 Jefferson Valente1,2
Jefferson Valente1,2 Paola López Del-Tejo3
Paola López Del-Tejo3 Nadia Carolina Cubas-Vega4
Nadia Carolina Cubas-Vega4 Maria Gabriela de Almeida Rodrigues1,2Francisco Railson Bispo de Barros1,2
Maria Gabriela de Almeida Rodrigues1,2Francisco Railson Bispo de Barros1,2 Márcia Araújo Alexandre2Guilherme Peixoto Tinoco Arêas5
Márcia Araújo Alexandre2Guilherme Peixoto Tinoco Arêas5 Michele Bastos2,5
Michele Bastos2,5 Sérgio Damasceno Pinto2
Sérgio Damasceno Pinto2 Camila Miriam S. S. Barros1,2Eveny Perlize Marinho5Sabrina Mello5Ewerton Ferreira5
Camila Miriam S. S. Barros1,2Eveny Perlize Marinho5Sabrina Mello5Ewerton Ferreira5 Valderjane Aprigio5Rossiclea Lins Monte2
Valderjane Aprigio5Rossiclea Lins Monte2 Vanderson Sampaio1,6
Vanderson Sampaio1,6 Marcus Lacerda1,2,7,8
Marcus Lacerda1,2,7,8 Djane Clarys Baia-da-Silva1,2,5,7,9†
Djane Clarys Baia-da-Silva1,2,5,7,9† Fernando Val1,2,5*†
Fernando Val1,2,5*†- 1Programa de Pós-graduação em Medicina Tropical, Universidade do Estado do Amazonas, Manaus, Brazil
- 2Instituto de Pesquisa Clínica Carlos Borborema (IPCCB), Fundação de Medicina Tropical Doutor Heitor Vieira Dourado, Manaus, Brazil
- 3Facultad de Ciencias de la Salud, Universidad Autónoma de Santo Domingo, Santo Domingo, Dominican Republic
- 4Facultad de Ciencias Medicas, Universidad Nacional Autónoma de Honduras, Tegucigalpa, Honduras
- 5Universidade Federal do Amazonas, Manaus, Brazil
- 6Instituto Todos pela Saúde, São Paulo, Brazil
- 7Instituto Leônidas and Maria Deane, Manaus, Brazil
- 8University of Texas Medical Branch (UTMB), Galveston, TX, United States
- 9Universidade Nilton Lins, Manaus, Brazil
Background: Progressive Multifocal Leukoencephalopathy (PML) is an opportunistic neurological disease that mainly affects individuals with HIV/AIDS and has high morbidity and mortality, due to its demyelinating characteristic. This co-infection has been reported since the begging of HIV/Aids epidemic with increasing unfavorable outcomes, however, factors associated to sequelae and death are greatly unknown. In this study we aimed to understand factors associated with the main outcomes of individuals diagnosed with PML and HIV/AIDS, in addition to reporting the characteristics of patients presenting to a referral center in infectious diseases in the Brazilian Amazon.
Methods: A systematic review was performed until July 2022, following the PRISMA guidelines, at Medline/Pubmed, Web of Science, Lilacs and Scielo databases using combinations of HIV, Aids, JC Virus and Progressive Multifocal Leukoencephalopathy, with no restriction to publication date. Additional cases, meeting the eligibility criteria, were added from our hospital database, which consisted of patients presenting PML/HIV between 2010 and 2022. A meta-analysis aiming to explore factors associated to sequelae and death was performed. Baseline characteristics were described using mean and standard deviation, or median and interquartile range when appropriate; multivariate analysis was performed to study factors associated to death and sequelae outcomes.
Results: Eighteen patients were diagnosed between 2010 and 2022, of these, 10 had positive PCR for JC virus. In the Systematic Review, 216 studies yielded 235 confirmed cases of co-infection. A total of 245 were included for analysis. The rates of death and sequelae were, respectively, 47.1% (114/242) and 41.2% (54/131). The use of antiretroviral therapy was more associated with a lower chance of death (OR 0.30, 95% CI: 0.11-0.83), while muscle weakness (OR 4.82, 95% CI: 2.07-11.21) and muscle spasms (OR 6.12, 95% CI: 1.05-35.76) were associated with greater chances of sequelae.
Conclusion: Those on antiretroviral therapy appear to be less likely to die, and among those who survive, those who have muscle weakness as a symptom on admission are more likely to develop sequelae. Adherence to ART, as well as a comprehensive clinical evaluation and follow-up may help to improve clinical outcomes and awareness of morbidities.
1 Introduction
Progressive Multifocal Leukoencephalopathy (PML) is a rare and usually fatal opportunistic neurological infection caused by the John Cunningham virus (JCV) (1–4). In the vast majority of cases reported in the literature, the infection is associated with immunodeficiencies of different etiological origins, the main ones being immunosuppressive conditions such as Acquired Immunodeficiency Syndrome (AIDS), post solid organ and bone marrow transplant recipients, cancer or immunomodulatory drugs such as natalizumab (1, 2, 5–9). Since 1981, human immunodeficiency virus (HIV) infection and AIDS have been the main predisposing condition for PML, with high rates of morbidity and mortality reported (1, 10–13). Patients using antiretroviral therapy (ART), however, may have an improvement in immunosuppression and consequent stabilization and regression of the disease (3, 14–17).
Despite being a rare disease, PML is of great clinical importance mainly due to the lack of a specific treatment, poor prognosis, and unfavorable outcomes (2, 3, 14). This is related to the central nervous system (CNS) tropism, more specifically to oligodendrocytes, cells responsible for the formation and maintenance of the myelin sheaths (3, 7). Without intervention, permanent sequelae and death are common events (9). Clinically, PML frequently manifests motor symptoms, including monoparesis, hemiparesis, ataxia, and occasionally, extrapyramidal manifestations such as tremors, walk disturbances, spasms, and involuntary movements (12). PML can be diagnosed using molecular methods for detecting JCV, imaging, and/or brain biopsy, which implies that the disease has an easier diagnosis (and consequently higher prevalence) in higher-income countries since it affords the necessary resources (6, 18–20).
The number of new cases of HIV/Aids has been rising in the last years, especially in the western Brazilian Amazon, with several cities above the Brazilian Aids detection rate (21). Despite its importance, evidence on HIV/JCV co-infection is still scarce in low and middle-income countries, like Brazil. Also, the literature, which is mostly based on case reports and case series, lacks evidence regarding the association of risk factors to important clinical outcomes, such as death and sequelae (22–24). The hypothesis of this study is that clinical factors at hospital admission may be predictors of death and sequelae in this population. We performed a systematic review of the literature available for HIV/JCV co-infection and report a series of cases of this co-infection in patients managed at a reference center for the treatment of infectious diseases in the Western Brazilian Amazon. Finally, we present a metanalysis aiming to study risk factors associated with death and sequelae in this population. Moreover, to our knowledge, this is the first study aiming to evaluate risk factors associated with both these outcomes on individuals with HIV/JCV co-infection.
2 Methods
2.1 Ethical considerations
FMT-HVD Ethics Review Board approved this study per the guidelines and standards for regulating research on human subjects established in Resolution 466/12, of the National Health Council of the Brazilian Ministry of Health (CAAE 89665118.6.0000.0005). A waiver of informed consent was obtained due to the retrospective nature of the study. Patient anonymity was preserved throughout data extraction and analysis.
2.2 Case series
All electronic medical records (EMR) of patients treated at Fundação de Medicina Tropical Doutor Heitor Vieira Dourado (FMT-HVD), between January 2010 and July 2022, were screened based on diagnoses. EMRs were carefully evaluated and those containing information from patients diagnosed with PML and HIV were eligible. Patients with confirmed HIV infection and diagnosis of PML were included. Those without a diagnosis of the diseases of interest or with insufficient records in the database were discarded. FMT-HVD is a tertiary-care referral hospital for infectious diseases located in Manaus, Western Brazilian Amazon, which receives patients seeking medical care as well as those referred from public and private healthcare units in surrounding localities. FMT-HVD adopts all Brazilian guidelines for the management of sexually transmitted infections and HIV infection (25), since it belongs to the Brazilian Unified Health Care System (SUS). HIV infection was previously determined by two positive rapid diagnostic tests (Abbott, Chicago, United States and Bio-Manguinhos, Fiocruz, Rio de Janeiro, Brazil) and confirmed by an immunoassay test, as defined by the Brazil Ministry of Health (26). HIV diagnosis, treatment, and follow-up are free of charge to all Brazilians and foreigners. The diagnosis of PML was performed using laboratory confirmation when available. In those cases where this confirmation was not possible/available, the physicians performed the diagnosis following clinical and imaging evaluations accompanied by differential diagnosis. These followed the Brazilian Guidelines for HIV and Co-infections management (25). All physicians are trained and highly experienced in tropical medicine. Before the inclusion of participants in this study, the medical charts were reviewed by experienced physicians who authored this manuscript (MAA and ML). Only those with PCR confirmation for JCV were included in the metanalysis. Data on demographics, clinical, radiological, and/or laboratory diagnosis, length of hospitalization, and any supportive procedures and outcome (sequelae and death) described in the electronic medical records were retrieved from Individual EMRs and sent anonymously to the database. Sequelae were only considered present when there was a detailed description of their characteristics on the medical charts. Muscle weakness was assessed through the capacity of contraction against applied manual resistance, asthenia was described as a feeling of extreme tiredness or generalized lack of physical energy, and spams were described as involuntary contractions, all assessed at hospital admission. Data collection was carried out by two independent researchers in an anonymous manner. Any disagreements were resolved by consensus.
