 Vánio André Mugabe1,2,3*†
Vánio André Mugabe1,2,3*† Osvaldo Frederico Inlamea3*†§
Osvaldo Frederico Inlamea3*†§ Sádia Ali3Plácida Maholela3Bibiana Melchior3Argentina Felisbela Muianga3
Sádia Ali3Plácida Maholela3Bibiana Melchior3Argentina Felisbela Muianga3 John Oludele3Andarusse Sumail3Virgílio António3Vanessa Onofre Monteiro3Inocêncio Chongo3
John Oludele3Andarusse Sumail3Virgílio António3Vanessa Onofre Monteiro3Inocêncio Chongo3 Uriel Kitron4
Uriel Kitron4 Guilherme Sousa Ribeiro5,6‡Eduardo Samo Gudo3‡
Guilherme Sousa Ribeiro5,6‡Eduardo Samo Gudo3‡- 1Instituto de Saúde Coletiva, Universidade Federal da Bahia, Salvador, Brazil
- 2Departamento de Ciências e Tecnologia, Universidade Licungo – Quelimane, Zambézia, Mozambique
- 3Departamento de Vigilância, Instituto Nacional de Saúde, Maputo, Mozambique
- 4Department of Environmental Sciences, Emory University, Atlanta, GA, United States
- 5Instituto Gonçalo Moniz, Fundação Oswaldo Cruz, Salvador, Brazil
- 6Faculdade de Medicina, Universidade Federal da Bahia, Salvador, Brazil
The floods associated with the landfall of cyclones Idai and Kenneth in Mozambique between March and April 2019 had a major impact on the country’s public health and placed the affected population at risk for vector- and rodent-borne diseases. Aiming to improve the diagnostic capacity, yield information to guide public health responses, and assess potential short-term effects of cyclones Idai and Kenneth on arboviruses (dengue, Zika, and chikungunya) and leptospirosis, a clinical and laboratory surveillance for non-malarial acute febrile illness was established in six health units located in different districts within the two provinces (Sofala and Cabo Delgado) affected by the cyclones. Patients were tested using real-time reverse transcriptase polymerase chain reaction (qRT-PCR) for dengue (DENV), Zika (ZIKV), and chikungunya (CHIKV) viruses and using enzyme linked immunoassays (ELISA) to detect nonstructural DENV protein 1 (NS1), as well as DENV, ZIKV, CHIKV, and Leptospira IgM antibodies. From April to September 2019, 305 patients aged ≥15 years were enrolled, of which 58.4% were women and the median age was 30 years old. All patients were qRT-PCR negative for the targeted arboviruses, but three (1.0%) were positive for DENV NS1 ELISA. Specific IgM antibodies against DENV, ZIKV, CHIKV or Leptospira were found in the serum of 104 (34.1%) patients. Our results indicate that vector- and rodent-borne disease transmission occurred in all districts under investigation in the wake of cyclones Idai and Kenneth, including some regions where cases had not been previously detected. The investigation provided useful information for post-cyclone emergency response purposes.
Introduction
Mozambique’s geography predisposes the country to repeated weather-related events, such as severe droughts, storms, and floods. These extreme weather events exacerbate the disease burden in the country and reveal the fragility of the health system in dealing with multiple hazards (1). In mid-March and late April 2019, the Mozambican provinces of Sofala (in the central region) and Cabo Delgado (in the northern region) were massively hit by cyclones Idai and Kenneth, respectively [both were category 4 on the 1-5 Saffir-Simpson hurricane wind scale (2)], resulting in heavy rains and floods. Both cyclones caused wide destruction of dwellings and other essential infrastructures, left ∼2.2 million people in need of humanitarian assistance and protection, and were responsible for a direct death toll of 648 people (1, 3).
As the risk of climate-sensitive diseases tends to increase after devastating disasters (4), the occurrence of outbreaks became an immediate public health concern in Mozambique, given the displacement of hundreds of thousands of people who began to live in unhealthy, overcrowded, and flooded environments. An outbreak of cholera and an increase in malaria cases (1) were detected a few weeks after the cyclones hit. In addition, the Ministry of Health, through the National Institute of Health (INS) of Mozambique, reported an upsurge of non-malarial acute febrile illness in the most affected districts (5).
