
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Trop. Dis. , 17 November 2022
Sec. Neglected Tropical Diseases
Volume 3 - 2022 | https://doi.org/10.3389/fitd.2022.986884
This article is part of the Research Topic Clinical Review of Neglected Tropical Diseases View all 8 articles
 Luisa Frallonardo1†Francesco Di Gennaro1,2*†
Luisa Frallonardo1†Francesco Di Gennaro1,2*† Gianfranco Giorgio Panico1Roberta Novara1Elisabetta Pallara1Sergio Cotugno1Giacomo Guido1Elda De Vita1Aurelia Ricciardi1Valentina Totaro1Michele Camporeale1Giuseppina De Iaco1Davide Fiore Bavaro1Rossana Lattanzio1Giulia Patti1Gaetano Brindicci1Roberta Papagni1Carmen Pellegrino1Carmen Rita Santoro1Francesco Vladimiro Segala1Giovanni Putoto2Emanuele Nicastri3Annalisa Saracino1
Gianfranco Giorgio Panico1Roberta Novara1Elisabetta Pallara1Sergio Cotugno1Giacomo Guido1Elda De Vita1Aurelia Ricciardi1Valentina Totaro1Michele Camporeale1Giuseppina De Iaco1Davide Fiore Bavaro1Rossana Lattanzio1Giulia Patti1Gaetano Brindicci1Roberta Papagni1Carmen Pellegrino1Carmen Rita Santoro1Francesco Vladimiro Segala1Giovanni Putoto2Emanuele Nicastri3Annalisa Saracino1Human Onchocerciasis, caused by infection by the filarial nematode Onchocerca volvulus, is a neglected public health disease that affects millions of people in the endemic regions of sub-Saharan Africa and Latin America. It is also called river blindness because the Blackflies that transmit infection breeds in rapidly flowing fresh water streams and rivers. This review features state-of-the-art data on the parasite, its endobacteria Wolbachia, the prevalence of the infection and its geographical distribution, its diagnostics, the interaction between the parasite and its host, and the pathology of Onchocerciasis. By development and optimization of the control measures, transmission by the vector has been interrupted in foci of countries in the Americas (Colombia, Ecuador, Mexico, and Guatemala)and inSudan, followed by Onchocerciasis eliminations. The current state and future perspectives for vector control and elimination strategy are described.
Human Onchocerciasis is a vector-borne disease, a parasitic infection caused by filarial worms and transmitted by repeated bites of infected blackflies. Because the vectors - blackflies of the genus Simulium - are insects that breed as larvae in fast-flowing rivers and streams and bite humans near these sites, the disease is also known as “river blindness” (1).
Onchocerciasis’ physical manifestations include troublesome itching, skin rash, visual impairment, and irreversible blindness; these manifestations result from dying and dead microfilariae inciting an immunologic and inflammatory response, ultimately resulting in tissue damage and scarring. The disease is second to trachoma as the leading cause of blindness due to infection in the developing world (2).
Onchocerciasis causes morbidity and disability in affected populations and has a significant psychosocial and economic impact, including the depopulation of arable lands along river valleys. Historically, river blindness has impeded impeding the economic development of countries affected by the desertion of large areas of fertile land adjacent to vector breeding sites (3).
We searched PubMed, Scopus, Google Scholar, EMBASE, Cochrane Library, and the WHO website (http://www.who.int) for literature addressing Onchocerciasis published in the last 25 years. We used the following search strategy in Human Onchocerciasis [tiab] OR Onchocerca volvulus [mh] OR Onchocerca [tiab] OR river blindness [tiab] OR Simulium [tiab] OR Simulium blackflies [tiab] OR Onchocercomas [tiab]) All of the studies mentioned concern epidemiology, physiopathology, clinical characteristics, screening and diagnosis, therapy, management, and eradication programs.
Infections due to Onchocerca spp. are found in tropical climates and are currently endemic in 37 countries, of which 30 are in sub-Saharan Africa. The endemic area starts from Senegal in the west to Ethiopia in the east and extends to the south of the equator from Angola in the west to Tanzania in the east. Pockets of Onchocerciasis exist in Sudan and Yemen. The disease was previously endemic in small foci in 6 Latin American countries (Brazil, Colombia, Ecuador, Guatemala, Mexico, and Venezuela) (4).
Despite the adoption of specific plans, the proportion of people affected by the diseases is high, with about 37 million people in tropical Africa and 140,000 in Latin America and an incidence of approximately 40,000 cases per year in low-endemic countries (4).
Onchocerciasis causes 46,000 new cases of blindness annually, resulting in 270,000 individuals being blinded and an additional 500,000 developing visual impairment, making Onchocerciasis the second leading cause of infectious blindness worldwide (5).
The disease is generally more prevalent in males than females and individuals aged between 20 and 30. Men are more affected due to increased exposure to blackfly bites during their occupational activity (farmers, fishermen) (2).
The disease pattern varies considerably between geographical zones, with ocular pathology more common in hyperendemic localities with savanna climates. At the same time, forest communities are more affected by the dermatological manifestations of the disease. One hypothesis to explain this difference is the existence of two parasite strains in West Africa, namely forest and savannah strains (6), which differ significantly in epidemiology and disease severity and are carried by different vectors. The savannah strain found in West Africa is associated with blindness, while the forest strain causes less severe ocular diseases, even in individuals with high parasite load. However, according to a recent study, the evidence for a savannah blinding onchocerciasis strain in simple contrast with a non-blinding forest strain is equivocal. A re-appraisal of the strain hypothesis to explain patterns of ocular disease is needed to improve the understanding of onchocerciasis epidemiology and disease burden estimates (7).
Onchocerciasis was previously the most common filarial infection diagnosed outside the tropics, and it mainly occurs in immigrants and refugees. The incidence of imported infection appears to be decreasing, probably as a result ofvector control and elimination programs. However, it remains common in migrant populations from highly endemic areas of sub-Saharan Africa, among which is likely underdiagnosed (8) but also visitors or migrants from tropical countries and long-term European travelers (9).
For instance, almost 400 cases of onchodermatitis were identified in patients from Equatorial Guinea at a single Spanish center (10). In a multicentre cross-sectional study conducted in five tropical disease units in Italy (11), 9.25% of migrants from sub-Saharan Africa had a positive pan-filarial enzyme-linked immunoassay (ELISA), though only a fraction was likely caused by O. volvulus.
The primary vectors of human Onchocerciasis in Africa are blackflies belonging to the S. damnosum species complex. Among the 65 species described so far, at least 15 may act as parasite vectors (12). Humans are the only definitive host for O. volvulus, the infective larvae transmitted through Simulium blackflies’ bloodmeal. In Eastern Africa, the disease may also be transmitted by members of the S. neavei complex (subgenus Lewisellum, 9 species), which have their immature stages developing phoretic relationships with freshwater crabs. For this reason, people at risk of acquiring Onchocerciasis are those who live or work near streams or rivers where Simulium blackflies are present. It is assumed that Simulium biting rates follow a seasonal pattern (4).
Onchocerca volvulus has a complex life cycle (Figure 1) involving a definitive and intermediate host, respectively humans and Simulium blackflies. Common blackfly hosts include S. damnosum and S. neavei in Africa andS.ochraceum, S. metallicum, S. callidum, and S. exiguum in the Americas (13).
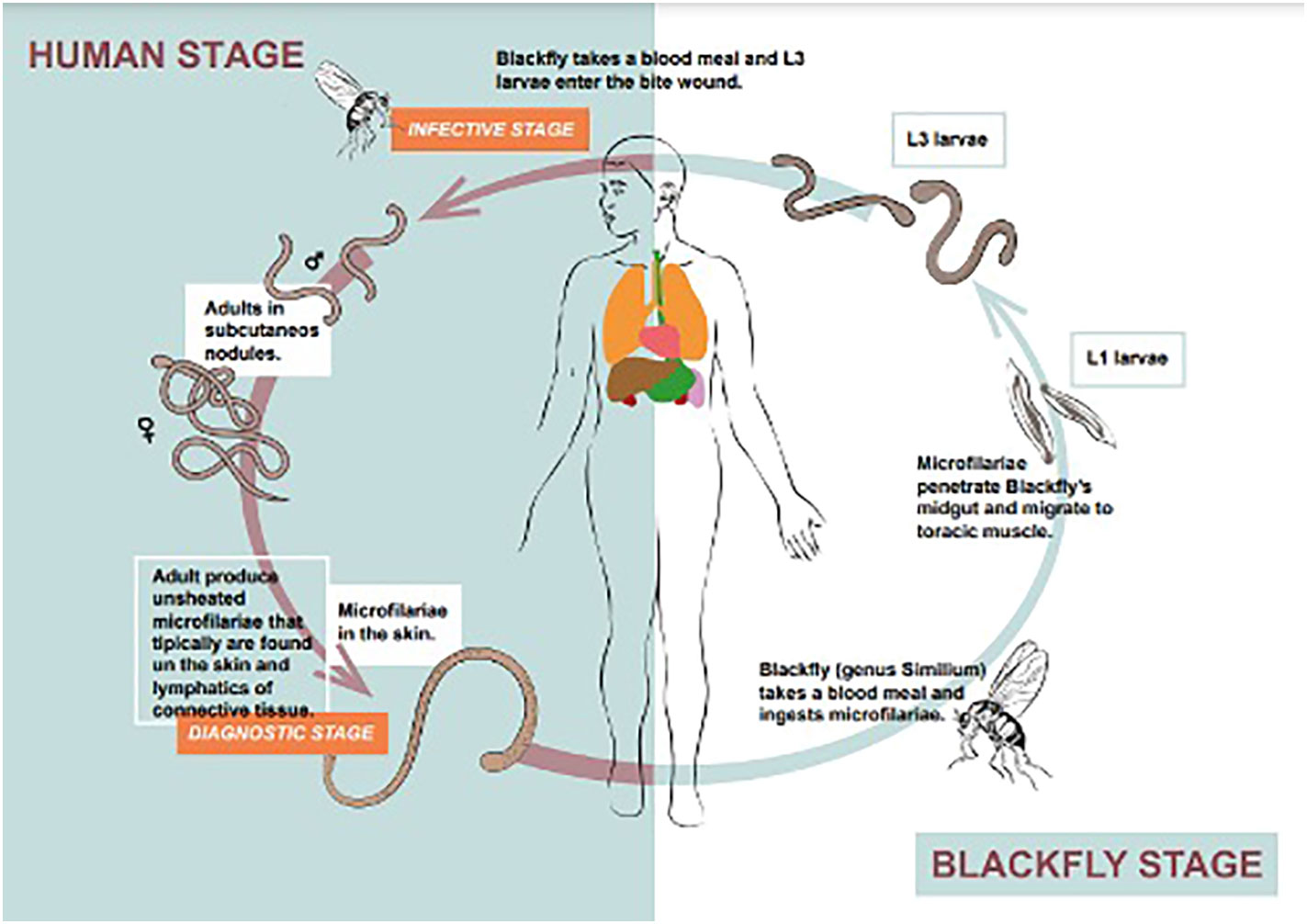
Figure 1 Life cycle of Onchocerca volvulus.
