 Solrun Søfteland1,2,3*
Solrun Søfteland1,2,3* Motshedisi Sebitloane4
Motshedisi Sebitloane4 Hashini Nilushika Galappaththi-Arachchige1,2Elisabeth Kleppa2
Hashini Nilushika Galappaththi-Arachchige1,2Elisabeth Kleppa2 Sigve Holmen5
Sigve Holmen5 Pavitra Pillay6Patrica Doris Ndhlovu7
Pavitra Pillay6Patrica Doris Ndhlovu7 Myra Taylor8
Myra Taylor8 Birgitte Jyding Vennervald9
Birgitte Jyding Vennervald9 Saloshni Naidoo8Anne Cathrine Staff1,10Manala Makua11,12Svein Gunnar Gundersen13Eyrun Floerecke Kjetland2,3,8
Saloshni Naidoo8Anne Cathrine Staff1,10Manala Makua11,12Svein Gunnar Gundersen13Eyrun Floerecke Kjetland2,3,8- 1Institute of Clinical Medicine, University of Oslo, Oslo, Norway
- 2Department of Infectious Diseases Ullevaal, Norwegian Centre for Imported and Tropical Diseases, Oslo University Hospital, Oslo, Norway
- 3Department of Global Health, Oslo University Hospital, Oslo, Norway
- 4Discipline of Gynecology at Nelson Mandela School of Medicine, University KwaZulu-Natal, Durban, South Africa
- 5Holmen Innovative Solutions AS, Hauge i Dalane, Norway
- 6Department of Biomedical and Clinical Technology, Faculty of Health Sciences, Durban University of Technology, Durban, South Africa
- 7Centre for Bilharzia and Tropical Health Research (CBTHR), Shelly Beach, South Africa
- 8Discipline of Public Health Medicine, University of KwaZulu-Natal, Durban, South Africa
- 9Section for Parasitology and Aquatic Pathobiology, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark
- 10Division of Obstetrics and Gynecology, Oslo University Hospital, Oslo, Norway
- 11National Department of Health, Pretoria, South Africa
- 12University of Pretoria, Pretoria, South Africa
- 13Department of Global Development and Planning, University of Agder, Kristiansand, Norway
Introduction: Female genital schistosomiasis is a common but neglected disease, which results in symptoms similar to sexually transmitted infections in Schistosoma haematobium-endemic areas of Africa and Middle East. In primary healthcare of low-income countries, healthcare professionals use syndromic management protocols for guidance when treating symptoms of genital infection, due to lack of laboratory resources. These protocols do not include treatment for female genital schistosomiasis, despite the overlap of symptoms. Women are at risk of not receiving the appropriate treatment. The aim of this study was to investigate challenges and missed opportunities when using syndromic management protocols for sexually transmitted infections in female genital schistosomiasis-endemic areas.
Methods: This is a secondary analysis of data from a large cross-sectional prevalence study conducted in 2011 in KwaZulu-Natal, South Africa. Young women in schistosomiasis-endemic areas were asked about genital symptoms and underwent laboratory testing and gynecological examinations to look for common genital infections including female genital schistosomiasis. We used the current South African syndromic management protocols as the basis and analyzed the associations between the reported genital symptoms and the differential diagnoses with logistic regression.
Results: By use of the syndromic approach the conditions gonorrhea, trichomoniasis and herpes could be identified. The symptom “lower abdominal pain” was significantly associated with documented female genital schistosomiasis. However, the same association was not found with gonorrhea or chlamydia. We found no significant association between reported vaginal discharge syndrome and female genital schistosomiasis or between genital ulcer syndrome and female genital schistosomiasis.
Discussion: Female genital schistosomiasis frequently co-exists with, and mimics other genital infections in rural areas of Sub-Saharan Africa. The management protocols in schistosomiasis endemic countries should include advice on how to diagnose and manage this chronic, waterborne genital condition. There is an urgent need to upscale laboratory and diagnostic resources in low-and middle-income countries and specifically schistosomiasis-endemic areas, to diagnose these common genital infections more accurately and to treat affected women accordingly.
1 Introduction
Female genital schistosomiasis (FGS) has remained a neglected entity since its discovery at the end of the 19th century (1). Despite an accelerating amount of evidence since the 1990s, healthcare professionals in endemic countries are generally not aware of the condition (2). Urinary schistosomiasis affects girls and women living in rural areas with infested water bodies, where as many as 30%–70% might have genital manifestations (3–6). The UNAIDS (2021) estimates that approximately 56 million girls and women live with genital schistosomiasis (7, 8). The parasite and their eggs reside in blood vessels in all parts of the female reproductive tract, and egg deposition may lead to long-lasting inflammatory reactions in the different tissues (9). For this reason, infection with Schistosoma haematobium can lead to a broad variety of gynecological symptoms, such as foul-smelling discharge, blood spotting, lower abdominal pain (LAP), genital ulcer, dyspareunia, and postcoital bleeding (9). In the long term, the damage caused by egg deposition may lead to a higher risk of infertility, ectopic pregnancies, and abortion (10–12). Importantly, individuals who have moved away from endemic areas may experience symptoms and complications many years after exposure, since water contact in childhood may result in chronic disease (13).
In low-resource settings, the World Health Organization (WHO) recommends that syndromic management protocols are used to determine management of genital symptoms and treatment of sexually transmitted infections (STIs) (14). The rationale is to reduce suffering, transmission, and complications when laboratory services are scarce, and patients may not have the possibility, time, or resources to return to a clinic for laboratory result-based treatment (14, 15). According to the WHO, research has previously shown that the syndromic management protocols are cost-effective (14–16). However, subsequent investigations have tempered the enthusiasm from the early years, showing low diagnostic accuracy and thereby a need to upscale laboratory diagnostics in low-resource healthcare settings (17, 18). The nature of syndromic management protocols may be outdated in light of changing disease profiles and emerging infections. Moreover, the present syndromic approach does not include FGS as a cause of genital illness. The WHO continues to advise healthcare authorities to implement syndromic management when there are no other options; hence, many countries use this as their local guidelines for the management of STIs (14). As a result, women in low-resource primary healthcare settings are treated syndromically, at the point of care, often without a gynecological examination or laboratory tests.
In South Africa, the “Standard Treatment Guidelines and Essential Medicines List for South Africa, Primary Health care level” (19) is used by primary healthcare professionals. Very often, these are nurses who diagnose and prescribe accordingly. If a woman presents with vaginal discharge at a low-resource primary healthcare clinic, the current guidelines recommend giving her ceftriaxone, azithromycin, and metronidazole to treat three diseases simultaneously, namely, gonorrhea, chlamydia, and trichomoniasis (14, 19). However, in areas endemic for S. haematobium, these symptoms may be caused by FGS (20, 21). Therefore, women are at risk of not receiving the appropriate treatment as per the current management protocols.
The aim of this paper was to investigate possible symptoms of FGS in relation to the current syndromic management protocol, using data from a previous project where FGS was diagnosed alongside other genital infections (22).
2 Methods
2.1 Study areas
The data were gathered in 2011–2013 by our group, in the districts of Ilembe, uThungulu, and Ugu in KwaZulu-Natal, South Africa (22, 23).
