 Upendo O. Kibwana1
Upendo O. Kibwana1 Joel Manyahi1
Joel Manyahi1 Sabrina J. Moyo1,2,3*
Sabrina J. Moyo1,2,3* Bjørn Blomberg2,4
Bjørn Blomberg2,4 Adam P. Roberts3
Adam P. Roberts3 Nina Langeland2,4
Nina Langeland2,4 Stephen E. Mshana5
Stephen E. Mshana5- 1Department of Microbiology and Immunology, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania
- 2Department of Clinical Science, University of Bergen, Bergen, Norway
- 3Department of Tropical Disease Biology, Liverpool School of Tropical Medicine, Liverpool, United Kingdom
- 4Norwegian National Advisory Unit on Tropical Infectious Diseases, Haukeland University Hospital, Bergen, Norway
- 5Department of Microbiology and Immunology, Catholic University of Health and Allied Sciences, Mwanza, Tanzania
Background: Enterococci are becoming clinically more important especially among immunocompromised patients. Of concern are vancomycin resistant enterococci (VRE) which have both intrinsic and acquired forms of resistance. This work aimed to determine the antimicrobial resistance patterns of Enterococcus spp. and characterize VRE isolate obtained from HIV-infected patient using whole genome sequencing (WGS).
Methods:: Antimicrobial susceptibility testing was done on 57 enterococci isolates by both the disk diffusion method and Epsilometer test (E-Test). WGS was performed on VRE isolate determined by E-test.
Results: Out of the 57 enterococci isolates; 58% (33/57) were E. faecalis, 39% (22/57) E. faecium and 4% (2/57) were E. gallinarum. The highest antimicrobial resistance was observed in E. faecalis isolates. The most prevalent antimicrobial resistance was observed towards quinupristin-dalfopristin (56%, 32/57), followed by ciprofloxacin (28%), tigecycline (18%), daptomycin (16%), chloramphenicol (14%), ampicillin and teicoplanin (2%). Multidrug resistance (MDR) was detected in 11% (6/57) of the isolates. Vancomycin resistance and high-level gentamycin resistance (HLGR) were observed in one E. faecium and one E. faecalis isolates respectively. The VRE was typed as ST80, carried vanA and other resistance genes for aminoglycosides, tetracyclines, quinolones and ampicillin. Furthermore, the isolate had chromosomal mutations responsible for quinolone (gyrA (p.S83I) and parC (p.S80I) and ampicillin (pbp5) resistance.
Conclusions: The detection of VRE, HLGR and MDR in the study settings underscores the sustained surveillance of VRE in high-risk groups and institution of infection control measures for prompt identification and isolation of carriers to prevent the spread of VRE in the community and hospital settings.
Introduction
Enterococcus spp. are Gram-positive bacteria found in various natural environments such as human and animal gastrointestinal track, soil and water (1). Although they are primarily regarded as normal flora of human gut, they are responsible for different community and hospital acquired infections such as urinary tract infections, bacteremia, endocarditis, intravenous catheter-related infections, surgical wound infections, and neonatal sepsis (2–4). Most of these infections originate from the gastrointestinal tract of colonized individuals (5).
Infections due to enterococci are often difficult to treat because they are usually resistant to most antibiotics due to either intrinsic resistance mechanisms e.g., towards cephalosporins (6) or acquired resistance mechanisms through mutations or horizontal gene transfer (2). Worldwide, enterococcal infections are reported to be among the four leading causes of nosocomial infections (1). It is reported that enterococci cause almost 15% of the healthcare-associated urinary tract infections in the ICU settings and about 5% to 15% of cases of infectious endocarditis are due to enterococci (7). In Africa the prevalence of enterococcal infections ranges from 2.7% in pediatric patients to 6.2% in a general population (1, 8). In Tanzania a prevalence of 2.1% enterococcal bacteremia was reported among pediatric patients (9).
In recent years, the emerging resistance to glycopeptide antibiotics (vancomycin and teicoplanin) observed in Enterococcus spp. has become one of the most serious issues related to infection control (10). The World Health Organization has listed vancomycin-resistant E. faecium (VREfm) under high priority list of pathogens which new antibiotics are urgently needed (11). Resistance towards vancomycin by Enterococcus spp. is mainly caused by the vanA and vanB genes which are usually acquired via horizontal gene transfer (12). Furthermore, many strains that are resistant to vancomycin also express high-level aminoglycoside resistance (HLAR), which poses a therapeutic challenge due to the ease acquisition and transfer of antimicrobial drug resistance (4). HLAR in enterococci is due to aminoglycoside-modifying enzymes (AMEs) of three classes namely: N-acetyltransferases (AAC), O-adenylyl transferases (ANT), and O-phosphotransferases (APH) (13).
Patients asymptomatically colonized with VRE in the gastrointestinal tract act as both a reservoir and a source for dissemination of VRE into the environment. In addition, many of VRE infections originate from the gastrointestinal tract of colonized individuals (5). HIV-infected individuals who are more likely to receive multiple antibiotic therapy and have frequent contact with the healthcare system, have been associated with an increased risk of infections including vancomycin resistant enterococcal infections (14).