2.3 Systematic review and meta-analysis
An Individual participant data (IPD) systematic review of HIV/AIDS-associated PML was performed in accordance with the Preferred reporting items for a systematic review and meta-analysis of individual participant data (PRISMA-IPD) (27). Studies reporting cases of co-infection were systematically identified from multiple electronic databases (Medline/PubMed, Web of Science, Lilacs, and Scielo), using the following Keywords in the Search strategy: (Hiv AND Progressive Multifocal Leukoencephalopathy) OR (Aids AND Progressive Multifocal Leukoencephalopathy) OR (Hiv AND JC virus) OR (Aids AND JC virus) in English, Portuguese and Spanish. The last search was performed in July 2022, considering all publications, with no restrictions on the start date. All cases included in the systematic review have laboratory confirmation of HIV/JCV co-infection. Suspected or inconclusive cases were discarded. Studies identified by searching the bibliographic references of the articles were also included. Duplicate articles were removed. Additional studies titles and abstracts were reviewed to confirm the inclusion criteria. Included studies were assessed for eligibility by a full-text review (Figure 1). Two independent authors of the study conducted the systematic review process. Disagreements were resolved by consensus. The following data were retrieved: author, year of publication, country, demographic, clinical, and laboratory data. To compose the meta-analysis, we considered all cases reported in the literature identified through the systematic review plus the cases seen at the FMT-HVD (Figure 1). We considered death and sequelae as the main outcomes, which should be clearly stated in the description of the original articles or in the electronic medical record.
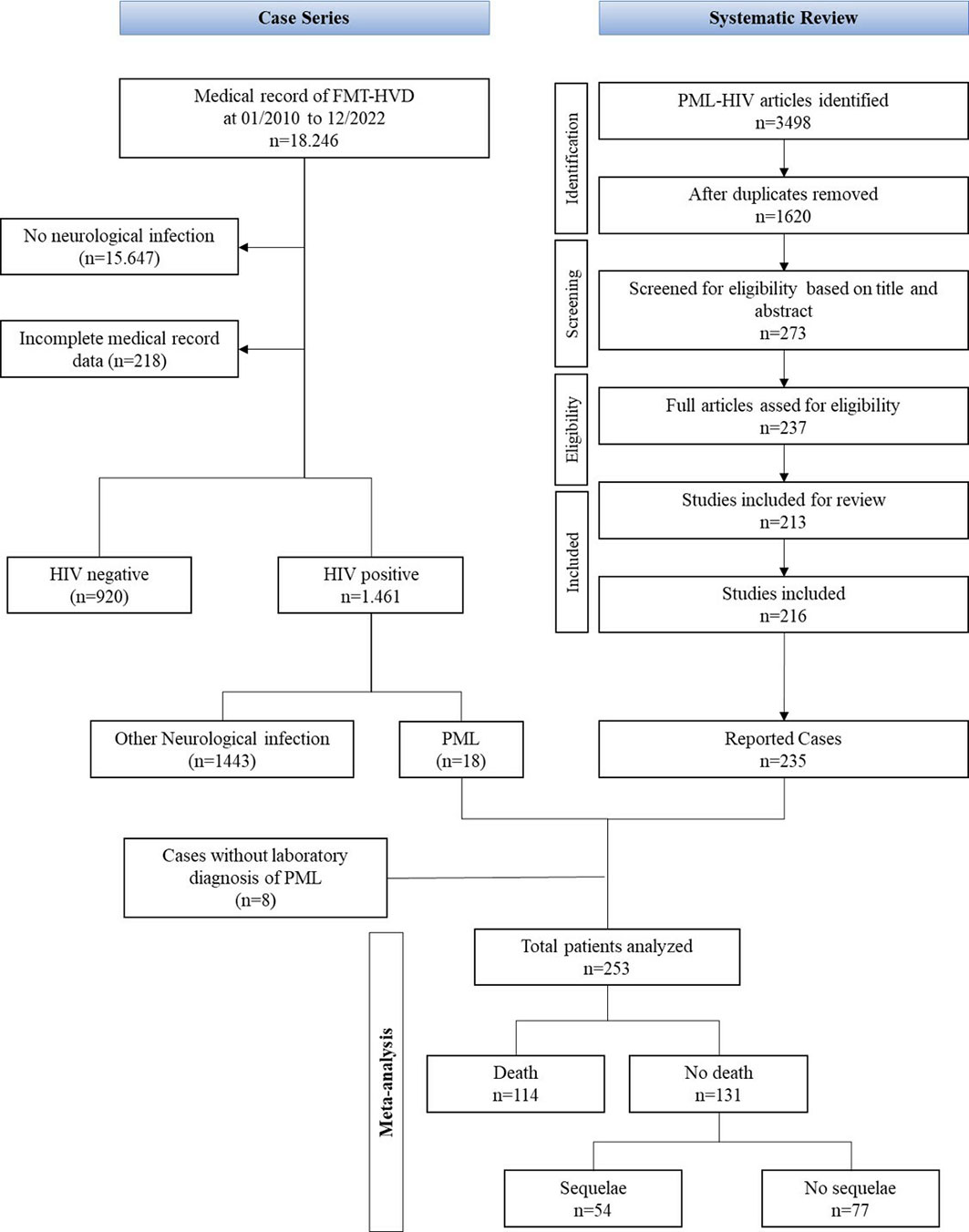
Figure 1 Systematic Review and Case series Flowchart.
2.4 Statistical analysis
The baseline characteristics of individuals were summarized as medians with interquartile range (IQR) or means with standard deviation (SD). The proportions between the groups (sequelae x no sequelae/deaths x non-deaths) were compared using the chi-square or Fisher test for categorical variables. Mean and standard deviation, as well as median and interquartile range, were calculated for continuous variables and analyzed using ANOVA or Wilcoxon test, respectively. Those presenting inclusive data regarding clinical outcomes (sequelae and/or death) were excluded from the analysis. To analyze the factors associated with sequelae and death, univariate and multivariate logistic regression models were applied, using the automatic backward stepwise method. A significance level of p<0.2 in the univariate analysis was considered to compose the multivariate analysis. Statistical significance was considered if p<0.05 in the final multivariate model. All analyzes were performed using the statistical package Stata (v.17).
3 Results
3.1 Case series
A total of 18.246 medical records of patients treated at the FMT-HVD between January 1, 2010 and May 31, 2022 were screened. Of these, 15.647 had no neurological infection, 218 had incomplete data in the medical record, 1.461 were HIV positive and among these, 18 had HIV/AIDS and PML (1.2%) (Figure 1). Table 1 shows a summary of HIV/AIDS and PML patients. Nine (50%) were men. The mean age was 35,2 ( ± 10.7 years), with the youngest patient being 21 (case 7). All had a previous diagnosis of HIV. 61% (11/18) were on regular ART use. Neurotoxoplasmosis (44.4%) and tuberculosis (27.7%) were the most evidenced infectious comorbidities. The mean hospitalization time was 69.2 days. Lumbar puncture for cytochemical analysis was performed in 16 patients (88.9%). Mean glucose and protein in CSF were 57.3 (2-138) and 114.4 (14-831), respectively. Sequelae were evidenced in 10 (55%) patients, and they were mainly related to movement/locomotion. Lesions such as cerebral abscesses/edema and ventricular lesions were less present, and all brain regions were affected (Table 1). Figure 2 shows the magnetic resonance images of case 7, where we can observe the areas of lesion in the white matter (indicated by the arrows): multifocal lesions with emphasis on the involvement of the U fibers and the cerebellar peduncle. In Figure 3, we observe the magnetic resonance images of case 8, where we were also able to identify multifocal lesions in the white matter, with emphasis on the frontal cortico-subcortical involvement, which worsens and extends to the left, reaching the temporal region.
