 Xiaoyan Yin1*
Xiaoyan Yin1* Eliézer K. N’Goran2Mamadou Ouattara2NAD. Aka2
Eliézer K. N’Goran2Mamadou Ouattara2NAD. Aka2 Nana R. Diakité2Fidèle K. Bassa2
Nana R. Diakité2Fidèle K. Bassa2 Elly Kourany-Lefoll3Aliona Tappert4
Elly Kourany-Lefoll3Aliona Tappert4 Özkan Yalkinoglu4Eric Huber5,6Deon Bezuidenhout7
Özkan Yalkinoglu4Eric Huber5,6Deon Bezuidenhout7 Wilhelmina M. Bagchus8
Wilhelmina M. Bagchus8 Brooke Hayward1 on behalf of
Brooke Hayward1 on behalf of - 1Global Biostatistics, EMD Serono Research & Development Institute, Inc., Billerica, MA, United States, an Affiliate of Merck KGaA, Darmstadt, Germany
- 2Université Félix Houphouët-Boigny, Abidjan, Côte D’Ivoire
- 3Ares Trading S.A., Eysins, Switzerland, an Affiliate of Merck KGaA, Darmstadt, Germany
- 4Translational Medicine, Clinical Pharmacology, Merck KGaA, Darmstadt, Germany
- 5Department of Medicine, Swiss Tropical and Public Health Institute, Basel, Switzerland
- 6University of Basel, Basel, Switzerland
- 7Clinical Delivery Unit, Clinical Trial Execution, Merck (Pty) Ltd., Modderfontein, South Africa, an Affiliate of Merck KGaA, Darmstadt, Germany
- 8Translational Medicine, Merck Institute of Pharmacometrics, Lausanne, Switzerland, an Affiliate of Merck KGaA, Darmstadt, Germany
Introduction: Traditionally Schistosoma mansoni infection is diagnosed by the Kato-Katz method. Thick smears from each stool sample are prepared on slides and eggs are counted microscopically. Commercially available point-of-care circulating cathodic antigen (POC-CCA) cassette tests detect schistosomiasis antigens from urine samples in 20 minutes. POC-CCA results are qualitative or semi-quantitative: signal intensity is an indicator of the amount of worm antigens in the sample. Both methods were used in a phase II trial investigating the efficacy and safety of new pediatric formulations of praziquantel (PZQ) among children ≤6 years (NCT02806232). This secondary analysis evaluated the consistency of results between the Kato-Katz and POC-CCA methods.
Methods: POC-CCA was used to pre-screen for S. mansoni infection. Children with positive results were tested by the Kato-Katz method, and those with positive Kato-Katz results (>1 egg/1 occurrence) were enrolled. Participants (N=444) were treated with different formulations and doses of PZQ. POC-CCA and Kato-Katz were performed at 2–3 weeks after treatment to evaluate drug efficacy. Cure rate (CR) was defined as the proportion of participants with a negative result per POC-CCA, or no eggs in the stool samples per Kato-Katz. Kappa statistic was used to assess the agreement on cure status, and Spearman correlation between POC-CCA positivity and Kato-Katz egg counts was evaluated. Sensitivity and specificity of POC-CCA were calculated using Kato-Katz as a reference standard.
Results: CR per POC-CCA, measured 2–3 weeks after treatment, was 52% [95% confidence interval (CI): 48%, 57%] across all treatment arms except in infants aged 3–12 months. CR per Kato-Katz was 83% (95% CI: 79%, 87%). Kappa statistic was 0.16 (95% CI: 0.09, 0.23), indicating that the agreement was slightly better than by chance. Relative to Kato-Katz, POC-CCA’s sensitivity to detect infection was 70% and specificity was 57%. Spearman correlation coefficient between POC-CCA positivity and Kato-Katz egg counts was 0.26 (95% CI: 0.17, 0.34).
Conclusion: POC-CCA is sensitive and rapid for diagnosing S. mansoni infection, but its performance and consistency with Kato-Katz requires further investigation among young children.
Introduction
Schistosomiasis is a neglected tropical disease affecting communities with limited access to safe water and adequate sanitation provision (1–3). The disease is caused by a parasitic worm of the genus Schistosoma, of which there are five species responsible for the major forms of disease (intestinal and urogenital schistosomiasis). The parasite infests water sources and transmission to humans occurs through the skin following routine contact with unsafe, infested water (3). It has been widely recognized that both pre-school-age and school-age children are at significant risk of schistosomiasis with at least 25 million infected, often with serious consequences to health (4, 5). The health impact includes anemia as well as poor growth, nutrition, and cognition in affected children (5). Recent studies suggest that, in highly endemic areas, children under 6 years of age, including infants, can carry a medium to heavy infection burden and that infection burden increases with age (6–8). The World Health Organization (WHO)-recommended treatment for schistosomiasis is praziquantel (PZQ) at a single oral dose of 40mg/kg body weight. This agent is effective in killing adult worms and indirectly triggers an immune response as the contents of the worms are released (1).
Traditionally Schistosoma mansoni infection is diagnosed by the Kato-Katz method according to WHO recommendations: two stool samples are collected from a person over 3 to 5 days and four Kato-Katz thick smears in total are read microscopically for egg counts (9, 10). However, the Kato-Katz test is not sufficiently sensitive to diagnose low egg counts, and therefore may over-estimate drug efficacy in clinical trials, especially in children with low infection intensity (11).
The Point-of-care circulating cathodic antigen (POC-CCA) cassette test, a commercially available tool, detects Schistosoma circulating antigens from adult worms that are ultimately secreted into urine. Test results can be observed on strips in about 20 minutes. The commercial provider claims that the kit can differentiate active from non-active infection (https://www.rapid-diagnostics.com/). POC-CCA positivity in urine samples may therefore be a more appropriate diagnostic tool in very young individuals who often have a low worm burden (12–14). Indeed, several studies have indicated that the POC-CCA test is a promising method for the diagnosis of intestinal schistosomiasis in pre-school-age and school-age children given its sensitivity, promptness of results and convenience (15–17).
POC-CCA and Kato-Katz have been compared in several surveillance studies, with POC-CCA consistently showing higher sensitivity. In a surveillance program in Tanzania among 404 children aged 9 to 12 years, 66.1% vs 28.7% of participants were positive for S. mansoni by POC-CCA and Kato-Katz, respectively (18). Similar results were observed in a prevalence study in Chad, although the prevalence was much lower: 6.9% by POC-CCA vs only 0.5% by the Kato-Katz method (19). Another study assessing the rate of S. mansoni infection in 979 HIV-positive adults in Tanzania reported positivity rates of 60.5% vs 47.3% by POC-CCA and Kato-Katz, respectively (20). Finally, a large study with more than 4000 children from areas endemic for schistosomiasis across five countries showed an overall prevalence of 55.2% by a single POC-CCA assay vs 38.8% by three Kato-Katz smears. The trend was similar in each individual country apart from Côte d’Ivoire, where the prevalence was 45.5% by a single POC-CCA assay vs 57.7% by three Kato-Katz smears (21).
