 Lioba Huelsboemer1,†
Lioba Huelsboemer1,† Sam Boroumand1,†
Sam Boroumand1,† Alejandro Kochen1,2,†Alna Dony1,3
Alejandro Kochen1,2,†Alna Dony1,3 Jake Moscarelli1Sacha C. Hauc1Viola A. Stögner1Richard N. Formica4Bohdan Pomahac1,‡
Jake Moscarelli1Sacha C. Hauc1Viola A. Stögner1Richard N. Formica4Bohdan Pomahac1,‡ Martin Kauke-Navarro1*‡
Martin Kauke-Navarro1*‡
- 1Division of Reconstructive and Plastic Surgery, Yale School of Medicine, New Haven, CT, United States
- 2Regenerative Wound Healing Center, Yale School of Medicine, New Haven, CT, United States
- 3School of Medicine, University of Leeds, Leeds, United Kingdom
- 4Department of Medicine, Section of Nephrology and Transplantation, Yale School of Medicine, New Haven, CT, United States
Background: Recipients of Vascularized Composite Allotransplants require effective immunosuppressive therapy to prevent graft rejection. This systematic review summarizes the current body of literature on immunosuppressive regimens used in face and hand transplants while summarizing their outcome in terms of rejection, renal failure, and infections.
Methods: A systematic search of electronic databases was conducted to identify relevant studies from 1998 until July 1st, 2023. We included all studies that discussed immunosuppressive strategies in face and hand transplant recipients according to PRISMA.
Results: The standard triple maintenance therapy was mostly adjusted due to nephrotoxicity or high incidence of rejection. The most common alternative treatments utilized were sirolimus (25/91; 27.5%) or everolimus (9/91; 9.9%) following hand- and photophoresis (7/45; 15.6%), sirolimus (5/45; 11.1%) or belatacept (1/45; 2.2%) following face transplantation. Episodes of rejection were reported in 60 (65.9%) of hand- and 33 (73%) of face transplant patients respectively. Graft loss of 12 (13.2%) hand and 4 (8.9%) face transplants was reported. Clinical CMV infection was observed in 6 (6.6%) hand and 7 (15.5%) face transplant recipients.
Conclusions: Based on the herein presented data, facial grafts exhibited a heightened incidence of rejection episodes and CMV infections. Facial mucosa adds complexity to the immunological graft composition highlighting the need of individualized immunosuppressive regimens and further research.
Introduction
Vascularized Composite Allotransplantation (VCA) is currently the highest available reconstructive option on the reconstructive ladder as it uniquely offers both functional (motor, sensory) and aesthetic reconstruction at the same time. A total of 300 VCAs including 148 upper extremity, 80 uterus, 48 face, 46 abdominal wall, five penis, and two lower extremity transplantations have been performed worldwide (1–5). In contrast, about 25,000 kidney transplantations have been performed in the United States in 2022 alone (6). Major obstacles such as short ischemia time tolerance of muscles and acute and chronic rejection prevent VCA from becoming a more widely utilized reconstructive procedure (7, 8). In contrast to solid organ transplantation (SOT), VCA is not categorized as a life-saving procedure; instead, it is regarded as a life-giving intervention. Therefore, the side effects of long-term immunosuppressive therapy (for example, cancer development and opportunistic infections) have so far been difficult to reconcile with the benefits of VCA. Due to the lack of longer-term follow up and smaller number of patients, the risk-benefit ratios of VCAs has yet to be formally defined. Immunosuppressive (IS) regimens have largely been adopted from SOT. Induction is often done with antithymocyte globulin (T cell depleting drug) or alternatively monoclonal antibodies such as Basiliximab or Alemtuzumab, followed by a triple maintenance therapy of Tacrolimus, Mycophenolate Mofetil (MMF), and steroids (9). Even though the different levels of immunogenicity in skin and kidney are well described (e.g., by Moseley et al.), with skin being more immunogenic than kidneys, VCA IS regimens are largely based on experience in SOT (10). Additionally, research in the field of face transplantation revealed that mucosa might be more immunogenic than skin and may reject at a higher frequency (11–13). These findings could lead to the assumption that VCA and especially face transplant patients must be treated differently as the immunogenicity of skin and mucosa seem to differ from solid organs. New treatment options, improved understanding of the molecular rejection mechanisms in skin and mucosa, and standardized guidelines for VCA are urgently needed to not only reduce toxic long term side effects of immunosuppressants but to also allow more targeted IS in VCA recipients. Current research in animal models mostly focuses on the principle of tolerance induction by directly targeting the recipient's immune system through cellular or pharmaceutical approaches (9, 14, 15). As new therapeutics are not yet available for humans and standardized guidelines are non-existent, this systematic review aims to provide a comprehensive overview of current treatment regimen in humans following VCA to give an update on treatment options worldwide.
Methods
Literature search
We conducted a systematic review of manuscripts listed in PubMed, MEDLINE, and Embase databases following the “preferred reporting items for systematic reviews and meta-analysis” (PRISMA) guidelines. The search strategy included both medical subject headings (MeSH) and directly quoted keywords relating to the following two concepts: VCA and immunosuppression treatments. We assessed outcomes such as graft survival, rejection rates, and complications in face and hand transplant recipients. Subgroup analyses investigated the impact of immunosuppression on face or hand or hand and face transplantation. This search strategy was adapted across each of the databases according to their individual requirements. The full electronic search strategies for each database are shown in the Supplementary Figure S1. We included all studies from inception of each database to the search date of July 1st, 2023. Utilizing a two-step approach, S.B. and A.K. independently examined the results of the search criteria for titles and abstracts. Any discrepancies in study inclusion/exclusion were resolved by a third reviewer (L.H.). Subsequently, both S.B. and A.K. performed full-text review of all included studies.