Vancomycin resistance is usually accompanied by resistance to other antimicrobial agents, such as penicillin, ampicillin, erythromycin, ciprofloxacin and gentamicin (15). Several studies in different parts of the world have reported high resistance rates to other antimicrobial agents among VRE isolates (1, 16, 17). Understanding the mechanisms underlying antimicrobial resistance requires molecular epidemiological analysis for clinical management of infections, including active surveillance and rapid recognition of outbreaks (18). Importance of whole-genome sequencing (WGS) in identifying reservoirs of multidrug-resistant organisms and transmission of these pathogens has been documented (19).
Despite the emerging importance of Enterococcus spp. as multidrug-resistant pathogens around the world including Africa, and the high burden of HIV infection in Tanzania, there is a paucity of data on the colonization and antimicrobial resistance pattern of Enterococcus spp. in Tanzania. Furthermore, there is little information (20) on the molecular characterization of VRE using whole genome sequencing in the African continent as whole. This study, therefore, was conducted to report the colonization and antimicrobial susceptibility patterns of the Enterococcus spp. and further characterize VREfm isolate by whole genome sequencing.
Materials and methods
Study design and study population
This was a laboratory- based retrospective study using archived isolates obtained between April 2017 to May 2018 from newly diagnosed HIV infected adults in Dar es Salaam, Tanzania who were part of the randomized clinical trial CoTrimResist (ClinicalTrials.gov identifier: NCT03087890, registered on 23rd March, 2017). Sample size for the present study was determined by using the Kish Lisle (Kish,1967) formula below:
Considering P to be 7.7%, the reported magnitude of VRE colonization among HIV infected people in Sudan (82), and assuming at Z=1.96 and ϵ= margin of error at 7%, a minimum of 56 samples were required for the study.
Specimen and data collection
From each participant, a rectal swab was collected and transported in liquid Cary-Blair medium (Fecal Transwab, MWE Co Bath Ltd., Corsham, United Kingdom) in a cool box and maintained at -80°C until the time of processing. REDCap system (Research Electronic Data Capture, Vanderbilt University, Nashville, TN) was used by healthcare workers to collect demographics and clinical information including age, sex, height, weight, current and previous hospitalizations and HIV clinical staging.
Microbiological procedures
Bacterial culture and identification
Rectal swabs were inoculated into brain heart infusion (BHI) broth and incubated for 24 hours at 37°C. Two drops (0.1 mL) from BHI broth were sub-cultured on ChromID VRE media (BioMérieux, Marcy l’Etoile, France) to detect vancomycin resistant enterococci isolates. The plates were incubated at 37°C for 24 hours and positive growth was interpreted as a possible VRE isolate.
Bacterial isolates were identified to species level by Matrix-assisted laser desorption/ionization-time of flight (MALDI-TOF) mass spectrometry (MS) using the Microflex LT instrument and MALDI Biotyper 3.1 software (Bruker Daltonics, Bremen, Germany).
Antimicrobial susceptibility testing
Antimicrobial susceptibility was determined by the disk diffusion method, following Clinical and Laboratory Standards Institute (CLSI) (USA) guidelines (21). Muller Hinton agar plates were incubated aerobically at 35°C for 16-18 hours. The antibiotic disks used were; chloramphenicol (30mcg), tigecycline (15mcg), ciprofloxacin (5mcg), quinupristin-dalfopristin (15mcg), teicoplanin (30mcg) and ampicillin (10mcg). All antibiotics were from Oxoid, Basingstoke UK. Also, Minimum Inhibitory Concentration (MIC) was determined by Epsilometer test (E-test) for vancomycin, linezolid, daptomycin antibiotic strips and gentamycin (MIC 500 µg/ml) for detection of high-level resistance (Biomerieux, Marcy-I’Etoile, France). Interpretation of results was done based on CLSI guidelines (21). Intermediate susceptible isolates were regarded as resistant. E. faecalis ATCC 29212 was used a quality control.
Whole genome sequencing and analysis
WGS was performed for one VRE isolate as determined by E-test, using HiSeq (2 × 250 bp paired-end reads protocol) platform by MicrobesNG (MicrobesNG, Birmingham, UK) (22).
Determination of antimicrobial resistance genes and Multi locus sequence type (MLST) were done using ResFinder and MLST tools respectively using the Centre for Genomic Epidemiology database (http://www.genomicepidemiology.org/).
Quality control
All procedures were performed according to manufactures instructions. E. faecalis ATCC 29212 was used a quality control.
Results
Distribution of Enterococcus spp.
A total of 57 Enterococcus spp. were isolated and identified by MALDI-TOF MS. The majority of the isolates (57.9%, 33/57) were E. faecalis followed by E. faecium (38.6%, 22/57) and E. gallinarum were 3.5% (2/57).
Antimicrobial resistant pattern of different Enterococcus species
Antimicrobial resistance rates were more prominent among E. faecalis isolates, up to 87.5% to some antimicrobials, while less resistance was seen among E. gallinarum isolates. As shown in Table 1, out of 57 isolates which grew on CHROMagar™ VRE media, only one was VRE which was E. faecium with MIC value of > 256 µg/ml. The VRE isolate was also resistant to ampicillin and teicoplanin which was not the case for the non-VRE isolates. High-level gentamycin resistance with MIC > 500 µg/ml was observed in one non-vancomycin resistant E. faecalis isolate.
