 Jean Kwun
Jean Kwun Joseph M. Ladowski
Joseph M. Ladowski Annette M. Jackson
Annette M. Jackson Stuart Knechtle
Stuart Knechtle
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Transplant., 28 March 2025
Sec. Immunosuppression
Volume 4 - 2025 | https://doi.org/10.3389/frtra.2025.1559512
This article is part of the Research TopicDecedent Model vs Primate Model - Do We Know Enough?View all 3 articles
For decades xenotransplantation, the use of genetically modified pigs as organ donors, has held promise as a potential solution to the organ shortage. However, the field has recently experienced a resurgence and in the last two years witnessed several novel medical innovations—highlighted by two cases of clinical human cardiac xenografts and xenotransplantation in brain-dead human recipients (decedent model) (1–3). Undoubtedly, the success in extending xenograft survival in non-human primates (NHPs) fostered this translation. Progress in the NHP model is attributed to (1) additional genetic modifications of pig donors (4) and (2) availability of agents targeting the anti-CD40/CD154 signaling pathway (5–7). Despite the significant progress, there remains debate in the field regarding the ideal clinical pig: the inclusion of human complement regulatory proteins, anti-inflammatory proteins, and additional genetic mutations of glycans and SLAs. Still, consensus remains that the clinical pig genetic background should possess nullifying-mutations in the three enzymes responsible for creation of the three known xenoantigens (i.e., a TKO pig) (8).
Recent outcomes with this genetically edited pig donor have demonstrated impressively prolonged kidney graft survival, lasting up to 2 years (9). A pig with a similar level of genetic modification served as the heart donor for the historical first pig-to-human clinical xenotransplantation performed in 2022, resulting in 61-day patient survival (1). It is important to note that this transplant was not performed as part of a clinical trial, but rather through an emergency use of an investigational drug (eIND) for a recipient with no other medical life-prolonging options. However, this approval did not exclude donor animals that are not designated pathogen-free. Clearly, the federal regulatory officials viewed it as non-prohibitory and granted an additional eIND in September 2023. Subsequently, the second clinical cardiac xenotransplantation took place in September 2023 and resulted in a survival benefit of 40 days. Both experts and the general public accepted these outcomes as successful achievements but also highlight that the optimal pig genotype and immunosuppression regimen have not yet been identified. Given the regulatory issues with a clinical xenoheart study, it is likely that other organ systems will be looked to.
The greatest clinical need in solid organ transplantation exists for end-stage renal failure patients, for which over 90,000 await a kidney transplant in the United States alone (10). Allo-kidney transplantation offers significant benefits over dialysis, including improved patient survival and quality of life. However, there is huge gap between organ supply and demand and approximately 40% of patients on the waiting list die within 5 years (11). As suggested for decades, xenotransplantation could be a solution to this issue. Now the question is, are we ready for a large-scale clinical xenotransplant trial for patients with end-stage renal disease? While xenotransplantation presents many significant challenges, including physiological discordance, microbial safety, and regulatory aspects, our focus is on the current issues surrounding xenograft rejection.
The most note-worthy of the recent xenotransplantation efforts is the clinical human cardiac and renal xenograft (1, 12, 13). The two cases of human cardiac xenotransplantation resulted in graft and recipient survival of 61 and 40 days. Additionally, no other option for life-prolonging medical or surgical therapy was available for these patients, and the alternative care pathway would likely have been a transition to comfort measures. The extension of their lives by month or two, with a potential of longer survival, is a commendable effort. Additionally, to evaluate the functionality and immunological response to a xenokidney in a human context, the decedent model has been employed (2, 3). In this model, brain-dead organ donors, deemed ineligible for organ donation due to trauma or physiological considerations, are utilized as recipients for xenokidneys or xenohearts (2, 3). The organs are monitored for signs of rejection and function with encouraging results to date. These studies provide reassurance regarding the low likelihood of immediate graft failure due to hyperacute rejection. However, it is worth noting that studies involving brain-dead individuals do not require approval from the FDA, but rather from local Institutional Review Boards (IRBs). Nevertheless, research involving brain-dead individuals would be encompassed within Clinical Trial Applications to FDA, akin to data obtained from non-clinical studies. Secondly, studies in brain-death individuals could be suboptimal due to injuries to vital organs, changes in hormones, metabolism, hemodynamics, and excessive inflammation, etc. (14). Therefore, the outcome from decedent models could be difficult to interpret and less informative than results of organ transplantation in living recipients.