In Mozambique, 70% of the population depends on agriculture and livestock breading, being at increased risk of vector-borne and zoonotic diseases during their daily activities. Although the real burden of arboviral and zoonotic diseases is unknown in the country due to the lack of a surveillance system for these diseases, dengue has been recognized as an emerging public health problem, especially in the city of Pemba, Cabo Delgado province, where it caused two outbreaks, the most recent in 2014 (6, 7). Conversely, although outbreaks of Chikungunya, Zika, and Leptospirosis have not been clearly detected, serological studies have pointed to their endemic transmission across the country (8–13). Furthermore, Aedes mosquitoes (Ae. aegypti and Ae. albopictus) have been found countrywide (14, 15) and unpublished data from a rodent survey carried out by INS before cyclone Idai showed the existence of Rattus norvegicus and Rattus rattus, main species involved in transmission of Leptospira, in the peripheral neighborhoods of the city of Beira. Therefore, it was suspected that, besides malaria, which is known to be endemic in Mozambique (16), arboviral (8, 17, 18) and rodent-borne diseases (13) could be responsible for the rise in the number of acute febrile illness cases.
Despite the recurrence of extreme climate events in Mozambique in recent years, there is still lack of evidence on the occurrence and burden of mosquito-borne viral diseases and rodent-borne infections in the aftermath of these disasters. With the aim of assessing the occurrence and trends of arboviruses (dengue, Zika, chikungunya) and rodent-borne diseases’ (leptospirosis) transmission in the aftermath of cyclones Idai and Kenneth, in order to guide public health responses, a clinical and laboratory surveillance for non-malarial acute febrile illness was established in six health units located in several districts situated in the two provinces (Sofala and Cabo Delgado) that were struck by the cyclones.
Materials and methods
The surveillance system was implemented from April 22nd to September 15th, 2019, in Sofala province, in the districts of Beira, Buzi, Dondo, and Nhamatanda and initiated a month later, on May 22nd, in Cabo Delgado province, in the district of Macomia and in the city of Pemba. The two provinces are located by the Indian Ocean, in the central-eastern and northernmost regions of the country, respectively (see Figure 1). In Sofala, the altitude ranges from ≤ 10 meters of the sea level in Beira, to about 70 meters in Nhamatanda. In Cabo Delgado, the altitude is ≤ 20 meters of the sea level in Pemba city and about 240 meters in Macomia. Based on available data from the electronic real-time mobile surveillance system (EWARS M-alert platform), developed during the emergency period to improve the detection of disease outbreaks, the health facilities that recorded the highest frequency of cases of non-malarial acute febrile illness within a few weeks after the arrival of the cyclones were selected to host the surveillance.
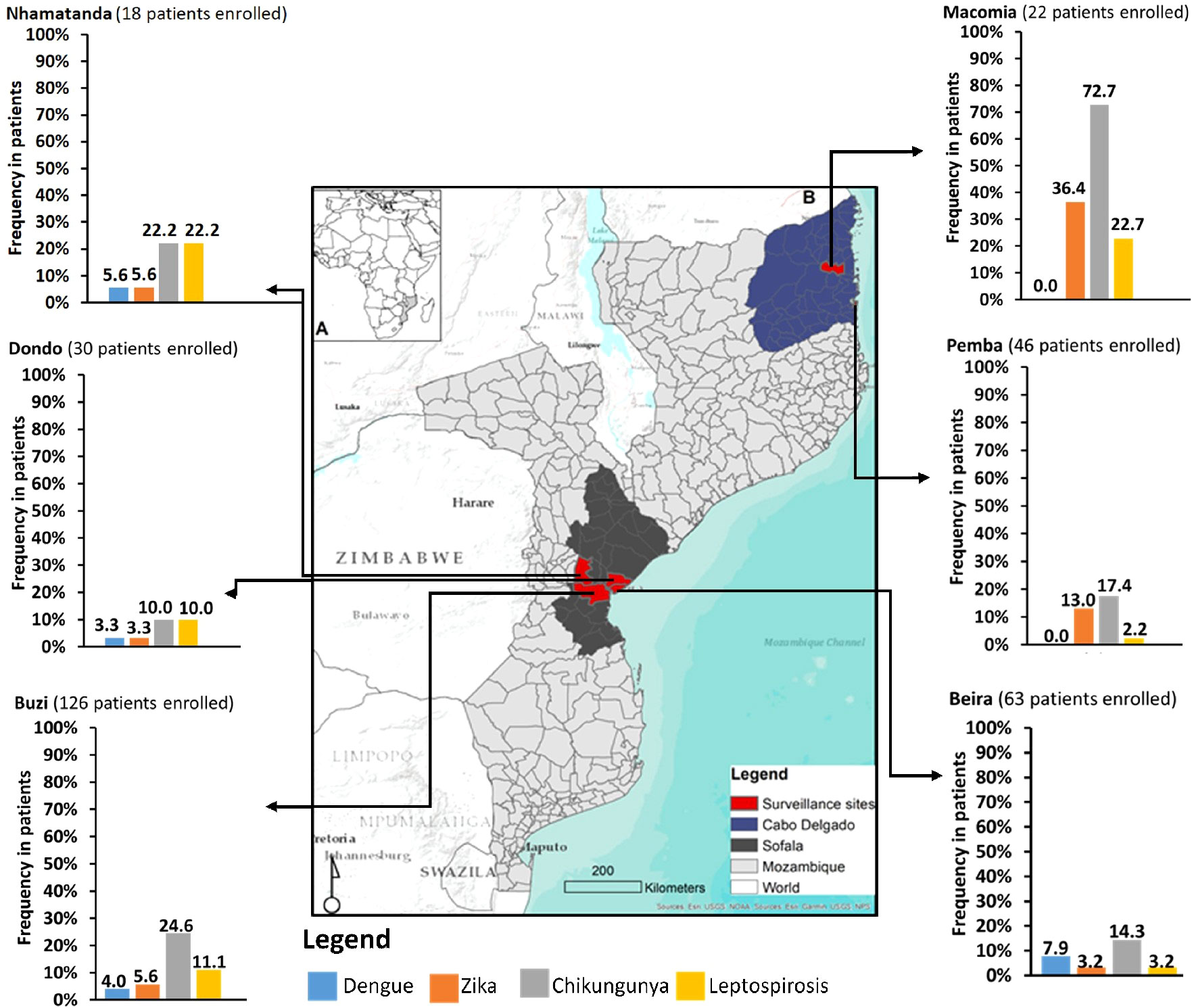
Figure 1 Relative frequencies of patients with laboratory evidence of recent infections by dengue, Zika and chikungunya viruses and by Leptospira sp. among non-malarial outpatients with acute febrile illness following Idai and Kenneth cyclones in six districts of two provinces of Mozambique, April-September 2019.
