 Marina Oliveira Hermsdorf1
Marina Oliveira Hermsdorf1 Tércia Moreira Ribeiro da Silva1
Tércia Moreira Ribeiro da Silva1 Sheila Aparecida Ferreira Lachtim1
Sheila Aparecida Ferreira Lachtim1 Fernanda Penido Matozinhos1,2
Fernanda Penido Matozinhos1,2 Mark Anthony Beinner1
Mark Anthony Beinner1 Ed Wilson Rodrigues Vieira1*
Ed Wilson Rodrigues Vieira1*- 1Department of Maternal-Infant and Public Health, Universidade Federal de Minas Gerais, Belo Horizonte, Brazil
- 2Postgraduate Nursing Program, Universidade Federal de Minas Gerais, Belo Horizonte, Brazil
Objectives: To analyze the availability of the Yellow Fever (YF) vaccine at Primary Health Care (PHC) services located in areas with vaccine recommendation in Brazil between two different periods.
Methods: Secondary data from the Program for Improving Access and Quality in PHC, with 13,666 services in 2013-14, and 19,125 in 2017-18, were used. A structured questionnaire was used for the data collection. Pearson’s chi-square and thematic cartographic maps were used to analyze the frequency of the YF vaccine, and Poisson regression with robust variances was used to analyze the associated factors.
Results: The overall frequency of PHC facilities with YF vaccine always available increased from 87.0% (CI 95%; 86.4-87.5) in 2013-14 to 89.7% (CI 95%; 89.2-90.1) in 2017-18. Facilities located in the South, Southeast, Midwest and Northern regions and in non-state capitals, as well as centers that had adequate facilities for vaccination actions, as well as an adey -50quate cold chain network, showed a greater prevalence of YF vaccine always available.
Conclusion: The frequency of a steady supply of YF vaccine available at PHC facilities, located in Areas with Routine Vaccination Recommendations, increased between 2013-14 and 2017-18. Geographical and structural characteristics related to vaccine actions at PHC facilities influenced access. The effective supply chain networks for the YF vaccine, together with adequate services at PHC facilities are essential to ensuring that the YF vaccine is always available.
Introduction
Despite the importance of epidemiological control of the Yellow Fever (YF), many countries have reported shortages of vaccine for up to three or more years during the last decade (1) and others have constantly faced situations of insufficient stock, even while experiencing disease outbreaks (2–4). Considering that such a vaccine is highly effective and that a single dose provides immunity throughout life, the inadequate availability of vaccines, in the face of demand, may be one of the answers to the persistence of the problem that poses risks to global health (2, 5).
In addition to the shortcomings in the supply of the vaccines, recognized in many countries, problems with continued access can affect the day-to-day of the health services that should consistently offer it as part of the immunization program supply chain. In this regard, the lack of vaccines, when individuals seek them out, has been repeatedly identified as one of the main causes of missed opportunities in vaccination (6, 7).
There are no studies that analyze the continued availability of the YF vaccine in Brazilian Primary Health Care (PHC) services. Additionally, there is still no evidence that the expansion of the Areas with Routine Vaccination Recommendations (ARVR) (8), beginning in 2001, in Brazil, has been accompanied by an adequate supply of vaccine in these services. On the another hand, there is evidence that geographical and structural characteristics of the services can influence the continued availability of vaccines at PHC facilities (5, 7, 9, 10).
The expansion of ARVR was intensified simultaneously with the emergence of an YF outbreak in Brazil from 2016 to 2017 (8). This outbreak may have contributed to the availability of the YF vaccine at PHC facilities. In fact, the acquisition of YF vaccine was expanded in response to the outbreak by the Brazilian Minister of Health in 2016. However, the distribution of this vaccine to the PHC facilities did not occur equally, resulting in shortages of this vaccine throughout metropolitan regions (11).
Considering this context and the recommendations for assessing the distribution of YF vaccines (3), the objective of this study was to analyze the availability of the YF vaccine at PHC facilities located in ARVR in Brazil, between the periods 2013-14 and 2017-18.