In the case of clinical xenokidney transplantation, the comparison of outcomes must be against the medical alternative: dialysis. While allotransplantation is a preferable option to dialysis for most patients and associated with prolonged survival, improved quality of life, and decreased financial costs, it is unknown how xenotransplantation will compare to dialysis with respect to outcomes. Unfortunately, the most recent xenotransplantation results in NHPs with a TKO pig possessing human proteins show 40% graft loss due to rejection within 2–3 months (9). Even for patients experiencing a poor quality of life on dialysis, the current outcomes of xenokidney transplantation are not comparable to those of dialysis. However, unlike heart transplantation, xenokidney failure would not likely precipitate patient death as the patient could return to dialysis. Therefore, it will be crucial to discuss with potential candidates in a xenokidney clinical trial the relative risks following xenograft rejection, such as return to dialysis and subsequent allotransplantation. An important consideration is whether xenograft failure results in antibody development and sensitization against human kidneys. Given the significant homology between the pig and human MHC, xenotransplantation may further limit the patient's potential pool of allogeneic donor kidneys. This issue represents another of the points that should be addressed prior to a clinical xenokidney trial.
Anand et al. present favorable outcomes in a pig-to-NHP xenokidney transplantation model employing a TKO pig with additional human proteins under anti-CD154mAb immunosuppression (9). As previously emphasized, the longest graft survival in this study is close to 2 years, with a mean survival time of 241.2 days (Median, 176 days). This achievement stands out significantly when compared to previous NHP xenograft survival rates using a similar donor pig genetic background. Nevertheless, it is imperative to not overlook the outcomes of animals that did not attain long-term graft survival. In the cited study, 40% (6 out of 15 animals) of NHP recipients did not survive past 2 months. The consistent occurrence of early xenograft failures in virtually all nonhuman primate xenotransplantation studies is a matter of concern, often without clearly discernible pathophysiology (15).
In the 1970s, clinical allotransplantation experienced a resurgence due to the discovery and implementation of a powerful immunosuppressive agent—cyclosporine. The addition of cyclosporine to the recipient's immunosuppressive regimen led to improved survival and graft outcomes. Unfortunately, the drawback of any immunosuppression drug is the overimmunosuppression of the recipient immune system and the resulting infections and side-effects. In xenotransplantation, the recognition that CD40/CD154 blockade could prolong xenograft survival led to the efforts to prolong survival with further immunosuppression. To this point, a myriad of agents targeting alternative mechanisms have been tried in xenotransplantation. Not surprisingly, the implemented clinical regimen includes diverse agents targeting many potentially relevant mechanisms, some perhaps redundant. While an aggressive immunosuppressive approach could facilitate long-term xenograft survival in a subset of animals, it concurrently led to a high incidence of infectious complications and recipient euthanasia not directly reported but reflected by highly censored data (15). One example of profound immunosuppression is the repeated use of rituximab to control post-xenotransplantation humoral responses (9, 16). While an excellent proof of concept approach, repeated depletion of B cells may not lend itself to safe human translation in the clinic. Overimmunosuppression puts patients at risk of irreversible infection and death, pertinent to the case of porcine CMV that likely contributed to the patient's demise in the first clinical xenoheart study (Table 1) (1). Other agents targeting more specific immune cell populations involved in the humoral response such as proteasome inhibitors or anti-CD38 mAbs may improve efficacy. However, these agents have not been tested in xenotransplantation yet. Several other pathological features are relevant to xenograft rejection besides AMR, including TMA and interstitial hemorrhage. It is challenging to determine if these features are truly “specific” for xenotransplantation, as we can observe similar injury patterns in other settings such as ABO mismatch in allotransplantation. Additionally, these features may occur secondary to AMR. Consequently, it remains unclear whether these factors alone are sufficient to reject the graft independently of AMR.
