 Houari Aissaoui1Milene Chaptal1Vincent Thomas2Dominique Louvel2Antoine Adenis3,4
Houari Aissaoui1Milene Chaptal1Vincent Thomas2Dominique Louvel2Antoine Adenis3,4 Kinan Drak Alsibai5,6*
Kinan Drak Alsibai5,6*- 1Department of Medicine, Pulmonology Unit, Cayenne Hospital Center Andrée Rosemon, Cayenne, French Guiana
- 2Department of Medicine B, Cayenne Hospital Center Andrée Rosemon, Cayenne, French Guiana
- 3Centre d’Investigation Clinique Antilles-Guyane (Inserm 1424), Cayenne Hospital Center Andrée Rosemon, Cayenne, French Guiana
- 4Epidemiology of Tropical Parasitoses, Université de Guyane, Cayenne, French Guiana
- 5Department of Pathology, Cayenne Hospital Center Andrée Rosemon, Cayenne, French Guiana
- 6Center of Biological Resources (CRB Amazonie), Cayenne Hospital Center Andrée Rosemon, Cayenne, French Guiana
The hostile conditions at informal and illegal mining sites in the Amazonian forest erode the miner’s health, exposing workers to a broad range of diseases because most of the gold is extracted using mercury (Hg). The Hg vapor used daily at gold panning sites presents an environmental threat to the ecosystems and human health. We report the case of a 58-year-old man who has worked in gold panning for over 30 years, presented with diffuse interstitial pneumonia characterized by bilateral images of ground glass and mosaic opacities on the chest CT scan. Based on the negative differential diagnosis (cardiovascular, infectious, autoimmune or cancer), the context of chronic exposure to Hg in a patient who has been working for decades on illegal gold panning sites, we concluded to a chronic form of heavy metal hypersensitivity pneumonia. This hypothesis was supported by high levels of mercury in blood and urine. Mercury hypersensitivity pneumonia might be more frequent than presently thought with thousands of workers chronically exposed to high mercury concentrations among others pollutants. Medical practitioners should systematically seek for chronic respiratory illnesses associated with pollutants exposure in these vulnerable workers with poor health.
Introduction
French Guiana is a European territory located on the Guiana Shield in South America where informal and illegal gold panning takes place on its entire plateau. The annual production of this informal gold panning is around 10 tons of gold for 10,000 illegal gold miners working in about 600 sites in the Amazonian forest (1). The hostile conditions at mining sites erode the miner’s health exposing workers to a broad range of diseases (1). Moreover, this informal exploitation of gold mines presents an environmental threat to the ecosystems and human health, because most of the gold is extracted using mercury (Hg) (2).
Mercury is a ubiquitous element that is found in small amount in the environment and has several chemical forms. The elemental Hg (Hg0) form has low vapor pressures and low water solubility, whether the divalent Hg (Hgþþ) form has strong affinity for ligands such as chlorine, sulphur, hydroxyl ions, and methyl ion CH3 þ (methylmercury, CH3Hgþ) (3, 4). Hgþþ shows a strong tendency to become bioaccumulative within different organisms and is also the most toxic chemical form for humans. Once Hg0 is introduced into aquatic environments, it can be transformed into CH3Hgþ by bacterial action in the anoxic spaces surrounding aquatic plants (5). It is intensely accumulated in predatory fish, whose consumption is one of the main sources of health risks for indigenous and riparian populations in the Amazonian region (2, 4).
Hg is used in massive quantities in informal gold panning, estimated at 1.3 g of Hg for every 1 g of gold recovered (6). The Hg released worldwide from this activity is estimated at 650 to 1000 tons per year (7, 8). Gold miners use mercury to amalgamate gold flakes or dust, and then heat these amalgams to recover the gold. The mercury vapor released is inhaled by the gold miners daily.
Mercury intoxication is characterized by neurological, cutaneous and respiratory damage. Respiratory intoxication by mercury can lead to hypersensitivity pneumonia (HP), which may become chronic, as we will describe in the following report.
