 Susan F. D’Souza1
Susan F. D’Souza1 John P. Awio2
John P. Awio2 Jehoshaphat Albarka3
Jehoshaphat Albarka3 Windtaré Roland Bougma4
Windtaré Roland Bougma4 Sarah Bartlett1
Sarah Bartlett1 Christian Nwosu5
Christian Nwosu5 Babacar Ngom6Anthony Wani7Anita Gwom3Moses Okello7Abraham Aba3
Babacar Ngom6Anthony Wani7Anita Gwom3Moses Okello7Abraham Aba3 Sarah Irema7Martins Imhansoloeva8Dauda Nurudeen9Charles Wamboga10Mark T. Debam11Haruna Zainab12Attahiru Aleiro13Malam H. Salah14
Sarah Irema7Martins Imhansoloeva8Dauda Nurudeen9Charles Wamboga10Mark T. Debam11Haruna Zainab12Attahiru Aleiro13Malam H. Salah14 Philip Downs15*
Philip Downs15*- 1Neglected Tropical Diseases Department, Sightsavers, Haywards Heath, United Kingdom
- 2Department of Surgery, Lira University, Lira, Uganda
- 3Operations Planning and Finance Department, Sightsavers, Kaduna, Nigeria
- 4Neglected Tropical Diseases Department, Sightsavers, Ouagadougou, Burkina Faso
- 5Neglected Tropical Diseases Department, Sightsavers, Abuja, Nigeria
- 6Neglected Tropical Diseases Department, Sightsavers, Dakar, Senegal
- 7Operations Planning and Finance Department, Sightsavers, Kampala, Uganda
- 8Neglected Tropical Diseases Research Department, Abuja, Nigeria
- 9Neglected Tropical Diseases Department, Sightsavers, Kaduna, Nigeria
- 10Programme for the Elimination of Lymphatic Filariasis, Ministry of Health, Kampala, Uganda
- 11Neglected Tropical Disease Programme, Benue State Ministry of Health and Human Services, Makurdi, Nigeria
- 12Neglected Tropical Diseases Office, Kaduna State Ministry of Health, Kaduna, Nigeria
- 13Neglected Tropical Diseases Office, Department of Public Health, State Ministry of Health, Birnin Kebbi, Nigeria
- 14Neglected Tropical Diseases Control, Program, Sokoto State Ministry of Health, Sokoto, Nigeria
- 15Neglected Tropical Diseases Department, Sightsavers, Durham, NC, United States
Introduction: Surgery for hydrocele is part of the WHO recommended essential package of care for people affected by Lymphatic filariasis (LF). In Uganda and Nigeria, LF programme support for hydrocele surgery began in 2017. In 2021 the two programmes adopted a newly developed smartphone-based application to monitor hydrocele surgery and outcome. The application, referred to as the Hydrocele Tracker, gathers information on surgical registration, preoperative information, intraoperative information, postoperative information and follow-up evaluations. It was developed to improve supervision, understand surgical outcomes and reasons for complications, improve reporting and improve data quality for Ministries of Health with active LF programmes.
Methods: Hydrocele patient information was collected between October 2021 and May 2023 in Uganda (Lango sub-region, 9 districts) and March 2021 - September 2022 in Nigeria (Benue, Kaduna, Kebbi, Sokoto and Kogi States). Additionally patient feedback surveys were undertaken to elicit patient experience and satisfaction with the hydrocele surgery.
Results: Patient data from 2,911 records in the Hydrocele Tracker are presented.
Discussion: The discussion highlights the implications of the data for LF programming, the value of digitisation and approaches to address data quality.
Introduction
Lymphatic filariasis (LF) is a preventable neglected tropical disease (NTD) caused by infection with the filarial nematode parasites Wuchereria bancrofti, Brugia malayi or B. timori (with the Brugia spp being confined to Southeast Asia) (1). The parasites are transmitted person to person by mosquitos in the genera Culex, Anopheles, Mansonia and Aedes. The nematode larvae grow into adults in the lymphatic system where resulting damage causes dilation of the vessels. Estimates suggest that 63% of symptomatic infections are men who exhibit urogenital manifestations including hydrocele and penoscrotal lymphoedema, resulting in physical discomfort, psychosocial sequelae and economic loss (1).
Surgical hydrocelectomy is an essential component of the WHO recommended minimum package of care for LF morbidity management and disability prevention (MMDP) (2), also referred to as disease management and disability inclusion (DMDI). Hydrocelectomy is recommended for all stages of hydrocele, even small hydrocele, to prevent progression to more severe and therefore more difficult to treat stages. However, support for and reporting of hydrocele surgeries has lagged behind that of LF mass drug administration (MDA) and concerted effort is often required to fulfil the LF elimination dossier requirement to evidence the number of patients with hydrocele and the availability of care/readiness of designated health facilities (3). In the 2022 reporting period to WHO, nine of 34 LF endemic countries reported care (surgery) for men with hydrocele. Among the 19 countries that have achieved elimination of LF as a public health problem, only three have reported on MMDP after validation (4).
With regard to surgical approaches, the WHO (2019) report from an informal consultation of experts is a central guiding document providing the latest recommendation for standard surgical procedures and processes around post operative care (1). The report recommends that patients with uncomplicated LF hydroceles (Stage I–II or I-III), Grade 0–1 should be treated at First Level Hospitals, while those with complicated hydroceles (Stage III or IV–VI), Grade 2–4 should be treated at Second or Third Level Hospitals (DCP3 terminology, WHO 2019). To reduce the risk of recurrence the “technique of excision/resection of the tunica vaginalis is recognised as the preferred procedure for all stages of LF hydrocele” (1).
Risk estimates for complications after hydrocelectomy (both filarial and non-filarial) vary. In the high income setting of Helsinki (Finland), 16% of non-filarial hydroceles developed complications within 90 days post-surgery (5). In African settings, complications from filarial hydroceles range between 3 and 12% between day 1 and 14 post surgery (6–8). Estimates of recurrence vary from 3-5% in Ghana, Burkina Faso and Togo (7), around the one year follow-up point to 7% in Nigeria, 1-3 years post-surgery (8). Poor follow-up and under reporting of complications is a known challenge (9).
The efforts to strengthen surgical reporting and outcome monitoring described in this paper respond not only to the needs of the global effort to eliminate LF as a public health problem but also national efforts to strengthen data collection, data quality and data use in the health sector more broadly (10, 11). As described in the Uganda Health Information and Digital Health Strategic Plan 2020/21-2024/25 “Health information is a vital component in a health system and is a critical precursor for effective decision-making for achieving Universal Health Coverage (UHC) of interventions and positive health outcomes” (11). The need for robust information systems that promote monitoring and accountability related to surgical and anaesthesia care is highlighted in the National Surgical, Obstetrics, Anaesthesia & Nursing Plan (NSOANP) for Nigeria, 2019-2023 (10).
Against this backdrop, the objectives of this paper are to contribute towards the development of a standardised care plan for hydrocele patients that is “sufficiently routine to allow evaluation of outcomes as well as reporting and publication in order to benefit other clinicians and patients” (1) by:
1) Learning from the efforts of two national programmes (Uganda and Nigeria) to scale up their support for hydrocele surgeries.
2) Documenting the epidemiological findings from an interrogation of routinely collected (pre-, intra- and post-operative) programme data.
3) Learning from the piloting of a digital tool, the Hydrocele Tracker, developed to improve patient follow-up and supervision, understand surgical outcomes and reasons for complications, improve reporting and improve data quality.
Country background
Uganda
Endemicity of LF has been reported from 70 districts, covering much of the Northern and Eastern regions and two districts (Bundibugyo & Ntoroko) in the Western region (12). The national programme to eliminate LF (PELF) was launched in 2002 and the initial focus was on MDA with ivermectin and albendazole1. The PELF started supporting MMDP, including hydrocele surgeries in 2017. Currently all 70 districts are under post MDA surveillance and the programme is planning to submit its elimination dossier to WHO in 2026. All 70 endemic districts have or are within the catchment of designated facilities for hydrocele surgeries and 33 of these districts have hydrocele burden estimates. A hydrocele surgery indicator (“Patient with LF(hydrocele)”) was included in the national health management information system (HMIS) in 2020 and hydrocele surgeries were first reported to WHO in 2021. Prior to the implementation of the surgeries reported in this paper, a total of 1,448 hydrocele surgeries had been reported by the national programme.
The Lango sub-region LF MMDP project (reported upon in this paper), was informed by a knowledge, attitude, and practice (KAP) study conducted on the chronic manifestations of LF, undertaken in the Northern region of Uganda in 2017 in the districts of Lira, Kitgum and Yumbe (13). The challenges of hydrocele surgery in the Lango sub-region were recognised as early as 1924 (14).
Outside the targeted support of the LF programme, hydrocele surgery in Uganda is dependent upon referrals (in both the state and private sector), and surgical camps (15, 16). Notably, hydrocelectomy was the commonest operation performed in the pilot surgical camp undertaken in Apac and Lira districts (Lango sub-region) in 1998 (16).
Nigeria
The National LF Elimination Programme (NLFEP) started in 1997 (17). Across the country, 583 (or 75% of total) Local Government Areas (LGAs) are endemic for LF. Within the five States (Benue, Kaduna, Kebbi, Kogi and Sokoto) reported in this paper, LF endemicity ranges from 52% of LGAs (in the case of Kogi) to 95% (in the case of Kebbi). Across Kaduna, Kebbi, Kogi and Sokoto 25 of 69 endemic LGAs have stopped MDA. All five states are targeting 2030 for elimination of LF as a public health problem. Hydrocele surgeries have been reported from the states to the FMOH since 2017 (Kebbi), 2018 (Kogi and Sokoto) and 2019 (Benue and Kaduna). Designated secondary hospitals for hydrocele surgeries ensure coverage of all health facility catchment areas in these states. In the national HMIS there is an LF morbidity indicator for cases of elephantiasis though no specific indicator for hydrocele surgeries. Hydrocele surgeries are captured under a general HMIS indicator for surgeries (which is not disaggregated).
Outside the targeted support of the LF programme, hydrocele surgery in Nigeria is usually provided by general practitioners on a patient-by-patient basis (in both state and private sector).
Methods
Study area
The hydrocele surgery patient information presented in this paper was collected between October 2021 and July 2023 in the Lango sub-region of Uganda and March 2021 - September 2022 in Benue, Kaduna, Kebbi, Kogi and Sokoto States, Nigeria.
Designated facilities
In the case of Uganda, the hydrocele surgeries reported in this paper were undertaken in all nine government HC IV hospitals, one government district/general hospitals and one Private and Not for Profit district/general hospital, in Lango sub region in Northern Uganda (Figure 1). These hospitals are categorised as DCP 3/WHO (2019) first level hospitals and the doctors present are general practitioners. In the case of Nigeria, the hydrocele surgeries reported in this paper were undertaken in 21 secondary health facilities (level 2 hospitals), in Benue, Kaduna, Kebbi, Kogi and Sokoto (Figure 1).
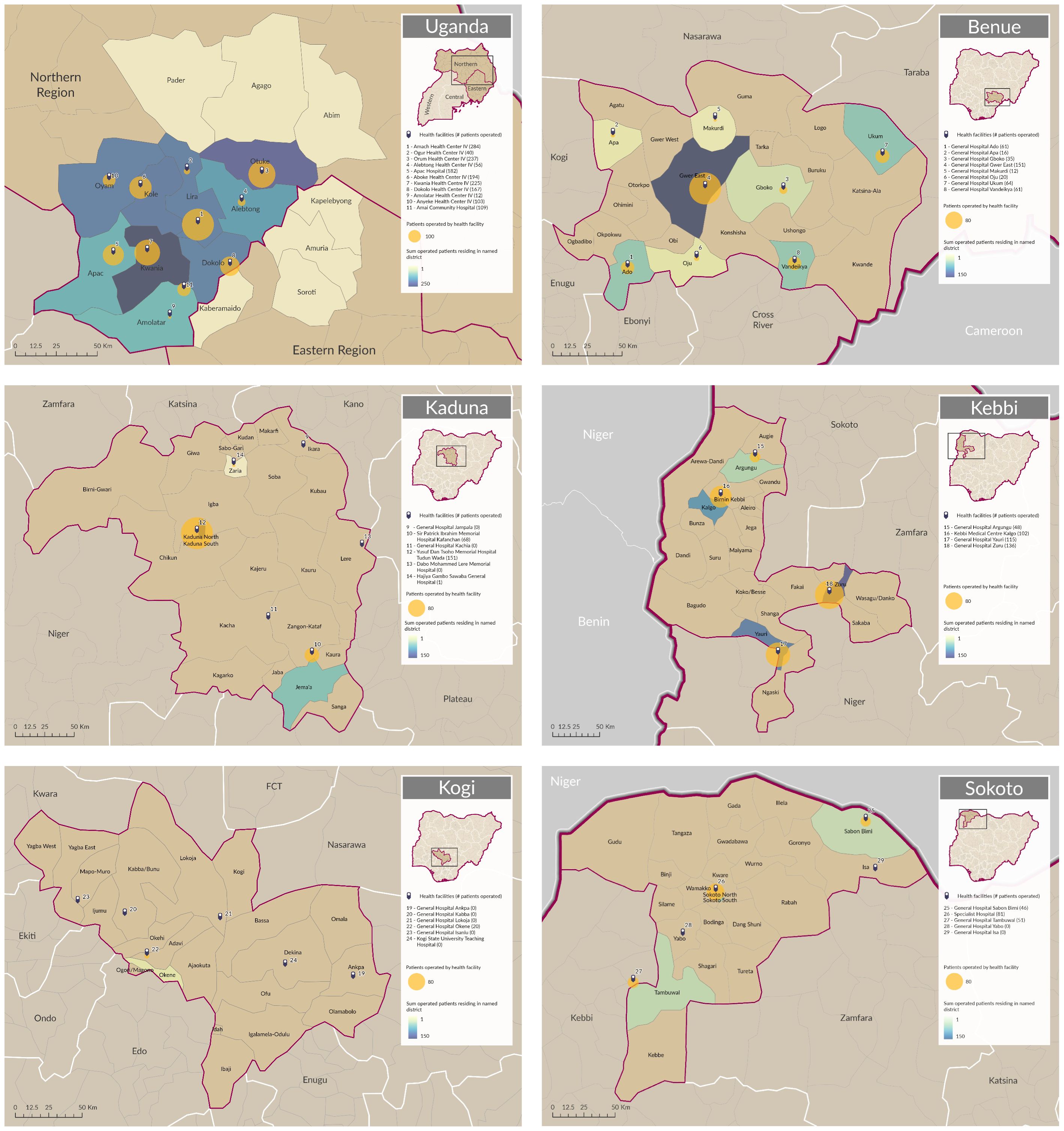
Figure 1 Maps showing sum of operated patients residing in named districts and sum of patients operated by health facility.