Blackflies ingest microfilariae during blood meals. After ingestion, microfilariae migrate from the blackfly’s midgut through the hemocoel to the thoracic muscles. Here, microfilariae develop from first-stage larvae to third-stage infective larvae, that may be introduced into human skin by a second Simulium bloodmeal, where they mature into adult parasites (macrofilariae) over the next 6 to 12 months. Adult filariae reside in subcutaneous nodules connective called “Onchocercomas”, where they can survive for approximately 15 years. Each nodule is made of numerous worms. Older nodules often contain necrotic material with calcified remnants of filariae and numerous male and female worms. Nodule location depends on geographical area: most infections in Central America exhibit nodules above the waist (especially on the neck and head), and those in Central Africa exhibit nodules below the waist (especially on the knees and pelvic area). This relationship is based on the biting preferences of the blackfly vector (14).
Clinical manifestation may be influenced by host genetic factors and duration of exposure to infective bites, and begins to occur one to three years after parasite injection. The main clinical findings are dermatological and ophthalmological alterations, in addition to some systemic features (15). Clinical manifestations of 272 Onchocerciasis are summarized in Table 1 and Figure 2.
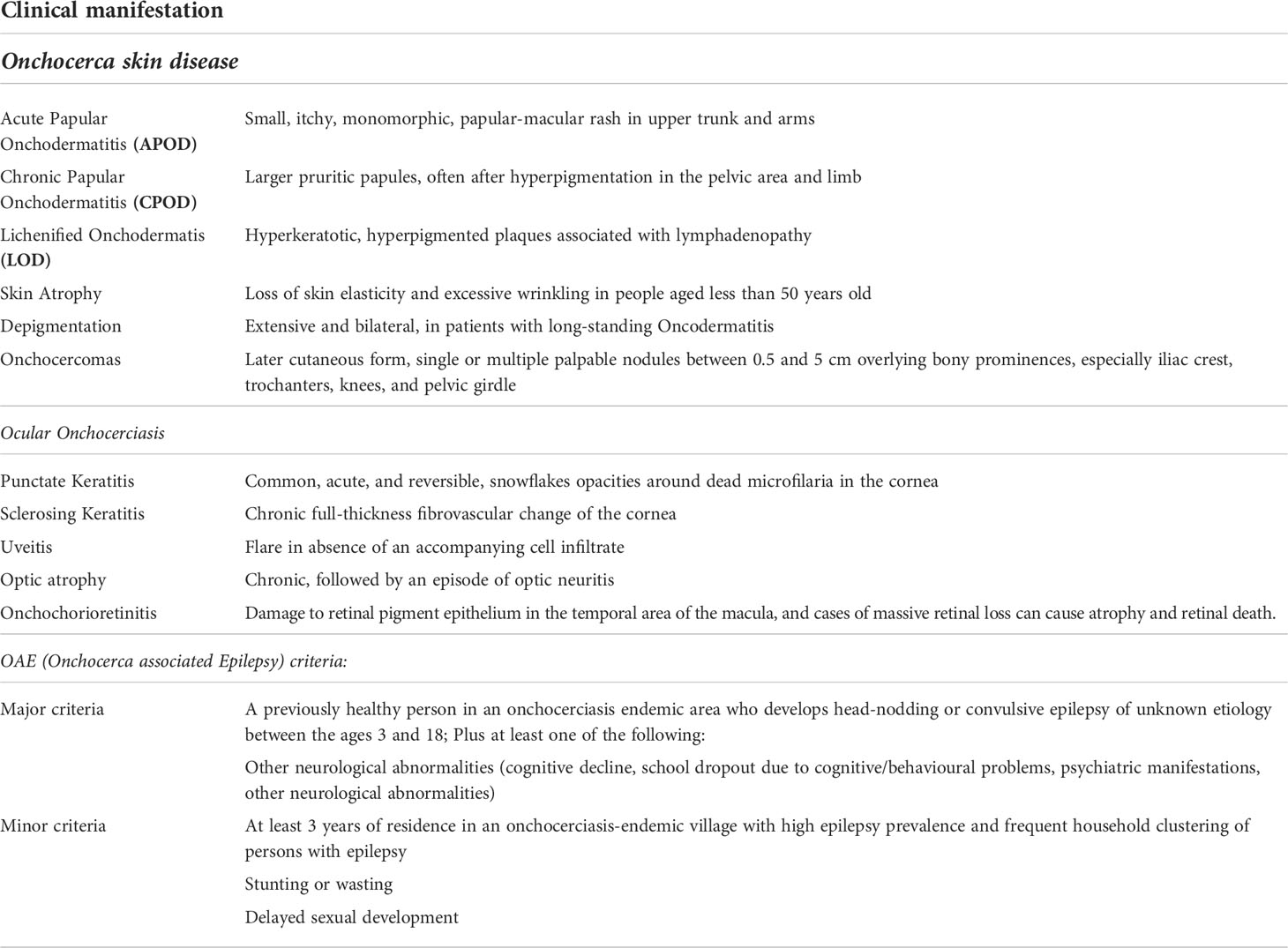
Table 1 Clinical manifestation of Onchocerciasis.
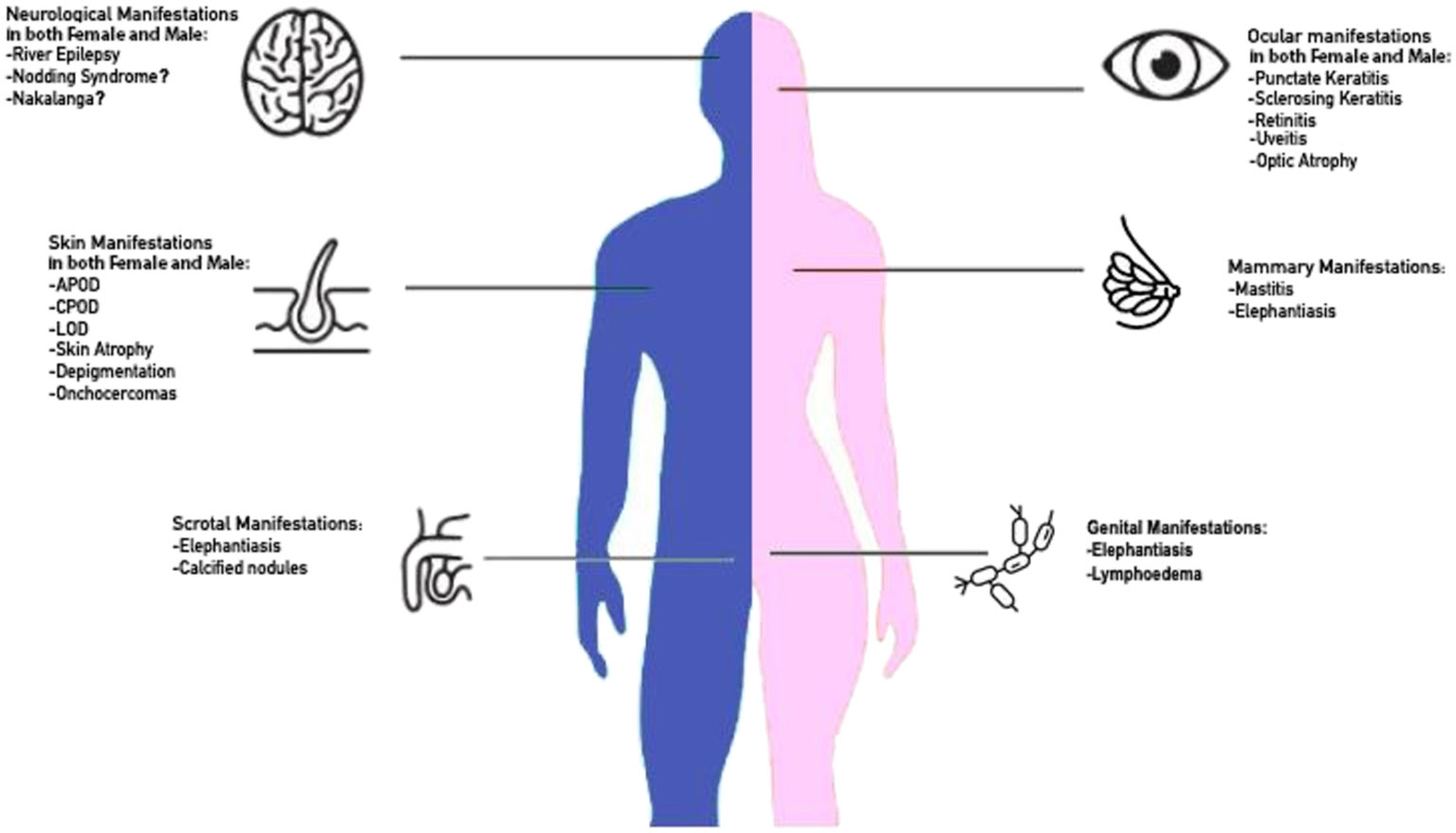
Figure 2 Clinical manifestation of Onchocerciasis.