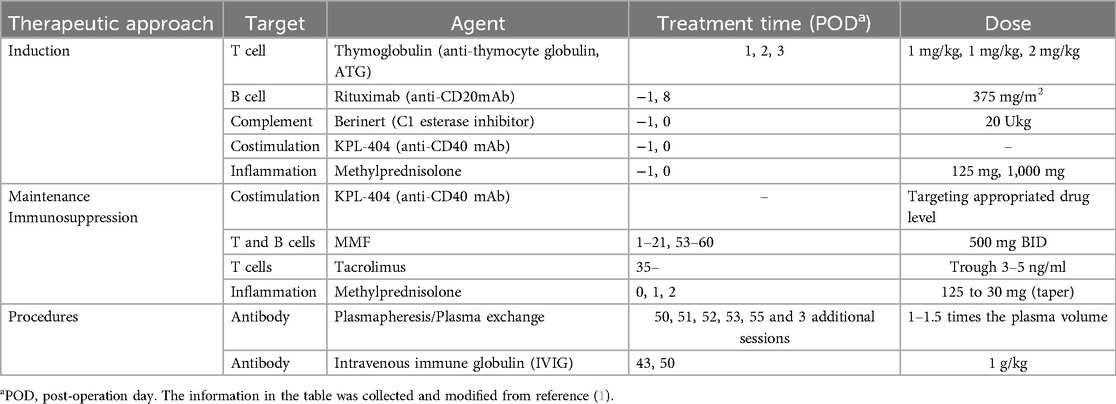
Table 1. The list of immunosuppressive agents used in the first human cardiac xenotransplantation.
Improvements in human allotransplant survival mirrored advancements in histocompatibility testing to assess immunologic risk and monitor de novo donor specific antibody development. Cellular flow cytometry crossmatch data has been generated in NHP studies, but thresholds correlated with early rejection phenotypes (such as antibody-mediated rejection and thrombotic microangiopathy) have not been establishment. Additionally, thorough investigations to determine the specificity of human preformed anti-pig antibodies across different xenotransplant models have not been reported. Current clinical histocompatibility thresholds in allotransplantation stratify patients according to immunological risk and inform clinical decision-making surrounding the need for induction therapy and baseline immunosuppression levels. Establishing appropriate recipient/pig-donor pairs in conjunction with optimal immunosuppression regimens in human xenotransplant trials will require adequate histocompatibility tools and thresholds.
The xenotransplantation field has achieved commendable success through the utilization of the NHP model. Studies to date serve as a proof-of-concept, demonstrating that pig-to-NHP or human transplantation can be achieved without hyperacute rejection and providing insights regarding the human immune response to a xenograft. However, the field must now transition into an optimization phase before larger human clinical trials can be initiated. To accomplish this, more mechanism-driven studies of rejection in xenotransplant models are imperative, with a focus on investigating therapeutics to target these pathways in combination with new or currently used genetically modified donor organs and appropriate histocompatibility testing.