Both Kato-Katz and POC-CCA methods were used in a phase II clinical trial investigating the efficacy and safety of new oral disintegrating tablet (ODT) formulations of PZQ among children aged ≤6 years in a single center in Côte d’Ivoire (NCT02806232) (ClinicalTrials.gov 22, 23). The trial assessed a racemate (rac-PZQ) formulation containing a mixture of R- (–)-Praziquantel (levo-PZQ or L-PZQ) and S-(+)-Praziquantel (dextro-PZQ or D-PZQ) in a 1:1 ratio, and the other one containing only L-PZQ, which is devoid of the biologically inactive D-PZQ enantiomer. It was concluded that both novel formulations were highly efficacious in pre-school-age children and L-PZQ ODT was efficacious in infants aged ≤2 years; no new safety concerns were identified (23).
Here, we present the results of the secondary analysis of this phase II clinical trial, evaluating the sensitivity and specificity of the POC-CCA assay and its concordance with the Kato-Katz method used to determine infection status at baseline before any treatment and over time after treatment.
Methods
Full details of the conduct of the phase II trial (NCT02806232) are reported in the primary analysis (23). In brief, it was a two-part, open-label, dose-finding study of the efficacy and safety of PZQ formulations in children and infants infected with S. mansoni in Côte d’Ivoire. In Part 1, children aged 2–6 years were randomized to receive commercially available rac-PZQ at 3x20 mg/kg (treatment arm 1, n=60) or 40 mg/kg (treatment arm 2, n=60); rac-PZQ ODT at 40 mg/kg (treatment arm 3, n=60) or 60 mg/kg (treatment arm 4, n=60); or L-PZQ ODT at 30 mg/kg (treatment arm 5, n=60), 45 mg/kg (treatment arm 6, n=60) or 60 mg/kg (treatment arm 7, n=60). The formulation and dose identified as optimal in terms of safety and efficacy in Part 1, i.e. 50 mg/kg L-PZQ ODT, was used in Part 2 for infants aged 13–24 months (treatment arm 8, n=20) and 3–12 months (treatment arm 9, n=4). The primary endpoint of the phase II trial was cure rate (CR) based on egg counts measured using the Kato-Katz method. POC-CCA urine cassette test was used as a pre-screening tool and as a secondary endpoint for CR at follow-up. No statistical comparison was planned between different treatments/formulations of PZQ. Rather, as accepted by the European Medicines Agency, the sample size for each treatment arm in Part 1 was determined to provide reasonable precision for the estimated CR.
The outcome of the POC-CCA test used in this trial was qualitative with four visual levels: negative, positive (+), positive (++), or positive (+++) (in positive results, more plusses were assigned to higher signal intensity and were used to indicate higher amounts of antigens in the sample). Details for this product can be found on the manufacturer’s website: https://www.rapid-diagnostics.com/products.html. A semi-quantitative scoring system using a portable reader has since been developed and is gaining popularity. The device grades the test result in terms of a score (G-score) ranging from 1 to 10, with higher values indicating heavier infection (24). In our trial, we used the 4-level visual scores because the G-score system was not available when the clinical trial protocol was developed in 2017.
We defined the day when the treatment was administered as Day 1, and last measurement prior to study treatment was defined as baseline. Children from villages in endemic area were pre-screened (Day -28 to -1) for S. mansoni by POC-CCA, followed by Kato-Katz method, and for S. haematobium by the urine filtration method. Participants were included if they had positive results for both POC-CCA and Kato-Katz and a negative result for S. haematobium (i.e. participants with mixed infection were excluded).
Kato-Katz was performed at baseline and 2–3 weeks after treatment follow-up (Day 14–21; Figure 1). At each time point, two stool samples were collected from each participant on different days within a maximum of 5 days. Three Kato-Katz thick smears (41.7 mg) were prepared from each stool sample (for a total of six smears), and read under a microscope following the WHO Kato-Katz manual (25). Baseline infection intensity was defined as either light (1–99 eggs/gram) or moderate/heavy (≥100 eggs/gram). The participant was defined to be cured if egg count at the follow-up visit was 0.
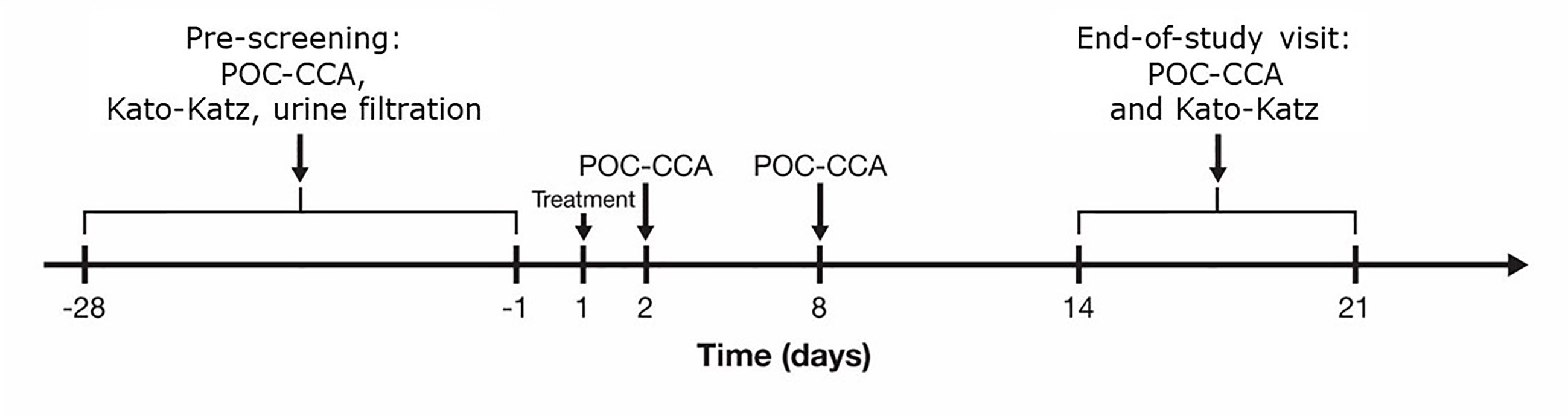
Figure 1 Schedule of diagnostic assessments of infection burden. POC-CCA, point-of-care circulating cathodic antigen.
Urine samples for POC-CCA testing were collected at follow-up visits to understand how worm burden changes over time after treatment, and to evaluate the sensitivity and specificity of POC-CCA as compared with Kato-Katz (Figure 1). Trace results were recorded as positive + infections for treatment arms 1 to 7; however, traces were considered negative when pre-screening for participants 3 months to 2 years old (arms 8 and 9) after observing that the majority of traces have negative results for Kato-Katz in this age group.