In all facilities, ‘readiness’ to support hydrocele surgeries was assessed prior to the start of activities. In Uganda the WHO Situational Analysis to Assess Emergency and Essential Surgical Care (EESC) tool was used (18). In Nigeria the Hydrocele Surgery Facility Assessment tool of Martindale et al. (2022) was used (19). The facility assessments confirmed readiness for implementation of hydrocele surgeries/identified quality improvement recommendations which needed to be addressed prior to the start of implementation.
Training for hydrocele surgery
In Uganda, most health facilities lacked qualified surgeons, therefore general medical officers were selected for training on hydrocele surgery. Training/re-training sessions led by a consultant urologist from Lira University, with support from both the regional and district level NTD teams, took place in the Lango sub-region, December 2020, February and April 2021, and January and July, 2022. In the case of Nigeria, government employed consultant surgeons and surgeons from the designated facilities were trained or retrained through central level trainings (for all states) in Kwara (2021) and Benue (2022). The training was led by a consultant urologist from University of Jos Teaching Hospital. Both consultant urologists were WHO certified trainers for hydrocele surgeries.
In Uganda 12 surgeons and six anaesthetists were trained, in Nigeria 24 surgeons were trained. In both countries the content of the training was guided by the WHO (2019) report, ‘Surgical approaches to the urogenital manifestations of lymphatic filariasis’, and current practices (1). In Uganda training was five days; with two days of theory and three days of practical training. In Nigeria training was conducted for three days; with one day of theory and two days of practical training. The above-mentioned consultant urologists supervised trainees during the practical sessions to ensure quality of surgeries. In Uganda, the same consultant urologist provided subsequent support supervision to the teams in the field. In Nigeria, senior surgeons identified by the Ministry of Health at state level conducted supervisory visits.
Patient mobilisation and screening
Patient mobilisation was conducted using a mixture of approaches aimed at uptake of hydrocele surgeries. In the case of Uganda, the first approach was to train Community Health Workers (CHWs) in case identification (both hydrocele and lymphoedema). Two CHWs were trained in each parish as representatives of the village health teams (VHTs). The CHWs worked in their respective communities to linelist suspected hydrocele (and lymphoedema) cases and refer them for confirmation at the nearest health centre. Confirmed cases were then informed of the hospital at which free hydrocele surgery would be available at a later date. During the period 2020- 2023, 1027 (810 male, 217 female) CHWs registered 2036 suspected hydrocele cases across the nine districts in the Lango sub-region. The ongoing activities of the CHWs, who continued to refer patients throughout the programme, were complemented by social behaviour change communication (SBCC) materials such as radio spots, community events and health talks in the outpatient departments of the health facilities providing the surgeries.
In the case of Nigeria, volunteer Community Drug Distributors and paid health workers were trained to identify suspected cases of hydrocele when they moved house to house for MDA. Identification and reporting of patients was based on genital swelling along with the diameter of hydroceles to determine an index of suspicion. Mobilisation was also supported through announcements encouraging community members with scrotal swellings to visit designated facilities for screening and confirmation. Announcements were made by religious leaders, town announcers and facility mobilisation officers at places of worship, market squares and hospitals/health facilities respectively. In addition, the Chief Medical Officers (CMOs) cascaded memos and galvanised the support of facility staff. Community members were notified of planned dates and locations for both screening and surgery. Surgeons supported the screening of suspected cases.
Surgery costs and financial support
Costs were primarily shared between the Ministry of Health and Sightsavers (the main partner). In both countries the surgery was free to the patient. In the case of Uganda, patients covered costs related to transport to the health facilities and basic provisions (e.g. food, soap, water). In Nigeria, Sightsavers paid for patient transportation to the facility. In both countries the Ministry of Health provided (existing) human resources at all levels, together with office and facility space. Sightsavers supported key consumable costs associated with the surgeries, the delivery of training, expenditure associated with advocacy and sensitisation, and mobile phones for data collection purposes.
Examination by physician and preoperative procedures
Although ultrasound is a preferred diagnostic modality (1), the availability of ultrasonography was an issue in both countries (e.g. ultrasound machines unavailable or broken). Surgical training therefore emphasised physical examination and the use of transillumination tests, even though transillumination may not be sufficient to rule in or out other scrotal pathology. When the test was determined to be non-translucent, a flowchart provided guidance as to what to do to rule out other groin pathologies. Cases of hydrocele were characterised by duration (years), type (unilateral, bilateral) and side (left, right). Additionally, in the case of Nigeria, some surgeons measured the diameter of the swelling (though most diameter measurements in the patient case file are those from the CHWs). In this paper we do not report on stage and grade (as per the standardised international clinical classification of Capuano and Capuano, 2012, referenced in WHO (2019) (1, 20)) as the Hydrocele Tracker did not record these variables at the time.
In Nigeria, patients presenting with severe comorbidities (as indicated by physical examination, patient history or laboratory test results) and with large size hydrocele (>1,000ml), were referred to level three hospital for surgery. Patients with comorbidities that had been controlled were given surgery at level 2 hospitals. Additionally, as of July 2021, guidance was given for any paediatric cases <15 years of age to be referred to a specialist in a level 3 facility. Cases referred to level 3 facilities were not captured in the Hydrocele Tracker (and are therefore out of scope of this paper). In the case of Uganda, while the referral system was set up to refer complicated cases to level 3 facilities, no patients were referred during the period this paper covers. Patients <12 years of age presenting with congenital rather than filarial hydrocele were operated in the level HCIVs facilities. However, guidance during the training was given for patients <12 years not to be included in the Hydrocele Tracker.
Preoperative blood tests were undertaken to check PCV/HCT >30% (Nigeria) or haemoglobin > 10 g/dL (Uganda) to check for anaemia. Urine analyses were undertaken to check for abnormally high levels of glucose (to check for diabetes). In both countries the programme supported herniorrhaphy if there was comorbidity with hydrocele and hernia. Additionally, patients presenting with hernia only were operated on by the programme’s trained surgeons, with the MoH covering the costs and materials for the surgery. Written patient informed consent was prerequisite for surgery to proceed.
In both countries instruction was given to avoid use of pre-operative non-steroidal anti-inflammatory drugs (NSAID) e.g., diclofenac due to the risk of internal bleeding (WHO 2019). Patients in both countries received intravenous cephalosporin, or in some cases in Nigeria quinolone, as antibiotic prophylaxis one hour before surgery.
Intraoperative procedures
Anaesthesia
In the case of Nigeria local anaesthesia (typically with lignocaine or lignocaine + adrenaline) was the preferred choice for simple uncomplicated hydrocele surgeries in level 2 facilities. Spinal and general anaesthesia was only recommended for complicated cases referred to level 3 facilities. In the case of Uganda, the training emphasised use of local anaesthesia though acknowledged possible need for spinal or general anaesthesia for hydroceles of large volume (e.g. > 500mls) or complicated cases.
Surgical technique
The programmes used well established surgical techniques, including subtotal excision of the tunica vaginalis (“excision”/”resection”) and eversion of the tunica vaginalis without excision (Jaboulay or “eversion”) (1). Training recognised that excision is the preferred technique in filarial areas (1) though in practice eversion was often used. In the case of Uganda, the majority of surgery before WHO guidance was eversion or plication (i.e. plication of the tunica vaginalis with over-sewing (Lord’s procedure)) and “excision” was for the very big hydroceles/specific cases.
Volumes of hydrocele fluids (ml) were estimated using calibrated bottles and in some cases in Nigeria, the volume of a kidney dish. Volumes were categorised as <250, between 250 and 500 or >500ml. Additionally the nature of the filarial fluid was described as either chylous, citrine, haematic or purulent. Chylous fluid refers to a milky appearance composed of lymph and fat globules, which is highly indicative of a filarial hydrocele requiring complete excision of the tunica vaginalis. Citrine fluid refers to the brownish-yellow appearance due to a type of yellow fluorescent protein; it is seen in both filarial and non-filarial hydroceles and can be managed with excision of the tunica vaginalis. Haematic fluid refers to a reddish coloration or containing blood. This can be indicative of repeated trauma to the scrotum by repeated needle tapping/scarification to let out fluid or chronic infections. It can be managed with total excision and sometimes an orchidectomy. Purulent fluid refers to that which contains pus or produces pus and is indicative of infectious micro-organisms. It can also be managed with total excision of the tunica vaginalis and cover with broad-spectrum antibiotics.
Haemostasis was achieved using suture ligation and/or electrocautery. Compressive dressings were applied on the scrotum, with scrotal elevation for five days (whether in hospital or at home after discharge). All patients continued with antibiotics for three to five days from the day of surgery.
Hospitalisation
In both counties programme guidance on duration of hospitalisation is for the patient to stay on the ward for 48 hours post-operatively. Patients are seen on day-1 to ensure their wound is clean and intact, with no immediate post-operative complication (haemorrhage, haematoma). If complications are present, they are promptly managed with antibiotic therapy and effective pain management. On day-2 post-operatively, in the absence of any complication, especially if they live close to the facility, they are discharged with instructions for wound care and when to come back to the facility. In Uganda, patients undergoing surgery for small hydrocele under local anaesthetics are discharged on the same day with antibiotic.
Reporting on complications and patient follow-up
The Hydrocele Tracker used in both countries was built to capture both immediate and late complications. In both countries late complications were reported during the planned follow-up dates at week 1, week 2 and month 1 post-surgery. In the case of Uganda there was an additional follow up point at month 6 post-surgery.
Patient feedback
A set of patient feedback tools and resources were developed to elicit patient experiences and satisfaction with the hydrocele surgery. An initial version of the beneficiary feedback tool (Supplementary Information Table 1) was first piloted in Uganda, and it included closed-ended questions centred on five broad themes: 1) the patients’ overall satisfaction with the surgery, 2) the change in ability to work, 3) the change in economic situation, 4) the change in family life, and 5) the change in community perception. The first four themes correspond to those used in Mante and Seim (2017) (21). During the pilot in Uganda, the assessment was performed six months after hydrocele surgery on all eligible patients.
The feedback tool was refined, updated (version 2), and tested in the five Nigerian states following the Uganda trial. In the new version of the tool, the initial set of questions was expanded to a mixture of eight open and closed ended (Likert scale) questions, which were then included in the Hydrocele Tracker. Following that, the revised tool was used to collect data during the 10-to-14-day post-operative follow-up phase (see Supplementary Information Table 2).
The feedback instrument was administered independently by supervisors from the Ministry of Health and Sightsavers who were not directly involved with hydrocele treatment delivery to reduce bias and subjectivity. Data was entered into the Hydrocele Tracker. The findings were used to develop a feedback response action plan to address negative feedback and adapt the programme to meet acceptable patient expectations. The responses to open-ended questions were coded into different themes for thematic analysis and reporting.
Development and rollout of the Hydrocele Tracker
The Hydrocele Tracker is a tool made up of a smartphone application and set of online dashboards. It was developed to improve patient follow-up and supervision, understand surgical outcomes and reasons for complications, and improve reporting and data quality for Ministries of Health with active LF programs. While clinical records are still kept, this tool reduces the need to collect and file paper and excel-based reports. It can make data monitoring, reporting and use more efficient. In each country, indicators on the electric forms were decided through a consultative process with the national programme.
Technical specifications
The Hydrocele Tracker uses CommCare2 as a data-collection tool and Metabase3 as a data-visualisation tool. Surgeons are granted access to patient information within their ministry-designated working area and only chosen system administrators for the country can access patient information. Data visualisation dashboards on Metabase do not include patient information. All data are owned by the Ministries of Health.
Data entry forms on the mobile phone app capture surgical registration/preoperative information, intraoperative information and follow-up evaluations. The information then feeds into online dashboards, which users can filter by location and time, including a surgery activity dashboard, an outcome assessment and follow-up completion dashboard, and a data quality assessment dashboard. (Figures 2, 3).