A prominent surgical educator of the 20th century, Dr. David Sabiston, warned his trainees against holding back surgical innovation by making rash pronouncements. This advice seems wise, and while we hold the opinions expressed above regarding the current immunologic risks of xenotransplantation, no one would be more delighted to see successful clinical implementation of xenotransplantation than us. In fact, we are working hard to evaluate and improve immunosuppression to permit safe and successful xenotransplantation. It is our humble suggestion that the group that leads the first clinical xenotransplant trial should possess the following: (1) a rigorously defined pig genome including information regarding off-target integration of any transgenes (2) a FDA-approved or clinically acceptable regimen that routinely leads to long-term xenograft survival (3) sufficient pre- and post-xenotransplant assays that replicate those utilized in clinical allotransplantation to monitor the immunologic and infectious status of the recipient and (4) consistent success in a preclinical model with a mechanistic explanation for outliers or early rejections. We expect that progress in the field may open the door to consistent long-term survival of xenografts.
It is indeed an exciting era for xenotransplantation. While the manuscript was under preparation and review, three xenokidney transplantations have been approved by FDA (compassionate use) and conducted during the processing this manuscript (17–19). So far, a total of six pig-to-human clinical xenotransplantation cases have been reported from 2022 to 2025, with an average patient age of 56.8 years (four males and two females) (Table 2). Similar to findings in nonhuman primate (NHP) models, some patients have experienced early xenograft rejection or complications (mean graft survival less than 2 months), while two patients remain ongoing with functioning graft, including one with the longest xenograft survival (∼3 months post-transplantation). Detailed information on the first three cases is now available in academic publications (1, 12, 13) while latter three cases are not available yet.

Table 2. The list of clinical xenotransplantation cases.
As of February 2025, the U.S. FDA has approved two clinical trials for genetically engineered pig kidney transplantation into humans. The first trial, led by Massachusetts General Hospital (MGH) with eGenesis, involves up to three patients with end-stage kidney disease. The initial transplant in this series was already initiated (Case#6 in Table 2). The second trial, sponsored by United Therapeutics, has received FDA approval to transplant genetically modified pig kidneys into up to 50 patients. This large-scale study aims to evaluate the safety and efficacy of xenokidney transplantation as a solution to the organ shortage crisis. The progression, timing, and phenotype of rejection of these patients will provide the field with significant directions to pursue further advancements.
JK: Conceptualization, Writing – original draft, Writing – review & editing. JL: Writing – original draft, Writing – review & editing. AJ: Writing – original draft, Writing – review & editing. SK: Writing – original draft, Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the National Institute of Allergy and Infectious Diseases of the National Institutes of Health under R01AI175411 (awarded to J.K.), NIH R38AI140297 (awarded to J.M.L.), NIH F32AI174651 (awarded to J.M.L.), and the American Society of Transplant Surgeons Jon Fryer Resident Research Scholarship (awarded to J.M.L.). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Griffith BP, Goerlich CE, Singh AK, Rothblatt M, Lau CL, Shah A, et al. Genetically modified porcine-to-human cardiac xenotransplantation. N Engl J Med. (2022) 387:35–44. doi: 10.1056/NEJMoa2201422
2. Montgomery RA, Stern JM, Lonze BE, Tatapudi VS, Mangiola M, Wu M, et al. Results of two cases of pig-to-human kidney xenotransplantation. N Engl J Med. (2022) 386:1889–98. doi: 10.1056/NEJMoa2120238