Clinical and laboratory technicians at each selected health center were trained in bioethics, inclusion and exclusion criteria, proper filling of the survey form, and collection and storage of blood samples for surveillance purposes. The enrollment of participants was closely monitored during the first three days of surveillance in each health center. Patients were considered eligible if they were aged 15 or older (to facilitate blood sample collection), had reported or measured fever (axillary temperature ≥ 37.5° C) lasting up to seven days after the onset of symptoms, and tested negative for malaria on a rapid diagnostic test or blood smear. Patients with pneumonia detected by chest X-ray or with suspected tuberculosis, bronchitis or pharyngitis were also not eligible for study enrollment. Those who met the inclusion criteria were invited to participate in a non-random and non-systematic manner. Daily recruitment of at least five patients per health center was requested. Overall, it was expected to enroll around 600 patients, of whom 400 would be from Sofala and 200 from Cabo Delgado (about 100 patients from each health center).
Prior to enrollment, each patient was informed about the aims and importance of the investigation. For eligible patients under 18 years of age, enrollment occurred if a parent or guardian was present and had authorized. Each patient was enrolled only once and all provided oral consent to participate in this surveillance. The Ethical Research Committee for the National Institute of Health of Mozambique granted ethical approval for the survey.
After consenting, a standardized questionnaire was applied to collect socio-demographic (age, sex, district of provenance) and clinical data (e.g. fever, arthralgia, myalgia, rash) and ∼10 ml of blood was obtained for further tests. Serum was separated from whole blood at the local health centers on the same day and the samples were stored at -20 °C in separate cryovials for subsequent biweekly shipment under cold conditions to the Viral Isolation Laboratory at the National Institute of Health (INS), where the sera were stored at -80 °C until testing.
At INS, sera samples were tested by real-time reverse transcriptase polymerase chain reaction (qRT-PCR) for DENV, ZIKV and CHIKV [Trioplex, Centers for Disease Control and Prevention, Atlanta, USA (19)] and RNA extraction was performed using QIAamp Viral RNA Mini Kit (QIAGEN, Germany). Serum samples were also tested by capture enzyme-linked immunoassays (ELISA) to detect DENV nonstructural protein 1 (NS1) and IgM antibodies against DENV, ZIKV, and CHIKV, using commercially available kits (Euroimmun, Luebeck, Germany). Previous infections by CHIKV and ZIKV were also assessed through detection of IgG using an indirect ELISA (Euroimmun, Luebeck, Germany kits).Testing for the detection of leptospirosis was performed by IgM capture ELISA, using a commercial kit (Leptospira IgM ELISA, Panbio Pty., Ltd., Queensland, Australia). Positive controls were used for both ELISA and qRT-PCR reactions. All tests were performed following manufacturer’s instructions. After testing, data were entered into a Microsoft Excel spreadsheet, double-checked and then shared with provincial health authorities.
