 Sofie J. Dragsbæk1,2
Sofie J. Dragsbæk1,2 Sofie K. Carstens1,2
Sofie K. Carstens1,2 Ida Savkov1,2
Ida Savkov1,2 Karoline Jøker1,2
Karoline Jøker1,2 Bodo S. Randrianasolo3
Bodo S. Randrianasolo3 Peter D. Leutscher1,2
Peter D. Leutscher1,2 Louise Arenholt1,2,4*
Louise Arenholt1,2,4*- 1Center for Clinical Research, North Denmark Regional Hospital, Hjørring, Denmark
- 2Department of Clinical Medicine, Aalborg University, Aalborg, Denmark
- 3Association K’OLO VANONA, Antananarivo, Madagascar
- 4Department of Obstetrics and Gynaecology, North Denmark Regional Hospital, Hjørring, Denmark
Background: Female genital schistosomiasis (FGS) is characterised by cervico-vaginal lesions such as grainy sandy patches, homogeneous yellow sandy patches, and abnormal blood vessels. Diagnosis, treatment, and surveillance of FGS presents challenges due to the absence of diagnostic tools in endemic areas. Likewise, a tool for quantification of the lesions is missing. This study aimed to validate the digital gridded imaging technique (DGIT) for quantification of three specific cervical lesion types associated with FGS.
Methods: Using the QubiFier software program, 70 cervical photographic images obtained from women diagnosed with FGS and treated with Praziquantel (PZQ) were randomly sampled for a validation study. The women lived in a S. haematobium-endemic area of Madagascar. For each image, a semi-transparent grid was applied, composed of 424 equally sized squares positioned to cover the cervix. Squares exhibiting any of the specific lesions were marked by three observers to determine the grainy sandy patches proportion (GSP), homogeneous yellow sandy patches proportion (HSP), and abnormal blood vessel proportion (BVP). To train the observers, a set of ten images was utilized, leaving 60 images for the validation. To test inter-rater reliability, the 60 cervical images were scored independently by three observers. To test intra-rater reliability, ten images were scored twice with a two-week interval. Intraclass correlation coefficient (ICC) was used as the main statistical method to assess the reliability between observers.
Results: The median age of the included women was 26.5 (IQR 20.8-33.0) years, and 74% of them had detectable S. haematobium eggs in their urine. The three proportions were found to be consistent and reliable across the observers, as well as the rescoring on Days 0 and 14. Inter-rater reliability was good for all three cervical lesion types (ICC 0.768-0.890). Intra-rater reliability was good for GSP (ICC 0.832) and excellent for HSP and BVP (ICC 0.932 and 0.982, respectively).
Conclusion: In this study DGIT was validated as a potential morbidity detection method for quantification of the three lesion types associated with FGS.
Introduction
Female genital schistosomiasis (FGS) covers a broad spectrum of distinct gynaecological manifestations, including chronic lower abdominal pain, vaginal discharge, dyspareunia, and postcoital bleeding, in addition to infertility (1–3). Intestinal schistosomiasis and urogenital schistosomiasis are the two highly prevalent forms found in Sub-Saharan Africa (4). Urogenital schistosomiasis is caused by the Schistosoma haematobium flatworm. The life cycle of the parasite involves a snail of the Bulinus genus as an intermediate host. In women, eggs from the adult worms dwelling in the pelvic venous plexus system, are trapped in the cervico-vaginal mucosa, uterus, fallopian tubes, and other parts of the genital tract. The entrapped eggs cause various pathophysiological lesions of immune-inflammatory origin followed by further progression of fibrosis and calcification (5–7). Homogeneous yellow sandy patches, grainy sandy patches, abnormal blood vessels, and rubbery papules are four distinct types of cervico-vaginal lesion described in women with FGS (1–3).
The presence of at least one of the four cervicovaginal lesions established by a pelvic examination, typically aided by a colposcope, is considered diagnostic for FGS (2, 3, 8). However, a colposcope is an expensive diagnostic instrument that is rarely available in primary healthcare settings in endemic areas (9, 10). Moreover, not all colposcopes are equipped for clinical image documentation and storage, thus impeding the ability to track changes in cervical pathology over time (11, 12). With the aim of exploring a simpler solution, particularly in scenarios where colposcopes are unavailable, Arenholt et al. (13) tested the use of a digital camera for the recording and storage of cervical lesions in women with FGS, with promising outcomes. The study was carried out in Madagascar. The authors additionally developed a digital gridded imaging technique (DGIT) tool utilising the QubiFier software program for the evaluation of cervical images obtained from the women with FGS. By placing a semi-transparent grid composed of 424 equally sized squares on the cervical image, meticulous documentation and quantification of cervical lesions was carried out. The DGIT method was successfully validated for quantifying the overall cervical lesion proportion (CLP) and rubbery papule count (RPC) (13). However, validation of the quantification method for the other three cervical lesion types, namely homogeneous yellow sandy patches proportion (HSP), grainy sandy patches proportion (GSP), and abnormal blood vessel proportion (BVP), remained unaddressed. The aim of this study was thus to test and validate the DGIT for the quantitative assessment of cervical HSP, GSP, and BVP in women with FGS living in an S. haematobium endemic area.
Methods
Study design and ethics
The present study design mirrors the previous study by Arenholt et al. (13), which developed and validated the DGIT by use of QubiFier software for the quantitative assessment of CLP and RPC in women with FGS. In the present next-step validation study, the technique was tested and validated for the quantitative assessment of cervical HSP, GSP and BVP. Both studies utilised 70 digital cervical images obtained during a randomised controlled trial (RCT) conducted in Madagascar between September 2019 and March 2020 (14). The RCT aimed to evaluate the effectiveness of a single dose Praziquantel (PZQ) (40 mg/kg) and repeated doses of PZQ (40 mg/kg at baseline supplemented by doses after 12 hours and 24 hours, and after 5 and 10 weeks) in reducing cervical pathology and symptoms associated with FGS. Follow-up assessments were conducted at week 5, week 10, and week 15 following the initial dose.
Ethical approval was obtained from the Ethics Committee at the Ministry of Health in Antananarivo (Authorisation Number: 098-MSANP/CERBM; Number: 059-MSANP/CERBM; Number: 065 MSANP/SG/-AGMED/CNPV/CERBM). All the women included in the study provided informed written consent. Given that girls can potentially be affected by FGS from pre-puberty onwards and recognising that the consequences of FGS may manifest during adolescence, we deemed it ethically unacceptable to exclude girls aged 15 to 17. To ensure the confidentiality for these adolescent participants, we refrained from requesting informed consent from a third party, such as a parent or legal guardian. This procedure was approved by the Ethics Committee.
Participants in the randomised controlled trial
In total, 116 female participants were recruited for the RCT from two primary health centres in the municipalities of Antsakoamanondro and Antranokarany, both of which are considered endemic areas (14). All examinations were conducted at the two health centres. For inclusion, the women had to be in the age range of 15 to 35 years. The inclusion criterion was the presence of cervical lesions resulting from FGS, identified during pelvic examination using a digital camera. The exclusion criteria ere no prior sexual intercourse, pregnancy, a history of tumours in the vulva, vagina, or uterus, prior hysterectomy, HIV positive status, medical conditions requiring hospitalisation, recent treatment with PZQ (within the past three months), and any contraindication to PZQ (14).
