
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CLINICAL TRIAL article
Front. Trop. Dis., 12 October 2021
Sec. Neglected Tropical Diseases
Volume 2 - 2021 | https://doi.org/10.3389/fitd.2021.679373
This article is part of the Research TopicHighlights in Neglected Tropical Diseases 2021/22View all 8 articles
 Eliézer K. N’Goran1
Eliézer K. N’Goran1 Özkan Yalkinoglu2
Özkan Yalkinoglu2 Elly Kourany-Lefoll3
Elly Kourany-Lefoll3 Aliona Tappert4
Aliona Tappert4 Brooke Hayward5
Brooke Hayward5 Xiaoyan Yin5Deon Bezuidenhout6Eric Huber7,8N. A. David Aka1Mamadou Ouattara1
Xiaoyan Yin5Deon Bezuidenhout6Eric Huber7,8N. A. David Aka1Mamadou Ouattara1 Wilhelmina Bagchus9* on behalf of the Pediatric Praziquantel Consortium
Wilhelmina Bagchus9* on behalf of the Pediatric Praziquantel ConsortiumIntroduction: Two novel formulations of praziquantel (PZQ) and Levo-(L-)PZQ (arpraziquantel) have been developed for the treatment of schistosomiasis in preschool-age children and infants.
Methods: This open-label, dose-finding Phase 2 study assessed the efficacy and safety of PZQ formulations in children and infants infected with Schisostoma mansoni in Côte d’Ivoire. In Part 1, 420 children aged 2.1–6.9 years (weight 10.0–29.9 kg) were enrolled and randomized to one of 7 treatment arms (n=60 per arm): commercially available racemate (rac)-PZQ at 3x20 mg/kg or 40 mg/kg (treatment arms 1 and 2); rac-PZQ orodispersible tablet (ODT) at 40 mg/kg or 60 mg/kg (treatment arms 3 and 4); or L-PZQ ODT at 30 mg/kg, 45 mg/kg, or 60 mg/kg (treatment arms 5, 6, and 7). The optimal formulation and dose identified (L-PZQ ODT 50 mg/kg) was used in Part 2, which enrolled 24 infants aged 6–24 months (weight 7.5–14.8 kg). Infants were treated in an age-staggered approach: age 13–24 months (treatment arm 8, n=20) and age 6–12 months (treatment arm 9, n=4). The primary endpoint was clinical cure rate (CR) demonstrated by the Kato–Katz method 14–21 days post-treatment. Secondary endpoints included CR by point-of-care circulating cathodic antigen, egg reduction rate (ERR), and adverse events (AEs).
Results: In Part 1, CRs ≥70% were achieved in all treatment arms and were highest with L-PZQ ODT 60 mg/kg (89.7%), rac-PZQ 3x20 mg/kg (89.5%), and L-PZQ ODT 45 mg/kg (86.0%). In Part 2, CRs were >90%. All treatment arms had ERRs >95%. Treatment-related AEs were reported by 71 participants (16.0%) and were similar across treatment arms; most were mild and transient. The most common treatment-emergent AEs were laboratory abnormalities. No deaths or discontinuation due to treatment-emergent AEs were reported and no new safety concerns were identified.
Conclusion: New rac-PZQ and L-PZQ ODT formulations used as single-dose therapy against S. mansoni demonstrated acceptable overall efficacy and safety in preschool-age children and infants, warranting further studies in this population.
Clinical Trial Registration: ClinicalTrials.gov, identifier NCT02806232; Pan African Clinical Trials Registry, identifier PACTR201604001493593.
Schistosomiasis, an acute and chronic disease caused by trematode parasitic worms of the genus Schistosoma, belongs to a group of neglected tropical diseases and represents a major health problem in many developing countries worldwide, including sub-Saharan Africa, where it accounts for 200,000 deaths annually (1, 2).
Schistosoma mansoni is responsible for the vast majority of intestinal schistosomiasis infections in South and Central America and in sub-Saharan Africa (1). The parasite penetrates human skin during contact with infested water (e.g. during swimming or domestic activities). Chronic schistosomiasis is associated with significant morbidity; school-age and preschool-age children are particularly vulnerable to infection, and often suffer from serious consequences such as delayed physical and cognitive development (1, 3, 4).
The World Health Organization (WHO) recommends preventive chemotherapy against schistosomiasis with a single, oral dose of praziquantel (PZQ) at 40 mg/kg body weight. The main target population are school-age children; however, the exposure of adults and preschool-age children/infants to infection is recognized, and WHO now recommends extending preventive campaigns to children under the age of 6 years (3–5). Early targeting of schistosome infections would help achieve maximum benefit for the long-term health of affected children (3, 6).
PZQ, which is administered as a racemic mixture of R-(-)-praziquantel (levo-PZQ or L-PZQ; arpraziquantel) and S-(+)-praziquantel (dextro-PZQ or D-PZQ) (the racemic mixture is hereafter referred to as rac-PZQ), is currently available in the form of large 600 mg tablets that need to be crushed for oral administration in children, given the size of the tablet. Consequently, there is the potential for imprecise dosing; compliance issues can also arise due to the bitter taste of the formulation, which is largely attributed to D-PZQ (7). Against this background, the WHO has long recognized a medical need for a more palatable, easy-to-administer pediatric formulation of PZQ (4), which led to the establishment of the Pediatric Praziquantel Consortium in 2012 (6, 8). This international, non-profit, public-private partnership aims to reduce the global disease burden of schistosomiasis by addressing the medical need of infected preschool-age children (https://www.pediatricpraziquantelconsortium.org/). The consortium subsequently developed two innovative orodispersible tablet (ODT) formulations for PZQ for pediatric use: a rac-PZQ formulation containing a mixture of the enantiomers in a 1:1 ratio, and the other containing only L-PZQ, which is devoid of the biologically inactive enantiomer. Both have been developed as a 150 mg ODT that are smaller, compared with the existing rac-PZQ tablet formulation, and can be taken with or without water. The formulation also includes sweeteners to enhance palatability (less bitterness) and has been formulated with an appropriate shelf-life to withstand challenging logistics and field temperatures that prevail in Africa. Previous studies have shown these formulations to be more palatable to children than the existing tablet formulation of rac-PZQ (7, 9), and would allow for more precise dosing of children and infants of different body weights.
This open-label, dose-finding study assessed the efficacy and safety of three formulations of PZQ (commercially available rac-PZQ tablet, rac-PZQ ODT, and L-PZQ ODT) in preschool-age children and infants infected with S. mansoni in Côte d’Ivoire (NCT02806232).