POC-CCA results were summarized by visits, age group and infection intensity at baseline. The analysis included the modified intent-to-treat population (mITT), defined as all participants who had baseline disease and did not use antimalarial medication during the study period (23). CR was defined as the proportion of participants with a negative result per POC-CCA or no eggs in stool sample per Kato-Katz at Day 14–21 of follow-up. Kappa statistic was calculated to assess the agreement on cure status between the two methods, overall and by infection intensity at baseline.
Spearman correlation between POC-CCA positivity and egg counts by Kato-Katz method at Day 14–21 of follow-up was also calculated. Sensitivity and specificity of POC-CCA were evaluated using Kato-Katz as the reference standard, though with reservations that the latter might not be perfectly sensitive especially among young children. These statistics were evaluated for the overall mITT population and each of the baseline infection intensity subgroups.
The trial was conducted in compliance with Good Clinical Practice and the Declaration of Helsinki. Written informed consent was obtained from one of the participant’s parents, legal representatives, or guardians prior to any trial-related procedure. In addition, oral assent was recorded for children aged >3 years, if they were capable of doing so. The trial protocol and associated documents were approved by the Independent Ethics Committees/Institutional Review Boards in Switzerland and in Côte d’Ivoire.
Results
A total of 7906 subjects were pre-screened using the S. mansoni POC-CCA test; 710 children tested positive for S. mansoni by POC-CCA and Kato-Katz method, and negative for S. haematobium by the urine filtration method. Of these, N=444 met the inclusion/exclusion criteria and were enrolled and treated (23). The mITT population consisted of n=421 participants including n=10 participants who did not have POC-CCA results from the Day 14–21 follow-up visit and were imputed using last observation carried forward (LOCF) approach. Baseline characteristics have been published elsewhere (23). Briefly, all participants were Black, aged 0.5 to 6.9 years, 46% were female, and 62% had light infection.
In general, POC-CCA results showed a trend towards negativity over time. This trend was observed in all treatment arms, except treatment arm 9 which was composed of four infants <1 year of age. In most treatment arms, immediately on the day after treatment some participants become negative (~10%) or went from positive (+++) to positive (++) or positive (+) (Figure 2). By Day 8, about 40% of participants became negative by POC-CCA; by Day 14–21, over 50% became negative by POC-CCA. The trend over time was similar among the children with light infection at baseline (n=259) and those with moderate/heavy infection (n=162), but it is noticeable that at each visit there were more negative POC-CCA results for the light infection subgroup than for the moderate/heavy infection subgroup. For example, at the last follow-up visit the negative rates were 61.8% and 37.7% for light vs moderate/heavy infection, respectively.
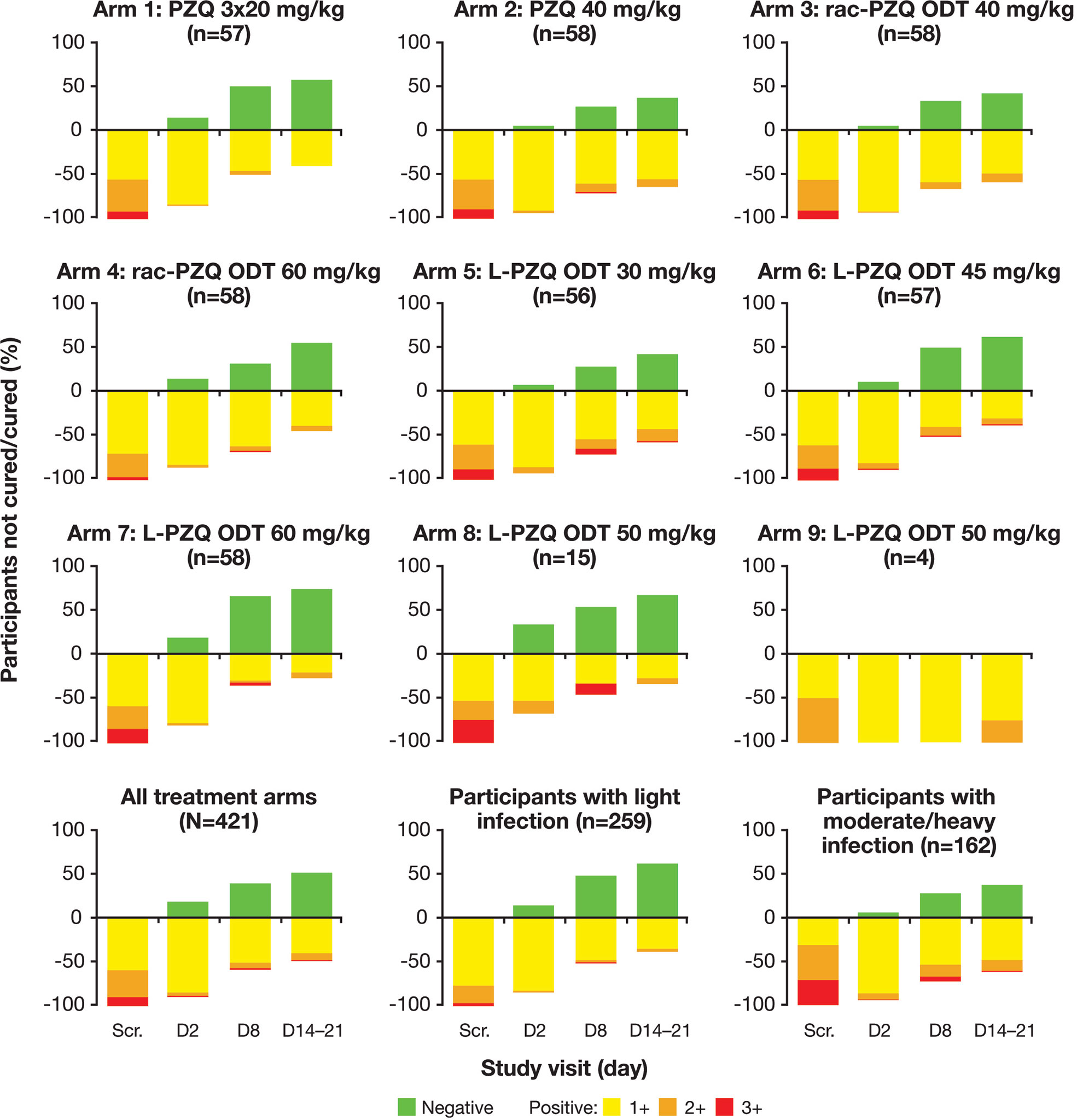
Figure 2 POC-CCA results over time by treatment arm and by infection intensity. Participants’ age: Treatment arms 1–7 (2–6 years); Treatment arm 8 (13–24 months); Treatment arm 9 (3–12 months). D, day; ODT, oral disintegrating tablet; POC-CCA, point-of-care circulating cathodic antigen; PZQ, praziquantel; rac, racemate; Scr., screening.