Case Report
We report a 58-year-old male with a past history of smoking (40 pack-year), drug addiction to marijuana, malaria and treated infectious pneumonia. The patient mentioned that he quit smoking in 1992, but he did not wish to give more details about his drug addiction. He has been working in gold panning for more than 30 years. The patient has recently consulted the Respiratory Unit of our hospital following an alteration in his general health condition. He was suffering from marked asthenia, a dry cough, and stage 3 of mMRC (modified medical research council) Dyspnea Scale for a year, without chest pain.
On clinical examination, there was digital hippocratism, palpable cervical adenopathy and skin lesions on the hands and legs. Stethoscope revealed regular heart sounds, but diffuse rhonchi with some crackles in both lungs. Respiratory functional exploration (RFE) found a severe restrictive syndrome with total lung capacity (TLC) = 55%, forced expiratory volume in 1 s/forced vital capacity (FEV1/FVC) ratio = 86%, FEV1 = 34% and FVC = 32% of the predicted values. In the 6 min walk test (6MWT), the patient walked 480 meters (theoretical distance 753 meters) with desaturation at 85% at the end of the test and dyspnea of 6/10 on the Borg scale. The partial pressure of oxygen (PaO2) was 72 mm/Hg in ambient air with a saturation of 97%. The Brain natriuretic peptide (BNP) and the electrocardiogram (ECG) were normal.
The chest computed tomography (CT) scan shows diffuse ground glass images without craniocaudal gradient, mosaic-like attenuation, linear and retractile opacities, and some bilateral bronchiectasis (Figure 1).
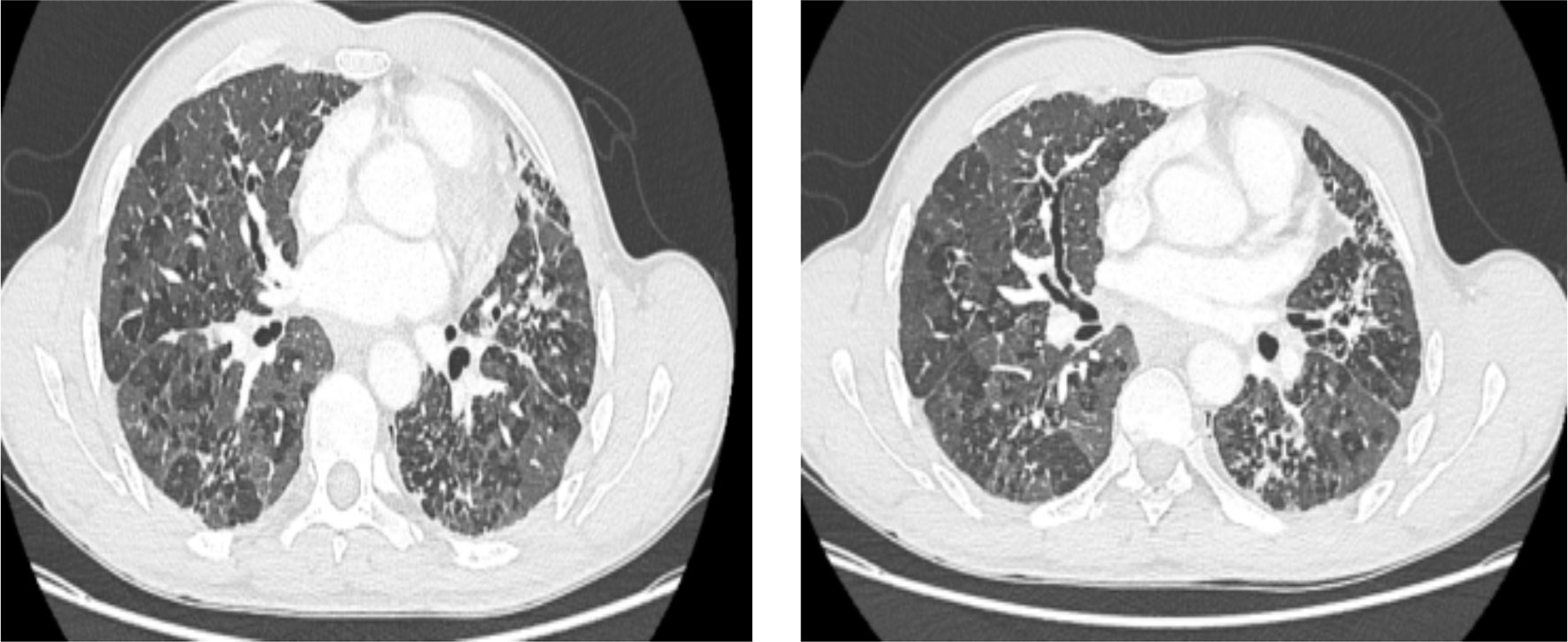
Figure 1 Chest CT scan shows at different levels diffuse, bilateral ground glass opacities and mosaic-like attenuation associated with signs of chronic interstitial involvement: reticulations and lobular distortion, bronchiectasis and traction of lung fissures.