2.2 Study populations
In schistosomiasis-endemic areas of KwaZulu-Natal, school-going adolescents and young women were recruited for examinations, as described previously (22). Virgins, pregnant women, and seriously ill women were excluded.
2.3 Study design
From the results of a cross-sectional study, diagnostic data were analyzed with the focus on syndromic diagnosis of genital symptoms. Syndromic management guidelines from the WHO (14) and South Africa (19) were used for defining the syndromic approach.
After consent procedures, all participants underwent a detailed questionnaire in the local language. In addition to age, history of contact with possible schistosomiasis-infested water bodies, recent sexual contact, and general health issues such as HIV, the participants were asked about genital symptoms such as history of discharge, genital ulcers, Lower Abdominal Pain (LAP), and dyspareunia. Owing to the chronic nature of FGS lesions, the participants were asked whether they had experienced these symptoms the last week or sometime before. Consenting participants underwent gynecological examination and laboratory analyses for the common genital infections including S. haematobium (24).
2.4 Ethics
Ethical approvals were given by the Biomedical Research Ethics Committee (BREC), University of Kwa-Zulu-Natal, South Africa (Ref BF09/07); the Department of Health, Pietermaritzburg, South Africa (Ref HRKM010-08); and the Regional Committees for Medical and Health Research Ethics (REC), Southeast Norway (Ref 469-07066a1.2007.535, renewed in 2011). All participants signed a consent form that had been thoroughly explained by a trained research assistant fluent in the local language. The gynecological examination was carried out by female doctors only, following a thorough explanation of the procedure before the participants entered the examination room. Girls and women who had been subject to abuse or had a current disease were offered counseling or were referred for further follow-up, if they wished.
2.5 Laboratory analysis
Urine samples were collected from all participants, centrifuged, and examined with a light microscope for S. haematobium ova (22, 23). As has been reported previously, cervicovaginal samples were collected and analyzed for Chlamydia trachomatis, Neisseria gonorrhoeae [ligase chain reaction (LCR)], and Trichomonas vaginalis [polymerase chain reaction (PCR)] (22, 24). A subsample of the participants was tested for Herpes simplex virus type 2 using ELISA, and high-risk human papillomavirus (HPV) by PCR. Bacterial vaginosis was diagnosed using Nugent’s criteria. Candidiasis was diagnosed by Gram stain under a light microscope. HIV and Treponema pallidum serology were done in all consenting participants. For further details regarding laboratory analysis, see previously published material (22, 24).
2.6 Gynecological examination and the diagnosis of female genital schistosomiasis
After a visual inspection of the vulva and cervix, the physician did a colposcopic examination of the cervix and the vaginal walls, as has been reported previously (25). The findings were documented using conventional stationary colposcopes, either an Olympus OCS 500 colposcope with a mounted Olympus E 420 10-megapixel single-lens reflex device (Olympus, Tokyo, Japan) or a Leisegang colposcope (Leisegang, Berlin, Germany) with a Canon EOS 40D 10-megapixel single-lens reflex device (Canon, Tokyo, Japan). Papanicolaou (Pap) smears were taken. Lesions suspicious of FGS were categorized as recommended by the WHO Pocket Atlas for Female Genital Schistosomiasis (Figure 1) (1): grainy sandy patches, (2) homogeneous yellow sandy patches, (3) rubbery papules, and (4) abnormal blood vessels (2, 21, 26). To date, no single laboratory analysis has been found to be accurate enough to diagnose FGS (10, 20, 22). The current consensus for FGS diagnosis during research is visual inspection by colposcopy confirmed by one positive laboratory test for schistosomiasis (21, 27). In the present analyses, the visual diagnosis was confirmed by either urine microscopy, circulating anodic antigen (CAA), or PCR from a genital or urinary specimen.
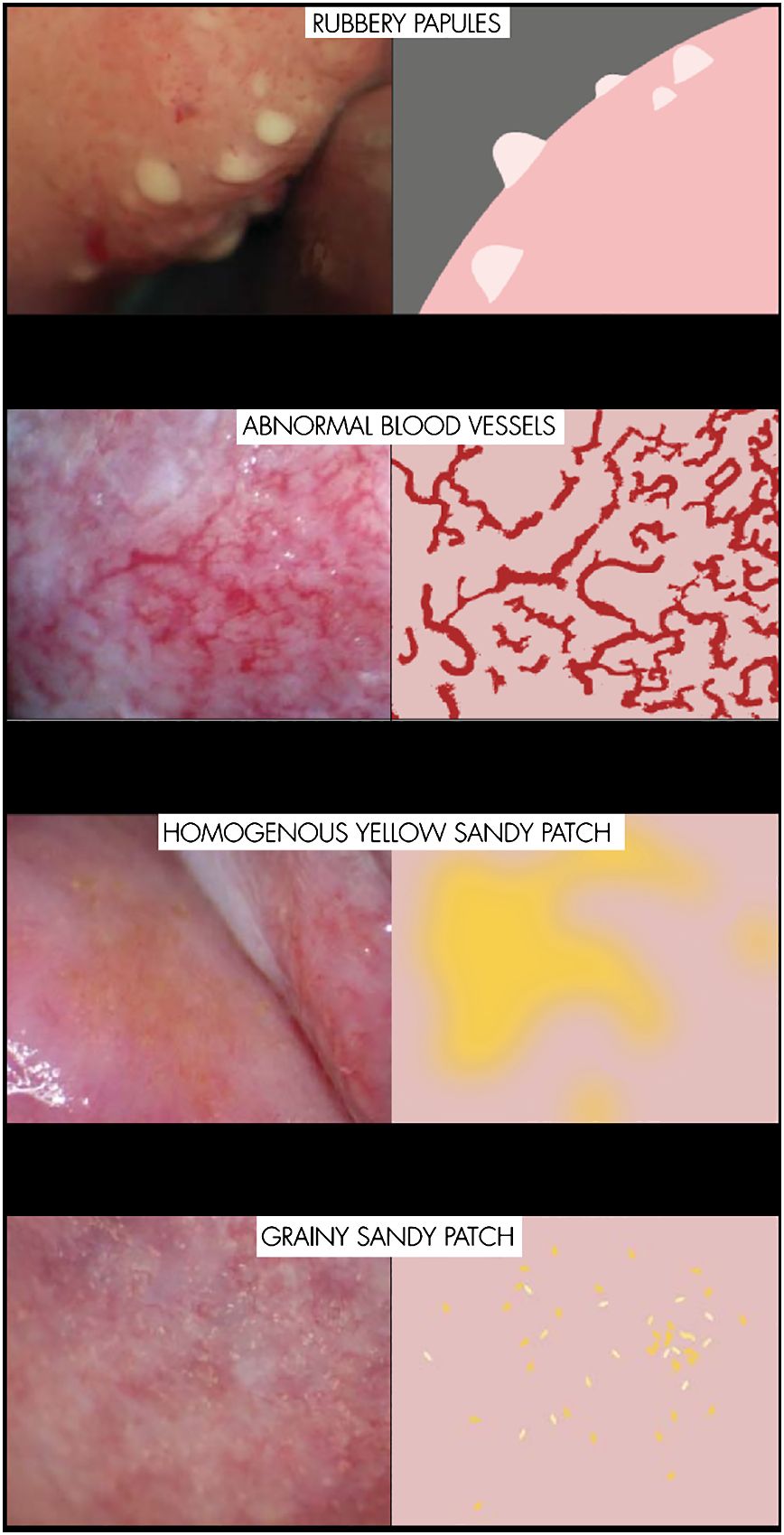
Figure 1 The four different lesions of female genital schistosomiasis.
