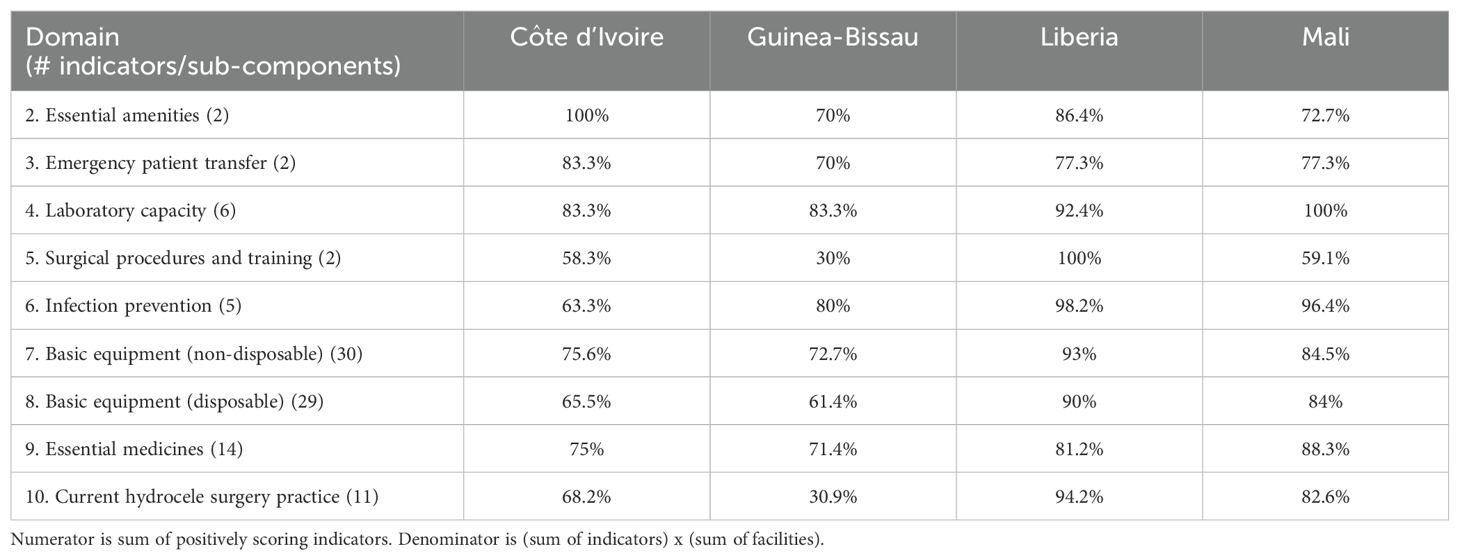
Table 6. Overall percentage of positively scoring indicators by HFAT domain.
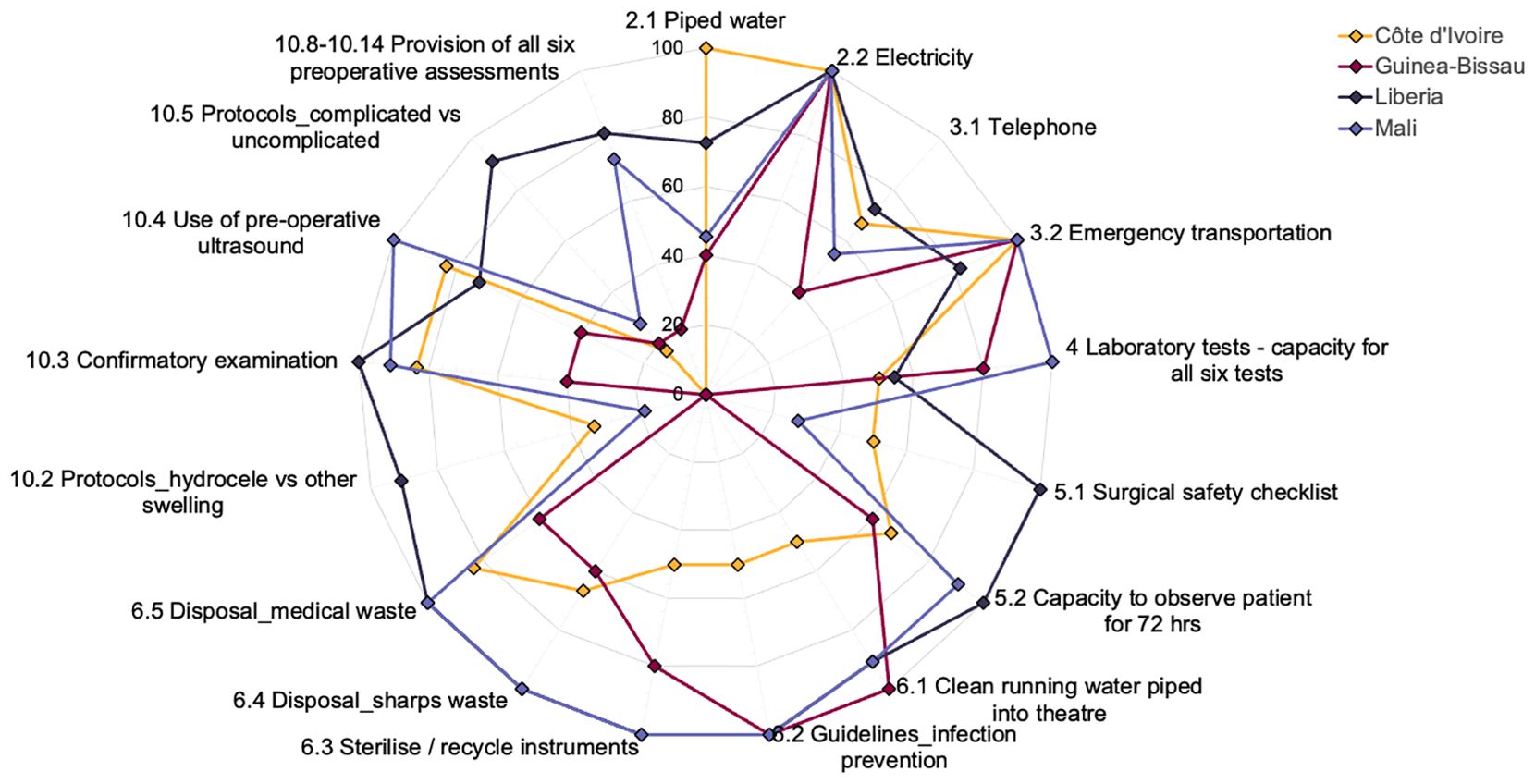
Figure 6. % Facilities achieving HFAT quality indicator criteria (domains 2-6 & 10).
Additional detail for domain 4 (four scored indicators), domain 7 (30 scored indicators), domain 8 (29 scored indicators), domain 9 (11 scored indicators) and domain 10 (seven scored indicators) is provided in Supplementary Material: Tables 4–6. Across countries and domains the overall percentage of indicators scoring positively was, in descending order, Liberia (90.5%), Mali (85.3%), Côte d’Ivoire (71.9%) and Guinea-Bissau (64.8%).
Across the domains ‘Surgical procedures and training’ (domain 5) stands out as a particularly poorly performing domain in all countries except Liberia, where the percentage of positively scored indicators was 100%. By contrast the overall percentage of positively scored indicators was < 60% in Côte d’Ivoire, Guinea-Bissau and Mali. In descending order, the % of facilities routinely using a surgical safety checklist was Côte d’Ivoire (50.0%), Mali (27.7%) and Guinea-Bissau (0%).
Breakdown by domain
Essential amenities (domain 2)
In all countries 100% of facilities reported positively on indicator 2.2 - availability of electricity supply. However, less than 50% of facilities in Mali and Guinea-Bissau reported positively against ‘water piped directly into facility’ (indicator 2.1).
Emergency patient transfer (domain 3)
The percentage of facilities reporting positively on 3.2 (‘Facility with an available functional ambulance or other vehicle for emergency transportation’) was 100% in Côte d’Ivoire, Guinea-Bissau and Mali and 81.8% in Liberia. The percentage of facilities reporting positively on 3.1 (facility with functioning telephone available to call outside at any time) varied from 40% (in the case of Guinea-Bissau) to 72.% (in the case of Liberia).
Laboratory capacity (domain 4)
The percentage of facilities with capacity to do all six tests (Haemoglobin testing, blood glucose tests, urine dipstick, malaria rapid diagnostic test, HIV screening, general blood clotting tests) was in descending order: Mali (100%), Guinea-Bissau (80%), Liberia (54.5%), Côte d’Ivoire (50%). Looking across countries, all facilities had capacity to do blood glucose test, malaria rapid diagnostic test and HIV screening, and all with the exception of one facility in Côte d’Ivoire had capacity for the haemoglobin tests.