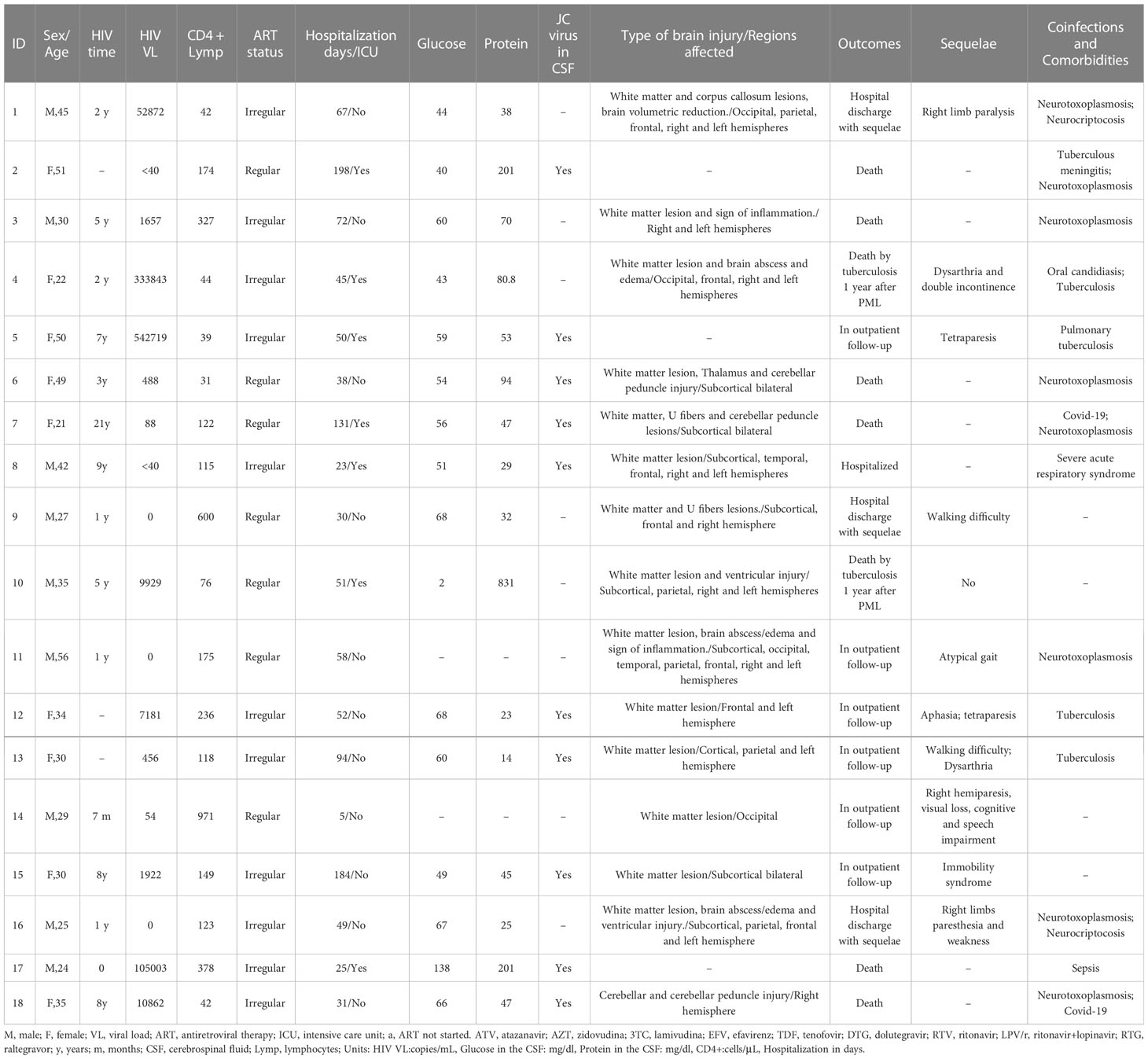
Table 1 Clinical characteristics of patients diagnosed with PML and HIV hospitalized at FMT-HVD.
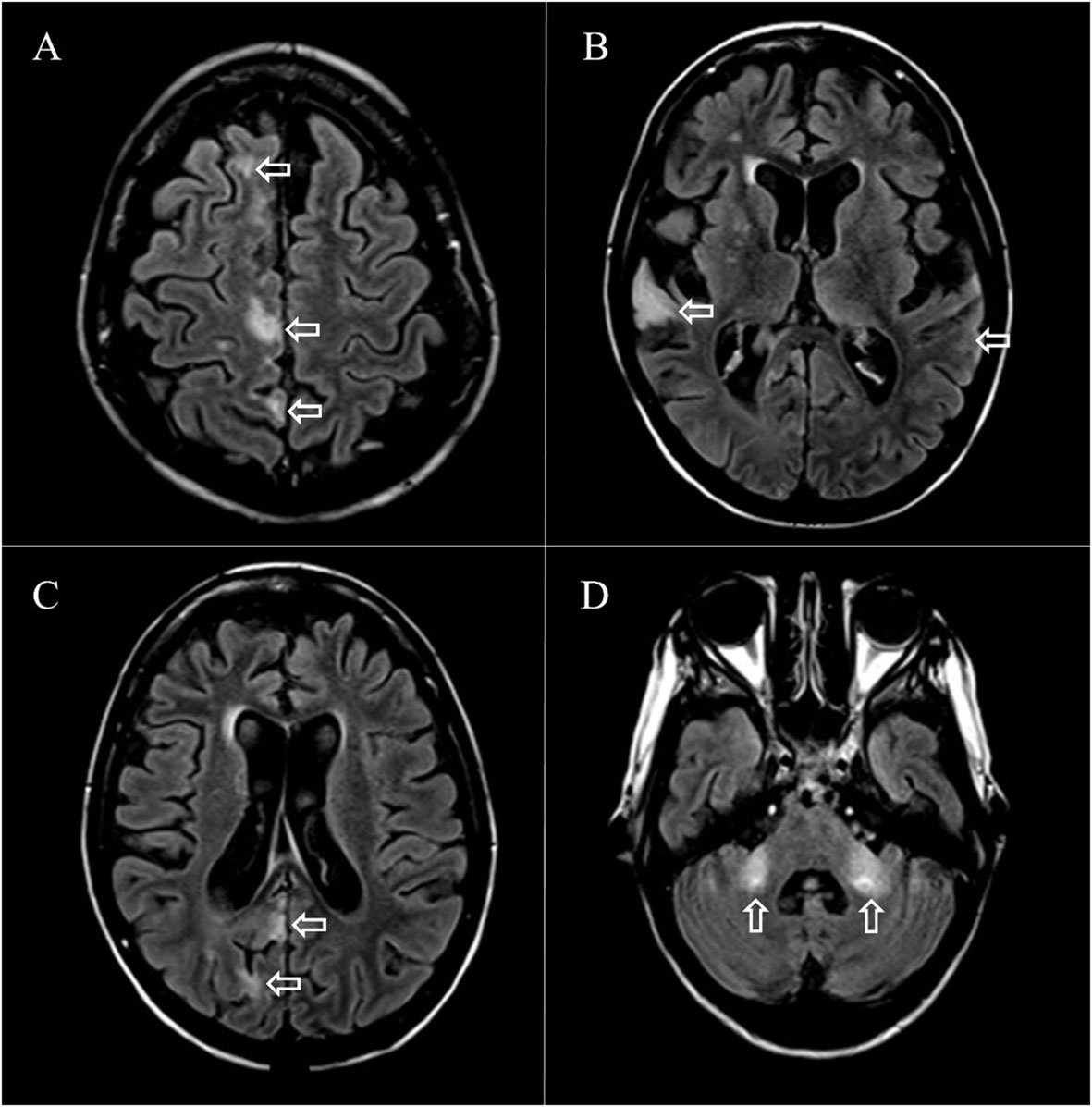
Figure 2 Magnetic resonance imaging findings of case 7: Areas with increased signal and hyperintensity were observed on T2-weighted and FLAIR (Fluid-Attenuated Inversion Recovery) sequences, without contrast enhancement, showing asymmetric, multilobar, and multifocal white matter lesions (A, B) involving U-shaped fibers (C) and affecting the medial cerebellar peduncles bilaterally (D).
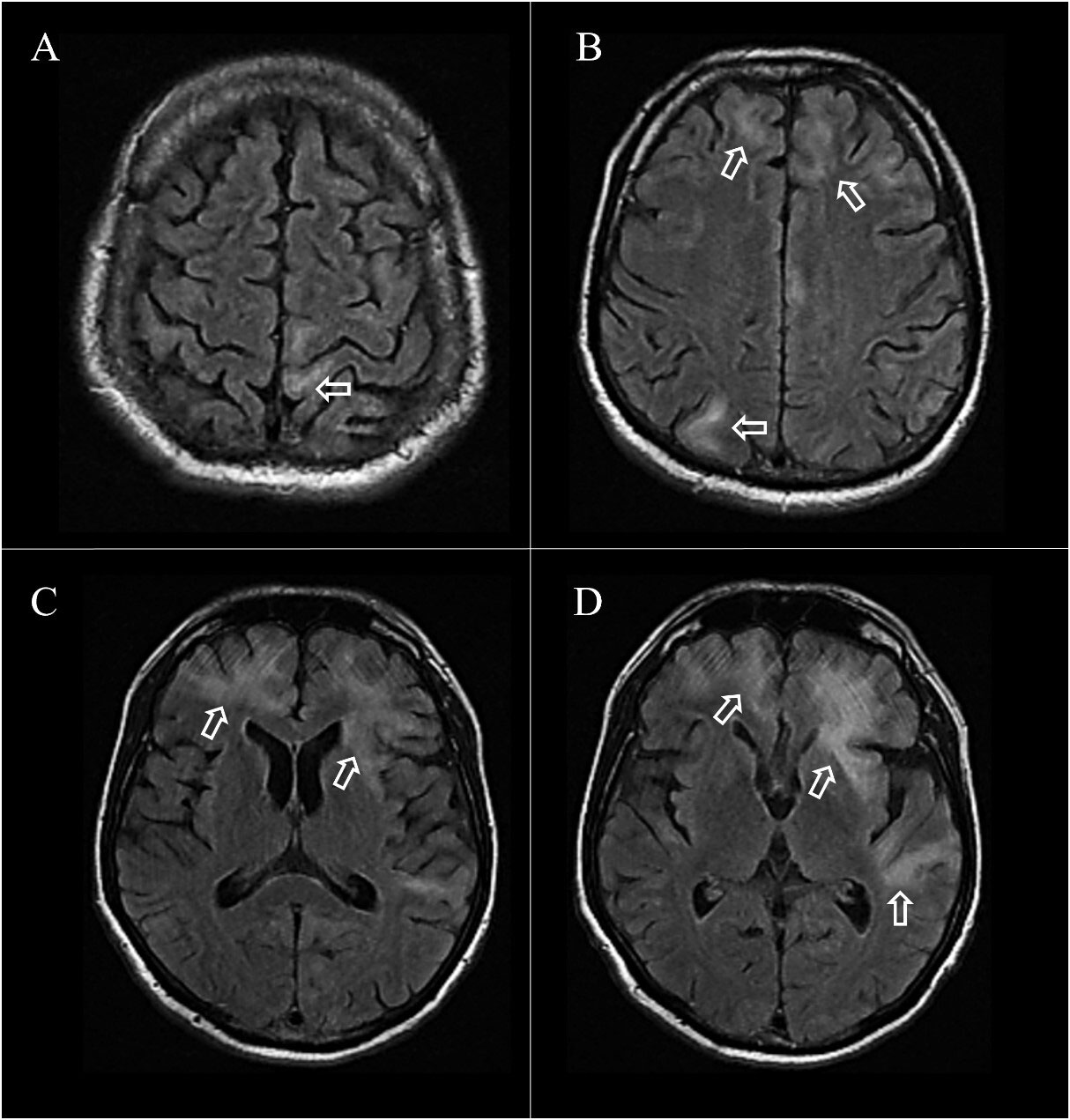
Figure 3 Magnetic resonance findings in case 8: Areas with increased signal and hyperintensity were observed on T2-weighted and FLAIR (Fluid-Attenuated Inversion Recovery) sequences, without contrast enhancement, showing multifocal and bilateral white matter lesions affecting cortical areas (A, B) and greater cortico-subcortical involvement, bilaterally in the frontal region and predominantly in the left hemisphere with extension to the temporal region (C, D).