2.7 Syndromic approach
Using “Standard Treatment Guidelines and Essential Medicines List for South Africa, Primary Health care level” (19) as a basis, we focused on the symptoms that constitute vaginal discharge syndrome (VDS), Lower Abdominal Pain (LAP), and genital ulcer syndrome (GUS). These symptoms were previously found to be associated with FGS (9, 10, 28, 29). As per the standard treatment guidelines, we categorized the women as “sexually active in the last 3 months” and “not sexually active in the last 3 months”.
VDS: We included only those who reported smelly and/or abnormal discharge color in the preceding week. Although patients with FGS might experience genital symptoms over time, these were healthy volunteers and we wished to reduce the risk of recall bias.
LAP: We included women reporting LAP in the preceding week but excluded cases reporting being on the first day of menstruation.
GUS: We included women reporting GUS in the preceding week.
2.8 Statistical analysis
IBM SPSS Statistics Version: 28.0.0.0 (190) was used for the statistical analysis. After running chi-square tests with all the different genital symptoms against the different diagnoses, we did logistic regression with the syndromes—VDS, LAP, and GUS—as dependent variables, and the confirmed diagnoses—C. trachomatis, N. gonorrhoeae, T. vaginalis, bacterial vaginosis, candidiasis, Herpes simplex 2, T. pallidum, and FGS—as independent variables. We adjusted for age and calculated the odds ratios (ORs) with 95% confidence intervals.
3 Results
A total of 2,388 women aged 16–34 years were included (see Table 1 for the characteristics of the participants). Sixty percent reported having current freshwater contact and over 90% reported freshwater contact at some time in their life. The majority of the participants reported being sexually active in the last 3 months, but only one-third used condoms in the preceding week. Most knew what an STI is and 1 in 10 had been treated for one. Seven percent said they had been forced to have sex.
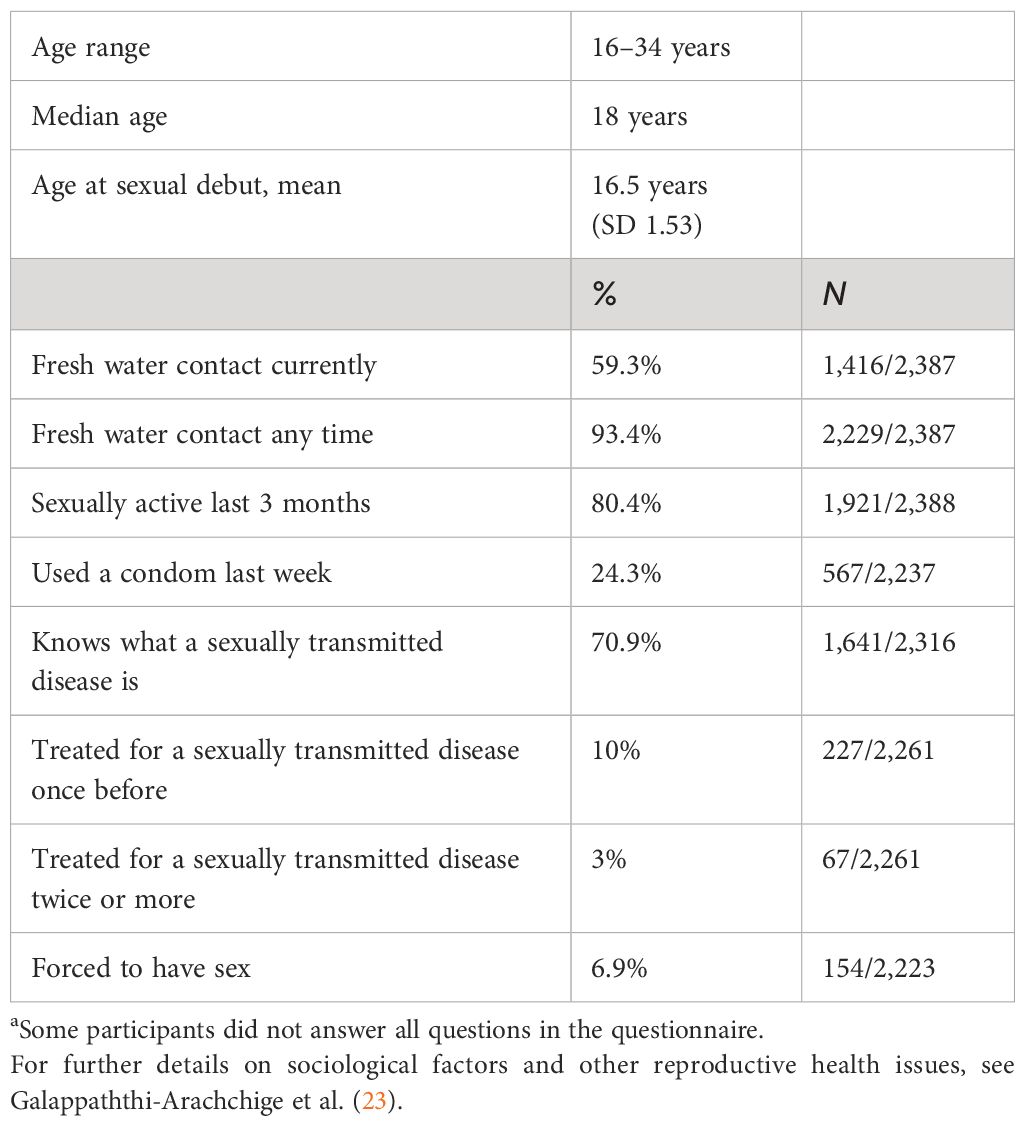
Table 1 General characteristics of 2,388a female study participants from three districts in South Africa.
Table 2 shows the genital ailments found in this group of young women. Because of financial and practical constraints, not all participants were tested for all diseases. Overall, 81.1% tested positive for one STI or more. Among the sexually active, the rate was 83%, and in the sexually non-active group, it was 76.4%. Of specific interest, gonorrhea was found in 7.8% of the reportedly non-sexually active women. In addition, 23.6% of these were found to have C. trachomatis and 17.6% had T. vaginalis. Urinary schistosomiasis was found in one in five and FGS was diagnosed in 12.5% of the study population.