This open-label Phase 2 study was performed at the District Hospital of Man in Côte d’Ivoire (between 12 June 2016 and 17 November 2018). The hospital has a catchment area of villages located in the prefectures of Biankouman, Facobly, Kouibly, and Man, where S. mansoni is endemic (10). The study consisted of two parts. Part 1 was a randomized, dose-finding study comparing rac-PZQ tablet, rac-PZQ ODT, and L-PZQ ODT in children aged 2–6 years infected with S. mansoni with the main objective of identifying the optimal single dose of rac-PZQ ODT or L-PZQ ODT formulation that would have a clinically meaningful cure rate (CR) and an acceptable safety profile for further studies. Part 2 assessed the efficacy and safety of the ODT formulation and dosage selected in Part 1 in infants aged 3–24 months infected with S. mansoni.
The study included male and female children and infants (minimum weight 8.0 kg and 4.0 kg, respectively), diagnosed with S. mansoni infection (>1 egg/1 occurrence). Participants were excluded from enrollment if they had a history of adverse reactions to PZQ or of acute or severe chronic disease, liver transaminases above 3x upper limit of normal, fever, another debilitating illness, evidence of mixed S. haematobium and S. mansoni infection, or exposure to any medication that might affect the efficacy or pharmacokinetics of PZQ in the 4 weeks prior to study screening. Participants were also excluded if, in the opinion of the investigator, their participation constituted a risk or a contraindication that could interfere with the study objectives, or they were unlikely to comply with study requirements.
In Part 1 of the study, preschool-age participants were randomized to one of 7 treatment arms. Randomization was stratified by subjects’ infection intensity at baseline (60% light and 40% moderate/heavy infections), according to WHO categories: light/moderate/heavy corresponding to 1–99/100–399/≥400 eggs per gram of stool, respectively (11). Participants were randomized sequentially by the investigator to receive commercially available rac-PZQ at 20 mg/kg three times a day (treatment arm 1); commercially available rac-PZQ at 40 mg/kg single dose (treatment arm 2); rac-PZQ ODTs at 40 mg/kg single dose (treatment arm 3); rac-PZQ ODTs at 60 mg/kg single dose (treatment arm 4); L-PZQ ODTs at 30 mg/kg single dose (treatment arm 5); L-PZQ ODTs at 45 mg/kg single dose (treatment arm 6); or L-PZQ ODTs at 60 mg/kg single dose (treatment arm 7).
For Part 2, the optimal ODT formulation and dose level for investigation were chosen by the Safety Monitoring Committee (SMC) based on a pre-specified decision algorithm developed by Merck and endorsed by the Pediatric Praziquantel Consortium, which incorporated efficacy and safety results observed in Part 1 of the study. In brief, both efficacy (overall CR, CR by infection intensity, and egg reduction rate [ERR]) and safety (number, type, and severity of adverse events [AEs]) criteria for each of the 5 ODT treatment arms and 2 reference treatment arms included in Part 1 were considered. This allowed for generation of a utility score for each treatment arm according to the number of points assigned for each of the desired attributes. The 45 mg/kg dose of L-PZQ ODT emerged from this assessment of Part 1 as the optimal formulation and dose, followed by the 60 mg/kg dose of L-PZQ ODT. On this basis and given that the ODT tablets have a 150-mg strength, a dose of 50 mg/kg (nearest to 45 mg/kg) was selected for Part 2. Infants were to be enrolled in an age-staggered approach: infants aged 13–24 months (treatment arm 8) and infants aged 3–12 months (treatment arm 9). No randomization was performed in Part 2 of the study because subjects were assigned to treatment arms according to their age, regardless of infection intensity.
All participants received study treatment either three times on a single day or in a single dose after a meal. The actual doses were based on measured body weight and rounded to the closest folds of 150 mg. In this open-label study, no allocation concealment or blinding was performed regarding participants and investigators. The primary endpoint (i.e. egg counts from fecal samples) was evaluated by laboratory staff without being aware of the actual treatment received by subjects.
Analysis sets were: safety analysis set (all participants who received study treatment), modified intent-to-treat (mITT) set (participants who received study treatment and did not receive anti-malarial medications during the study), and per-protocol (PP) analysis set (all participants with no protocol deviation).
The primary efficacy endpoint was CR, defined as the proportion of participants with absence of S. mansoni parasite eggs in stool demonstrated by the Kato–Katz method 14–21 days after treatment.
Secondary efficacy endpoints were ERR, calculated based on either arithmetic or geometric group mean egg count per gram of stool determined by the Kato–Katz method before treatment and 14–21 days after treatment, and CR, defined as absence of parasite antigens in the urine as assessed by the commercially available point-of-care circulating cathodic antigen (POC-CCA) test for S. mansoni. Safety endpoints were laboratory safety parameters, vital signs, and AEs.
Egg counts in stool were assessed by triplicate Kato-Katz on 2 samples (a total of 6 slides) collected within 5 days, with the first sample collected 14–21 days after treatment. POC-CCA test scores were done using a commercially available POC-CCA cassette at screening and at Days 2, 8, and 14–21 after treatment.
AEs were assessed continuously throughout the study (during the hospital stay and follow-up visits) and included any unfavorable changes reported by the participant or observed by the investigator. In accordance with routine practice for assessment of safety during clinical trials (https://www.ema.europa.eu/en/documents/scientific-guideline/international-conference-harmonisation-technical-requirements-registration-pharmaceuticals-human-use_en-15.pdf), all AEs reported on the same day of study medication – or events that worsened after dosing – were considered treatment-emergent AEs (TEAEs). Regarding severity, investigators rated AEs as mild, moderate, or severe according to standard criteria related to the degree of tolerability/discomfort and impact on functioning. Serious AEs included any untoward medical occurrence that resulted in death, was life-threatening, required inpatient hospitalization or prolonged an existing hospitalization, resulted in persistent or significant disability or incapacity, was a congenital anomaly or birth defect, or was otherwise considered to be medically important. Consideration of causality was based on the investigator’s medical judgement, taking into account available data such as medical history, concomitant medication and conditions, possible worsening of underlying conditions, timing of AE in relation to dosing, and laboratory analysis before and after dosing.
There was no hypothesis testing for the primary endpoint, as this study was intended to determine the dose and formulation to be tested in a subsequent Phase 3 trial. The sample size was based on the minimum number of participants required to reach a meaningful precision (indicated by the lower bound of the 95% confidence interval [CI]) of the primary efficacy endpoint (CR) in each arm. The minimum clinically meaningful CR was considered to be 70% based on literature (12), with the corresponding lower bound of 95% CI greater than 58%. Taking into account the infection intensity stratification factor and assuming approximately 17% dropout rate, the sample size for Part 1 was set at 60 participants per treatment arm, in order to have at least n=50 evaluable participants per arm.
For Part 2, the number of participants envisaged to be enrolled to evaluate efficacy and safety was n=30 for treatment arm 8 (infants aged 13–24 months) and n=10 for treatment arm 9 (infants aged 3–12 months).