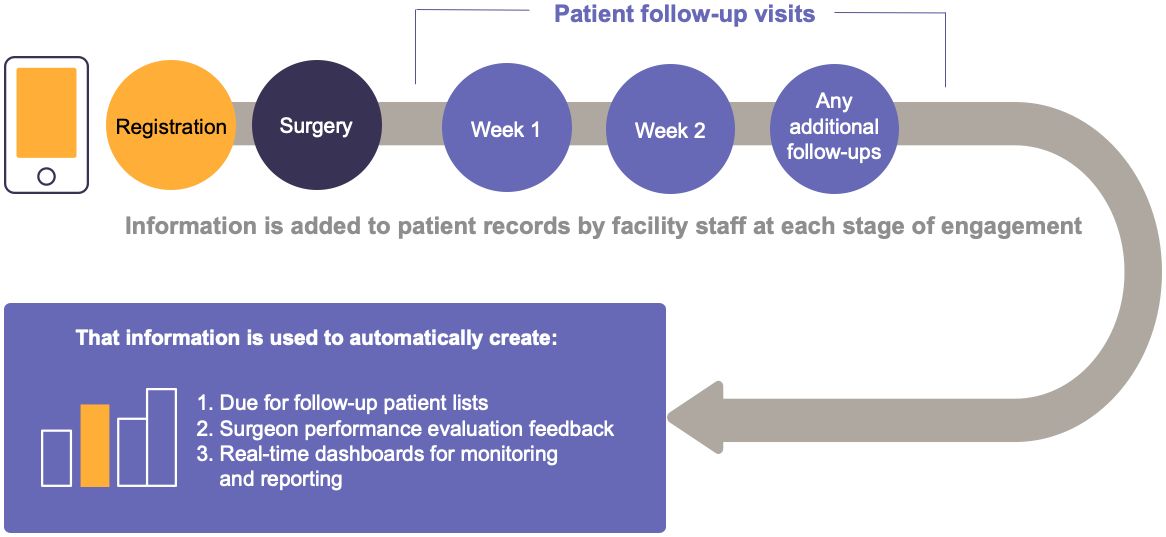
Figure 2 Data flow in the Hydrocele Tracker.
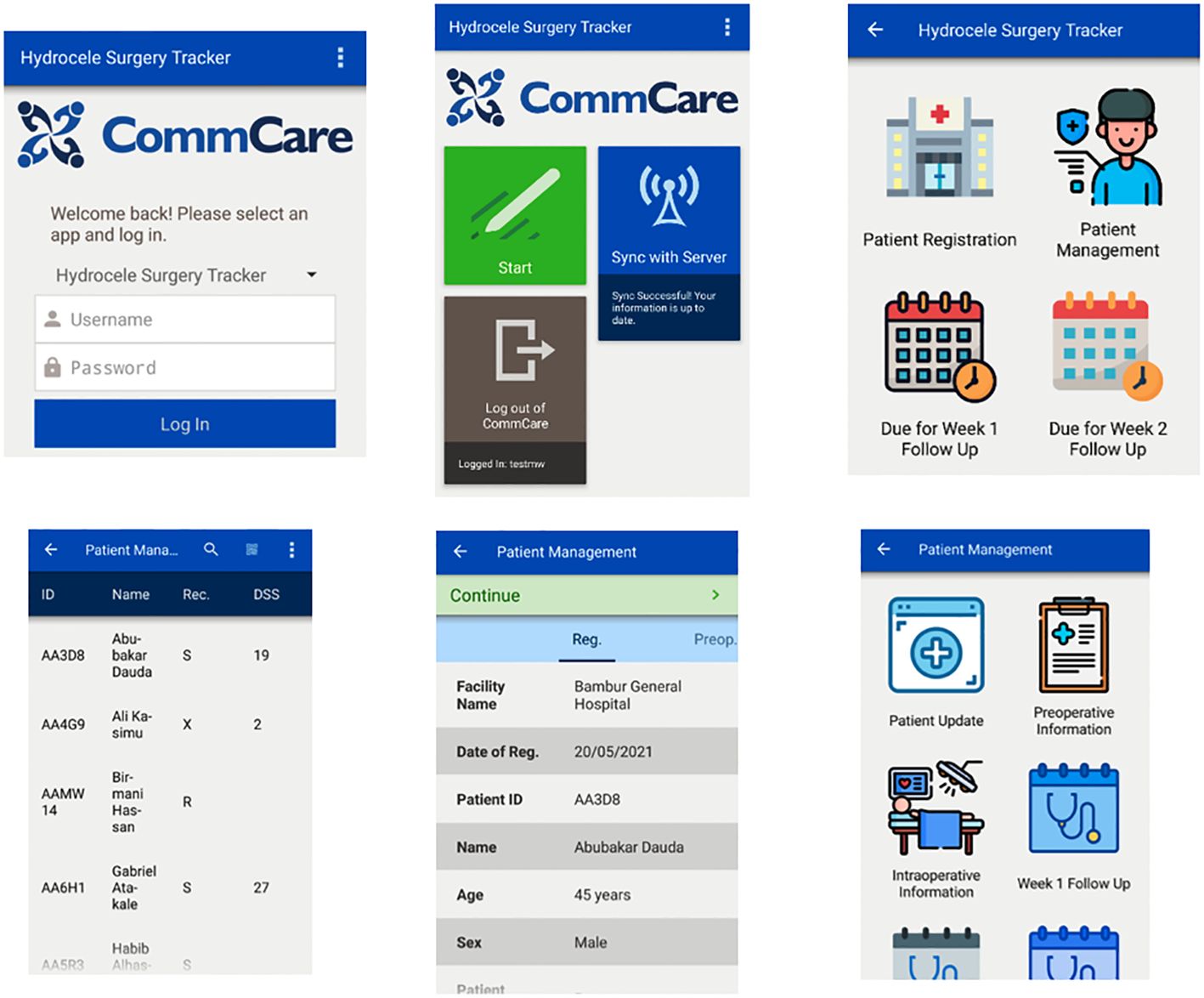
Figure 3 Hydrocele Tracker data collector’s view (note that the figure uses dummy data).
The tool also promises to help countries with active LF programmes accurately report the requested annual MMDP (hydrocele) data to the World Health Organization through the Epidemiological Data Reporting Form (22).
Hydrocele Tracker data entry and transcription from paper records
Only patients who received surgery were entered in the Hydrocele Tracker. All pre- and intra- operative patient information was entered into the Hydrocele Tracker retrospectively (from hard copies), ideally immediately after surgery, though in practice (due to work backlog) often after seven days post-surgery. Post-operative data was also entered into the Hydrocele Tracker retrospectively, ideally within 24 hours of manual entry into hospital forms. Beneficiary feedback and socio-economic data were also entered retrospectively.
Data collection and use: roles and responsibilities
In Uganda data entry was managed by surgical team members, nurses, medical officers, theatre assistants, health information assistants or the NTD focal person - depending on the facility - though entries were mainly done by someone in the surgical team. In Nigeria, MoH staff who capture data on other surgeries performed in the facilities entered the data into the Hydrocele Tracker, with support from State-level Sightsavers M&E staff. In Uganda, the Director of LF the Programme at the Ministry of Health, District Health Officers, the head of surgical teams, and certain Sightsavers programme staff had access to the dashboards; in Nigeria State M&E officers, certain State team members and certain Sightsavers programme staff had access. In both countries, the system administrators were the Hydrocele Tracker Support team from Sightsavers.
Hydrocele Tracker training
In Uganda the first training in the use of the Hydrocele Tracker was conducted in November 2021 in Lira for Otuke, Lira and Alebtong districts. Subsequently, in August 2022 training was conducted in Kole, Oyam, Apac, Amolatar, Dokolo and Kwania districts. In the case of Nigeria, the training for the five piloted states was conducted in 2021 via a hybrid training (i.e. in person and webinar) from Sightsavers’ Abuja office. The trainings were supported by the Sightsavers Hydrocele Tracker support team.
Data analysis
An anonymised download of the CommCare dataset was analysed (with simple descriptive statistics) in Excel. Duration surgery was described using median, 25th and 75th quartiles (interquartile range, IQR) after removing values which based on expert opinion and statistical inspection of the raw data were considered reporting errors; conservatively, values < 20 mins or > 180 mins were excluded from the analysis. Maps were generated in ArcGIS pro.
Results
Across the programme period a total of 1,253 and 1,658 patients were registered in the Nigeria and Uganda Hydrocele Trackers, respectively. Among these, intraoperative data (taken as affirmation of surgery) was entered for 1,239 patients in Nigeria and 1,609 patients in Uganda.
Spatial distribution of patients receiving surgery
Maps showing sum of operated patients residing in named districts and sum of patients operated by health facility are shown in Figure 1.
In the case of Uganda, 98.2% of patients operated (n=1609) were from the Lango sub-region, with the greatest number of patients reporting from Kwania district (n=239) and the least from Amolatar district (n=122). Outside the Lango sub region, 14 patients (0.9%) were from other districts within the Northern/Eastern region, two patients (0.1%) reported their district of origin as Kampala and 13 (0.8%) patients reported their district of origin as ‘other’. A comparison of surgeries supported by health facility shows the highest numbers being supported in Amach Health Center IV, Lira district (n=284) and the fewest in Amolatar Health Center IV, Amolatar district (n=12).
Patients in Uganda did not necessarily receive surgery in the designated health facility within their district of residence. For example, of the 207 patients reporting to be from Otuke, 88.4% had surgery in Orum health center (Otuke district) while 9.7% had surgery in Amach health center, (Lira district). Amach district does not border Otuke and the distance from the border of Otuke district to Amach health center is > 35km.
In Nigeria, the number of people operated varied by state. In Benue - 420 (from 8 health facilities), Kebbi - 401 (from 4 health facilities), Kaduna -220 (from 3 health facilities), Sokoto -178 (from 3 health facilities) and Kogi - 20 (from 1 health facility). Although all the facilities across the states were quality assessed, not all reported surgical data. Four health facilities in Kaduna did not report surgeries due to insecurity in the two areas where facilities are located. An additional facility conducted surgeries before the deployment of the Hydrocele Tracker and no data was reported. In Kogi, five facilities did not report surgeries due to patient unavailability while two did not report in Sokoto because of insecurity in those areas which affected staff monitoring and the upload of data to the Hydrocele Tracker. Of all the states, Kogi reported the least number of surgeries (less than 50). This might be due to the reduced number of hydrocele caseload in the state resulting from previous interventions.
Patient age distribution
The reported mean age and range of patients registered in the Hydrocele Tracker (including those without intraoperative data) was 50 years (range 1-99) and 44 years (range 3 – 96 years), in Uganda and Nigeria, respectively (Figure 4). In the case of Nigeria four patients had reported age ≥ 90 years and 32 patients < 15years. The evaluation year for 29 of the 32 patients with age < 15 year was 2021 – the year that guidance on paediatric cases was developed. In the case of Uganda 46 patients had reported age < 15 years and nine > 90 years.
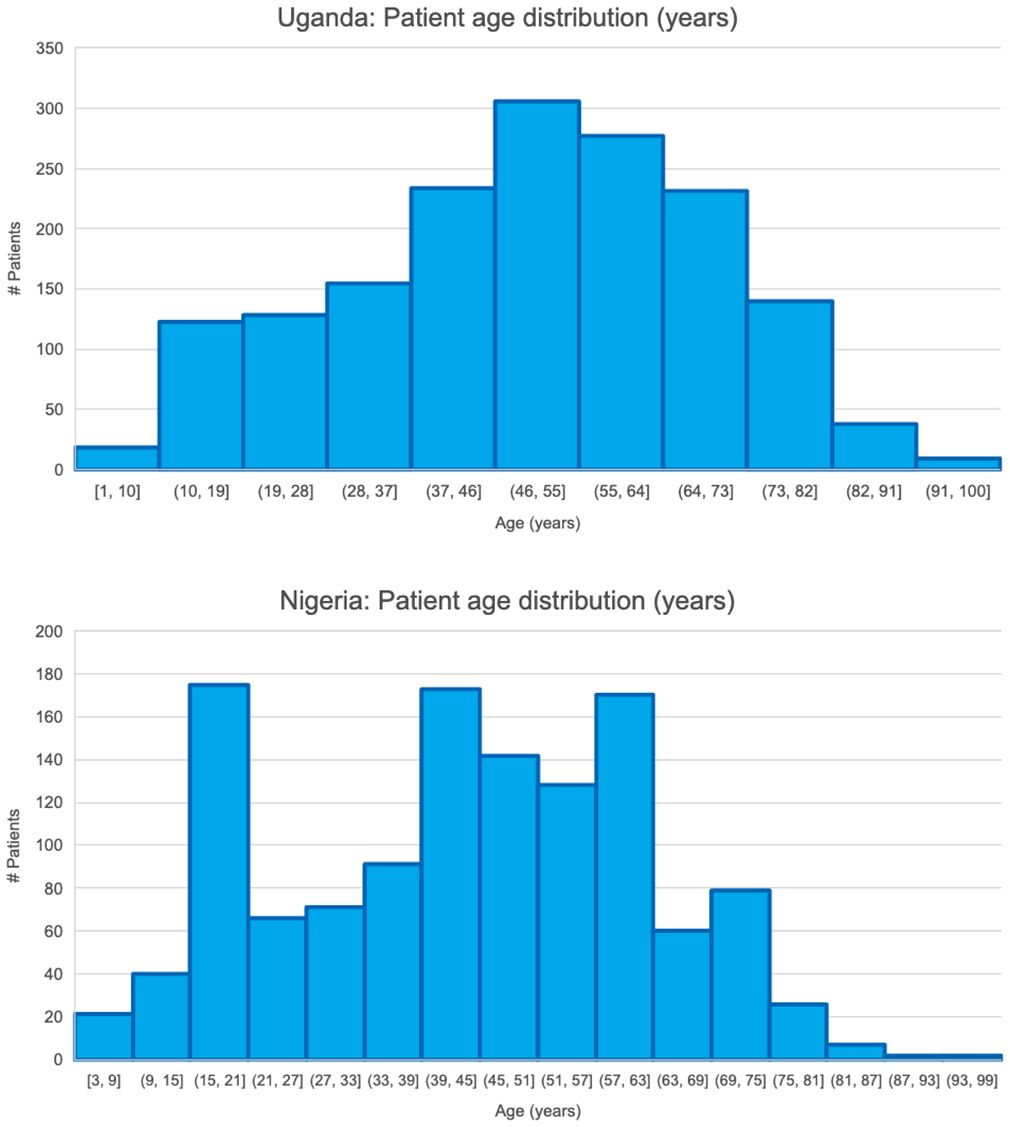
Figure 4 Patient age distributions.