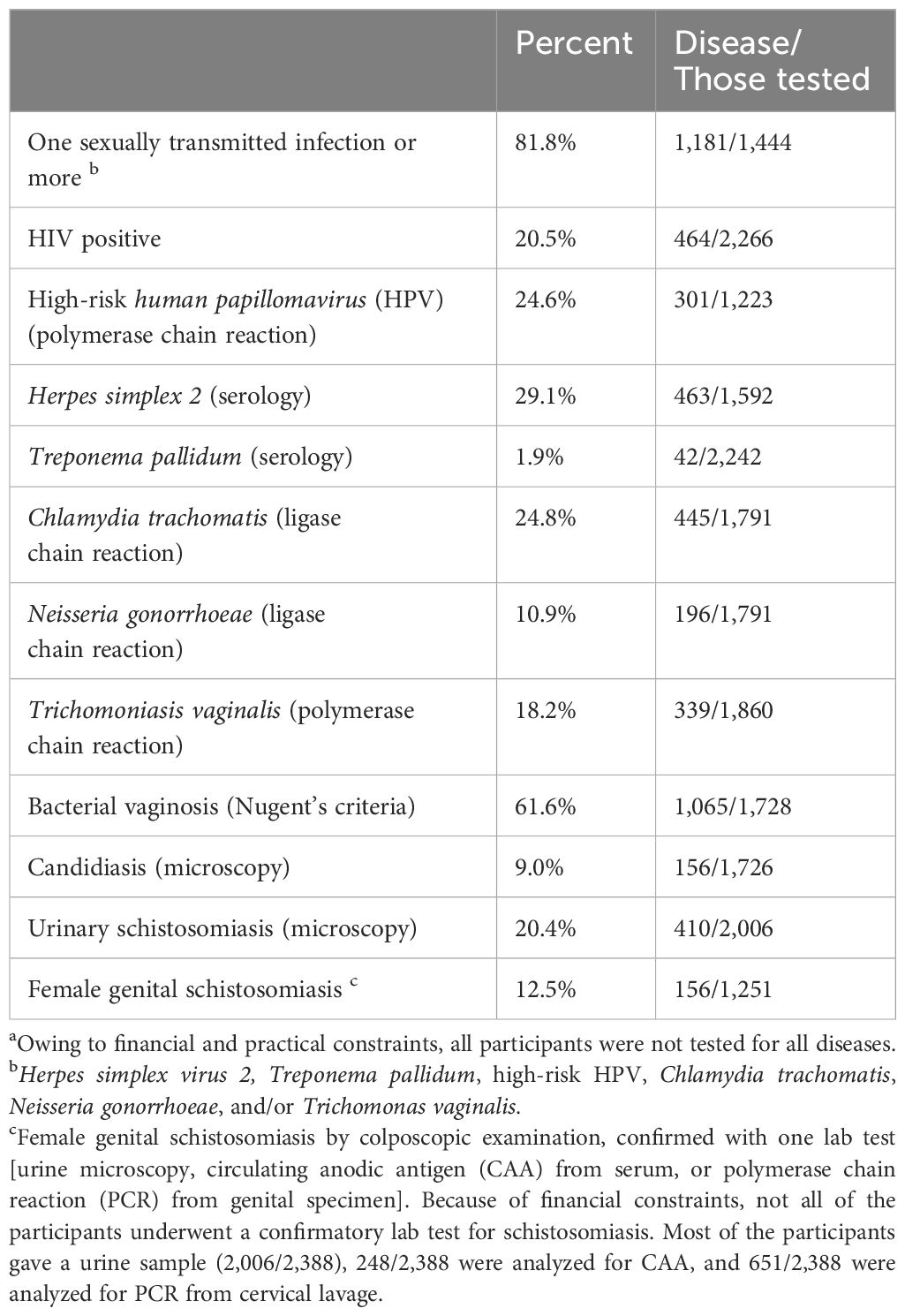
Table 2 Genital ailments in study participants (n = 2,388a).
3.1 Vaginal discharge syndrome
Table 3 shows a significant association between infection with N. gonorrhoeae and self-reported symptoms qualifying for a diagnosis of VDS. There is association with T. vaginalis. There was no statistically significant difference in the rates of reported vaginal discharge between women with and without FGS. More than 20% of those with a positive chlamydia test did not report vaginal discharge and would not have received the right treatment according to existing management protocols.
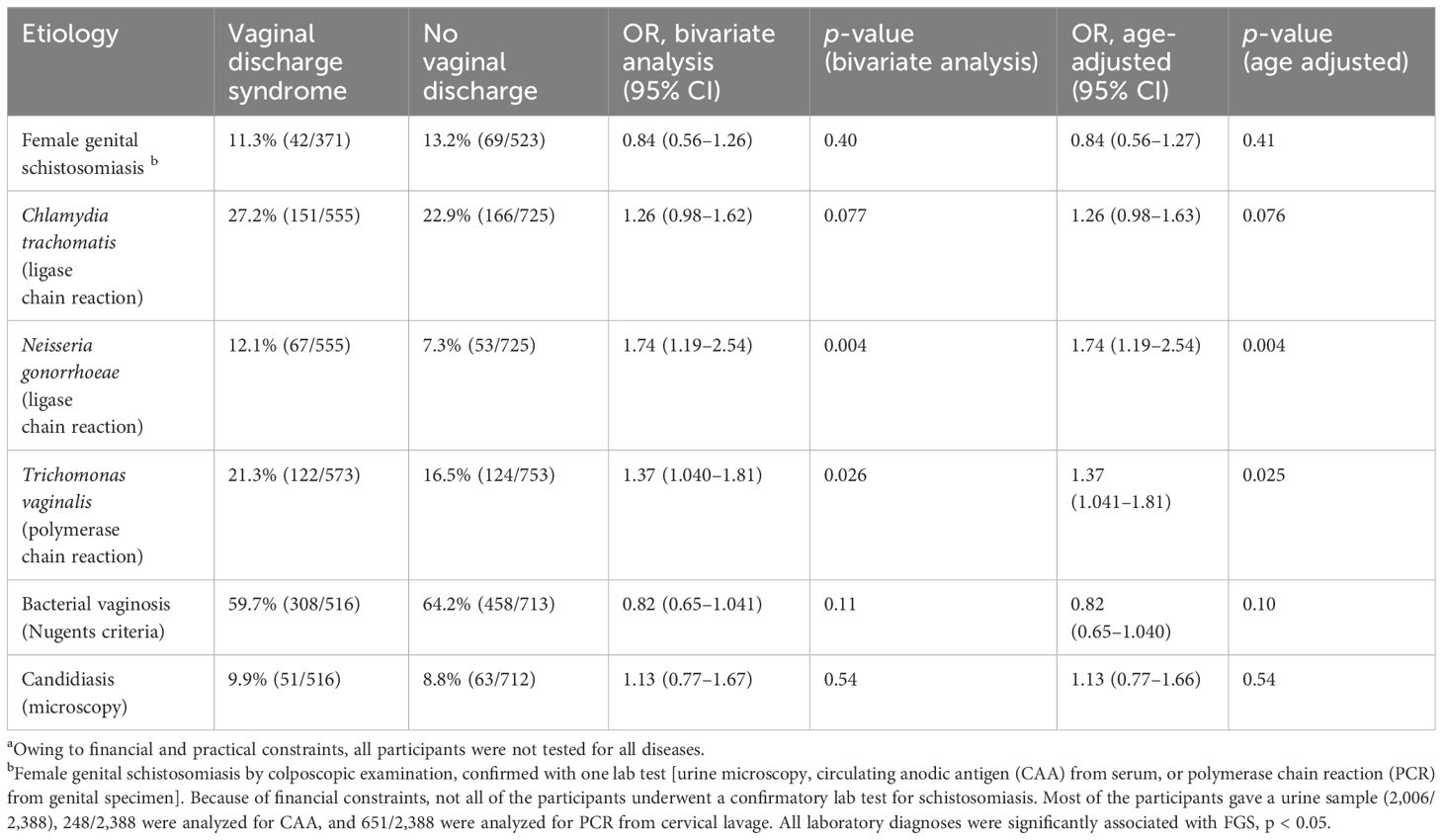
Table 3 Associations between vaginal discharge syndrome (VDS) and discharge-generating infections (n = 2,388a).