The spectrum of skin pathology manifestation is broad. Dermatitis is variable in appearance, probably in relation to the chronicity of infection, host age, geographic area of acquisition, and relative immune responsiveness. The development of a formal clinical classification and grading system describing the cutaneous changes in Onchocerciasis facilitated formal mapping of the true global burden of onchocercal skin disease (OSD). The categories of Onchocercal skin disease delineated are summarised in Table 1.
A study carried out in the northern Nigeria by skin observation of in 6,790 individuals in endemic communities and 1,343 individuals in nonendemic communities declared the association between Onchocercal Skin disease and markers of infection (16). A population survey of residents in savanna mesoendemic Villages Northern Nigeria showed that the presence of nodules was the most common finding (21.2%), followed by atrophy (6.1% of those <50 years), APOD (3.4%), depigmentation (3.2%), itching (9.5%) (Michele E. M., Trop. Med. Infect. Dis.).
In travelers returning from endemic areas, itchy papular dermatitis may occur early in the course of the infection, often localized to one extremity (17). According to data collected from 1994 to 2014 among expatriates and travellers from non-endemic areas the most frequent clinical manifestations are itching (76.7%), unilateral leg or forearm swelling (43.3%) and rash (40%), minimally (6.9%) two (6.9%) ocular symptoms.
Onchocerciasis is characterised by eosinophilia and IgE production due to the Th2 response mediated by CD4+ T cells and macrophages producing IL-10 and TGF-β, suppressive cytokines. In hyperreactive onchocercomas there is less expression of TGF-β, thus the Th2 response and consequently IL-13 production, resulting in increased IgE synthesis by plasma cells. (Low levels of transforming growth factor-beta (TGF-beta) and reduced suppression of Th2-mediated inflammation (18).
Eosinophilia is very common, with median counts of 2915/μL among migrants and 1960/μL among travellers and expatriates (19).
The more common generalized form presents with subclinical or intermittent dermatitis (acute and chronic papular dermatitis). It may progress to skin hyperpigmentation or depigmentation (leopard skin) and atrophy and elasticity loss, thus resulting in chronic distressing pruritus and disfiguring lesions. After years of repeated exposures, itching reduces, while atrophic and hypopigmented lesions (leopard and lizard skin) and, lastly, subcutaneous nodules appear (Onchocercomas) (20). Generalized onchocerciasis (GE) is characterized by high microfilarial burden and immunological tolerance to the worms. However, in rare cases infection leads to the sowda form of the disease displaying low microfilarial numbers, i.e. microfilarial control a T helper 2, Th helper 17-type immune response and an high immunoglobulin (Ig)E levels. This pathogenetic mechanism could partecipate in the development of severe Onchocercias (18) In this regard Hoerauf et al., suggested that Arg110Gln variant of IL-13 (which confers an IgE-independent risk for asthma and atopy) may lead to increase IL-13, promoting hyper-reactivity against the helmints (21).
Sowda, a lichenified onchodermatitis prevalent in Yemen is an hyperreactive skin condition characterized by intense pruritus and hyperpigmentation of the skin mainly affecting the legs below the knees, but may extend to the thighs and gluteal region, with common secondary suppurative and papular dermatitis (22); [Michele, (23)]. In Central America, another manifestation of acute Onchocerciasis includes facial swelling with itching and erythema, a finding known as erysipelas de la costa. In Zaire and Central America, acute urticarial eruption may be seen, while the association of hyperpigmentation with signs of inflammation is also known as mal morado (24). Secondary to onchocercal skin disease, lymphadenopathy may develop, most commonly in the groin area and in the mammary region, eventually leading to genital elephantiasis or mimicking a metastatic breast mass (25). Calcified nodules are typically seen in the scrotal region and around the hip and elbow but, rarely, similarly to cysticercosis and echinococcosis, they may also be found within the central nervous system (26).
Ocular damage depends on both mechanical invasion of microfilariae and deposition of immune complexes. Conventionally, anterior chamber lesions had been attributed to a cascade of inflammatory processes triggered by filarial products. In this regard, a pathogenetic hypothesis suggests that the pro-inflammatory events leading to increasing corneal opacity are stimulated not only by the parasite itself but also by its recently discovered endosymbiotic Wolbachia bacteria when released by dying microfilariae.
The most common ocular pathology involves the cornea, but other structures of the anterior and posterior segments of the eye can also be affected. Corneal pathology begins with “snow-flake” opacities (punctate keratitis), which later coalesce and may become hyperpigmented (sclerosing keratitis) (3). In addition to the multiple risks to the visual apparatus, as shown by a cross-sectional case-control study, there is a positive association between subclinical onchocerciasis and glaucoma (27). Studies using animal models have shown the essential role of innate immune response in Onchocerca keratitis: toll-like receptors 2 and 6are expressed in the cornea, and activation can induce keratitis as a consequence of activation of keratocytes caused by death and degeneration of microfilariae into the confined environment of the corneal stroma. Activated keratocytes can mature into stromal fibroblasts, which produce pro-inflammatory cytokines and chemokines and can induce the expression of adhesion molecules on vascular endothelial cells. Underlying this pathogenetic mechanism is the role of Wolbachia-derived diacyl-lipoproteins, which stimulate molecules required for TLR2/6 ligation and produce pro-inflammatory cytokine and chemokine responses [Turner (28)].
TLR4 role in neutrophil recruitment to the development of corneal haze was denied as number of macrophages in TLR4-deficient animals after intrastromal injection of O. volvulus remains comparable to those with no TLR4-deficiency. [Gillette-Ferguson, et al. (29)].
These changes mediate neutrophil recruitment from peripheral, limbal vessels into the avascular corneal stroma, stimulating further neutrophil infiltration, degranulation, and secretion of cytotoxic products such as nitric oxide and myeloperoxidase and oxygen radicals. A cytotoxic effect on keratocytes and corneal endothelial cells will lead to loss of corneal clarity (3, 30).
There is increasing epidemiological evidence that Onchocerciasis is associated with a spectrum of epileptic seizures, mainly generalized tonic-clonic seizures, but also atonic neck seizures, myotonic, and absence (31).
This strong association allows the definition of Onchocerciasis-associated epilepsy (OAE), also known as “River epilepsy” which is characterized by recurrent episodes in more than 60% of cases. It has been estimated that approximately 400,000 cases of epilepsy in Africa could be prevented by appropriate onchocerciasis control (32).
Furthermore, onchocerciasis may be implicated in the pathogenesis of Nodding syndrome, a yet unexplained neurologic condition mainly affecting children living in South Sudan, Tanzania and Uganda, characterized by paroxysmal head nodding frequently accompanied by epileptic manifestations and mental decline. In this regard, studies indicate that skin microfilarial density in early childhood is associated with the risk of developing epilepsy later in life, and that this association may be time and dose-dependent (33, 34), the pathological basis for this association being a neuroinflammatory disorder possibly induced by antibodies directed against Leiomodin-1, that may cross-react with a similar protein that is present in the O. volvulus parasite (32). Onchocerciasis may also be associated with Nakalanga syndrome, a condition characterized by stunted growth, delayed pubertal development, mental impairment and, in some cases, epileptic manifestations (32). However, for both Nodding and Nakalanga syndromes, along with Onchicerciasis, various infectious, toxic, nutritional, metabolic and genetic causes have been proposed and investigated (35).
From a pathological perspective, the role of O.volvulus CNS invasion in the pathophysiology of onchocerciasis-associated neurological manifestations is debated, as recent studies involving subjects with OAE and high skin microfilariae load showed no signs of microfilariae in the cerebrospinal fluid the infected hosts (36).
In 2017, Colebunders et al. suggest an association between ivermectin coverage and reduction of epilepsy and seizer frequency in OAE; this correlation would have major consequences on reducing the burden of epilepsy in onchocerciasis-endemic regions. Another clinical trial postulates that the administration of doxycycline can improve outcomes in Nodding Syndrome by targeting O. volvulus through cross-reaction of doxycycline effects on Wolbachia (37).
The tools for diagnosis of Onchocerciasis in the laboratory include examination of skin snips by microscopy for emergent microfilariae, the Mazzotti test, detection of antibodies to onchocercal antigens, or use of highly sensitive polymerase chain reaction-based (PCR) techniques for detection of microfilariae DNA in skin snips (14).
Currently, the diagnosis of infection with O.volvulus is predominantly based on nodule palpation and microscopic detection of microfilariae in superficial skin biopsies (Skin Snips). This technique is the most widely used standardized technique for Onchocerciasis in many endemic regions. Samples are usually collected from the scapula over the iliac crest or calf. Its use is discouraged because of the invasiveness and lack of sensitivity when microfilarial densities are low, as in O.volvulus-hypoendemic areas (14, 17).
Obtaining the biopsies is both painful and carries some risk of transmitting blood-borne infections for these reasons WHO does not recommend the use of skin snip-based assays as a primary diagnostic for the verification of elimination (38).
