 Márcia Marcondes1
Márcia Marcondes1 Eduardo Brandão2Paula Oliveira2
Eduardo Brandão2Paula Oliveira2 Cristine Bonfim3Tereza Miranda4Heloísa Rodrigues5Cynthia Braga6Abraham Rocha2*
Cristine Bonfim3Tereza Miranda4Heloísa Rodrigues5Cynthia Braga6Abraham Rocha2*- 1Recife Municipal Health Department, State Department of Health of Pernambuco, Recife, Brazil
- 2National Reference Service in Filariasis, Department of Parasitology, Aggeu Magalhães Institute, Oswaldo Cruz Foundation, Recife, Brazil
- 3Social Research Department, Joaquim Nabuco Foundation, Recife, Brazil
- 4Olinda Municipal Health Department, State Department of Health of Pernambuco, Olinda, Brazil
- 5Federal Institute of Pernambuco, Recife, Brazil
- 6Department of Parasitology, Aggeu Magalhães Institute, Oswaldo Cruz Foundation, Recife, Brazil
Background: Lymphatic filariasis (LF) is a stigmatizing and debilitating disease that represents a significant global public health challenge. Information regarding the knowledge and practices of individuals with filarial morbidities is limited, and this understanding is crucial for the implementation of effective control strategies. This study aimed to investigate the knowledge and practices of individuals with filarial morbidity residing in two intervention areas of the Elimination Program in the city of Olinda, Brazil.
Methods: A cross-sectional study was carried out with residents who reported filarial morbidity in 2010, four years after the start of mass drug administration, in the intervention areas of the LF Elimination Program in the city of Olinda, Brazil. The knowledge and practices of patients with reported filarial morbidity in an endemic area were scrutinized using a semi-structured questionnaire to collect pertinent information. Data were analyzed utilizing the R language version 3.6.1.
Results: Filarial morbidity was reported in 338 patients. Dermatolymphangioadenitis emerged as the most frequently reported clinical form (50.9%). Mosquito bites were the most commonly cited form of transmission, accounting for 296 cases (87.6%). Approximately 80% (266) confirmed the adoption of prevention measures. Participants reported that the treatment involved the administration of medication. The existence of a cure for parasitosis was indicated by 212 subjects (62.7%).
Conclusions: Individuals with reported filarial morbidity exhibit varying levels of conceptions, knowledge, and practices regarding the disease, despite residing in an endemic area and receiving consistent visits from family health teams. Health services must identify shortcomings in this approach to minimize disparities, thereby enabling health education to effectively contribute to disease control and elimination in the municipality.
Introduction
Lymphatic filariasis (LF) is a neglected tropical parasitic disease caused by nematode helminths of the Wuchereria bancrofti and Brugia spp species. The disease is transmitted by the bite of different species of mosquitoes, mainly Anopheles in Africa and Culex in the Americas (1). It is estimated that around 882 million people are currently at risk of acquiring filarial infection because they live in 44 countries with active transmission. Approximately 36 million people remain with manifestations of chronic diseases. As part of the actions established by the Global Programme to Eliminate Lymphatic Filariasis (GPELF), the Mass Drug Administration (MDA) of around 9 billion doses has been performed since the beginning of the program, leading to a reduction in the number of infected people from 199 million in 2000 to 51 million in 2018 (1, 2).
Lymphatic filariasis is considered an important cause of physical disability because of its disfiguring and disabling sequelae (3) that lead to social stigmatization, reduced work opportunities (economic losses), and negatively affect the quality of life of those affected, in addition to increasing costs of health services (4). Filarial morbidity in chronic conditions most commonly leads to the development of swelling of the limbs (lymphedema or elephantiasis - acute dermatolymphangioadenitis—ADLA), testicles (hydrocele) and breasts. Other less commonly reported clinical expressions include swelling of the vulva and rheumatic and respiratory problems (5).
Considering the problem on a global scale, in 2000, the World Health Organization (WHO) launched the GPELF with the goal to eliminate LF by 2030 using strategies based on two main components: prevent the spread of infection through the large-scale annual treatment of all eligible people in an area or region where the infection is present; and alleviate the suffering caused by LF by providing the recommended essential package of care (2).
Faced with the challenge of ensuring the success of GPELF actions, the WHO draws attention to the importance of obtaining the knowledge, attitudes and practices (KAP) of the target population where the treatment intervention for a given endemic disease will be performed as a foundation for health promotion campaigns in the scope of public health (6, 7). Lack of knowledge about the disease and behavior of seeking to improve health conditions can improve or interfere with the effectiveness of control measures. Thus, feedback from the population regarding knowledge and practices on LF can greatly enhance the coordination of National Elimination Programs. The information obtained through this tool would greatly help the GPELF to direct the actions and procedures to be adopted in the communities for a better adherence of the population to disease control interventions. Furthermore, National Programs to eliminate LF involving the management and care of those with morbidity increase the population’s awareness about the disease and adherence to treatment (7).
In Brazil, LF is exclusively caused by W. bancrofti and transmitted by the Culex quinquefasciatus mosquito (8). Currently, the Recife Metropolitan Region, in the state of Pernambuco, is the remaining focus of LF in Brazil, and covers the cities of Recife, Olinda, Jaboatão dos Guararapes and Paulista (9, 10). The interventions to eliminate LF in these areas were implemented between 2003 and 2017 (11–13). Importantly, unlike most other LF-endemic countries, the Brazilian Ministry of Health decided to use only the single-dose diethylcarbamazine citrate (DEC) monotherapy for MDA, citing lack of evidence that DEC-albendazole coadministration was more effective than DEC alone (11, 14, 15). By 2018, these cities had halted MDA and implemented TAS 2 and TAS 3, during which no infected children were identified (15). Until the beginning of treatment implementation, there were no studies in Brazil evaluating knowledge and practices the KAP.
The goal of this study was to investigate the knowledge and practices of individuals with filarial morbidity residing in two intervention areas of the Elimination Program in the city of Olinda. The study data will contribute to improving strategic information, education and communication activities aimed at assisting patients in LF endemic areas.
Methods
Design and study area
A cross-sectional study was conducted with residents who reported filarial morbidity (RFM) in intervention areas of the LF Elimination Program in the municipality of Olinda, located in the Metropolitan Region of Recife, state of Pernambuco, Brazil. It encompasses a territorial area of 41,300km2 and is divided into 31 urban neighborhoods. As of 2022, the population was 349,976 inhabitants (16).
