
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Trop. Dis. , 02 April 2024
Sec. Neglected Tropical Diseases
Volume 5 - 2024 | https://doi.org/10.3389/fitd.2024.1333862
This article is part of the Research Topic Female Genital Schistosomiasis: Research Needed to Raise Awareness and Deliver Action View all 14 articles
 Valencia J. Lambert1*†
Valencia J. Lambert1*† Anna Samson2†
Anna Samson2† Dunstan J. Matungwa3
Dunstan J. Matungwa3 Agnes L. Kosia4Rhoda Ndubani5Marriam Hussein6Khumbo Kalua6
Agnes L. Kosia4Rhoda Ndubani5Marriam Hussein6Khumbo Kalua6 Amaya Bustinduy7
Amaya Bustinduy7 Bonnie Webster8
Bonnie Webster8 Virginia A. Bond5,7
Virginia A. Bond5,7 Humphrey D. Mazigo9
Humphrey D. Mazigo9Objectives: Female Genital Schistosomiasis (FGS) causes gynecologic symptoms among women and girls living in sub-Saharan Africa. Despite continued efforts to raise awareness in communities about schistosomiasis, FGS remains poorly recognized. This study aimed to understand men’s knowledge and perceptions of FGS in northwestern Tanzania, and how this affects or can promote women’s uptake of FGS services.
Design and methods: We conducted a qualitative, formative survey called “Broad Brush Survey” (BBS) using 30 focus group discussions (FGDs) and 29 key informant interviews in five (5) districts across three regions in northwestern Tanzania. Participants were purposively selected in collaboration with village leaders and provided a written consent and/or assent to participate and be voice recorded. They included adolescent girls and boys (15-20 years), adult women and men (21-45 years), older women and men (≥46 years), village leaders (village chairpersons and executive officers), community health workers (CHWs), traditional healers, retail drug sellers, religious leaders, and opinion leaders (influential women and men). This analysis focuses and draws on 18 FGDs and 19 KIIs in which participants discussed or explained the importance and potential role of men in promoting FGS care.
Results: Most participants were not aware of FGS. Despite having adequate knowledge about urogenital schistosomiasis, they perceived FGS to be a sexually transmitted infection (STI). Three main themes emerged during analysis. First, most men reported perceiving women suffering from FGS as “promiscuous” or “unfaithful” due to misperceiving FGS as an STI. Such misperception could result in men ending a relationship. Second, participants reported that their engagement in FGS interventions would be critical to the interventions’ effectiveness because men often regulate women’s access to healthcare. Third, participants argued that men could be empowered through education to promote women’s uptake of FGS services. Finally, they argued that if men are educated about FGS like women, they can both work together in seeking care for FGS
Conclusion: Engaging men to address FGS holds potential to transform their negative perceptions of FGS. Further, participants described men’s potential to support and even advocate for women’s healthcare seeking when women experience symptoms that could be consistent with FGS. Including men more explicitly in FGS community education efforts could facilitate the provision of high-quality sexual and reproductive health care for women living in many communities where FGS is endemic but access to care is limited. We propose that public health interventions in such communities, which are often highly patriarchal, should leverage men’s positions within society by engaging them in promoting women’s health interventions. While we only interviewed participants from five (5) districts across three (3) regions, we are confident that their perceptions are reflective of many similar communities in Tanzania and beyond.
Female Genital Schistosomiasis (FGS) is complication of infection caused by Schistosoma haematobium (1, 2). In sub-Saharan Africa, approximately 56 million women and girls are estimated to have FGS (3–5). FGS is caused by the damaging effects of S. haematobium eggs in a woman’s reproductive organs including the vagina, uterus, cervix and fallopian tubes (2, 6). FGS transmission occurs through skin contact with cercariae-contaminated fresh water (6–8). Women and girls living in S. haematobium endemic areas can get infected with S. haematobium when they engage in water contact activities such as fetching water, washing dishes, washing clothes, and agriculture (2, 7). Women and girls suffering from FGS experience symptoms such as vaginal discharge and itching, bleeding or blood spots after sexual intercourse, genital and pelvic pain, bloody discharge and pain during or after sexual intercourse (7, 9, 10). Untreated FGS may lead to ectopic pregnancy, irregular menstrual period, infertility, spontaneous abortion, and pain during sexual intercourse. FGS also may increase the risk of contracting human immunodeficiency virus (HIV) and human papilloma virus (HPV) (2, 8–10).
Despite the high burden of FGS prevalence and morbidity in sub-Saharan Africa, FGS screening, treatment and prevention are not prioritized in many schistosomiasis endemic communities, including in Tanzania (8–11). For example, in mainland Tanzania, the neglected tropical diseases control program (NTDCP) that distributes Praziquantel for schistosomiasis control primarily targets school children while out-of-school girls and women are often left out (5, 7, 12). In addition, the probability of individuals seeking FGS treatment is lowered by inadequate understanding of FGS, its symptoms mimicking sexually transmitted infections (STIs), social stigma, and lack of men’s involvement in supporting women and girls for treatment-seeking (12, 13). However, based on the health consequences of FGS and the challenges that hinder access to FGS treatment, prevention and care, some studies have advocated for an integrated approach by integrating FGS services with sexual and reproductive health (SRH) services in primary health care, instead of focusing on FGS as a single disease (14, 15). The integrated approach can be important in a low-resource settings like Tanzania, as it offers the opportunity to use the available resources to reach, as well, women and girls with FGS (16).