3.2 Systematic review
The original search yielded 3498 studies. After removing duplicates, applying criteria for study inclusion, and searching for references, 216 studies were considered eligible, covering 235 reported cases (Figure 1). The highest number of related cases and studies was found in high-income countries (78.7%). Supplementary Table 1 describes the characteristics of included patients. The average age was 38.6 (28–42). Most cases were reported in men (78.2%). Upon admission to the health service, the most frequently reported symptoms were limb paresis (52.3%), aphasia (50.2%), ataxia (41.3%), visual changes (31%), cranial nerve palsy (30.2%), changes in consciousness (28%) and muscle weakness (26.8%). A total of 66.6% (55/77) were ART users. Abnormal CT and MRI findings were evidenced in 77.2% (78/101) and 99% (212/214), respectively. In the MRI reports, white matter lesions were the most common finding (90.1%), followed by cerebellar (46.4%) and ventricular (15%) lesions, and the most reported affected brain regions were the parietal and frontal lobes, with frequency of 33% and 29.6%, respectively. None of the patients were using immunomodulatory drugs or underwent any complementary drug therapy. As for the outcomes, 45.9% of the individuals died, and, among the survivors, 38.8% had sequelae, with limb paresis and communication disorders being the most frequent.
3.3 Study outcomes
The characteristics of the total study population (systematic review + case series), according to the outcomes, are shown in Table 2. Muscle weakness (OR 4.82, 95% CI: 2.07-11.21, p=0.001) was considered associated with sequelae on follow-up, while muscle spasm (OR 6.12, 95% CI: 1.05-35.76, p=0.04) also presented positive association, showing that muscular impairments are more associated with post-discharge sequelae (Figure 4B; Supplementary Table 2). ART use (OR 0.30, 95% CI: 0.11-0.83, p=0.02) was less associated with death, in line with what is established about the link between ART and co-infection (Figure 4A; Supplementary Table 2).
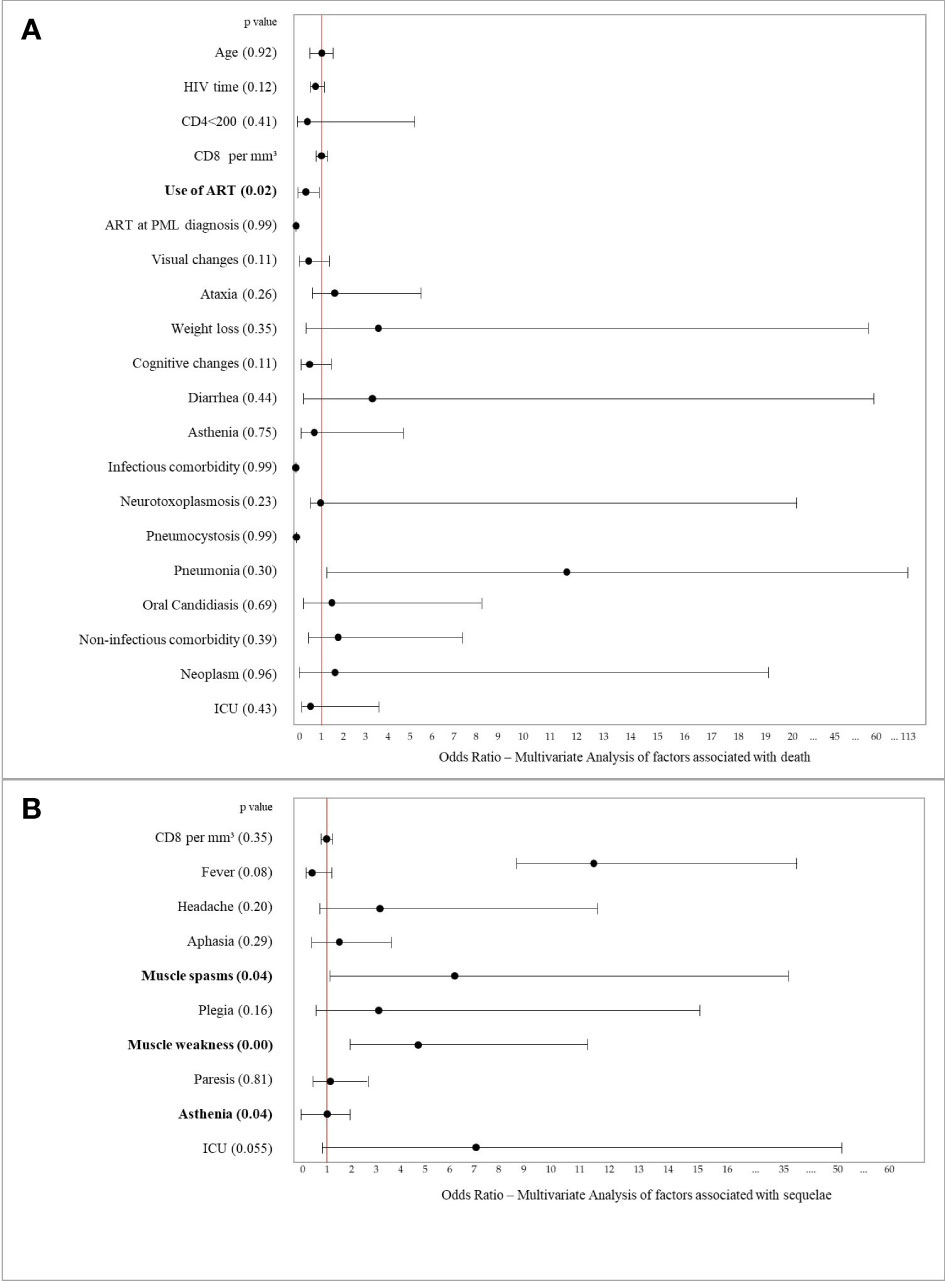
Figure 4 Multivariate analysis of factors related to (A) deaths and (B) sequelae.
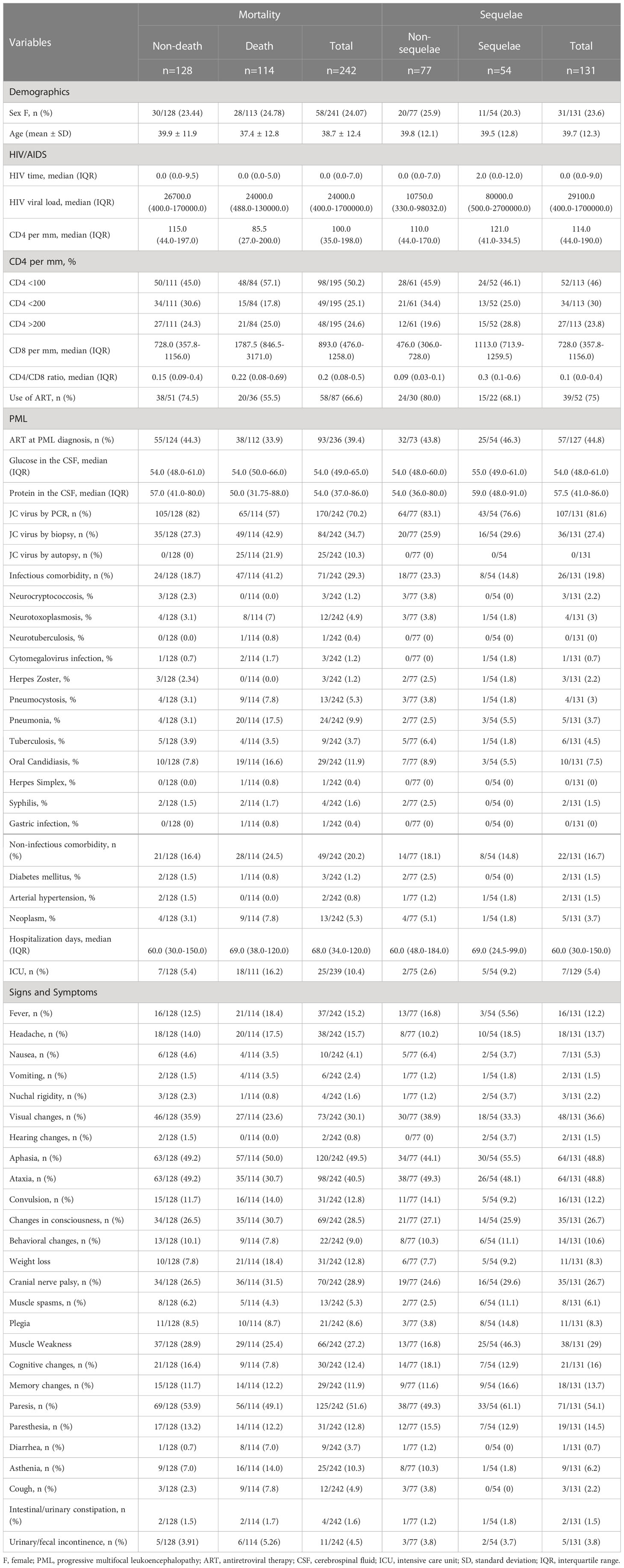
Table 2 Clinical and laboratorial characteristics of the total sample according to mortality and sequelae.