Baseline information on medical history and complaints was acquired from the study participants using a questionnaire in Sakalava, the local dialect of the study area (14). While the questionnaire was pre-tested according to relevance and interpretation, it was not validated. For documentation of cervical lesions, an image of the cervical surface was obtained from all included women using a digital camera as described below. Urine samples were collected, and 50 ml of urine was filtered through a polycarbonate membrane to determine the presence of schistosome eggs. The present study will not present data on complaints alongside other outcomes from the RCT including pelvic exam abnormalities, cervicovaginal S. haematobium DNA and circulating anodic antigens (CAA) in serum. At baseline, all women underwent testing for sexually transmitted infections (STIs), including Human papillomavirus, Herpes simplex virus, Neisseria gonorrhoeae, Chlamydia trcachomatis, Trichomonas vaginalis, Mycoplasma genitalium and bacterial vaginosis (14). No testing for STI’s was conducted at Week 5 and Week 10. Throughout all visits, STI treatment was administered to the women based on the syndromic approach recommended by the Ministry of Health of Madagascar. After treatment at baseline with PZQ, all study participants were followed up after 5, 10, and 15 weeks involving a clinical reassessment and additional photographic documentation of the cervix (14).
Pelvic examination and digital images of cervix
Pelvic examination, including bimanual palpation and inspection using a vaginal speculum, was performed at baseline and all follow-up visits for each woman (14). All examinations were conducted by two physicians with extensive experience in diagnosing and treating women with FGS. During the pelvic examination, photographic documentation of the cervix was obtained using a Canon EOS M50 camera equipped with a 100 mm macro lens and lens-mounted circular LED light. A polarisation filter was mounted in front of the camera lens to eliminate light reflection from the surface of the cervix. The camera was placed at a distance of 30 cm from the cervix on a tripod mounted on a microscope sledge to allow for precise focus adjustment. The microscope sledge was adjusted to ensure the orifice of the cervix was localised in the centre of the camera display with a 3-5 mm free fringe around the rims of the cervix. This approach was selected to ensure the uniformity of images and to enhance image comparability regarding lighting and reflection. All digital images captured during the RCT were stored in the REDCap (Research Electronic Data Capture Version 9.5.6) data management system hosted by the North Denmark Region and saved for later offline assessment using the DGIT.
Quantification of cervical lesions
JavaScript programming was employed to create FGS QubiFier, a DGIT tool designed to assess and quantify cervical lesions resulting from S. haematobium infection. Whitin the software program, a cervical image can be downloaded for further offline evaluation. The software superimposes a semi-transparent circular grid consisting of 424 equally sized squares as an additional layer on the digital image of the cervix. Adjusting the zoom level of the image ensures that the grid covers the whole circumference of the cervix with the orifice centered in the grid. Apart from the zoom feature, adjustment for brightness, contrast, saturation, and hue shift are available for further image analysis. The gridding enables the observer to manually mark the squares containing any FGS-associated lesion type in a structured manner. The lesion-free squares are left unmarked. For each lesion type, the number of affected squares (HS, GS, and BV) are quantified and reviewed separately for the subsequent calculation of their proportion of all affected areas, as displayed in Figure 1. For each image, the proportion is calculated as the number of affected squares dived by 424. The proportion is counted automatically by the FGS QubiFier software program. The estimated proportion ranges from zero to 100 (13).
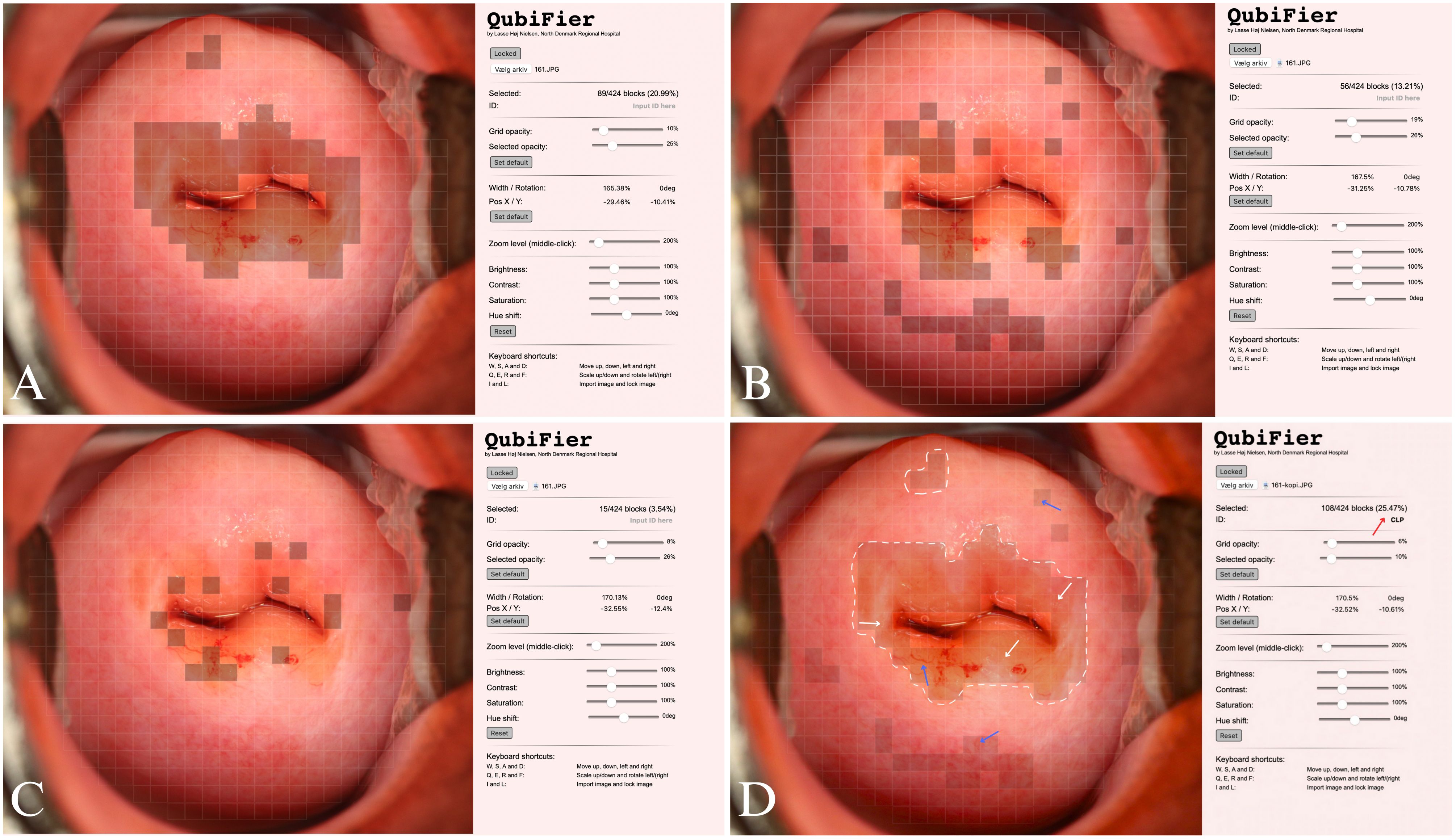
Figure 1 Digital cervical images demonstrating evaluation of FGS-associated lesions using QubiFier and the digital gridded imaging technique. (A) Illustration of HSP evaluation. (B) Illustration of BVP evaluation. (C) Illustration of GSP evaluation. (C) Illustration of BVP evaluation. (D) All FGS associated lesions are digitally marked in QubiFier to determine the CLP. The white dashed lines show areas, which contain homogenous sandy patches appearing as a yellow-colored area. The white and blue arrows indicate the following lesion types: grainy sandy patches (white arrow) and abnormal blood vessels (blue arrow). The red arrow shows the CLP of the cervix covered by any type of pathognomonic lesions. FGS, Female genital schistosomiasis; HSP, homogeneous yellow sandy patches proportion; GSP, grainy sandy patches proportion; BVP, abnormal blood vessels proportion; CLP, cervical lesion proportion.