All efficacy data were analyzed using descriptive statistics: frequency counts and percentages for qualitative variables, mean, median, quartiles, minimum and maximum values for continuous variables. The calculation of 95% CI for was based on the Clopper-Pearson (exact) method for CR and on resampling for ERR.
The primary analysis for CR was based on the mITT set, with missing follow-up assessment imputed as not cured (mITT with imputation). Sensitivity analyses were performed: 1) excluding mITT participants with missing egg counts (mITT without imputation); and 2) including only PP participants with no imputation. Logistic regression was also performed to determine the impact of baseline characteristics (infection intensity, age group, and sex) and baseline egg counts on CR. No imputation was performed for ERR calculation.
A total of 7906 subjects (5570 children aged 2–6 years; 2336 infants aged 3–24 months) were pre-screened for S. mansoni by POC-CCA urine test. The majority were excluded from further participation because screening results were negative for infection. Some 710 subjects tested positive for S. mansoni by the Kato–Katz method and negative for S. haematobium by the urine filtration method and were invited to the study center for further screening. Of these, 444 subjects met the inclusion/exclusion criteria and were subsequently enrolled, randomized, and treated (safety analysis set), as described below. The reasons for 266 patients not to be enrolled were that they met one or more exclusion criteria (n=124), withdrew consent (n=76), study recruitment had finished before they could be randomized (n=49), or contact was lost between pre-screening and screening (n=17).
In Part 1 (Figure 1), the safety analysis set comprised 420 children aged 2–6 years (60 subjects per treatment arm): treatment arm 1 (rac-PZQ 3x20 mg), treatment arm 2 (rac-PZQ 40 mg/kg single dose), treatment arm 3 (rac-PZQ ODT 40 mg/kg single dose), treatment arm 4 (rac-PZQ ODT 60 mg/kg single dose), treatment arm 5 (L-PZQ ODT 30 mg/kg single dose), treatment arm 6 (L-PZQ ODT 45 mg/kg single dose), and treatment arm 7 (L-PZQ ODT 60 mg/kg single dose). Of these, 18 participants were excluded from the mITT analysis because they were receiving anti-malarial medication (n=16) or S. mansoni infection was not confirmed (n=2). The mITT population for efficacy analysis therefore comprised 402 patients. In Part 2 (Figure 1), the safety analysis set comprised 24 infants aged 6–24 months who were enrolled and treated with L-PZQ ODT 50 mg/kg (treatment arms 8 and 9). After excluding participants receiving anti-malarial medication (n=5), 19 were included in the mITT analysis set (Figure 1). Baseline demographics and disease characteristics are presented for all treatment arms in Table 1. All participants were Black; 53.8% were male; and aged 0.5–6.9 years.
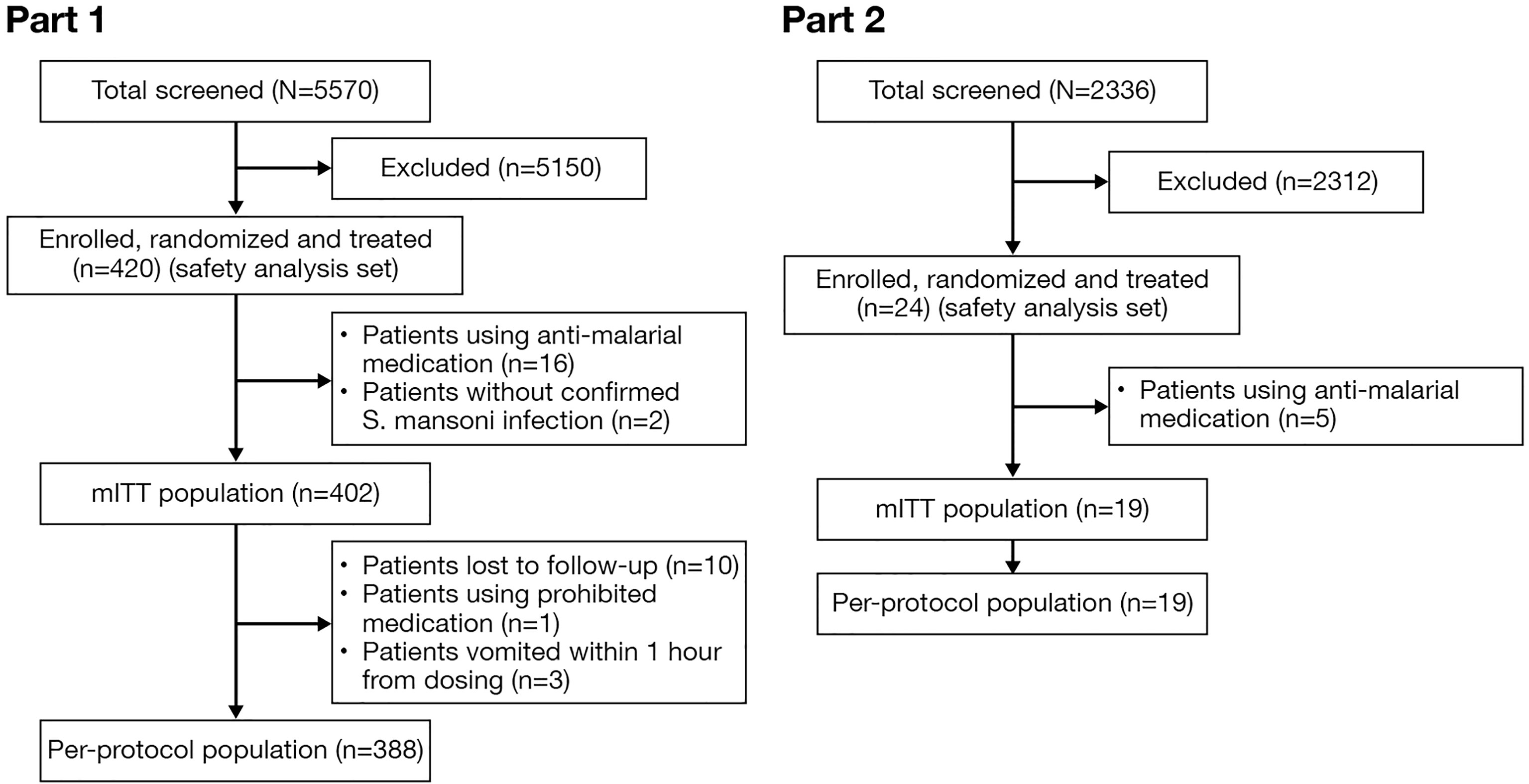
Figure 1 Participant disposition (CONSORT diagram). mITT, modified intent-to-treat.