4 Discussion
Opportunistic infections represent the major cause of mortality in individuals living with HIV/AIDS. In addition, sequelae that persist after treatment are important outcomes of opportunistic CNS infections (43, 44). PML stands out with expressive clinical relevance for its lethality and sequelae (2), and although relevant, only 235 cases of HIV/JCV patients are reported in the literature until July 2022, which may be related to the rarity of the disease or the difficulty of timely and/or appropriate diagnosis. Our results showed that muscle weakness and spasms were associated with sequelae in the study population, evidencing that our initial hypothesis did not was null, while the use of ART, as expected and delimited in the literature, showed a lower association with chances of death.
Through our systematic review, we were able to observe that reports of co-infection are scarce in lower-middle and upper-middle income countries (about 22%), such as Brazil. It is important to consider that in low-income countries there is no report of co-infection in the literature, although in these countries HIV infection is highly prevalent (28, 45, 46). PML might be more frequently diagnosed in developing countries where modern diagnostic procedures are more frequently employed (18–20, 24).
PML has been highly associated with HIV and at the height of the AIDS pandemic was present in about 5% of people living with HIV (29). In the pre-ART era, PML affected about 3% to 9% of patients living with HIV infection and was a cause of up to 18% of death (30). Currently, however, the incidence of PML has decreased and life-year rates in patients with HIV and PML have increased, mainly due to antiretroviral therapies, PML is still the second most common cause (14%) of all AIDS-related deaths (31). A hospital-based study recently carried out in São Paulo showed PML in 6% of patients with HIV, a rate similar to the one found in developed countries in the pre-ART era (24). In this study, we showed a low prevalence (1.23%) of HIV and JCV co-infection, 46,8% of the patients died and important sequelae were evidenced. Demographic, clinical and laboratory characteristics presented here are similar to recent reports in different countries (10, 24, 32, 33). Also, the most frequent symptoms presented at admission (limb paresis, aphasia, ataxia, visual changes, cranial nerve palsy, and muscle weakness) are symptoms common to PML (29, 34). PML usually develops in patients with CD4+ lymphocytes < 200 cells/mm3 and can occur in patients receiving ART (35). In our case series, 72,2% (13/18) were immunosuppressed, 33% (6/18) were severely immunosuppressed (CD4+ < 100 cells/mm3), and 61% (11/18) were on regular ART use. These findings differ little from what has been shown in a series of 20 PML/HIV cases in Portugal, where patients were also suppressed and on irregular use of ART, evidencing a high death rate (81%) (36). Here, a lower death rate was evidenced both in our case series (44%) and in our systematic review (47%).
The understanding of the factors associated with PML survival remains lacking (37). Older patients at the onset of PML are significantly different between survivors and non-survivors (38). However, age was not a significant factor for death outcomes in this study, and the use of ART showed a tendency to be an important factor in reducing them. It is known that the treatment of HIV patients with continuous ART and obtaining undetectable levels of viral load are good predictors of survival (14, 15, 39, 40). Thus, the therapeutic approach may include initiating ART in untreated patients or optimizing previous ART regimens (36). Some factors were associated with an improved outcome of PML. Better chances of survival have been correlated with (i) higher CD4+ cell counts at disease onset, (ii) immunological responsiveness, (iii) particularly an improvement in CD4 lymphocyte counts and (iv) reduced JCV load in the CSF (36, 41). Baseline CD4+ count is considered a prognostically significant variable. One study showed that patients with a CD4+ cell count <100 cells/μL have a 2.8 more chance of death (42). In addition, patients harboring JCV-specific CD8+ CD8+ T lymphocytes (CTL) have a significantly increased survival, however, the beneficial effect of CTL is predominant in individuals whose immunosuppression may be reversible, such as in HIV+ patients treated with ART (37), which again evidences the role of therapy in the best outcome associated with survival.
The use of ART and increased survival in people living with HIV and PML has made PML a chronic disease rather than a fatal disease, for this reason, it is important to understand the clinical course of survivors (47). People who survive PML may develop neurological sequelae due to patterns of demyelination in the CNS (48). In our study, 42.8% of the individuals who survived PML had sequelae, the main ones being related to muscle health, movement, locomotion, and communication. Sequelae related to visual disturbances, memory and cognitive functions were also evidenced in our systematic review, although it was observed in only 1 of the 18 cases presented in the case series, although the different regions of the brain that are related to these functions have been shown to be injured. Out of the 18 cases reported, we had access to MRI images of two of them, cases 7 and 8 (Figures 2, 3). In these cases, we observe the multifocal demyelinating lesions in the white matter, which are the main characteristic of PML (49, 50). The main affected regions visualized presented similarity with findings from other studies, with the involvement of U fibers, lesions in the cerebellar peduncle, and lesions with cortical and subcortical involvement (51–54). In an appropriate clinical context, brain imaging can strongly support the diagnosis of PML (49). Since the 1990s, pioneering studies involving patients with PML have already established that cranial MRI is much more sensitive for identifying white matter lesions than methods such as computed tomography (55, 56). In the cases presented here, the lesions were visualized in a hyperintense manner on T2 FLAIR, which is the most sensitive modality for visualizing these lesions (49).
In general, permanent neurological deficits reflect the functional region injured in the infection, interestingly, lesions that affect the cerebellum are associated with ataxia and incoordination of gait, which makes independent living troublesome (47). In addition to white matter lesions, cerebellar lesions, ventricular injury, edema, inflammation, thalamus and corpus callosum injury were frequently evidenced in our study. In the classical form widely described in the HIV population, PML manifests as white matter lesions affecting subcortical U-shaped fibers with a decreased signal on T1-weighted sequences and an increased signal on T2-weighted sequences (57). Contrast enhancement (CE) of PML lesions on CT or MRI is associated with a favorable prognosis if the patient survives (37). Neurodegenerative changes with focal atrophy (including ex vacuo dilatation of CSF spaces) can develop over weeks to months (29). These characteristic findings of PML are also important to differentiate these cases from diseases with similar involvement, such as HIV-associated encephalopathies, characterized by encephalitis and encephalopathies that present cerebral atrophy as the most common finding on magnetic resonance imaging and are reported as lesions that can evolve into the “Dementia Complex Associated with HIV/AIDS”, with symptoms predominantly focused on aspects cognitive, behavioral and memory disorders and, together with Asymptomatic Neurocognitive Disorder (ANI) and Mild Neurocognitive Disorder (DMN) make up the set of diseases called HAND (HIV-Associated Neurocognitive Disorders) (58, 59).
Important neurological sequelae are reported in HIV-PML patients, even though the average survival time has increased for people leaving with HIV since ART (36). However, the factors associated with sequelae are poorly known. In the present study, muscle weakness was significantly associated with the presence of sequelae, with high OR (5.72), with muscle spasms tending to be associated with sequelae. Muscle symptoms have been cited in studies on PML as a prevalent symptom (33, 50, 60). Aspects of muscle tissue health are involved with limb paresis, the most reported sequelae in the studies from our systematic review. Limb paresis is closely associated with peripheral neuropathy. PML and peripheral neuropathy have been described in a man who presented with limb weakness and numbness (61). Spinal cord injuries, such as those caused by JCV, can cause muscle denervation and consequent muscle impairments (62, 63). Muscle health may also be linked to weight loss (and loss of muscle tissue) associated with HIV, which is established in the literature as one of the presentations of people living with HIV (64, 65). The time of disease progression and the patient’s time in bed can also be related to muscle deficits. Most critically ill patients lose muscle because of an inability to maintain protein synthesis rates and showing a decline in muscle health, starting to present muscle weakness, spasms, paresthesias and, in more severe cases, plegia (66–68). The management of critically ill patients in the ICU alone indicates an important risk factor for sequelae regardless of the underlying disease. Neuromuscular weakness and impairments in physical function and quality of life abnormalities are common and can be long-lasting (69–75).