For diagnosis of human infection several approaches have been considered using antibodies, antigens or nucleic acid detection for the development of a diagnostic tool based on a biomarker (39).
Many antibody tests have been identified as candidate tests and as surveillance tools for control programs, but the major drawback is the need for laboratory infrastructure to support the performance of Enzyme-Linked Immunosorbent Assay (ELISA) tests. Serological assessments for human Onchocerciasis are based on IgG4 reactivity against the OV-16 antigen, with sensitivities of 60-80% (39).
Recent studies showed that a combination of rOVOC3261 with OV-16 improved serologic assessment of O.volvulus infection (40). The relevance of developing tests that incorporate a wider range of antigens has been highlighted in a study from Yemen that evaluated the diagnostic potentials of OvMCBL02 multiepitope antigen to differentiate between infected individuals and patients who had been undergoing treatment (41).
Therefore, novel diagnostic tests are needed that can be used singly or in combination with the Ov-16 test to improve its sensitivity.
A study by Hotterbeekx et al. made a comparison between the sensitivity of the Ov-16 test alone with the tandem use of OvMANE1 and Ov-16, assuming that the tandem use of OvMANE1 and Ov-16 tests may represent a more appropriate tool for onchocerciasis elimination mapping because of the improved sensitivity (42).
For rapid assessment of O. volvulus infection, it is possible to test a mixture of four recombinantly produced Onchocerca volvulus antigens (Ov-FAR-1, Ov-API-1, Ov-MSA-1, and Ov-CPI-1) using luciferase immunoprecipitation systems (LIPS)
The multi-antigen LIPS assay can be used as a rapid and specific tool not only to diagnose individual Ov infections but also as a sensitive and potentially point-of-care method for early detection of recrudescent infections in areas under control and for mapping new areas of transmission [Burbelo, et al. (43)].
Some studies have already demonstrated that the detection of O.volvulus DNA using PCR in such skin biopsies has a higher sensitivity than this classical approach (44). Similar sensitivities can be achieved with the O.volvulus cox1 LAMP assay (45). The cox1 LAMP assay has comparable clinical sensitivity and specificity to those of the O-150 qPCR assay, even though the latter has the advantage of targeting a repeat sequence that is present multiple times in the O.volvulus genome. Moreover, the cox1 LAMP assay is capable of providing results within 30 min (46).
Ophthalmologic evaluations, obtained before treatment of eye lesions, are often necessary to detect microfilariae in the cornea or anterior chamber on slit-lamp examination or find adult worms on a nodule biopsy specimen. The literature describes the development of humanized mouse models that are susceptible to O.volvulus infection. These novel mouse models could play an important role in the development of specific and sensitive diagnostic tests for the presence of parasites (47).
Several studies have been performed in West Africa to evaluate the patch test, demonstrating that it constitutes a valuable tool to evaluate the levels of endemicity and to detect recrudescence of transmission in previously controlled areas (48). One exampleis the Mazzotti test, which uses Diethylcarbamazine (DEC) for the detection of skin microfilariae. The Mazzotti reaction is an immunological reaction that can occur within a very short time under anthelmintic therapy, triggered by an exuberant reaction of the immune system due to the death of the worms (49).
The complex life cycle of Onchocerciasis poses an exceptional challenge to the therapeutic strategy. In addition, several drugs used in the past 70 years have proved to be independently toxic to the host at the same dose levels used to cure the infection, while some others have caused adverse reactions associated with parasite death (50).
Diethylcarbamazine (DEC) has been the mainstay of Treatment for Onchocerciasis for many years. It is a micro and macrofilaricidal molecule, affecting the neuromuscular system of the parasites and promoting cellular cytotoxicity mediated by immune factors. Side effects of DEC include itching and urticaria (reactions to disintegrating microfilariae), facial swelling, headache, nausea, vomiting, fever, joint pain and anorexia. Due to the severity of adverse reactions, DEC is now contraindicated except for diagnostic purposes (see above) (14).
Ivermectin (IVM), the first-line option according to the Center for Disease Control and Prevention (CDC), is a safe and efficacious anthelmintic drug that acts as microfilaricidal, embryostatic (temporary inhibition of microfilarial release from female worms) and modest permanent sterilizing action of O. volvulus (4). Ivermectin has been shown to reduce the number of microfilariae in the skin and eyes and to decrease microfilariae production for several months. However, the effect of IVM on the viability of the adult worms (macrofilaricidal effect) is considered moderate, and treatments have to be repeated every year (or at shorter intervals) to maintain skin microfilarial densities at low enough levels not to be associated with clinical manifestations (51).
To this matter, in a trial conducted by Campillo et Al., when compared to annual regimens or higher doses, a 3-monthly IVM regimen appeared to be associated with a significant reduction in the number of new onchocercal nodules (52). Nevertheless, the use of IVM is associated with common dermatologic adverse reactions triggered by the death of the microfilariae: itching, edema, and urticarial rash, while IVM use is not associated with the worsening of eye symptoms (14).
Recently, novel chemotherapeutic approaches focus on the use of antibiotics against the endosymbiotic bacteria Wolbachia, as long-term depletion of this endosymbiont impairs worm reproduction and survival (53). Daily treatment with 100 milligrams of doxycycline for six weeks (or 200 milligrams daily for four weeks) leads to an interruption of embryogenesis that lasts for 18 months or more (54).
However, these regimens are difficult to include in mass chemotherapy programs. This is due to the prolonged duration of treatment, the various contraindications to antibiotics, and the risk of inducing resistance in other pathogens. The impact of doxycycline on the duration of therapy has not been studied in nonendemic settings; however, mathematical modeling of clinical trial data from endemic areas estimated a 70–80% decrease in the lifespan of Wolbachia-depleted O. volvulus worms (54). Ivermectin treatment should be given a few days before Doxycycline. The dosage of doxycycline is 100-200 mg daily for 6 weeks. Several studies showed that administration of Doxycycline 200mg/day for six weeks followed by Ivermectin at 3 and 12 months can induce the sterility of adult female worms and can reduce the number of skin microfilariae over a long period (15). Also, a single dose combination of Ivermectin and Albendazole did not have a greater effect than Ivermectin alone. Rifampicin and azithromycin, despite their activity against Wolbachia, are not effective for clinical management of Onchocerciasis (55). Table 2 shows WHO indications for onchocerciasis treatment. Before Treatment with Ivermectin, patients should be evaluated for co-infection with Loa loa, another filarial parasite, due to the risk of potentially fatal encephalitic reaction to Ivermectin in Loa loa infected patients (56). At this regard, a ‘test-and-treat’ (TNT) strategy involving the use of a smartphone microscope device (LoaScope) has been introduced for endemic areas to identify individuals with a high risk of post-ivermectin severe adverse events (55). Treatment of co-infected people with doxycycline has only been studied in persons with Loa loa counts of <8000 microfilariae per mL. In areas of O. volvulus and Loa loa co-endemicity, new approaches for onchocerciasis elimination include the combination of test-and-treat strategy with doxycycline andthe spreading in the ground of the organophosphate larvicide temephos (57). (Wanji, et al., Implementation of test-and-treat with doxycycline and temephos ground larviciding as alternative strategies for accelerating onchocerciasis elimination in an area of loiasis co-endemicity: the COUNTDOWN consortium multi-disciplinary study protocol, 4 Dec 2019).

Table 2 Pharmaceuticals indicated or in development for onchocerciasis.
Moxidectin is an anthelmintic drug recently approved by the FDA for single-dose treatment of onchocerciasis in persons aged ≥12 years. Moxidectin (8 mg) exerts a potent microfilaricidal effect and leads to prolonged suppression of microfilaraemia, which may be the result of a robust embryostatic effect (temporary inhibition of microfilarial production by adult female worms) (58). According to a recently published, large phase 3 clinical trial conducted in the Democratic Republic of Congo, Ghana and Liberia moxidectin may be superior to Ivermectin in suppressing the presence of parasites (microfilariae) in the skin that cause the disease and that are taken up by blackflies (58). Compared to Ivermectin, Moxidectin is a stronger and longer microfilarial suppressor: its microfilaricidal effect leads to almost complete clearance of skin microfilariae, and it could be used in Loa co-endemic areas excluding people with high Loa loa microfilaremia (4). However, after a single dose, moxidectin is not considered to be curative or macrofilaricidal (killing of adult worms), while these results may be reached by the administration of repeated doses but data on repeated treatments with long follow-up times are lacking (59). A small-scale trial conducted in Ghana evaluated the efficacy, toxicity and safety profile of moxidectin, hinting at the possibility of being used after large-scale evidence for mass treatment (49).
Besides moxidectin, also flubendazole, an inhibitor of tubulin polymerization, has been investigated as a candidate drug, since it has been shown to have the ability to kill adult filarial worms. Despite this promise, flubendazole has several limitations that complicate its use, including limited oral bioavailability and human embryotoxicity (60) because of this, it is not possible to identify a flubendazole treatment regimen that would prove to be safe for humans while keeping its efficacy (61).
1-2 Several studies are paving the way to alternate anti-Wolbachia drugs with promising results. Among these, a notable example is a tylosin analogue ABBV-4083 (TylAMac), now called flubentylosin, a macrolide veterinary antibiotic, an inhibitor of bacterial protein synthesis currently in clinical development. [Taylor et al., (62)]. Flubentylosin is orally available, induces a robust anti-Wolbachia effect in several in vivo models, demonstrates clear superiority over the current treatment doxycycline, and is effective after a shorter dosing regimen (https://dndi.org/research-development/portfolio/flubentylosin/).
Treatment through Flubentylosin resulted in a >99% elimination of Wolbachia after 1-2 weeks of treatment initiation. Moreover, it has an embryostatic action leading to complete clearance of circulating microfilariae, along with expressing relatively low activity against microfilariae of L. loa (39).