The CR at the last follow-up visit (Day 14–21) per POC-CCA, ranging from 0% to 66.7%, was substantially lower than the CR based on Kato-Katz method in every treatment arm, ranging from 74.1% to 100% (Table 1, Figure 2). These results indicate that POC-CCA may be more sensitive in detecting the disease. No statistical comparison was performed, but the CRs per Kato-Katz were similar across different treatment arms. In contrast, the CR per POC-CCA varied across treatment arms: none of the four infants aged <1 year (treatment arm 9) became negative by POC-CCA on Day 14–21, but all of them were egg-free by the Kato-Katz method (Table 1, Figure 3). On the other hand, out of 15 participants aged 13–24 months, 10 became negative by POC-CCA, which is close to the treatment arms treated with ≥45 mg/kg L-PZQ ODT.
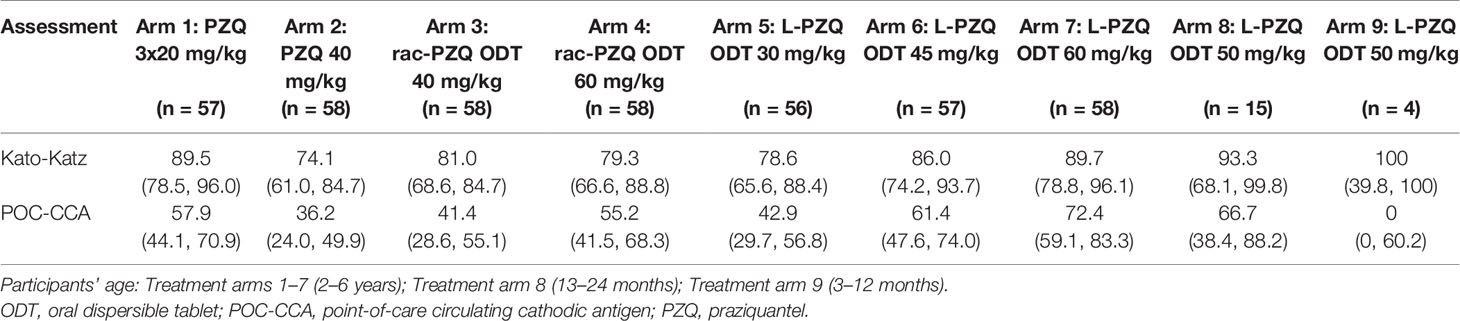
Table 1 Day 14–21 follow-up cure rates [% (95% confidence interval)] per Kato-Katz and POC-CCA.
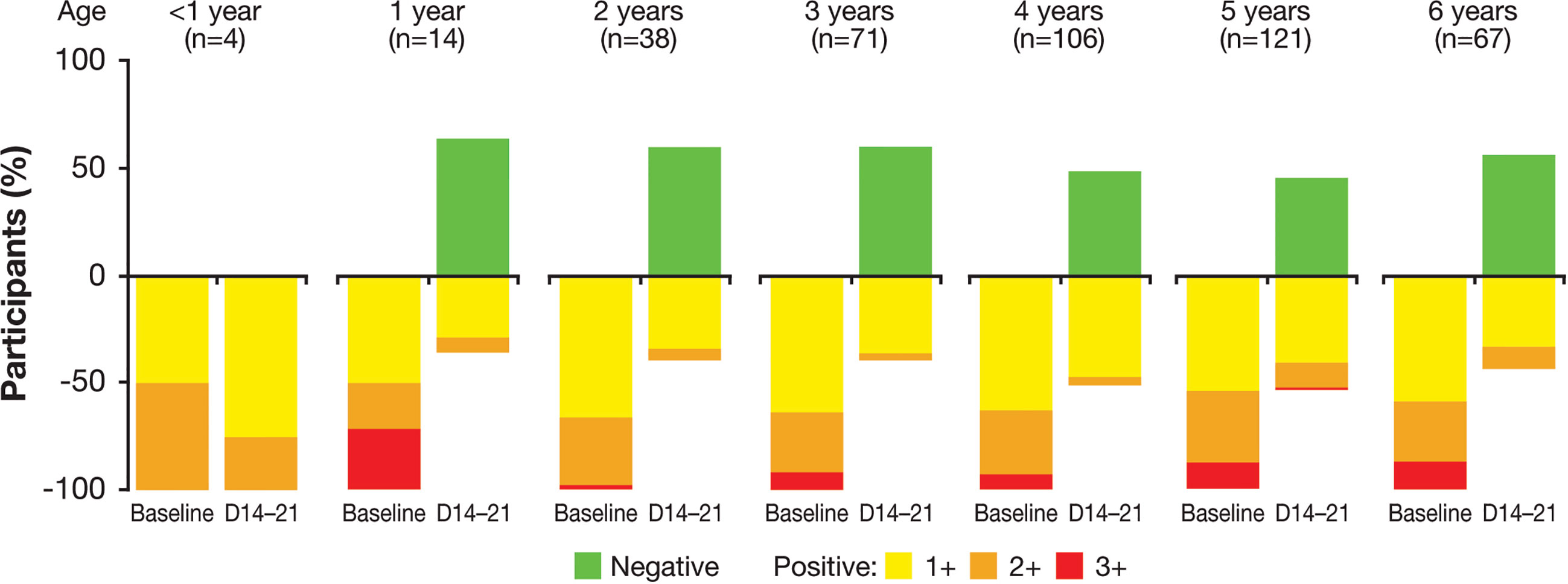
Figure 3 POC-CCA results by age group, from baseline to 2–3 weeks after treatment. D, day; POC-CCA, point-of-care circulating cathodic antigen.
In the analysis of agreement between POC-CCA and Kato-Katz assessment at Day 14–21of follow-up, the Kappa coefficient was 0.16 (95% CI: 0.09, 0.23), suggesting that the agreement was only slightly better than what would be expected by chance (Table 2) (26). The agreement between POC-CCA and Kato-Katz was better in those with moderate/heavy infection than in those with light infection at baseline: Kappa coefficients were 0.23 (95% CI: 0.12, 0.33) and 0.04 (95% CI: -0.05, 0.14), respectively. Relative to Kato-Katz, sensitivity of POC-CCA to detect infection was 70% and specificity for cure was 57%. The most frequent discordant situation was POC-CCA-positive but “cured” per Kato-Katz (150 out of 421, 36%). In contrast, only 21 (5%) had negative POC-CCA but visible eggs in Kato-Katz. Among children with moderate/heavy infection at baseline, the sensitivity and specificity at Day 14–21 were 86% and 46%; among those with light infection at baseline, the sensitivity and specificity at Day 14–21 were 46% and 63%. The Spearman correlation coefficients between POC-CCA positivity and Kato-Katz egg counts were 0.52 (95% CI: 0.45, 0.59) for the overall mITT population, 0.50 (95% CI:0.37, 0.60) for moderate/heavy infection, and 0.17 (95% CI: 0.05, 0.29) for light infection at baseline. The overall Spearman correlation was 0.26 (95% CI: 0.17, 0.34) at Day 14–21 of follow-up.