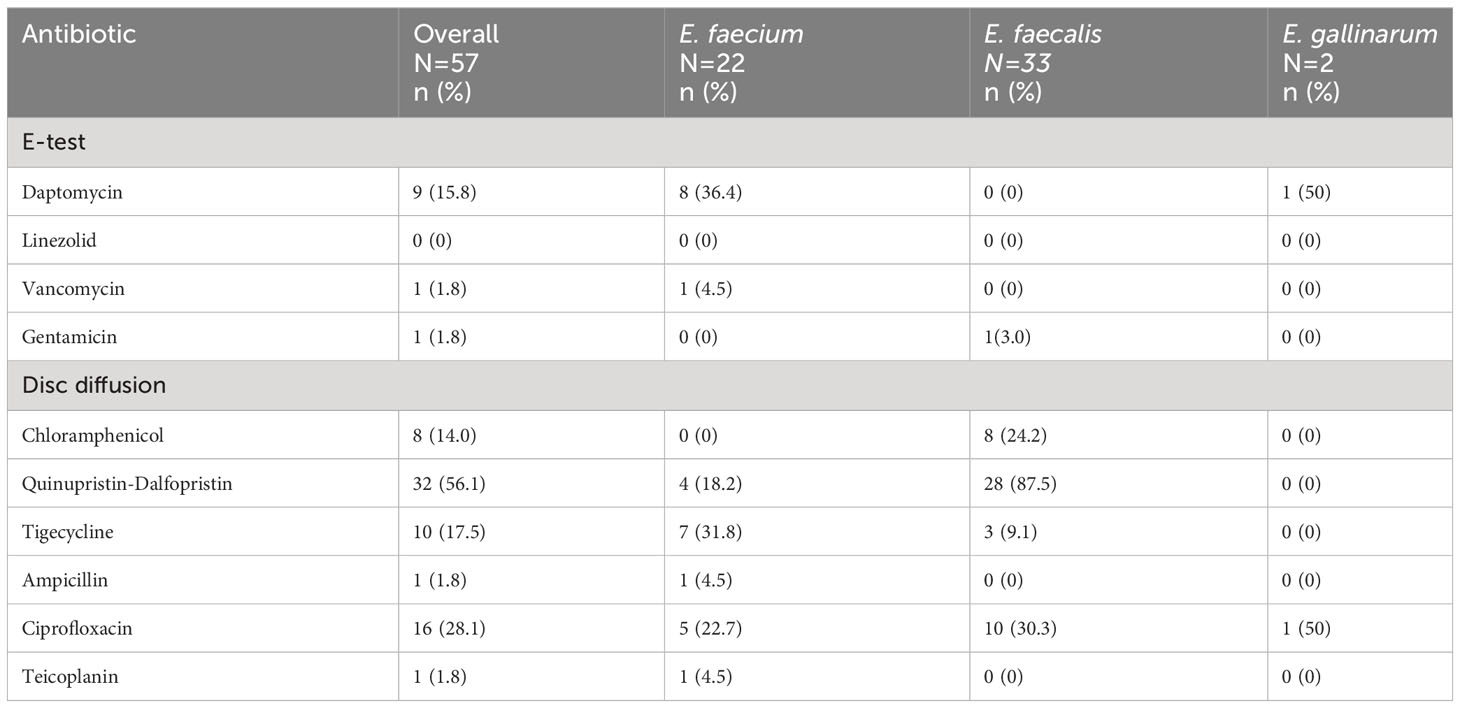
Table 1 Antimicrobial resistance pattern of Enterococcus isolates obtained from newly diagnosed HIV infected adult patients.
Overall, the rate of resistance towards quinupristin-dalfopristin was high (56.1%; 32/57) among Enterococcus species. The resistance towards this antibiotic was higher among E. faecalis (87.5%; 28/33) in comparison to E. faecium (18.2%; 4/22).
Resistance towards daptomycin was only observed in E. faecium isolates (36.4%; 8/22) and none of the Enterococcus spp. were resistant to linezolid.
Six out of 57 of Enterococcus spp. (11%) were also resistant to three or more classes of antibiotics, qualifying them as multidrug resistant bacteria (MDR). The majority of the MDR isolates were resistant to fluroquinolones, tetracycline and streptogramin classes of antibiotics (50%;3/6) as shown in Table 2.