Methods
This was a study that used secondary data from a cross-sectional survey applied to the professionals responsible for the PHC facilities that participated in the second and third cycles of the Program for Improving Access and Quality in Primary Health Care (PIAQ-PHC). The PIAQ-PHC is a financial incentive program of the Brazilian Ministry of Health that aims to improve access and quality of PHC in the context of the National Health System (Sistema Único de Saúde - SUS)
These evaluation cycles were conducted by the Ministry of Health in partnership with 41 research institutions under the leadership of the Oswaldo Cruz Foundation (12). Data collection was conducted in 2013-14 (second cycle) and in 2017-18 (third cycle), using a structured questionnaire. On-site guided inspections and verification of records was also done in order to certify the information contained in the questionnaire. About one thousand trained interviewers took part in data collection using electronic devices (tablets). The questionnaire responses were automatically sent to a central server, and the evaluation of data consistency was performed under the coordination of the Department of Primary Care of the Ministry of Health. The data resulting from these two processes are available at https://aps.saude.gov.br/ape/pmaq.
The original data totaled 24,499 PHC services evaluated in 2013-14 and 30,346, in 2017-18. In this study, was considered: services located in the ARVR that offered vaccinations regularly. Applying these criteria, 13,666 PHC facilities from the second cycle and 19,125 from the third were studied, corresponding to approximately 45.0% and 78.0% of the total Brazilian PHC facilities, respectively. The exclusion of services did not represent losses for this study. We selected all vaccination services that should mandatorily offer the YF vaccine in municipalities that adhered to the Program.
The dependent variable was “YF vaccine always available” (Yes/No), which means that when a person seeks the service to receive the vaccine, the vaccine is always available. The independent variables, chosen on the basis of previous studies and for theoretical reasons (7, 9, 13), were geographical (municipalities, capitals [Yes/No], the 26 Brazilian States and the Federal District Capital and the country’s five Regions [North, Northeast, South, Southeast, and Midwest]); the adequacy of the PHC facility services for vaccination actions (Yes/No) and adequate cold chain network (Yes/No). “Adequate facilities for vaccination actions” were defined as a PHC facility with adequate capacity specifically for this purpose. “Adequate cold chain network” was assumed when the PHC facility had a vaccination room exclusively for vaccination actions, exclusive refrigerators and thermal vaccine boxes for vaccines.
The analyses were performed using the Statistical Package for Social Sciences (SPSS) software, version 20.0. Initially, the geographical characteristics and those related to the facilities and functioning of the PHC services were analyzed, considering absolute and relative frequencies, according to the periods. Next, the frequency of “YF vaccine always available” was analyzed, for both periods, according to the independent variables, considering the 95% confidence intervals (CI) and Pearson’s chi-square test. Additionally, the frequency of “YF vaccine always available” in the municipalities were analyzed using Choropleth Thematic maps. The frequency was calculated considering the number of PHC facilities responding “Yes” to “YF vaccine always available” over the number of services studied multiplied by 100. Poisson regression models were used to analyze possible differences in the availability of the vaccine between the periods 2013-14 and 2017-18. In the complete model (model 2), using a multivariate Poisson regression with robust variances, the analyze was controlled by geographic variables and those related to the structure and functioning of the services, considering those with p-value <0.05 in Pearson’s chi-square. For these models, the prevalence ratios were estimated, with their respective 95%CI, using the Wald test. The level of statistical significance was set at 5% (p <0.05) for all analyzes.
Results
Data from 32,791 PHC facilities assessments, from both periods and distributed across country, was included in this study. The largest number of services evaluated was in the Northeast region and the smallest was in the Northern region. The states of Minas Gerais and Bahia had the largest number of facilities included, ranging from 13.9 to 15.2%. The facilities located in the state capitals represented just under 7% of the total. The vast majority had adequate physical capacities for vaccination actions and an adequate cold chain network (Table 1).