There is evidence showing the importance of integrating family planning, STIs and maternal and child health with SRH services (15). Some studies have cited the importance of integrating STI’s services such as HIV and SRH to include improving access to HIV testing services, prevention and care, combating stigma and symptoms of STIs, as well as better and effective use of scarce resources for health (15). Others have mentioned non-stigmatized services, ongoing capacity building among health care workers (HCWs), positive attitude and good customer care among HCWs, and involvement of male partners as factors that can promote linkage between SRH services (17). Currently, the importance of involving men in SRH interventions and programs is well-recognized around the world (18–20). Several studies show that men’s participation in SRH interventions and programs will help them in taking care of their health and understand their roles and responsibilities in improving the health of women and girls, including their partners (21).
In FGS-endemic areas, the views of different stakeholders—including men themselves—on the potential roles of men in FGS care is understudied. Obtaining views of different stakeholders on the potential roles of men in promoting FGS prevention, control, and treatment-seeking on the one hand and men’s perception regarding FGS-related symptoms and social stigma toward women and girls suffering from FGS on the other is unique and not commonly done in FGS and urogenital schistosomiasis prevention and control programs. This paper draws on the analysis of a qualitative, formative survey called “Broad Brush Survey” (BBS) that was conducted in mainland Tanzania, Malawi, and Zambia to inform FGS community education design and delivery. However, the analysis presented here focuses only on the BBS conducted in mainland Tanzania and examines the participants’ views on men’s willingness to participate in FGS interventions and the roles they would play in promoting care for FGS. The findings of this analysis are significant in two notable ways. First, they will help in understanding how men’s participation in FGS and urogenital schistosomiasis prevention and control interventions can promote and improve FGS treatment-seeking among women and girls. Second, they will provide input and guidance to the authorities involved in planning and implementing FGS and urogenital schistosomiasis prevention and control programs and other SRH sexual and reproductive health programs.
In mainland Tanzania, BBS was conducted at Itilima district, in Simiyu region, from September 2020 to February 2021 using focus group discussions (FGDs) and key informant interviews (KIIs) (22–24). Additional funding was secured to adapt BBS by conducting cross-sectional FGDs and KIIs in four additional districts in two neighboring regions and evaluate the impact of the FGS community education intervention that was informed by BBS and implemented in Itilima district. Additional districts were where FGDs and KIIs were conducted are Maswa and Shinyanga Rural in Shinyanga region as well as Misungwi and Kwimba in Mwanza region in northwestern Tanzania. When selecting these five (5) districts as study sites, the Tanzanian research team relied on two key factors. First, most inhabitants in these districts rely on open sources of water such as Lake Victoria, rivers, marshes, swamps, and ponds. Second, data from the districts’ neglected tropical diseases (NTD) coordinators showed that these districts had some of the highest burden of S. haematobium infection compared to the other neighboring districts in the Lake Zone and across Tanzania. As such, residents of these districts are more vulnerable to S. Haematobium infection than other places in Tanzania. In other terms, there is a high risk of S. Haematobium transmission and infection in these districts. In both the formative multi-country study and the Tanzanian specific study, the issue of men’s potential role in the promotion of care for FGS emerged.
The regions and districts where this study was conducted are ethnically homogenous with the Sukuma as the dominant ethnic group. The Sukuma are both patriarchal and patrilocal (that is, after marriage, women relocate to their husband’s home where the couple then lives. As such, the gender norms and values that govern these communities put men in dominant social positions of power compared to women who occupy subordinate social positions. This gender arrangement influences many aspects of women’s lives including the decisions on their health, specifically their reproductive health (25–27).
Participants were purposively selected in collaboration with village leaders. Inclusion criteria were permanent residence in the study village, age (≥15 years), social or political position within the community, and willingness to provide a written informed consent, parental consent, and assent for both participation and being voice recorded in the FGD or KII. Those who did not meet these criteria were excluded from participation. The BBS recruited adolescent boys (15-20 years), adolescent girls (15-20 years), adult women (21-45 years), adult men (21-45 years), older men (≥46 years), older women (≥46 years), and opinion leaders to participate in FGDs. We included adolescent boys and girls in the sample because Tanzania experiences a high prevalence of both early sexual debut (having had first sexual intercourse at or before age 14 years of age) and child marriage (marriage before age 18 years) (28, 29). Opinion leaders included participants that were well known in the community and had influence over different community affairs despite not holding any religious, medical, or government position or title. Village chairpersons, village executive officers (VEOs), community health workers (CHWs), traditional healers, retail drug sellers, religious leaders, and some opinion leaders were invited to participate in KIIs (30).
The BBS data were collected using FGDs and KIIs. Each FGD was conducted by three trained research assistants, each of whom served as either the moderator, the note taker, or the person digitally recording the interview. Moderators and interviewers used a guide with open-ended questions that had been previously pilot-tested. Each KII was conducted by a trained research assistant who was served as interviewer. All the FGDs and KIIs were conducted in a private and quiet area within the community. They were conducted in Kiswahili, Tanzania’s national language, spoken by most people across different ethnic groups. A total of 30 FGDs and 29 KIIs were conducted in all five (5) districts (Tables 1, 2) (30).