Validation process
From the four visits during the RCT, a total of 402 cervical images were obtained (Figure 2). To test the reliability of scoring the HSP, GSP, and BVP, 70 images from Week 5 and Week 10 were randomly selected using block randomization with the assistance of the RStudio computer software program (version 1.2.5033) and blinded by a member of the research group who was not involved in the validation of the DGIT. Images obtained in Week 5 and Week 10 were selected due to images obtained at baseline and Week 15 had already been evaluated by one of the observers, rendering them unblinded. Validating these images allowed for the possibility that some women might not exhibit FGS-associated cervical lesions, given that they had undergone treatment with PZQ.
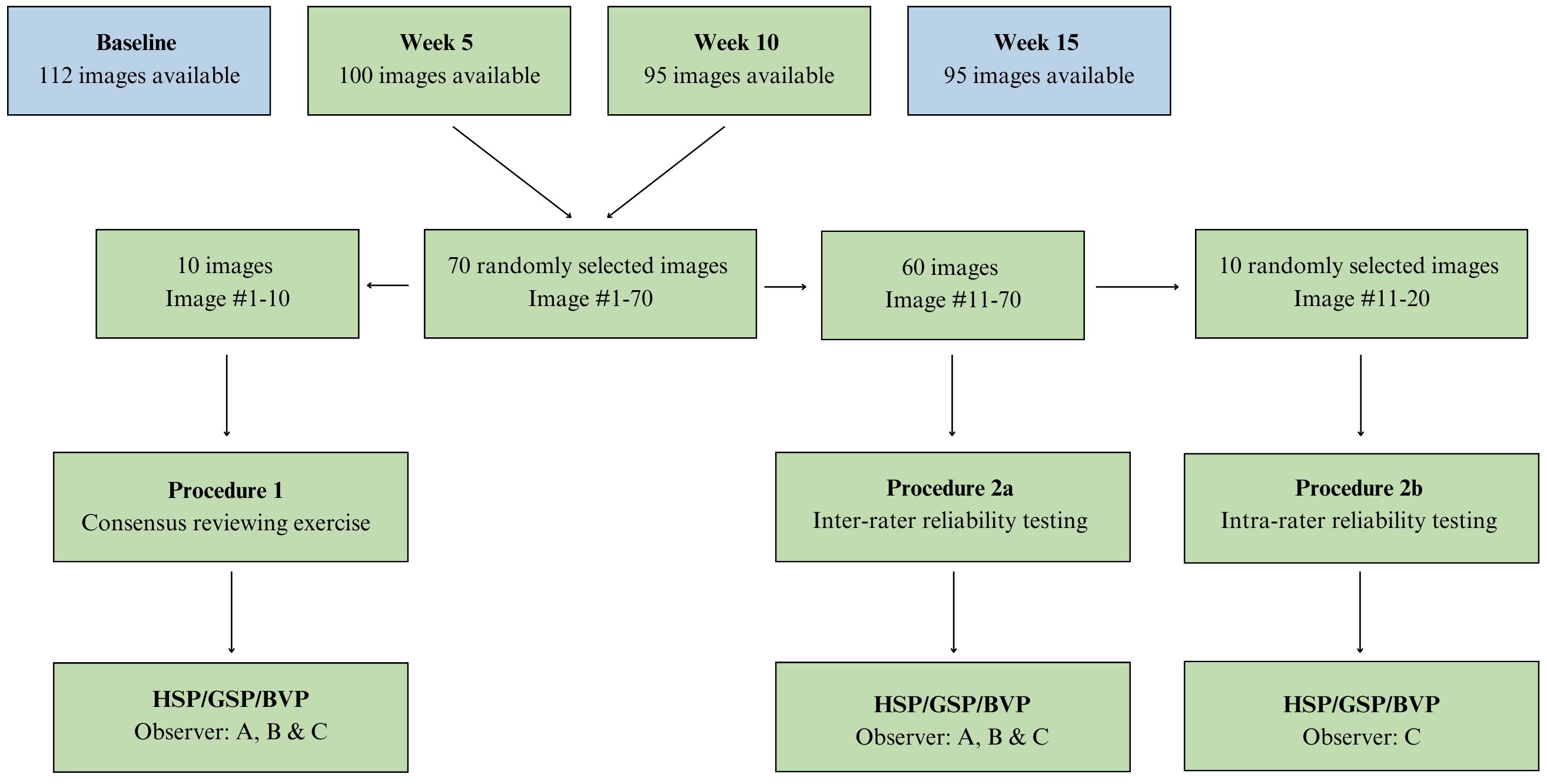
Figure 2 Flowchart displaying the different steps in the validation procedures in the FGS digital gridded imaging technique study. A total of 70 images of the cervix were reviewed for HSP, GSP and BVP. HSP, homogeneous yellow sandy patches proportion; GSP, grainy sandy patches proportion; BVP, abnormal blood vessels proportion.
The observers’ level of clinical experience varied regarding gynaecology in general and FGS specifically: Observer A (with almost completed MD qualification; familiar with FGS at a textbook level), Observer B (gynaecology consultant experienced in the with FGS field and previous use of DGIT) and Observer C (three medical students with almost completed BSc degree; familiar with FGS at textbook level, rated the images as a group). The reason for combining the three medical students into one group was their limited experience in gynaecology and FGS. Initial workshop training and a consensus rating exercise were given in which each observer independently examined ten randomly sampled images (Images 1-10) and rated the three individual lesion proportions (HSP, GSP, and BVP) (Figure 2). The observers subsequently shared and discussed their findings to reach consensus on the rating of the images. Sixty images (Images 11-70) were independently assessed for each lesion type by Observers A, B, and C. This procedure was implemented to test the inter-observer reliability. Two weeks after the initial assessment of a lesion, the intra-rater reliability was evaluated by reviewing ten randomly sampled images (Images 11-20) from the original image portfolio (Images 11-70) again. The re-testing was performed only by the medical students (Observer C) (Figure 2).