Biological analysis shows a C reactive protein (CRP) at 20 mg/l without sign of an inflammatory syndrome. Serum protein electrophoresis and immunological analyses were normal. Microbial serology, HIV serology, and serum precipitins to Farmer’s lung and Bird Breeder’s lung were negative.
The bronchoalveolar lavage liquid (BAL) shows a cellularity at 100 000 cells/ml with inflammatory cellular formula (macrophages 56%, neutrophils 35%, lymphocytes 5%, and eosinophils 4%). There were no tumor cells or infectious pathogens in the BAL. The biopsy of the salivary glands was normal.
The heavy metal analyses show elevated levels of mercury in blood 41.3 ug/L (standard < 5 ug/L) and in urine 6.2 ug/g creatinine (standard < 5 ug/g creatinine). The thiocyanate and lead levels were normal in the blood and urine.
Considering the diffuse interstitial pneumonia, characterized by bilateral images of ground glass and mosaic opacities on the chest CT scan, the negative workup looking at differential diagnoses (cardiovascular, infectious, autoimmune or cancer), the context of chronic exposure to pollutants in a patient working for decades at illegal gold panning sites, we concluded on a chronic form of heavy metals hypersensitivity pneumonia. This hypothesis was supported by the occupational exposure to mercury during the entire period of gold panning (> 30 years) and the high levels of mercury in blood and urine.
The management of our patient consisted of a symptomatic treatment with antibiotics during an episode of bronchial infection, oxygen therapy and analgesics. The chest CT scan performed 6 months later showed stable lung lesions.
Discussion
The hypersensitive pneumonia (HP) is a pulmonary pathology of immunologic mechanism with humoral and cellular mediation (9). It is often due to chronic inhalation of microbial or fungal antigens, and sometimes to chemical or metal agents (10). The HP related to chemical or heavy metal agents is an interstitial lesion caused often by the inhalation of antigen from the professional environment of the patient. The frequency of HP varies according to the causal agent. For example, the prevalence among workers in the mushroom industry is estimated at 5% (11), 5.3% in the tobacco industry (12) and up to 37.5% among machine operators (13).
To our knowledge, this is the first description of an occupational interstitial lung disease in clandestine gold miners linked to the use of mercury.
In our observation, the HP was caused by mercury. To confirm this hypothesis other etiologies of diffuse chronic interstitial pulmonary pathology must be eliminated as infectious, drug-induced, neoplastic and idiopathic diseases as well as pneumoconiosis and sarcoidosis.
The infectious cause was ruled out because the biological, bacteriological and cytological analyses confirmed the absence of infectious pathogens: (i) Mycobacterium tuberculosis is absent on direct examination and in culture, (ii) Quantiferon test is negative, (iii) Infectious serology and urinary antigens of legionella and pneumococcus are negative and (iv) Bacteriological, mycological, and parasitological analyses on BAL were negative.