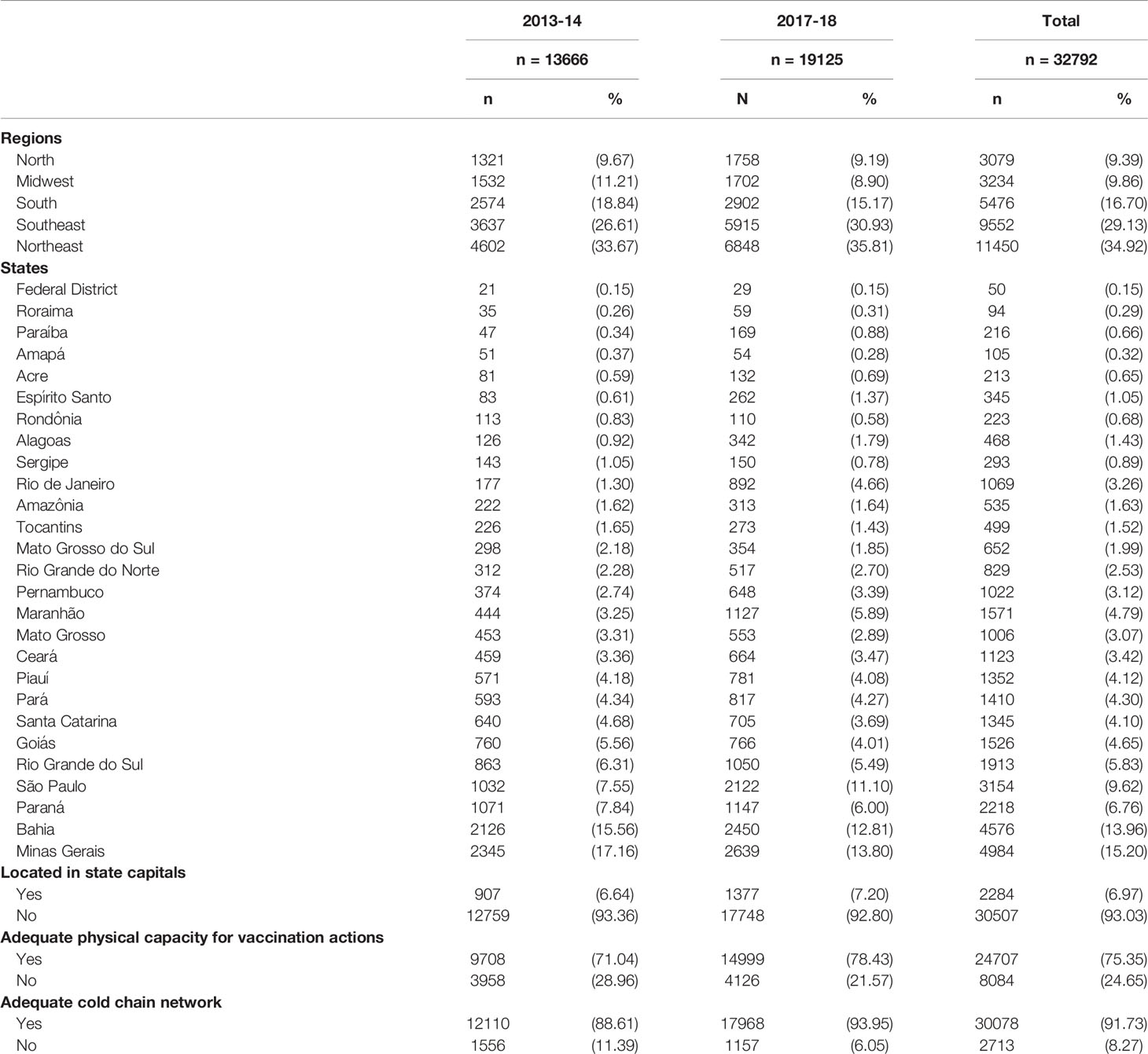
Table 1 Geographic and structural characteristics of the Primary Health Care facilities studied in 2013-14 and 2017-18, Brazil.
The overall frequency of PHC facilities with YF vaccine, always available, was 87.0% (CI 95%; 86.4-87.5) in 2013-14 and 89.7% (CI 95%; 89.2-90.1) in 2017-18. In both study periods, the services located in the Northeast region had the YF vaccine always available with less frequency when compared to those located in the other regions (p<0.001). Also, during both periods, services located in state capitals had YF vaccine always available with less frequency (p<0.001). A greater frequency of availability was identified at PHC facilities that possessed an adequate physical capacity and an adequate cold chain network for vaccination actions (Table 2).