Surgical procedures and training (domain 5)
The overall percentage of positively scoring indicators was in descending order: Liberia (100%), Mali (59.1%), Côte d’Ivoire (58.3%), Guinea-Bissau (30%). Looking beyond Liberia, the percentage of facilities routinely using a surgical checklist (indicator 5.1) varied from 0% in Guinea-Bissau to 50% in Côte d’Ivoire and the percentage of facilities with capacity to observe the hydrocele patients for 72 hours (indicator 5.2) varied from 60% in Guinea-Bissau to 91% in Mali.
Infection prevention (domain 6, five indicators)
The overall percentage of positively scoring indicators varied from over 96% in Liberia and Mali to 80.0% and 63.3% in Guinea-Bissau and Côte d’Ivoire, respectively. In the case of Liberia and Mali, a single facility in each country did not have clean running water available in the surgery theatre (indicator 6.1) though otherwise all facilities scored positively against all the indicators. In the case of Côte d’Ivoire only 50% of facilities scored positively against the following indicators: clean running water available in the surgery theatre (6.1), guidelines on standard precautions for infection prevention (6.2), functional process to sterilise/recycle surgical instruments. In the case of Guinea-Bissau, 100% of facilities scored positively against indicators 6.1 and 6.2 though only 60% scored positively against ‘functional process to finally dispose of waste sharps’ (6.4) and ‘functional process to finally dispose of medical waste other than sharps waste’ (6.5).
Basic equipment – non disposable (domain 7, monitoring items n=8, surgical items n=22)
The overall percentage of positively scoring indicators was in descending order: Libera (93.0%), Mali (84.5%), Côte d’Ivoire (75.6%), Guinea-Bissau (72.7%). The percentage of facilities equipped with all the items for monitoring varied from 81.8% in Guinea-Bissau to 16.7% in Côte d’Ivoire. The following items were available in less than 75% of the assessed facilities: Ambu bag - Côte d’Ivoire (50.0%), Mali (72.7%); Laryngoscope – Côte d’Ivoire (66.7%), Guinea-Bissau (66.0%); Endotracheal tube – Mali (72.7%); Thermometer – Côte d’Ivoire (33.3%). The percentage of facilities equipped with all 22 non-disposable surgical items was 45.5% in Liberia, 36.4% in Mali, 20.0% in Guinea-Bissau and 0% in Côte d’Ivoire.
Basic equipment – disposable (domain 8, 29 items)
The overall percentage of positively scoring indicators was in descending order: Libera (90.0%), Mali (84.0%), Côte d’Ivoire (65.5%), Guinea-Bissau (61.4%). The percentage of facilities equipped with all 29 disposable items was 36.4% in Liberia, 18.2% in Mali and 0% in Côte d’Ivoire and Guinea-Bissau. Across countries, the least available item was surgical mesh (for hernia) – available in <28% of facilities in Côte d’Ivoire, Guinea-Bissau and Mali and in 63.6% of facilities in Liberia.
Essential medicines (domain 9, 14 medicines)
The availability of 14 essential medicines was assessed. In Mali 10 of the 14 medicines were found in all 11 facilities assessed. In Liberia 13 of the 14 medicines were available in 81.8% of the facilities assessed. In Côte d’Ivoire two of the medicines were available in all facilities assessed and in Guinea-Bissau one of the 14 medicines was available in all facilities assessed.
Current hydrocele surgery practices (domain 10, 11 indicators)
The overall % of positively scoring indicators was (in descending order): Liberia (90.5%), Mali (85.3%), Côte d’Ivoire (71.9%), Guinea-Bissau (64.8%). The percentages of facilities with protocols available to support staff to distinguish between LF hydroceles and other causes of scrotal swellings (indicator 10.2) and between complicated and uncomplicated hydrocele cases (indicator 10.5) were particularly low in Côte d’Ivoire (10.2 – 33.3%, 10.5 – 16.7%), Guinea-Bissau (10.2 – 0%, 10.5 – 20%) and Mali (10.2 – 18.2%, 10.5 – 27.7%). By contrast 91.0% of the facilities assessed in Liberia had these protocols available. The percentages of facilities reporting that the operating surgeon conducted confirmatory examination before the patient is brought to the operating theatre and surgery undertaken (10.3) varied from 40% in Guinea-Bissau to 100% in Liberia. Reported facility level use of ultrasound for preoperative differential diagnosis (10.4) varied from 40% in Guinea-Bissau to 100% in Mali. The percentage of facilities providing all seven components of the pre-operative assessment was (in descending order): Liberia (81.0%), Mali (72.7%), Guinea-Bissau (20.0%), Côte d’Ivoire (0.0%).