Another candidate in clinical trials is the azaquinazolin AWZ1066S an antiWolbachia agent, has the potential to deliver a novel antifilarial therapy that could be deployed in target populations in a sub–7-day dosing regimen (63) (https://clinicaltrials.gov/ct2/show/NCT05084560?term=AWZ1066S&draw=2&rank=1).
In conclusion, the next years will be key for offering new safe and effective onchocerciasis drug development in an efficient strategy to definitive eradicate it (64–66).
Onchocerciasis elimination is defined as the reduction of local onchocerciasis infection and transmission to such low levels that transmission can no longer sustain itself and treatment can be safely stopped without risk of recrudescence of infection and transmission (67). In 1974, the WHO established the Onchocerciasis Control Program (OCP), while spraying started in 1975, with the aim of interrupting transmission for twenty years to allow for all existing adult worms to die. The OCP Initially implemented weekly larvicidal administration on vector breeding grounds and, after achieving this, elimination strategies required abolishing vector sources for as long as microfilariae remain in human skin. This duration was deemed to be at least 14 years (considering the life expectancies of both adult worms and microfilariae) (55, 68).
In 1987, the advent of Ivermectin has enhanced prospects for control or elimination of the disease in many areas, including Africa. The medicine is provided free of charge by Merck & Co., Inc. under the Mectizan Donation Program. Mass distribution of Mectizan (to all those aged five years or older, excluding pregnant women and those breastfeeding a child younger than one week old) revolutionized the approach to onchocerciasis control and has, since then, led to the development of similar mass drug administration programs for other neglected tropical diseases (NTDs). Every year, the program reaches more than 300 million people in 35 countries, with more than 3.4 billion treatments. (69, 70).
The first empirical evidence on the feasibility of IVM-based elimination strategies is available from studies conducted in three onchocerciasis foci in Senegal and Mali. These studies showed that after 15 to 17 years of treatment, the prevalence of infection and the intensity of transmission had fallen below postulated threshold values for elimination (71). As stated above, the effectiveness of Ivermectin on microfilarial reproductive capacity and longevity seems to be affected mainly by treatment frequency (72).
In Latin America, the areas affected by onchocerciasis were small and well-circumscribed, with an estimated half a million people infected. Here, the strategy has been based on the treatment of everyone at risk and not taking into account the levels of endemicity. The Onchocerciasis Elimination Program for the Americas (OEPA) started in 1995 and has regional resolutions to recommend periodic treatment for elimination in the WHO Region of the Americas. Eligible populations in countries endemic to the disease in this region have been treated twice or more per year (72). As a result, onchocerciasis has been eliminated from Colombia, Ecuador, Mexico and likely now Guatemala under these strategies. Only Venezuela and Brazil still have some cases, particularly deep in the Amazon forest, on their common border (73).
In sub-Saharan Africa, the African Programme for Onchocerciasis Control (APOC) was launched in 1995 to control Onchocerciasis in the remaining 19 African countries (5). Its main strategy has been the establishment of sustainable Community-Directed Treatment with Ivermectin (CDTI) aiming to obtain a beneficial effect on the incidence of onchocercal optic nerve disease and visual field loss, along with a substantial reduction in other clinical symptoms. Moreover, the APOC carried out successful anti-vector activities using aerial spraying with organophosphate and ground larvicide along thousands of kilometers of rivers in West Africa at very regular intervals during the peak breeding season, often using helicopters to treat inaccessible areas (74). Since then, CDTI strategy has proven to be extremely useful, becoming a community platform for the integration of other interventions, above all the chemotherapeutic and pharmacological ones (i.e., vitamin A supplementation and albendazole for lymphatic filariasis treatment) (5, 75).
However, as mentioned above, ivermectin-based strategies are not applicable to areas of onchocerciasis and loiasis co-endemicity (mainly in central Africa) since IVM treatment may result in severe adverse events (76).
In 2015, APOC was replaced by the Expanded Special Project for Elimination of NTDs (ESPEN), with the aim of alleviating the burden of Onchocerciasis in Africa. ESPEN relies on population-based treatment with Ivermectin, with a minimum requirement of 80% therapeutic coverage which has to go on for about 15 years of yearly treatment corresponding to the lifespan of adult O. volvulus worms (77).
In meso-and hyperendemic onchocerciasis areas (i.e., onchocercal nodule prevalence >20% in adults) in 2017 a test-and-not-treat (TaNT) strategy was launched and successfully piloted in Cameroon (Wanji, Patrick, & Ndongmo, Impact of repeated annual community directed treatment with ivermectin on loiasis parasitological indicators in Cameroon: Implications for onchocerciasis and lymphatic filariasis elimination in areas co-endemic with Loa loa in Africa, 2018).
By this approach, the relatively small proportion of L. loa-infected individuals at risk of SAEs (those with > 30,000 mf/ml) are identified and excluded from treatment with Ivermectin. This could help to prevent severe adverse events (SAEs) post-ivermectin treatment (including neurological sequelae and fatal encephalopathy).
Because polyparasitism is still widespread especially in rural communities, exploring other potential therapeutic strategies is of great interest. Commercially available aspartyl protease inhibitors (APIs) immunodeficiency syndrome (AIDS)) have been shown to have macrofilaricidal effects in in vitro studies with L4 stages of O. volvulus (78). Alternative strategies to achieve onchocerciasis elimination is a test-and-treat with the doxycycline and ground larviciding, with a large-scale implementation trial in Cameroon being currently evaluated.
The advantages of this model are a reduction in community prevalence of skin microfilaria by 37% and a superior range of anti-filarial efficacies of Doxycycline in the absence of loiasis-associated SAE [Wanji et al., (57)]. In 2020 despite disruptions caused by the COVID-19 pandemic in endemic countries for Onchocerciasis WHO Department of Control of Neglected Tropical Diseases continued the prevention of the transmission by distributing ivermectin treatment to more than 112 million people (79).
In order to improve the effectiveness of the control program, OCP has sponsored the development of ONCHOSIM, a computer program that models onchocerciasis transmission and control. According to ONCHOSIM predictions, the outcome of elimination of onchocerciasis depends on pre-control endemicity level, frequency of MDA and treatment coverage (TC) achieved (80).
As a result, in 2016, the WHO recommended stopping mass drug administration (MDA) programs from verifying the interruption of transmission using geostatistical models (69). To accelerate the elimination of Onchocerciasis by 2025, the WHO recommends the Ov-16 serological test for onchocerciasis mapping to determine eligibility for MDA, as this would help to detect a status of infection and parasite transmission at a low level of endemicity. According to the WHO Onchocerciasis Technical Advisory Subgroup’s report of 2018, the provisional threshold for commencing mass ivermectin treatment is set at 2% Ov-16 seropositivity (44). Conflicts and civil wars are further obstacles to the monitoring of endemic areas and the widespread distribution of medicines. In such contexts, MDA could be carried out through collaboration with local NGOs or humanitarian organizations, whose volunteers are often present in war zones to achieve an improved geographic coverage of Ivermectin (81). Furthermore, there is an effort run by The Sabin Vaccine Institute Product Development Partnership (Sabin PDP) and other partners to prophylactic or therapeutic onchocerciasis vaccine. Also, a global initiative known as TOVA – The Onchocerciasis Vaccine for Africa – was launched in 2015 to evaluate vaccine development as a complementary control tool (68).
To date, three candidate antigens have proven to be efficacious in three different filarial animal model systems and three independent laboratories. A recently published study showed the feasibility of eliciting significant protective immunity in mice using selected recombinant Onchocerca volvulus antigens produced in yeast or bacteria, including Ov-103, Ov-RAL-2, and Ov-CPI-2M (45, 69).
Finally, other strategies are primarily based on vector elimination: the Esperanza Window Trap (EWT) was used for monitoring the transmission of O. volvulus in Mexico in elimination programs. The program consisted in positioning a vertical blue and black striped sheet with a sticky surface that attracted black flies. Later, EWT was optimized in Northern Uganda and has resulted in vector biting rates reduction (82). Also, on the Bioko islands, Republic of Guinea, a seasonally adjusted vector control model based on the use of larvicides (temephos) spread by helicopters on riverbeds and areas with high density, led to the successful elimination of the vector (67, 83–89).
Finally, in the Democratic Republic of Congo and South Sudan, the “Slash and Clear” strategy, which involves the removal of vegetation from S. damnosum breeding sites considering climatic and seasonal variations, showed also to be able to reduce vector populations (82).
Despite the various control programs implemented in recent decades, river blindness remains a global health problem, a cause of disability and stigma, a disfiguring skin disease and a source of poverty in countries where it is endemic (90–95). Although valuable diagnostic tools are available for individual use, community-based onchocerciasis control needs a reliable, cheap, and more practical technique for rapid epidemiological assessments. Numerous efforts to develop novel diagnostic assays that support the monitoring of current and future control measures are underway (96-100). Future epidemiology-directed control strategies need to take into account challenges such as Loa loa co-infections and environmental sustainability and will likely have to combine vector control, community-directed mass administration programs and future therapeutic perspective i.e. CC6166 an anthelmintic molecules with macrofilaricidal action in phase I development with DNDi (95, 101-103). (https://dndi.org/wp-content/uploads/2021/06/DNDi-RFP-Filarial-PharmaceuticalDevelopment-June2021.pdf).
Conceptualization, FD, and MC; methodology, FD; investigation, FVS, FB and FD; writing—original draft preparation, GGP; RN; EP; SC; GG; ED; AR; VT; MC; RL; GP; BG; RP; CP; CR; GP; writing—review and editing, AS, FB, and EN; supervision, AS, FD and GD. All authors have read and agreed to the published version of the manuscript.