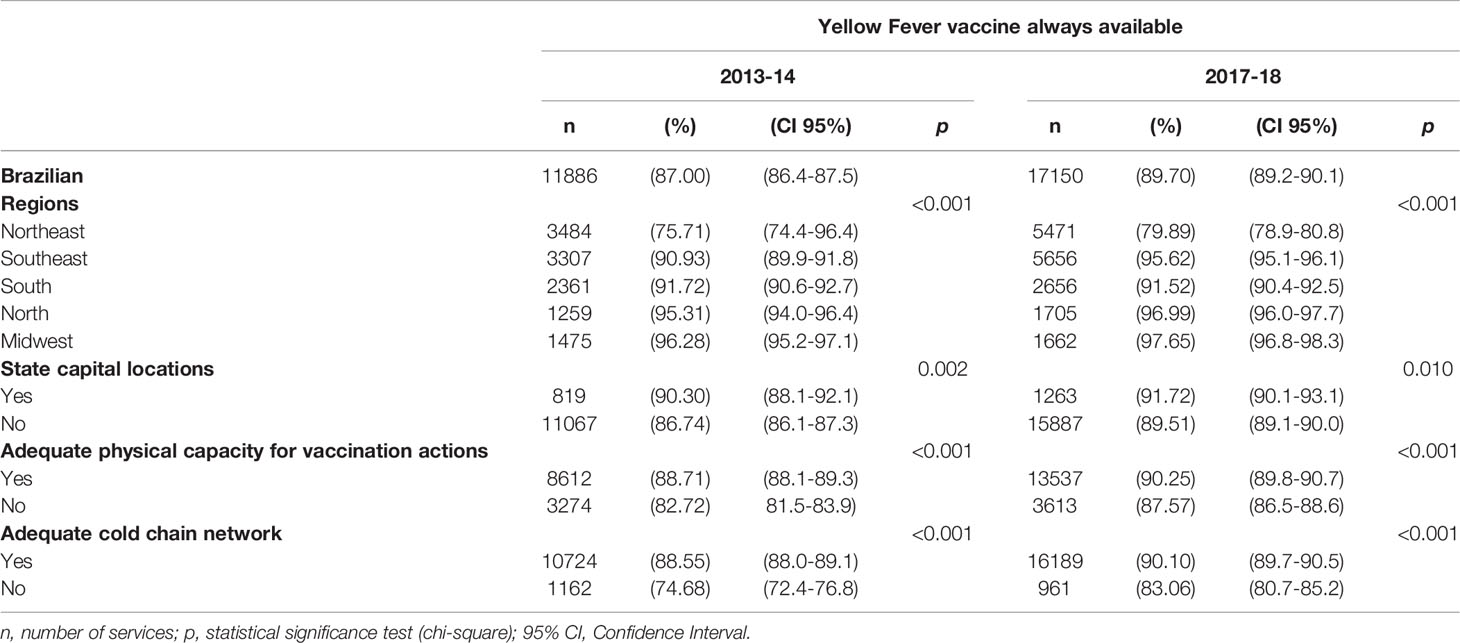
Table 2 Analysis of the of the availability of the Yellow Fever vaccine at Primary Health Care facilities in the second and third cycles of external evaluations of the Program for Improving Access and Quality in Primary Health Care, according to geographic and structural variables related to vaccine actions, Brazil, 2013-2014 (n = 13666) and 2017-2018 (n = 19125).
The frequency distribution of the available on demand YF vaccine always available at PHC facilities across the country, during both periods, is presented in Figure 1. The maps stand for the spatial differences for the availability of the YF vaccine. In 2017-18, there was a greater proportion of municipalities having dark tones when compared to 2013-14.