Interviews
A total of 21 patients were interviewed, 15 in Mali, four in Côte d’Ivoire and two in Liberia (Table 7). All patients (100%) reported that they had received enough knowledge to make an informed decision about accepting hydrocele surgery. Overall satisfaction with service delivery was 81%. Among the 21 patients 52% reported improvement/significant improvement in socioeconomic status and 81% reported improvement/dramatic improvement in family life.

Table 7. Summary results from HFAT patient interview showing % respondents giving most positive response (from multiple choice options).
Discussion
Global picture
Previous DIP assessments conducted in Ghana (13) and Vietnam (14) for lymphedema management, and Bangladesh, Malawi, Nepal, Benin, Burkina Faso, Ghana, Guinea, Niger, and Nigeria for hydrocele services (7) demonstrated the important use of DIPs to document which facilities are offering services and yielded actionable suggestions to strengthen MMDP services and compliance to WHO’s recommended essential package of care. Data from these assessments will support individual country claims to have eliminated LF as a public health problem as part of dossier submission to WHO for validation.
This paper has described the process and approach of using DIP methodologies for both lymphedema and hydrocele in Côte d’Ivoire, Guinea-Bissau, Liberia and Mali through the facilitation of the electronic based LFAT and HFAT tools. The ability of these countries to successfully document results of the assessments in 10% of health facilities for lymphedema and 100% of hospitals targeted to provide hydrocele surgery will also assist the country programmes to achieve the dossier requirements set out by the World Health Organization for the elimination of LF.
Similar to other DIP assessments the results indicate that each country has unique areas for improvement and the data generated from the assessment can be used to develop a quality improvement plan, such that countries can be better assured that people affected by LF morbidity are being offered quality hydrocoele surgery and instruction on the management of their lymphedema. Because quality issues may compromise the availability of essential packages of care it is important that national LF programmes track completion of action steps that arise from the assessment. The potential use of these tools to assist in the maintenance of general health services to communities suggests that national programmes could apply these tools to other surgical services such a trichiasis surgeries and management of other skin diseases such as leprosy, yaws, Buruli ulcer, and scabies.
LFAT: key learnings and actions arising
The results of the lymphedema facility assessments may be linked to prior experience in implementing lymphedema management at both the level of the country and the specific geographic area. As highlighted in the introduction, it was only in Liberia that all the facilities assessed had experience in implementing lymphedema management prior to the assessments. However, even in Liberia only 12% of the facilities assessed attained the 75% benchmark.
While the attainment of the 75% facility benchmark for the LFAT assessments was notably low in all countries, we acknowledge that the 75% figure (or any score) - as explained in the WHO DIP guidance - does not indicate pass/fail (6). Instead it indicates the considerable need to explore specific causes of underperformance and develop site specific corrective actions. The scores from these assessments may help country programmes set benchmarks for future assessments and track quality improvements over time.
With regard to indicator scores, the only indicator that did not achieve the 75% indicator benchmark in any of the countries was ‘trained staff - Community Health Care Providers trained in lymphoedema management’. The need for staff training was corroborated by both the interviews with facility staff on staff knowledge, challenges and service improvement suggestions, and the patient interviews. In the case of Mali, Guinea-Bissau and Côte d’Ivoire, related quality improvement actions led to the training of health workers, community health workers and patients. The issue of technical capacity and health care workforce is highlighted in the LF disease summary of the WHO 2021-2030 NTD Roadmap - with the recommendation to “include LF morbidity management modules in health workforce training curriculums” (15). Programmes may look to The Togo National Lymphedema Management Programme which achieved inclusion of lymphedema management in the routine healthcare package for learnings in this regard (integrating lymphedema management into the curriculum for medical staff was one of the five major components of the programme) (16). The evaluation by Dung et al. of lymphedema management services in Vietnam, two years prior to WHO validation (in 2018) illustrates how lack of trained staff is not just an issue for new lymphedema management programmes (14); their evaluation found that none of the facilities assessed had any staff who had been trained in the last two years.