We thank Marco Rossetti, who created our figures (cm9zc2V0dGltYXJjb3Bhc3F1YWxlQGdtYWlsLmNvbQ==).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Vinkeles Melchers N. V. S., Stolk W. A., Murdoch M. E., Pedrique B., Kloek M., Bakker R., et al. (2021). How does onchocerciasis-related skin and eye disease in Africa depend on cumulative exposure to infection and mass treatment? PloS Negl. Trop. Dis. 15 (6), e0009489. doi: 10.1371/journal.pntd.0009489
2. World Health Organization (WHO). Onchocerciasi Key Fact (Geneva) (2022). Available at: https://www.who.int/news-room/fact-sheets/detail/onchocerciasis.
3. Pearlman E, Gillette-Ferguson I. Onchocerca volvulus, wolbachia and river blindess. Chem Immunol Allergy (2007) 92:254–65. doi: 10.1159/000099276
4. CDC. Tratto da (2020). Available at: https://www.cdc.gov/parasites/onchocerciasis/index.html.
5. World Health Organization & African Programme for Onchocerciasis Control. The WHO african programme for onchocerciasis control: final evaluation report. african programme for onchocerciasis control. (2015). Available at: https://apps.who.int/iris/handle/10665/275724.
6. Chekea RA, Garmsb R. Indices of onchocerciasis transmission by different members of the simulium damnosum complex conflict with the paradigm of forest and savanna parasite strains. Elsevier-Acta Tropica (2013) 125(1):43–52. doi: 10.1016/j.actatropica.2012.09.002
7. Cheke R, Little K, Young S, Walker M, Basáñez M. Taking the strain out of onchocerciasis? a reanalysis of blindness and transmission data does not support the existence of a savannah blinding strain of onchocerciasis in West Africa. Adv Parasitol (2021) 112:1–50. doi: 10.1016/bs.apar.2021.01.002
8. Showlera AJ, Nutmanb TB. Imported onchocerciasis in migrants and travelers. Curr Opin Infect Dis (2018), 393–8. doi: 10.1097/QCO.0000000000000483
9. Bottieau E, Huits R, Van Den Broucke S. Human filariasis in travelers and migrants: A retrospective 25-year analysis at the institute of tropical medicine, Antwerp, Belgium. Clin Infect Dis (2021) 74. doi: 10.1093/cid/ciab751
10. Puente S, Ramirez-Olivencia G, Lago M, Subirats M, Perez-Blazquez E, et al. Dermatological manifestations in onchocerciasis: A retrospective study of 400 imported cases. Enferm Infecc Microbiol Clin (Engl Ed) (2018) 10:633–9. doi: 10.1016/j.eimc.2017.11.016
11. Hamad IC, Ciannameo A, Grilli E, Urbinati L, Monteiro G, Scarcella C, et al. Seroprevalence of five neglected parasitic diseases among immigrants accessing five infectious and tropical diseases units in Italy: A cross-sectional study. Clin Microbiol Infect (2017) 23(5):335.e1–5. doi: 10.1016/j.cmi.2017.02.024
12. Adler PH, Cheke RA, Post RJ. Evolution, epidemiology, and population genetics of black flies (Diptera: Simuliidae). Infection Genet Evolution (2010) 10(7):846–65. doi: 10.1016/j.meegid.2010.07.003
13. Egbert P. R., Jacobson D. W., Fiadoyor S., Dadzie P., Ellingson K. D. (2005). Onchocerciasis: A potential risk factor for glaucoma. Br. J. Ophthalmol. 89 (7), 796–798. doi: 10.1136/bjo.2004.061895
14. Center Diseases Control and Prevention (CDC). (2022). Parasites - Onchocerciasis (also known as River Blindness). Available at https://www.cdc.gov/parasites/onchocerciasis/index.html. Last access 20 October 2022
16. Murdoch ME, Murdoch IE, Evans J, Yahaya H, Njepuome N, Cousens S, et al. Pre-control relationship of onchocercal skin disease with onchocercal infection in Guinea Savanna, Northern Nigeria. PLoS Negl Trop Dis (2017) 11(3):e0005489. doi: 10.1371/journal.pntd.0005489
17. Kaiser C., Rubaale T., Tukesiga E., Kipp W., Kabagambe G., Ojony J. O., et al. (2011). Association between onchocerciasis and epilepsy in the itwara hyperendemic focus, West Uganda: controlling for time and intensity of exposure. Am. J. Trop. Med. Hyg. 85 (2), 225–228. doi: 10.4269/ajtmh.2011.10-0544
18. Katawa G, Layland L. Hyperreactive onchocerciasis is characterized by a combination of Th17-Th2 immune responses and reduced regulatory T cells. PLoS Negl Trop Dis (2015) 9(1):e3414. doi: 10.1371/journal.pntd.0003414
19. Antinori S, Parravicini C, Galimberti L, Tosoni A, Giunta P, Galli M, et al. Is imported onchocerciasis a truly rare entity? case report and review of the literature. Travel Med Infect Dis (2017) 16:11–17. doi: 10.1016/j.tmaid.2017.02.006
20. Mauprivez C., Harlay P., Gruffaz F., Goudot P. (2016). Calcified onchocercal nodule in the infratemporal fossa: a rare case. Br. J. Oral. Maxillofac. Surg. 54 (4), 463–465. doi: 10.1016/j.bjoms.2015.09.012
21. Hoerauf A, Kruse S, Brattig N, Heinzmann A, Mueller-Myhsok B, Deichmann K. The variant Arg110Gln of human IL-13 is associated with an immunologically hyper-reactive form of onchocerciasis (sowda). Microbes Infect (2002) doi. doi: 10.1016/s1286-4579(01)01507-6
22. Abdul-Ghani R, Mahdy M, Beier J. Onchocerciasis in Yemen: Time to take action against a neglected tropical parasitic disease. Acta Trop (2016) 162:133–41. doi: 10.1016/j.actatropica.2016.06.017
23. Michele EM. Onchodermatitis: Where are we now? Disease Trop Med Infectious. (2018) 3(3):94). doi: 10.3390/tropicalmed3030094
24. Traore M. O., Sarr M. D., Badji A., Bissan Y., Diawara L., Doumbia K., et al. (2012). Proof-of-principle of onchocerciasis elimination with ivermectin treatment in endemic foci in Africa: final results of a study in Mali and Senegal. PloS Negl. Trop. Dis. 6 (9), e1825. doi: 10.1371/journal.pntd.0001825
25. Nava VE, Ejilemele AA. Onchocerca volvulus mimicking metastatic breast carcinoma. Am Soc Trop Med Hygiene (2020), 487–8. doi: 10.4269/ajtmh.19-0740
26. Martelli G., Di Girolamo C., Zammarchi L., Angheben A., Morandi M., Tais S., et al. (2017). Seroprevalence of five neglected parasitic diseases among immigrants accessing five infectious and tropical diseases units in Italy: a cross-sectional study. Clin. Microbiol. Infect. 23 (5), 335.e1–335.e5. doi: 10.1016/j.cmi.2017.02.024
27. Egbert PR, Jacobson DW, Fiadoyor S, Dadzie P, Ellingson KD. Onchocerciasis: A potential risk factor for glaucoma. Br J Ophthalmol (2005) 89(7):796–8. doi: 10.1136/bjo.2004.061895
28. Turner JD. Wolbachia lipoprotein stimulates innate and adaptive immunity through toll-like receptors 2 and 6 to induce disease manifestations of filariasis. J Biol Chem (2009) 284(33):22364–78. doi: 10.1074/jb
29. Gillette-Ferguson I, Daehnel K, Hise A, Sun Y, Carlson E, Diaconu E, et al. Toll-like receptor 2 regulates CXC chemokine production and neutrophil recruitment to the cornea in onchocerca volvulus/Wolbachia-induced keratitis. Infect Immun (2007) 75(12):5908–15. doi: 10.1128/IAI.00991-07
30. Mauprivez C, Harlay A, Gruffaz A, Goudot P. Calcified onchocercal nodule in the infratemporal fossa:a rare case. Br J Oral Maxillofac Surgery Elservier (2016) 54(4):463–5. doi: 10.1051/sfco/20156302034
31. Hong WD, Benayoud F, Nixon GL, Ford L, Johnston KL, Clare RH, et al. (2019). AWZ1066S, a highly specific anti-Wolbachia drug candidate for a short-course treatment of filariasis. Proc. Natl. Acad. Sci. U S A. 116 (4), 1414–1419. doi: 10.1073/pnas.1816585116
32. Hotterbeekxa A, Ssonkob VN, Oyetc W, Lakwod T. Neurological manifestations in onchocerca volvulus infection: A review. Brain Res Bulletin Elsevier (2019), 39–44. doi: 10.1016/j.brainresbull.2018.08.024
33. Colebunders R, Mandro M. Risk factors for epilepsy in bas-uélé province, democratic republic of the Congo: a case–control study. Internation J Infect Dis (2016) 49):1–8.