Occupation of patients
In both countries the most common occupation was farming (Uganda 86.6%, Nigeria 65.3%) followed by student (Uganda 6.7%, Nigeria 16.6%).
Duration of scrotal swelling
The mean duration of scrotal swelling among patients registered in the Hydrocele Tracker (including those without intraoperative data) was 8.6 years in Uganda (range 1-60 years) and 7.7 years in Nigeria (range 1-55 years) (Figure 5). The duration of swelling was ≤ 4yrs for 42.5% and 38.1% of patients in Nigeria and Uganda respectively. By contrast, duration swelling was > 10 years for 24% patients in Uganda and 20.7% patients in Nigeria.
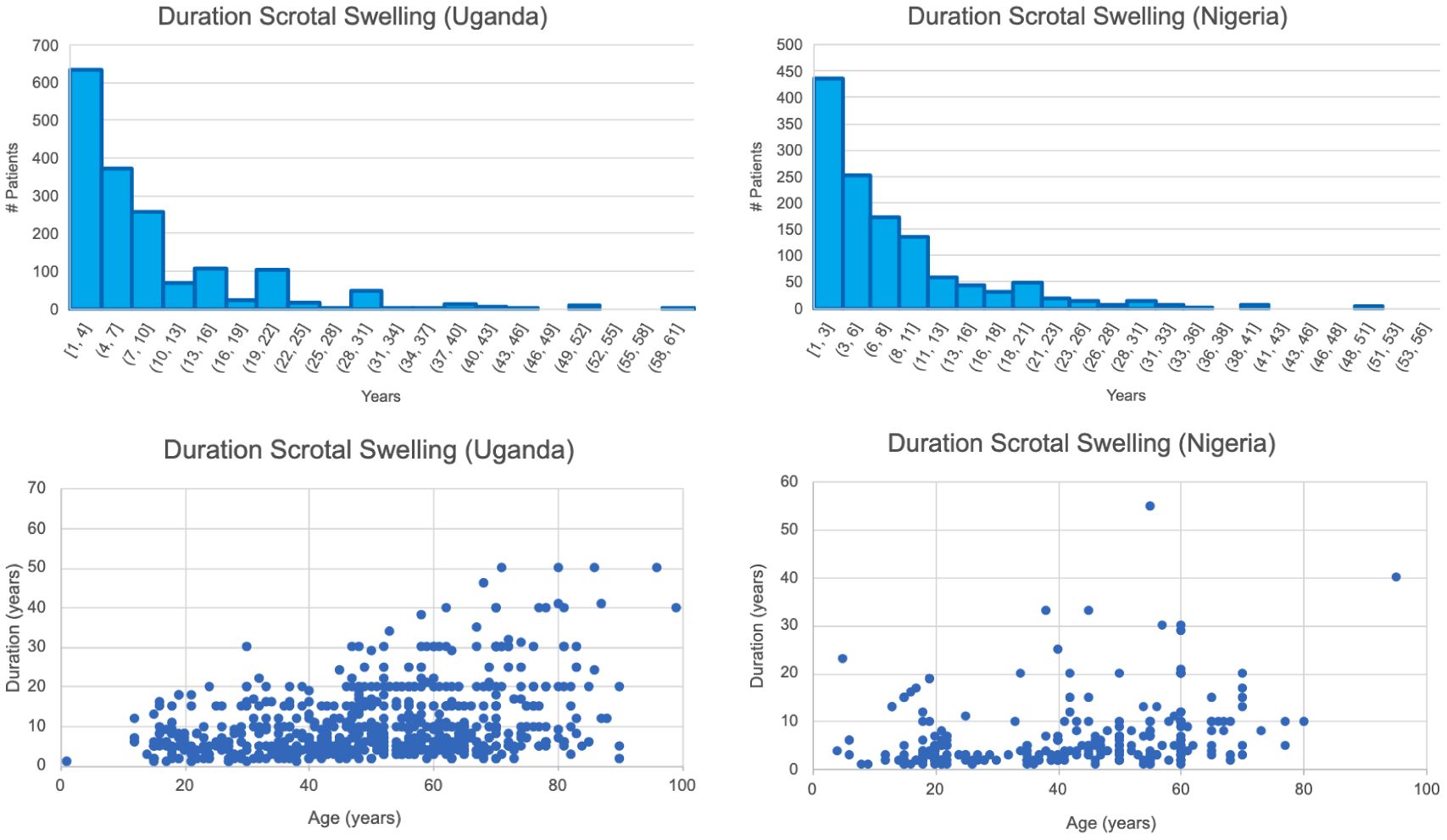
Figure 5 Frequency distributions of duration patient swelling and scatterplots of duration swelling against patient age. In the case of Nigeria note one anomalous data point where age reported as 5 years and duration swelling as 23 years.
Hydrocele diameter (field for Nigeria only)
Hydrocele diameter measurements (requested by community health workers in Nigeria to support index of suspicion) were reported for 1,253 patients. Measurements ranged from 1-70 cm, with median 5cm and IQR 4-7cm. The measurement was >10cm for 166 cases (13.2%).
Diagnostic technique (transillumination versus ultrasound)
Ultrasound was reported to be the diagnostic technique for 31.8% (n=398) and 1.7% (n=29) of patients in Nigeria (n=1,253) and Uganda (n=1,658), respectively. However, the reported use of ultrasound by facility is not consistent with the known availability of ultrasound. In the case of Uganda, of the eight facilities with reported use of ultrasound, only one (Dokolo HC) had ultrasound available (though it broke during the course of the project). In the case of Nigeria, five of the eleven facilities with reported use of ultrasound were known to have ultrasound.
Characteristics of hydrocele and other pathological conditions (pre-operative assessment)
A (pre-operative) diagnosis of bilateral hydrocele was given for 14.3% and 17.8% of the hydrocele patients registered in Uganda (n=1658) and Nigeria (n=1253), respectively. Among the registered hydrocele cases, hernia co-morbidity was reported among 15.3% and 19.9% of cases, lymphoedema of limbs among 0.1% and 0.3% of cases and associated scrotal conditions among 8.3% and 10.3% of cases, in Uganda and Nigeria respectively. Most (89.5%) of the patients categorised under the Hydrocele Tracker field for ‘other pathological conditions’ could have been categorised under the aforementioned categories for ‘hydrocele’, ‘hernia’ and ‘Associated scrotal conditions’.
Intraoperative characteristics of hydrocele: volume and nature of filarial fluid
The volume of filarial fluid was categorised as <250ml for 32.9% and 58.5% of operated patients in Uganda and Nigeria respectively (Table 1). By contrast 21.6% of patients in Uganda and 8.1% of patients in Nigeria had filarial volume >500ml.
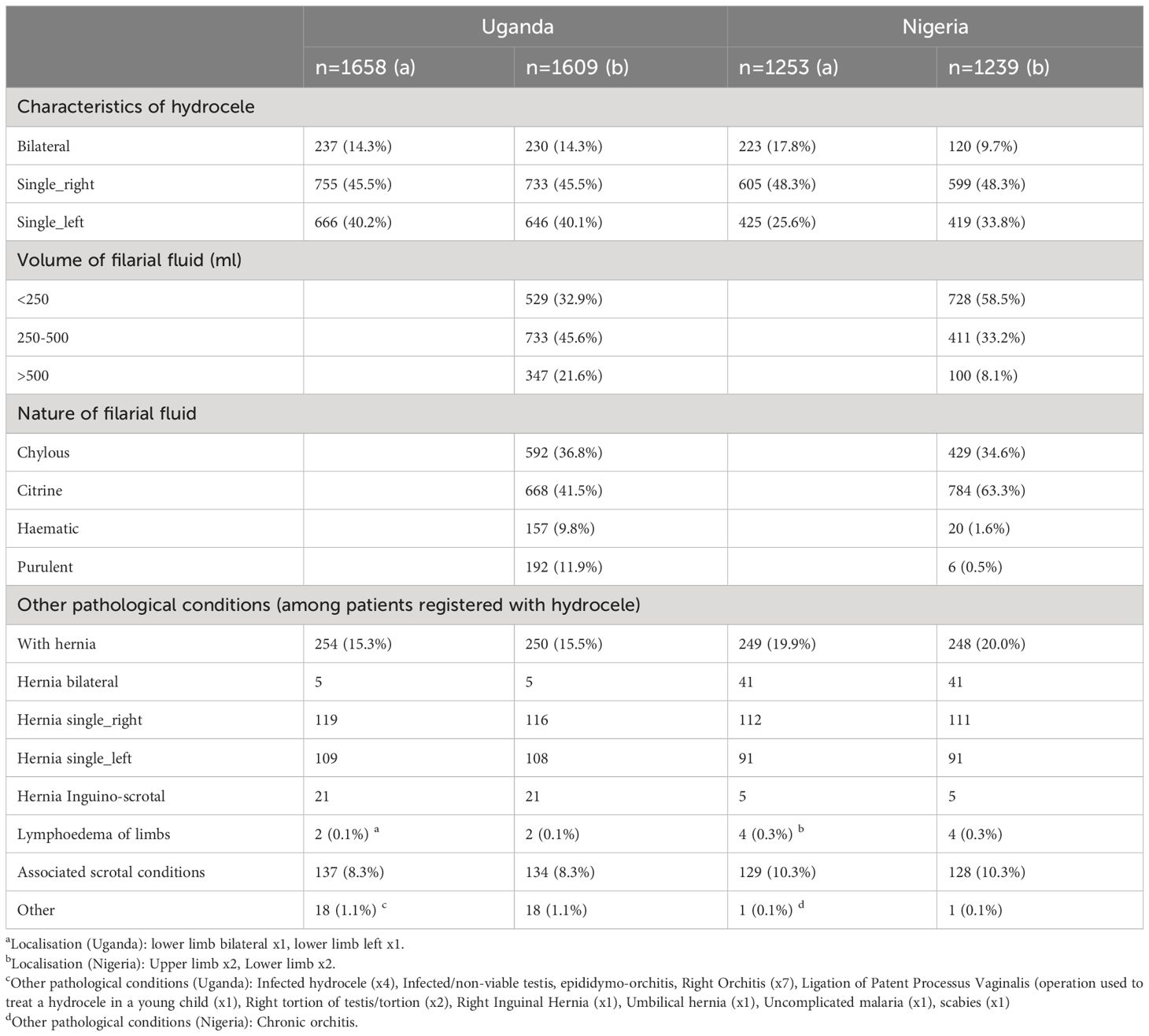
Table 1 Characteristics of hydrocele and other pathological conditions among: a) all patients registered; b) those patients with intraoperative data.
The nature of the filarial fluid was categorised (in descending order) as citrine (41.5% Uganda, 63.6% Nigeria), chylous (36.8% Uganda, 34.6% Nigeria), purulent (11.9% Uganda, 0.5% Nigeria) and haematic (9.8% Uganda, 1.6% Nigeria) (Table 1). The high percentage of citrine/chylous (Uganda - 78.3%, Nigeria - 98.0%) fluid appearances is consistent with hydrocele of filarial origin. Chylous is the classic presentation of hydrocele of filarial origin. Citrine can present with filarial and non-filarial hydroceles.
Surgical procedure
A total of 1,609 and 1,239 patients were operated in Uganda and Nigeria respectively. The most reported surgical procedure was ‘eversion’ in Nigeria (57.0%) and ‘hydrocelectomy’ in Uganda (58.2%) (Table 2). An accurate comparison of the extent of eversion versus excision/resection is not possible as, a) in the case of Nigeria, the field ‘other’ was used to register 160 occurrences of ‘hydrocelectomy’, b) in the case of Uganda, 936 patients were categorised against ‘hydrocelectomy’. Hernia repair was reported for 462 (28.7%) and 230 (18.6%) patients in Uganda and Nigeria respectively – contrasting with preoperative diagnosis of 254 and 249 patients with hernia in Uganda and Nigeria respectively. Surgical procedure was reported as orchidectomy for <1% persons operated in both countries.