A comprehensive depiction of the entire cervical surface was occasionally challenged by reflections from light or anatomical complexities such as anteverted or retroverted cervix. Consequently, each observer conducted a thorough assessment to evaluate the impact of image quality on the scoring of cervical lesions. The evaluation categorised the digital image quality based on whether the cervix surface was depicted in its entirety or only partially. The assessment was reached through consensus among the three observers following their individual evaluations of image quality.
Data management and statistical analysis
For the statistical analysis, the individual scorings were manually entered into Microsoft Excel software for transferal to IBM SPSS Statistics 28.0.1.1 software (SPSS). To determine the presence of significant difference in the scoring of cervical lesions among the three independent observers (inter-rater agreement), the intraclass correlation coefficient (ICC) was calculated in a two-way mixed-effects model based on average rating values and absolute agreement. Likewise, the ICC was calculated in between every single observer as a pairwise (Observer A and B, A and C, and B and C) inter-rater agreement. The ICC is a statistical measure used to assess the reliability or consistency of measurements obtained by multiple observers or raters. The mixed-effects model was chosen to account for systematic differences between raters, ensuring that the ICC reflected the consistency of ratings beyond what could be expected by chance alone. By considering absolute agreement, the calculation method also accounts for random variability in the ratings (15). To test the agreement between Observer C on Days 0 and 14 (intra-rater agreement), ICC was likewise calculated using a two-way mixed-effects model based on a single-rating and absolute agreement.
The ICC ranges from 0 to 1, with higher values indicating greater consistency or agreement between observers. Specifically, ICC values are interpreted as <0.5 (poor), 0.5 to 0.75 (moderate), 0.76 to 0.9 (good) and > 0.9 (excellent) (15). For both HSP, GSP, and BVP, a median and interquartile ranges (ICQ) were calculated and visually represented using a box-and-whisker plot. The included women’s ages and the number of S. haematobium eggs per 50 ml of urine were reported as median and ICQ.
Results
Baseline characteristics
From the 70 randomly sampled images, sixty were selected for the validation procedure as described above. As a result of the randomisation process, twenty images were derived from ten women, captured both at Week 5 and Week 10, leaving forty images sourced from forty distinct women, either at Week 5 or Week 10 (Figure 2). The median age of the 50 women was 26.5 years (IQR 20.8-33.0). In 37 women (74%) S. haematobium eggs could be detected in the urine and median number of eggs per 50 ml of urine was 2.5 (IQR 0-62.0). In 13 women, the filtration of 50 ml of urine yielded no detectable eggs.
Quality of the digital images
Of the 60 digital images used for testing the reliability of the inter- and intra-raters, 33 images (55%) provided a complete view of the cervix. The remaining 27 images (45%) covered between 80 and 100% of the cervical surface. Despite this limitation, the observers deemed all images to be of adequate quality to determine HSP, GSP, and BVP. All 60 images were thus included in the subsequent analysis.
Homogeneous yellow sandy patches proportion
The median HSP for the three observers is illustrated in Figure 3. The individual measured HSP for each image ranged from 0% to 50% for Observer A, from 0% to 48.35% for Observer B, and from 0% to 30.66% for Observer C (Supplementary Figure 1). Testing inter-rater reliability for all three observers (A, B and C) for HSP by ICC yielded a value of 0.851 (95% CI 0.678-0.923), indicating a good performance (Table 1). However, only a moderate reliability was calculated between Observer A and C (Table 1). The intra-rater reliability for Observer C was investigated by ICC and found to be 0.932 (95% CI 0.108-0.987), indicating excellent performance (Table 1).
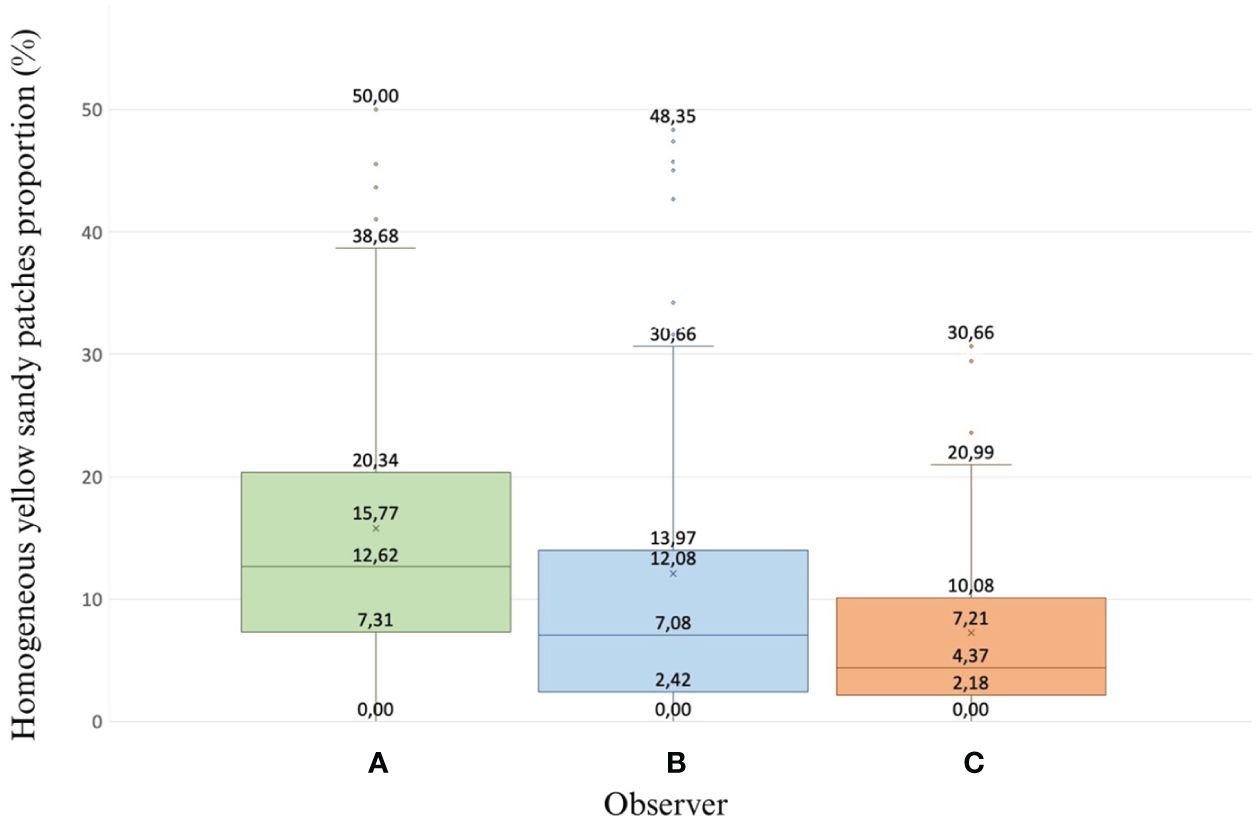
Figure 3 A box-and-whisker-plot showing the proportion (%) of homogeneous yellow sandy patches for each observer (A–C) who rated the 60 digital images. The interquartile range is represented by the upper and lower lines of the box, while the median is indicated by the horizontal line.