3.2 Lower abdominal pain
As shown in Table 4, there was a significant association between reported LAP and FGS, OR 1.54 (1.03–2.29), p = 0.035. However, in this population, there was no significant association between chlamydia or gonorrhea and the symptom “lower abdominal pain”.
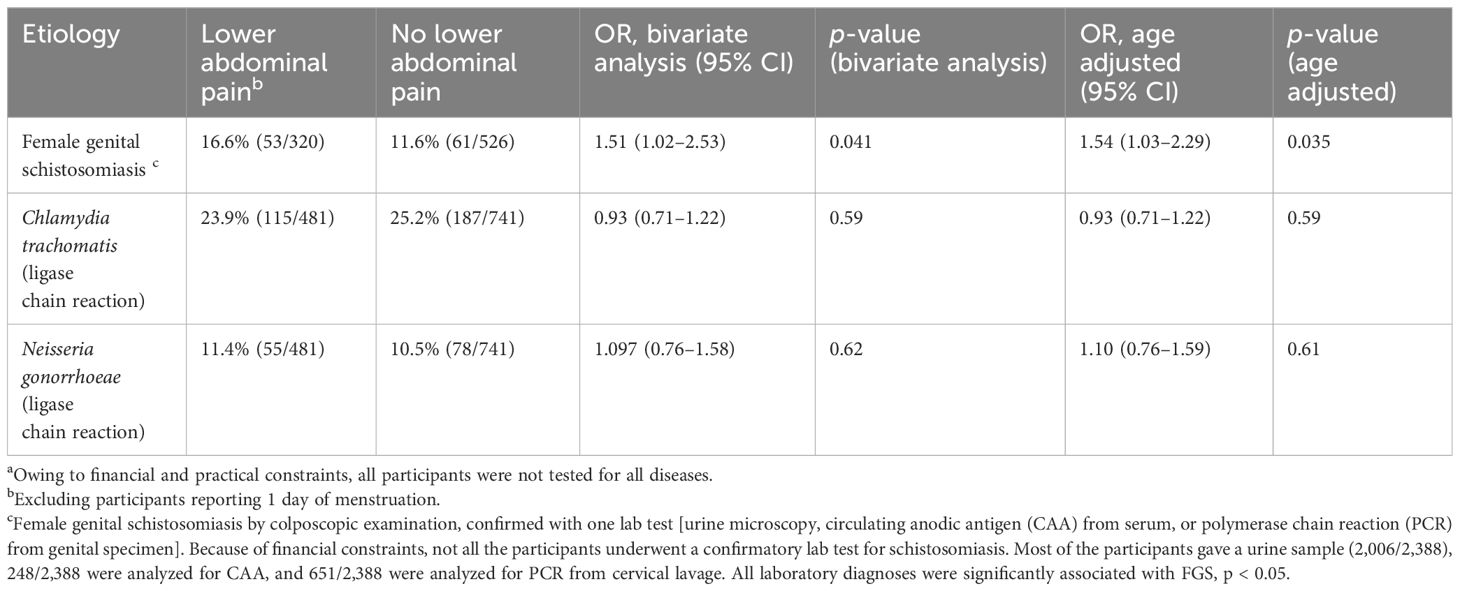
Table 4 Associations between lower abdominal pain (LAP) and relevant infections (n = 2,388a).
3.3 Genital ulcer syndrome
Table 5 shows that the management protocols are well suited to indicate infection with Herpes simplex 2 in this study, OR 2.73 (1.71–4.35), p < 0.001. There was, however, no significant association between the symptom “genital ulcer” and infection with T. pallidum or FGS.
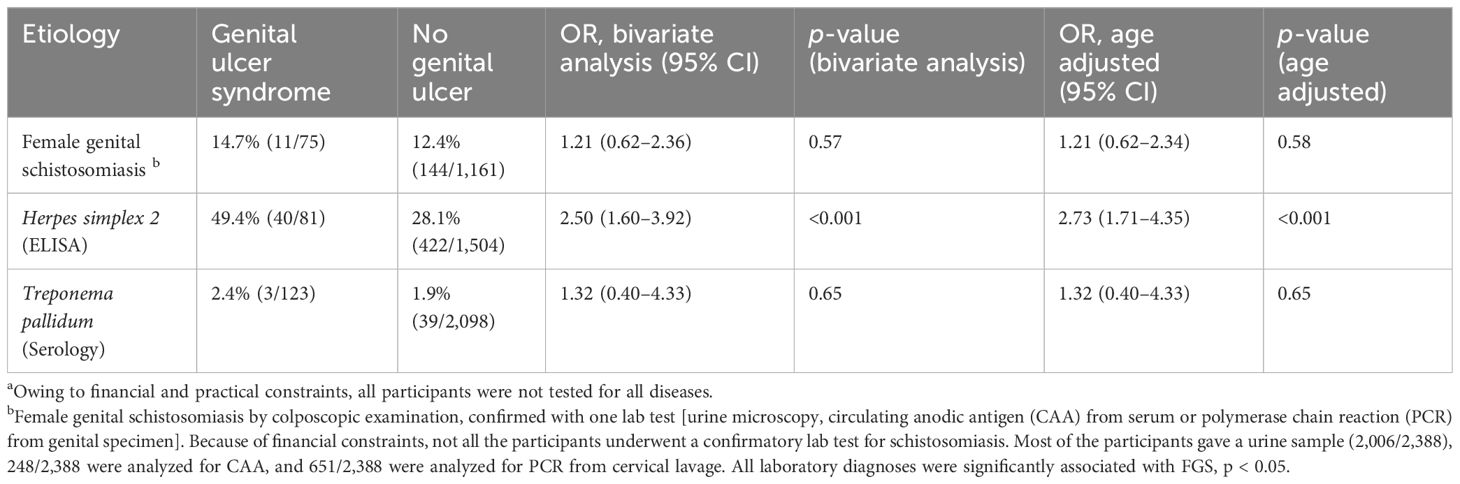
Table 5 Associations between genital ulcer syndrome (GUS) and ulcer-generating infections (n = 2,388a).
4 Discussion
The currently used clinical management protocols do not include any advice to healthcare workers about FGS. Like previous studies, we found that FGS may mimic and frequently co-exists with other genital infections (20, 24). We found FGS to be as prevalent as other well-known genital diseases in our relatively large study from rural South Africa, and there is reason to believe that this could hold true in many regions of Sub-Saharan Africa (8, 24, 30, 31). The chronic inflammation resulting from FGS may lead to an increased susceptibility to other infections, as seems to be the case for HIV transmission; women with FGS have a two- to threefold risk of having HIV (32–34). More longitudinal research is needed to investigate the association between HPV and FGS (10, 35). Girls and women with FGS are currently not being managed and are not receiving treatment for at least one or possibly several of their genital infections.