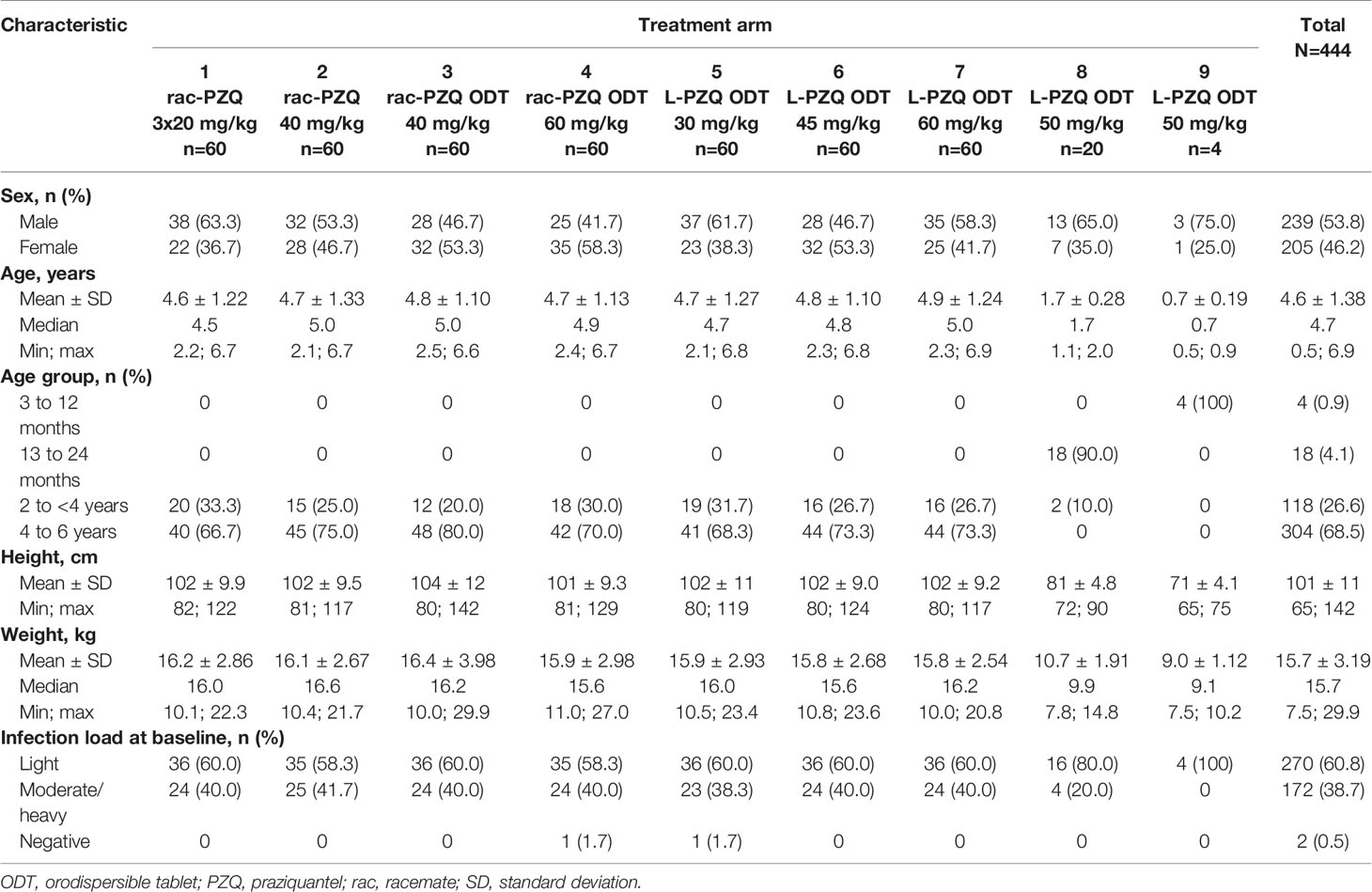
Table 1 Baseline demographics and disease characteristics (safety analysis set).
Concomitant medical events were reported for 28.6% of study participants at baseline; in 76 participants (17.1%) the events were ongoing at the time of study start. Most frequently reported events were infections and infestations (9.7%), gastrointestinal disorders (8.1%), blood and lymphatic system disorders (7.4%), and skin and subcutaneous tissue disorders (5.0%).
A total of 214 (50.8%) study participants used concomitant medication (Supplementary Table 1).
Mean baseline egg counts were 197–434 per gram of stool in treatment arms 1–7, 80 per gram of stool in treatment arm 8, and 43 per gram of stool in treatment arm 9 (Table 2); 60.8% of participants in Part 1 had light infection at baseline.

Table 2 Baseline egg counts (eggs per gram of stool) measured by the Kato–Katz method (modified intent-to-treat analysis set).
Clinically meaningful CRs (≥70%) were achieved in all treatment arms (Figure 2). In Part 1, the highest CRs (approaching 90%) were observed in participants receiving L-PZQ ODT 60 mg/kg (treatment arm 7; CR=89.7%), commercially available rac-PZQ 3x20 mg/kg (treatment arm 1; CR=89.5%), and L-PZQ ODT 45 mg/kg (treatment arm 6; CR=86.0%). In Part 2, treatment with L-PZQ ODT 50 mg/kg resulted in a CR of 93.3% in treatment arm 8 and 100% in treatment arm 9. Similar trends were obtained from the sensitivity analysis (data not shown).