Actions to control LF transmission in the municipality commenced in 2005. Neighborhoods with microfilaremia prevalence exceeding 1% and a high socio-environmental risk of transmission were incorporated into the MDA. Treatment initiation took place in the Alto do Sol Nascente neighborhood, employing a door-to-door supervised treatment strategy that expanded across 17 neighborhoods (17–19). At the time, measures to identify and monitor morbidity cases had not yet been implemented in the municipality (20).
The study focused on the neighborhoods of Alto da Bondade and Alto da Conquista, characterized by a pre-MDA antigenemia prevalence of approximately 10% in schoolchildren who underwent MDA between 2007 and 2013, achieving treatment coverage exceeding 65% (18, 21). The inclusion criteria comprised patients with RFM (erysipelas-ADLA, lymphedema, elephantiasis, chyluria and hydrocele) identified and registered by Community Health Agents (CHA) during home visits conducted from 2007 and 2010 in all residences within the selected neighborhoods. The complaint of filarial morbidity was identified using a panel of representative images depicting various clinical manifestations related to filarial morbidity (22).
Data collection
Data collection took place in the months of April and May 2010, four years after the start of mass drug administration. Individual data concerning morbidity complaints were gathered using a semi-structured questionnaire adapted from the study with patients in Ghana (23). The questionnaire comprised both open-ended and multiple-choice questions. Information on interviewees’ knowledge regarding the transmission, diagnosis, treatment, and cure for lymphatic filariasis, as well as practices related to individual measures to prevent mosquito bites and combating the vector was collected.
Variables were categorized as follows: information about transmission, diagnosis, treatment, and cure, classified as adequate (good), regular and inadequate (insufficient). The diagnosis and cure variables included only two dimensions; adequate (good) or inadequate (insufficient). Variables related to the identification of practices in seeking service, avoiding mosquito bites and combating the vector were comparatively described by sex, age group, and literacy status.
Data analysis
The frequency distribution of individual characteristics and knowledge about filariasis in the study population were outlined. The association of categorical variables with the type of morbidity was made using Pearson’s Chi-square test. Descriptive levels were measured utilizing a Monte Carlo simulation with 10,000 replications, given that numerous cells in the contingency tables had values lower than 5.
Key questions pertaining to transmission, treatment, and protective measures, along with their relative frequencies, were considered in the knowledge measurement. The instrument for measuring knowledge about lymphatic filariasis (score) was developed through multiple correspondence analysis (MCA), utilizing the first dimension generated by the technique.
Multiple correspondence analysis is a multivariate statistical analysis technique facilitating dimensionality reduction for categorical data based on the association between the categories of analyzed variables (24). This reduction generates new variables (dimensions), representing linear combinations of weights assigned to each category of variables included. The application of MCA to variables yields dimensions to which the total variance of the original system is allocated in an ordinal manner, with dimension 1 having the highest quantity of general variance and dimension p having the smallest.
For an easier interpretation of the score, its scale was transformed to range from 0 to 100; 0 indicates high knowledge and 100 indicates low knowledge. The following formula was used to obtain the score on the new scale:
Knowledge groups were created utilizing the k-means segmentation algorithm with the elbow method employed to determine the optimal number of groups.
Subsequently, after establishing the knowledge score groups, the behavior concerning various variables was investigated. The sample used to generate the knowledge score did not contain missing values for any of the questions, ensuring a consistent number of observations for all analyzed variables.
All computations were conducted using the R language version 3.6.1, placing emphasis on the FactoMineR package version 2.0 to perform the MCA and the Rcompanion package version 2.3.25 for the permutation median comparison test. Monte Carlo simulations and all calculations involving randomness were performed with seed 17052020.
Ethical considerations
The interviews for the questionnaire application were conducted following the participants’ or their legal guardian’s authorization and the signing of the informed consent form. In the case of minors, the information was conveyed to parents or the legal guardian, who responded on their behalf. The study received approval from the Research Ethics Committee of the Centro de Pesquisas Aggeu Magalhães - CEP/CPqAM/FIOCRUZ under number CAAE 0054.0.000.095–09.
Results
In this study, 338 individuals (229 from the Alto da Bondade and 109 from Alto da Conquista) of both sexes with an average age of 51.2 years, ranging from 17 to 92 years, were interviewed. Table 1 provides the characterization of interviewees, where 170 (50.3%) were male, the majority identified as mixed race/brown skin color (136 or 40.2%) and 213 (63%) were literate. The most frequently reported clinical form was Acute Dermatolymphangioadenitis (ADLA or erysipelas) at 50.9%, followed by hydrocele at 34.0% and lymphedema at 14.2%, all reported in females.
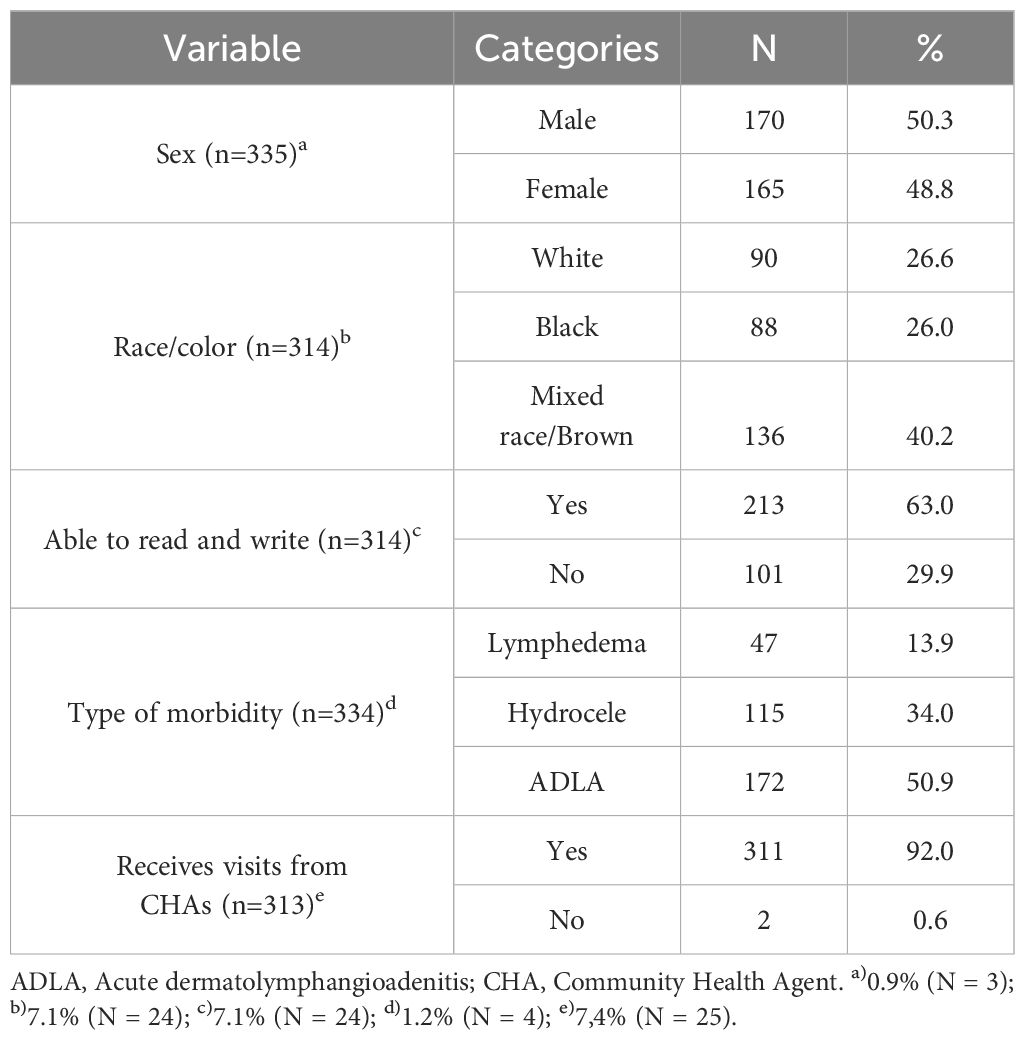
Table 1 Sociodemographic and health characteristics of respondents.