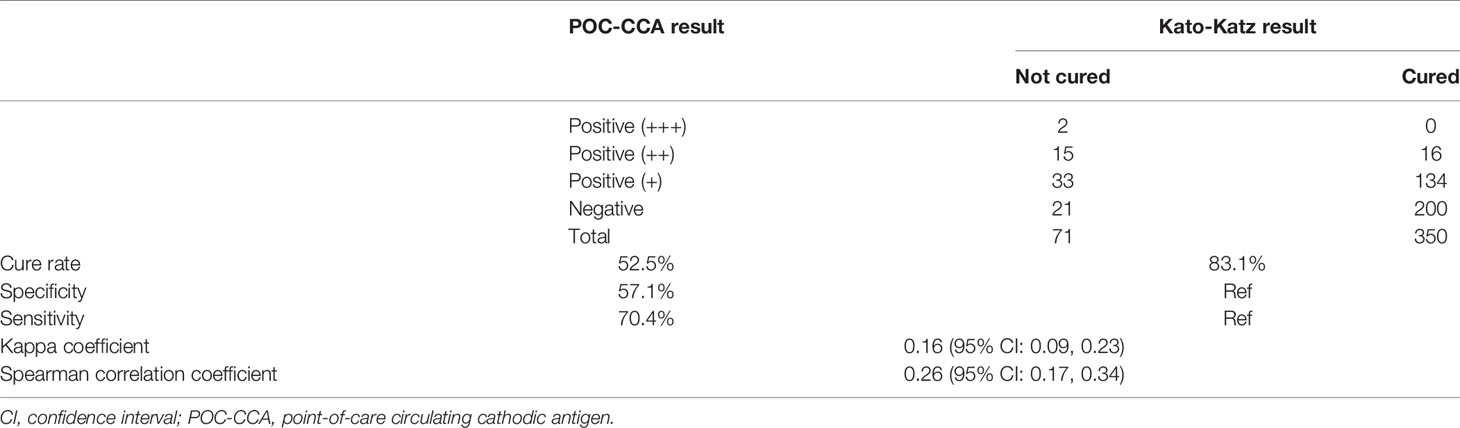
Table 2 Sensitivity and specificity of POC-CCA, using Kato-Katz as standard, at 2–3 weeks after treatment.
Discussion
Both Kato-Katz and POC-CCA methods have advantages and limitations. While POC-CCA may be particularly suitable for infection monitoring, Kato-Katz provides an egg count that allows for calculation of the egg reduction rate and is a widely used measure of treatment efficacy.
Current consensus is that POC-CCA is more sensitive than the Kato-Katz method in diagnosing S. mansoni infection, and a number of large studies recommend POC-CCA as an easy, rapid test with high sensitivity (12, 15, 16). The sensitivity of Kato-Katz varies with the number of stool samples and the number of thick smears per stool sample that are examined under the microscope. A recently published model of fecal egg-count data estimated the difference in sensitivity of the Kato-Katz method to be about 30% depending on whether 1 or 2 samples per patient were used for quantification (sensitivity was 50% and 80%, respectively). These results were applicable to patients with moderate infection (100–399 eggs/gram stool) (27). Another study showed that the proportion of positive samples analyzed by the Kato-Katz method increased from 11% to 19% for 4 vs 24 smears, respectively (28).
There are other diagnosis methods for S. mansoni, such as the Point-of-care circulating anodic antigen (POC-CAA) test and molecular approaches including PCR, real-time PCR, TaqMan® fecal assays, SmMITLAMP (a LAMP-based method to detect S. mansoni DNA), etc. No conclusive results were obtained in various comparison studies (29–33), hence no consensus on a gold standard for the diagnosis of S. mansoni has been reached. One of the limitations of current molecular approaches is that they are based on the DNA of parasite eggs present in the stool. Detection is therefore linked to a minimum threshold and is subject to variations over time. Unlike egg DNA-based assays, POC-CAA and POC-CCA detect the presence of the parasite even in the absence of eggs (e.g. isolated males). In our trial, the diagnostic methods to measure disease control and cure in pre-school-age children were chosen based on previous experience in other age groups and programs, i.e. the Kato-Katz method and POC-CCA as a promising alternative method. The POC-CAA testing kit was not commercially available when the trial protocol was developed.
Due to the lack of a gold standard, the sensitivity and specificity of the POC-CCA assay were assessed in our trial relative to the Kato-Katz method (six smears from two samples), but with reservations. Barenbold et al. used a model with a latent variable to estimate the sensitivity and specificity of POC-CCA, avoiding the use of a gold standard; in their study, POC-CCA was characterized by high sensitivity (>95% for moderate/heavy infection and >75% for light infection) and >95% specificity across the infection spectrum (34). In another study in a low endemic area, when the reference standard was established using 16 Kato-Katz slides from three samples (12 from the first fecal sample, two from the second and two from the third), the comparison with POC-CCA revealed a sensitivity of 65.7%, a specificity of 80.4%, and Kappa coefficient of 0.27 (slightly higher than that observed in our trial) (35). Based on these results, the specificity of POC-CCA remains to be determined. There are also concerns about the lack of consistency with results obtained using the Kato-Katz method which remains the WHO-recommended method of diagnosis (9, 10).
Furthermore, possible reasons of simultaneous negative Kato-Katz and positive POC-CCA results have been summarized previously including infection with single-sex worms, infection with infertile female worms, host’s anti-fecundity immunity (17), and cross-reactivity of POC-CCA in pregnant women (19). Absolute false POC-CCA is possible but was deemed relatively rare: a study of 100 children performed in a non-endemic area in Ethiopia showed that only one POC-CCA test (1%) had a trace positive result, while none of the children was identified to have any eggs per Kato-Katz (21). POC-CCA can also detect moderate/heavy S. haematobium infection (https://www.rapid-diagnostics.com/); however, it is highly unlikely that urogenital infection was the cause of false positive results in this trial, as participants with S. haematobium infection were excluded at screening. Although the possibility of a new urogenital infection between screening and post-treatment follow-up could not be excluded, the study period of 3–5 weeks was too short to allow for worm maturation to result in moderate/heavy infection.
The consistency between POC-CCA and Kato-Katz was modest in the clinical trial presented here. At the end of the trial, overall CRs were 74.1–100% with Kato-Katz and 0–72.4% with POC-CCA. The Kappa coefficient was modest (0.16; 95% CI: 0.09, 0.23), indicating that the agreement between Kato-Katz and POC-CCA was only slightly better than just by chance. The agreement between the two methods was more pronounced in individuals with moderate/heavy baseline infection than in individuals with light infection; indeed, we obtained a higher Kappa coefficient, sensitivity, and Spearman correlation for those with moderate/heavy infection. These results are in line with previous observations that POC-CCA is more sensitive than Kato-Katz method when used in surveillance studies (18–21).