Data were imported from Excel into the Stata 14 software (Stata Corp., College Station, TX) for further statistical analyses. The main outcome of interest was acute infection by any of the pathogens under investigation, considered as a positive qRT-PCR or NS1 ELISA test result. Patients in whom IgM antibodies were detected in the serum, regardless of the presence of IgG antibodies, were classified as having evidence of recent infection. Evidence of previous ZIKV and CHIKV infections were also verified, defined by the presence of only IgG antibodies in the serum.
The types of infections were categorized into acute, recent or previous, according to the previous definitions, and as single or dual based on laboratory evidence of infection by one or by more than one pathogen, respectively. Patients’ characteristics were described according to infection types and infecting pathogens, using absolute and relative frequencies, or median and interquartile ranges (IQR). Graphs were used to show the frequency of pathogen-positive patients in each district.
Results
During this investigation, a total of 305 patients were enrolled, of which 237 were from Sofala and 68 from Cabo Delgado. Among them, 178 (58.4%) were women and the median age was 30 (IQR: 23 – 41) years old. Besides fever, headache, arthralgia, myalgia, chills, and weakness were the most common reported symptoms and the median time between fever onset and care seeking was of 3 days (IQR: 2 – 4).
All 305 patients had negative qRT-PCR results for DENV, ZIKV, and CHIKV. However, three (1.0%) patients were positive for DENV NS1 ELISA, indicating an acute DENV infection (one also had IgM antibodies against DENV and CHIKV, suggesting a recent CHIKV infection). In addition, specific IgM antibodies against DENV, ZIKV, CHIKV, or Leptospira were found in the serum of 104 (34.1%) patients, suggesting a recent infection by these pathogens. Of them, 73 (23.9%) had evidence of a recent single infection [7 (2.3%) by DENV, 43 (14.1%) by CHIKV, 6 (2.0%) by ZIKV, and 17 (5.6%) by Leptospira], and 19 (6.2%) had evidence of a recent infection by more than one arbovirus [1 (0.3%) by DENV/ZIKV/CHIKV, 2 (0.7%) by DENV/CHIKV and 16 (5.2%) by ZIKV/CHIKV], and 12 (3.9%) by an arbovirus and Leptospira [3 (1.0%) by DENV/Leptospira, 2 (0.7%) by ZIKV/CHIKV/Leptospira, and 7 (2.3%) by CHIKV/Leptospira]. Previous CHIKV and ZIKV infections, showed by the detection only of IgG antibodies in the serum, were found for 141 (46.2%) patients [117 (38.4%) for CHIKV, 12 (3.9%) for ZIKV and 12 (3.9%) for both]. Table 