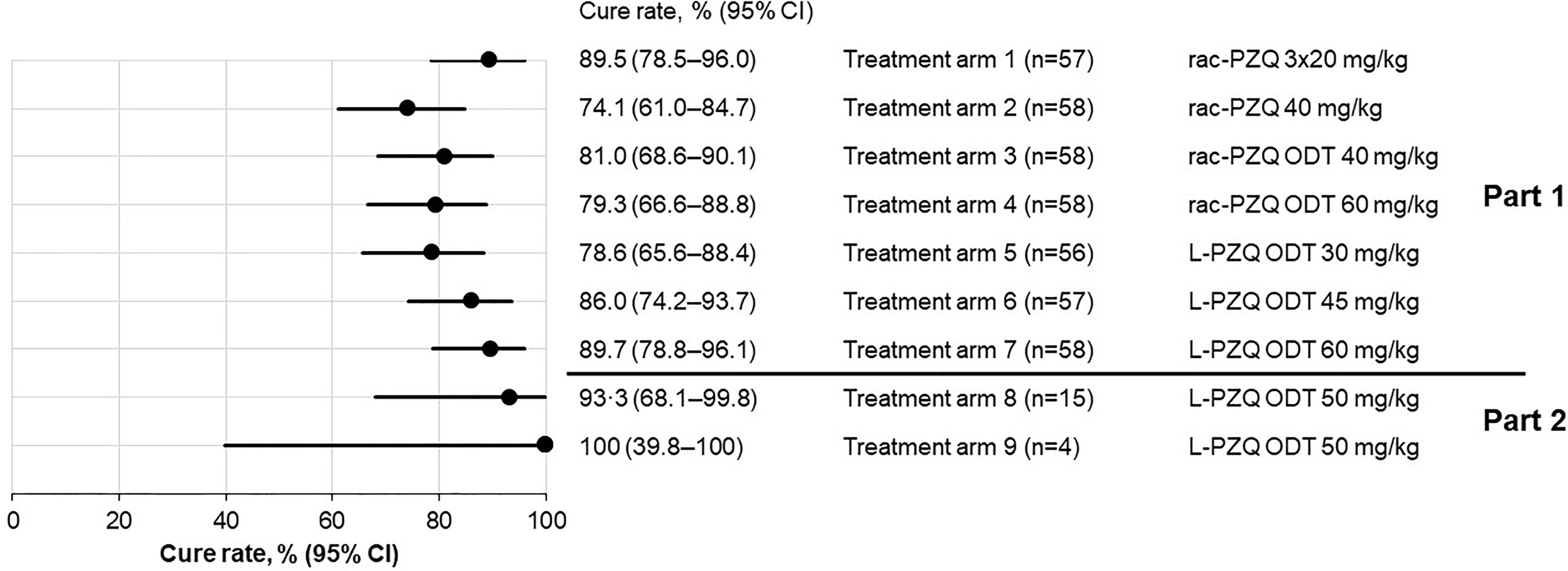
Figure 2 Overall clinical cure rate by the Kato–Katz Method (modified intent-to-treat analysis set, with imputation). Participants with missing follow-up egg counts were imputed as not cured. CI, confidence interval; ODT, orodispersible tablet; PZQ, praziquantel; rac, racemate.
In the logistic regression analysis of the primary endpoint, infection intensity was the only covariate significantly associated with CR. Participants with light infections had higher cure rates than those with moderate/heavy infections in all treatment arms; CRs for light infections were between 82.9% and 100%, and for moderate/heavy infections between 56.5% and 85.7% across treatment arms (Table 3). Among participants with moderate/heavy infections, the CRs were 69.6%, 72.7%, and 82.6% for the 30 mg/kg, 45 mg/kg, and 60 mg/kg L-PZQ ODT dosing groups, respectively, and 78.3% and 69.6% for the 40 mg/kg and 60 mg/kg rac-PZQ ODT dosing groups, respectively.

Table 3 Clinical cure rate by the Kato–Katz method (modified intent-to-treat analysis set).
Both ERRs based on arithmetic mean and geometric means were >95% in all treatment arms (Table 4).
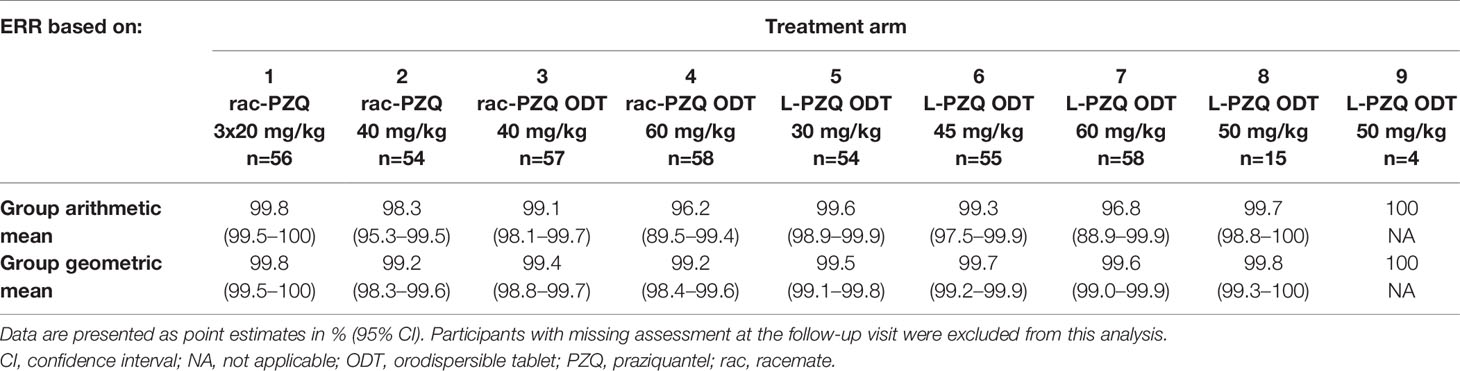
Table 4 Egg reduction rate (modified intent-to-treat analysis set, without imputation).
CRs assessed by POC-CCA on Day 14–21 were lower than those assessed by the Kato–Katz method and ranged from 36.2% to 72.4%; the highest CRs were observed for the L-PZQ ODT 45 mg/kg and 60 mg/kg treatment arms (Supplementary Table 2).
A total of 286 (64.4%) study participants experienced at least one TEAE; of these, TEAEs were considered related to study treatment in 71 (16.0%) study participants (Table 5). No deaths or discontinuation due to TEAEs were reported. Almost all TEAEs that occurred at the time of treatment were mild and resolved within 2 days after dosing. There were two serious TEAEs, both were events of increased transaminases. One of these, occurring in a study participant who received rac-PZQ ODT 40 mg/kg, was considered by the investigator to be related to study treatment. Nine severe adverse events, all related to laboratory abnormalities, were reported: increased C-reactive protein (n=3), leukocyturia (n=3), increased transaminases (n=2), and thrombocytopenia (n=1). All such events were considered to be related to underlying concomitant diseases.