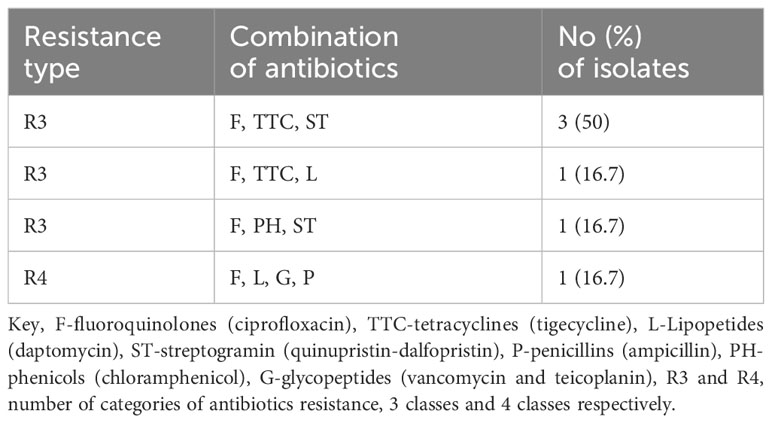
Table 2 Multidrug resistance patterns of Enterococcus spp. isolates obtained from newly diagnosed HIV infected adult patients (n=6).
Molecular characteristics of the VRE isolate
Using Centre for Genomic Epidemiology database (http://www.genomicepidemiology.org/), we found the one VRE isolate harbors vanA gene responsible for vancomycin and teicoplanin resistance. The VRE isolate also carried resistance genes towards aminoglycosides; aph (3’)-III, ant(6)-Ia and aac(6’)-aph(2’’); Streptogramin b msr I and tetracycline; tet (L) and tet (S). In addition to acquired resistance genes, we also found chromosomal mutations responsible for quinolone resistance (dual mutations i.e., gyrA (p.S83I) and parC (p.S80I) as well as ampicillin resistance single mutation pbp5. All tested antibiotics which were resistant by phenotypic method revealed resistance genes by molecular method with exception of quinupristin which was sensitive by phenotypic method, but resistant gene for the antibiotic (msr I) was detected by WGS (Table 3). Furthermore, the VRE isolate also had the virulence factor acm (adhesin of collagen from E. faecium) which mediates E. faecium adherence to collagen. The isolate carried three plasmids; Inc18, Rep3 and RepA-N.
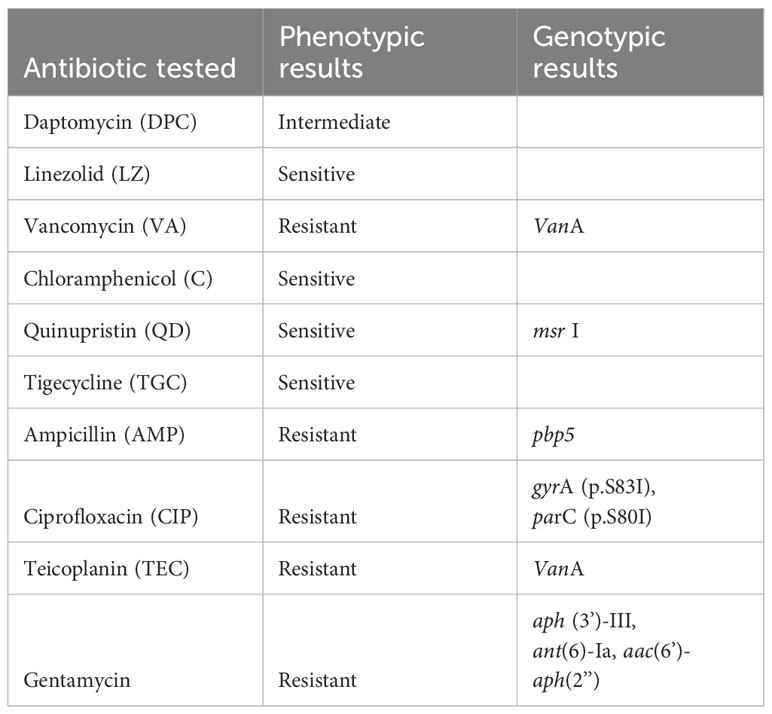
Table 3 Phenotypic and genotypic comparison results for VRE isolate ID 2006.
Based on MLST tool from the Centre for Genomic Epidemiology database (http://www.genomicepidemiology.org/), the VRE isolate belong to sequence type ST80.
Discussion
To date, there is no study in Tanzania which has provided data on Enterococcus spp. among HIV infected people who are among the high-risk group of being colonized as well as getting infections caused by Enterococcus spp. In this study we report the detection of multidrug resistant enterococci and VREfm among the newly diagnosed HIV infected patients in Dar es Salaam, Tanzania.
Different Enterococcus spp. are known to cause infections in human, with literature demonstrating high prevalence of E. faecalis among other species (23). This was also the case for the present study, E. faecalis was the most prevalent species among others (57.9%). This finding is in agreement with studies from West Africa, South America and Asia (16, 24, 25). However, dominance of E. faecium has been reported among Enterococcus spp. isolated from the intestinal tract of hospitalized patients in Ethiopia (26) and healthy individuals in Nigeria (5) suggesting diversity in the distribution of Enterococcus spp. across countries. Rarely, enterococci other than E. faecalis and E. faecium are isolated from clinical specimens, unless in immunocompromised or chronically ill patients (27). In the present study we report E. gallinarum carriage (3.5%) in HIV infected patients.