The absence of regular drug use confirmed with a negative drug screen in urine and absence of exposure to exogenous agents such as silicosis and asbestos confirmed with a blood screening ruled out the drug-induced pathology and pneumoconiosis respectively. In addition, BAL did not find malignant cells and the chest CT scan was not evocative of cancer. Similarly, characteristic tomographic honeycomb lesions with a caudal craniocaudal gradient of idiopathic pulmonary fibrosis were not found.
Because of the patient’s age, the predominance of upper lung lesions, mediastinal adenopathy, and the absence of inflammatory syndrome, the diagnosis of sarcoidosis was considered in the first place. Nevertheless, the conversion enzyme was normal, and there was no lymphopenia or polyclonal hypergammaglobulinemia on serum protein electrophoresis. In addition, cytological analysis of BAL did not show lymphocytosis and histological analysis of bronchial and salivary gland biopsies did not find the typical sarcoidosis granuloma.
In our observation, the diagnosis of HP in its chronic form is based on Lacasse’s criteria (14). The patient presented chronic respiratory symptoms (cough and dyspnea), crackling rales and digital hippocratism, ground glass opacities, restrictive respiratory syndrome on RFE and high levels of heavy metals in blood and urine. Unfortunately, mercury serum precipitin level was not performed and unavailable at the time of diagnosis.
The absence of significant lymphocytosis in BAL in this chronic form of HP was probably related to withdrawal from exposure to mercury several months ago. Nevertheless, the absence of hyperlymphocytosis in HP has already been described in a Danish cohort in pediatric patients (15) and in an adult population in a Portuguese cohort that found normal lymphocyte levels in 25.3% of chronic HP (16).
In this observation, in addition to lung involvement, other less specific signs of mercury exposure are also present such as asthenia, cervical adenopathy, and skin lesions on the hands and legs (Figure 2).

Figure 2 Cutaneous lesions on the hands and legs are characterized by slightly raised papules with a flat, hypopigmented surface in the center. These lesions are compatible with lichenoid contact dermatitis.
The illegal gold miners are exposed primarily to inhalation of mercury vapor. Thus, toxicity primarily affects the respiratory pathway even though skin or eye irritation may occur. Cutaneous lesions associated with prolonged exposure to mercury are often non-specifics. They correspond to contact dermatitis or lichenoid reaction (17). In addition, the inhalation of mercury vapor can cause exanthem-type lesions (18). Furthermore, mucocutaneous lymph node syndrome was also described in patients with increased urinary mercury excretion (19, 20).
The reference therapy in this type of chronic HP, apart from symptomatic treatment, is to avoid contact with mercury. In our case, the second chest CT scan performed 6 months showed stable lung lesions.
For all these reasons, susceptible workers must use the protective gears to avoid health problem related to chronic exposure to mercury vapor. Protection of at least level C (Yellow Zone) could be used, since the contaminant and its concentration are more or less known. In the case of gold miners, the use of a certified APR CBRN mask (Air Purifying Respirators - Chemical, Biological, Radiological, Nuclear mask) is strongly recommended. In addition, coveralls and chemical resistant gloves and boots are also recommended (21). In case of exposure to other mercury compounds, the respiratory recommendations and the type of mask are adjusted to the exposure concentration measured by the mg/m3 unit (21).
A regular follow-up of at least one per year by a pulmonary, dermatological and biological check-up in these vulnerable workers can avoid occupational diseases.
In order to prevent the catastrophic consequences of mercury on the environment and the health of workers, its use in illegal gold mining sites must be avoided. In France, this use is normally prohibited in the regulated gold panning site. Nevertheless, we are aware that such prevention and monitoring applied in many legal gold mining sites, are difficult to apply in illegal workers as they have difficult access to the health care system. In addition, the illegal gold miners work in the Amazon rainforest in conditions of extreme heat and humidity and without hygiene rules.
Finally, we recommend further research and environmental analysis to better understand the working conditions of illegal gold miners, and to determine the chemical and environmental elements impacting the health status of these workers.