In cases of neurological sequelae, rehabilitation through a multidisciplinary approach, including physical therapy, should be prioritized, aiming to minimize, or even revert, possible disabilities caused by disease; moreover, interventions leading to an individual’s functional capacity and general quality of life are of great importance (76–78). Physical therapy is essential in cases of demyelinating/opportunistic diseases, easing the progression of sequelae and preserving the musculoskeletal tissue in people living with HIV/AIDS (79). Demyelinating opportunistic diseases present a similar spectrum of symptoms that mainly involve motor deficits such as weakness, contractures, gait and balance disorders, among others (24, 56, 78–80). Several studies have already shown the improvement of balance deficits, strength gain, and maintenance of muscle tissue and general functional performance through rehabilitation by a multidisciplinary team (81, 82). Even though the importance of physical therapy in such cases is well known, studies included in this systematic review rarely mentioned any rehabilitation approach. This should be a priority for future studies to better comprehend post-acute disease scenarios.
This study had several limitations. Its retrospective nature of case reports accounts for incomplete data available in patient’s medical charts, mostly due to the absence of detailed targeted investigation, including proper registration of imaging, laboratory studies, adherence to ART therapy, survival time, and greater details about the sequelae and the persistence time in survivors. Patient admission and clinical management were made at the physician’s discretion and may have resulted in classification bias. Of the cases presented, 8 were diagnosed through medical evaluation of clinical presentation, specific findings in imaging tests, and ruling out other diagnostic possibilities, in the absence of confirmation by PCR, biopsy, or autopsy. Regarding the systematic review, prevalence studies and case reports or case series exploring clinical outcomes may underestimate the HIV-PML co-infection and may have influenced the associations of clinical aspects and relevant outcomes, such as sequelae and deaths. The existence of coinfections such as neurotoxoplasmosis (17 cases out of 250), which also favor the appearance of symptoms such as weakness and muscle spasms, is also a limitation since the likelihood to associate these symptoms to one or another is very limited when both are present. In addition, the absence of systematic screening for PML, in general, due to the lack of more sensitive techniques, such as the evidence of JCV in CSF by PCR in low and middle-income countries may reduce the evidence of the high prevalence of this co-infection. In these countries, the diagnosis performed at the discretion of a clinician upon clinical suspicion can impair the rapid and adequate management and treatment which can culminate in unfavorable outcomes. Even so, our findings elucidate aspects not previously addressed about predictive factors of outcomes and death and sequelae of co-infection.
In conclusion, people living with HIV coinfected with JCV using antiretroviral treatment may be less likely to die. Among those who survive, those who have muscle weakness as a symptom on hospital admission are more likely to have sequelae. These findings may contribute to the implementation of a more detailed clinical evaluation, mainly on the muscular aspects of individuals admitted to health units, helping to improve the treatment and specific management of this population to avoid or minimize its sequelae. In addition, our results reinforce the importance of ART by the population living with HIV and/or the regularization of failed schemes, since it is a key factor for better clinical outcomes. In this regard, physical therapy could optimize patient management. Also, the awareness of the occurrence of these important clinical signs may perhaps influence the reduction of mortality rates and long-term morbidities.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author contributions
CB, DB-D-S, FV, GA, JV, ML, NC-V and PD-T participated in study conception and design. JV and PD-T performed the systematic review. JV, NC-V, FB, SP, EM, MA, SM, EF, VA, RM and MB were responsible for collecting and reviewing patient data from the FMT-HVD. JV was responsible for the manuscript writing. FV and DB-D-S critically reviewed the manuscript. MR and VS were responsible for the statistical analysis. All authors read and approved the final manuscript.
Funding
This study was funded by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES)/PROAP 1247/2022. JV received a scholarship from FAPEAM (Fundação de Amparo à Pesquisa do Estado do Amazonas) for the master's degree. MVGL is a fellow from CNPq. DB-D-S was supported by FAPEAM (National Visiting Researcher Scholarship). Funding was also obtained from FAPEAM (FAPEAM/PPP-CNPq, 355 EDITAL N. 016/ 2014 and FAPEAM/PCTI/EMERGESAÚDE/AM, EDITAL N. 006/2020). The funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report. The corresponding author had full access to all data in the study and had final responsibility for submitting it for publication.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fitd.2023.1050477/full#supplementary-material
References
1. Seth P, Diaz F, Major EO. Advances in the biology of JC virus and induction of progressive multifocal leukoencephalopathy. J Neurovirol (2003) 9(2):236–46. doi: 10.1080/13550280390194019
2. Hatchwell E. Is there a (Host) genetic predisposition to progressive multifocal leukoencephalopathy? Front Immunol (2015) 6:216/abstract. doi: 10.3389/fimmu.2015.00216/abstract
3. Engels EA, Rollison DE, Hartge P, Baris D, Cerhan JR, Severson RK, et al. Antibodies to JC and BK viruses among persons with non-Hodgkin lymphoma. Int J Cancer (2005) 117(6):1013–9. doi: 10.1002/ijc.21277
4. Tan CS, Ellis LC, Wüthrich C, Ngo L, Broge TA, Saint-Aubyn J, et al. JC virus latency in the brain and extraneural organs of patients with and without progressive multifocal leukoencephalopathy. J Virol (2010) 84(18):9200–9. doi: 10.1128/JVI.00609-10
5. Ferenczy MW, Marshall LJ, Nelson CDS, Atwood WJ, Nath A, Khalili K, et al. Molecular biology, epidemiology, and pathogenesis of progressive multifocal leukoencephalopathy, the JC virus-induced demyelinating disease of the human brain. Clin Microbiol Rev (2012) 25(3):471–506. doi: 10.1128/CMR.05031-11
6. Bartsch T, Rempe T, Leypoldt F, Riedel C, Jansen O, Berg D, et al. The spectrum of progressive multifocal leukoencephalopathy: a practical approach. Eur J Neurol (2019) 26(4):566–e41. doi: 10.1111/ene.13906
7. Amend KL, Turnbull B, Foskett N, Napalkov P, Kurth T, Seeger J. Incidence of progressive multifocal leukoencephalopathy in patients without HIV. Neurology (2010) 75(15):1326–32. doi: 10.1212/WNL.0b013e3181f73600
8. Meza LF, Walia R, Buddhdev B, Muley S, Tokman S. Progressive multifocal leukoencephalopathy presenting as expressive aphasia in a lung transplant recipient. J Hear Lung Transplant (2022) 41(4):S281. doi: 10.1016/j.healun.2022.01.690
9. Tan CS, Koralnik IJ. Progressive multifocal leukoencephalopathy and other disorders caused by JC virus: clinical features and pathogenesis. Lancet Neurol (2010) 9(4):425–37. doi: 10.1016/S1474-4422(10)70040-5
10. Piza F, Fink MC, Nogueira GS, Pannuti CS, de Oliveira ACP, Vidal JE. JC virus-associated central nervous system diseases in HIV-infected patients in Brazil: clinical presentations, associated factors with mortality and outcome. Braz J Infect Dis (2012) 16(2):153–6. doi: 10.1016/S1413-8670(12)70297-0
11. Skiest DJ. Focal neurological disease in patients with acquired immunodeficiency syndrome. Clin Infect Dis (2002) 34(1):103–15. doi: 10.1086/324350
12. Baqi M, Kucharczyk W, Walmsley SL. Regression of progressive multifocal encephalopathy with highly active antiretroviral therapy. AIDS (1997) 11(12):1526–7.
13. Pasqualotto AC, de Mattos AJZ, Rocha MM. Leucoencefalopatia multifocal progressiva confirmada por PCR para vírus JC no líquor: relato de caso. Arq Neuropsiquiatr (2004) 62(2b):550–4. doi: 10.1590/S0004-282X2004000300034
14. De Luca A, Giancola ML, Ammassari A, Grisetti S, Cingolani A, Paglia MG, et al. Cidofovir added to HAART improves virological and clinical outcome in AIDS-associated progressive multifocal leukoencephalopathy. AIDS (2000) 14(14):F117–21. doi: 10.1097/00002030-200009290-00001
15. Miralle P, Berenguer J, Lacruz C. (2001). Paradoxical worsening of AIDS-associated progressive multifocal leukoencephalopathy following HAART. In: Proceedings of the 8th Conference on Retroviruses and Opportunistic Infections, Chicago.
16. Cettomai D, McArthur JC. Mirtazapine use in human immunodeficiency virus–infected patients with progressive multifocal leukoencephalopathy. Arch Neurol (2009) 66(2):255–8. doi: 10.1001/archneurol.2008.557
17. Palella FJ, Delaney KM, Moorman AC, Loveless MO, Fuhrer J, Satten GA, et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. N Engl J Med (1998) 338(13):853–60. doi: 10.1056/NEJM199803263381301
18. Caniglia EC, Cain LE, Justice A, Tate J, Logan R, Sabin C, et al. Antiretroviral penetration into the CNS and incidence of AIDS-defining neurologic conditions. Neurology (2014) 83(2):134–41. doi: 10.1212/WNL.0000000000000564
19. Matinella A, Lanzafame M, Bonometti MA, Gajofatto A, Concia E, Vento S, et al. Neurological complications of HIV infection in pre-HAART and HAART era: a retrospective study. J Neurol (2015) 262(5):1317–27. doi: 10.1007/s00415-015-7713-8
20. Riveiro-Barciela M, Falcó V, Burgos J, Curran A, Van den Eynde E, Navarro J, et al. Neurological opportunistic infections and neurological immune reconstitution syndrome: impact of one decade of highly active antiretroviral treatment in a tertiary hospital. HIV Med (2013) 14(1):21–30. doi: 10.1111/j.1468-1293.2012.01033.x
21. Secretaria de Vigilância em SaúdeMinistério da saúde, brasil. boletim epidemiológico – HIV/Aids 2022. departamento de doenças de condições crônicas e infecções sexualmente transmissíveis; secretaria de vigilância em saúde. Brasília:Secretaria de Vigilância em Saúde (2022).