Out of the 57 isolates, 28.1%, 17.5% and 14% were resistant to ciprofloxacin, tigecycline and chloramphenicol respectively which are comparable resistance levels reported among enterococci isolated from HIV patients on anti-retroviral therapy in Ethiopia by Belayneh et al. (28). Comparable resistance rates of enterococci against ciprofloxacin (31.3%) have also been reported in the northern part of Tanzania among patients with infected wounds (29). Contrary to our findings, higher resistance rates of enterococci against ampicillin (47% vs 1.8%) and chloramphenicol (67% vs 14%) were reported in similar settings between 2001-2002 (9, 30), however at that time resistance towards ciprofloxacin was not observed in the isolates, as opposed to the 28.1% resistance against ciprofloxacin reported in the present study. Recent literature from Tanzania (31) indicates ciprofloxacin among the top-ranking antibiotic consumed in the country between 2010-2016 which might not have been the case between 2001-2001 accounting for the differences in ciprofloxacin resistance between the two studies.
Generally, E. faecium are less susceptible to β-lactam agents than E. faecalis because their penicillin-binding proteins (PBPs) have lower affinities for these antibiotics. In this study, resistance to ampicillin was observed among E. faecium isolates only (4.5%). On the other hand, E. faecalis is known to have intrinsic resistance towards quinupristin/dalfopristin (32); this was evident in the present study where we have reported high rate of resistance (87.5%) for quinupristin/dalfopristin among E. faecalis isolates. Multidrug resistant enterococcal infections are usually treated with linezolid and daptomycin. Of concern, we report 36.4% resistance rate towards daptomycin observed among E. faecium isolates including the VREfm. Resistance towards daptomycin has also been reported elsewhere (33). Whilst daptomycin resistance has often been associated with prior daptomycin usage, resistance in the absence of previous exposure has been documented (34). Fortunately, similar to what was reported more than a decade ago in the study setting (30), all isolates were susceptible to linezolid suggesting that linezolid is potentially effective for infections caused by VRE in our settings.
The current study showed that 11% of the isolates were MDR, which higher than the prevalence reported in a neighboring country, Uganda among enterococci isolates obtained from patients attending a national hospital (35). Nonetheless, this finding is much lower compared to reports from Northwest Ethiopia, where the reported prevalence of MDR among HIV infected patients is 92.8% (14). Usually, resistance to vancomycin in Enterococcus spp. is accompanied with resistance to multiple classes of antimicrobials qualifying them as MDR. A study conducted in Northwest Ethiopia had higher prevalence of VRE (7.8%) among HIV infected patients compared to the present study (1.8%), therefore the difference in percentage of VRE isolates may account for the differences of the reported MDR rate between the two studies. Furthermore, the Ethiopian study determined VRE isolates by disk diffusion method which is associated with false positive results due to lower sensitivity in VRE detection compared to molecular methods (36) used in the present study, possibly accounting for the difference in percentage between the two studies.
Combination therapy of an aminoglycoside with β-lactams drugs such as penicillin/ampicillin is usually used for treatment of serious enterococcal infections. For strains that exhibit high-level aminoglycoside resistance (HLAR), this combination therapy can no longer be used for treatment (37). We report expression of HLGR in 3% of E. faecalis isolates which was also reported in similar settings in a different population (9, 30) Detection of HLGR isolate is worrisome since this resistance determinant is transferable among bacteria via plasmids (38).
We also report presence of VRE in one E. faecium isolate, mediated by vanA gene, the most common mediator of vancomycin resistance in Enterococcus species. Detection of vanA gene in VREfm has also been reported in Europe, Asia and Africa (39–41). The proportion of VREfm reported here (4.5%) is lower than what was reported in Nigeria (42.9%) and Ethiopia (22.7%) (16, 42), but comparable to what has been reported in European countries such as Netherlands (2%) and Belgium (3.5%) (43). Differences in geographical location, the study population and type of specimen analyzed and different detection methods may account for the differences observed. Most of the African studies report VRE based on disk diffusion methods which are associated with false positive results leading to overestimated prevalence. Albeit different study populations, VRE was not detected in the same settings between 2001-2002 (9) more than a decade before the present study. This finding signifies the importance of strengthening surveillance for MDR bacteria including VRE in order to combat the ongoing antimicrobial resistance pandemic.
In the present study, VRE was typed as ST80, this concurs with the studies in other parts of the world (44) where predominance of ST80 among vanA isolates has been reported. The VREfm isolated in this study exhibited dual chromosomal mutations (gyrA, and parC) responsible for quinolone resistance, and it also possessed single mutation (pbp5) for ampicillin resistance. Detection of these mutations aligns with the phenotypic antibiotic susceptibility patterns of the isolate which was resistant to both ciprofloxacin and ampicillin.
The detected virulence factor (adhesin of collagen from E. faecium, (acm)) reported here has been connected with high-risk Enterococcus strains, with a major role of binding to the collagen types I and IV reported in endocarditis infection (45). Although the isolate was from a colonized patient, the detected virulence factor might play a role in pathogenicity should infection occur preceding colonization.
In conclusion the high prevalence of various antimicrobial resistance and the detection of VRE and HLGR isolates in a high-risk group of patients in our setting should be a reason for concern, since infections are usually preceded by colonization and the control of infections resulting from these resistant bacteria is difficult. Therefore, screening of at-risk individuals for VRE colonization should be taken into consideration as one of the infection controlling measures for prompt identification and isolation of carriers to avoid spread of such pathogens within the healthcare settings.