In all countries except Liberia, scores on availability of MMDP guidelines were notably low. The low rates are due to the lack of implementation of morbidity management activities in the targeted areas of these three countries. With the exception of Côte d’Ivoire (with score of 100%), the results were similar for indicator 3.4 assessing the availability of local language/pictorial patient education/awareness. Development of Information, Education and Communication (IEC) materials/implementation of IEC activities was subsequently included as a corrective action in all four countries.
The availability of the named medicines was variable both within and between countries. The absence of ivermectin in any of the health facilities assessed in Mali was linked to the fact that LF mass drug administration (ivermectin + albendazole) has been stopped throughout the country; albendazole, which is also used as an intestinal dewormer, was available in 36.8% of health facilities. The cross-country issue with the availability of medications was corroborated by the interviews with health facility staff. The lack of medication/supplies was highlighted as top challenge to providing quality lymphedema care to patients. Whether availability of a named medication translates through to availability for a lymphedema patient may be questioned. Edmiston et al. reporting on the results of a lymphedema facility assessments in Ghana noted that “health facilities may feel as though LF patients should be treated with medicines and commodities that have been provided by the NTD Program, and do not consider those patients as part of the general patient population” (13).
The availability of the components of the washing kit was variable both within and between countries, and notably low in Côte d’Ivoire. Among the list of components, gloves scored relatively high as gloves are part of the items regularly available in health facilities. Subsequent to this assessment, partners supported the provision of washing kits (free of charge) to all patients within the assessment areas of all four countries.
HFAT: key learnings and actions arising
As explained above, scores may be linked with prior implementation experience at both the national and sub-national level. In the case of the HFAT, Mali, the country with the most experience with offering hydrocele surgeries through the LF programme, had the highest overall score. The Mali LF programme started support for hydrocele surgery in 2008 with the National Programme for LF Elimination free hydrocele surgery campaign in Kolokani district (Koulikoro region). Five of the ten districts covered by the hydrocele facility assessments reported in this manuscript had received former support through the LF programme for the provision of hydrocele surgeries.
Across the nine scored domains, the results from domain 5 ‘surgical procedures and training’ were notably low (30.0-59.1%) in all countries, with the exception of Liberia (with a score of 100%). The results from this domain highlighted that the use of the WHO surgical safety checklist is not a widespread practice; in the case of Guinea-Bissau, none of the facilities assessed routinely used the surgical checklist.
The results around current hydrocele practice highlighted relatively good practice in Liberia (all ≥73%) though significant room for improvement in the other countries – with for example poor availability of protocols to support staff with differential diagnosis and in the case of Guinea-Bissau, no indicator scoring positively for >40% of the facilities assessed. Notably all facilities assessed in Mali used pre-operative ultrasound. As described in WHO (2019) ultrasound (as opposed to transillumination which is non-specific) and a good physical examination is the preferred diagnostic modality as it may rule in or out other scrotal pathologies, confirm Stage I-II hydroceles and identify hernias (17).
The results from domains 5 and 10 informed the training of surgeons, provision of Filaricele Anatomical Surgical Task Trainer (FASTT) training material4, and the development and implementation of guidelines to distinguish hydrocele from LF and non-LF (Mali), ensuring that the hydrocele surgery checklist is available in each facility.
The results on basic equipment and medicines highlight significant deficit with regard to the availability of the listed disposable and non-disposable items and medicines. However, as highlighted by Martindale et al. (7), such deficits can be resolved in the short term through purchasing additional supplies and in the longer term through strengthening stock management and supply chain processes. Related quality improvement actions taken (prior to the start of programme activities) as a consequence of these assessments included the provision of surgery boxes with instruments (scissors, forceps) and operating kits containing medicines and consumables to all assessed hospitals in the four countries and electrocautery machines being acquired for Côte d’Ivoire and Guinea-Bissau. In one facility in Guinea-Bissau, gas for resuscitation was recharged and technical staff were brought in from the capital (surgeons, instrumentalist, anaesthetist) in order to raise the hospital’s score beyond 75% and be able to carry out the training of surgeons and a hospital surgery camp.
Programme managers should carry out an in-depth analysis of these shortcomings and develop realistic action plans with the technical and financial support of partners and Ministries of Health to increase the provision of quality care.