22. Lanjewar DN, Jain PP, Shetty CR. Profile of central nervous system pathology in patients with AIDS. AIDS (1998) 12(3):309–13. doi: 10.1097/00002030-199803000-00009
23. Lucas SB, Hounnou A, Peacock C, Beaumel A, Djomand G, N'Gbichi J-M, et al. The mortality and pathology of HIV infection in a West African city. AIDS (1993) 7(12):1569–79. doi: 10.1097/00002030-199312000-00005
24. Vidal JE, de Oliveira ACP, Fink MCDS, Pannuti CS, Trujillo JR. Aids-related progressive multifocal leukoencephalopathy: a retrospective study in a referral center in são paulo, Brazil. Rev Inst Med Trop Sao Paulo (2008) 50(4):209–12. doi: 10.1590/S0036-46652008000400004
25. Ministério da Saúde M. Prevenção e controle das infecções sexualmente transmissíveis, do HIV/Aids e das hepatites virais. In: Protocolo clínico e diretrizes terapêuticas para manejo da infecção pelo HIV em adultos. Brasília: Secretaria de Vigilância em Saúde (2020).
26. Brasil M da S. Manual técnico para o diagnóstico da infecção pelo HIV em adultos e crianças. In: Edição, Vol. 4. Brasília: Secretaria de Vigilância em Saúde (2018).
27. Stewart LA, Clarke M, Rovers M, Riley RD, Simmonds M, Stewart G, et al. Preferred reporting items for a systematic review and meta-analysis of individual participant data. JAMA (2015) 313(16):1657. doi: 10.1001/jama.2015.3656
28. Nangendo J, Katahoire AR, Armstrong-Hough M, Kabami J, Obeng-Amoako GO, Muwema M, et al. Prevalence, associated factors and perspectives of HIV testing among men in Uganda. PloS One (2020) 15(8):e0237402. doi: 10.1371/journal.pone.0237402
29. Cortese I, Reich DS, Nath A. Progressive multifocal leukoencephalopathy and the spectrum of JC virus-related disease. Nat Rev Neurol (2021) 17(1):37–51. doi: 10.1038/s41582-020-00427-y
30. Cinque P, Vago L, Dahl H, Brytting M, Terreni MR, Fornara C, et al. Polymerase chain reaction on cerebrospinal fluid for diagnosis of virus-associated opportunistic diseases of the central nervous system in HIV-infected patients. AIDS (1996) 10(9):951–8. doi: 10.1097/00002030-199610090-00004
31. Wyen C, Hoffmann C, Schmeier N, Wöhrmann A, Qurishi N, Rockstroh J, et al. Progressive multifocal leukencephalopathy in patients on highly active antiretroviral therapy. JAIDS J Acquir Immune Defic Syndr (2004) 37(2):1263–8. doi: 10.1097/01.qai.0000136093.47316.f3
32. Fournier A, Martin-Blondel G, Lechapt-Zalcman E, Dina J, Kazemi A, Verdon R, et al. Immune reconstitution inflammatory syndrome unmasking or worsening AIDS-related progressive multifocal leukoencephalopathy: A literature review. Front Immunol (2017) 8:577/full. doi: 10.3389/fimmu.2017.00577/full
33. Summers NA, Kelley CF, Armstrong W, Marconi VC, Nguyen ML. Not a disease of the past: A case series of progressive multifocal leukoencephalopathy in the established antiretroviral era. AIDS Res Hum Retroviruses (2019) 35(6):544–52. doi: 10.1089/aid.2018.0232
34. Bennett CL, Focosi D, Socal MP, Bian JC, Nabhan C, Hrushesky WJ, et al. Progressive multifocal leukoencephalopathy in patients treated with rituximab: a 20-year review from the southern network on adverse reactions. Lancet Haematol (2021) 8(8):e593–604. doi: 10.1016/S2352-3026(21)00167-8
35. Falcó V, Olmo M, del Saz SV, Guelar A, Santos JR, Gutiérrez M, et al. Influence of HAART on the clinical course of HIV-1-Infected patients with progressive multifocal leukoencephalopathy: Results of an observational multicenter study. JAIDS J Acquir Immune Defic Syndr (2008) 49(1):26–31. doi: 10.1097/QAI.0b013e31817bec64
36. Augusto L, Neves N, Reis C, Abreu C, Sarmento A. Clinical and radiological characterization of progressive multifocal leukoencephalopathy in HIV-infected patients: A retrospective analysis and review of the literature. Acta Med Port (2015) 28(3):286. doi: 10.20344/amp.5950
37. Marzocchetti A, Tompkins T, Clifford DB, Gandhi RT, Kesari S, Berger JR, et al. Determinants of survival in progressive multifocal leukoencephalopathy. Neurology (2009) 73(19):1551–8. doi: 10.1212/WNL.0b013e3181c0d4a1
38. Lima MA, Silva MTT, Afonso LA, Vaz BJP. Post-cART progressive multifocal leukoencephalopathy era in a Brazilian center. J Neurol Sci (2017) 381:321–4. doi: 10.1016/j.jns.2017.09.002
39. Grabar S, Lanoy E, Allavena C, Mary-Krause M, Bentata M, Fischer P, et al. Causes of the first AIDS-defining illness and subsequent survival before and after the advent of combined antiretroviral therapy. HIV Med (2008) 9(4):246–56. doi: 10.1111/j.1468-1293.2008.00554.x
40. Lima MA. Progressive multifocal leukoencephalopathy: new concepts. arq neuropsiquiatr. Arquivos de Neuro-psiquiatria (2013) 71(9B):699–702. doi: 10.1590/0004-282X20130154
41. De Luca A, Giancola ML, Ammassari A, Grisetti S, Paglia MG, Gentile M, et al. The effect of potent antiretroviral therapy and JC virus load in cerebrospinal fluid on clinical outcome of patients with AIDS-associated progressive multifocal leukoencephalopathy. J Infect Dis (2000) 182(4):1077–83. doi: 10.1086/315817
42. Berenguer J, Miralles P, Arrizabalaga J, Ribera E, Dronda F, Baraia-Etxaburu J, et al. Clinical course and prognostic factors of progressive multifocal leukoencephalopathy in patients treated with highly active antiretroviral therapy. Clin Infect Dis (2003) 36(8):1047–52. doi: 10.1086/374048
43. Grahn A, Studahl M. Varicella-zoster virus infections of the central nervous system – prognosis, diagnostics and treatment. J Infect (2015) 71(3):281–93. doi: 10.1016/j.jinf.2015.06.004
44. Croxford S, Kitching A, Desai S, Kall M, Edelstein M, Skingsley A, et al. Mortality and causes of death in people diagnosed with HIV in the era of highly active antiretroviral therapy compared with the general population: an analysis of a national observational cohort. Lancet Public Heal (2017) 2(1):e35–46. doi: 10.1016/S2468-2667(16)30020-2
45. Wiginton JM, Mathur S, Gottert A, Pilgrim N, Pulerwitz J. Hearing from men living with HIV: Experiences with HIV testing, treatment, and viral load suppression in four high-prevalence countries in Sub-Saharan Africa. Front Public Heal (2022) 10:861431/full. doi: 10.3389/fpubh.2022.861431/full
46. Gottert A, Pulerwitz J, Siu G, Katahoire A, Okal J, Ayebare F, et al. Male Partners of young women in Uganda: Understanding their relationships and use of HIV testing. PloS One (2018) 13(8):e0200920. doi: 10.1371/journal.pone.0200920
47. Lima MA, Bernal-Cano F, Clifford DB, Gandhi RT, Koralnik IJ. Clinical outcome of long-term survivors of progressive multifocal leukoencephalopathy. J Neurol Neurosurg Psychiatry (2010) 81(11):1288–91. doi: 10.1136/jnnp.2009.179002
48. Anand P, Hotan GC, Vogel A, Venna N, Mateen FJ. Progressive multifocal leukoencephalopathy. Neurol - Neuroimmunol Neuroinflamm (2019) 6(6):e618. doi: 10.1212/NXI.0000000000000618
49. Berger JR, Aksamit AJ, Clifford DB, Davis L, Koralnik IJ, Sejvar JJ, et al. PML diagnostic criteria. Neurology (2013) 80(15):1430–8. doi: 10.1212/WNL.0b013e31828c2fa1
50. Williamson EML, Berger JR. Diagnosis and treatment of progressive multifocal leukoencephalopathy associated with multiple sclerosis therapies. Neurotherapeutics (2017) 14(4):961–73. doi: 10.1007/s13311-017-0570-7
51. Yousry TA, Pelletier D, Cadavid D, Gass A, Richert ND, Radue E-W, et al. Magnetic resonance imaging pattern in natalizumab-associated progressive multifocal leukoencephalopathy. Ann Neurol (2012) 72(5):779–87. doi: 10.1002/ana.23676