Strength and limitations
The study utilizes a comprehensive approach to investigate the prevalence of Enterococcus spp, antimicrobial resistance patterns, and the molecular characterization of VRE in Tanzania where there is a significant number of people who are regarded as a high-risk population (HIV-infected individuals). The use of WGS in the present study provides insights into the genetic basis of antimicrobial resistance and the characteristics of VRE isolate necessary for infection prevention control measures. However, the small sample size used in the present study might hinder the generalizability of the results and underestimate the prevalence of VRE. Furthermore, WGS testing on one isolate might not provide enough information for the studied population.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: https://www.ncbi.nlm.nih.gov/genbank/, JAUFRI000000000.
Ethics statement
The studies involving humans were approved by CUHAS/BMC Research and Ethical Committee (CREC) with approval number CREC/610/2022. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
UK: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Validation, Writing – original draft, Writing – review & editing. JM: Conceptualization, Data curation, Funding acquisition, Supervision, Validation, Writing – review & editing. SM: Conceptualization, Funding acquisition, Methodology, Supervision, Validation, Writing – review & editing. BB: Funding acquisition, Methodology, Resources, Supervision, Validation, Writing – review & editing. AR: Formal analysis, Methodology, Software, Validation, Writing – review & editing. NL: Methodology, Resources, Supervision, Validation, Writing – review & editing. SM: Conceptualization, Formal analysis, Methodology, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by 1; CAMRIA -Centre for Antimicrobial Resistance in Western Norway, funded by Trond Mohn Foundation, grant number TMS2020TMT11, and 2; STRESST -Antimicrobial Stewardship in Hospitals, Resistance Selection and Transfer in a One Health Context, University of Bergen funded by JPIAMR grant number NFR333432.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Yilema A, Moges F, Tadele S, Endris M, Kassu A, Abebe W, et al. Isolation of enterococci, their antimicrobial susceptibility patterns and associated factors among patients attending at the University of Gondar Teaching Hospital. BMC Infect Dis (2017) 17(1):276. doi: 10.1186/s12879-017-2363-3
2. Ali S, Alemayehu M, Dagnew M, Gebrecherkos T. Vancomycin-resistant enterococci and its associated risk factors among HIV-positive and -negative clients attending dessie referral hospital, northeast Ethiopia. Int J Microbiol (2018) 2018:4753460. doi: 10.1155/2018/4753460
3. Ejaz H. Emerging resistance of van genotype in enterococci: A potential menace for therapeutic failure. Pak J Med Sci (2019) 35:1659–63. doi: 10.12669/pjms.35.6.1145
4. Sood S, Malhotra M, Das BK, Kapil A. Enterococcal infections & antimicrobial resistance. Indian J Med Res (2008) 128(2):111–21.
5. Adesida SA, Ezenta CC, Adagbada AO, Aladesokan AA. Carriage of multidrug resistant enterococcus faecium and enterococcus faecalis among apparently healthy humans Vol. 11. . Lagos, Nigeria: Department Of Microbiology, Faculty of Science, University of Lagos (2017) p. 83–9.
6. Labibzadeh M, Kaydani GA, Savari M. Emergence of high-level gentamicin resistance among enterococci clinical isolates from burn patients in south-west of Iran : vancomycin still working. Pol J Microbiol (2018) 67:401–6. doi: 10.21307/pjm-2018-043
7. Malani PN, Kauffman CA, Zervos MJ. Enterococcal disease, epidemiology, and treatment. Enterococci (2014), 385–408. doi: 10.1128/9781555817923.ch10
8. Abera A, Tilahun M, Tekele SG, Belete MA. Prevalence, Antimicrobial Susceptibility Patterns, and Risk Factors Associated with Enterococci among Pediatric Patients at Dessie Referral Hospital, Northeastern Ethiopia. Biomed Res Int (2021) 2021:5549847. doi: 10.1155/2021/5549847
9. Aamodt H, Mohn SC, Maselle S, Manji KP, Willems R, Jureen R, et al. Genetic relatedness and risk factor analysis of ampicillin-resistant and high-level gentamicin-resistant enterococci causing bloodstream infections in Tanzanian children. BMC Infect Dis (2015) 15:1–9. doi: 10.1186/s12879-015-0845-8
10. Thaker MN, Kalan L, Waglechner N, Eshaghi A, Patel SN, Poutanen S, et al. Vancomycin-variable enterococci can give rise to constitutive resistance during antibiotic therapy. Antimicrob Agents Chemother (2015) 59(3):1405–10. doi: 10.1128/AAC.04490-14