1 shows demographic and clinical characteristics of patients with and without evidence of infection, according to the type of infection (acute vs recent) and the infecting pathogen. In general, infections by arboviruses were more common among younger patients (median age range: 24-28 years old) and in women, whereas infections by Leptospira were more common in older patients (median age range: 42-50 years old) and in men.
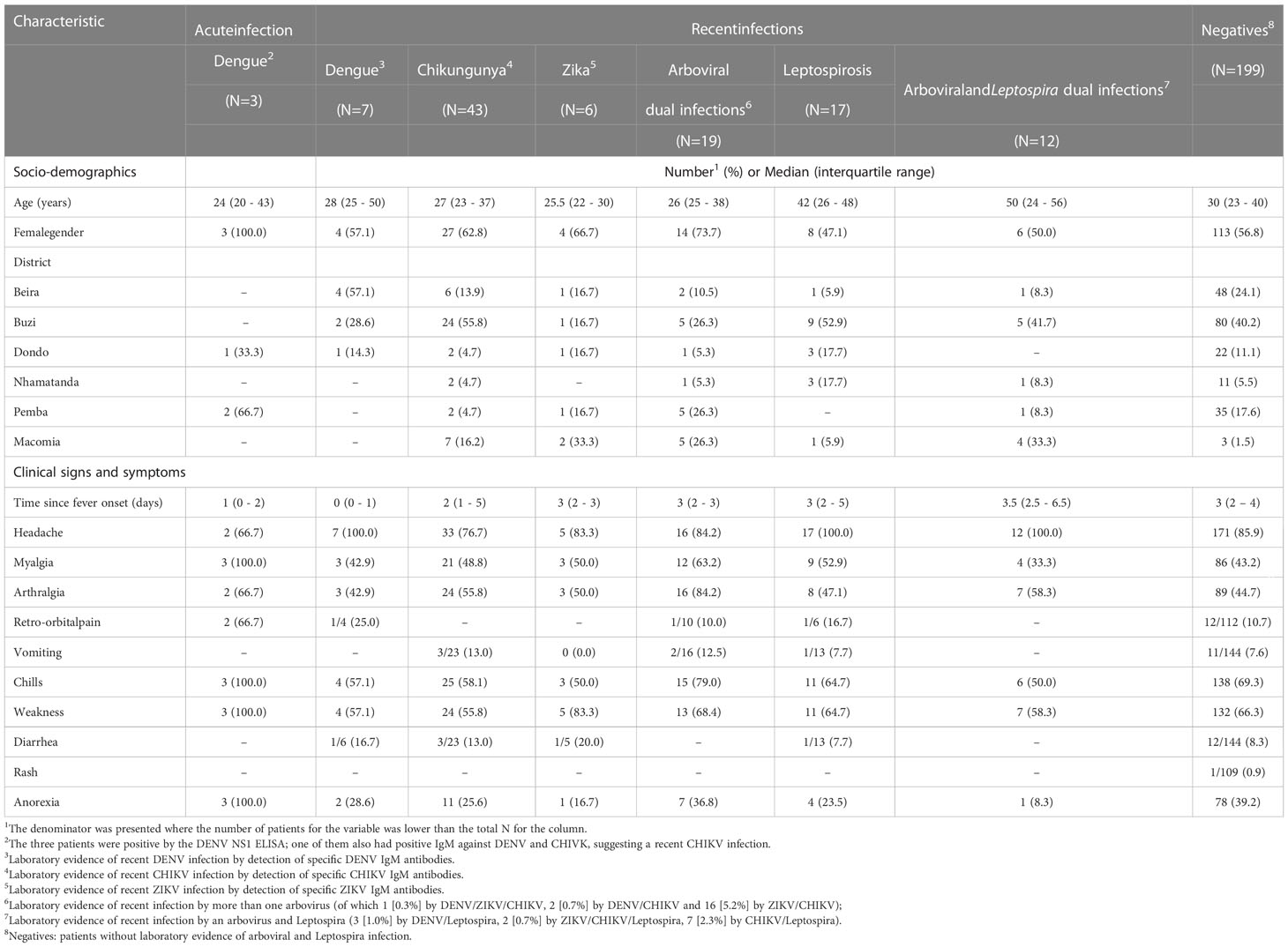
Table 1 Characteristics of acute febrile patients with laboratory evidence of recent infection by dengue, Zika, chikungunya viruses and Leptospira following Idai and Kenneth cyclones in Sofala and Cabo Delgado provinces, Mozambique.
Figure 1 shows the proportion of participants with evidence of recent infection by infecting pathogen and district. All districts had at least one patient with evidence of recent infection for each investigated pathogens, except for Macomia and Pemba, where patients were negative for recent DENV infection. Recent DENV infections were more frequent in Beira, while recent ZIKV infections were more frequent in Macomia and Pemba. Recent CHIKV infection was frequently detected in almost all districts, but its frequency was much higher in Macomia district (72.7%; 16/22) compared to the others. Leptospira infections were more frequent in Nhamatanda (22.2%; 4/18) and Macomia (22.7%; 5/22).
Discussion
The implementation of surveillance actions to investigate and prevent the occurrence of diseases after catastrophes is complex and often not carried out, hampering the production of useful information to guide preparation for further disaster events. This scenario holds true for several countries in sub-Sharan Africa, where data on the occurrence and burden of mosquito-borne viral diseases and rodent-borne infections following severe natural disasters are lacking. Our surveillance system, implemented in response to an increase in non-malarial acute febrile illnesses in the districts most devastated by cyclones Idai and Kenneth in Mozambique, found consistent evidence of transmission of arboviruses and Leptospira. Vector- and rodent-borne diseases are well-known to be impacted by climate events, especially those involving torrential rains and floods. These climate events may create breeding sites for mosquito reproduction and expose the population to water potentially contaminated with Leptospira (20, 21). Outbreaks of Dengue and seroprevalence evidence for Zika, Chikungunya and Leptospirosis (7–10) have been previously reported in the country.