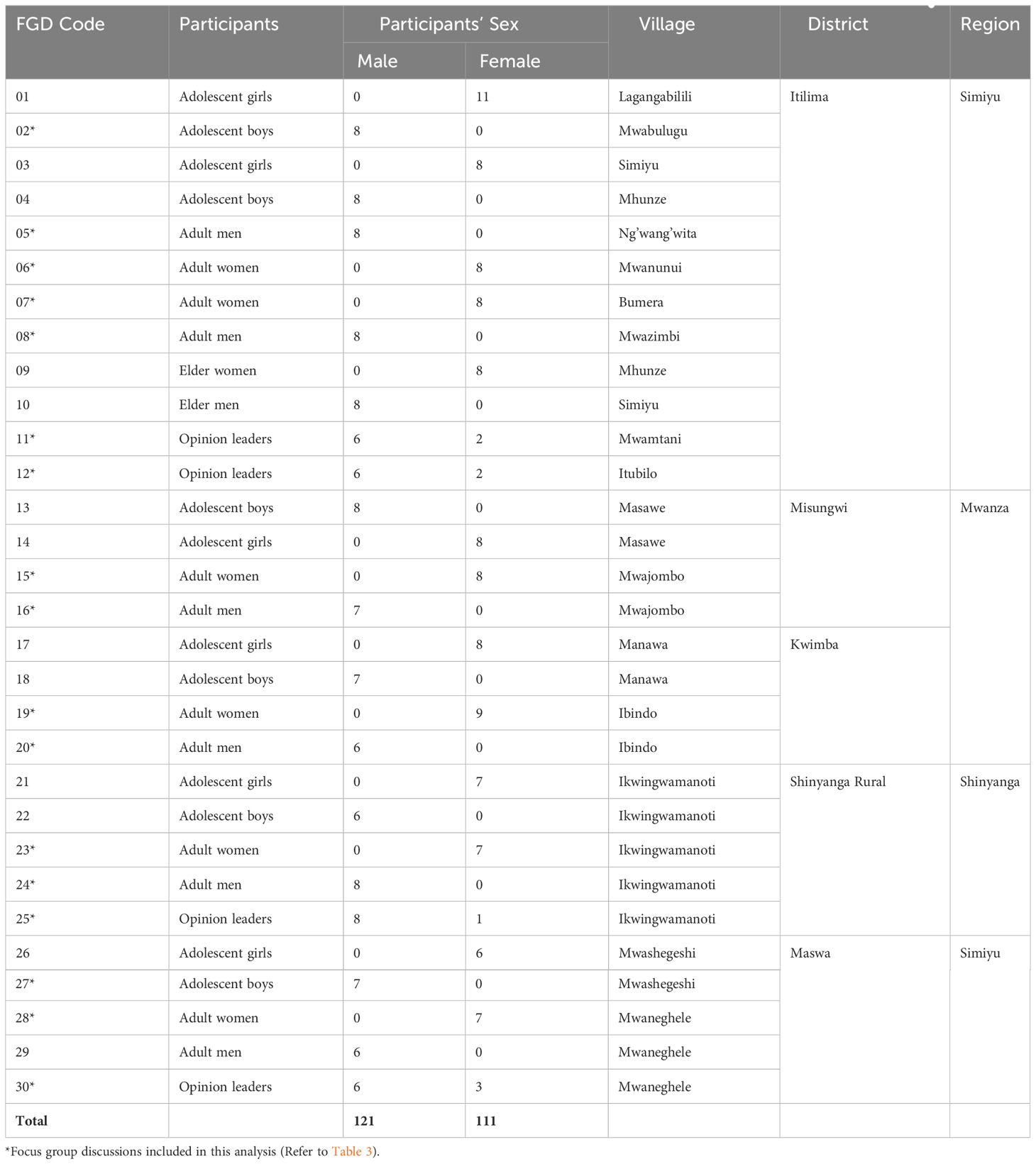
Table 1 A list of the Broad Brush Survey (BBS) focus group discussions.

Table 2 A list of Broad Brush Survey (BBS) key informant interviews.
Digitally recorded audio interviews were transcribed verbatim by experienced research assistants. Four members of the study team (VL, AS, AK, and DM) read several transcripts, reviewed field notes, reflected on their field experience, and suggested the main themes and sub-themes of the analysis—all pertaining to the potential role of men in the promotion of care for FGS. The study team agreed on the final themes and sub-themes, which were then compiled into a codebook. The codebook was further modified throughout the analysis process to include in vivo codes (31). Two investigators (VL and AS) fluent in both Kiswahili and English, coded 59 Kiswahili transcripts (30 FGDs and 29 KIIs) with the aid of NVivo version 12 and translated relevant quotes. After data coding, information on the role of men in FGS care were found in 37 transcripts, that is, 18 FGDs and 19 KIIs (Tables 3, 4). Thus, the analysis focused on these 18 FGDs and 19 KIIs in which participants discussed or explained what they thought could be the role of men in promoting FGS care and the underlying reasons for their thoughts. Lastly, the codes were grouped into overarching themes with supporting quotations to highlight major findings.