Knowledge of lymphatic filariasis
The primary mode of transmission reported by respondents was the mosquito bite, (296 or 87.6%). About 80% (266) adopted some preventive measure, the most common being the use of fans (244 or 91.7%). Concerning methods to prevent mosquito proliferation, care for the septic tank (292 or 86.4%) and the water tank (280 or 82.8%) predominated (Table 2). Regarding diagnosis, 292 (86.4%) respondents were aware that filariasis is diagnosed through a blood test (Table 2).
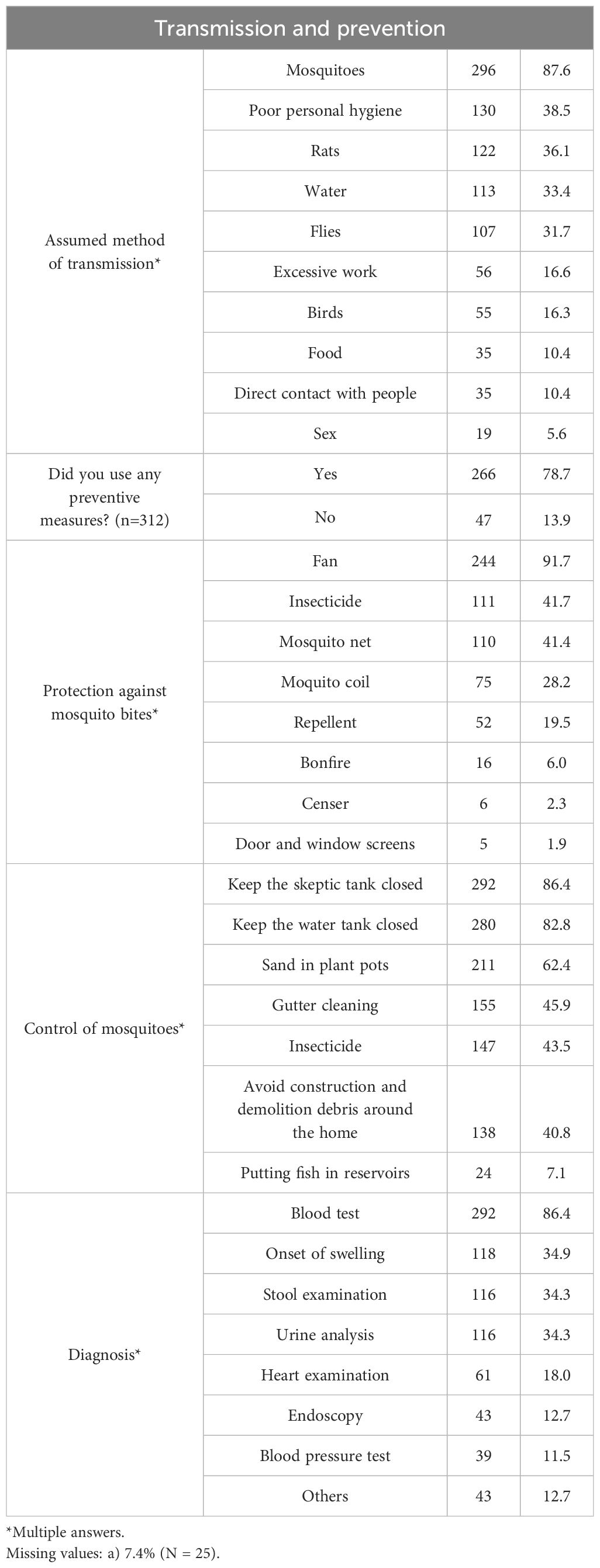
Table 2 Respondents’ knowledge with filarial morbidity in an endemic area in northeastern Brazil, about transmission and ways to prevent lymphatic filariasis.
The knowledge and practices of interviewees related to the treatment of filariasis are presented in Table 3. Of the interviewees, 125 (37.0%) stated that filariasis can be treated and for 119 (95.2%) of them, this treatment can be done with medication. The existence of a cure for the parasitosis was reported by 212 (62.7%) individuals. Approximately 60% (198) of respondents had already undergone treatment. Among those who did not undergo treatment, the main reason given was not being able to schedule an appointment (37 or 33.3%). When asked whether they had sought any health service, 46.7% (158) answered yes. Family health units (89 or 56.3%) and hospitals (87 or 55.1%) were the main health services mentioned. Almost 80% (126) followed the indicated treatment, which was prescribed by a physician (120 or 95.2%) and reported that the accessed health service was able to treat them (90 or 71.4%).