34. Colebunders R, Siewe Fodjo JN, Hopkins A, Hotterbeekx A, Lakwo TL, Kalinga A, et al. From river blindness to river epilepsy: implications for onchocerciasis elimination programmes. PLoS Negl Trop Dis (2019) 13(7):e0007407. doi: 10.1371/journal.pntd.0007407
35. Abd-Elfarag GO, Edridge AWD, Spijker R, Sebit MB, van Hensbroek MB. Nodding syndrome: A scoping review. Trop Med Infect Dis (2021) 6(4):211. doi: 10.3390/tropicalmed6040211
36. Hotterbeekxa A, Raimonb S, Abd-Elfaragc G, Cartere JY, Sebitf W. Onchocerca volvulus is not detected in the cerebrospinal persons with onchocerciasis-associated epilepsy. Int J Infect Dis (2020) 119–23. doi: 10.1016/j.ijid.2019.11.029
37. Idro R, Anguzu R, Ogwang R, Akun PA, Mwaka A, Opar B, et al. Doxycycline for the treatment of nodding syndrome (DONS); the study protocol of a phase II randomised controlled trial. BMC Neurol (2019) doi. doi: 10.1186/s12883-019-1256-z
38. Unnasch TR, Golden A. Diagnostics for onchocerciasis in the era of elimination. (P. 29471336, & p. PMC5881263., a cura di). Int Health (2018) 10(suppl_1):i20–6. doi: 10.1093/inthealth/ihx047
39. Brattig NW, Cheke RA, Garms R. Onchocerciasis (river blindness) – more than a century of research and control. Acta Trop (2021) 218:105677. doi: 10.1016/j.actatropica.2020.105677
40. Bennuru S, Oduro-Boateng G, Osigwe C, Del Valle P, Golden A, Ogawa GM, et al. Integrating multiple biomarkers to increase sensitivity for the detection of onchocerca volvulus infection. J Infect Dis (2020) 221(11). doi: 10.1093/infdis/jiz307
41. Yengo BN, Shintouo CM, Hotterbeekx A, Yaah NE, Shey RA, Quanico J, et al. Immunoinformatics design and assessment of a multiepitope antigen (OvMCBL02) for onchocerciasis diagnosis and monitoring. Diagnostics (Basel) (2022) 12(6):1440. doi: 10.3390/diagnostics12061440
42. Shintouo C, Ghogomu S, Shey R, Hotterbeekx A, Yagmur E, Mets T, et al. Tandem use of OvMANE1 and ov-16 ELISA tests increases the sensitivity for the diagnosis of human onchocerciasis. Life (Basel) (2021) 11(12):1284. doi: 10.3390/life11121284
43. Burbelo P, Leahy H, Iadarola M, Nutman T. A four-antigen mixture for rapid assessment of onchocerca volvulus infection. PLoS Negl Trop Dis (2009) 3(5):e438. doi: 10.1371/journal.pntd.0000438
44. Organization. W. H (2017). Report of the 1st meeting of the WHO onchocerciasis technical advisory subgroup, in: Varembé Conference Centre, Geneva, Switzerland.
45. Lagatie O, Merino M, Batsa Debrah L, Debrah AY, Stuyver LJ. An isothermal DNA amplification method for detection of onchocerca volvulus infection in skin biopsies. Parasit Vectors (2016) 9(1):624. doi: 10.1186/s13071-016-1913-7
46. Noormahomed EV, Akrami K, Mascaró-Lazcano C. Onchocerciasis, an undiagnosed disease in Mozambique: identifying research opportunities. Parasites vectors. (2016) doi. doi: 10.1186/s13071-016-1468-7
47. Patton JB, Bennuru S, Eberhard ML, Hess JA, Torigian A, Lustigman S, et al. Development of onchocerca volvulus in humanized NSG mice and detection of parasite biomarkers in urine and serum. PLoS Negl Trop Dis (2018) 12(12):e0006977. doi: 10.1371/journal.pntd.0006977
48. Stingl P. Onchocerciasis: developments in diagnosis, treatment and control. Trop Med Dermatol (2009) 48(4):393–6. doi: 10.1111/j.1365-4632.2009.03843.x
49. Awadzi K, Opoku ON, Attah SK, Lazdins-Helds J, Kuesel AC. A randomized, single-Ascending-Dose, ivermectin-controlled, double-blind study of moxidectin in onchocerca volvulus infection. PLoS Negl Trop Dis (2014) 8(6):e2953. doi: 10.1371/journal.pntd.0002953
50. Higazi TB, Geary TG, Mackenzie CD. Chemotherapy in the treatment, control, and elimination of human onchocerciasis. Res Rep Trop Medicine 5 (2014), 77–93. doi: 10.2147/RRTM.S36642
51. World Health Organization, African Programme for Onchocerciasis Control. Conceptual and operational framework of onchocerciasis elimination with ivermectin treatment. In: African Programme for Onchocerciasis Control (2010). Available at: https://apps.who.int/iris/handle/10665/275466
52. Campillo JT, Chesnais CB, Pion SDS, Gardon J, Kamgno J, Boussinesq M. Individuals living in an onchocerciasis focus and treated three-monthly with ivermectin develop fewer new onchocercal nodules than individuals treated annually. Parasites Vectors (2020) 13(1):258. doi: 10.1186/s13071-020-04126-x
53. Hoerauf A, Specht S, Büttner M, Pfarr K, Hoerauf S, Specht SK. Wolbachia endobacteria depletion by doxycycline as antifilarial therapy has macrofilaricidal activity in onchocerciasis:a randomized placebo-controlled study. Med Microbiol Immunol (2008) 197:295–311. doi: 10.1007/s00430-007-0062-1
54. Walker M, Specht S, Churcher TS, Hoerauf A, Taylor H, Basáñez M-G. Therapeutic efficacy and macrofilaricidal activity of doxycycline for the treatment of river blindness. Clin Infect Dis (2015) 60:1199–207. doi: 10.1093/cid/ciu1152
55. Boussinesqa M, Fobi GC, Kuesel C. Alternative treatment strategies to accelerate the elimination of onchocerciasis. Int Health (2018) 10:i40–8. doi: 10.1093/inthealth/ihx054
56. Vinkeles Melchers NVS, Coffeng LE, Boussinesq M, Pendrique. B, Pion SDS, Tekle A, et al. Projected number of people with onchocerciasis-loiasis coinfection in Africa, (1995 to 2025). Clin Infect Dis (2020), 2281–9. doi: 10.1093/cid/ciz647
57. Wanji S, Nji TM, Hamill L, Dean L, Ozano K. Implementation of test-and-treat with doxycycline and temephos ground larviciding as alternative strategies for accelerating onchocerciasis elimination in an area of loiasis co-endemicity. Parasites Vectors (2019) 12(574). doi: 10.1186/s13071-019-3826-8
58. Opoku NO, Bakajika DK, Kanza EM, Howard H, Mambandu GL, Nyathirombo A, et al. Single dose moxidectin versus ivermectin for Onchocerca volvulus infection in Ghana, Liberia, and the Democratic Republic of the Congo: a randomised, controlled, double-blind phase 3 trial. Lancet (2018) 392(10154):1207–16. doi: 10.1016/S0140-6736(17)32844-1
59. Milton P, Hamley JI, Walker M, Basáñez M-G. Moxidectin: an oral treatment for human onchocerciasis. Expert Rev Anti-infective Ther (2020). doi: 10.1080/14787210.2020.1792772
60. Akama T, Freund RY, Berry PW, Carter DS, Easom EE, Jarnagin K. Macrofilaricidal benzimidazole–benzoxaborole hybrids as an approach to the treatment of river blindness: Part 1. amide linked analogs. ACS Infect Dis (2019). doi: 10.1021/acsinfecdis.9b00396
61. Lachau-Durand S, Lammens L. Preclinical toxicity and pharmacokinetics of a new orally bioavailable flubendazole formulation and the impact for clinical trials and risk/benefit to patients. PLoS Negl Trop Diseases. (2019). doi: 10.1371/journal.pntd.0007026
62. Taylor MJ, von Geldern TW, Ford L, Hübner MP, Marsh K, Johnston KL, et al. Preclinical development of an oral anti-wolbachia macrolide drug for the treatment of lymphatic filariasis and onchocerciasis. Sci Transl Med (2019) 11(483):eaau2086. doi: 10.1126/scitranslmed.aau2086
63. Hendy A., Krüger A., Pfarr K., De Witte J., Kibweja A., Mwingira U., et al. (2018). The blackfly vectors and transmission of onchocerca volvulus in mahenge, south eastern Tanzania. Acta Trop. 181:50–59. doi: 10.1016/j.actatropica.2018.01.009
64. Johnston KL, Hong WD, Turner JD, O'Neill PM, Ward SA, Taylor MJ. Anti-Wolbachia drugs filariasis. Trends Parasitol (2021) 37(12):1068–81. doi: 10.1016/j.pt.2021.06.004
65. Ngwewondo A, Scandale I, Specht S. Onchocerciasis drug development: from preclinical models to humans. Parasitol Res (2021) 120(12):3939–64. doi: 10.1007/s00436-021-07307-4
66. Ehrens A, Hoerauf A, Hübner MP. Current perspective of new anti-wolbachial and direct-acting macrofilaricidal drugs as treatment strategies for human filariasis. GMS Infect Dis (2022) 10:Doc02. doi: 10.3205/id000079
67. Traorè S, Wilson M, Sima A, Barro T, Diallo A. The elimination of the onchocerciasis vector from the island of bioko as aresult of larvicing by WHO African programme for onchocerciasis control. ELSEVIER (2009) 111:211–8.
68. Boatin B. The onchocerciasis control programme in West Africa (OCP). Ann Trop Med Parasitol (2008) 102 Suppl 1:13–7. doi: 10.1179/136485908X337427
69. WHO. Guidelines for stopping mass drug administration and verifying elimination of human onchocerciasis: criteria and procedures. In: . Geneva (2016).