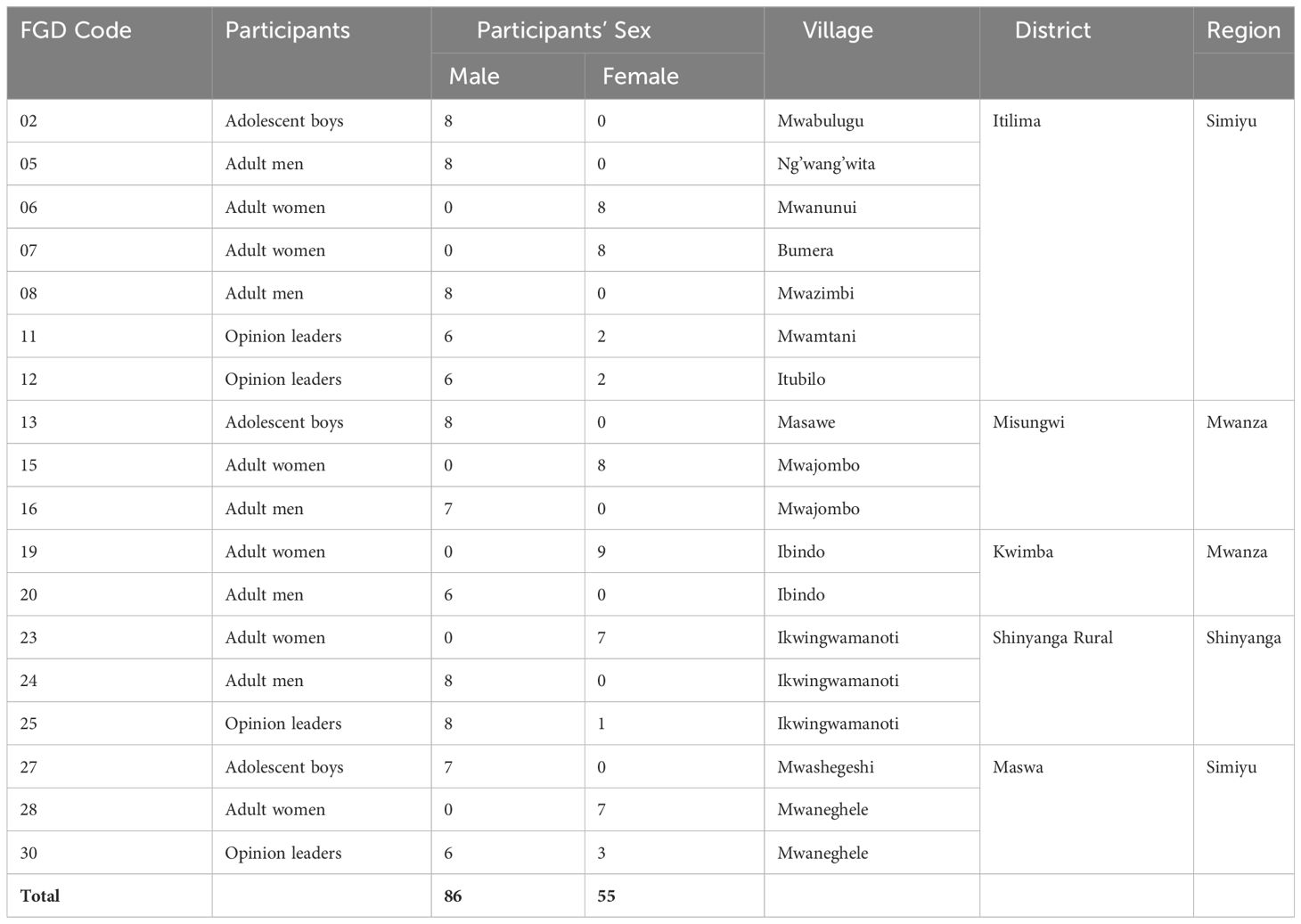
Table 3 A list of focus group discussions included in this analysis .

Table 4 A list of key informant interviews included in this analysis.
Four themes emerged during the analysis. First, men frequently perceived women suffering from FGS as being “promiscuous” or “unfaithful.” This theme explores community-shared misperceptions (of FGS) and how women suffering from FGS are discriminated against. Second, men’s inclusion in FGS interventions is vital. This theme focuses on the role of men as heads of households and the fact that men can be empowered to be educators and promoters of FGS treatment-seeking. Third, men can be empowered to promote uptake of FGS services. This theme focuses on men’s readiness to be educated about FGS, and the fact that educated men can better support their partners. Finally, if men are educated about FGS like women, they can both work together in seeking care for FGS
Two sub-themes emerged when participants described how FGS is transmitted. First, misconceptions of how FGS is transmitted influenced how men perceived women suffering from FGS and their reactions to a hypothetical scenario of their partners suffering from the same disease. Second, men described instances of community discrimination against women suffering from FGS that are directly influenced by these misperceptions.
The majority of participants stated that they had never heard of FGS but were aware of schistosomiasis. Furthermore, of those that were not aware of FGS, a majority of them perceived FGS as being sexually transmitted, with only a handful stating that FGS is transmitted via the same routes as schistosomiasis. For example, when asked if a woman can transmit FGS to another person or their sexual partner, one adult man in an FGD stated that:
Eh, a woman suffering from schistosomiasis can transmit the disease to a man because when they are having sexual intercourse and there is friction, schistosomiasis parasites can be transmitted through the blood. And so, the man too can be infected. (FGD 16, adult men, Mwajombo village).
Additionally, participants reported that most men do not know that FGS is a possibility when a woman has genital symptoms and therefore assume women have STIs.
The problem is that schistosomiasis is associated with STIs. It means that when a young adult woman is suffering from schistosomiasis, they [people] will not know if it is schistosomiasis, syphilis or gonorrhea [ … ] because schistosomiasis is like a forgotten disease. They will associate it with STIs. They will not think it is schistosomiasis. (KII 23, Influential man, Ikwingwamanoti village).
Others took this perception—of FGS being an STI—further, explaining that this could lead to men perceiving married women suffering from FGS as being “unfaithful” in sexual relationships including marriage:
“Even her husband might say that she was in an extramarital relationship. He might ask where did you get this infection from?” (KII 22, VEO).
Some of the female participants expressed similar opinions and went further to show how such misperceptions by men can even lead to intimate partner violence. One female participant described how misperceptions of FGS, accusations of unfaithfulness in marriage, and intimate partner violence are linked.
[ … ] he will ask her to sit down and ask her questions like, ‘Where did you get this disease because I do not have it myself?’, ‘Where did you get it?’, ‘Maybe you went somewhere else [had a sexual affair with another man] and brought this illness. Please tell me. How did you get it?’ He might even hit her [ … ] with the intention of making her speak out while in fact she does not know where the illness came from. But FGS is a disease that is not sexually transmitted. (FGD 06, adult women, Mwanunui village).