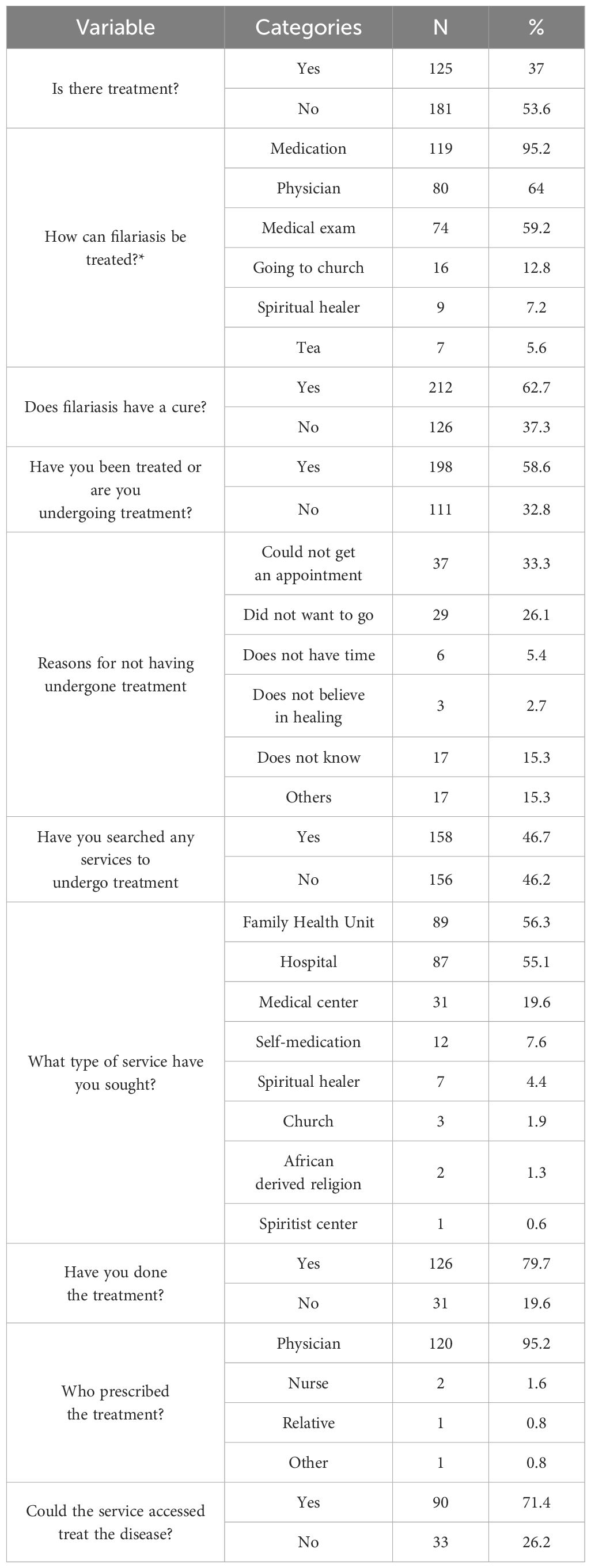
Table 3 Respondents’ knowledge and practices regarding the treatment of lymphatic filariasis.
Table 4 displays how the knowledge score was formulated, segmented into four groups. The positive weights surpassed negative weights. Questions yielding higher scores for obtaining a low score (indicating high knowledge) were related to awareness of preventive measures, treatment availability, medication usage, and preventive actions like cleaning drains. Conversely, questions leading to higher scores (indicating low knowledge) related to actions like keeping the septic tank closed and taking steps to avoid mosquito bites.
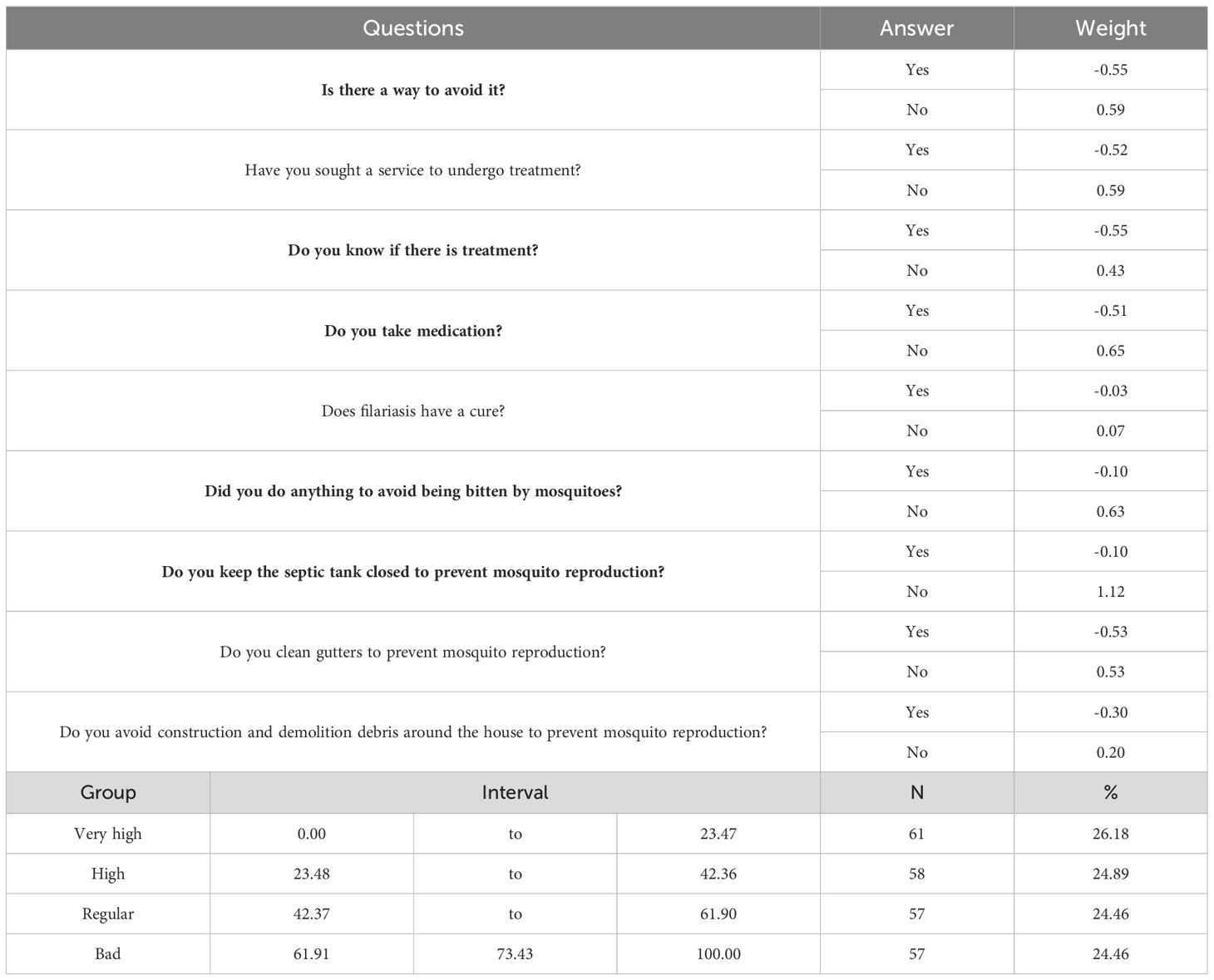
Table 4 Weights and questions relating to the knowledge score in conjunction with the score groups.