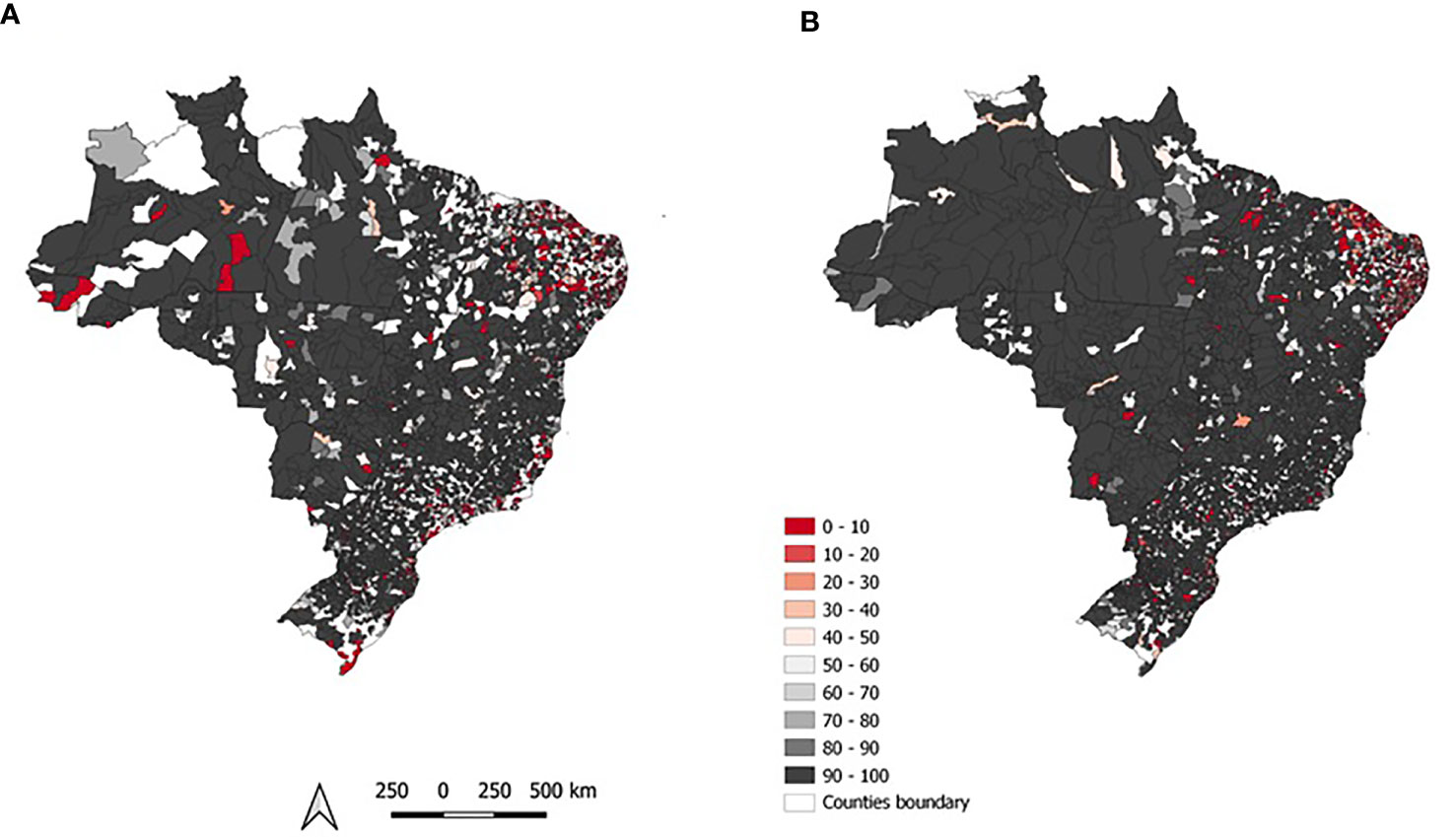
Figure 1 – Geographical distribution of the Yellow Fever vaccine (always available) at primary health care facilities located in Areas with Routine Vaccination Recommendations in Brazil between the periods 2013-14 (A) and 2017-18 (B).