3. Porrett PM, Orandi BJ, Kumar V, Houp J, Anderson D, Cozette Killian A, et al. First clinical-grade porcine kidney xenotransplant using a human decedent model. Am J Transplant. (2022) 22:1037–53. doi: 10.1111/ajt.16930
4. Lai L, Kolber-Simonds D, Park K-W, Cheong H-T, Greenstein JL, Im G-S, et al. Production of alpha-1,3-galactosyltransferase knockout pigs by nuclear transfer cloning. Science. (2002) 295:1089–92. doi: 10.1126/science.1068228
5. Mohiuddin MM, Singh AK, Corcoran PC, Thomas III ML, Clark T, Lewis BG, et al. Chimeric 2C10R4 anti-CD40 antibody therapy is critical for long-term survival of GTKO.hCD46.hTBM pig-to-primate cardiac xenograft. Nat Commun. (2016) 7:11138. doi: 10.1038/ncomms11138
6. Längin M, Mayr T, Reichart B, Michel S, Buchholz S, Guethoff S, et al. Consistent success in life-supporting porcine cardiac xenotransplantation. Nature. (2018) 564:430–3. doi: 10.1038/s41586-018-0765-z
7. Kim SC, Mathews DV, Breeden CP, Higginbotham LB, Ladowski J, Martens G, et al. Long-term survival of pig-to-rhesus macaque renal xenografts is dependent on CD4T cell depletion. Am J Transplant. (2019) 19:2174–85. doi: 10.1111/ajt.15329
8. Yamamoto T, Iwase H, Patel D, Jagdale A, Ayares D, Anderson D, et al. Old world monkeys are less than ideal transplantation models for testing pig organs lacking three carbohydrate antigens (triple-knockout). Sci Rep. (2020) 10:9771. doi: 10.1038/s41598-020-66311-3
9. Anand RP, Layer JV, Heja D, Hirose T, Lassiter G, Firl DJ, et al. Design and testing of a humanized porcine donor for xenotransplantation. Nature. (2023) 622:393–401. doi: 10.1038/s41586-023-06594-4
10. Porrett PM, Locke JE. A roadmap for human trials of xenotransplantation. J Clin Invest. (2022) 132. doi: 10.1172/JCI164484
11. Locke JE, Kumar V, Anderson D, Porrett PM. Normal graft function after pig-to-human kidney Xenotransplant. JAMA Surg. (2023) 158:1106–8. doi: 10.1001/jamasurg.2023.2774
12. Griffith BP, Grazioli A, Singh AK, Tully A, Galindo J, Saharia KK, et al. Transplantation of a genetically modified porcine heart into a live human. Nat Med. (2025) 31(2):589–98. doi: 10.1038/s41591-024-03429-1
13. Kawai T, Williams WW, Elias N, Fishman JA, Crisalli K, Longchamp A, et al. Xenotransplantation of a porcine kidney for End-stage kidney disease. N Engl J Med. (2025). doi: 10.1056/NEJMoa2412747
15. Firl DJ, Markmann JF. Measuring success in pig to non-human-primate renal xenotransplantation: systematic review and comparative outcomes analysis of 1051 life-sustaining NHP renal allo- and xeno-transplants. Am J Transplant. (2022) 22:1527–36. doi: 10.1111/ajt.16994
16. Ma D, Hirose T, Lassiter G, Sasaki H, Rosales I, Coe TM, et al. Kidney transplantation from triple-knockout pigs expressing multiple human proteins in cynomolgus macaques. Am J Transplant. (2022) 22:46–57. doi: 10.1111/ajt.16780
17. Rabin RC. Surgeons transplant pig kidney into a patient, a medical milestone. New York Times. (2024).
18. New Jersey woman receives pig kidney along with mechanical heart pump. The Guardian. (2024). Available at: https://www.theguardian.com/us-news/2024/apr/24/new-jersey-woman-pig-kidney-transplant
Keywords: xenotransplantation, xenotransplantation clinical trials, immunosuppression, nonhuman primate (NHP), pig-to-human transplantation
Citation: Kwun J, Ladowski JM, Jackson AM and Knechtle S (2025) The current issues of translating clinical xenokidney transplantation, with an emphasis on prevention of rejection. Front. Transplant. 4:1559512. doi: 10.3389/frtra.2025.1559512
Received: 12 January 2025; Accepted: 18 March 2025;
Published: 28 March 2025.
Edited by:
Gaurav Gupta, Virginia Commonwealth University, United StatesReviewed by:
Akshay Athreya, Virginia Commonwealth University, United StatesCopyright: © 2025 Kwun, Ladowski, Jackson and Knechtle. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jean Kwun, amVhbi5rd3VuQGR1a2UuZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.