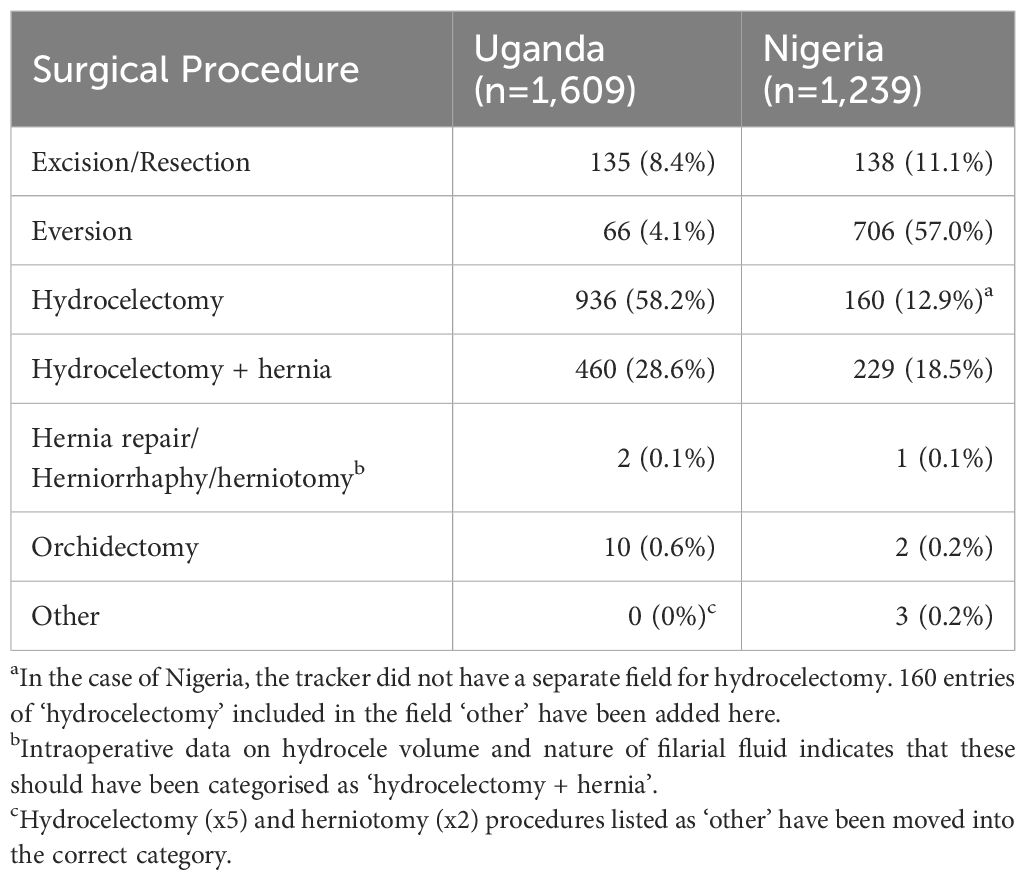
Table 2 Type of surgical procedure by country.
Pre-operative lab data
In the case of Nigeria, the completeness of tracker fields for pre-operative laboratory data was 100% (n=1,253) for Haematocrit (HCT), urine sugar and HIV (reflecting the fact that these fields were mandatory) and 26.1% for blood group. For HCT, biological implausibility was flagged for 2.6% data entries (i.e. value <10% threshold used by Hinzmann et al. (23)); beyond these entries, 22 (operated) patients had HCT values in the range 17-29% (i.e. outside >30% threshold for surgery) – this is indicative of laboratory/transcribing errors or physical examination by the surgeon which deemed the patient otherwise fit for surgery. Urine sugar was positive for 16 (operated) patients – indicative that further investigations would have been required to rule out Diabetes mellitus. Eight operated patients were positive for HIV.
In the case of Uganda (n=1658), the completeness of Hydrocele Tracker fields for pre-operative laboratory data was 55.2% for Hb, 25.9% for urine sugar, 39.3% for urine pus cells and 81.0% for blood group. The lower level of completeness corresponds to the fact that the fields were only mandatory during the initial phase of the Hydrocele Tracker rollout. Among Hb records, two very low records were considered biologically implausible [i.e. outside range of 4 g/dL to 20 g/dL referenced in Pullman et al. (24)]; beyond these, 13 entries fell below the recommended threshold of 10g/dL. All urine sugar results were recorded as normal. 14.7% of urine pus cells results (n=652) were positive. An oversight in the Hydrocele Tracker form there meant that either a urine sugar result or a urine pus cells result was recorded for a single patient (i.e. never both results). Blood group was recorded for 80.1% of patients.
Anaesthesia
In both countries the majority of operations were conducted under local anaesthesia (Uganda – 64.9%, Nigeria – 85.0%) (Table 3). Spinal anaesthesia was reported from 0.1% and 32.3% of operations in Nigeria and Uganda, respectively. General anaesthesia was reported from 11.7% and 2.6% of operations in Nigeria and Uganda, respectively.
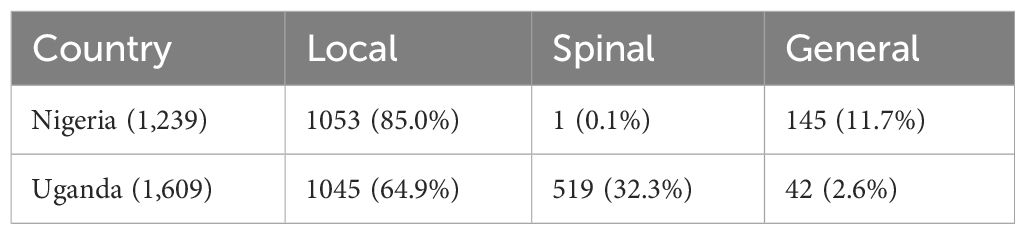
Table 3 Use of local, spinal and general anaesthesia in Nigeria and Uganda.
In the case of Uganda, the type of local/spinal anaesthesia was mainly recorded as lignocaine (63.3%) or lignocaine + bupivacaine (25.8%) and the type of general anaesthesia mainly reported as ketamine (97.6%) (Table 3). In the case of Nigeria, the type of local anaesthesia was mainly lignocaine (72.4%) or lignocaine + adrenaline (13.8%), the type of spinal anaesthesia was ketamine (but just one patient) and the type of general anaesthesia, mainly ketamine (96.6%). The reports of ketamine use for spinal anaesthesia (in both countries) is considered a reporting error as ketamine is not used for spinal anaesthesia.
Complications
Immediate complications (haemorrhage/haematoma/infection) were reported for 20 (1.2%) patients in Uganda and eight (0.6%) patients in Nigeria (Table 4). For two patients the date of the immediate complication (six and eight days post surgery) was recorded to be outside the ‘standard’ 0-5 day post surgery window for immediate complications.
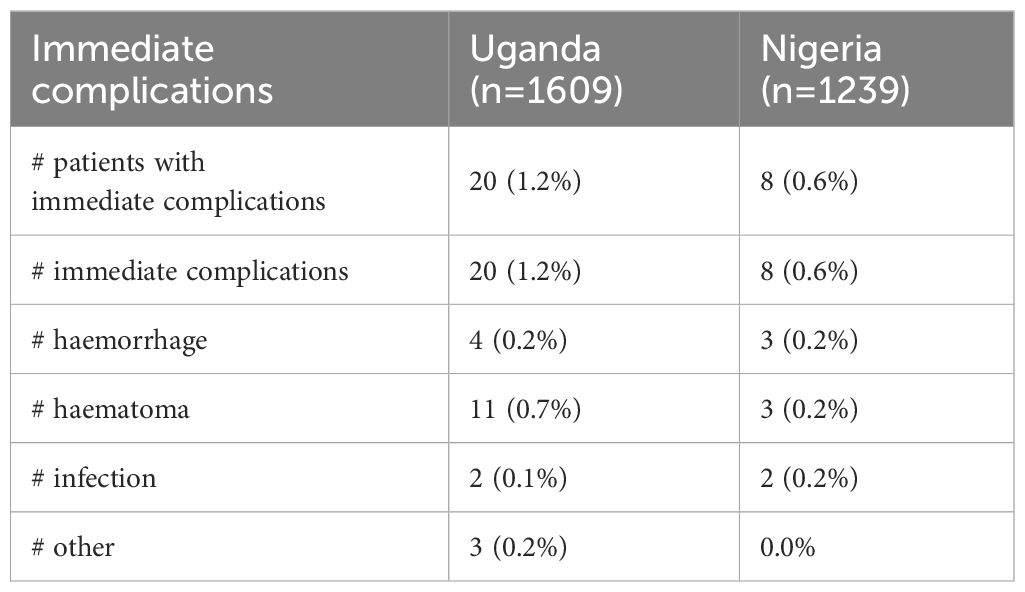
Table 4 Occurrence of immediate complication.
In Uganda late complications were reported among 16 (2.2%), five (1.0%) and three (0.7%) patients at week 1, week 2 and month 1 follow ups respectively (Table 5). In Nigeria late complications were reported among three patients (0.3%) at the ‘week 1’ follow up, six patients (0.6%) at the ‘week 2’ follow up and 0 patients at the month 1 follow up. Reported complications concerned haematoma, infection and wound breakdown (both countries), haemorrhage (Nigeria), necrotic tissue, lymphoedema of scrotum and epididiymo-orchitis (Uganda). The reports of recurrence in both Uganda (3 patients) and Nigeria (2 patients) are considered inaccurate as they occurred at or before the month 1 follow up (see discussion). A patient in Uganda marked for reoperation due to recurrence (at month 1) was retrospectively linked to haematoma formation (rather than recurrence). Late complications were reported for none of the 58 Ugandan patients with month 6 follow up. There was no month 6 follow up in Nigeria.
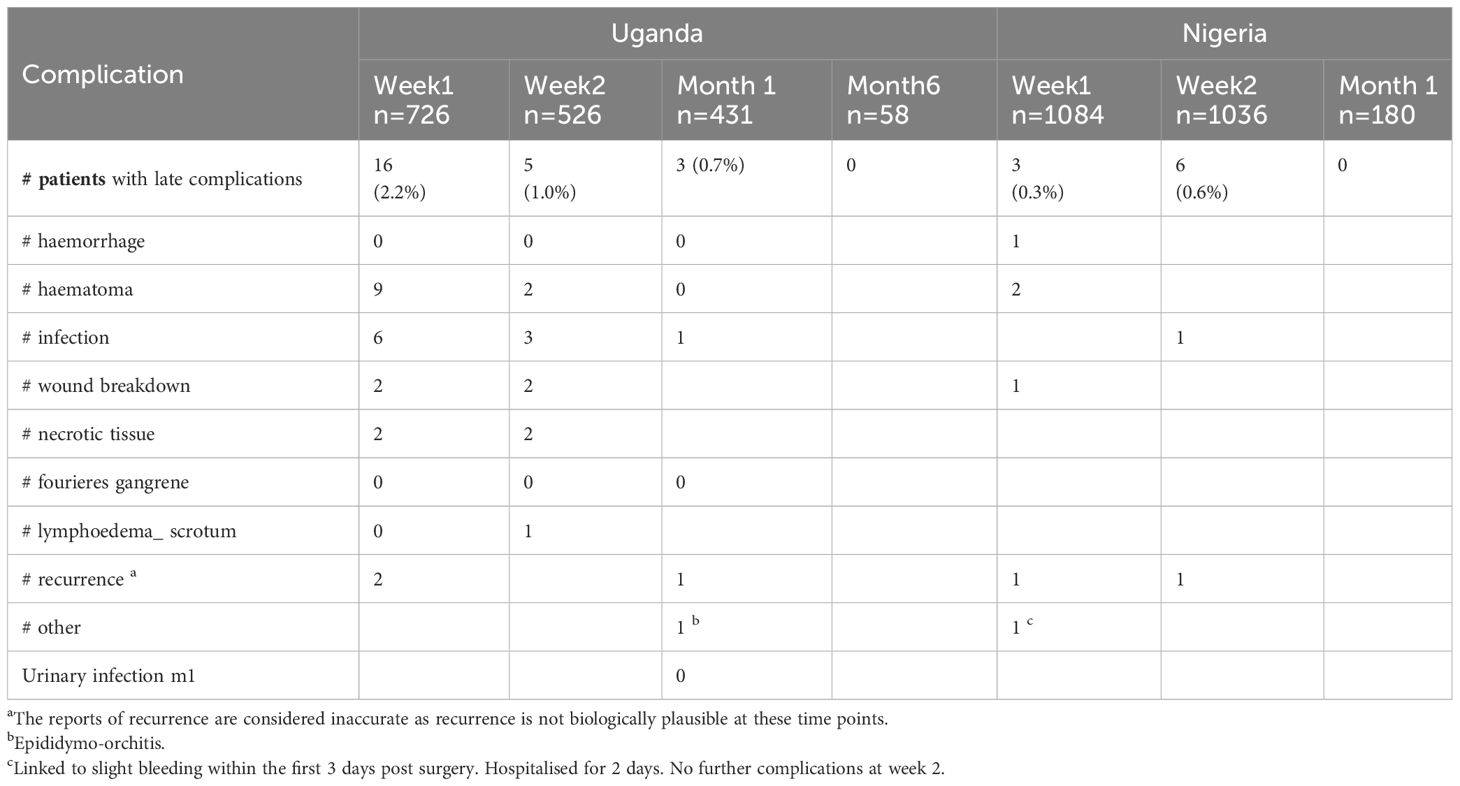
Table 5 Occurrence of late complications.