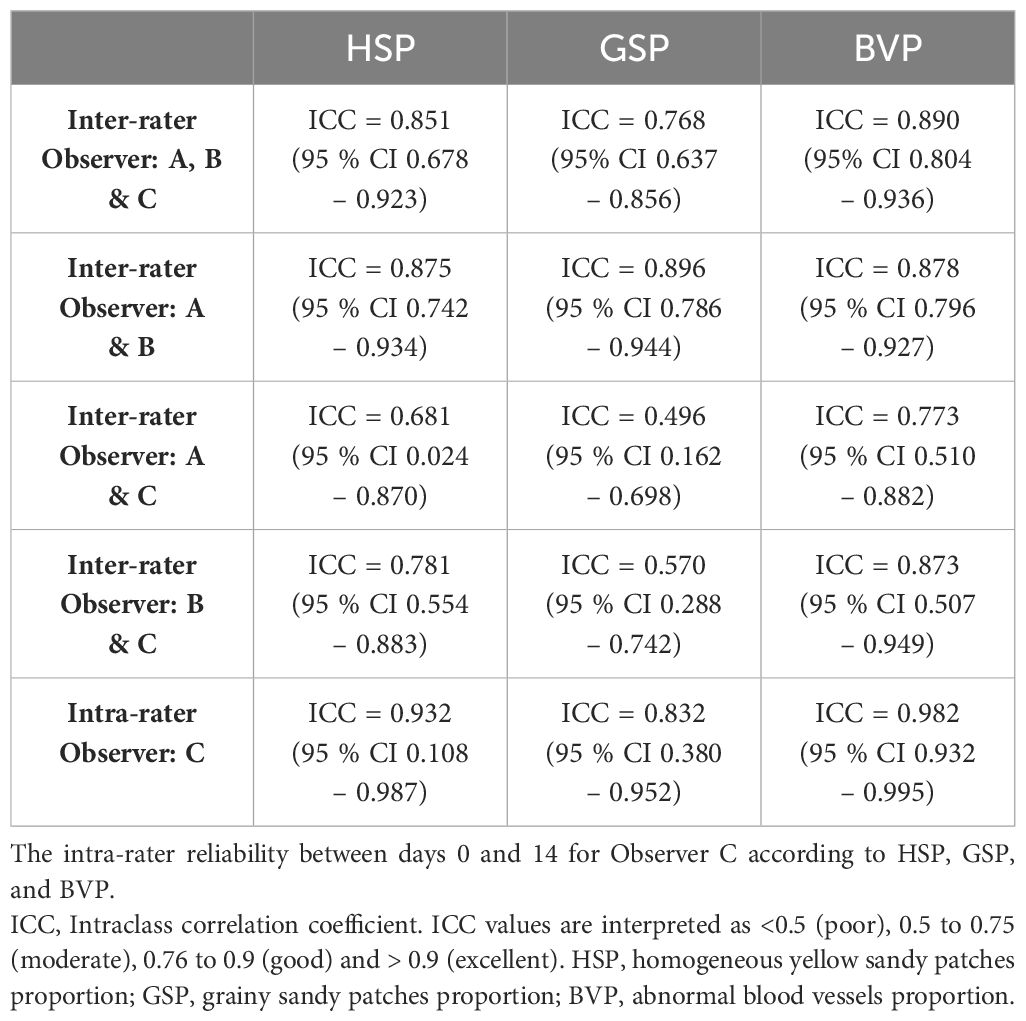
Table 1 The inter-rater reliability between Observers A, B, and C, A and B, A and C, and B and C according to HSP, GSP, and BVP.
Grainy sandy patches proportion
The median GSP, as assessed by the three observers, is illustrated in Figure 4. The individual measured GSP for each image varied between 0.94% and 33.96% for Observer A, from 0% to 25.71% for Observer B, and from 0.24% to 26.89% for Observer C (Supplementary Figure 2). The inter-rater reliability ICC for GSP yielded a value of 0.768, signifying a good performance (95% CI 0.637-0.856). The ICC revealed a poor reliability between Observer A and C, a moderate reliability between Observer B and C but a good performance between Observer A and B (Table 1). The intra-rater reliability was determined to be 0.832, indicating a good performance (95% CI 0.380-0.957) (Table 1).
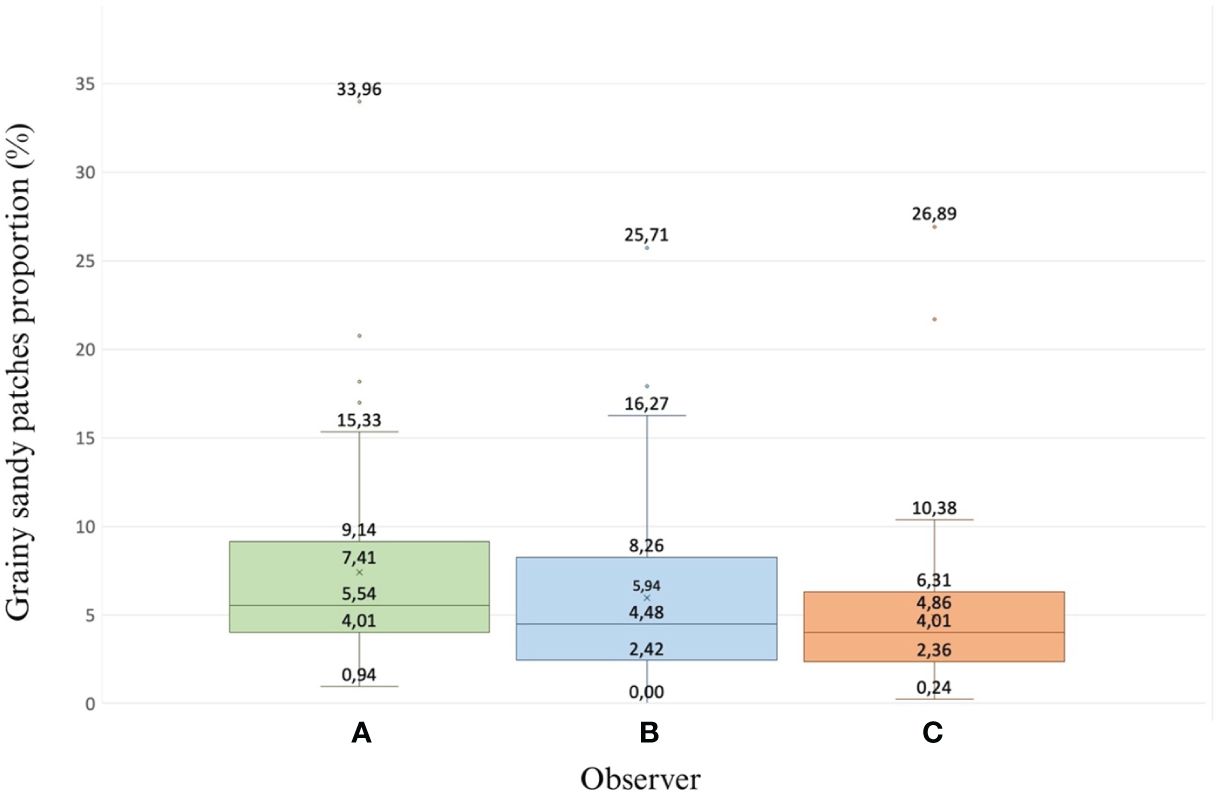
Figure 4 A box-and-whisker plot that displays the proportion (%) of grainy sandy patches as assessed by the three observers (A–C) for the set of 60 digital images. The upper and lower lines of the box signify the interquartile range, and the horizontal line represents the median.