Programmatic use of data
The Hydrocele Surgery Facility Assessment Tool (HSFAT) and the DIP (WHO Direct Inspection Protocol) for lymphedema gave Sightsavers exceptional foundations to build from. While the digitisation of data collection tools has been previously demonstrated (7, 14) one of the main benefits of the system we report on in this paper are the automated dashboards and automated reports. These highlight challenge areas for each country and facilitate the creation of action plans, focusing on areas which need improvement. They also help programme managers easily complete the two indicators on the WHO EPIRF (Number of implementation units with at least one facility designated to provide recommended essential package of care and Total number of designated health facilities providing care) (11). Results can also be used to complete the elimination dossier by providing the number of health facilities evaluated as part of LF morbidity management. Future implementation of these assessments will include stronger training for LF focal persons in national programmes in these areas of data use.
Limitations and challenges
There were some challenges faced while undertaking the assessments that should be taken into consideration while planning for future use of both tools. Insecurity in certain areas was a challenge, for example in Mali respondents from three health facilities who could not be reached on site because of insecurity were interviewed by telephone to collect all the information required for the assessment. Additionally, there was on occasion resistance to use the tool in the fear that results may not be flattering to the programme. This was mitigated through communicating the purpose of the assessments – which is to help identify challenges and improve services. Timing of the assessments was also sometimes a challenge, as Sightsavers requested countries complete them before the WHO’s two-year prior to dossier submission timeline. However, doing them early builds skills and familiarises health personnel so they are better prepared for the assessments needed for dossier development – when this perspective was shared, national programmes were agreeable.
In terms of data collection, the knowledge of survey teams/enumerators around lymphedema management was sub-optimum - pointing to the need for better training of survey teams in future assessments. In some cases elucidation of ‘intended’ responses may also be brought into question e.g. where positive scores for soap were linked to soap available for staff use (as opposed to lymphedema patients).
In terms of the analyses present in this manuscript, we acknowledge shortcomings related to the fact that the results from some of the non-scored indicators in the assessments (e.g. HFAT 10.15-10.23) have not been covered. An important finding was that the technique of excision of the tunica vaginalis as recommended by GAELF and WHO is not well known and applied in countries (17). The need for continuous training prior to the start of surgical activities in all countries was the first step in the process of implementation of hydrocele surgery. We also acknowledge that we have not presented LFAT results by facility type.
Contributions to health systems strengthening
The HFAT and LFAT assessments have the potential of contributing to wider health system strengthening efforts and progress countries towards greater universal health coverage (UHC) - where all people, including people with disabilities, have access to the full range of quality health services they need, when and where they need them, without financial hardship. We note a few key areas where their use contributed more broadly to strengthening the health system. One is strengthening the capacities of personnel in digital data collection, data use, and in best practices in undertaking facilities assessments. Another is through strengthening the systems for acquisition of essential drug stock and equipment for health facilities – e.g. provision of drugs, consumables, surgical boxes, and cautery machines. LF programmes may wish to look to Liberia to learn from national experience in the integration of case management medicines and supplies into the national supply chain (18).
In Mali the low presence of basic washing kits in health facilities may in part be due to the fact that these items are considered to be non-medical by health systems and not part of the essential supply list, with an unwritten expectation that such materials would need to be furnished by individuals or external programmes. The Mali programme is planning advocacy efforts around integration of these non-medical items into the supply chain, especially in districts where lymphedema cases are recorded and in high numbers.
A lack in availability and readiness to provide high quality morbidity management care to patients for one condition is likely to be an issue for other health conditions as well. Sub-optimal scores on health facility assessments may indicate more systemic accessibility issues and point towards similar corrective actions. In the case of LFAT, these corrective actions may particularly benefit individuals requiring long-term care to manage the debilitating symptoms of other skin related conditions (e.g. inflammatory episodes of adenolymphangitis (ADL), onchocerciasis related skin disease, leprosy, etc.).
Results from more general domains (i.e. those not specific to LF), such as infrastructure-improve water source, have great significance for broader health service delivery and as such may be used to support the prioritisation of quality improvements more widely. Achieving this will require effective dissemination to decision makers such that this evidence can inform wider and more comprehensive national health policies, development plans and budget allocations. Collaboration, both within other departments in the MoH (e.g. national hospital evaluation agency) and beyond is pivotal.
Assessment results also highlighted the constant and ongoing need for health facilities to ensure disease specific guidelines for the treatment and monitoring of chronic disease in patients are kept updated and available to health workers. Moreover, these guidelines should be reinforced through ongoing refresher trainings of health staff.