Others participants extended these perceptions to unmarried women as well, saying that
“our society might perceive a young adult woman who is suffering from FGS as being ‘promiscuous’…” (KII 05, VEO).
While reacting to a hypothetical scenario of their partners suffering from FGS, majority of men participating in this study reported that men would neglect or discriminate against their sexual partner if she was experiencing genital symptoms. A pastor described that a girl suffering from FGS would be at risk of being dumped by their partner, if the latter would observe the symptoms displayed by her girlfriend.
Her boyfriend might break up with her [ … ] He might say that she is not suffering from schistosomiasis and instead is suffering from an STI. [The boyfriend might think that] she will kill me [by sexually transmitting the STI to him]. (KII 15, Pastor).
Another adult man explained that because the society is unaware of FGS,
“when many people find out that their sexual partner has that disease, they end the relationship.” (FGD 08, adult men, Mwazimbi village).
Further, women affected with long-term consequences of FGS such as infertility were at risk of being abandoned by their husbands:
A family is not a family without children. The husband and the wife might separate [because of not having a child]. The husband and the wife can break up and each can find someone else whom they can have children with. Therefore, [FGS] causes family problems … even though it is something that is treatable. It can cause problems to a person who does not seek medical services early enough. (FGD 13, adolescent boys, Masawe village).
Men stated that it is essential to include men in FGS interventions because of their social standing in their communities (and families), which are often highly patriarchal. In addition, in these communities, men are more often educated than women and likely more knowledgeable than are their counterparts.
Men need to be included in FGS education interventions for several reasons. First, men have the decision-making authority in many households, including about what their wives do and where they go during the day.
There is the patriarchal system in which you cannot just go to a place and invite women (to participate in an intervention). The woman can come one day, and the next day she is forbidden to go and receive those services. She gets educated, but at home, she is told not to go. However, if you include men, they will know what is happening and the benefits [of the intervention]. I think it will be very good if men are included. (FGD 11, opinion leaders, Mwamtani village).
I find it important to involve men [in FGS interventions] because there are some men who are the head of the family and do not allow their wives to go out [to certain places]. Therefore, in order to make it easier for women, men should also be educated to allow their wives to access such services [FGS services]. (FGD 07, adult women, Bumera village).
Secondly, men who participated in this study stated that they could advocate for FGS screening and lead the family, as the head of the household, to receive care for FGS:
“Because a man is the head of the household and so he must be included [in the education seminar] so that he can encourage the family to go to the hospital.” (FGD 24, adult men, Ikwingwamanoti village). Additionally, all female and male
participants in the FGDs supported the inclusion of men in FGS interventions because
“men in our community, [ … ] are the ones who have a voice. When they say something, they are immediately listened to.” (FGD 30, popular people, Mwaneghele village)
Furthermore, they stated that it is important to include men because
“sometimes there are some expenses that the family might have to cover [ … ]. If the man knows [about FGS), it can be easier to take his wife to the health center [for FGS services].” (FGD 25, Opinion leaders, Ikwingwamanoti village)
Furthermore, an adolescent boy stated that it is important that they are included in FGS interventions because
“sometimes the man may easily understand [when taught]” so that in situations in which women did not understand well, “he can educate his wife about what he learnt…” (FGD 02, adolescent boys, Mwabulugu village)
A sheikh agreed, stating that if the husband and wife both receive education about FGS, but the woman is unclear about what was taught,
“[then] the partner [husband] who also attended [the seminar] and understood [what was taught]can share the information so that they both understand [what was taught].” (KII 29, Sheikh)
Male participants stated that they were eager and ready to be educated about FGS in order to better support their partners and encourage them to seek medical help when experiencing FGS symptoms. They requested FGS interventions to include both men and women in order to promote the uptake of FGS services.
In addition to their expressed desire to participate in FGS interventions, a majority of men stated that both men and women in their communities would be eager to learn about FGS:
I would like to ask for an effective intervention in the near future because currently we, the people present here, have been motivated a little bit. We are happy if this [intervention] is brought to us. I want to ask that you do not take a lot of time to come back. Please come back and educate people about schistosomiasis [ … ]. (FGD 05, adult men, Ng’wang’wita village).
Some men, particularly adolescent boys, noted the need for such an intervention urgently in order to prevent long-term side effects that consequently affect intimate relationships and the community as a whole:
“Can you please educate us soon so that we can know how to prevent ourselves [from this disease] so that it does not cause major side effects in our society.” (FGD 13, adolescent boys, Masawe village).
Lastly, both male and female participants reported that if men were equipped with adequate education about FGS, they would be able to better support their partners and advise them to seek medical care early to prevent them from long lasting side effects of FGS such as ectopic pregnancy and infertility.
It is important to involve men in this exercise [FGS education intervention]. It is very crucial for them to participate in these activities [FGS education interventions]. They will know the effects of this disease [FGS] such as ectopic pregnancy and infertility. They will know how this disease [FGS] is very dangerous. They will then support us like permitting us to go for screening and treatment [ … ].” (FGD 28, adult women, Mwaneghele village).
[ … ] if men are educated about FGS they can tell their partners [women] to go for a checkup at the hospital instead of prohibiting them [from seeking medical help]. (FGD 27, adolescent boys, Mwashegeshi village).
Sometimes we do not do what is right for women. She says she is ill, but you only think of going to work. You tell her, ‘let us go to the farm.’ You perceive her illness as a just common illness. So, men should be educated about this disease [FGS] so that they can take their partners to the health facilities display symptoms [of FGS] or whenever they are ill. (FGD 25, Opinion leaders, Ikwingwamanoti village).