Our study on healthy volunteers identified an association between LAP and FGS. However, we did not find LAP to be associated with C. trachomatis and N. gonorrhoeae in our material. A plausible explanation could be that the chronic inflammation from S. haematobium leads to diffuse low-grade abdominal pain, while chlamydia and gonorrhea rarely result in abdominal pain until the infection has developed into more advanced pelvic inflammatory disease (PID) and acute illness (36). Surprisingly, we did not identify a significant association between VDS and FGS. In our analysis, we included only the women reporting vaginal discharge the last week, with the purpose of adapting the analysis to the management protocols and to avoid recall bias. Women with FGS may experience symptoms over months and years; hence, we may have missed some cases with this approach. Another possible explanation for this finding could be that the affected women may have adapted to the inflammatory response in their genitals and perceive their discharge as normal (5).
A remarkable finding is that these women who were invited from randomly selected schools for investigation in an FGS study had such a high level of genital symptoms and ailments. Even though many of them had health complaints, they had not sought treatment. Our analyses indicate that had they come for treatment, a symptom-focused protocol would not properly differentiate those with treatable causative agents from those without, nor would symptoms resulting from the chronic condition FGS have been recognized.
The question about being sexually active in the last 3 months or not decides the treatment plan in syndromic management of STIs. In our data, we found a high prevalence of gonococcal infection also among the “sexually non-active” participants. Questions about sexual behavior could be a sensitive issue when young women meet healthcare professionals (37). However, previous studies have shown that even gonococcal infections may persist more than 90 days after exposure (38). Our study indicates that there are challenges with categorizing women as “not sexually active” when it comes to treatment for genital infections. Furthermore, FGS is not a sexually transmitted disease and must be considered equally in both sexually active and non-active groups.
Our analysis confirms that the syndromic approach is highly inaccurate as a diagnostic tool to identify FGS, and likely leads to incorrect treatment of STIs, as has been shown before (39).
4.1 Limitations
The most important limitation of our study is that the participants were recruited as healthy volunteers, not as patients contacting a clinic due to genital issues. Hence, they do not necessarily represent the patients attending a primary healthcare clinic, which the management protocol is intended for.
Another limitation is that the study material is over 10 years old. The morbidity of S. haematobium may be influenced by treatment, migration, and environmental factors (7). However, no anti-schistosomal mass drug administration has been offered in South Africa. Furthermore, the chronic inflammatory damages from FGS may last many years after infection and praziquantel is shown not to be sufficiently effective on the chronic genital lesions (10, 13). We have thus chosen to carry out this study on historic material, since few studies exist on the clinical manifestations of FGS.
Our study data are from premenopausal women, with a median age of 18, and our findings might not be reproducible in older populations (22). S. haematobium egg deposition varies through life and seem to be highest in early teenage years (9). To the best of our knowledge, no studies on the clinical manifestations of FGS in post-menopausal women have been conducted. Since the frequency of STIs decreases with age, the risk of misdiagnosis might be lower for these diseases in the postmenopausal population (40). However, the management protocols we have used as a basis for our analysis do not distinguish between age groups. Cervical cancer is a more relevant differential diagnosis in older women, and there is a need for further research to provide guidelines for the management of postmenopausal women with genital lesions, discharge, abdominal pain, or vaginal bleeding in schistosomiasis-endemic areas.
In this study, we did not measure the body temperature of the participants, and bi-manual palpations were not carried out. We therefore cannot state from our data whether women had PID. This represents a limitation, as the STI guidelines are focused on detecting PID. LAP is an unspecific symptom with many possible causes, e.g., adenomyosis, endometriosis, fibroids, intestinal issues, and pathology in other organ systems not discussed in the STI management protocols. In our data, we do not have enough information to determine all the possible gynecological or non-gynecological reasons for the reported symptom of abdominal pain.
FGS is a visual diagnosis as no laboratory test has yet been found to be sufficiently sensitive and specific (2). The colposcopic examination required to identify lesions in the lower genital tract is provider dependent. We might have missed some FGS-positive cases due to these limitations.
4.2 Conclusion
Healthcare professionals working in areas with limited resources deserve clear guidance on how to manage genital diseases. Based on current knowledge, we cannot distinguish FGS from other infections based on symptoms only. However, in light of FGS, healthcare authorities should also ask questions on the risk factors, which are fresh water contact currently—or in childhood. Reports of LAP in both sexually active and non-sexually active women should raise suspicion of FGS as an important differential diagnosis. A correct diagnosis is essential for offering the proper care to any woman suffering from genital symptoms, including the correct treatment option. Improvements in diagnostic approaches are necessary.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: The data is de-identified but not anonymized. Data may be made available upon reasonable request as we are still analyzing data. Requests to access these datasets should be directed to c29scnVuc29lQGdtYWlsLmNvbQ==.
Ethics statement
The studies involving humans were approved by The Biomedical Research Ethics Committee (BREC), University of Kwa-Zulu-Natal, South Africa (Ref BF09/07), the Department of Health, Pietermaritzburg, South Africa (Ref HRKM010-08) and the Regional Committees for Medical and Health Research Ethics (REC) Southeast Norway (Ref 469-07066a1.2007.535, renewed in 2011). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
SS: Conceptualization, Data curation, Formal analysis, Methodology, Visualization, Writing – original draft, Writing – review & editing. MS: Funding acquisition, Project administration, Writing – review & editing. HG-A: Data curation, Investigation, Writing – review & editing. EK: Investigation, Writing – review & editing. SH: Data curation, Software, Writing – review & editing. PP: Funding acquisition, Investigation, Project administration, Writing – review & editing. PN: Funding acquisition, Project administration, Resources, Writing – review & editing. MT: Conceptualization, Funding acquisition, Project administration, Writing – review & editing. BV: Conceptualization, Funding acquisition, Project administration, Writing – review & editing. SN: Funding acquisition, Project administration, Writing – review & editing. AS: Methodology, Supervision, Writing – review & editing. MM: Conceptualization, Validation, Writing – review & editing. SG: Conceptualization, Funding acquisition, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing. EFK: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The research leading to these results has been funded by the European Research Council under the European Union’s Seventh Framework Program (PIRSES-GA-2010-269245), University of Copenhagen with the support from the Bill and Melinda Gates Foundation (grant #OPPGH5344), the Norwegian Research Council (grant #213702), the South-Eastern Regional Health Authority of Norway (grant #2014065), Oslo University Hospital, Norway and EU Horizon, European Health and Digital Executive Agency (HADEA), and project DUALSAVE-FGS (grant#101057853).
Acknowledgments
We sincerely thank the research team at BRIGHT: Silindile Gagai, Lars Holten, Roy Manyaira, Glory Kholeka Hlengwa, Nozipho Elizabeth Mkhabela, Nombeko Mpofana, Khuthala Elphina Khwela, and Thobeka Sylvia Sosibo for their hard work. We would also like to thank all the South African young women who participated in this study. We acknowledge Dr. Jaco J. Verweij and Eric A.T. Brienen for their contributions in performing the PCR analysis. The authors would also like to thank the DUALSAVE-FGS team for all valuable input.