Abnormal blood vessels proportion
The median BVP values as determined by the three observers are illustrated in Figure 5. For Observer A, the individual measured BVP for each image ranged from 0.24% to 54.95%, from 0% to 54.24% for Observer B, and from 0% to 40.80% for Observer C (Supplementary Figure 3). Inter-rater reliability for BVP was investigated using ICC, which was determined to be 0.890, indicating a good performance (95% CI 0.804-0.936). Testing the reliability between the individual observers showed good performance (Table 1). Correspondingly, intra-rater reliability for Observer C revealed an ICC of 0.982, demonstrating an excellent performance (95% CI 0.932-0.995) (Table 1).
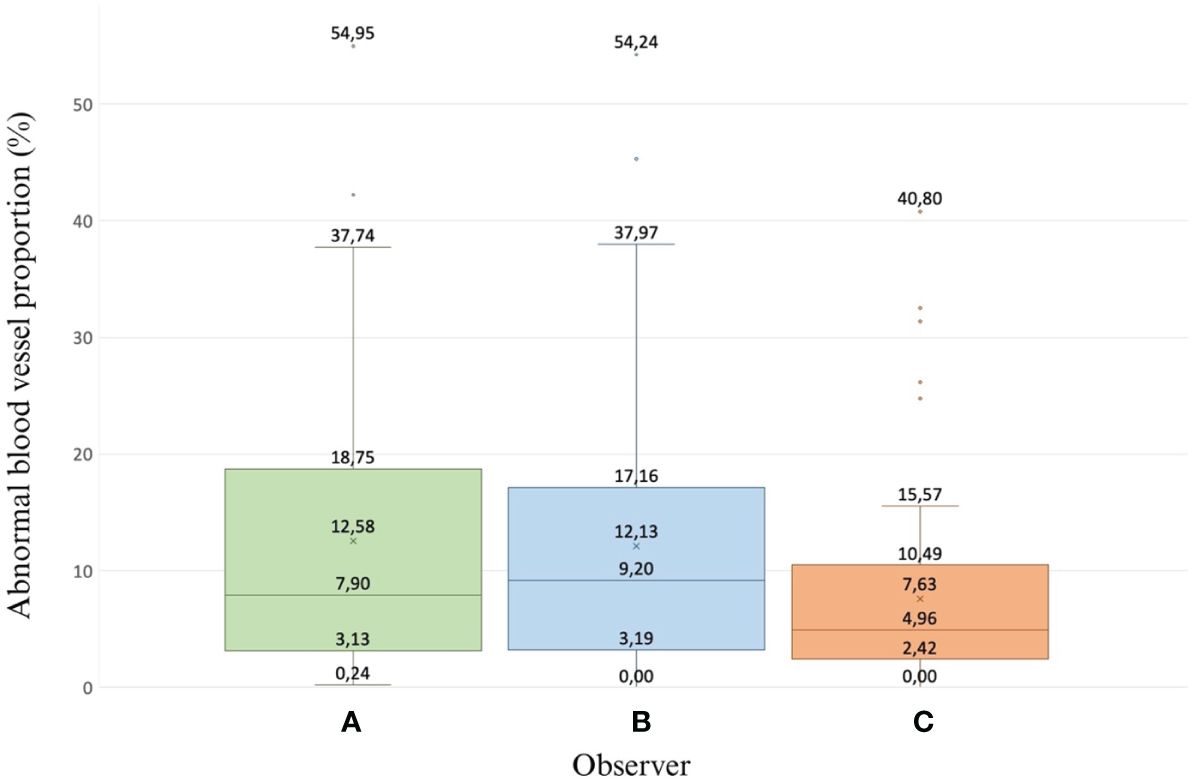
Figure 5 A box-and-whisker plot depicts the proportion (%) of abnormal blood vessels as assessed by the three observers (A–C) who evaluated the 60 digital images. The upper and lower lines of the box represent the interquartile range, while the horizontal line indicates the median.
Discussion
This study has further validated the DGIT tool for quantitative assessment of cervical lesions associated with FGS, namely homogenous yellow sandy patches, grainy sandy patches, and abnormal blood vessels. The ICC values for HSP, GSP, and BVP all indicated a good performance (0.851, 0.768 and 0.890, respectively), suggesting reliable and consistent measurements across the observers. Similarly, the ICC values for the re-scoring of HSP and BVP on both Day 0 and Day 14 showed excellent performance, while the ICC value for GSP indicated a good performance. The results show that the re-scoring performed by Observer C was highly reliable.
While consensus among the observers was indeed significant, a closer examination of the individual scores revealed that Observer C consistently had the lowest scores, along with the lowest ICC scores when compared to the two other observers. This discrepancy could be attributed to differences in experience levels among the observers. Likewise, an explanation could be that Observers A and B were single individuals whereas Observer C consisted of three individuals, which necessitated consensus in scoring. The collaborative scoring approach likely resulted in a more meticulous evaluation of lesions as every assessment had to gain approval from all three group members. To bridge the scoring gap between individual and consensus evaluations, it would be beneficial to disaggregate Observer C into three individual observers to yield a greater volume of data and potentially enhance the reliability of the results. According to the ICC combining all three observers and by pairwise ICC comparisons, GSP appeared to be the most challenging lesion to assess. This could be attributed to reflections on the cervix that mimic grainy sandy patches. Besides group composition, other challenges associated with the scoring of cervical lesions included the quality of the digital images such as blur caused by camera settings, partial visibility of the cervix, grid placement, reflection, and the observers use of different computer screens. Both individually and combined, such challenges contribute to discrepancies among the observers, as discussed in Arenholt et al. (13). The positioning of the grid and the chosen zoom level for cervical images may have introduced disparity among the images. For this reason, ensuring a consistent position of the grid across all images is crucial when assessing images captured at different time points within the same woman. Failure to do so may result in inaccurate evaluations and conclusions. For instance, if a lesion is located at the outer circumference of the cervical surface and is excluded from the proportion in one image due to the grid failing to cover it, while being counted in another image.
In 45% of the images, the cervical circumference was not fully visible, potentially leading to overlooked lesions. To enhance the image quality in future studies, we plan to investigate the image-capturing process, which may involve instructing women to perform a Valsalva manoeuvre during image capture or choosing alternative types of speculums.