Study participants also reported that seeking care for FGS and other gynecological problems is not the responsibility of women only, but rather the responsibility of both women and men (or husbands and their wives). They emphasized that educating men about FGS is beneficial to both men and women because they can figure out how and where to seek for treatment together. They also emphasized that when a woman is unwell or when she is suffering from any disease including FGS, it becomes a concern for both the husband and wife, not solely the woman. As such treatment-seeking should also be responsibility of both husband and wife; not women alone. As one participant summed up this argument,
“[ … ] if a woman is ill, the man is also affected and has to take care of his partner’s health” (KII 27, Village chairperson)
Thus, educating men about FGS will enhance the collaboration between the husband and wife in seeking treatment.
[ … ] when the woman has forgotten about the symptoms [of FGS]; the man can remind her. Therefore, when the man is also educated, they [husband and wife] can work together and support each other throughout her treatment. (FGD 16, adult men, Mwajombo village)
Yes, it is important to involve men [in FGS interventions] because it affects them directly. If your wife is suffering from this disease [FGS] and she informs you [about the symptoms she is observing], if you have also been educated about this matter you can go together to the health center [for FGS services]. (FGD 23, adult women, Ikwingwamanoti village).
Our findings illustrate the fact that despite having little knowledge about and possessing negative perceptions of FGS, men in northwestern Tanzania were eager and willing to learn about this disease in order to better support their partners in the process of treatment seeking. We hypothesize that the transformative effects of engaging and including men in FGS education and treatment seeking would be a meaningful way to improve women’s access to both FGS and other SRH services particularly in communities where FGS is endemic and access to care is limited.
Male involvement in women’s health has been documented in numerous studies as an effective strategy to promote maternal and family health and increase the uptake of maternal and child services (18, 21, 32–35). Additionally, since men often are the primary decision makers within Tanzanian families as the head of the household, they can either act as barriers or enablers to women seeking health care services (25–27, 35, 36). Therefore, it is imperative to leverage men’s positions within these patriarchal societies by engaging men in FGS interventions in order to increase the interventions’ effectiveness and uptake.
As the study findings show, men’s inclusion in FGS interventions was supported by both male and female participants who participated in the FGDs and KII included in this analysis. In particular, all female participants supported the inclusion of men in FGS educational seminars because men are often the main breadwinners and primary decision makers in most Tanzanian households. As such, they have influence on women’s uptake of FGS services. As some studies have shown, men’s financial and decision-making power influences the way in which women access and use SRH services, including family planning (25–27, 35, 36). Furthermore, female participants also emphasized that when men are educated about FGS, it will be easier for women to confide in their partners when experiencing FGS symptoms. Finally, men reported that they are eager and willing to be educated about FGS in order to better support their partners and promote the uptake of FGS services and treatment within their households and communities. Indeed, as study participants noted, it is important to have both women and men be educated about FGS because women’s health is not their personal matter but a matter that involves men and the entire family.
This study was conducted with a purposively selected sample of participants in five (5) districts in three (3) regions of northwestern Tanzania. However, we are confident that these findings are transferrable to many similar communities in Tanzania and beyond. Engaging men in FGS interventions has the potential to transform men’s negative perceptions of FGS and make them change agents. Thus, involving men in FGS community education programs will improve uptake of FGS services and facilitate the provision of high-quality SRH services for women and girls living in many poor communities where FGS is endemic but access to care is limited. We propose that public health interventions in such communities, which are often highly patriarchal, should leverage men’s positions within society by engaging them in learning about women’s health challenges and promoting women’s health interventions.
The datasets presented in this article are not readily available because the data supporting the conclusions of this article are not publicly available because they contain information that could compromise the privacy or research participants. Requests to access the datasets should be directed to Directorate of Research and Publications of the Catholic University of Health and Allied Sciences (CUHAS),dmNAYnVnYW5kby5hYy50eg==.
The studies involving humans were approved by Tanzanian Lake Zone Institutional Review Board (MR/53/100/649) and Weill Cornell Medicine (certificate number 20-07022381). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin. The participants provided their written informed consent to participate in this study.
VL: Data curation, Formal analysis, Investigation, Writing – original draft, Writing – review & editing. AS: Data curation, Formal analysis, Investigation, Writing – original draft, Writing – review & editing. DM: Data curation, Formal analysis, Investigation, Writing – review & editing. AK: Data curation, Formal analysis, Investigation, Writing – review & editing. RN: Writing – review & editing. MH: Writing – review & editing. KK: Conceptualization, Funding acquisition, Methodology, Project administration, Supervision, Writing – review & editing. AB: Conceptualization, Methodology, Writing – review & editing. BW: Conceptualization, Methodology, Writing – review & editing. VB: Conceptualization, Formal analysis, Funding acquisition, Methodology, Project administration, Supervision, Writing – review & editing. HM: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Writing –review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work received financial support from the Coalition for Operational Research on Neglected Tropical Diseases, which is funded at The Task Force for Global Health primarily by the Bill & Melinda Gates Foundation, by the United States Agency for International Development through its Neglected Tropical Diseases Program, and with the UK AID from the UK Government. Specifically, this project was made possible through the support of UK AID Department for International Development (DFID) through the Task Force for Global Health and UK Foreign Commonwealth and Development OLice (FCDO) and through the Accelerating the Sustainable Control and Elimination of Neglected Tropical Diseases (ASCEND) program (FCDO grant number PO-8374). The opinions expressed in this publication are those of the authors and do not necessarily reflect the views of DFID.