The concentration of individuals in knowledge group exhibited homogeneity in frequency distribution. However, the knowledge group categorized as “bad” was approximately twice as extensive as the other groups. A significant association was observed between the variables: “sex”, “literacy”, “morbidity”, and knowledge levels (Figure 1). Women outperformed in all knowledge groups. The morbidity variable also demonstrated a statistically significant association among different knowledge groups, suggesting a pattern where individuals with hydrocele are less likely to possess better knowledge, followed by those with lymphedema and ADLA. Additionally, respondents reporting ADLA displayed greater knowledge about filariasis (33.9%).
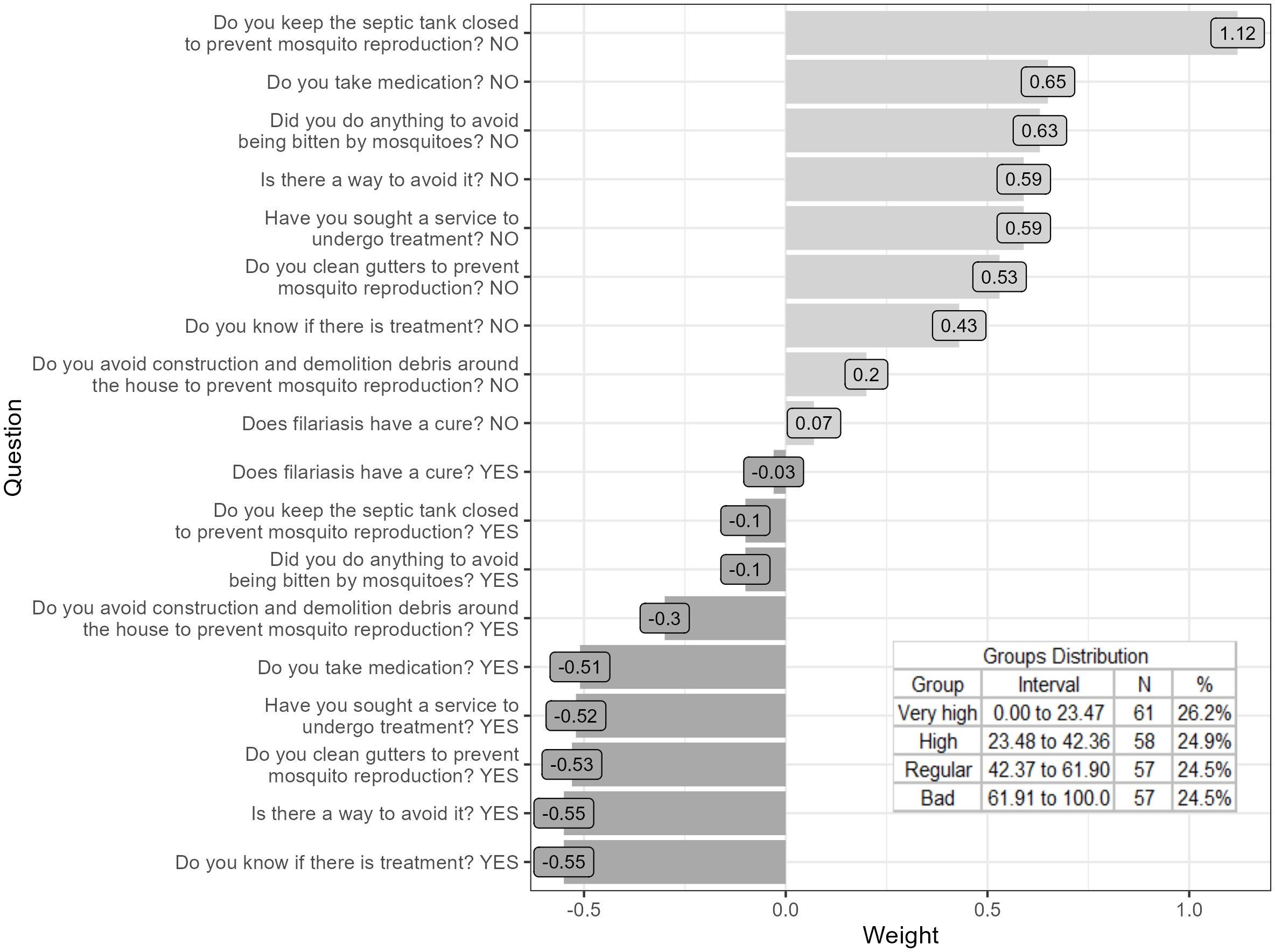
Figure 1 Association between knowledge about lymphatic filariasis, sociodemographic variables and morbidity, Olinda, Pernambuco, Brazil.
Discussion
The study demonstrated that individuals with RFM in an endemic area undergoing MDA in Brazil generally possess a good level of information about knowledge and practices related to the transmission, prevention, treatment, and diagnosis of LF. A subsequent study in the same study area supports these findings, since nearly all individuals recognized LF as a disease and associated it with chronic forms (21). This contrasts with studies conducted before MDA interventions, where individuals with clinical forms of FL often did not link them to filariasis, attributing them to heredity or supernatural factors, particularly “demonic spirits” (25–27).
In this study, hydrocele was the most frequently reported clinical form, differing from studies showing a higher frequency of lymphedema (27, 28). The prevalence of hydroceles was 2.45 times higher than reported lymphedema, aligning with the study by Machenzie and Mante in 2020 (29). These findings are significant for health services, as the psychosocial burden of hydrocele sufferers affects individuals, their family, and the community (28).
Regarding CHA visits, most interviewees reported receiving regular visits with CHA providing LF-related information. In many cases, these agents are acknowledged by community as “family members”, instilling confidence, and sometimes they even have free access to homes. However, the periodic home visits by CHA were not sufficient to significantly influence the participants’ knowledge levels about filariasis.