Conflict of interest
Author SH was employed by the company Holmen Innovative Solutions AS.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
CAA, Circulating anodic antigen; FGS, Female genital schistosomiasis; GUS, Genital ulcer syndrome; HPV, Human papilloma virus; LCR, Ligase chain reaction; LAP, Lower abdominal pain; PCR, Polymerase chain reaction; S. haematobium, Schistosoma haematobium; STIs, Sexually transmitted infections; VDS, Vaginal discharge syndrome; WHO, World Health Organization.
References
1. Madden F. A case of bilharzia of the vagina. Lancet (British edition). (1899) 153:1716. doi: 10.1016/S0140-6736(01)51385-9
2. World Health Organisation (WHO). Female genital schistosomiasis. A pocket atlas for clinical health-care professionals Vol. 2015. Mbabazi PS, Vwalika B, Randrianasolo BS, Roald B, Ledzinski D, Olowookorun F, et al, editors. Geneva: WHO (2015). Available at: https://www.who.int/publications/i/item/9789241509299.
3. Renaud G, Devidas A, Develoux M, Iamothe F, Blanchi G. Prevalence of vaginal schistosomiasis caused by Schistosoma haematobium in an endemic village in Niger. Trans R Soc Trop Med Hyg. (1989) 83:797. doi: 10.1016/0035-9203(89)90333-7
4. Kjetland EF, Poggensee G, Helling-Giese G, Richter J, Sjaastad A, Chitsulo L, et al. Female genital schistosomiasis due to Schistosoma haematobium Clinical and parasitological findings in women in rural Malawi. Acta Trop. (1996) 62:239–55. doi: 10.1016/S0001-706X(96)00026-5
5. Kjetland EF, Gwanzura L, Ndhlovu PD, Mduluza T, Gomo E, Mason PR, et al. Simple clinical manifestations of genital Schistosoma haematobium infection in rural Zimbabwean women. Am J Trop Med hygiene. (2005) 72:311–9. doi: 10.4269/ajtmh.2005.72.311
6. Poggensee G, Kiwelu I, Weger V, Goppner D, Diedrich T, Krantz I, et al. Female genital schistosomiasis of the lower genital tract: prevalence and disease-associated morbidity in Northern Tanzania. J Infect Dis. (2000) 181:1210–3. doi: 10.1086/315345
7. World Health Organization (WHO). Schistosomiasis Fact Sheet (2023). Available online at: https://www.who.int/news-room/fact-sheets/detail/schistosomiasis.
8. UNAIDS, World Health Organization (WHO). No more neglect. Female genital schistosomiasis and HIV. Integrating reproductive health interventions to improve women’s lives. Geneva, Switzerland, UNAIDS/JC2979 (2019). Available at: https://www.unaids.org/sites/default/files/media_asset/female_genital_schistosomiasis_and_hiv_en.pdf.
9. Kjetland EF, Leutscher PDC, Ndhlovu PD. A review of female genital schistosomiasis. Trends Parasitol. (2012) 28:58–65. doi: 10.1016/j.pt.2011.10.008
10. Bustinduy AL, Randriansolo B, Sturt AS, Kayuni SA, Leustcher PDC, Webster BL, et al. An update on female and male genital schistosomiasis and a call to integrate efforts to escalate diagnosis, treatment and awareness in endemic and non-endemic settings: The time is now. Adv Parasitol. (2022) 115:1–44. doi: 10.1016/bs.apar.2021.12.003
11. Kjetland EF, Kurewa EN, Mduluza T, Midzi N, Gomo E, Friis H, et al. The first community-based report on the effect of genital Schistosoma haematobium infection on female fertility. Fertil Steril. (2010) 94:1551–3. doi: 10.1016/j.fertnstert.2009.12.050
12. Miller-Fellows SC, Howard L, Kramer R, Hildebrand V, Furin J, Mutuku FM, et al. Cross-sectional interview study of fertility, pregnancy, and urogenital schistosomiasis in coastal Kenya: Documented treatment in childhood is associated with reduced odds of subfertility among adult women. PLoS Negl Trop Dis. (2017) 11:e0006101–e0006101. doi: 10.1371/journal.pntd.0006101
13. Kjetland EF, Ndhlovu PD, Kurewa EN, Midzi N, Gomo E, Mduluza T, et al. Prevention of gynecologic contact bleeding and genital sandy patches by childhood anti-schistosomal treatment. Am J Trop Med Hyg. (2008) 79:79–83. doi: 10.4269/ajtmh.2008.79.79
14. World Health Organization. Female genital schistosomiasis: a pocket atlas for clinical health-care professionals. World Health Organization (2015). Available at: https://iris.who.int/handle/10665/180863.
15. Bosu WK. Syndromic management of sexually transmitted diseases: is it rational or scientific? Trop Med Int Health. (1999) 4:114–9. doi: 10.1046/j.1365-3156.1999.00360.x
16. Mabey D, Ndowa F, Latif A. What have we learned from sexually transmitted infection research in sub-Saharan Africa? Sex Transm Infect. (2010) 86:488–92. doi: 10.1136/sti.2009.041632
17. Eem L, Dubbink JH, Struthers HE, McIntyre JA, Ouburg S, Morré SA, et al. Evaluation of syndromic management guidelines for treatment of sexually transmitted infections in South African women. Trop Med Int Health. (2016) 21:1138–46. doi: 10.1111/tmi.12742
18. Zemouri C, Wi TE, Kiarie J, Seuc A, Mogasale V, Latif A, et al. The performance of the vaginal discharge syndromic management in treating vaginal and cervical infection: A systematic review and meta-analysis. PLoS One. (2016) 11:e0163365. doi: 10.1371/journal.pone.0163365
19. The National Department of Health South Africa. Primary Healthcare Standard Treatment Guideline and Essential Medicine List (2020). Available online at: https://www.kznhealth.gov.za/pharmacy/PHC-STG-2020.pdf.