Longer term plans for LFAT and HFAT assessment tools
In terms of longer terms planning in individual countries, Mali, for example have used the assessments as a catalyst: since these assessments were done, further LFAT and HFAT assessments have been supported in the Koulikoro region and the district of Bamako in Mali. At the time of writing, plans are underway to extend assessments to Kayes and Segou and mobilise funds for Mopti region. The country also plans to do advocacy with the WASH sector to improve water supply at the level of health facilities in the region, establish support groups for hydrocele and lymphedema patients in endemic communities and collaborate with nutrition support groups to improve the identification of lymphedema cases.
Based on feedback from the four countries who undertook assessments, Sightsavers will be updating the tools, including the addition of patient interview results into dashboards and reformatting of the final automated report. Sightsavers is also working on better aligning the content and scoring protocol of the LFAT with the WHO DIP.
This paper illustrates the value of using these assessment tools in countries at various stages towards the elimination of LF and with varying levels of LF morbidity management experience. The tools are available to all national LF programmes and implementing partners; interested parties can contact the corresponding author of this paper.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: The datasets are owned by the national LF programmes of each country. If needed they can be contacted through the corresponding author: cGRvd25zQHNpZ2h0c2F2ZXJzLm9yZw==.
Author contributions
WB: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. VA: Supervision, Writing – review & editing. BA: Investigation, Writing – review & editing. SB: Conceptualization, Writing – original draft, Writing – review & editing. KB: Supervision, Writing – review & editing. MC: Investigation, Writing – review & editing. YC: Supervision, Writing – review & editing. BD: Supervision, Writing – review & editing. SD’S: Formal analysis, Writing – original draft, Writing – review & editing. SD: Writing – review & editing. GG: Writing – review & editing, Investigation. BM: Writing – review & editing, Supervision. BN: Writing – review & editing, Conceptualization, Software. DN: Writing – review & editing, Supervision. CN: Writing – review & editing, Conceptualization, Software. AP: Supervision, Writing – review & editing. ER: Supervision, Writing – review & editing. AS: Writing – review & editing, Supervision. PD: Conceptualization, Methodology, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
Côte d’Ivoire, Guinea-Bissau, Liberia, and Mali Ministries of Health. The funders who made the related programmatic work possible. Andy Tate, Sightsavers, for developing maps. Konan Nguessan, previously with Sightsavers, for work on the assessments in Côte d’Ivoire.
In memoriam
This manuscript it dedicated in memory to Dr. Massitan Dembele from the National LF Elimination Programme in Mali.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fitd.2024.1380042/full#supplementary-material
Footnotes
- ^ https://www.who.int/news-room/fact-sheets/detail/lymphatic-filariasis.
- ^ https://www.dimagi.com/commcare/.
- ^ Metabase. San Francisco, CA, USA: Metabase. Available at: https://www.metabase.com/.
- ^ FASTT SIMULATOR: Manufacturing Manual. Available at https://www.hki.org/wp-content/uploads/2019/10/HKI_FASTTSimulatorManual_FINAL_digital.pdf.
References
1. WHO. Guideline: Alternative Mass Drug Administration Regimens to Eliminate Lymphatic Filariasis. Geneva: World Health Organization (2017). Available at: https://www.ncbi.nlm.nih.gov/books/NBK487830/.
2. World Health Organization. (2012). Global programme to eliminate lymphatic filariasis: progress report, 2011. In: Weekly Epidemiological Record, vol. 87(37). Geneva: World Health Organization. p. 346–356. Available at: https://iris.who.int/handle/10665/241959.
3. World Health Organization. (2023). Global programme to eliminate lymphatic filariasis: progress report, 2022. In: Weekly Epidemiological Record, vol. 98. Geneva: World Health Organization. p. 489–501. Available at: https://iris.who.int/handle/10665/373357.
4. WHO. Validation of elimination of lymphatic filariasis as a public health problem. Geneva: World Health Organization (2017). Available at: https://apps.who.int/iris/bitstream/handle/10665/254377/9789241511957-eng.pdf.
5. WHO-GAELF. Lymphatic filariasis - managing morbidity and preventing disability: an aide-mémoire for national programme managers, second edition. Geneva: World Health Organization (2021). Available at: https://www.who.int/publications/i/item/lymphatic-filariasis-managing-morbidity-and-preventing-disability-an-aide-m%C3%A9moire-for-national-programme-managers-2nd-ed.
6. Web Annex A. Protocol for evaluating minimum package of care of morbidity management and disability prevention for lymphoedema management in designated health facilities. In: Lymphatic filariasis - managing morbidity and preventing disability- an aide-mémoire for national programme managers, second edition. World Health Organization, Geneva (2021). Available at: https://iris.who.int/bitstream/handle/10665/339870/9789240017085-eng.pdf.