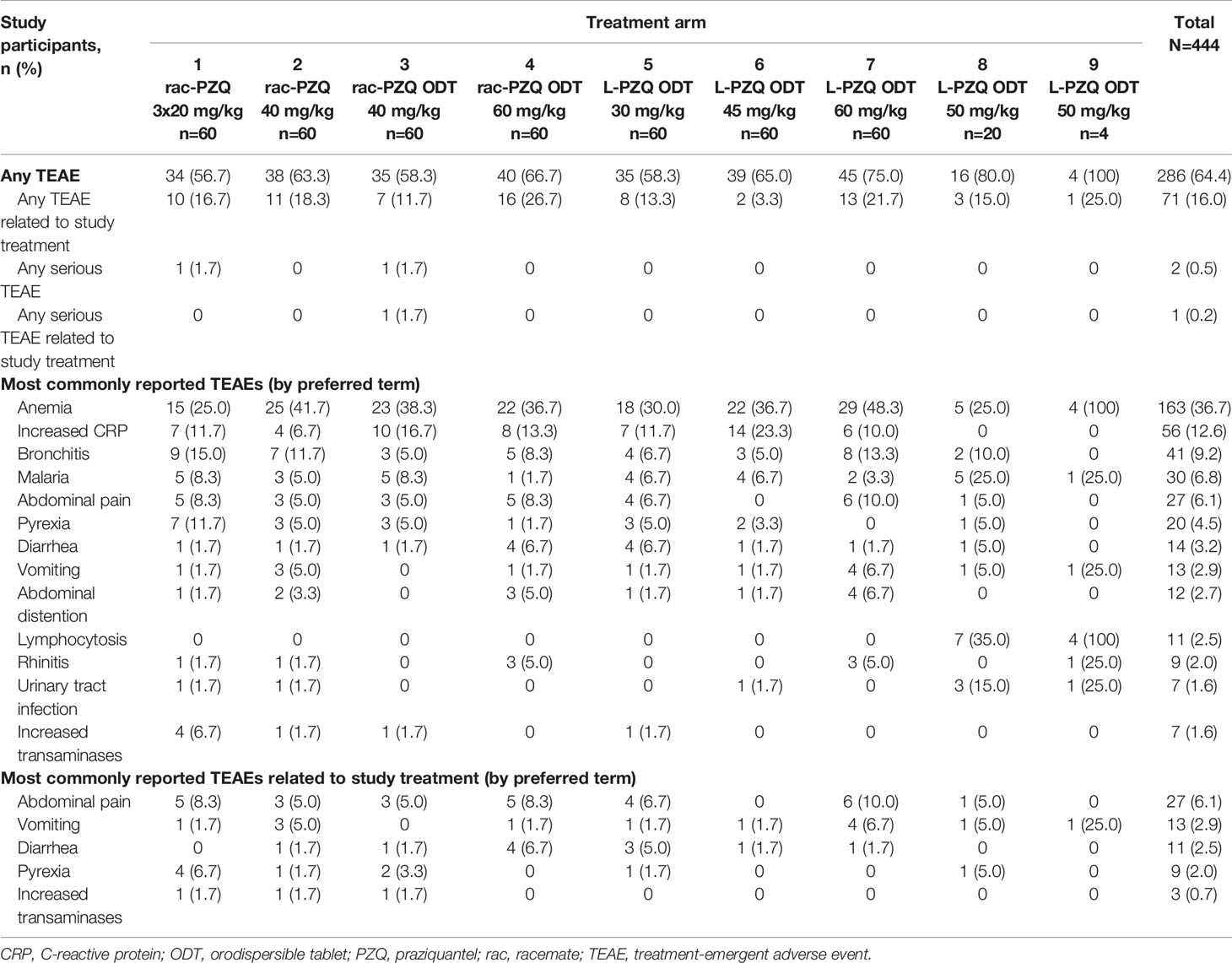
Table 5 Treatment-emergent adverse events (safety analysis set).
This was the first study assessing the efficacy and safety of novel pediatric oral formulations of rac-PZQ and L-PZQ in preschool-age children and infants infected with S. mansoni. The primary objective of Part 1 was met: clinically meaningful CRs (≥70%) were achieved in all treatment arms. In children aged 2–6 years, a single dose of L-PZQ ODT 45 mg/kg was found to have the best benefit–risk profile with a clinically meaningful CR of 86.0%. L-PZQ ODT at 50 mg/kg, recommended by SMC for Part 2, showed acceptable efficacy and safety in enrolled infants aged 6–24 months. The CRs in this study were slightly higher than those reported previously in studies using commercial rac-PZQ formulation in school-age and preschool-age children (12–14).
CRs assessed by the POC-CCA method showed a similar trend, but were generally lower than those assessed by the Kato–Katz method in detecting S. mansoni infection (15). This is in line with previous publications that showed that POC-CCA has higher sensitivity than the Kato–Katz method, especially in light infection (16). Efficacy analyses performed on the mITT analysis set with imputation (when participants with missing post-treatment assessment were defined as not cured) and without imputation, and on the PP analysis set, reached similar conclusions. ERRs were >95% across all treatment arms, suggesting acceptable efficacy of the novel pediatric ODT formulations of PZQ.
In line with previous results obtained for rac-PZQ, our results suggest that rac-PZQ ODT and L-PZQ ODT are more potent in clearing light than heavy infection with S. mansoni (12, 13, 17). However, due to the small sample size in the subgroup of patients with moderate/heavy infections in this study, further studies are needed to determine whether a higher dose of rac-PZQ ODT or L-PZQ should be used in individuals with heavy infection.
The safety profiles of all tested formulations were generally similar to the previously described safety profile of rac-PZQ (18), and no new safety concerns were identified in the pediatric population investigated in this study. TEAEs were mostly mild and transient, and no TEAEs led to death, discontinuations or withdrawal, indicating that the treatment had an acceptable tolerability profile. The high incidence of anemia recorded in the study has previously been noted in association with malaria and schistosomiasis in Africa and may be common in individuals suffering from S. mansoni infection (17, 19). TEAEs related to abnormal laboratory findings, such as anemia, were detected on samples taken before the administration of study treatment, albeit on the same day, and may therefore reflect the baseline underlying disease status of participants.
Studies of infection prevalence in preschool-age children induced an extension of preventive chemotherapy campaigns against schistosomiasis to preschool-age children (20–22); however, studies using crushed commercially available rac-PZQ tablets noted a lower efficacy in this population compared with school-age children (13, 14). Lower CRs may be explained by imprecise dosing of crushed tablets and/or by different bioavailability of rac-PZQ in children versus adults (23, 24). A recent study using a syrup-based pediatric formulation of rac-PZQ showed a much lower efficacy against S. mansoni than against S. haematobium in preschool-age children (25). Our study thus reports the first successful use of novel ODT pediatric formulations of PZQ in Sub-Saharan Africa, with acceptable efficacy and safety.
This study had several limitations. First, children with S. haematobium infection were excluded from the study; consequently, the efficacy of pediatric ODT formulations of PZQ against this species and against mixed S. mansoni/S. haematobium infections remains to be determined. Second, while the study protocol allowed for patients aged 3–24 months to be screened for inclusion in Part 2, the youngest patient enrolled and treated was aged 6 months. Third, the efficacy results obtained for L-PZQ ODT suggest a dose-dependent response; however, the study was not powered for dose–response analysis. These limitations will be addressed in future studies, which will gain further insights concerning the efficacy of the new ODT formulations of PZQ.
The regions of Man and Biankouman of Côte d’Ivoire were selected as representative regions with high incidence of S. mansoni infections, where treatment programs can be expanded in a real-world setting (10, 26). During study conduct, investigators met with a number of challenges related to local community, cultural, ethical, and economic aspects (26). The successful completion of the study set an example of an effective collaboration of multiple stakeholders in pediatric clinical research in sub-Saharan Africa.