70. Thylefors B. The mectizan donation program (MDP). Ann Trop Med Parasitol (2008) 102. doi: 10.1179/136485908X337481
71. Diawara L, Traoré MO, Badji A, Bissan Y, Doumbia K, Goita SF, et al. Feasibility of onchocerciasis elimination with ivermectin treatment in endemic foci in Africa: First evidence from studies in Mali and Senegal. (2009). doi: 10.1371/journal.pntd.0000497
72. Puente S., Ramirez-Olivencia G., Lago M., Subirats M., Perez-Blazquez E., Bru F., et al. (2018). Dermatological manifestations in onchocerciasis: A retrospective study of 400 imported cases. Enferm Infecc Microbiol. Clin. (Engl Ed). 36 (10), 633–639. doi: 10.1016/j.eimc.2017.11.016
73. Hopkins A. Onchocerciasis then and now: achievements, priorities and challenges. Community Eye Health (2017) 30:92–5.
74. Sauerbrey M., Rakers L. J., Richards F. O. (2018). Progress toward elimination of onchocerciasis in the americas. Int. Health 10 (suppl_1), i71–i78. doi: 10.1093/inthealth/ihx039
75. Tamarozzi F, Halliday A, Gentil K, Hoerauf A. Onchocerciasis: the role of wolbachia bacterial endosymbionts in parasite biology, disease pathogenesis, and treatment. Americ Soc microbiology-Clinical Microbiol Rev (2011) 24(3):459–68. doi: 10.1128/CMR.00057-10
76. Cano J, Basáñez M-G, Pullan RL. Identifying co-endemic areas for major filarial infections in sub-Saharan Africa: seeking synergies and preventing severe adverse events during mass drug administration campaigns. Parasites Vectors (2018) 70:11. doi: 10.1186/s13071-018-2655-5
77. Hopkins AD. Neglected tropical diseases in Africa: a new paradigm. Int Health (2016) 8. doi: 10.1093/inthealth/ihv077
78. Beld L, Jung H, Bulman CA. Aspartyl protease inhibitors as anti-filarial drugs. pathogens (2022) 11:707. doi: 10.3390/pathogens11060707
79. World Health Organitation (WHO). Onchocerciasis (river blindness). (2022) Availble at: https://www.who.int/health-topics/onchocerciasis#tab=tab_1 (last access 20 October 2022)
80. Duamor CT, Datchoua-Poutcheu FR, Chounna Ndongmo WP, Yoah AT, Njukang E, Kah E, et al. Programmatic factors associated with the limited impact of community-directed treatment with ivermectin to control onchocerciasis in three drainage basins of south West Cameroon. PLoS. (2017) 11(11):e0005966. doi: 10.1371/journal.pntd.0005966
81. Colebunders R, Mandro M, Njamnshi AK, Boussinesq M, Hotterbeekx A, Kamgno J, et al. Report of the first international workshop on onchocerciasis-associated epilepsy. Infect Dis Poverty (2018) 7:23. doi: 10.1186/s40249-018-0400-0
82. Lakwo T, Oguttu D, Ukety T, Post R. Onchocerciasis elimination: Progress and challenges. Res Rep Trop Med (2021), 81–95.
83. Hess JA, Zhan B, Bonne-Année S, Deckman JM, Bottazzi ME, Hotez PJ, et al. Vaccines to combat river blindness: expression, selection and formulation of vaccines against infection with onchocerca volvulus in a mouse model. Int J Parasitol (2014) 44(9):637–46. doi: 10.1016/j.ijpara.2014.04.006
84. World Health Organization, African Programme for Onchocerciasis Control. Report of the consultative meetings on strategic options and alternative treatment strategies for accelerating onchocerciasis elimination in Africa. African Programme for Onchocerciasis Control. (2015). Available at: https://apps.who.int/iris/handle/10665/343028
85. Al-Kubati AS, Mackenzie CD, Boakye D, Al-Qubati Y, Al-Samie AR, Awad IE. Onchocerciasis in Yemen: moving forward towards an elimination program. Int Health (2018) doi. doi: 10.1093/inthealth/ihx055
86. Christop K, Sebastien DS, Boussineq P. Case-control studies on the relationship between onchocerciasis and epilepsy: Systematic review and meta-analysis. PLoS Negl Trop Dis (2013) 7). doi: 10.1371/journal.pntd.0002147
87. Chesnais CB, Pion D, Boullé C, Gardon J, Gardon-Wendel N, Al. E. Individual risk of post-ivermectin serious adverse events in subjects infected with loa loa. E Clin medicine-Elsevier (2020) 28(100582). doi: 10.1016/j.eclinm.2020.100582
88. Colebunders R, Basanez MG, Siling K, Post RJ, Rotsaert B, mbando M, et al. From river blindness control to elimination: bridge over troubled water. Infect Dis Poverty (2018) 7(1):21. doi: 10.1186/s40249-018-0406-7
89. Tratto da. Available at: https://dndi.org/research-development/portfolio/flubentylosin/.
90. Tratto da. Available at: https://dndi.org/wp-content/uploads/2021/06/DNDi-RFP-Filarial-PharmaceuticalDevelopment-June2021.pdf.
91. Kaiser C, Pion SD, Boussinesq M. Case-control studies on the relationship between onchocerciasis and epilepsy: Systematic review and meta-analysis. PLoS (2013) 13. doi: 10.1371/journal.pntd.0002147
92. Kareva I. Immune suppression in pregnancy and cancer: Parallels and insights. Transl Oncol (2020) 13(7):100759. doi: 10.1016/j.tranon.2020.100759
93. Koehler J, Ritzer B, Gebhardt F, Kirchhoff C. Use of monoclonal antibody therapy for nosocomial SARS-CoV-2 infection in patients at high risk for severe COVID-19: Experience from a tertiary-care hospital in Germany. Infection. (2021) 49(6):1313–8.
94. Lagatie O, Merino M, Debrah LB, Debrah AY, Stuyver LJ. An isothermal DNA amplification method for detection of onchocerca volvulus infection in skin biopsies. Parasites Vectors (2016) 624). doi: 10.1186/s13071-016-1913-7
95. Lustigman S, Makepeace BL, Klei TL, Babayan SA, Hotez P, Abraham D, et al. Onchocerca volvulus: the road from basic biology to a vaccine. Trends Parasitol (2018) 34(1):64–79. doi: 10.1016/j.pt.2017.08.011
96. VinkelesMelchers NVS, Stolk WA, van Loon W, Pedrique B, Bakker R, Murdoch ME, et al. The burden of skin disease and eye disease due to onchocerciasis in countries formerly under the African programme for onchocerciasis control mandate for 1990, 2020, and 2030. PLoS Negl Trop Dis (2021) 15(7):e0009604. doi: 10.1371/journal.pntd.0009604
97. Poverty TF. Tratto da (2018). Available at: https://www.who.int/tdr/news/2018/moxidectin-approved-as-treatment-for-river-blindness/en/.
98. WHO. Progress towards eliminating onchocerciasis in the WHO region of the americas: verification by WHO of elimination of transmission in Colombia Vol. 88:381–5. Wkly Epidemiol Rec. (2013).
99. Colebunders R, Hendy A, Mokili JL, Wamala JF, Kaducu J, Kur L, et al. Nodding syndrome and epilepsy in onchocerciasis endemic regions: comparing preliminary observations from south Sudan and the democratic republic of the Congo with data from Uganda. BMC Res Notes (2016) 9:182. doi: 10.1186/s13104-016-1993-7
100. World Health Organization, African Programme for Onchocerciasis ControlThe blackfly vectors and transmission of onchocerca volvulus in mahenge, south eastern Tanzania. Acta Tropica (2018) 181:50–9. doi: 10.1016/j.actatropica.2018.01.009
101. Rawson TM, Moore LSP, Castro-Sanchez E, Charani F, Davies G, Satta MJ, et al. COVID-19 and the potential long-term impact on antimicrobial resistence. J Antimicrob Chemother (2020) doi. doi: 10.1093/jac/dkaa194
102. Wanji S, Chounna Ndongmo WP, Fombad FF, Kengne-Ouafo JA, Njouendou AJ, Longang Tchounkeu YF, et al. Impact of repeated annual community directed treatment with ivermectin on loiasis parasitological indicators in Cameroon: Implications for onchocerciasis and lymphatic filariasis elimination in areas co-endemic with loa loa in Africa. PLoS Negl Trop Dis (2018) 12(9):e0006750. doi: 10.1371/journal.pntd.0006750
103. World Health Organization, African Programme for Onchocerciasis Control Informal consultation on elimination of onchocerciasis transmission with current tools: "shrinking the map". (2009). African Programme for Onchocerciasis Control. https://apps.who.int/iris/handle/10665/275793.
Keywords: Onchocerciasis, Ivermectin, Diethylcarbamazine, blindness, microfilariae; NTDs, Africa
Citation: Frallonardo L, Di Gennaro F, Panico GG, Novara R, Pallara E, Cotugno S, Guido G, De Vita E, Ricciardi A, Totaro V, Camporeale M, De Iaco G, Bavaro DF, Lattanzio R, Patti G, Brindicci G, Papagni R, Pellegrino C, Santoro CR, Segala FV, Putoto G, Nicastri E and Saracino A (2022) Onchocerciasis: Current knowledge and future goals. Front. Trop. Dis. 3:986884. doi: 10.3389/fitd.2022.986884
Received: 05 July 2022; Accepted: 18 October 2022;
Published: 17 November 2022.
Edited by:
Joseph Daniel Turner, Liverpool School of Tropical Medicine, United KingdomReviewed by:
Sindhu Chadalawada, Alameda Health System, United StatesCopyright © 2022 Frallonardo, Di Gennaro, Panico, Novara, Pallara, Cotugno, Guido, De Vita, Ricciardi, Totaro, Camporeale, De Iaco, Bavaro, Lattanzio, Patti, Brindicci, Papagni, Pellegrino, Santoro, Segala, Putoto, Nicastri and Saracino. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francesco Di Gennaro, ZnJhbmNlc2NvLmRpZ2VubmFybzFAdW5pYmEuaXQ=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.