This study revealed that individuals with reported morbidity in the assessed areas had high understanding of how LF is transmitted. Most RFM in the present study knew that LF is transmitted through mosquito bites. Our findings align with some studies (26, 30, 31). The robust knowledge about LF transmission may result from the effective MDA coverage in the studied areas (21, 32). In contrast to these studies, a 2017 study in the same area reported that only 20% of those interviewed had knowledge about how LF is transmitted (21). Some other studies demonstrated the same (33, 34).
According to our findings, the majority of RFM used at least one means of protection to minimize or reduce human-mosquito contact. In our study the most cited means of protection were the fan, followed by insecticide and mosquito nets. However, a study in the Republic of Guinea (27) found an inverse order of the means of protection used by the population. This difference may be related to these populations’ access to electronic equipment, as purchasing power is linked to their way of life, and the fan is more expensive than the mosquito net. Another hypothesis would be related to the lack of recognition of ways to minimize contact with the mosquito, reflecting a lack of interest and knowledge of the disease’s implications (35).
In the present study, most interviewees (86.4% and 95.2%) knew that LF diagnosis involves a blood test, and its treatment typically includes medication, respectively. Furthermore, 62.7% believed in a cure, and 60.0% had already undergone treatment. In contrast to some studies, where 28.4% knew about the blood test for LF diagnosis and 96.1% were unaware of the treatment used for LF (30, 31), our study demonstrates higher awareness. Moreover, 80% of interviewees underwent treatment at the community’s primary health care facility, unlike other endemic areas where patients face challenges traveling long distances to reach the health centers, leading them to resort to healers in many situations (34).
Individuals with hydrocele exhibited the least knowledge about LF among the identified clinical forms. A study in Nepal aligns with this finding, as hydrocele sufferers often did not attribute this clinical form to LF, nor recognize the mosquito as the disease transmitter (36). The authors also highlight that most hydrocele sufferers attributed the development of this clinical form to exhaustive physical work and sexual activity outside of marriage. Conversely, ADLA patients, mostly women, demonstrated greater knowledge about LF. The enhanced knowledge of ADLA patients may result from women’s presence at home, receiving constant visits from CHA, and women’s increased health care-seeking behavior, especially during acute attacks when they receive health care and information about the disease.
Acute dermatolymphangioadenitis emerged as the most frequent complaint in the study, consistent with a morbidity report conducted in the municipality of Jaboatão dos Guararapes, Brazil (22). Similar results were observed in Haiti, particularly among women (14). The epidemiological association between the frequency/incidence of ADLA attacks serves as a sensitive indicator for the progression of lymphedema severity. A study by Dreyer and Addiss in 2000 in Brazil demonstrated that the management of lymphedema through hygiene, elevation of the affected limb, and treatment of interdigital lesions significantly reduces the frequency and duration of ADLA attacks (37). This was confirmed in a recent study, emphasizing the strong epidemiological association between repeated ADLA episodes and the progression of lymphedema, an important factor in disease progression (38). Consequently, it prevents the progression of lymphedema to severe forms (elephantiasis) and significantly improves the quality of life of patients with ADLA/lymphedema.
The National Filariasis Reference Service from the Oswaldo Cruz Foundation in Pernambuco, Brazil, emphasizes that in addition to the measures indicated by Dreyer and Addis 2000 to reduce ADLA episodes, continuous knowledge transmission about self-care is essential for individuals with ADLA/lymphedema. A recent study in Brazil during the COVID-19 pandemic observed that around 70% of patients evaluated reported maintaining daily hygiene of the limb affected by lymphedema. Despite this, there was a higher presence of interdigital lesions, dermal ulcers, and number of ADLA attacks, possibly contributing to an increase in lymphedema volume (39).
Simultaneously, this knowledge must be coupled with adequate management involving physiotherapy through the complex decongestive therapy (CDT) technique (40, 41). This therapy comprises procedures such as hygiene, manual lymphatic drainage, compressive bandages, myolymphokinetic exercises, skin care, and precautions in daily activities, and appears to induce behavioral changes in treated patients. Patients instructed in self-care, observing significant improvement through therapy, play a decisive role in maintaining treatment continuity. The authors also highlight that CDT can be applied with low-cost materials, such as cotton fabrics. In Haiti (42), however, the incidence of ADLA episodes increased when using compressive bandages (Comprilan®, commercially available) to reduce lymphedema of the lower limbs in LF-endemic areas, possibly due a lack of prior hygiene of the affected limbs before applying the compression bandage.
The study presents notable limitations that warrant consideration and should be addressed in future research. These include: I) CHAs were trained to identify the clinical forms of LF but did not classify the reported degree of lymphedema; II) Despite the clinical form of ADLA being frequently mentioned, individuals were not queried about the frequency of ADLA episodes nor about the presence of interdigital lesions; III) The referred morbidity was identified by the CHA, and IV) No survey was carried out to evaluate the impact of MDA on the clinical forms of LF.
One of the limitations in this study is the lack of specific questions related to the flow that individuals with filarial morbidity should follow to manage their clinical condition.
In conclusion, the population in areas that received actions from National Programs to Eliminate LF demonstrated a high level of knowledge about filariasis and practices aiding in the prevention and treatment of the disease. Furthermore, it has been demonstrated that National Programs to Eliminate LF involving the management and care of those with morbidity increase awareness about the disease in the population, thereby enhancing residents’ adherence to MDA. Given the high MDA coverage in the studied areas of AB and AC, despite periodic home visits from CHA, we believe their influence on individuals’ knowledge in the present study was limited. Evaluation of post-intervention MDA is crucial to infer the impact on improving the quality of life of those with morbidity by the reduction of acute inflammatory episodes (ADLA), lymphedema, and/or or hydrocele.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The study was approved by the Research Ethics Committee of the Centro de Pesquisas Aggeu Magalhães - CEP/CPqAM/FIOCRUZ under number CAAE 0054.0.000.095-09. The interviews for application of the questionnaire were performed after authorization by participants or their legal guardians and signature of the informed consent form. For minors, the information was transmitted to the parents or the legal guardian, who responded for them.