In this trial, two stool samples were collected per participant and three smears were examined from each sample. With this standard procedure, one could expect higher sensitivity of the Kato-Katz method than in studies using fewer than six smears. However, the CR (which reflects the proportion of positive samples at follow-up) per Kato-Katz was higher than per POC-CCA. The high CR (possibly reflecting lower than expected sensitivity of Kato-Katz) could be linked to the fact that ~60% of the trial participants had light infection (1–99 eggs/gram feces) at baseline. In light infection, there is a chance of missing sparse eggs in stool samples examined by the Kato-Katz method due to human error, leading to a false negative result. In contrast, the chemical reaction-based POC-CCA is able to show some positivity as long as there are antigens excreted in the urine. Our data showed that the consistency between these two tests is greater when analyzing moderate/heavy infection and aligns with WHO’s recommendation to use the Kato-Katz method to diagnose moderate/heavy infection (21, 25, 27). Due to the general low sensitivity of stool sampling and possible observer bias, Kato-Katz often fails to detect light infection. However, for most of this trial (treatment arms 1 through 7; approx. 95% of participants) POC-CCA traces were recorded as positive (+), which partially explains much lower CR of POC-CCA compared with Kato-Katz. Another possible reason for the differences is that batches of POC-CCA can have variable quality leading to inconsistent positivity thresholds (information provided through personal communication with experts) (36).
Another possible reason for the difference in CRs per Kato-Katz and POC-CCA is that worm antigens may persist in the body longer than worms and eggs. Indeed, previous studies have shown that the number of antigen-positive, egg-negative individuals decreases after treatment with PZQ (34, 37). In this trial, the participants were assessed by POC-CCA until Day 14–21, and we noted a trend towards lower POC-CCA positivity over time. It is also important to note that classifying trace results as positive may have an influence on CRs. A longer follow-up should be used in future studies to assess the clearance time of Schistosoma antigens and compare it with the time required for egg clearance from stool.
This trial enrolled participants aged between 3 months and 6 years, i.e. younger than the populations included in the previous prevalence studies comparing the Kato-Katz method with POC-CCA. The younger age of the participants may have contributed to the difference in detection rate; we observed that many children aged <2 years had a positive POC-CCA result of ++ or +++, but showed no eggs by Kato-Katz. Notably, an ongoing prospective cohort study is assessing the use of POC-CCA for qualitative detection of S. japonicum in children ≥2 years of age (38). Future studies should assess the sensitivity of POC-CCA in the detection of S. mansoni in infants. A validated test with high sensitivity and specificity is urgently needed in the context of elimination of schistosomiasis, as it will provide researchers with benchmark CRs.
Conclusion
This phase II clinical trial showed a low level of correlation between the results derived using POC-CCA vs Kato-Katz, especially in light infection; this difference in test sensitivity may be more pronounced among children of pre-school age, whose infection is often light. POC-CCA is a convenient tool for evaluating the burden of S. mansoni over time. It is sensitive, quick, and affordable and may play an important role in schistosomiasis control programs, especially in developing countries. However, partly due to a lack of a gold standard, the absolute performance of POC-CCA has not been objectively quantified.
Data Availability Statement
Any requests for data by qualified scientific and medical researchers for legitimate research purposes will be subject to Merck KGaA’s Data Sharing Policy. All requests should be submitted in writing to Merck KGaA’s data sharing portal https://www.merckgroup.com/en/research/our-approach-to-research-and-development/healthcare/clinical-trials/commitment-responsible-data-sharing.html. When Merck KGaA has a co-research, co-development, or co-marketing or co-promotion agreement, or when the product has been out-licensed, the responsibility for disclosure might be dependent on the agreement between parties. Under these circumstances, Merck KGaA will endeavor to gain agreement to share data in response to requests.
Ethics Statement
The studies involving human participants were reviewed and approved by Independent Ethics Committees (IECs)/Institutional Review Boards (IRBs): Ethikkommission Nordwest- und Zentralschweiz in Switzerland, the National Committee of Ethics and Research in Ivory Coast. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author Contributions
EN’G, ÖY, EK-L, AT, EH, NA, MO, and WB designed the study. EN’G, DB, EH, NA, MO, ND, and FB supervised clinical patient management and ensured quality data collection. BH and XY analyzed the data. All authors contributed to the article and approved the submitted version.
Funding
Since the start of the project in 2012, apart from in-kind contributions by partners, the Pediatric Praziquantel Consortium has received funding from Merck KGaA, Darmstadt, Germany, and grant support from the Bill & Melinda Gates Foundation (BMGF; Grant no. OPP1063223), and the Global Health Innovative Technology (GHIT) Fund (Grant nos. 2013-212, 2014-206, 2016-110 and 2018-210). Furthermore, this project is part of the second European & Developing Countries Clinical Trials Partnership (EDCTP2) programme supported by the European Union (grant number RIA2016S1641).
Conflict of Interest
EN’G, EH, NA, and MO report grants from the Global Health Innovative Technology Fund and the European and Developing Countries Clinical Trials Partnership. ÖY and AT are employees of Merck KGaA, Darmstadt, Germany. EK-L is an employee of Ares Trading S.A., Eysins, Switzerland, an affiliate of Merck KGaA, Darmstadt, Germany. BH and XY are employees of EMD Serono Research & Development Institute, Inc., Billerica, MA, United States, an affiliate of Merck KGaA, Darmstadt, Germany. DB is an employee of Merck (Pty) Ltd, Modderfontein, South Africa, an affiliate of Merck KGaA, Darmstadt, Germany. WB is an employee of Merck Institute of Pharmacometrics, Lausanne, Switzerland, an affiliate of Merck KGaA, Darmstadt, Germany. All authors are members or affiliates of the Pediatric Praziquantel Consortium.
The authors declare that this trial received funding from Merck KGaA, Darmstadt, Germany. The funder had the following involvement with the trial: study design, data collection and analysis, decision to publish, and preparation of the manuscript.
Acknowledgments
We acknowledge the support given from the Consortium partners in making this work possible, the funders for financial assistance, the Man district council for allowing investigators to conduct the trial, and lastly children and parents for their participation. Statistical analysis support was provided by Triclinium Clinical Development, Centurion, South Africa. Editorial support was provided by Jackie Campbell and Olga Ucar of inScience Communications, Springer Healthcare Ltd, UK, and was funded by Merck KGaA, Darmstadt, Germany.
References
1. WHO. Schistosomiasis and Soil-Transmitted Helminthiases: Number of People Treated in 2016. Wkly Epidemiol Rec (2017) 92(49):749–60.