Two different regression models were considered for the analysis of the availability of the YF vaccine (Table 3). The basic model (model 1) considered only the variable “period” (2017-18 and 2013-14). In the complete model (model 2) all independent variables were included in the analysis, including the variable “period”. Model 1 shows that, in the most recent period, PHC facilities had a greater frequency of YF vaccine always available (PR = 1.027; 95%CI: 1.020-1.035). After adjusting for all independent variables, in model 2, the prevalence ratio for the most recent period dropped from 1.027 to 1.025 but maintained statistical significance (p<0.001). Services located in the South, Southeast, Midwest and North regions and in non-state capitals, as well as services that had adequate facilities for vaccination actions, as well as an adequate cold chain network, demonstrated a greater prevalence of YF vaccine always available.

Table 3 Poisson regression analysis for the Yellow Fever vaccine (always available) at primary health care facilities located in Areas with Routine Vaccination Recommendations in Brazil between the periods 2013-14 and 2017-18.
Discussion
The proportion of PHC facilities located in the ARVR with YF vaccine always available increased from 2013-14 to 2017-18. With this result, we can assume that the number of vaccine doses were more sufficient for the population in the second studied period. Geographical aspects and an adequate cold chain network and an adequate capacity for facilities to engage in vaccination actions influenced YF vaccine availability.
In addition to geographic and structural factors, the increase in the availability of the YF vaccine may have been related to the emergence of an YF outbreak in Brazil, when the acquisition of YF vaccine by Brazilian Minister of Health was expanded (8, 14). The availability of the YF vaccine was greater in non-capital cities, reinforcing that the distribution of this vaccine to the PHC facilities did not occur equally (11).
As reported by other studies, cold chain networks that fail to guarantee safe and uninterrupted conservation and maintenance of immunobiologicals, compromise logistical and operational sustainability of immunization services, resulting in reductions in vaccine stocks (15–17). The lack of inputs and equipment essential for the conservation of immunobiologicals, such as coolers and refrigerators, imposes the first barrier to the availability of the YF vaccine, with risks at compromising vaccination coverage and the formation of grouping of individuals susceptible to the virus (6, 7, 18–21). When infrastructure of the services is inadequate, and large dose losses occur, the population’s access to vaccines can be greatly compromised (22, 23).
It should be noted, considering the samples of facilities studied, that the number of PHC facilities in the ARVR increased between the studied periods, reflecting the decision for expansion by the National Immunization Program. However, the frequency of availability of the YF vaccine at PHC facilities increased relatively less than the number of services in the ARVR between the two study periods.
In examining the findings of this study, we conclude that, in addition to expansion of ARVR, it is essential to expand the availability of the YF vaccine in PHC facilities. From a public health standpoint, our findings suggest that the effective supply chain networks for YF vaccine, combined with the adequate capacity of PHC facilities and services, are essential to ensuring their availability in order to achieve universal access to immunoprevention and to improve vaccine coverage indicators.
In view of the last outbreak of YF in Brazil, and the results of our findings, consideration should be directed at the factors related to the physical capacity of PHC facilities and services throughout Brazil targeting actions aimed at maintaining optimal vaccination coverage against the disease. Furthermore, the same factors that are related to YF vaccine availability may also be implicated in the risk of resurgence of other preventable diseases in the country. Studies that consider factors possibly related to vaccine availability at the central levels of distribution and logistics networks are recommended.
As this was a nationwide study, it was possible to assess and compare the availability of YF vaccine at PHC facilities from the five regions of Brazil. However, this study had some intrinsic limitations, including the impossibility of proving causal inferences, since the data were collected over a single moment. Another limitation was related to the lack of evaluation of PHC facilities along remote riverbeds in the Amazon rainforest region.
In 2020, the National Immunization Program in Brazil expanded the recommendation of vaccination against YF to the entire national territory. This expansion occurred in response to a growing number of cases of the disease, which alerted to the reemergence of urban YF in the country. In this sense, structural problems, probably related to regional differences in investments in the health sector, need to be the focus of public policy decision makers.
Data Availability Statement
Publicly available datasets were analyzed in this study. This data can be found here: https://aps.saude.gov.br/ape/pmaq/ciclo3/.
Author Contributions
EV, conceived and designed the analysis, collected the data, wrote the paper, performed the analysis, analysis and interpretation of data, and drafting of manuscript. MH and TDS, contributed data or analysis tools, wrote the paper, analysis and interpretation of data, and drafting of manuscript. SL, FM, and MB, wrote the paper, analysis and interpretation of data, and drafting of manuscript.