As examples of individual patient follow-up histories, in the case of Uganda all patients with haemorrhage reported as an immediate complication had a week 1 follow up; one of these patients continued to have complications at week 2 follow up (infection – ‘severe wound dehiscence with pus and necrosis’, necrotic tissue and wound breakdown – ‘dead tissue’) and was hospitalised for a total of 22 days. In the case of Nigeria, one 80-year-old patient with immediate complication reported as haemorrhage and haematoma continued to have late complications; these complications were linked to a fall within 24 hours of surgery.
The Hydrocele Tracker has no systematic capture of steps taken to manage complications though some information was recorded in the fields for ‘surgery notes’ and ‘notes associated with each follow up’. For example in Uganda two patients with necrotic tissue at week 2 had orchidectomy; notably the surgical procedure for these two patients was recorded as hydrocelectomy only.
Among the patients for which intraoperative data was recorded, complications (at any time point) were reported from 40 (2.5%) and 15 (1.2%) patients in Uganda (n=1609) and Nigeria (n=1239) respectively.
Patient follow up
In the case of Nigeria (among the patients with intraoperative data, n=1,239) follow up rates were 1084 (87.5%), 1036 (83.6%) and 180 (14.5%) at week 1, week 2 and month 1, respectively. All month 1 follow ups were from Kaduna and Kebbi states only. In the case of Uganda (among the patients with intraoperative data, n=1,609), follow up rates were 711 (44.2%), 515 (32.0%), 422 (26.2%) and 58 (3.6%) at week 1, week 2, month 1 and month 6 respectively.
Duration hospitalisation
In the case of Nigeria, among 1,182 patients with hospitalisation start and end dates or hospitalisation status recorded as ‘no’, (indicating that the patient was omitted only for day surgery, not that the patient wasn’t hospitalised) duration hospitalised was calculated as follows: 0 days (571 patients, 48.3%), 1-2 days (300 patients, 25.4%), 2-3 days (262 patients, 22.2%), 4-5 days (2 patients, 0.2%), 6-7 days (16 patients, 1.4%) and 8+ days (31 patients, 2.6%). In the case of Uganda, among 628 patients with hospitalisation start and end dates or hospitalisation status recorded as ‘no’, duration hospitalised was calculated as follows: 0 days (114 patients, 18.2%), 1-2 days (95 patients,15.1%), 2-3 days (208 patients, 33.3%), 4-5 days (143 patients, 22.8%), 6-7 days (49 patients, 7.8%) and 8+ days (19 patients, 3.0%). In both datasets there were some traceable data quality issues – notably among patient records with duration > 8 days.
Duration surgery
Among patients with intraoperative data, duration surgery was 20-180 mins (inclusive) for 1116 (90%) and 1577 (98%) records in Nigeria and Uganda, respectively. Median duration surgery (regardless of surgery type and whether hydrocele bilateral or unilateral) was 30 mins in Nigeria (IQR: 30-45 mins) and 50 mins in Uganda (IQR: 35-120 mins). In both countries the median, Q1 and Q3 values were higher for excision than eversion (Uganda excision: median=60, IQR: 50-61 mins (n=134); Uganda eversion: median=45, IQR: 25-60 mins (n=61); Nigeria excision: median=42, IQR: 32-51 mins (n=129); Nigeria eversion: median=30, IQR: 26-35 mins (n=610)).
Beneficiary feedback
In Uganda, 58 patients (3.6%) out of 1,609 with intra-operative data took part in the beneficiary feedback assessment at month six post surgery. Results showed that the majority of the patients expressed satisfaction with the service received across all the domains. For the general satisfaction domain, 57 persons (98.2%) reported they were happy they had the surgery and had no problems afterwards, while only one individual (1.8%) reported experiencing some problems after the operation, although was glad to have had the surgery. In the change in ability to work domain, 53 people (91.4%) reported significantly improved ability to work following surgery compared to pre-surgery, and five individuals (8.6%) reported somewhat improved ability. In the change in economic situation domain, 52 people (89.6%) reported significantly better improvement in their economic situation after surgery, compared to one person (1.7%) who reported little improvement. When asked how their family life has changed since the surgery, 57 participants (98.2%) said it had become much better, while one participant (1.7%) said it had not improved that much. In response to the question around change in community perception, 51 patients (87.9%) reported that members of their community were much more accepting of hydrocele and aware that surgery is a treatment option, compared to only 7 patients (12.0%) who said that members of their community were somewhat accepting of hydrocele and aware of surgery as a treatment option.
In Nigeria, 887 patients (71.6%) out of the 1239 patients who underwent the hydrocele surgery participated in the feedback assessment during the 10 to 14 day post operative follow up. According to the Likert scale results, the majority of patients expressed high levels of satisfaction with the quality of care they received (99%), the hospital’s atmosphere (96%), and the attitude of the medical staff performing the hydrocele surgeries (98%). The emerging themes from the open-ended questions included a general expression of satisfaction with the quality of service and success of the surgeries; the duration of surgery (which were perceived as safe, fast, and simple); the attitude of health workers (noted as being friendly, nice, and kind to patients); and the provision of additional support (in the form of feeding, medication and transport money) to facilitate patients’ participation in the surgical procedure. Themes around patients’ dissatisfaction with the services included the hospital environment (particularly the absence of mosquito bednets), the attitude of the staff and nurses, the experience of pain following surgery, the lengthy turnaround times for procedures (particularly for laboratory test results), and the timing of the surgical procedure (which was performed during the farming season). Participants offered suggestions to improve the provision of hydrocele surgery services, such as raising awareness and mobilising additional affected persons to take part in the surgeries and expanding the number of surgical centres to increase proximity for patients. Participants also recommended that the outreach programme include the provision of hernia surgeries and be scheduled during the dry season.
Discussion
National LF elimination programs benefit from timely access to pre, intra and post operative clinical data in order to evaluate factors that influence surgical outcomes, patient experience and uptake of services in endemic areas. The ability to provide quality assurance becomes increasingly important as national countries scale up support for hydrocele surgeries, monitor the number of reference hospitals providing hydrocelectomies (including the availability and quality of an essential package of care) and strengthen the capacity of referral hospitals to manage incident cases of disease after LF elimination requirements are validated by the WHO.
Our retrospective analysis of programmatic data collected from hydrocele patients registered in the Nigeria and Uganda Hydrocele Tracker respectively demonstrates how national LF elimination programmes can, 1. use available data to evaluate the current package of care offered to hydrocele patients and 2. use patient level data to drive programmatic changes in services. The piloting of the digital-based Hydrocele Tracker has provided insight to current patient follow-up rates and the outcomes of those follow-ups in improving supervision, surgical planning and execution, and overall improvements to facility-based surgical care needed in LF endemic countries.
Patient numbers
The numbers of hydrocele surgeries with intraoperative data reported in this paper are significant: Nigeria -1239 (March 2021 - September 2022); Uganda -1609 (October 2021-July 2023). In the case of Uganda, prior to the implementation of the surgeries reported in this paper, a total of 1,448 hydrocele surgeries had been recorded by the national programme. Notably, there is indication that patients do not necessarily opt to receive surgery in the health facility in their district of residence; this is important for future implementation planning.
Characteristics of hydrocele
The Hydrocele Tracker pre-operative classification included “side” and “unilateral/bilateral” though did not include stage and grade, the standardised international clinical classification of Capuano and Capuano, 2012 (1, 20). Standardised disease severity grading is important as it helps with development of standard operating procedures/management algorithms and helps monitoring of post operative outcomes, so this should be reviewed.
In both countries the nature of the filarial fluid was mainly consistent with hydrocele of filarial origin (i.e. 98% and 78% in Nigeria and Uganda respectively chylous or citrine). There was a higher percentage of purulent/haematic in Uganda (9.8% haematic, 11.9% purulent) than Nigeria (1.6% haematic 0.5% purulent). Possible explanations for the higher levels in Uganda include a higher endemicity burden, longer duration swelling (the hydrocele is less likely to become purulent if the patient presents early on), hydrocele of non-filarial origin, or higher usage of community level interventions before reaching the facilities e.g. aspiration with needles. In our experience, the latter explanation is thought unlikely as aspiration (a practice that can lead to infection/haematic presentation) is not commonly known in the study area. Additionally in the case of Nigeria, it is possible that some patients with purulent/haematic hydroceles diagnosed through ultrasound might have been referred to a higher level facility, which would have been outside the scope of the Hydrocele Tracker.
A pre-operative diagnosis of hernia co-morbidity was common in both countries (Uganda - 250 cases or 15.5%, Nigeria – 248 cases or 20%), though operative data from Uganda (462 cases or 29%) was indicative of under-diagnosis or under-reporting. Under-reporting may have happened where the hernia and hydrocele presented on the same side and a single operation was planned. Under-diagnosis and the discovery of hernia cases on the operating table may be linked to the use of transillumination rather than ultrasound diagnosis.
Among the registered hydrocele cases, lymphoedema of limbs was reported among 0.1% and 0.3% of cases, in Uganda and Nigeria respectively. These figures contrast with those of Kebede et al. (25) where 34% hydrocele cases also had leg lymphoedema (Ethiopia); and Mwingira et al. (26) where 10% hydrocele cases also had leg lymphoedema (Tanzania). The low levels of co-morbidity in Uganda and Nigeria did not come as a surprise to either programme. In the case of Uganda, Lango sub-region, very few patients have been known to present with both hydrocele and lymphoedema of the limbs during activity implementation. In the case of Nigeria, case searches (supported by Sightsavers) in Kebbi, Kwara, Kogi and Sokoto in 2017 showed that only four persons out of 707 had co-morbidity (i.e. 0.01% co-morbidity) (unpublished data). Nevertheless, due to the fact that the focus of the Hydrocele Tracker is hydrocele it is prudent not to rule out underreporting of limb lymphedema in the Hydrocele Tracker.
With regard to diagnostic modality the results highlight low usage and over-reporting of ultrasound (particularly in Uganda). As described in WHO (2019) ultrasound (as opposed to transillumination which is non-specific) and a good physical examination is the preferred diagnostic modality as it may rule in or out other scrotal pathologies, confirm Stage I-II hydroceles and identify hernias (1). Improved diagnoses promise patients better peri-operative counselling (e.g. from the Uganda programme where non-functioning testis was discovered on operated table) and is important for peri-operative preparations and management pathways more generally. Both countries plan to improve the availability and usage of ultrasound in future programming; the aspect of overreporting needs to be addressed through related training of data reporters.
Surgical management and diagnostic algorithms
In both countries the recommendation for surgery followed similar pre-operative lab and clinical findings though referral practices/pathways differed e.g. in the case of Uganda formal referral of more complicated cases or patients < 15 years of age to WHO level 3 facilities was not done. With regard to pre-operative laboratory tests, data in the Hydrocele Tracker shows issues of completeness (particularly in Uganda where unlike Nigeria, entry of laboratory data was only mandatory for the initial phase of the programme) and accuracy (in both countries).
In the operating room, anaesthesia type was mainly recorded as “local” in both countries (85% Nigeria, 65% Uganda), though also notable differences with Uganda reporting 32% “spinal” and Nigeria reporting 12% “general”. In the case of Nigeria, the entries for “general” came as a surprise and there is some suspicion that these are data entry errors linked to the fact that Hydrocele Tracker entries were done by non-medical personnel. In the case of Uganda, the higher use of spinal may be linked to: 1) complicated cases (which were in the case of Uganda in scope for the Hydrocele Tracker), 2) surgeon/anaesthetist/patient preference (e.g. in view of anxiety), 3) data entry issues (considered minimal). While local anaesthesia was advocated for during training (because of the advantages it carries), there was no clinical guideline for this. The data in the Hydrocele Tracker has highlighted the need to standardise guidance around the use of anaesthesia and address unforeseen findings e.g. relatively high use of spinal anaesthesia for hydroceles of small volumes. The Uganda programme will be consulting with surgeons to better understand choice and reiterate advantages and disadvantages. e.g. relating to risk, cost, duration surgery.
An accurate comparison of the extent of eversion versus excision/resection (the WHO (2019) preferred technique) was not possible due to usage of the generic term ‘hydrocelectomy’. Nevertheless, data in the Hydrocele Tracker was consistent with eversion being the more commonly practised technique, e.g. in Nigeria 57% patients had surgical procedure reported as ‘eversion’. This finding highlights the need for: 1) renewed emphasis on scientific rationale for preference for resection/excision during training of surgeons, 2) a Hydrocele Tracker field titled hydrocelectomy procedure (as opposed to surgical procedure), 3) training of surgeons to specify type of hydrocelectomy procedure in patient file, 4) training of data entry persons. The scientific rationale for the preference for excision of the tunica vaginalis for all stages of hydroceles links to the fact that the primary cause of hydroceles is damage of the lymphatics of the tunica vaginalis. “Leaving the tunica in place can invite recurrence, as has been documented in one observational study” (1, 27).
The time points for follow up reported in this paper are, for the most part, not sufficient for any assessment of recurrence i.e. no follow up after month 1 in Nigeria and only 56 patients followed up after month 1 in Uganda (at month 6). The inadequacy of recurrence reporting and poor follow up is a widely recognised challenge (9). While there is no international agreement on the timeline for recurrence/definition of recurrence onset (27), granted a minimum of eight weeks for healing post surgery (28) - any reports of recurrence before this time may be considered erroneous.