7. Martindale S, Mableson H, Bodimeade C, Hume H, Badia-Rius X, Karim J, et al. The development and roll-out of a new hydrocoele surgery facility assessment tool for the elimination of lymphatic filariasis. Int Health. (2022) 14:II55–63. doi: 10.1093/inthealth/ihac020
8. World Health Organization. Tool for situational analysis to assess emergency and essential surgical care(2007). Available online at: https://www.who.int/docs/default-source/integrated-health-services-(ihs)/csy/gieesc/whotoolsituationalanalysiseesc.pdf?sfvrsn=fccb6814_5 (Accessed November 20, 2024).
9. World Health Organization. Service availability and readiness assessment (SARA): an annual monitoring system for service delivery(2013). Available online at: https://www.who.int/data/data-collection-tools/service-availability-and-readiness-assessment-(sara) (Accessed November 20, 2024).
10. WHO/UNICEF. Joint Monitoring Programme for Water Supply and Sanitation. Core questions and indicators for monitoring WASH in health care facilities in the Sustainable Development Goals. Geneva: World Health Organization and the United Nations Children’s Fund (UNICEF) (2018). Available at: https://www.who.int/publications/i/item/9789241514545.
11. WHO. PC Epidemiological Data Reporting Form v6. Available online at: https://apps.who.int/neglected_diseases/ntddata/forms/jap/en/WHO_EPIRF_PC.xlsm.
12. Falchetta G, Hammad AT, Shayegh S. Planning universal accessibility to public health care in sub-Saharan Africa. Proc Natl Acad Sci U S A. (2020) 117:31760–9. doi: 10.1073/pnas.2009172117
13. Edmiston M, Atinbire S, Mensah EO, Mensah E, Alomatu B, Mensah KA, et al. Evaluating the availability and quality of services for lymphatic filariasis morbidity in Ghana. PloS Negl Trop Dis. (2023) 17:e0010805. doi: 10.1371/journal.pntd.0010805
14. Dung DT, Binh VTL, Worrell CM, Brady M, Walsh V, Yajima A, et al. Evaluation of a facility-based inspection tool to assess lymphedema management services in Vietnam. PloS Negl Trop Dis. (2020) 14:1–13. doi: 10.1371/journal.pntd.0008773
15. WHO. Ending the neglect to attain the Sustainable Development Goals: a road map for neglected tropical diseases 2021–2030. Geneva: World Health Organization (2020).
16. Mathieu E, Dorkenoo AM, Datagni M, Cantey PT, Morgah K, Harvey K, et al. It is possible: availability of lymphedema case management in each health facility in Togo. Program description, evaluation, and lessons learned. Am J Trop Med Hyg. (2013) 89:16–22. doi: 10.4269/ajtmh.12-0453
17. WHO. Surgical approaches to the urogenital manifestations of lymphatic filariasis. Surgical approaches to the urogenital manifestations of lymphatic filariasis. Report from an informal consultation among experts. Geneva: World Health Organization (2019).
Keywords: lymphatic, filariasis, hydrocele, lymphedema, assessments, digitisation
Citation: Bougma WR, Aiogalé VM, Attoumbre BY, Bartlett S, Brahima K, Coulibaly M, Coulibaly YI, Dicko BM, D’Souza S, Doumbia SS, Gargannah GM, Musa B, Ngom B, Norbert DN’G, Nwosu C, Papique AL, Rogers EJ, Sarr A and Downs P (2024) Use of digital assessment tools to measure health facility readiness to provide the WHO recommended package of care for lymphatic filariasis morbidity. Front. Trop. Dis. 5:1380042. doi: 10.3389/fitd.2024.1380042
Received: 31 January 2024; Accepted: 11 November 2024;
Published: 17 December 2024.
Edited by:
Sunny Doodu Mante, African Filariasis Morbidity Project, GhanaReviewed by:
Ramaswamy Kalyanasundaram, University of Illinois Chicago, United StatesAnders Seim, Health and Development International, United States
Copyright © 2024 Bougma, Aiogalé, Attoumbre, Bartlett, Brahima, Coulibaly, Coulibaly, Dicko, D’Souza, Doumbia, Gargannah, Musa, Ngom, Norbert, Nwosu, Papique, Rogers, Sarr and Downs. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Philip Downs, cGRvd25zQHNpZ2h0c2F2ZXJzLm9yZw==