Funding
Progrma de Pós Graduação em Enfermagem da Escola de Enfermagem da UFMG
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Adrien N, Hyde TB, Gacic-Dobo M, Hombach J, Krishnaswamy A, Lambach P. Differences Between Coverage of Yellow Fever Vaccine and the First Dose of Measles-Containing Vaccine: A Desk Review of Global Data Sources. Vaccine (2019) 37(32):4511–7. doi: 10.1016/j.vaccine.2019.06.063
2. Baba MM, Ikusemoran M. Is the Absence or Intermittent YF Vaccination the Major Contributor to its Persistent Outbreaks in Eastern Africa? Biochem Biophys Res Commun (2017) 492(4):548–57. doi: 10.1016/j.bbrc.2017.01.079
3. Kraemer MUG, Faria NR, Reiner RC, Golding N, Nikolay B, Stasse S, et al. Spread of Yellow Fever Virus Outbreak in Angola and the Democratic Republic of the Congo 2015-16: A Modelling Study. Lancet Infect Dis (2017) 17(3):330–8. doi: 10.1016/S1473-3099(16)30513-8
4. Zhao S, Stone L, Gao D, He D. Modelling the Large-Scale Yellow Fever Outbreak in Luanda, Angola, and the Impact of Vaccination. PLoS Negl Trop Dis (2018) 12(1):e0006158. doi: 10.1371/journal.pntd.0006158
5. Barrett ADT. Yellow Fever in Angola and Beyond — The Problem of Vaccine Supply and Demand. N Engl J Med [Internet] (2016) 375(4):301–3. doi: 10.1056/NEJMp1606997
6. Gomes Araújo MC, Ferreira da Silva L, Stanford Baldoino L, Rodrigues dos Santos Porto TN, De Sousa Martins V, Pereira Carvalho D, et al. Fatores Que Interferem No Cumprimento do Calendário Vacinal Na Infância. Rev Eletrônica Acervo Saúde (2020) 42):e2874. doi: 10.25248/reas.e2874.2020
7. Silva F de S, Barbosa YC, Batalha MA, Ribeiro MRC, Simões VMF, Branco M dos RFC, et al. Incompletude Vacinal Infantil De Vacinas Novas E Antigas E Fatores Associados: Coorte De Nascimento BRISA, São Luís, Maranhão, Nordeste do Brasil. Cad Saude Publica (2018) 34(3):e00041717. doi: 10.1590/0102-311x00041717
8. Brasil. Monitoramento do Período Sazonal Da Febre Amarela - Brasil 2017/2018. In: Inf Epidemiológico. Ministério da Saúde Brasil (2019) p. 1–12. Available at: https://saude.campinas.sp.gov.br/doencas/febre_amarela/2018/Informe_MS_15_F_Amarela_monitoramento.pdf
9. Hirsh Bar Gai D, Graybill Z, Voevodsky P, Shittu E. Evaluating Scenarios of Locations and Capacities for Vaccine Storage in Nigeria. Vaccine [Internet] (2018) 36(24):3505–12. doi: 10.1016/j.vaccine.2018.04.072
10. de Noronha TG, Camacho LAB. Controversies in the Expansion of Areas With Routine Yellow Fever Vaccination in Brazil. Cad Saude Publica [Internet] (2017) 33(10):e00060917. doi: 10.1590/0102-311x00060917
11. Cavalcante KRLJ, Tauil PL. Risco De Reintrodução Da Febre Amarela Urbana No Brasil. Epidemiol E Serv Saude Rev Do Sist Unico Saude Do Bras (2017) 26(3):617–20. doi: 10.5123/S1679-49742017000300018
12. Brasil. Programa de Melhoria do Acesso e da Qualidade. Manual Instrutivo Para as Equipes De Atenção Básica E Nasf. Vol. 1, BRASIL, Ministério Da Saúde.Secretaria De Vigilância Em Saúde. In: Coordenação-Geral De Desenvolvimento Da Epidemiologia Em Serviços, vol. 89. Brasília (2017). Avaliable at: https://bvsms.saude.gov.br/bvs/publicacoes/manual_instrutivo_pmaq_atencao_basica.pdf