The three patients with a positive DENV NS1 result were detected in the districts of Dondo (1 patient) and Pemba (2 patients), confirming ongoing transmission of DENV in both provinces affected by the cyclones. Recent infections by CHIKV in Macomia and by Leptospira in Macomia and Nhamatanda, recorded after Idai and Kenneth, were higher than the frequencies observed in previous studies developed in areas not affected by cyclones (8, 10, 13). Thus, it is likely that the storms and floods associated with cyclones Idai and Kenneth contributed to the increased frequency of these diseases. However, response actions taken to improve health and minimize potential post-cyclone diseases may have played a role in preventing larger outbreaks of vector- and rodent-borne diseases. The malaria control program promptly intervened, through campaigns of indoor residual insecticide spraying and distribution of insecticide-treated bed nets for the most affected people (22), which may have helped to reduce the mosquito population or exposure to mosquitoes bites, thus decreasing further transmission of arboviruses. In addition, massive interventions to improve drinking water supply and hygiene and sanitation conditions (WASH) (23) might have contributed to the control of rodent-borne diseases. Nevertheless, we highlight that the destruction of natural habitats and the ecological changes induced by cyclones and floods could exacerbate the transmission of arboviruses and leptospirosis in the future.
Establishing a clinical and laboratory surveillance system in the aftermath of a large-scale disaster presented major challenges, as it was not possible to enroll the expected number of patients, nor to collect convalescence samples from patients, due to logistical issues and to large and frequent movement and displacement of people. Some health centers had their infrastructure damaged and the supply of materials for blood collection was intermittent, hampering proper surveillance operation. The low installed capacity for local handling, storage of sera at -20°C before shipping to the INS and challenges in establishing proper transportation, may have compromised the quality of the samples and, consequently, hindered the detection of infections by qRT-PCR. Furthermore, we may have underestimated the frequency of both arboviruses and leptospirosis, as the optimal performance of the IgM ELISA occurs in samples collected 5 days after the onset of symptoms (24, 25). As a positive IgM test could represent current or recent infection, we also cannot rule out that some of the patients in whom IgM antibodies were detected may have had an arbovirus or Leptospira infection that occurred a few weeks earlier and was not the clinical reason for seeking health care. Lastly, the etiology of the non-malarian febrile illness was not found for 65% of the studied patients. Further diagnostic studies of patients seeking health care after a disaster should be broadened to include other pathogens.
An important caveat of this investigation was the absence of baseline, long-term surveillance data to assess the impact of cyclones Idai and Kenneth on the transmission of vector- and rodent-borne diseases. Yet, our investigation provided useful information for the post-cyclone emergency response, including the detection of arboviruses and Leptospira transmission in some regions of the country where cases had not been previously detected. Surveillance has also proven to be an important tool to expand diagnostic capacity and ensure monitoring of vector-borne and rodent-borne diseases in Mozambique. Our findings reinforce the need to consider these diseases in the differential diagnosis of acute febrile illnesses in Mozambique, as well as possible co-infections with malaria.
Given Mozambique’s susceptibility to extreme weather events, the country’s natural disaster emergency preparedness and response plan should continue to be improved, emphasizing the importance of 1) building a robust surveillance and warning systems, within the scope of a One Health approach, to facilitate the early detection of changes in the pattern of occurrence of climate-sensitive diseases throughout the country; 2) using the network of public health laboratories established at national level and equipped with molecular techniques to respond to the covid-19 pandemic, for surveillance and early detection of emerging diseases, including arboviruses and zoonoses; 3) expanding the use of screening algorithms for febrile illnesses in health centers, to increase the probability of suspecting and diagnosing arboviruses and zoonosis, as well as training and expanding health professionals countrywide; 4) and expanding and improving the vector control program, currently focused on malaria control, to include the systematic monitoring of Aedes spp mosquitoes.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Comité institucional de ética do Instituto Nacional de Saúde (CIE-INS). Written informed consent for participation was not provided by the participants’ legal guardians/next of kin because: inclusion was through verbal consent.
Author contributions
VAM, OI, GR, EG and UK conceived the study. VAM, OI, BM, AM, JO and AS collected the data. OI, SA, PM, BM, AM, JO, AS, VA, VOM, IC performed the laboratory work. EG, GR supervision. VAM and OI performed the data analysis and wrote the first draft of the manuscript. GR, UK, EG, revised the data analysis. GR, UK, OI, EG, VAM revised and edited the manuscript. All authors contributed to the article and approved the submitted version.
Funding
The surveillance was funded by the Instituto Nacional de Saúde of Mozambique. VAM and GR received scholarships from the Brazilian National Council for Scientific and Technological Development (CNPq: 311365/2021-3). The funders had no role in the writing of the manuscript or the decision to submit it for publication.