Author contributions
MM: Writing – original draft, Writing – review & editing. EB: Writing – original draft, Writing – review & editing. PO: Writing – original draft, Writing – review & editing. CBo: Writing – original draft, Writing – review & editing. TM: Writing – original draft. HR: Writing – review & editing. CBr: Writing – original draft, Writing – review & editing. AR: Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Serviço de Referência Nacional em Filarioses do Instituto Aggeu Magalhães/Fundação Oswaldo Cruz/Pernambuco was supported by the Sistema Nacional de Laboratórios de Saúde Pública (National System of Public Health Laboratories) (VPGDI-005-FIO-18).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Cromwell EA, Schmidt CA, Kwong KT, Pigott DM, Mupfasoni D, Biswas G, et al. The global distribution of lymphatic filariasis, 2000–18: a geospatial analysis. Lancet Glob Health. (2020) 8:e1186–94. doi: 10.1016/S2214–109X(20)30286–2
2. WHO. Facts 7 (2023). World Health Organization. Available online at: https://www.who.int/news-room/fact-sheets/detail/lymphatic-filariasis (Accessed September 12, 2023).
3. World Health Organization. Lymphatic filariasis: managing morbidity and preventing disability An aide-mémoire for national programme managers. Geneva: World Health Organization (2013).
4. Mathew CG, Bettis AA, Chu BK, English M, Ottesen EA, Bradley MH, et al. The health and economic burdens of lymphatic filariasis prior to mass drug administration programs. Clin Infect Dis. (2020) 70:2561–7. doi: 10.1093/cid/ciz671
5. Melrose WD. Lymphatic filariasis: New insights into an old disease. Int J Parasitol. (2002) 32:947–60. doi: 10.1016/S0020-7519(02)00062-0
6. Mathieu E, Lammie PJ, Radday J, Beach MJ, Streit T, Wendt J, et al. Factors associated with participation in a campaign of mass treatment against lymphatic filariasis, in Leogane, Haiti. Ann Trop Med Parasitol. (2004) 98:703–14. doi: 10.1179/000349804X3135
7. Addiss DG, Brady MA. Morbidity management in the global Programme to eliminate lymphatic Filariasis: a review of the scientific literature. Filaria J. (2007) 6:2–21. doi: 10.1186/1475-2883-6-2
8. Dreyer G, Pimentael A, Medeiros Z, Béliz F, Moura I, Coutinho A, et al. Studies on the periodicity and intravascular distribution of Wuchereria bancrofti microfilariae in paired samples of capillary and venous blood from Recife, Brazil. Trop Med Int Health. (1996) 1:264–72. doi: 10.1111/j.1365-3156.1996.tb00037.x
9. Pan American Health Organization. Fortalecimento da vigilância para alcançar e manter a eliminação da transmissão da filariose linfática e combater outras doenças infecciosas negligenciadas na Região das Américas. In: 16a. Reunião Regional de Gerentes do Programa para Eliminação da Filariose Linfática e 15°. Grupo Regional de Análise do Programa para Eliminação da Filariose Linfática. World Health Organization, Recife (2015).
10. Nascimento JB, Brandão E, da Silva FD, Bernart FD, Rocha A. The situation of lymphatic filariasis in the municipality of Paulista, Pernambuco, Brazil. Rev Patologia Tropical/Journal Trop Pathol. (2018) 47:1–8. doi: 10.5216/rpt.v47i4.56470
11. Fontes G, Rocha EMM, Scholteb RGC, Nicholls RS. Progress towards elimination of lymphatic filariasis in the Americas region. Int Health. (2021) 13:S33–8. doi: 10.1093/inthealth/ihaa048
12. Medeiros Z, Cesse EP, Menezes JA, Lessa F. Controle da filariose linfatica no Brasil, 1951 –2000. Epidemiol Serv Saude. (2003) 12:77–86. doi: 10.5123/S1679-49742003000200003
13. Fontes G, Leite AB, de Lima AR, Freitas H, Ehrenberg JP, da Rocha EM. Lymphatic filariasis in Brazil: epidemiological situation and outlook for elimination. Parasit Vectors. (2012) 26:272. doi: 10.1186/1756-3305-5-272
14. Addiss D, Gamble CL, Garner P, Gelband H, Ejere HOD, Critch-ley JA. Albendazole for lymphatic filariasis. Cochrane Database Syst Rev. (2005) 4:CD003753. doi: 10.1002/14651858.CD003753.pub3
15. World Health Organization. Global programme to eliminate lymphatic filariasis: progress report. Wkly Epidemiol Rec. (2019) 94:457–72.
16. Instituto Brasileiro de Geografia e Estatística (IBGE). Censo demográfico 2022: Características populacionais e domiciliares do município de Olinda (2022). Available online at: https://cidades.ibge.gov.br/brasil/pe/olinda/panorama (Accessed September 13, 2023).
17. Braga C, Ximenes RAA, Albuquerque MFPM, Souza WV, Miranda J, Brayner F, et al. Avaliação de indicador socioambiental utilizado no rastreamento de áreas de transmissão de filariose linfática em espaços urbanos. Cad Saúde Pública. (2001) 17:1211–8. doi: 10.1590/S0102-311X2001000500021
18. Rocha A, Marcondes M, Nunes JRV, Miranda T, Veiga J, Araújo P, et al. Programa de controle e eliminação da filariose linfática: uma parceria da Secretaria de Saúde de Olinda, PE, Brasil, com o Serviço de Referência Nacional em Filariose. Rev Patol Trop. (2010) 39:233–49. doi: 10.5216/rpt.v39i3.12215
19. Rocha A, Santos EM, Oliveira P, Brandão E. Histórico das ações de controle da filariose linfática em Olinda, Pernambuco, Brasil. Rev Patol Trop. (2016) 45:339–48. doi: 10.5216/rpt.v45i4.44603
20. Morais EA, Oliveira DSC, Cavalcanti FS, Da Silva JS, Lima RAF. Analysis ofthe economic cost ofcollective treatmentfor Iymphatic jilariasis in the city of Recife in 2007. Saúde em Debate. (2010) 34:129–36. doi: 10.11606/s1518-8787.2020054001649
21. Cabral S, Bonfim C, Oliveira R, Oliveira P, Guimarães T, Brandão E, et al. Knowledge, attitudes and perceptions regarding lymphatic filariasis: study on systematic noncompliance with mass drug administration. Rev do Instituto Medicina Trop São Paulo. (2017) 59:e23. doi: 10.1590/s1678-9946201759023
22. Netto MJ, Bonfim C, Brandão E, Aguiar-Santos AM, Medeiros Z. Burden of lymphatic filariasis morbidity in an area of low endemicity in Brazil. Acta Tropica. (2016) 163:54–60. doi: 10.1016/j.actatropica.2016.07.006
23. Gyapong M. Socio-Cultural Aspects of Lymphatic Filariasis and The Role of Communities in its Control in Ghana (2000). Universität Basel. Available online at: https://core.ac.uk/download/pdf/18233356.pdf (Accessed Octuber 15, 2010).