This Phase 2 study demonstrated acceptable efficacy and safety of new pediatric ODT formulations of rac-PZQ and L-PZQ against S. mansoni infection in preschool-age children; treatment with L-PZQ ODT 50 mg/kg also resulted in CRs >90% in infants. The promising profile of the new ODT formulations supports further clinical development for treatment of schistosomiasis in preschool-age children and infants from high-risk regions.
Any requests for data by qualified scientific and medical researchers for legitimate research purposes will be subject to Merck Data Sharing Policy. All requests should be submitted in writing to Merck’s data sharing portal https://www.merckgroup.com/en/research/our-approach-to-research-and-development/healthcare/clinical-trials/commitment-responsible-data-sharing.html. When Merck has a co-research, co-development, or co-marketing or co-promotion agreement, or when the product has been out-licensed, the responsibility for disclosure might be dependent on the agreement between parties. Under these circumstances, Merck will endeavour to gain agreement to share data in response to requests.
Written informed consent was obtained from one of the participant’s parents, legal representatives, or guardians prior to any study-related procedure. In addition to parental consent, children aged >3 years and capable of assenting provided oral assent, which was recorded on the informed consent form. The study was conducted in compliance with guidelines on Good Clinical Practice and ethical principles of the Declaration of Helsinki. Study protocol and associated documents were reviewed and approved by the Independent Ethics Committees/Institutional Review Boards in Switzerland (Ethikkommission Nordwest- und Zentralschweiz [EKNZ] Req-2016-098) and in Côte d’Ivoire (Comité National d’Ethique de Recherche [CNER] approval 039/MSHP/CNER). Study protocol and associated documents were submitted to Côte d’Ivoire Health Authorities in accordance with all national regulations and requirements.
EN’G, ÖY, EK-L, AT, EH, NADA, MO, and WB designed the study. EN’G, DB, WB, EH, NADA, and MO supervised clinical patient management and ensured quality data collection. BH and XY analyzed the data. All authors contributed to data interpretation, participated in critical revisions of the manuscript and read and approved the final submitted version of the manuscript.
This study was sponsored by Merck (CrossRef Funder ID: 10.13039/100009945) and the Global Health Innovative Technology Fund (Grant nos. 2013-212, 2014-206 and 2016-110).
EN’G, EH, NADA, and MO report grants from the Global Health Innovative Technology Fund (GHIT) and the European and Developing Countries Clinical Trials Partnership (EDCTP). OY and AT are employees of Merck KGaA, Darmstadt, Germany. EK-L is an employee of Ares Trading S.A., Eysins, Switzerland, an affiliate of Merck KGaA, Darmstadt, Germany. BH and XY are employees of EMD Serono Research & Development Institute, Inc., Billerica, MA, United States, an affiliate of Merck KGaA, Darmstadt, Germany. DB is an employee of Merck (Pty) Ltd, Modderfontein, South Africa, an affiliate of Merck KGaA, Darmstadt, Germany. WB is an employee of Merck Institute of Pharmacometrics, Lausanne, Switzerland, an affiliate of Merck KGaA, Darmstadt, Germany. The authors declare that this study received funding from Merck. The funder had the following involvement with the study: Merck provided the study drug and worked with investigators on the trial design and plan, collection and analyses of data, and interpretation of results. Merck also provided funding for a professional medical writer (as noted in the acknowledgements), who had access to the data. All authors are members or affiliates of Pediatric Praziquantel Consortium that receives funding from Merck KGaA, Darmstadt, Germany. In addition, in 2012 the Consortium received grant support from the Bill and Melinda Gates Foundation (BMGF; Grant no. OPP1063223; www.gatesfoundation.org), from the GHIT Fund (Grant nos. 2013-212, 2014-206, 2018-210) and the EDCTP (Grant no. RIA2016S-1641).
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We acknowledge the support given from the Consortium partners in making this work possible, the funders Merck and the Global Health Innovative Technology Fund for financial assistance, the Man district council for allowing investigators to conduct the study, and lastly children and parents for their participation. Statistical analysis support was provided by Triclinium Clinical Development, Centurion, South Africa. Editorial support was provided by Olga Ucar, Clair Clowes, and Steve Winter of in Science Communications, Springer Healthcare Ltd, UK, and was funded by Merck Healthcare KGaA, Darmstadt, Germany.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fitd.2021.679373/full#supplementary-material
1. World Health Organization. Schistosomiasis Fact Sheet (2019). Available at: https://www.who.int/news-room/fact-sheets/detail/schistosomiasis.
2. World Health Organization. Schistosomiasis. Epidemiological Situation (2018). Available at: https://www.who.int/schistosomiasis/epidemiology/en/.
3. Osakunor DNM, Woolhouse MEJ, Mutapi F. Paediatric Schistosomiasis: What We Know and What We Need to Know. PLoS Negl Trop Dis (2018) 12:e0006144. doi: 10.1371/journal.pntd.0006144
4. World Health Organization. Report of a Meeting to Review the Results of Studies on the Treatment of Schistosomiasis in Preschool-Age Children. Geneva, Switzerland (2011). Available at: https://apps.who.int/iris/handle/10665/44639.
5. World Health Organization. Schistosomiasis and Soil-Transmitted Helminthiases: Number of People Treated in 2016. Wkly Epidemiol Rec (2017) 92:749–60. Available at: https://www.who.int/publications/i/item/who-wer9249.
6. Mduluza T, Mutapi F. Putting the Treatment of Paediatric Schistosomiasis Into Context. Infect Dis Poverty (2017) 6:85. doi: 10.1186/s40249-017-0300-8
7. Meyer T, Sekljic H, Fuchs S, Bothe H, Schollmeyer D, Miculka C. Taste, a New Incentive to Switch to (R)-Praziquantel in Schistosomiasis Treatment. PLoS Negl Trop Dis (2009) 3:3–7. doi: 10.1371/journal.pntd.0000357
8. Reinhard-Rupp J, Klohe K. Developing a Comprehensive Response for Treatment of Children Under 6 Years of Age With Schistosomiasis: Research and Development of a Pediatric Formulation of Praziquantel. Infect Dis Poverty (2017) 6:122. doi: 10.1186/s40249-017-0336-9
9. Mahende MK, Huber E, Kourany-Lefoll E, Ali A, Hayward B, Bezuidenhout D, et al. Comparative Palatability of Orally Disintegrating Tablets (ODTs) of Praziquantel (L-PZQ and Rac-PZQ) Versus Current PZQ Tablet in African Children: A Randomized, Single-Blind, Crossover Study. PLoS Negl Trop Dis (2021) 15:e0007370.