We thank the UK AID Department for International Development (DFID) through the Task Force for Global Health and UK Foreign Commonwealth and Development Office (FCDO) through the Accelerating the Sustainable Control and Elimination of Neglected Tropical Diseases (ASCEND) programme (FCDO grant number PO-8374) for funding this study. We thank Professor Jennifer Downs, M.D., Ph.D., for her guidance throughout this study and her insightful comments on earlier drafts of this publication. We thank the communities where this study was conducted for supporting this study. We specifically thank the leaders of these communities for facilitating entry into their jurisdiction and supporting the process of recruiting study participants. In a special way, we thank the study participants for accepting to participate in the study and providing responses that form the core of this paper. Finally, we thank the reviewers for their invaluable comments.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The opinions expressed in this publication are those of the authors and do not necessarily reflect the views of DFID.
1. Bland KG, Gelfand M. The effects of schistosomiasis on the cervix uteri in the African female. BJOG. (1970) 77:1127–31. doi: 10.1111/j.1471-0528.1970.tb03477.x
2. Kjetland EF, Poggensee G, Helling-Giese G, Richter J, Sjaastad A, Chitsulo L, et al. Female genital schistosomiasis due to Schistosoma haematobium Clinical and parasitological findings in women in rural Malawi. Acta Tropica. (1996) 62:239–55. doi: 10.1016/S0001-706X(96)00026-5
3. UNAIDS. No more neglect – Female genital schistosomiasis and HIV – Integrating sexual and reproductive health interventions to improve women’s lives. Geneva: Joint United Nations Program on HIV/AIDS (UNAIDS (2019).
4. Kjetland EF, Kurewa EN, Ndhlovu PD, Midzi N, Gwanzura L, Mason PR, et al. Female genital schistosomiasis – a differential diagnosis to sexually transmitted disease: genital itch and vaginal discharge as indicators of genital Schistosoma haematobium morbidity in a cross-sectional study in endemic rural Zimbabwe. Trop Med Int Health. (2008) 13:1509–17. doi: 10.1111/j.1365-3156.2008.02161.x
5. Engels D, Hotez PJ, Ducker C, Gyapong M, Bustinduy AL, Secor WE, et al. Integration of prevention and control measures for female genital schistosomiasis, HIV and cervical cancer. Bull World Health Organ. (2020) 98:615–24. doi: 10.2471/BLT.20.252270
6. Colley DG, Bustinduy AL, Secor WE, King CH. Human schistosomiasis. Lancet. (2014) 383:2253–64. doi: 10.1016/S0140-6736(13)61949-2
7. Galappaththi-Arachchige H, Amlie Hegertun I, Holmen S, Qvigstad E, Kleppa E, Sebitloane M, et al. Association of urogenital symptoms with history of water contact in young women in areas endemic for S. haematobium. A cross-sectional study in rural South Africa. IJERPH. (2016) 13:1135. doi: 10.3390/ijerph13111135
8. Downs JA, Dupnik KM, Van Dam GJ, Urassa M, Lutonja P, Kornelis D, et al. Effects of schistosomiasis on susceptibility to HIV-1 infection and HIV-1 viral load at HIV-1 seroconversion: A nested case-control study. PloS Negl Trop Dis. (2017) 11:e0005968. doi: 10.1371/journal.pntd.0005968
9. Kjetland EF, Hegertun IE, Baay MF, Onsrud M, Ndhlovu PD, Taylor M. Genital schistosomiasis and its unacknowledged role on HIV transmission in the STD intervention studies. Int J STD AIDS. (2014) 25:705–15. doi: 10.1177/0956462414523743
10. Poggensee G, Kiwelu I, Weger V, Göppner D, Diedrich T, Krantz I, et al. Female genital schistosomiasis of the lower genital tract: prevalence and disease-associated morbidity in northern Tanzania. J Infect Dis. (2000) 181:1210–3. doi: 10.1086/315345
11. Wall KM, Kilembe W, Vwalika B, Dinh C, Livingston P, Lee YM, et al. Schistosomiasis is associated with incident HIV transmission and death in Zambia. PloS Negl Trop Dis. (2018) 12:e0006902. doi: 10.1371/journal.pntd.0006902
12. Jacobson J, Pantelias A, Williamson M, Kjetland EF, Krentel A, Gyapong M, et al. Addressing a silent and neglected scourge in sexual and reproductive health in Sub-Saharan Africa by development of training competencies to improve prevention, diagnosis, and treatment of female genital schistosomiasis (FGS) for health workers. Reprod Health. (2022) 19:20. doi: 10.1186/s12978-021-01252-2
13. Ruane-McAteer E, Amin A, Hanratty J, Lynn F, Corbijn Van Willenswaard K, Reid E, et al. Interventions addressing men, masculinities and gender equality in sexual and reproductive health and rights: an evidence and gap map and systematic review of reviews. BMJ Glob Health. (2019) 4:e001634. doi: 10.1136/bmjgh-2019-001634
14. Dehne KL, Snow R, O’Reilly KR. Integration of prevention and care of sexually transmitted infections with family planning services: what is the evidence for public health benefits? Bull World Health Organ. (2000) 78:628–39.