24. Ye T, Yi Y. Sample size calculations in clinical research Vol. 2017. Chow S-C, Shao J, Wang H, Lokhnygina Y, editors. New York: Taylor & Francis (2017). p. 510. pp.
25. Eberhard ML, Walker EM, Addis DG, Lammie PJ. A survey of knowledge, attitude, and perceptions (KAPs) of lymphatic filariasis, elephantiasis and hydrocele among residents in an endemic area in Haiti. Am J Trop Med Hygiene. (1996) 54:299–303. doi: 10.4269/ajtmh.1996.54.299
26. Rath K, Nayak AN, Babu BV. Community’s knowledge and perceptions about filarial elephantiasis and hydrocele in coastal Orissa, India. Asia Pac J Public Health. (2007) 19:28–33. doi: 10.1177/10105395070190010601
27. Kouassi BL, Barry A, Heitz-Tokpa K, Krauth SJ, Goépogui A, Baldé MS, et al. Perceptions, knowledge, attitudes and practices for the prevention and control of lymphatic filariasis in Conakry, Republic of Guinea. Acta Tropica. (2018) 179:109–16. doi: 10.1016/j.actatropica.2017.12.002
28. Eneanya OA, Garske T, Donnelly CA. The social, physical and economic impact of lymphedema and hydrocele: a matched cross-sectional study in rural Nigeria. BMC Infect Dis. (2019) 19:1–16. doi: 10.1186/s12879-019-3959-6
29. Mackenzie CD, Mante S. Caring for patients in the global programme to eliminate lymphatic filariasis. Int Health. (2020) 13:S48–54. doi: 10.1093/inthealth/ihaa080
30. Azzuwut MP, Sambo M, Hadejia I. Assessment of the knowledge, attitude and practices related to the treatment and prevention of lymphatic filariasis among the adult residents of Bokkos local government area of Plateau state, Nigeria. Jos J Med. (2012) 6:16–8.
31. Al-Abd NM, Nor ZM, Ahmed A, Al-Adhroey AH, Mansor M, Kassim M. Lymphatic filariasis in Peninsular Malaysia: a cross-sectional survey of the knowledge, attitudes, and practices of residents. Parasites Vectors. (2014) 7:1–9. doi: 10.1186/s13071-014-0545-z
32. da Silva JS, Braga C, Duarte FM, Oliveira P, Luna CF, Marcondes M, et al. Effectiveness of annual single doses of diethylcarbamazine citrate among bancroftian filariasis infected individuals in an endemic area under mass drug administration in Brazil. Pathog Global Health. (2018) 112:274–80. doi: 10.1080/20477724.2018.1498821
33. Adhikari RK, Sherchand JB, Mishra SR, Ranabhat K, Pokharel A, Devkota P, et al. Health-seeking behaviors and self-care practices of people with filarial lymphoedema in Nepal: a qualitative study. J Trop Med. (2015) 2015:1–6. doi: 10.1155/2015/260359
34. Maritim P, Silumbwe A, Zulu JM, Sichone G, Michelo C. Health beliefs and heath seeking behavior towards lymphatic filariasis morbidity management and disability prevention services in Luangwa district, Zambia: community and provider perspectives. PloS Negl Trop Dis. (2021) 15:1–14. doi: 10.1371/journal.pntd.0009075
35. Wynd S, Melrose WD, Durrheim DN, Carron J, Gyapong M. Understanding the community impact of lymphatic filariasis: a review of the sociocultural literature. Bull World Health Organ. (2007) 85:493–8. doi: 10.2471/BLT.00.000000
36. Lama Yonzon C, Padmawati RS, Subedi RK, Paudel S, Ghimire A, Murhandarwati EH. Exploring determinants of hydrocele surgery coverage related to Lymphatic Filariasis in Nepal: An implementation research study. PloS One. (2021) 16:e0244664. doi: 10.1371/journal.pone.0244664
37. Dreyer G, Addiss D. Hope clubs: new strategy for lymphatic filariasis endemic areas. Trans R Soc Trop Med Hyg Bull Trop Med Int Hlth. (2000) 8:1–8. doi: 10.1590/s0037-86822006000400009
38. Giovanella L, Martufi V, Ruiz Mendoza DC, Mendonça MH, Bousquat A, Aquino R, et al. The contribution of primary health care in the SUS network to face Covid-19. Saúde debate. (2020) 44:161–76. doi: 10.1590/0103–11042020E410
39. de Aquino LT, Aguiar-Santos AM, Rocha A, Coutinho AVA, do Nascimento MSB, Moretti EC, et al. The impact of the COVID-19 pandemic on people with lymphedema in an endemic area for lymphatic filariasis in Brazil. Int J Public Health. (2023) 68:1605317. doi: 10.3389/ijph.2023.1605317
40. Soares HPDS, Rocha A, Aguiar-Santos AM, Santos BDS, Melo CMLD. Andrade MDA Terapia complexa descongestiva com uso de material alternativo na redução e controle do linfedema em pacientes de área endêmica de filariose: um ensaio clínico. Fisioterapia e Pesquisa. (2016) 23:268–77. doi: 10.1590/1809-2950/15476523032016
41. da Silva LF, Souza OEV, Soares PSH, Siqueira SR, Roque SCCL, Aguiar-Santos A, et al. Use of complex descongestive therapy with low cost material in a patiente with lymphedema living in na endemic área for filariasis. Rev Patologia Trop. (2018) 47:55–66.
Keywords: knowledge, practices, lymphatic filariasis, morbidity, Brazil
Citation: Marcondes M, Brandão E, Oliveira P, Bonfim C, Miranda T, Rodrigues H, Braga C and Rocha A (2024) Knowledge and practices on lymphatic filariasis in patients with filarial morbidity in an endemic area in Northeastern Brazil. Front. Trop. Dis 5:1368589. doi: 10.3389/fitd.2024.1368589
Received: 12 January 2024; Accepted: 29 May 2024;
Published: 18 June 2024.
Edited by:
Nikhilesh Joardar, Washington University in St. Louis, United StatesReviewed by:
Robert Adamu Shey, University of Buea, CameroonJoseph Daniel Turner, Liverpool School of Tropical Medicine, United Kingdom
Copyright © 2024 Marcondes, Brandão, Oliveira, Bonfim, Miranda, Rodrigues, Braga and Rocha. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Abraham Rocha, YWJyYWhhbS5yb2NoYUBmaW9jcnV6LmJy