13. Barrett ADT. Yellow Fever Live Attenuated Vaccine: A Very Successful Live Attenuated Vaccine But Still We Have Problems Controlling the Disease. Vaccine Elsevier Ltd; (2017) 35:5951–5. doi: 10.1016/j.vaccine.2017.03.032
14. Brasil. Monitoramento do Perı́odo Sazonal Da Febre Amarela - 2017/2018. In: Inf Epidemiológico. Ministério da Saúde vol. 2019. p. 1–12. Available at: https://saude.campinas.sp.gov.br/doencas/febre_amarela/2018/Informe_MS_15_F_Amarela_monitoramento.pdf
15. Aina M, Igbokwe U, Jegede L, Fagge R, Thompson A, Mahmoud N. Preliminary Results From Direct-to-Facility Vaccine Deliveries in Kano, Nigeria. Vaccine (2017) 35(17):2175–82. doi: 10.1016/j.vaccine.2016.11.100
16. Ngcobo NJ, Kamupira MG. The Status of Vaccine Availability and Associated Factors in Tshwane Government Clinics. S Afr Med J (2017) 107(6):535–8. doi: 10.7196/SAMJ.2017.v107i6.12149
17. Songane M. Challenges for Nationwide Vaccine Delivery in African Countries. Int J Heal Econ Manage (2018) 18(2):197–219. doi: 10.1007/s10754-017-9229-5
18. Barros MGM, Santos MC da S, Bertolini RPT, Pontes Netto VB, Andrade MS. Perda De Oportunidade De Vacinação: Aspectos Relacionados À Atuação Da Atenção Primária Em Recife, Pernambuco, 2012. Epidemiol E Serviços Saúde (2015) 24(4):701–10. doi: 10.5123/S1679-49742015000400012
19. Belda K, Tegegne AA, Mersha AM, Bayenessagne MG, Hussein I, Braka F, et al. Supplement Article Measles Outbreak Investigation in Guji Zone of Oromia. Pan Afr Med J (2017) 27(Supp 2):1–5. doi: 10.11604/pamj.supp.2017.27.2.10705
20. Lemos DRQ, Franco AR, de Sa Roriz MLF, Carneiro AKB, de Oliveira Garcia MH, de Souza FL, et al. Measles Epidemic in Brazil in the Post-Elimination Period: Coordinated Response and Containment Strategies. Vaccine (2017) 35(13):1721–8. doi: 10.1016/j.vaccine.2017.02.023
21. Vieira EW, Pimenta AM, Montenegro LC, da Silva TMR. Estrutura E Localização Dos Serviços De Vacinação Influenciam a Disponibilidade Da Tríplice Viral No Brasil. REME Rev Min Enferm (2020) 24:e1325–5. doi: 10.5935/1415-2762.20200062
22. Oyekale AS. Assessment of Primary Health Care Facilities’ Service Readiness in Nigeria. BMC Health Serv Res (2017) 17(1):172. doi: 10.1186/s12913-017-2112-8
Keywords: vaccines, yellow fever vaccine, yellow fever, primary health care, cross-sectional study, health services accessibility
Citation: Hermsdorf MO, da Silva TMR, Lachtim SAF, Matozinhos FP, Beinner MA and Vieira EWR (2022) Availability of the Yellow Fever Vaccine in Primary Health Care Services in Brazil. Front. Trop. Dis 3:866554. doi: 10.3389/fitd.2022.866554
Received: 31 January 2022; Accepted: 12 April 2022;
Published: 06 June 2022.
Edited by:
Malcolm Scott Duthie, HDT Biotech Corporation, United StatesReviewed by:
Wildo Navegantes Araujo, University of Brasilia, BrazilJaime Torres, Central University of Venezuela, Venezuela
Copyright © 2022 Hermsdorf, da Silva, Lachtim, Matozinhos, Beinner and Vieira. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ed Wilson Rodrigues Vieira, ZWR3aWxzb252aWVpcmFAdWZtZy5icg==