10. Assare RK, Hurlimann E, Ouattara M, N'Guessan NA, Tian-Bi YN, Yapi A, et al. Sustaining the Control of Schistosoma Mansoni in Western Cote D'ivoire: Baseline Findings Before the Implementation of a Randomized Trial. Am J Trop Med Hyg (2016) 94:352–60. doi: 10.4269/ajtmh.15-0530
11. Montresor A, Crompton DWT, Gyorkos TW, Savioli L, World Health Organization. Helminth Control in School-Age Children: A Guide for Managers of Control Programmes. Geneva: World Health Organization (2002).
12. Zwang J, Olliaro PL. Clinical Efficacy and Tolerability of Praziquantel for Intestinal and Urinary Schistosomiasis: A Meta-Analysis of Comparative and Non-Comparative Clinical Trials. PLoS Negl Trop Dis (2014) 8:e3286. doi: 10.1371/journal.pntd.0003286
13. Kabuyaya M, Chimbari MJ, Mukaratirwa S. Efficacy of Praziquantel Treatment Regimens in Pre-School and School Aged Children Infected With Schistosomiasis in Sub-Saharan Africa: A Systematic Review. Infect Dis Poverty (2018) 7:73. doi: 10.1186/s40249-018-0448-x
14. Coulibaly JT, Panic G, Silue KD, Kovac J, Hattendorf J, Keiser J. Efficacy and Safety of Praziquantel in Preschool-Aged and School-Aged Children Infected With Schistosoma Mansoni: A Randomised Controlled, Parallel-Group, Dose-Ranging, Phase 2 Trial. Lancet Glob Health (2017) 5:e688–98. doi: 10.1016/S2214-109X(17)30187-0
15. Yin X, N’Goran EK, Ouattara M, Aka NAD, Diakite NR, Bassa FK, et al. Comparison of POC-CCA With Kato-Katz in Diagnosing Schistosoma Mansoni Infection in a Pediatric L-Praziquantel Clinical Trial. Front Trop Dis (2021) 2:686288. doi: 10.3389/fitd.2021.686288
16. Barenbold O, Garba A, Colley DG, Fleming FM, Haggag AA, Ramzy RMR, et al. Translating Preventive Chemotherapy Prevalence Thresholds for Schistosoma Mansoni From the Kato-Katz Technique Into the Point-of-Care Circulating Cathodic Antigen Diagnostic Test. PLoS Negl Trop Dis (2018) 12:e0006941. doi: 10.1371/journal.pntd.0006941
17. Butler SE, Muok EM, Montgomery SP, Odhiambo K, Mwinzi PM, Secor WE, et al. Mechanism of Anemia in Schistosoma Mansoni-Infected School Children in Western Kenya. Am J Trop Med Hyg (2012) 87:862–7. doi: 10.4269/ajtmh.2012.12-0248
18. Olliaro PL, Coulibaly JT, Garba A, Halleux C, Keiser J, King CH, et al. Efficacy and Safety of Single-Dose 40 Mg/Kg Oral Praziquantel in the Treatment of Schistosomiasis in Preschool-Age Versus School-Age Children: An Individual Participant Data Meta-Analysis. PLoS Negl Trop Dis (2020) 146:e0008277. doi: 10.1371/journal.pntd.0008277
19. Gasim GI, Adam I. Malaria, Schistosomiasis, and Related Anemia. In: Erkekoglu P, editor. Nutritional Deficiency. InTech Open. (2016) doi: 10.5772/63396
20. Coulibaly JT, N'Gbesso YK, N'Guessan NA, Winkler MS, Utzinger J, N'Goran EK. Epidemiology of Schistosomiasis in Two High-Risk Communities of South Cote d'Ivoire With Particular Emphasis on Pre-School-Aged Children. Am J Trop Med Hyg (2013) 89:32–41. doi: 10.4269/ajtmh.12-0346
21. Nalugwa A, Olsen A, Tukahebwa ME, Nuwaha F. Intestinal Schistosomiasis Among Preschool Children Along the Shores of Lake Victoria in Uganda. Acta Trop (2015) 142:115–21. doi: 10.1016/j.actatropica.2014.11.014
22. Ruganuza DM, Mazigo HD, Waihenya R, Morona D, Mkoji GM. Schistosoma Mansoni Among Pre-School Children in Musozi Village, Ukerewe Island, North-Western-Tanzania: Prevalence and Associated Risk Factors. Parasit Vectors (2015) 8:377. doi: 10.1186/s13071-015-0997-9
23. Keiser J, Ingram K, Utzinger J. Antiparasitic Drugs for Paediatrics: Systematic Review, Formulations, Pharmacokinetics, Safety, Efficacy and Implications for Control. Parasitology (2011) 138:1620–32. doi: 10.1017/S0031182011000023
24. Fernandez E, Perez R, Hernandez A, Tejada P, Arteta M, Ramos JT. Factors and Mechanisms for Pharmacokinetic Differences Between Pediatric Population and Adults. Pharmaceutics (2011) 3:53–72. doi: 10.3390/pharmaceutics3010053
25. Garba A, Lamine MS, Djibo A, Tahirou A, Aouami MA, Alfari A, et al. Safety and Efficacy of Praziquantel Syrup (Epiquantel) Against Schistosoma Haematobium and Schistosoma Mansoni in Preschool-Aged Children in Niger. Acta Trop (2013) 128:318–25. doi: 10.1016/j.actatropica.2012.12.003
26. N'Goran E, David Aka NA, Ouattara M, Huber E, Bezuidenhout D, Kourany-Lefoll E, et al. Challenges and Lessons From Conducting a Paediatric Clinical Trial in Sub-Saharan Africa: The Case of the Praziquantel Oral Dispersible Tablets Phase II Study in Cote D'ivoire. Adv Parasitol (2019) 103:75–89. doi: 10.1016/bs.apar.2018.09.002
Keywords: schistosomiasis, Schistosoma mansoni, clinical trial, praziquantel, pediatric
Citation: N’Goran EK, Yalkinoglu Ö, Kourany-Lefoll E, Tappert A, Hayward B, Yin X, Bezuidenhout D, Huber E, Aka NAD, Ouattara M and Bagchus W (2021) Efficacy and Safety of New Orodispersible Tablet Formulations of Praziquantel (Racemate and L-Praziquantel) in Schistosoma mansoni-Infected Preschool-Age Children and Infants: A Randomized Dose-Finding Phase 2 Study. Front. Trop. Dis 2:679373. doi: 10.3389/fitd.2021.679373
Received: 30 April 2021; Accepted: 17 September 2021;
Published: 12 October 2021.
Edited by:
Amaya L. Bustinduy, University of London, United KingdomReviewed by:
G. Butrous, University of Kent, United KingdomCopyright © 2021 N’Goran, Yalkinoglu, Kourany-Lefoll, Tappert, Hayward, Yin, Bezuidenhout, Huber, Aka, Ouattara and Bagchus. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wilhelmina Bagchus, d2lsaGVsbWluYS5iYWdjaHVzQG1lcmNrZ3JvdXAuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.