Acknowledgments
We would like to acknowledge the logistical support received from Centro de Investigação Operacional da Beira (CIOB) and Núcleo de Investigação Operacional de Pemba (NIOP). We extend our gratitude to all staff of health centers and their respective health authorities involved in the surveillance, for the support provided and to all patients who attended the survey. We also thank the following institutions for their collaboration: Instituto Nacional de Saúde (INS), Maputo, Mozambique; Instituto de Saúde Coletiva, Universidade Federal da Bahia, Salvador, Brazil; Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Brazil, and Universidade Licungo, Quelimane, Mozambique. The content of the manuscript is part of the VAM doctoral thesis defended on December 1, 2021.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Mugabe VA, Gudo ES, Inlamea OF, Kitron U, Ribeiro GS. Natural disasters, population displacement and health emergencies: Multiple public health threats in Mozambique. BMJ Glob Heal (2021) 6(9):1–11. doi: 10.1136/bmjgh-2021-006778
2. Team TS, Schott T, Landsea C, Hafele G, Lorens J, Thurm H, et al. The saffir-Simpson hurricane wind scale(2009). Available at: https://origin.www.nhc.noaa.gov/pdf/sshws.pdf.
3. MISAU INSO. Tropical cyclones idai and Kenneth, Mozambique national situation report 8, 2nd august 2019(2019). Available at: https://reliefweb.int/report/mozambique/tropical-cyclones-idai-and-kenneth-mozambique-national-situation-report-8-2nd.
4. Kouadio IK, Aljunid S, Kamigaki T, Hammad K, Oshitani H. Infectious diseases following natural disasters: Prevention and control measures. Expert Rev Anti Infect Ther (2012) 10(1):95–104. doi: 10.1586/eri.11.155
5. World Health Organization(WHO). Disease detection in a box – a high-tech solution for emergency settings(2019). Available at: https://www.afro.who.int/news/disease-detection-box-high-tech-solution-emergency-settings.
6. Massangaie M, Pinto G, Padama F, Chambe G, Silva M, Mate I, et al. Clinical and epidemiological characterization of the first recognized outbreak of dengue virus-type 2 in Mozambique , 2014. Am J Trop Med Hyg [Internet] (2016) 94(2):413–6. doi: 10.4269/ajtmh.15-0543
7. Gubler DJ, Sather GE, Kuno G, Cabral JR. Dengue 3 virus transmission in Africa. Am J Trop Med Hyg (1986) 35(6):1280–4. doi: 10.4269/ajtmh.1986.35.1280
8. Mugabe VA, Ali S, Chelene I, Monteiro VO, Guiliche O, Muianga AF, et al. Evidence for chikungunya and dengue transmission in quelimane, Mozambique: Results from an investigation of a potential outbreak of chikungunya virus. PloS One (2018) 13(2):1–13. doi: 10.1371/journal.pone.0192110
9. Aly MM, Ali S, Monteiro V, Gallego JG, Weyer J, Falk KI, et al. Severe chikungunya infection in northern Mozambique: A case report. BMC Res Notes (2017) 88:4–9. doi: 10.1186/s13104-017-2417-z
10. Gudo ES, Pinto G, Vene S, Mandlaze A. Serological evidence of chikungunya virus among acute febrile patients in southern. PLoS Negl Trop Dis (2015) 9(10):1–11. doi: 10.1371/journal.pntd.0004146
11. Chelene IR, Ali S, Mula FI, Muianga AF, Monteiro VO, Oludele J, et al. Retrospective investigation of IgM antibodies against zika virus in serum from febrile patients in Mozambique, 2009-2015. BMC Res Notes (2019) 12(1):469. doi: 10.1186/s13104-019-4511-x
12. Gudo ES, Falk KI, Ali S, Muianga AF, Monteiro V, Cliff J. A historic report of zika in Mozambique: Implications for assessing current risk. PloS Negl Trop Dis (2016) 10(12):1–7. doi: 10.1371/journal.pntd.0005052
13. Ribeiro P, Bhatt N, Ali S, Monteiro V, da Silva E, Balassiano IT, et al. Seroepidemiology of leptospirosis among febrile patients in a rapidly growing suburban slum and a flood-vulnerable rural district in Mozambique, 2012–2014: Implications for the management of fever. Int J Infect Dis [Internet] (2017) 64:50–7. doi: 10.1016/j.ijid.2017.08.018