In the case of Uganda, a validation exercise supported by Sightsavers in August 2023 in the Lango sub-region reported recurrence of 22.5% (n=40), approximately one year since patients had been operated (unpublished data). The validation report indicated that almost all patients had surgery by the eversion technique and even the few who had excision of the tunica had very minimal excision with eventual eversion. Additionally, there were a significant number of new hydroceles in the same patients. These findings, notwithstanding possible overdiagnosis (linked with absence of ultrasound) and small size, identified the need to put more emphasis in training on the resection/excision technique and rationale thereof.
Duration of surgery
Records on duration of surgery (as described by medians, 25th and 75th percentiles) are illustrative of hydrocelectomy being a relatively simple procedure and consistent with knowledge that excision is a lengthier procedure than eversion (7, 8). Granted expert opinion and published data on average operating time for excision of unilateral hydrocele of 45 min to 1 hr and for bilateral hydrocele of 1½ hr to 2hr, the median and IQR range for the excision durations from Nigeria (median=42, IQR: 32-51 mins (n=129)) are shorter than expected. This may be linked to surgeon practice or accuracy in data reporting.
Duration of hospitalisation
In both countries guidance on duration of hospitalisation is for the patients to stay in the hospital for 48 hours postoperatively; however, in the case of Uganda patients undergoing surgery for small hydrocele under local anaesthetics may be discharged on the same day with antibiotic. The guidance around staying in the hospital for 48 hours postoperatively is consistent with WHO (2019) guidance that “Patients should be observed in hospital for at least 2 days after surgery and until the first dressing change, especially if they live at a great distance from the hospital and do not have running water, soap or toileting facilities or vehicular transportation” (1).
In the Hydrocele Tracker datasets the percentage of patients reported as ‘not hospitalised’ (indicating ‘day surgery’ as opposed to strictly ‘not hospitalised’) was 18.2% in Uganda and 48.3% in Nigeria. In the case of Uganda, the percentage is as expected because during support supervision a number of surgeons reported performing hydrocelectomy as day care surgery, especially for people who live near the hospital. By contrast in the case of Nigeria the percentage of ‘day surgery’ was far higher than suspected, raising concern over the accuracy of the data reported and leading to suspicion that some enumerators were using the category ‘hospitalised’ for anything that wasn’t routine. In Uganda, the relatively high percentage of patients (10.8%) reported as hospitalised for more than 5 days points to the need for possible further investigation to understand context/rationale for decisions taken and verify accuracy of reporting. Possible explanations for a long duration hospitalised include results from pre-operative evaluation, complications after surgery, poor personal hygiene, long distance from home and specific request from patients. Thomas et al. (8), reporting on a programme of mass surgery in Nigeria describe how most patients were discharged on post operative day 1 or 2 though patients with very large hydroceles and/or living in a remote village with difficult transportation being hospitalised for 5-7 days. A similar situation may be apparent in the Lango region.
Post-operative follow-up
The data in the Hydrocele Tracker demonstrates both successes and known challenges with follow up (9). In the case of Nigeria follow up was >80% at both week 1 (1- 9 days post-surgery) and week 2 (10-14 days post-surgery) time points though fell to 15.5% at month 1. In the case of Uganda follow up was 44.2%, 32.0% and 26.3% at week 1, week 2 and month 1 follow up times, respectively. At month 6 it fell to 3.6%. In the case of Nigeria, the high week 1 and week 2 follow up rates may be linked to the incentives (e.g. transportation and feeding) provided by the programme to the patients. By contrast the low month 1 follow up rates in Nigeria may be linked to the fact that programmatically scheduled follow ups end after week 2 unless there is the need or complication. In the case of Uganda some possible explanations for the low follow up rates include: 1) distance from which patients were coming from e.g. 30km away, 2) referral of patients to nearby health centres for removal of stitches, 3) patients not appreciating the rationale for the follow-up review due for example to no evidence of/concern over complications and use of absorbable stitches, 4) ‘informal’ follow up not captured in the Hydrocele Tracker e.g. follow up through phone calls and work of VHTs to track down patients who did not come in for follow-up. Approaches to improve follow up reported elsewhere include the use of SMS to automate follow up reminders (29) and linking of financial remuneration to data collection (6). Using SMS to automate follow-up reminders is possible through the Hydrocele Tracker software, though was not set up for this pilot as many patients don’t have cell phones. SMS messages can however be sent to community health volunteers or family members on behalf of the patient, and this may be considered in the future in both countries.
Complications
In both countries the rates of complications (at any time point) were low (Nigeria 1.2%, n=1,239, Uganda 2.5%, n=1,609), and compare favourably to those previously reported - e.g. Mante and Gueye (7) reported 5-7% among patients admitted for at least 5 days post surgery (n=3000), Beyene et al. (6) reported no complications in the three days following surgery, when patients were still in the hospital though 12% between day 3 (the day of discharge) and day 14 (n=175), Thomas et al. (8) reported 3-4% complications between day 1 and 7 (n=301). However, caution is erred over possible underreporting of complications which may (for example) be linked to low hospitalisation rates and sub-optimum follow-up rates. Looking forward consideration needs to be given to how better to standardise the reporting of complications and what additional data reporting fields would be helpful. Programmes may for example wish to consider use of the Clavien Dindo grading of surgical complications – as used by Mäki-Lohiluoma et al. (5) in their retrospective analysis of complication risk after non-filarial hydrocele surgery. In addition to post operative care, improving the evidence base around complications is important for both patient management (in theatre) and patient counselling (pre-surgery). In the Uganda Hydrocele Tracker, it is notable that two patients with necrotic tissue at week two went on to have orchidectomy.
WHO guidance on the reporting and management of complications associated with LF morbidity management is primarily guided by practices and policies used for other ongoing surgical initiatives managed by national health services. For example, WHO recommends a 30-day post-operative follow-up period for common surgeries to support surgical site infection surveillance (30). Ideally, a total of three patient check-in points are scheduled during this surveillance period – week 1, week 2, and week 4. Conducting surveillance for a longer but limited period of time (such as three to six months) can be feasible, but again is often prohibitive in low-resource settings.
In the case of filarial hydrocele there is a lack of clear global guidance on follow-up points after 4 weeks. Mante and Seim (21) suggest that “After the wound heals and the patient is discharged from immediate post-operative follow-up at day 14, follow-up monthly is suggested for two months, then at 6 months and one year, then only if they have any problem”. Both countries in this study will need to focus on the best way to standardise and support (through human and financial resources) the associated costs of any long-term follow-up. The Uganda team are keen to ‘recommend’ that after month 1, follow ups are scheduled at month 6, year 1 and year 2 and greater attention is given to follow up in communities (rather than only health facilities).
Patient feedback
Patient feedback has been shown to be positively correlated with improved patient outcomes in surgical intervention cases (31) and can be integrated into the programme monitoring and evaluation process. The categorisation of the patient feedback tool used in this study into distinct domains facilitated the evaluation of various aspects of the service, allowing the programme to identify and implement necessary changes. Furthermore, the use of neutral individuals to facilitate the assessment provided impartial feedback on the quality of services received. The presence of different question formats between the two versions made conducting a comprehensive comparison of different domains between the two countries difficult. To allow for such comparison between settings the various versions will need to be harmonised. We found the revised version 2 with Likert scale questions to be ideal, as it allows for the evaluation of different domains on a scale. Based on the findings here the open-ended questions may need to be grouped, with the option to specify additional suggestions in an open-ended format.
The results indicate that a considerably greater proportion of patients in Nigeria (71.6% of all patients operated) participated in the beneficiary feedback process compared to Uganda (3.6%). This difference may be attributed to the interval between the time of surgery and the feedback evaluation. In Uganda, the feedback evaluation was conducted six months after the surgery, while in Nigeria it happened within one month of the procedure. Looking forward, we recommend considering the feedback evaluation as a continuum which is aligned with the schedule for post operative follow up and allows for both an evaluation of the patient’s experience of the actual service immediately after the surgery (e.g. at day 14 follow up) and an evaluation of the other aspects of the surgery’s impact on their quality of life at much later times. Such an approach will allow for a much more comprehensive assessment. For instance, data indicate that in Uganda, most respondents reported appreciable changes to their financial circumstances. This finding might be explained by the fact that the evaluation was carried out at 6 months after their surgeries, when patients would have been fully recovered and have fully returned to their financial activities. These additional aspects of reintegrating into society, like the capacity to resume the economic impact of surgery, are best assessed much later, ideally three to six months following the procedure, when the patient has had enough time to heal from the surgery and now fully resumed economic activities. We advise against reviewing feedback beyond six months, as this could lead to recall bias, unless ongoing care and engagement with the healthcare service is maintained throughout this period.
Digitised data and systems
We argue that the number of data entry errors or inconsistencies in the data sets from both countries stem from, 1. Data literacy challenges and 2. Programmes not following the process to undertake data quality checks as the activities were ongoing.
In the case of data literacy, the majority of data was entered into the system not by the surgeons themselves but instead data entry clerks and other staff who likely do not know all of the components of hydrocele surgery and could therefore easily make mistakes when entering data. Where use of the Hydrocele Tracker continues we would recommend further training on hydrocele surgery for those tasked with entering data. Sightsavers and national programmes will also continue to obtain user feedback to help avoid data entry errors, and the tool can be improved over time based on challenges (e.g. forms could make the selection of surgical procedure default to the procedure recommended by the country, and users would need to change the default if a different surgical technique is being used). It was not within the scope of this paper, but further research on the Hydrocele Tracker could compare paper records with digital ones – it may be the case that some errors were in paper records too.
In the case of data quality checks, we would recommend that the process – checking in on the Data Quality Dashboard (part of the data visualisation tool) every 2 weeks to find, investigate and fix errors – be more strictly followed. That dashboard can also be extended to flag additional errors, upon the national programme’s request. Further research on the Hydrocele Tracker alone could include a data quality review looking across the seven dimensions: accuracy, reliability, precision, completeness, timeliness, integrity and confidentiality (32). While undertaking analysis, accuracy and completeness seemed to be most challenging, with some questions answered inappropriately given the context of the patient, and at times patients entered with pre-operative and post-operative data but no inter-operative data. A data quality review would help the national programmes understand the challenges and take action where needed.
Data access is no doubt improved by a system like the Hydrocele Tracker, but developing a culture of data use is even more important. With subsequent use of the tool we would suggest more formalised roles for supervisors and more clear guidance on how the tool can be used (e.g. the dashboards can be used during programme review meetings and for national/regional presentations; the data set can be used to review surgeon performance and better plan subsequent surgeon training).
Looking ahead to future iterations of the Hydrocele Tracker, the experience from these pilots has brought to light potential changes to indicators and data quality checks. Examples of such changes among the pre-operative fields are removing ‘hydrocele diameter’ (used in Nigeria only), a field which isn’t part of any standardised classification. Adding hydrocele stage and buried penis grade as described by Capuano and Capuano (20) and recommended in the WHO (2019) manual ‘Surgical approaches to the urogenital manifestations of lymphatic filariasis (1) should be considered; a standardised methodology and terminology is important for both researchers and practitioners and will facilitate better patient care (9). Another possible addition to the pre-operative form would be asking patients if they had previous hydrocele surgery (as evidence for recurrence).
The inclusion of patients with values below ‘standard’ thresholds for decision to recommend surgery highlights the need for an additional field to support decisions taken e.g. i) a patient with purulent products or haematic fluids will have Hb<9 though still needs to be operated e.g. ii) some patients with HCT <30% may still get surgery, based on physical examination which deems the patient fit for surgery. Contingent upon such amendments in the Hydrocele Tracker and related training these fields may be used to evidence adherence to surgical standards/quality of surgical provision.
For the inter-operative form, the way volume (ml) is captured could be changed so that the actual volume is recorded rather than band; the current upper band (>500ml) does not capture very large volumes that may be present. Additionally, standardisation of information content relating to severity of complications and steps taken to manage complications would be useful. The DQA dashboard could include thresholds for implausibly long duration of hospitalisation and an additional check on out of sequence or oddly timed follow-up dates could also include date since surgery. Both would enable the programme to check with facilities to fix data entry errors.
As for the future of the system, one next step would be to hold a formal evaluation with a group of global experts both in LF, surgery and health data management. Greater engagement is also needed with the broader surgical community and Sightsavers would welcome other partners on the Hydrocele Tracker including, but not limited to, the West African College of Surgeons and the College of Surgeons of East, Central and Southern Africa. These additional perspectives, combined with that of the national programmes, could help shape what a version 2 of the system may look like. The amount of data being collected, the content of the dashboards, and broader questions around national ownership, resource considerations (both human and financial) and sustainability could be included in the evaluation.
Part of that sustainability is the aspect of health information systems and the larger picture in each country with surgical service monitoring and reporting systems. Each LF endemic country will differ greatly with current systems in place. In Uganda, for example, while all records are paper-based, some health facilities also use local health information systems to manage patient records. However these systems may not be sufficient to manage post-operative data, do not aggregate up and are not interoperable with the national HMIS (33, 34).
Universal Health Coverage (UHC) principles towards the realisation of the Sustainable Development Goals (SDGs) for 2030 include developing a sufficient health workforce able to deliver care - and also a workforce that is able to manage individual medical records, document access to services, and monitor outcomes of surgeries at district and facility level. However, in many countries the infrastructure is not yet in place to facilitate this. For national LF programmes wanting the ability to track patients over time and have multiple indicators automatically aggregated to district/regional/national levels for programme monitoring and EPIRF reporting needs, a system like the Hydrocele Tracker has the potential to be a provisionary solution as community health information or national electronic medical record systems are established.