52. Yousry TA, Major EO, Ryschkewitsch C, Fahle G, Fischer S, Hou J, et al. Evaluation of patients treated with natalizumab for progressive multifocal leukoencephalopathy. N Engl J Med (2006) 354(9):924–33. doi: 10.1056/NEJMoa054693
53. Harrison DM, Newsome SD, Skolasky RL, McArthur JC, Nath A. Immune reconstitution is not a prognostic factor in progressive multifocal leukoencephalopathy. J Neuroimmunol (2011) 238(1–2):81–6. doi: 10.1016/j.jneuroim.2011.07.003
54. Miller RF, Lucas SB, Hall-Craggs MA, Brink NS, Scaravilli F, Chinn RJ, et al. Comparison of magnetic resonance imaging with neuropathological findings in the diagnosis of HIV and CMV associated CNS disease in AIDS. J Neurol Neurosurg Psychiatry (1997) 62(4):346–51. doi: 10.1136/jnnp.62.4.346
55. Whiteman ML, Post MJ, Berger JR, Tate LG, Bell MD, Limonte LP. Progressive multifocal leukoencephalopathy in 47 HIV-seropositive patients: neuroimaging with clinical and pathologic correlation. Radiology (1993) 187(1):233–40. doi: 10.1148/radiology.187.1.8451420
56. Berger JR, Pall L, Lanska D, Whiteman M. Progressive multifocal leukoencephalopathy in patients with HIV infection. J Neurovirol (1998) 4(1):59–68. doi: 10.3109/13550289809113482
57. Alleg M, Solis M, Baloglu S, Cotton F, Kerschen P, Bourre B, et al. Progressive multifocal leukoencephalopathy: MRI findings in HIV-infected patients are closer to rituximab- than natalizumab-associated PML. Eur Radiol (2021) 31(5):2944–55. doi: 10.1007/s00330-020-07362-y
58. Vance DE, Cody SL, Moneyham L. Remediating HIV-associated neurocognitive disorders via cognitive training: A perspective on neurocognitive aging. Interdiscip Top Gerontol Geriatr (2017) 42:173–86. doi: 10.1159/000448562
59. Christo PP. Alterações cognitivas na infecção pelo HIV e aids. Rev Assoc Med Bras (2010) 56(2):242–7. doi: 10.1590/S0104-42302010000200027
60. Berger J, Major E. Progressive multifocal leukoencephalopathy. Semin Neurol (1999) 19(02):193–200. doi: 10.1055/s-2008-1040837
61. Deng Q, Yan Z, Yang Y, Wang J, Han Y, Feng X, et al. Progressive multifocal leukoencephalopathy and peripheral neuropathy in a patient with good’s syndrome. J Neurovirol (2022) 28(1):177–80. doi: 10.1007/s13365-021-01041-4
62. Bernal-Cano F, Joseph JT, Koralnik IJ. Spinal cord lesions of progressive multifocal leukoencephalopathy in an acquired immunodeficiency syndrome patient. J Neurovirol (2007) 13(5):474–6. doi: 10.1080/13550280701469178
63. Cohen LG, Topka H, Cole RA, Hallett M. Leg paresthesias induced by magnetic brain stimulation in patients with thoracic spinal cord injury. Neurology (1991) 41(8):1283–3. doi: 10.1212/WNL.41.8.1283
64. Mangili A, Murman DH, Zampini AM, Wanke CA, Mayer KH. Nutrition and HIV infection: Review of weight loss and wasting in the era of highly active antiretroviral therapy from the nutrition for healthy living cohort. Clin Infect Dis (2006) 42(6):836–42. doi: 10.1086/500398
65. Polsky B, Kotler D, Steinhart C. HIV-Associated wasting in the HAART era: Guidelines for assessment, diagnosis, and treatment. AIDS Patient Care STDS (2001) 15(8):411–23. doi: 10.1089/108729101316914412
66. Chambers MA, Moylan JS, Reid MB. Physical inactivity and muscle weakness in the critically ill. Crit Care Med (2009) 37:S337–46. doi: 10.1097/ccm.0b013e3181b6e974
67. Langer HT, Senden JMG, Gijsen AP, Kempa S, van Loon LJC, Spuler S. Muscle atrophy due to nerve damage is accompanied by elevated myofibrillar protein synthesis rates. Front Physiol (2018) 9:1220/full. doi: 10.3389/fphys.2018.01220/full
68. Thomas CK, Zaidner EY, Calancie B, Broton JG, Bigland-Ritchie BR. Muscle weakness, paralysis, and atrophy after human cervical spinal cord injury. Exp Neurol (1997) 148(2):414–23. doi: 10.1006/exnr.1997.6690
69. Herridge MS, Cheung AM, Tansey CM, Matte-Martyn A, Diaz-Granados N, Al-Saidi F, et al. One-year outcomes in survivors of the acute respiratory distress syndrome. N Engl J Med (2003) 348(8):683–93. doi: 10.1056/NEJMoa022450
70. Hudson LD, Lee CM. Neuromuscular sequelae of critical illness. N Engl J Med (2003) 348(8):745–7. doi: 10.1056/NEJMe020180
71. Latronico N, Shehu I, Seghelini E. Neuromuscular sequelae of critical illness. Curr Opin Crit Care (2005) 11(4):381–90. doi: 10.1097/01.ccx.0000168530.30702.3e
72. De Jonghe B. Paresis acquired in the intensive care unit: A prospective multicenter study. JAMA (2002) 288(22):2859. doi: 10.1001/jama.288.22.2859
73. Chaboyer W, Grace J. Following the path of ICU survivors: a quality-improvement activity. Nurs Crit Care (2003) 8(4):149–55. doi: 10.1046/j.1478-5153.2003.00020.x
74. van der Schaaf M, Beelen A, Dongelmans D, Vroom M, Nollet F. Poor functional recovery after a critical illness: A longitudinal study. J Rehabil Med (2009) 41(13):1041–8. doi: 10.2340/16501977-0443
75. Chelluri L, Im KA, Belle SH, Schulz R, Rotondi AJ, Donahoe MP, et al. Long-term mortality and quality of life after prolonged mechanical ventilation*. Crit Care Med (2004) 32(1):61–9. doi: 10.1097/01.CCM.0000098029.65347.F9
76. Vargas AL. Exercícios terapêuticos para portadores de esclerose múltipla com déficit de coordenação motora e equilíbrio. Fisioter Bras (2019) 3(3):151–6. doi: 10.33233/fb.v3i3.2954
77. Heesen C, Romberg A, Gold S, Schulz K-H. Physical exercise in multiple sclerosis: supportive care or a putative disease- modifying treatment. Expert Rev Neurother (2006) 6(3):347–55. doi: 10.1586/14737175.6.3.347
78. Braga DM, de Oliveira EML. Combinações de técnicas de reabilitação no paciente com esclerose múltipla (EM). Rev Neurociências (2012) 20(4):483–4. doi: 10.34024/rnc.2012.v20.8220
79. Pereira LVL, Sales WB, Andrade ACNB, Lucena EM de F, Quartarone RGN, Germoglio VG. Assistência fisioterapêutica ao paciente com HIV/SIDA em um hospital de referência do estado da paraíba. Res Soc Dev (2020) 9(9):e53996990. doi: 10.33448/rsd-v9i9.6990
80. Berger JR. The clinical features of PML. Cleve Clin J Med (2011) 78(11 suppl 2):S8–12. doi: 10.3949/ccjm.78.s2.03
81. Grzesiuk AK. Características clínicas e epidemiológicas de 20 pacientes portadores de esclerose múltipla acompanhados em cuiabá - mato grosso. Arq Neuropsiquiatr (2006) 64(3a):635–8. doi: 10.1590/S0004-282X2006000400022
Keywords: HIV, Progressive Multifocal Leukoencephalopathy, JC virus, sequelae, aids
Citation: Valente J, Del-Tejo PL, Cubas-Vega NC, Rodrigues MGdA, de Barros FRB, Alexandre MA, Arêas GPT, Bastos M, Pinto SD, Barros CMSS, Marinho EP, Mello S, Ferreira E, Aprigio V, Monte RL, Sampaio V, Lacerda M, Baia-da-Silva DC and Val F (2023) Sequelae and mortality in patients with HIV/AIDS and Progressive Multifocal Leukoencephalopathy: Systematic review and case series in the Brazilian Amazon. Front. Trop. Dis 4:1050477. doi: 10.3389/fitd.2023.1050477
Received: 21 September 2022; Accepted: 02 March 2023;
Published: 16 March 2023.
Edited by:
Carlos Brites, Federal University of Bahia (UFBA), BrazilReviewed by:
Cássia Goulart, Federal University of São Carlos, BrazilNatarajan Gopalan, Central University of Tamil Nadu, India
Antonio C. R. Vallinoto, Federal University of Pará, Brazil
Copyright © 2023 Valente, Del-Tejo, Cubas-Vega, Rodrigues, de Barros, Alexandre, Arêas, Bastos, Pinto, Barros, Marinho, Mello, Ferreira, Aprigio, Monte, Sampaio, Lacerda, Baia-da-Silva and Val. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fernando Val, ZmZhdmFsQGdtYWlsLmNvbQ==
†These authors have contributed equally to this work