2. WHO. Schistosomiasis. In: Epidemiological Situation. World Health Organization (2018). Available at: https://www.who.int/schistosomiasis/epidemiology/en/. 16 October 2019.
3. WHO. Schistosomiasis Fact Sheet (2019). Available at: https://www.who.int/news-room/fact-sheets/detail/schistosomiasis.
4. Mutapi F. Changing Policy and Practice in the Control of Pediatric Schistosomiasis. Pediatrics (2015) 135(3):536–44. doi: 10.1542/peds.2014-3189
5. Osakunor DNM, Woolhouse MEJ, Mutapi F. Paediatric Schistosomiasis: What We Know and What We Need to Know. PloS Negl Trop Dis (2018) 12(2):e0006144. doi: 10.1371/journal.pntd.0006144
6. Coulibaly JT, N’Gbesso YK, N’Guessan NA, Winkler MS, Utzinger J, N’Goran EK. Epidemiology of Schistosomiasis in Two High-Risk Communities of South Cote D’Ivoire With Particular Emphasis on Pre-School-Aged Children. Am J Trop Med Hyg (2013) 89(1):32–41. doi: 10.4269/ajtmh.12-0346
7. Nalugwa A, Olsen A, Tukahebwa ME, Nuwaha F. Intestinal Schistosomiasis Among Preschool Children Along the Shores of Lake Victoria in Uganda. Acta Trop (2015) 142:115–21. doi: 10.1016/j.actatropica.2014.11.014
8. Ruganuza DM, Mazigo HD, Waihenya R, Morona D, Mkoji GM. Schistosoma Mansoni Among Pre-School Children in Musozi Village, Ukerewe Island, North-Western-Tanzania: Prevalence and Associated Risk Factors. Parasit Vectors (2015) 8(1):377. doi: 10.1186/s13071-015-0997-9
9. Montresor A, Crompton DWT, Gyorkos TW, Savioli L, World Health Organization, Montresor A, et al. Helminth Control in School-Age Children: A Guide for Managers of Control Programmes. Geneva: World Health Organization (2002).
10. WHO. Preventive Chemotherapy in Human Helminthiasis (2006). Available at: https://apps.who.int/iris/bitstream/handle/10665/43545/9241547103_eng.pdf;jsessionid=0F319E2D9941ECB411F67EC69757C5F4?sequence=1.
11. Berhe N, Medhin G, Erko B, Smith T, Gedamu S, Bereded D, et al. Variations in Helminth Faecal Egg Counts in Kato-Katz Thick Smears and Their Implications in Assessing Infection Status With Schistosoma Mansoni. Acta Trop (2004) 92(3):205–12. doi: 10.1016/j.actatropica.2004.06.011
12. Shane HL, Verani JR, Abudho B, Montgomery SP, Blackstock AJ, Mwinzi PN, et al. Evaluation of Urine CCA Assays for Detection of Schistosoma Mansoni Infection in Western Kenya. PloS Negl Trop Dis (2011) 5(1):e951. doi: 10.1371/journal.pntd.0000951
13. Sousa-Figueiredo JC, Pleasant J, Day M, Betson M, Rollinson D, Montresor A, et al. Treatment of Intestinal Schistosomiasis in Ugandan Preschool Children: Best Diagnosis, Treatment Efficacy and Side-Effects, and an Extended Praziquantel Dosing Pole. Int Health (2010) 2(2):103–13. doi: 10.1016/j.inhe.2010.02.003
14. Stothard JR, Sousa-Figueiredo JC, Betson M, Adriko M, Arinaitwe M, Rowell C, et al. Schistosoma Mansoni Infections in Young Children: When are Schistosome Antigens in Urine, Eggs in Stool and Antibodies to Eggs First Detectable? PloS Negl Trop Dis (2011) 5(1):e938. doi: 10.1371/journal.pntd.0000938
15. Sousa-Figueiredo JC, Betson M, Kabatereine NB, Stothard JR. The Urine Circulating Cathodic Antigen (CCA) Dipstick: A Valid Substitute for Microscopy for Mapping and Point-of-Care Diagnosis of Intestinal Schistosomiasis. PloS Negl Trop Dis (2013) 7(1):e2008. doi: 10.1371/journal.pntd.0002008
16. Coulibaly JT, N’Gbesso YK, Knopp S, N’Guessan NA, Silue KD, van Dam GJ, et al. Accuracy of Urine Circulating Cathodic Antigen Test for the Diagnosis of Schistosoma Mansoni in Preschool-Aged Children Before and After Treatment. PloS Negl Trop Dis (2013) 7(3):e2109. doi: 10.1371/journal.pntd.0002109
17. Colley DG, King CH, Kittur N, Ramzy RMR, Secor WE, Fredericks-James M, et al. Evaluation, Validation, and Recognition of the Point-of-Care Circulating Cathodic Antigen, Urine-Based Assay for Mapping Schistosoma Mansoni Infections. Am J Trop Med Hyg (2020) 103(1_Suppl):42–9. doi: 10.4269/ajtmh.19-0788
18. Casacuberta M, Kinunghi S, Vennervald BJ, Olsen A. Evaluation and Optimization of the Circulating Cathodic Antigen (Poc-CCA) Cassette Test for Detecting Schistosoma Mansoni Infection by Using Image Analysis in School Children in Mwanza Region, Tanzania. Parasit Epidemiol Control (2016) 1(2):105–15. doi: 10.1016/j.parepi.2016.04.002
19. Greter H, Krauth SJ, Ngandolo BN, Alfaroukh IO, Zinsstag J, Utzinger J. Validation of a Point-of-Care Circulating Cathodic Antigen Urine Cassette Test for Schistosoma Mansoni Diagnosis in the Sahel, and Potential Cross-Reaction in Pregnancy. Am J Trop Med Hyg (2016) 94(2):361–4. doi: 10.4269/ajtmh.15-0577
20. Mazigo HD, Heukelbach J. Diagnostic Performance of Kato Katz Technique and Point-of-Care Circulating Cathodic Antigen Rapid Test in Diagnosing Schistosoma Mansoni Infection in HIV-1 Co-Infected Adults on the Shoreline of Lake Victoria, Tanzania. Trop Med Infect Dis (2018) 3(2):1–11. doi: 10.3390/tropicalmed3020054
21. Colley DG, Binder S, Campbell C, King CH, Tchuem Tchuente LA, N’Goran EK, et al. A Five-Country Evaluation of a Point-of-Care Circulating Cathodic Antigen Urine Assay for the Prevalence of Schistosoma Mansoni. Am J Trop Med Hyg (2013) 88(3):426–32. doi: 10.4269/ajtmh.12-0639
22. Merck KGAA. An Open Label Dose Finding Safety and Efficacy in Children and Infants Infected With Schistosomiasis (s.Mansoni) (2020). Available at: https://clinicaltrials.gov/ct2/show/NCT02806232.