Data availability statement
The data analysed in this study is subject to the following restrictions: The manuscript is based on secondary analysis of existing (anonymised) ‘Hydrocele Tracker’ datasets from Uganda and Nigeria. A data use agreement was signed between the national/state programmes and Sightsavers to support the writing of this manuscript. Restrictions apply to the dataset: The datasets presented in this article are not readily available because the data is owned by the respective national NTD programmes. Requests to access the anonymised datasets should be directed to the corresponding author (Philip Downs,cGRvd25zQHNpZ2h0c2F2ZXJzLm9yZw==) who will forward them to the relevant national or state programme.
Ethics statement
The requirement of ethical approval for studies involving humans was waived by the National Health Research Ethics Committee of Nigeria and the Uganda Vector Control Division - Research and Ethics Committee because according to the national codes the activity met the criteria for exemption. The manuscript is based on secondary analysis of existing (anonymised) NTD programme data from Uganda and Nigeria. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin because the manuscript is based on secondary analysis of existing (anonymised) NTD programme data from Uganda and Nigeria.
Author contributions
SD: Conceptualization, Formal Analysis, Writing – original draft, Writing – review & editing. JoA: Investigation, Writing – original draft, Writing – review & editing, Formal Analysis, Supervision. JeA: Formal Analysis, Investigation, Supervision, Writing – original draft, Writing – review & editing. WB: Conceptualization, Formal Analysis, Investigation, Supervision, Writing – original draft, Writing – review & editing. SB: Conceptualization, Methodology, Project administration, Writing – original draft, Writing – review & editing. CN: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Software, Supervision, Writing – original draft, Writing – review & editing. BN: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Software, Supervision, Writing – original draft, Writing – review & editing. AW: Investigation, Project administration, Supervision, Writing – review & editing. AG: Investigation, Project administration, Supervision, Writing – review & editing. MO: Investigation, Project administration, Writing – review & editing. AbA: Investigation, Project administration, Supervision, Writing – review & editing. SI: Investigation, Project administration, Writing – review & editing. MI: Formal Analysis, Writing – original draft, Writing – review & editing. DN: Conceptualization, Formal Analysis, Investigation, Writing – review & editing. CW: Resources, Writing – review & editing. MD: Resources, Writing – review & editing. HZ: Resources, Writing – review & editing. AtA: Resources, Writing – review & editing. MS: Resources, Writing – review & editing. PD: Conceptualization, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. We extend thanks to players of People's Postcode Lottery', the UK Foreign, Commonwealth and Development Office (FCDO) (contract number 205249) and an Anonymous Donor for supporting the related programme activities.
Acknowledgments
Nigeria Federal MOH, Nigeria State (Benue, Kaduna, Kebbi, Kogi, Sokoto) MOH NTD programmes, Uganda MOH Vector Control Division. Andy Tate, Sightsavers for developing maps.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fitd.2024.1379902/full#supplementary-material
Footnotes
- ^ Ministry of Health, Uganda, Vector Control Division. https://vectorcontroldivisionuganda.wordpress.com/programme-to-eliminate-lymphatic-filariasis-pelf/https://vectorcontroldivisionuganda.wordpress.com/programme-to-eliminate-lymphatic-filariasis-pelf/ [Accessed January 19, 2024]
- ^ CommCare. Cambridge, Massachusetts, USA: Dimagi. Available at: https://dimagi.com
- ^ Metabase. San Francisco, CA, USA: Metabase. Available at: https://www.metabase.com/
References
1. WHO. Surgical approaches to the urogenital manifestations of lymphatic filariasis. Report from an informal consultation among experts. Geneva: World Health Organization (2019). Available at: https://www.who.int/publications/i/item/WHO-CDS-NTD-PCT-2019.04.
2. WHO. Lymphatic filariasis: managing morbidity and preventing disability: an aide-memoire for national programme managers. 2nd edition. Geneva: World Health Organization (2021). Available at: https://www.who.int/publications/i/item/lymphatic-filariasis-managing-morbidity-and-preventing-disability-an-aide-m%C3%A9moire-for-national-programme-managers-2nd-ed.
3. WHO. Validation of elimination of lymphatic filariasis as a public health problem. Geneva: World Health Organization (2017). Available at: https://iris.who.int/bitstream/handle/10665/254377/9789241511957-eng.pdf.
4. WHO. Global programme to eliminate lymphatic filariasis; progress report (2022). Available online at: https://www.who.int/publications/i/item/who-wer9841-489-502.
5. Mäki-Lohiluoma L, Kilpeläinen TP, Järvinen P, Söderström HK, Tikkinen KAO, Sairanen J. Risk of Complications after hydrocele surgery: A retrospective multicenter study in helsinki metropolitan area. Eur Urol Open Sci. (2022) 43:22–7. doi: 10.1016/j.euros.2022.06.008
6. Beyene AD, Kebede F, Mammo BM, Negash BK, Mihret A, Abetew S, et al. The implementation and impact of a pilot hydrocele surgery camp for LF-endemic communities in Ethiopia. PloS Negl Trop Dis. (2021) 15:e0009403. doi: 10.1371/journal.pntd.0009403
7. Mante SD, Gueye SM. Capacity building for the modified filarial hydrocelectomy technique in West Africa. Acta Trop. (2011) 120 Suppl 1:S76–80. doi: 10.1016/j.actatropica.2010.09.008
8. Thomas G, Richards FO, Eigege A, Dakum NK, Azzuwut MP, Sarki J, et al. A pilot program of mass surgery weeks for treatment of hydrocele due to lymphatic filariasis in central Nigeria. Am J Trop Med Hygiene. (2009) 80:447–51. doi: 10.4269/ajtmh.2009.80.447
9. Lim KH, Speare R, Thomas G, Graves P. Surgical treatment of genital manifestations of lymphatic filariasis: A systematic review. World J Surg. (2015) 39:2885–99. doi: 10.1007/s00268-015-3220-4
10. Federal Ministry of Health, Nigeria. National Surgical, Obstetrics, Anaesthesia & Nursing Plan (NSOANP) for Nigeria. Strategic Priorities for Surgical Care (StraPS) Planning for a Future of Surgical Equity, Safety & Progress. 2019-2023 (2019). Available online at: https://www.pgssc.org/_files/ugd/d9a674_1f7aa8161c954e2dbf23751213bc6f52.pdf.
11. Ministry of Health, Uganda. The Uganda Health Information and Digital Health Strategic Plan 2020/21-2024/25. Kampala, Uganda: Ministry of Health. (2021). Available at: http://library.health.go.ug/health-information-systems/digital-health/uganda-health-information-and-digital-health-strategic.
12. Ministry of Health, Uganda. Neglected Tropical Diseases Masterplan, 2023-2027. Kampala, Uganda: NTDCP Control Program, MoH Vector Control Division. Available at: https://espen.afro.who.int/system/files/content/resources/Uganda_NTD_Master_Plan_2023_2027_Final.pdf.
13. Uganda MOH Vector Control Division. Knowledge, Attitude and Practices of Lymphatic Filariasis Chronic Manifestation in Uganda Dec 2017 . Available online at: https://research.sightsavers.org/wp-content/uploads/2021/06/KAP-Uganda-final-report.pdf.
14. Kelly WP. Hydrocele amongst the lango of Uganda. Br Med J. (1924) 1:746–7. doi: 10.1136/BMJ.1.3304.746-A
15. Galukande M, Kituuka O, Elobu E, Jombwe J, Sekabira J, Butler E, et al. Improving surgical access in rural africa through a surgical camp model. Surg Res Pract. (2016) 2016:9021945. doi: 10.1155/2016/9021945
16. Kakande, et al. Surgical camps: the Ugandan experience (2001). Available online at: https://tspace.library.utoronto.ca/bitstream/1807/52565/1/js01010.pdf.
17. Nigeria Federal Ministry of Health. Nigeria Masterplan for Neglected Tropical Diseases 2023-2027. Abuja, Nigeria: Federal Ministry of Health. (2023).
18. WHO Integrated Management for Emergency and Essential Surgical Care (IMEESC) Toolkit . Available online at: https://www.who.int/docs/default-source/integrated-health-services-(ihs)/csy/gieesc/whotoolsituationalanalysiseesc.pdf?sfvrsn=fccb6814_5.
19. Martindale S, Mableson H, Bodimeade C, Hume H, Badia-Rius X, Karim J, et al. The development and roll-out of a new hydrocoele surgery facility assessment tool for the elimination of lymphatic filariasis. Int Health. (2022) 14:ii55–63. doi: 10.1093/inthealth/ihac020
20. Capuano GP, Capuano C. Surgical management of morbidity due to lymphatic filariasis: The usefulness of a standardized international clinical classification of hydroceles. Trop Biomed. (2012) 29:24–38.
21. Mante S, Seim A. West Africa LF Morbidity Project: Surgical Handbook - An Aid to District Hospital Surgeons (2007). Available online at: https://hdi.no/wp-content/uploads/2018/03/lymphatic-filariasis-guide.pdf.
22. WHO PC Epidemiological Data Reporting Form v6 . Available online at: https://apps.who.int/neglected_diseases/ntddata/forms/jap/en/WHO_EPIRF_PC.xlsm (Accessed January 19, 2024).
23. Hinzmann R, Militz D, Zima T, Špaček M, Storm H, Chapanduka Z, et al. Real-world data from Europe and Africa suggest that accuracy of systems for self-monitoring of blood glucose is frequently impaired by low hematocrit. Diabetes Res Clin Pract. (2021) 177:108860. doi: 10.1016/j.diabres.2021.108860
24. Pullum T, Deborah KC, Sorrel N, Dean G. Hemoglobin Data in DHS Surveys: Intrinsic Variation and Measurement Error. DHS Methodological Reports No. 18. Rockville, Maryland, USA: ICF (2017). Available at: https://dhsprogram.com/publications/publication-mr18-methodological-reports.cfm.
25. Kebede B, Martindale S, Mengistu B, Kebede B, Mengiste A, H/Kiros F, et al. Integrated morbidity mapping of lymphatic filariasis and podoconiosis cases in 20 co-endemic districts of Ethiopia. PloS Negl Trop Dis. (2018) 12:e0006491. doi: 10.1371/journal.pntd.0006491
26. Mwingira U, Chikawe M, Mandara WL, Mableson HE, Uisso C, Mremi I, et al. Lymphatic filariasis patient identification in a large urban area of Tanzania: An application of a community-led mHealth system. PloS Negl Trop Dis. (2017) 11:e0005748. doi: 10.1371/journal.pntd.0005748
27. Noroes J, Dreyer G. A mechanism for chronic filarial hydrocele with implications for its surgical repair. PloS Negl Trop Dis. (2010) 4:e695. doi: 10.1371/journal.pntd.0000695
28. Brunicardi FC, Andersen DK, Billiar TR, Dunn DL, Hunter JG, Pollack RE. Schwartz’s Principles of Surgery. 8th Edition. New York: McGraw-Hill Education (2005). p. 1950.
29. Bartlett S, Ngom B, Olobio N, Badiane MD, Tarboh G, Diagne A, et al. Improving data use in trachomatous trichiasis programmes: operationalisation of the TT Tracker. Int Health. (2023) 15:ii73–6. doi: 10.1093/inthealth/ihad057
30. WHO. Protocol for surgical site infection surveillance with a focus on settings with limited resources. Geneva: World Health Organization (2018). Available at: https://cdn.who.int/media/docs/default-source/integrated-health-services-(ihs)/ipc/ssi-surveillance-protocol.pdf?sfvrsn=d24a1d1c_3.
31. Maruthappu M, Trehan A, Barnett-Vanes A, McCulloch P, Carty MJ. The impact of feedback of surgical outcome data on surgical performance: a systematic review. World J Surg. (2015) 39:879–89. doi: 10.1007/s00268-014-2897-0
32. WHO. Preventive chemotherapy: tools for improving the quality of reported data and information. A field manual for implementation. Geneva: World Health Organization (2019). Available at: https://www.who.int/publications/i/item/9789241516464.
33. Mariam B, Mutwalibi N. Information streams in health facilities: the case of Uganda. Data Intell. (2022) 4:882–98. doi: 10.1162/dint_a_00177
Keywords: lymphatic filariasis, hydrocelectomy, hydrocele, surgery, reporting, digitisation, Nigeria, Uganda
Citation: D’Souza SF, Awio JP, Albarka J, Bougma WR, Bartlett S, Nwosu C, Ngom B, Wani A, Gwom A, Okello M, Aba A, Irema S, Imhansoloeva M, Nurudeen D, Wamboga C, Debam MT, Zainab H, Aleiro A, Salah MH and Downs P (2024) Advances in filarial hydrocelectomy reporting in Uganda and Nigeria. Front. Trop. Dis 5:1379902. doi: 10.3389/fitd.2024.1379902
Received: 31 January 2024; Accepted: 05 March 2024;
Published: 23 April 2024.
Edited by:
Anders Seim, Health and Development International, United StatesReviewed by:
Alexander Kwarteng, Kwame Nkrumah University of Science and Technology, GhanaCatherine Devries, The University of Utah, United States
Copyright © 2024 D’Souza, Awio, Albarka, Bougma, Bartlett, Nwosu, Ngom, Wani, Gwom, Okello, Aba, Irema, Imhansoloeva, Nurudeen, Wamboga, Debam, Zainab, Aleiro, Salah and Downs. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Philip Downs, cGRvd25zQHNpZ2h0c2F2ZXJzLm9yZw==