Conclusion
Mercury use in the informal and illegal gold mining sites may lead to disastrous consequences in the environment, but it may also significantly impact the gold miners’ health notably through mercury vapor inhalation. This massive and prolonged inhalation may be responsible of chronic hypersensitivity pneumonia. The acute form of HP shows anamnestic and immunological reaction, whereas the chronic form presents with pulmonary fibrosis seen on chest CT scan. In clinical practice, HP diagnosis is considered as an elimination diagnosis but it is probably overlooked during regular differential diagnosis workup in the Amazonian region. Mercury HP might be more frequent than presently thought with thousands of workers chronically exposed to high mercury concentrations among others pollutants daily. Despite the informal and illegal practice of gold panning, the workers at risk of mercury exposure should wear certified protective mask, gloves, boots and coveralls. Medical practitioners should systematically seek for chronic respiratory illnesses associated with pollutants exposure in these vulnerable workers with poor health.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics Statement
All the patients of our institute are informed that their biological samples and associated data may be used for scientific purposes, and have the right to object. Cayenne hospital center welcome booklet contains information on biological sample and associated data written in several languages. An information leaflet is also given to the patient, in whom the information is reminded, and the procedure for withdrawing consent is described according to the European General Data Protection Regulation (GDPR 2018). Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author Contributions
Conceptualization, HA and KD. Investigation, HA, MC, VT, DL and KD. Resources, HA, MC, VT and KD. Writing – Original Draft Preparation, HA and KD. Writing – Review and Editing, HA, AA and KD. Supervision, KD. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Douine M, Mosnier E, Le Hingrat Q, Charpentier C, Corlin F, Hureau L, et al. Illegal Gold Miners in French Guiana: A Neglected Population With Poor Health [Published Correction Appears in BMC Public Health. 2017 Sep 22;17 (1):736]. BMC Public Health (2017) 18(1):23. doi: 10.1186/s12889-017-4557-4
2. Malm O. Gold Mining as a Source of Mercury Exposure in the Brazilian Amazon. Environ Res (1998) 77(2):73–8. doi: 10.1006/enrs.1998.3828
3. Gosar M, Pirc S, Sajn R, Bidovec M, Mashyanov N, Sholupov S. Distribution of Mercury in the Atmosphere Over Idrija, Slovenia. Environ Geochem Health (1997) 19:101–10. doi: 10.1023/A:1018402605831
4. Santos-Francés F, García-Sánchez A, Alonso-Rojo P, Contreras F, Adams M. Distribution and Mobility of Mercury in Soils of a Gold Mining Region, Cuyuni River Basin, Venezuela. J Environ Manage (2011) 92(4):1268–76. doi: 10.1016/j.jenvman.2010.12.003
5. Mauro JB, Guimarães JRD, Melamed R. Mercury Methylation in Macrophyte Roots of a Tropical Lake. Water Air Soil Pollut (2001) 127:271–80. doi: 10.1023/A:1005222902966
6. Muresan B. Orpaillage et Construction de Barrages en Guyane Française, Une Alchimie Risquee. Créteil, France: Centre pour la Communication Scientifique Directe (CCSD). (2008). (hal-00414234)
7. Olivero J, Solano B. Mercury in Environmental Samples From a Waterbody Contaminated by Gold Mining in Colombia, South America. Sci Total Environ (1998) 217:83–9. doi: 10.1016/S0048-9697(98)00175-2
8. Guedron S, Grangeon S, Lanson B, Grimaldi B. Mercury Speciation in a Tropical Soil Association; Consequence of Gold Mining on Hg Distribution in French Guyana. Geoderma (2009) 153:331–46. doi: 10.1016/j.geoderma.2009.08.017
9. Shaon G, Reboux S, Moulonguet JC. Dalphin: Hypersensitivity Pneumopathies in the Workplace. Rev Mal Respir (2006) 23:705–25. doi: 10.1016/S0761-8425(06)72084-8
10. Dalphin JC. Alvéolites Allergiques Extrinsèques en Milieu Agricole Extrinsic Allergic Alveolitis in Agricultural Environment. Rev Prat (1992) 42(14):11790–6.