11. WHO. Antimicrobial resistance. Global report on surveillance. World Health Organization (2014). doi: 10.1007/s13312-014-0374-3
12. Sparo M, Delpech G, Allende NG. Impact on public health of the spread of high-level resistance to gentamicin and vancomycin in enterococci. Front Microbiol (2018) 9:3073. doi: 10.3389/fmicb.2018.03073
13. El-Mahdy R, Mostafa A, El-Kannishy G. High level aminoglycoside resistant enterococci in hospital-acquired urinary tract infections in Mansoura, Egypt. Germs (2018) 8:186–90. doi: 10.18683/germs.2018.1145
14. Abebe W, Endris M, Tiruneh M, Moges F. Prevalence of vancomycin resistant Enterococci and associated risk factors among clients with and without HIV in Northwest Ethiopia: A cross-sectional study. BMC Public Health (2014) 14:185. doi: 10.1186/1471-2458-14-185
15. Moemen D, Tawfeek D, Badawy W. Healthcare-associated vancomycin resistant enterococcus faecium infections in the Mansoura university hospitals intensive care units, Egypt. Braz J Microbiol (2015) 46:777–83. doi: 10.1590/S1517-838246320140403
16. Olayinka K, Olufemi S, Sunday S. Prevalence of hospital-acquired enterococci infections in two primary-care hospitals in Osogbo, Southwestern Nigeria. Afr J Infect Dis (2011) 5:40–6. doi: 10.4314/ajid.v5i2.66513
17. Toner L, Papa N, Aliyu SH, Dev H, Lawrentschuk N, Al-Hayek S. Vancomycin resistant enterococci in urine cultures: Antibiotic susceptibility trends over a decade at a tertiary hospital in the United Kingdom. Investig Clin Urol (2016) 57:129–34. doi: 10.4111/icu.2016.57.2.129
18. Oh S, Nam SK, Chang HE, Park KU. Comparative analysis of short- and long-read sequencing of vancomycin-resistant enterococci for application to molecular epidemiology. Front Cell Infect Microbiol (2022) 12:857801. doi: 10.3389/fcimb.2022.857801
19. Brodrick HJ, Raven KE, Harrison EM, Blane B, Reuter S, Török ME, et al. Whole-genome sequencing reveals transmission of vancomycin-resistant Enterococcus faecium in a healthcare network. Genome Med (2016) 8(1):4. doi: 10.1186/s13073-015-0259-7
20. Mbelle NM, Maningi NE. Draft genome sequence of a clinical enterococcus faecium sequence type 18 strain from South Africa. Genome Announc (2017) 5(48):e01381-17. doi: 10.1128/genomeA.01381-17
21. Wayne P. Clinical and laboratory standards intitute performance standards for antimicrobial susceptibility testing. In: CLSI supllement M100, 29th ed, vol. 950. West Valley Road, Suite 2500 Wayne, PA 19087 USA: CLSI (2019).
22. MicrobesNG. Available at: https://microbesng.com/.
23. García-Solache M, Rice LB. The enterococcus: A model of adaptability to its environment. Clin Microbiol Rev (2019) 32(2). doi: 10.1128/CMR.00058-18
24. Bender EA, de Freitas ALP, Reiter KC, Lutz L, Barth AL. Identification, antimicrobial resistance and genotypic characterization of Enterococcus spp. isolated in Porto Alegre, Brazil. Braz J Microbiol (2009) 40:693–700. doi: 10.1590/s1517-83822009000300035
25. Fernandes SC, Dhanashree B. Drug resistance & virulence determinants in clinical isolates of Enterococcus species. Indian J Med Res (2013) 137:981–5.
26. Abamecha A, Wondafrash B, Abdissa A. Antimicrobial resistance profile of Enterococcus species isolated from intestinal tracts of hospitalized patients in Jimma, Ethiopia Microbiology. BMC Res Notes (2015) 8:213. doi: 10.1186/s13104-015-1200-2
27. Dargere S, Vergnaud M, Verdon R, Saloux E, Le Page O, Leclercq R, et al. Enterococcus gallinarum endocarditis occurring on native heart valves. J Clin Microbiol (2002) 40:2308–10. doi: 10.1128/JCM.40.6.2308-2310.2002
28. Dadi BR, Solomon Z, Tesfaye M. Vancomycin resistant Enterococci and its associated factors among HIV infected patients on anti-retroviral therapy in Ethiopia. PloS One (2021) 16:1–12. doi: 10.1371/journal.pone.0251727
29. Kassam NA, Damian DJ, Kajeguka D, Nyombi B, Kibiki GS. Spectrum and antibiogram of bacteria isolated from patients presenting with infected wounds in a Tertiary Hospital, northern Tanzania. BMC Res Notes (2017) 10(1):757. doi: 10.1186/s13104-017-3092-9
30. Blomberg B, Manji KP, Urassa WK, Tamim BS, Mwakagile DS, Jureen R, et al. Antimicrobial resistance predicts death in Tanzanian children with bloodstream infections: a prospective cohort study. BMC Infect Dis (2007) 7:43. doi: 10.1186/1471-2334-7-43
31. Sangeda RZ, Saburi HA, Masatu FC, Aiko BG, Mboya EA, Mkumbwa S, et al. National antibiotics utilization trends for human use in Tanzania from 2010 to 2016 inferred from Tanzania medicines and medical devices authority importation data. Antibiotics (2021) 10:1–16. doi: 10.3390/antibiotics10101249