20. Sturt A, Bristowe H, Webb E, Hansingo I, Phiri C, Mudenda M, et al. Visual diagnosis of female genital schistosomiasis in Zambian women from hand-held colposcopy: agreement of expert image review. Wellcome Open Res. (2023) 8:14. doi: 10.12688/wellcomeopenres
21. Kjetland EF, Norseth HM, Taylor M, Lillebø K, Kleppa E, Holmen SD, et al. Classification of the lesions observed in female genital schistosomiasis. International Journal of Gynecology and Obstetrics (2014) 127(3):227–228. doi: 10.1016/j.ijgo.2014.07.014
22. Galappaththi-Arachchige HN, Holmen S, Koukounari A, Kleppa E, Pillay P, Sebitloane M, et al. Evaluating diagnostic indicators of urogenital Schistosoma haematobium infection in young women: A cross sectional study in rural South Africa. PLoS One. (2018) 13. doi: 10.1371/journal.pone.0191459
23. Galappaththi-Arachchige HN, Zulu SG, Kleppa E, Lillebo K, Qvigstad E, Ndhlovu P, et al. Reproductive health problems in rural South African young women: Risk behaviour and risk factors. Reprod Health. (2018) 15. doi: 10.1186/s12978-018-0581-9
24. Shukla JD, Kleppa E, Holmen S, Ndhlovu PD, Mtshali A, Sebitloane M, et al. The association between female genital Schistosomiasis and other infections of the lower genital tract in adolescent girls and young women: A cross-sectional study in South Africa. J Low Genit Tract Dis. (2023) 27:291–6. doi: 10.1097/LGT.0000000000000756
25. Kleppa E, Ramsuran V, Zulu S, Karlsen GH, Bere A, Passmore JAS, et al. Effect of female genital schistosomiasis and anti-schistosomal treatment on monocytes, CD4 T-Cells and CCR5 expression in the female genital tract. PLoS One. (2014) 9:e98593. doi: 10.1371/journal.pone.0098593
26. Norseth HM, Ndhlovu PD, Kleppa E, Randrianasolo BS, Jourdan PM, Roald B, et al. The Colposcopic Atlas of Schistosomiasis in the Lower Female Genital Tract Based on Studies in Malawi, Zimbabwe, Madagascar and South Africa (2014). Available online at: http://www.scopus.com/inward/record.url?eid=2-s2.0-84920436432&partnerID=MN8TOARS.
27. Randrianasolo BS, Jourdan PM, Ravoniarimbinina P, Ramarokoto CE, Rakotomanana F, Ravaoalimalala VE, et al. Gynecological manifestations, histopathological findings, and schistosoma-specific polymerase chain reaction results among women with Schistosoma haematobium infection: a cross-sectional study in Madagascar. J Infect Dis. (2015) 212:275–84. doi: 10.1093/infdis/jiv035
28. Hegertun IEA, Sulheim Gundersen KM, Kleppa E, Zulu SG, Gundersen SG, Taylor M, et al. S. haematobium as a common cause of genital morbidity in girls: A cross-sectional study of children in South Africa. PLoS Negl Trop Dis. (2013) 7:e2104–4. doi: 10.1371/journal.pntd.0002104
29. Galappaththi-Arachchige HN, Hegertun IEA, Holmen S, Qvigstad E, Kleppa E, Sebitloane M, et al. Association of urogenital symptoms with history of water contact in young women in areas endemic for S. Haematobium. a cross-sectional study in rural South Africa. Int J Environ Res Public Health. (2016) 13:1135. doi: 10.3390/ijerph13111135
30. Wi TEC, Ndowa FJ, Ferreyra C, Kelly-Cirino C, Taylor MM, Toskin I, et al. Diagnosing sexually transmitted infections in resource-constrained settings: challenges and ways forward. J Int AIDS Soc. (2019) 22:e25343. doi: 10.1002/jia2.25343
31. Swai B, Poggensee G, Mtweve S, Krantz I. Female genital schistosomiasis as an evidence of a neglected cause for reproductive ill-health: A retrospective histopathological study from Tanzania. BMC Infect Dis. (2006) 6:134. doi: 10.1186/1471-2334-6-134
32. Downs JA, Dupnik KM, van Dam GJ, Urassa M, Lutonja P, Kornelis D, et al. Effects of schistosomiasis on susceptibility to HIV-1 infection and HIV-1 viral load at HIV-1 seroconversion: A nested case-control study. PLoS Negl Trop Dis. (2017) 11:1–15. doi: 10.1371/journal.pntd.0005968
33. Brodish PH, Singh K. Association between Schistosoma haematobium exposure and Human Immunodeficiency Virus infection among females in Mozambique. Am J Trop Med Hyg. (2016) 94:1040–4. doi: 10.4269/ajtmh.15-0652
34. Kjetland EF, Ndhlovu PD, Gomo E, Mduluza T, Midzi N, Gwanzura L, et al. Association between genital schistosomiasis and HIV in rural Zimbabwean women. New intervention points against HIV transmission? Harare, Zimbabwe: National Institute of Health Research Auditorium (2006). doi: 10.1097/01.aids.0000210614.45212.0a
35. Kjetland EF, Ndhlovu PD, Mduluza T, Deschoolmeester V, Midzi N, Gomo E, et al. The effects of genital schistosoma haematobium on human papillomavirus and the development of cervical neoplasia after five years in a Zimbabwean population. Eur J Gynaecol Oncol. (2010) 31(2):169–73.
36. Ross JM, Chacko MR M. Pelvic inflammatory disease: Clinical manifestations and diagnosis.UpToDate (2023). Available online at: https://www-uptodate-com.ezproxy.uio.no/contents/pelvic-inflammatory-disease-clinical-manifestations-and-diagnosis?search=pelvic%20inflammatory%20disease&topicRef=7580&source=see_link#H155838.
37. Geary RS, Gómez-Olivé FX, Kahn K, Tollman S, Norris SA. Barriers to and facilitators of the provision of a youth-friendly health services programme in rural South Africa. BMC Health Serv Res. (2014) 14:259. doi: 10.1186/1472-6963-14-259
38. Stupiansky NW, van der Pol B, Williams JA, Weaver B, Taylor SE, Fortenberry JD. The natural history of incident gonococcal infection in adolescent women. Sex Transm Dis. (2011) 38:750–4. doi: 10.1097/OLQ.0b013e31820ff9a4
39. Loh AJW, Ting EL, Wi TE, Mayaud P, Chow EPF, Santesso N, et al. The diagnostic accuracy of syndromic management for genital ulcer disease: A systematic review and meta-analysis. Front Med (Lausanne). (2022) 8:806605. doi: 10.3389/fmed.2021.806605
40. Ghanem KG, Tuddenham S. Screening for sexually transmitted infections. UpToDate (2022). Available at: https://www-uptodate-com.ezproxy.uio.no/contents/screening-for-sexually-transmitted-infections?search=Screening%20for%20sexually%20transmitted%20infections&source=search_result&selectedTitle=1%7E150&usage_type=default&display_rank=1.
Keywords: female genital schistosomiasis, genital infections, sexually transmitted infections, syndromic management protocols, schistosomiasis, praziquantel, neglected tropical diseases, low-and middle-income countries
Citation: Søfteland S, Sebitloane M, Galappaththi-Arachchige HN, Kleppa E, Holmen S, Pillay P, Ndhlovu PD, Taylor M, Vennervald BJ, Naidoo S, Staff AC, Makua M, Gundersen SG and Kjetland EF (2024) Diagnosis of female genital schistosomiasis and other genital infections in young South African women: challenges in the syndromic approach. Front. Trop. Dis 5:1379526. doi: 10.3389/fitd.2024.1379526
Received: 31 January 2024; Accepted: 19 March 2024;
Published: 09 April 2024.
Edited by:
Nilanjan Lodh, Marquette University, United StatesReviewed by:
Aldemir Branco de Oliveira Filho, Federal University of Pará, BrazilWilliam Evan Secor, Centers for Disease Control and Prevention (CDC), United States
Copyright © 2024 Søfteland, Sebitloane, Galappaththi-Arachchige, Kleppa, Holmen, Pillay, Ndhlovu, Taylor, Vennervald, Naidoo, Staff, Makua, Gundersen and Kjetland. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Solrun Søfteland, c29scnVuc29lQGdtYWlsLmNvbQ==