14. Higa Y, Abílio AP, Futami K, Lázaro MAF, Minakawa N, Gudo ES. Abundant aedes (Stegomyia) aegypti aegypti mosquitoes in the 2014 dengue outbreak area of Mozambique. Trop Med Health (2015) 43(2):107–9. doi: 10.2149/tmh.2014-29
15. Kampango A, Abílio AP. The Asian tiger hunts in Maputo city–the first confirmed report of aedes (Stegomyia) albopictus (Skuse, 1895) in Mozambique. Parasit Vectors (2016) 9(1):76. doi: 10.1186/s13071-016-1361-4
16. Alexandre J, Arroz H. Increase in cases of malaria in Mozambique , 2014 : epidemic or new endemic pattern. Rev Saude Publica (2016), 1–7. doi: 10.1590/S1518-8787.2016050006105
17. Antonio VS, Amade NA, Muianga AF A, S, Monteiro V, Mula F, Chelene I, et al. Retrospective investigation of antibodies against chikungunya virus ( CHIKV ) in serum from febrile patients in Mozambique , 2009 – 2015 : Implications for its prevention and control. PLoS One (2019) 84:2009–15. doi: 10.1371/journal.pone.0213941
18. Gudo ES, Pinto G, Vene S, Mandlaze A, Muianga AF, Cliff J, et al. Serological evidence of chikungunya virus among acute febrile patients in southern Mozambique. PloS Negl Trop Dis (2015) 9(10):1–11. doi: 10.1371/journal.pntd.0004146
19. CDC. Trioplex real-time RT-PCR assay(2016). Available at: https://www.cdc.gov/zika/pdfs/trioplex-real-time-rt-pcr-assay-instructions-for-use.pdf.
20. Kouadio IK, Aljunid S, Kamigaki T, Hammad K, Oshitani H. Infectious diseases following natural disasters: Prevention and control measures. Expert Rev Anti Infect Ther (2012) 10(1):95–104. doi: 10.1586/eri.11.155
21. Naing C, Reid SA, Aye SN, Htet NH, Ambu S. Risk factors for human leptospirosis following flooding: A meta-analysis of observational studies. PloS One (2019) 14(5):1–15. doi: 10.1371/journal.pone.0217643
22. HCT, UNRCO. Humanitarian response plan (Revised following cyclones idai and Kenneth, may 2019). Humanitarian Country Team United Nations Resident Coordinator’s Office Mozambique 2019 (2019). Available at: https://reliefweb.int/report/mozambique/2018-2019-mozambique-humanitarian-response-plan-revised-following-cyclones-idai.
23. Lequechane JD, Mahumane A, Chale F, Nhabomba C, Salomão C, Lameira C, et al. Mozambique’s response to cyclone idai: How collaboration and surveillance with water, sanitation and hygiene (WASH) interventions were used to control a cholera epidemic. Infect Dis Poverty (2020) 9(1):4–7. doi: 10.1186/s40249-020-00692-5
24. Rosa MI, dos Reis MF, Simon C, Dondossola E, Alexandre MC, Colonetti T, et al. ELISA IgM para diagnóstico de leptospirose: Revisão sistemática e meta-análise. Cienc e Saude Coletiva (2017) 22(12):4001–12. doi: 10.1590/1413-812320172212.14112016
Keywords: surveillance, arboviruses, leptospirosis, Cyclones Idai and Kenneth, Mozambique
Citation: Mugabe VA, Inlamea OF, Ali S, Maholela P, Melchior B, Muianga AF, Oludele J, Sumail A, António V, Monteiro VO, Chongo I, Kitron U, Ribeiro GS and Gudo ES (2023) Surveillance for arboviruses and leptospirosis among non-malarial acute febrile illness outpatients in areas affected by Cyclones Idai and Kenneth in Mozambique. Front. Trop. Dis 4:1091545. doi: 10.3389/fitd.2023.1091545
Received: 07 November 2022; Accepted: 01 February 2023;
Published: 15 February 2023.
Edited by:
Bapi Pahar, National Institute of Allergy and Infectious Diseases (NIH), United StatesReviewed by:
Basu Dev Pandey, Everest International Clinic and Research Center, NepalKhin Myint, Eijkman Institute for Molecular Biology, Indonesia
Copyright © 2023 Mugabe, Inlamea, Ali, Maholela, Melchior, Muianga, Oludele, Sumail, António, Monteiro, Chongo, Kitron, Ribeiro and Gudo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vánio André Mugabe, dmFuZHJlbXVAZ21haWwuY29t; Osvaldo Frederico Inlamea, b3N2YWxkby5pbmxhbWVhQGlucy5nb3YubXo=
†These authors have contributed equally to this work
‡These authors share last authorship
§ORCID: Osvaldo Frederico Inlamea, orcid.org/0000-0003-3930-7432