15. Haberlen SA, Narasimhan M, Beres LK, Kennedy CE. Integration of family planning services into HIV care and treatment services: a systematic review. Stud Family Plann. (2017) 48:153–77. doi: 10.1111/sifp.12018
16. Mutalemwa PP, Kisinza WN, Urassa JA, Kibona SN, Mwingira U, Lasway C, et al. Integrating reproductive and child health and HIV services in Tanzania: implication to policy, systems and services. Tanzania J Hlth Res. (2013) 15(2):1–10. doi: 10.4314/thrb.v15i2.8
17. Kennedy CE, Spaulding AB, Brickley DB, Almers L, Mirjahangir J, Packel L, et al. Linking sexual and reproductive health and HIV interventions: a systematic review. J Int AIDS Soc. (2010) 13:26–6. doi: 10.1186/1758-2652-13-26
18. Sharma S, Kc B, Khatri A. Factors influencing male participation in reproductive health: a qualitative study. JMDH. (2018) 11:601–8. doi: 10.2147/JMDH
19. Davis J, Vyankandondera J, Luchters S, Simon D, Holmes W. Male involvement in reproductive, maternal and child health: a qualitative study of policymaker and practitioner perspectives in the Pacific. Reprod Health. (2016) 13:81. doi: 10.1186/s12978-016-0184-2
20. Sternberg P. Evaluating men’s involvement as a strategy in sexual and reproductive health promotion. Health Promotion Int. (2004) 19:389–96. doi: 10.1093/heapro/dah312
21. Nkwonta M. Male participation in reproductive health interventions in sub-Saharan Africa: a scoping review. Int Perspect Sexual Reprod Health. (2019) 45:71. doi: 10.1363/45e8119
22. Bond V, Ngwenya F, Murray E, Ngwenya N, Viljoen L, Gumede D, et al. Value and limitations of Broad Brush Surveys used in community-randomized trials in Southern Africa. Qual Health Res. (2019) 29:700–18. doi: 10.1177/1049732318809940
23. Hennink MM. Focus group discussions. Oxford: Oxford University Press (2014). doi: 10.1093/acprof:osobl/9780199856169.001.0001
24. Gilchrist VJ, Williams RL. Key informant interviews. In: Crabtree BF, Miller WL, editors. Doing qualitative research. SAGE Publishing, Thousand Oaks, CA (1999). p. 71–88.
25. D’Exelle B, Ringdal C. Women’s use of family planning services: an experiment on the husband’s involvement. J Dev Economics. (2022) 158:102915. doi: 10.1016/j.jdeveco.2022.102915
26. Vermeulen E, Solnes Miltenburg A, Barras J, Maselle N, Van Elteren M, Van Roosmalen J. Opportunities for male involvement during pregnancy in Magu district, rural Tanzania. BMC Pregnancy Childbirth. (2016) 16:66. doi: 10.1186/s12884-016-0853-8
27. Sundararajan R, et al. “How gender and religion impact uptake of family planning: results from a qualitative study in Northwestern Tanzania”. BMC Women’ Health. (2019) 19:1–99. doi: 10.1186/s12905-019-0802-6
28. Millanzi WC, Osaki KM, Kibusi SM. Attitude and prevalence of early sexual debut and associated risk sexual behavior among adolescents in Tanzania; Evidence from baseline data in a Randomized Controlled Trial. BMC Public Health. (2023) 23:1758. doi: 10.1186/s12889-023-16623-6
29. Schaffnit SB, Urassa M, Lawson DW. “Child marriage” in context: exploring local attitudes towards early marriage in rural Tanzania. Sexual Reprod Health Matters. (2019) 27:93–105. doi: 10.1080/09688080.2019.1571304
30. Mazigo HD, Samson A, Lambert VJ, Kosia AL, Ngoma DD, Murphy R, et al. “We know about schistosomiasis but we know nothing about FGS”: a qualitative assessment of knowledge gaps about female genital schistosomiasis among communities living in Schistosoma haematobium endemic districts of Zanzibar and Northwestern Tanzania. PloS Negl Trop Dis. (2021) 15:e0009789. doi: 10.1371/journal.pntd.0009789
32. Ampt F, Mon MM, Than KK, Khin MM, Agius PA, Morgan C, et al. Correlates of male involvement in maternal and newborn health: a cross-sectional study of men in a peri-urban region of Myanmar. BMC Pregnancy Childbirth. (2015) 15:122. doi: 10.1186/s12884-015-0561-9
33. Bhatta DN. Involvement of males in antenatal care, birth preparedness, exclusive breast feeding and immunizations for children in Kathmandu, Nepal. BMC Pregnancy Childbirth. (2013) 13:14. doi: 10.1186/1471-2393-13-14
34. Yaya S, Okonofua F, Ntoimo L, Udenigwe O, Bishwajit G. Men’s perception of barriers to women’s use and access of skilled pregnancy care in rural Nigeria: a qualitative study. Reprod Health. (2019) 16:86. doi: 10.1186/s12978-019-0752-3
35. Schuler SR, Rottach E, Mukiri P. Gender norms and family planning decision-making in Tanzania: a qualitative study. J Public Health Afr. (2011) 2:25. doi: 10.4081/jphia.2011.e25
Keywords: female genital schistosomiasis, male involvement, FGS services, sexual and reproductive health, Tanzania
Citation: Lambert VJ, Samson A, Matungwa DJ, Kosia AL, Ndubani R, Hussein M, Kalua K, Bustinduy A, Webster B, Bond VA and Mazigo HD (2024) Female genital schistosomiasis is a women’s issue, but men should not be left out: involving men in promoting care for female genital schistosomiasis in mainland Tanzania. Front. Trop. Dis 5:1333862. doi: 10.3389/fitd.2024.1333862
Received: 06 November 2023; Accepted: 04 March 2024;
Published: 02 April 2024.
Edited by:
Roch Christian Johnson, CIFRED UAC, BeninReviewed by:
Verner Orish, University of Health and Allied Sciences, GhanaCopyright © 2024 Lambert, Samson, Matungwa, Kosia, Ndubani, Hussein, Kalua, Bustinduy, Webster, Bond and Mazigo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Valencia J. Lambert, dmpsMjJAY29ybmVsbC5lZHU=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.