At the baseline examination, only women diagnosed with FGS associated cervical lesions were selected for the study according to the RCT protocol. Even though only images obtained at the visits at Week 5 and Week 10 after inclusion and baseline treatment were used for this project, the chance of FGS cervical lesions being present remained high (7, 16). In a study conducted by Kjetland et al., there was no significant reduction in lesions observed among 427 women 12 months after PZQ treatment (7). Similarly, findings from the study by Kabengele et al. revealed that cervical lesions persisted in 77% of the 43 included women when evaluated 6 to 12 months after PZQ treatment (16). We believe that by utilizing images from Week 5 and Week 10, the risk of cervical lesions being present is even higher. With this awareness, it is conceivable that the ratings done by the observers may have been biased. To enhance the validity of the DGIT, it would be advantageous to incorporate control images of women without the FGS diagnosis. This would enable us to validate the method’s capability to distinguish between women with FGS associated cervical lesions and those without. In a study conducted by Sturt et al. (8), it was found that there existed a low level of correlation between two experts when diagnosing FGS through the review of colposcopic cervical images. Likewise, up to 20% of the images were deemed unsuitable for diagnosing FGS due to either poor image quality or inadequate visibility of the cervical region. This underscores the imperative for continued exploration into tools that enhance the visualization of FGS associated cervical lesions.
Cervical lesions, along with FGS associated symptoms reported by the women, can resemble those found in women with conditions such as cervical dysplasia and chlamydia (17, 18). Consequently, due to the lack of information on STIs at Week 5 and Week 10, this study cannot definitively rule out the possibility that some of the cervical lesions detected at these visits may be partly attributed to STIs rather than solely to FGS.
The DGIT would constitute a valuable tool in detecting and quantifying FGS associated cervical lesions in future control programs in schistosomiasis-endemic areas. However, further development is needed to improve its accuracy and efficacy and to reduce time consumption in the manual scoring of cervical lesions. More precise and reliable diagnosis of cervical lesions could be obtained by utilising machine learning-based algorithms and software tools for image analysis. The implementation of advanced automated software tools has potential to eliminate human discrepancies and a facilitate diagnosis and assessment of FGS, thereby reducing the workload on healthcare workers regarding the time spent on assessing the cervical lesions in a quantitative manner. At the time of writing, progress towards creating an automated lesion recognition system has already been made. In studies by Holmen et al., computerised imaging analysis techniques have been described aiming to identify sandy patches by differentiating among the colour variations seen in healthy cervical mucosa and the yellowish appearance of the sandy patches (19, 20). This method involves applying hue, saturation, red, green, and blue filters to highlight the yellowish areas of the cervix. Such filters are akin to those used for the manual scoring of HSP, GSP, and BVP in the QubiFier program. In the computer analysis, the scoring is based on the number of affected pixels to establish a diagnostic threshold. Combining the adaptive, colorimetric image analysis method with automated image pre-processing has also been reported to enable the detection of lesions with 83% sensitivity and 73% specificity. Similarly, strong correlations between the diagnoses given by colposcopy and by computer colour analysis have been observed, with 80.5% sensitivity and 66.2% specificity. The method proposed by Holmen et al. (19, 20) nevertheless faces limitations as it addresses only superficial grainy sandy patches and homogenous sandy patches on the ectocervix for lesion detection. This implies that deep grainy sandy patches, abnormal blood vessels, or superficial grainy sandy patches of white rather than yellow colour may go undetected. Even if an automated lesion detection tool was to be developed, costly equipment for the collection of cervical images would still be required. Søfteland et al. (21) present a systematic review of research on the use of handheld tools as an alternative to stationary colposcopes for detecting precancerous and cancerous lesions on the cervix, which can resemble lesions linked to FGS. Their study examined the advantages and disadvantages of compiling cervical images using four different types of handheld colposcopes, a digital camera, and a smartphone. Interestingly, the study found no statistically significant difference in specificity and sensitivity for the identification of lesions whether images were taken by a handheld colposcope, a digital camera, or a smartphone.
Utilising smartphones for the assessment of women infected with S. haematobium could potentially enhance diagnosis and treatment rates (22). Compared to other diagnostic tools, a smartphone is user-friendly and relatively inexpensive, and it could easily be integrated with the DGIT. Their accessibility in endemic areas, including among healthcare workers, has the further advantage of not requiring specialised training for operation.
Quantifying cervical lesions can serve as a useful tool for evaluating the efficacy of treatment or for establishing possible correlations between cervical lesions and symptom picture. Moreover, this assessment approach may enhance our understanding of the natural history and the complexity of clinical manifestations occurring in women with FGS. It may further provide opportunities for developing new preventive and therapeutic strategies for the millions of girls and women affected by FGS.
FGS-associated lesions are not confined to the cervical surface but can also manifest on the vaginal wall (2, 3). Depending solely on digital images of the cervix for FGS evaluation alone could lead to overlooking vaginal lesions. Our future work will therefore emphasise the structured documentation and quantification of vaginal lesions to ensure comprehensive assessment and management of FGS. Additionally, we plan to conduct further studies to explore the correlation between cervical lesion proportions and FGS biomarkers such as CAA and S. haematobium DNA, aiming to deepen our understanding of cervico-vaginal lesion pathophysiology in women with FGS. Likewise, comparing cervical lesion proportions with FGS biomarkers could provide additional validation for the DGIT tool as a diagnostic instrument.
Conclusion
The DGIT was found to be a reliable tool for assessing and quantifying cervical lesions in women with FGS. Both inter- and intra-rater agreement were good to excellent; the DGIT may thus serve as a valuable tool for future control programs in schistosomiasis-endemic areas. While the use of a digital camera for documenting and storing cervical images proved highly applicable, future studies should prioritise optimisation of image quality.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Committee of Ethics at the Ministry of Health in Antananarivo (Comité d’Ethique de la Recherche Bio-Médicale auprès du Ministère de la Santé Publique); (Authorization Number: 098-MSANP/CERBM; Number: 059-MSANP/CERBM; Number: 065 MSANP/SG/-AGMED/CNPV/CERBM). The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because Since girls can be affected by FGS since pre-puberty, and life-threatening sequels of FGS may already occur at an adolescent age, we considered it unethical to exclude women 15-17-years old from the study. To respect confidentiality of these adolescent participants, the informed consent of a third party (parent or legal guardian) was not asked for. The Ethics committee approved this procedure.