23. N’Goran EK, Yalkinoglu Ö, Kourany-Lefoll E, Tappert A, Hayward B, Yin X, et al. Efficacy and Safety of New Disintegrating Oral Formulations of Praziquantel (Racemate and L-praziquantel) in Schistosoma Mansoni-Infected Preschool-Aged Children and Infants: A Randomized, Exploratory, Dose-Finding Phase 2 Study. Manuscript in preparation (2021).
24. Casacuberta-Partal M, Hoekstra PT, Kornelis D, van Lieshout L, van Dam GJ. An Innovative and User-Friendly Scoring System for Standardised Quantitative Interpretation of the Urine-Based Point-of-Care Strip Test (POC-CCA) for the Diagnosis of Intestinal Schistosomiasis: A Proof-of-Concept Study. Acta Trop (2019) 199:105150. doi: 10.1016/j.actatropica.2019.105150
25. WHO. Bench Aids for the Diagnosis of Intestinal Parasites, 2nd ed. World Health Organization (2019).
26. Viera AJ, Garrett JM. Understanding Interobserver Agreement: The Kappa Statistic. Fam Med (2005) 37(5):360–3.
27. Barenbold O, Raso G, Coulibaly JT, N’Goran EK, Utzinger J, Vounatsou P. Estimating Sensitivity of the Kato-Katz Technique for the Diagnosis of Schistosoma Mansoni and Hookworm in Relation to Infection Intensity. PloS Negl Trop Dis (2017) 11(10):e0005953. doi: 10.1371/journal.pntd.0005953
28. Siqueira LM, Couto FF, Taboada D, Oliveira AA, Carneiro NF, Oliveira E, et al. Performance of POC-CCA(R) in Diagnosis of Schistosomiasis Mansoni in Individuals With Low Parasite Burden. Rev Soc Bras Med Trop (2016) 49(3):341–7. doi: 10.1590/0037-8682-0070-2016
29. Armoo S, Cunningham LJ, Campbell SJ, Aboagye FT, Boampong FK, Hamidu BA, et al. Detecting Schistosoma Mansoni Infections Among Pre-School-Aged Children in Southern Ghana: A Diagnostic Comparison of Urine-CCA, Real-Time PCR and Kato-Katz Assays. BMC Infect Dis (2020) 20(1):301. doi: 10.1186/s12879-020-05034-2
30. Gandasegui J, Fernandez-Soto P, Muro A, Simoes Barbosa C, Lopes de Melo F, Loyo R, et al. A Field Survey Using LAMP Assay for Detection of Schistosoma Mansoni in a Low-Transmission Area of Schistosomiasis in Umbuzeiro, Brazil: Assessment in Human and Snail Samples. PloS Negl Trop Dis (2018) 12(3):e0006314. doi: 10.1371/journal.pntd.0006314
31. Pontes LA, Oliveira MC, Katz N, Dias-Neto E, Rabello A. Comparison of a Polymerase Chain Reaction and the Kato-Katz Technique for Diagnosing Infection With Schistosoma Mansoni. Am J Trop Med Hyg (2003) 68(6):652–6. doi: 10.4269/ajtmh.2003.68.652
32. Price M, Cyrs A, Sikasunge CS, Mwansa J, Lodh N. Testing the Infection Prevalence of Schistosoma Mansoni After Mass Drug Administration by Comparing Sensitivity and Specificity of Species-Specific Repeat Fragment Amplification by PCR and Loop-Mediated Isothermal Amplification. Am J Trop Med Hyg (2019) 101(1):78–83. doi: 10.4269/ajtmh.19-0121
33. Utzinger J, Becker SL, van Lieshout L, van Dam GJ, Knopp S. New Diagnostic Tools in Schistosomiasis. Clin Microbiol Infect (2015) 21(6):529–42. doi: 10.1016/j.cmi.2015.03.014
34. Barenbold O, Garba A, Colley DG, Fleming FM, Haggag AA, Ramzy RMR, et al. Translating Preventive Chemotherapy Prevalence Thresholds for Schistosoma Mansoni From the Kato-Katz Technique Into the Point-of-Care Circulating Cathodic Antigen Diagnostic Test. PloS Negl Trop Dis (2018) 12(12):e0006941. doi: 10.1371/journal.pntd.0006941
35. de Sousa SRM, Dias IHL, Fonseca ÁLS, Contente BR, Nogueira JFC, da Costa Oliveira TN, et al. Concordance of the Point-of-Care Circulating Cathodic Antigen Test for the Diagnosis of Intestinal Schistosomiasis in a Low Endemicity Area. Infect Dis Poverty (2019) 8(1):1–9. doi: 10.1186/s40249-019-0551-7
36. Colley DG, Ramzy RMR, Maganga J, Kinung’hi S, Odiere MR, Musuva RM, et al. The POC-CCA Assay for Detection of Schistosoma Mansoni Infection Needs Standardization in Production and Proper Quality Control to be Reliable. Manuscript in preparation.
37. Adriko M, Standley CJ, Tinkitina B, Tukahebwa EM, Fenwick A, Fleming FM, et al. Evaluation of Circulating Cathodic Antigen (CCA) Urine-Cassette Assay as a Survey Tool for Schistosoma Mansoni in Different Transmission Settings Within Bugiri District, Uganda. Acta Trop (2014) 136:50–7. doi: 10.1016/j.actatropica.2014.04.001
38. Ina-Respond. Validation of POC-CCA Rapid Urine Test for Qualitative Detection of Schistosoma Japonicum (SchisCCA) (2019). Available at: https://clinicaltrials.gov/ct2/show/NCT03870204.
Keywords: schistosomiasis, Schistosoma mansoni, point-of-care circulating cathodic antigen, Kato-Katz, praziquantel, pediatric, clinical trial
Citation: Yin X, N’Goran EK, Ouattara M, Aka NAD, Diakité NR, Bassa FK, Kourany-Lefoll E, Tappert A, Yalkinoglu Ö, Huber E, Bezuidenhout D, Bagchus WM and Hayward B (2021) Comparison of POC-CCA with Kato-Katz in Diagnosing Schistosoma mansoni Infection in a Pediatric L-Praziquantel Clinical Trial. Front. Trop. Dis 2:686288. doi: 10.3389/fitd.2021.686288
Received: 26 March 2021; Accepted: 31 May 2021;
Published: 17 June 2021.
Edited by:
Joseph Daniel Turner, Liverpool School of Tropical Medicine, United KingdomReviewed by:
Russ Russell Stothard, Liverpool School of Tropical Medicine, United KingdomJose Ma. Moncada Angeles, University of the Philippines Manila, Philippines
Copyright © 2021 Yin, N’Goran, Ouattara, Aka, Diakité, Bassa, Kourany-Lefoll, Tappert, Yalkinoglu, Huber, Bezuidenhout, Bagchus and Hayward. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaoyan Yin, eGlhb3lhbi5hLnlpbkBlbWRzZXJvbm8uY29t