11. Tanaka H, Saikai T, Sugawara H, Tsunematsu K, Takeya I, Koba H Matsuura A, et al. Three-Year Follow-Up Study of Allergy in Workers in a Mushroom Factory. Respir Med (2001) 95:943–8. doi: 10.1053/rmed.2001.1187
12. Huuskonen MS, Husman K, Jarvisalo J, Korhonen O, Kotimaa M, Kuusela T, et al. Extrinsic Allergic Alveolitis in the Tobacco Industry. Br J Ind Med (1984) 41:77–83. doi: 10.1136/oem.41.1.77
13. Bernstein DI, Lummus ZL, Santilli G, Siskosky J, Bernstein IL. Machine Operator’s Lung. A Hypersensitivity Pneumonitis Disorder Associated With Exposure to Metalworking Fluid Aerosols. Chest (1995) 108:636–41. doi: 10.1378/chest.108.3.636
14. Lacasse Y, Selman M, Costabel U, Dalphin JC, Morell F, Erkinjuntti-Pekkanen R, et al. Classification of Hypersensitivity Pneumonitis: A Hypothesis. Int Arch Allergy Immunol (2009) 149(2):161–6. doi: 10.1159/000189200
15. Buchvald F, Petersen BL, Damgaard K, Deterding R, Langston C, Fan LL, et al. Frequency, Treatment, and Functional Outcome in Children With Hypersensitivity Pneumonitis. Pediatr Pulmonol (2011) 46:1098–107. doi: 10.1002/ppul.21479
16. Santos V, Martins N, Sousa C, Jacob M, Padrão E, Melo N, et al. Hypersensitivity Pneumonitis: Main Features Characterization in a Portuguese Cohort. Pulmonology (2020) 26(3):130–7. doi: 10.1016/j.pulmoe.2019.09.004
17. Boyd AS, Seger D, Vannucci S, Langley M, Abraham JL, King LE Jr. Mercury Exposure and Cutaneous Disease. J Am Acad Dermatol (2000) 43:81–90. doi: 10.1067/mjd.2000.106360
18. Rogers M, Goodhew P, Szafraniec T, McColl I. Mercury Exanthem. Australas J Dermatol (1987) 27:70–7. doi: 10.1111/j.1440-0960.1986.tb00292.x
19. Cheek DB. Comment on Mucocutaneous Lymph Node Syndrome: Could It Be a Heavy Metal Poisoning? Pediatrics (1975) 56:335–6.
20. Orlowski JP, Mercer RD. Urine Mercury Urine Mercury Levels in Kawasaki’s Disease. Pediatrics (1980) 66:633–6.
21. NIOSH Pocket Guide to Chemical Hazards - Mercury Compounds. National Institute for Occupational Safety and Health. Available at: https://www.cdc.gov/niosh/npg/npgd0383.html.
Keywords: gold miner, mercury, Amazonia, ecosystem, hypersensitivity pneumonia, occupational disease, occupational health and safety
Citation: Aissaoui H, Chaptal M, Thomas V, Louvel D, Adenis A and Drak Alsibai K (2021) Case Report: Gold Miner’s Lung: A Case of Chronic Hypersensitivity Pneumonia in Amazonian Forest. Front. Trop. Dis 2:685248. doi: 10.3389/fitd.2021.685248
Received: 24 March 2021; Accepted: 21 July 2021;
Published: 09 August 2021.
Edited by:
Suraj Bhattarai, Global Institute for Interdisciplinary Studies (GIIS), NepalReviewed by:
Semeeh Omoleke, World Health Organization - Regional Office for Africa, Republic of CongoAlvona Zi Hui Loh, MOH Holdings, Singapore
Copyright © 2021 Aissaoui, Chaptal, Thomas, Louvel, Adenis and Drak Alsibai. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kinan Drak Alsibai, a2RyYWsuYWxzaWJhaUBkb2N0b3IuY29t