Author contributions
SD: Data curation, Formal analysis, Investigation, Methodology, Validation, Writing – original draft. SC: Data curation, Formal analysis, Investigation, Methodology, Validation, Writing – original draft. IS: Data curation, Formal analysis, Investigation, Methodology, Validation, Writing – original draft. KJ: Data curation, Formal analysis, Investigation, Methodology, Validation, Writing – review & editing. BR: Conceptualization, Investigation, Writing – review & editing. PL: Conceptualization, Investigation, Methodology, Project administration, Writing – review & editing. LA: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The study was funded by Merck KGaA, Darmstadt, Germany.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor AS declared a past collaboration with the author(s) PL.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fitd.2024.1322696/full#supplementary-material
References
1. Orish VN, Morhe EKS, Azanu W, Alhassan RK, Gyapong M. The parasitology of female genital schistosomiasis. Curr Res Parasitol Vector Borne Dis. (2022) 2:100093. doi: 10.1016/j.crpvbd.2022.100093
2. Kjetland EF, Poggensee G, Helling-Giese G, Richter J, Sjaastad A, Chitsulo L, et al. Female genital schistosomiasis due to Schistosoma haematobium. Clinical and parasitological findings in women in rural Malawi. Acta Trop. (1996) 62:239–55. doi: 10.1016/s0001-706x(96)00026-5
3. Kjetland EF, Ndhlovu PD, Mduluza T, Gomo E, Gwanzura L, Mason PR, et al. Simple clinical manifestations of genital Schistosoma haematobium infection in rural Zimbabwean women. Am J Trop Med Hyg. (2005) 72:311–9. doi: 10.4269/ajtmh.2005.72.311
4. Colley DG, Bustinduy AL, Secor WE, King CH. Human schistosomiasis. Lancet. (2014) 383:2253–64. doi: 10.1016/S0140-6736(13)61949-2
5. Odegaard JI, Hsieh MH. Immune responses to Schistosoma haematobium infection. Parasite Immunol. (2014) 36:428–38. doi: 10.1111/pim.12084
6. Helling-Giese G, Kjetland E, Gundersen S, Poggensee G, Krantz I, Feldmeier H. Schistosomiasis in women: manifestations in the upper reproductive tract. Acta Tropica. (1996) 62:225–38. doi: 10.1016/S0001-706X(96)00025-3
7. Kjetland EF, Mduluza T, Ndhlovu PD, Gomo E, Gwanzura L, Midzi N, et al. Genital schistosomiasis in women: a clinical 12-month in vivo study following treatment with praziquantel. Trans R Soc Trop Med Hyg. (2006) 100:740–52. doi: 10.1016/j.crpvbd.2022.100093
8. Sturt A, Bristowe H, Webb E, Hansingo I, Phiri C, Mudenda M, et al. Visual diagnosis of female genital schistosomiasis in Zambian women from hand-held colposcopy: agreement of expert image review. Wellcome Open Res. (2023) 8:14. doi: 10.12688/wellcomeopenres
9. Basu P, Banerjee D, Mittal S, Mandal R, Ghosh I, Das P, et al. Evaluation of a compact, rechargeable, magnifying device to triage VIA and HPV positive women in a cervical cancer screening program in rural India. Cancer Causes Control. (2016) 27:1253–9. doi: 10.1007/s10552-016-0805-7
10. Lamberti O, Bozzani F, Kiyoshi K, Bustinduy AL. Time to bring female genital schistosomiasis out of neglect. Br Med Bull. (2024) 149:45–59. doi: 10.1093/bmb/ldad034
11. Makia CM, Fesuh NB, Amabo EN, Gamba VA, Oluwole AS, Stothard R. Urogenital schistosomiasis (UGS) and female genital schistosomiasis (FGS) in Cameroon: an observational assessment of key reproductive health determinants of girls and women in the Matta Health Area. BMJ Open. (2023) 13:e063392. doi: 10.1136/bmjopen-2022-063392
12. Midzi N, Sangweme D, Zinyowera S, Mapingure MP, Brouwer KC, Kumar N, et al. Efficacy and side effects of praziquantel treatment against Schistosoma haematobium infection among primary school children in Zimbabwe. Trans R Soc Trop Med Hyg. (2008) 102:759–66. doi: 10.1016/j.trstmh.2008.03.010
13. Arenholt LTS, Aaroe KK, Norderud K, Lumholdt M, Randrianasolo BS, Ramarokoto CE, et al. Cervical lesion proportion measure using a digital gridded imaging technique to assess cervical pathology in women with genital schistosomiasis. PloS Negl Trop Dis. (2022) 16:e0009995. doi: 10.1371/journal.pntd.0009995
14. Arenholt LTS, Randrianasolo BS, Rabozakandraina TOO, Ramarokoto CE, Jøker K, Aarøe KK, et al. Repeated versus Single Praziquantel Dosing Regimen in Treatment of Female Genital Schistosomiasis: A Phase 2 Randomised Controlled Trial Showing No Difference in Efficacy. Front Trop Dis - Negl Trop Dis. (2024).
15. Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. (2016) 15:155–63. doi: 10.1016/j.jcm.2016.02.012
16. Kabengele C, Mwangelwa S, Kilembe W, Vwalika B, Inambao M, Moonga V, et al. Female genital schistosomiasis lesion resolution post-treatment with praziquantel in Zambian adults. Am J Trop Med Hyg. (2024) 110:250–3. doi: 10.4269/ajtmh.23-0552
17. Sturt AS, Webb EL, Himschoot L, Phiri CR, Mapani J, Mudenda M, et al. Association of female genital schistosomiasis with the cervicovaginal microbiota and sexually transmitted infections in Zambian women. Open Forum Infect Dis. (2021) 8:ofab438. doi: 10.1093/ofid/ofab438
18. Rasool S, Naz F, Abdul Wahab T, Khidri FF, Riaz H, Abbasi N, et al. Frequency of abnormal Pap smear in patients presenting with postcoital bleeding in Tertiary Care Hospital, Karachi, Pakistan. Trop Doct. (2023) 53:267–70. doi: 10.1177/00494755221151092
19. Holmen SD, Kjetland EF, Taylor M, Kleppa E, Lillebø K, Gundersen SG, et al. Colourimetric image analysis as a diagnostic tool in female genital schistosomiasis. Med Eng Phys. (2015) 37:309–14. doi: 10.1016/j.medengphy.2014.12.007
20. Holmen SD, Kleppa E, Lillebø K, Pillay P, van Lieshout L, Taylor M, et al. The first step toward diagnosing female genital schistosomiasis by computer image analysis. Am J Trop Med Hyg. (2015) 93:80–6. doi: 10.4269/ajtmh.15-0071
21. Søfteland S, Sebitloane MH, Taylor M, Roald BB, Holmen S, Galappaththi-Arachchige HN, et al. A systematic review of handheld tools in lieu of colposcopy for cervicalneoplasia and female genital schistosomiasis. Int J Gynaecol Obstet. (2021) 153:190–9. doi: 10.1002/ijgo.13538
22. Martinez SG, Mbabazi PS, Sebitloane MH, Vwalika B, Mocumbi S, Galaphaththi-Arachchige HN, et al. The WHO atlas for female-genital schistosomiasis: Co-design of a practicable diagnostic guide, digital support and training. PloS Glob Public Health. (2024) 4:e0002249. doi: 10.1371/journal.pgph.000224
Keywords: female genital schistosomiasis, FGS, digital image, validation, cervical lesion, Schistosoma haematobium (S. haematobium)
Citation: Dragsbæk SJ, Carstens SK, Savkov I, Jøker K, Randrianasolo BS, Leutscher PD and Arenholt L (2024) Measurement of cervical grainy sandy patches, homogeneous yellow sandy patches, and abnormal blood vessels proportions in women with female genital schistosomiasis - a clinical validation study of a digital gridded imaging technique. Front. Trop. Dis 5:1322696. doi: 10.3389/fitd.2024.1322696
Received: 16 October 2023; Accepted: 10 July 2024;
Published: 02 August 2024.
Edited by:
Amy S Sturt, University of London, United KingdomReviewed by:
Olimpia Lamberti, University of London, United KingdomJane Maganga, Mwanza Intervention Trials Unit, Tanzania
Copyright © 2024 Dragsbæk, Carstens, Savkov, Jøker, Randrianasolo, Leutscher and Arenholt. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Louise Arenholt, bHRzYUBybi5kaw==