32. Golob M, Pate M, Kušar D, Dermota U, Avberšek J, Papit B, et al. Antimicrobial Resistance and Virulence Genes in Enterococcus faecium and Enterococcus faecalis from Humans and Retail Red Meat. Biomed Res Int (2019) 2019:2815279. doi: 10.1155/2019/2815279
33. Venter H, Coll F, Rasmussen M, Miller W, Carter GP, Li L, et al. Daptomycin Resistance Occurs Predominantly in vanA-Type Vancomycin-Resistant Enterococcus faecium in Australasia and Is Associated With Heterogeneous and Novel Mutations. Front Microbiol (2021) 12:749935. doi: 10.3389/fmicb.2021.749935
34. Gorrie C, Higgs C, Carter G, Stinear TP, Howden B. Genomics of vancomycin-resistant enterococcus faecium. Microb Genom (2019) 5(7). doi: 10.1099/mgen.0.000283
35. Kateete DP, Edolu M, Kigozi E, Kisukye J, Baluku H, Mwiine FN, et al. Species, antibiotic susceptibility profiles and van gene frequencies among enterococci isolated from patients at Mulago National Referral Hospital in Kampala, Uganda. BMC Infect Dis (2019) 9(1):486. doi: 10.1186/s12879-019-4136-7
36. Sreeja S, Sreenivasa Babu PR, Prathab AG. The prevalence and the characterization of the Enterococcus species from various clinical samples in a tertiary care hospital. J Clin Diagn Res (2012) 6:1486–8. doi: 10.7860/JCDR/2012/4560.2539
37. Weng PL, Ramli R, Shamsudin MN, Cheah YK, Hamat RA. High genetic diversity of Enterococcus faecium and Enterococcus faecalis clinical isolates by pulsed-field gel electrophoresis and multilocus sequence typing from a hospital in Malaysia. BioMed Res Int (2013) 2013. doi: 10.1155/2013/938937
38. Dadfarma N, Imani Fooladi AA, Oskoui M, Mahmoodzadeh Hosseini H. High level of gentamicin resistance (HLGR) among enterococcus strains isolated from clinical specimens. J Infect Public Health (2013) 6:202–8. doi: 10.1016/j.jiph.2013.01.001
39. Markwart R, Willrich N, Haller S, Noll I, Koppe U, Werner G, et al. The rise in vancomycin-resistant enterococcus faecium in Germany: Data from the german antimicrobial resistance surveillance (ars). Antimicrob Resist Infect Control (2019) 8:147. doi: 10.1186/s13756-019-0594-3
40. Zhou W, Zhou H, Sun Y, Gao S, Zhang Y, Cao X, et al. Characterization of clinical enterococci isolates, focusing on the vancomycin-resistant enterococci in a tertiary hospital in China: based on the data from 2013 to 2018. BMC Infect Dis (2020) 20(1):356. doi: 10.1186/s12879-020-05078-4
41. Ekuma AE, Oduyebo OO, Efunshile AM, Konig B. Surveillance for vancomycin resistant enterococci in a tertiary institution in South Western Nigeria. Afr J Infect Dis (2016) 10:121–6. doi: 10.21010/ajid.v10i2.8
42. Toru M, Beyene G, Kassa T, Gizachew Z, Howe R, Yeshitila B. Prevalence and phenotypic characterization of Enterococcus species isolated from clinical samples of pediatric patients in Jimma University Specialized Hospital, south west Ethiopia. BMC Res Notes (2018) 11:281. doi: 10.1186/s13104-018-3382-x
43. Janjusevic A, Markovic Denic L, Minic R, Grgurevic A, Cirkovic I. Intestinal carriage of vancomycin-resistant Enterococcus spp. among high-risk patients in university hospitals in Serbia: first surveillance report. Ann Clin Microbiol Antimicrob (2021) 20:18. doi: 10.1186/s12941-021-00423-0
44. Benammar S, Pantel A, Aujoulat F, Benmehidi M, Courcol R, Lavigne JP, et al. First molecular characterization of related cases of healthcare-associated infections involving multidrug-resistant enterococcus faecium vana in Algeria. Infect Drug Resist (2018) 11:1483–90. doi: 10.2147/IDR.S164487
Keywords: antimicrobial resistance, ciprofloxacin, HIV-infected adults, vancomycin, vancomycin resistant enterococci
Citation: Kibwana UO, Manyahi J, Moyo SJ, Blomberg B, Roberts AP, Langeland N and Mshana SE (2024) Antimicrobial resistance profile of Enterococcus species and molecular characterization of Vancomycin resistant Enterococcus faecium from the fecal samples of newly diagnosed adult HIV patients in Dar es Salaam, Tanzania. Front. Trop. Dis 5:1307379. doi: 10.3389/fitd.2024.1307379
Received: 05 October 2023; Accepted: 16 January 2024;
Published: 13 February 2024.
Edited by:
Mohammad Reza Arabestani, Hamadan University of Medical Sciences, IranReviewed by:
Tahereh Navidifar, Shoushtar Faculty of Medical Sciences, Shoushtar, IranNizami Duran, Mustafa Kemal University, Türkiye
Copyright © 2024 Kibwana, Manyahi, Moyo, Blomberg, Roberts, Langeland and Mshana. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sabrina J. Moyo, c2FicmluYS5tb3lvQHVpYi5ubw==