Study selection criteria
Following query of the search results, manuscripts were automatically excluded (utilizing database result filters) if they did not meet the following criteria: Full-Text availability, Human studies, and English language. After evaluating the remaining abstracts/titles, all editorials, reviews, commentaries, and conference abstracts were additionally excluded leaving primarily original articles and case reports. All remaining manuscripts received full-text evaluation to identify specific elements including: the VCA center responsible for the study, the type of VCA in the study (e.g., hand vs. face), the number of patients included, the immunosuppression regimens utilized, and any noted complications/effects of the immunosuppressive treatments based on systemic categories. Rejection in skin or mucosa (face transplant) or skin (hand transplant) was included if reported as graded >1 according to Banff Classification (T-cell mediated rejection). Clinical CMV infection was defined as serum positive plus clinical symptoms while CMV viremia was defined as isolated DNAemia without evidence of end-organ damage (16). References of included studies were reviewed for additional studies. All data extracted from included studies were independently entered by first author and year of publication into a Microsoft Excel worksheet by two reviewers (S.B. and A.K.) for tabulation and analysis. Disagreements between inputs were resolved by discussion and consensus from a third reviewer (L.H.).
Results
Search outcomes
The search strategy yielded 120 articles that met all inclusion criteria (Figure 1). The articles were published between 1999 and 2023. 47 articles discussed immunosuppressive regimens (Figure 2) for face VCAs, 71 articles pertain to the immunosuppressive regimen of hand VCAs, and two articles pertain to those patients who have received both hand and face VCAs. In total the search strategy captured 45 patients of facial transplantation, 91 cases of hand transplantation, and 3 cases of combined face and hand transplantation. A breakdown of the immunosuppressive treatments and associated complications for each VCA can be identified in Tables 1–3. Associated complications were broken down into the following applicable categories: Rejection, Infectious, Renal, Metabolic, Deaths, Graft Loss, Hematologic, Malignancy, and Other.
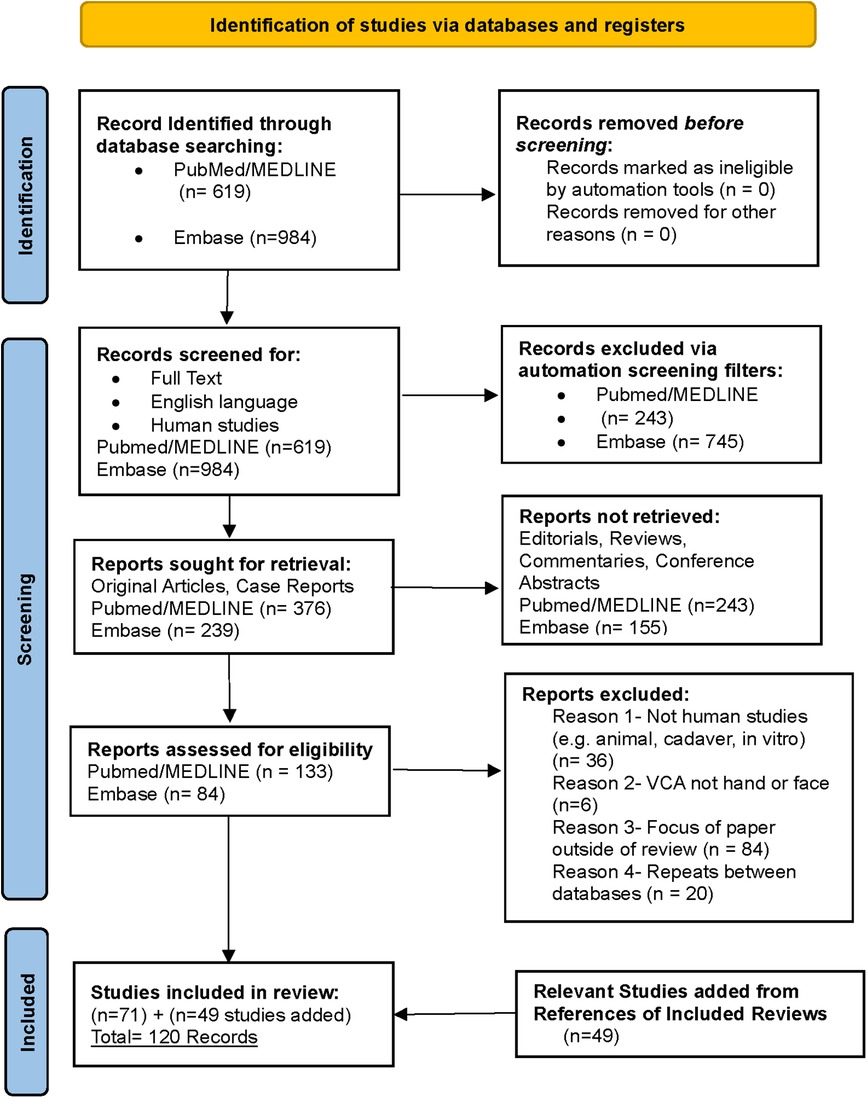
Figure 1. The search strategy according to the PRISMA guidelines yielded 120 articles that met all inclusion criteria. (Adapted from (17).
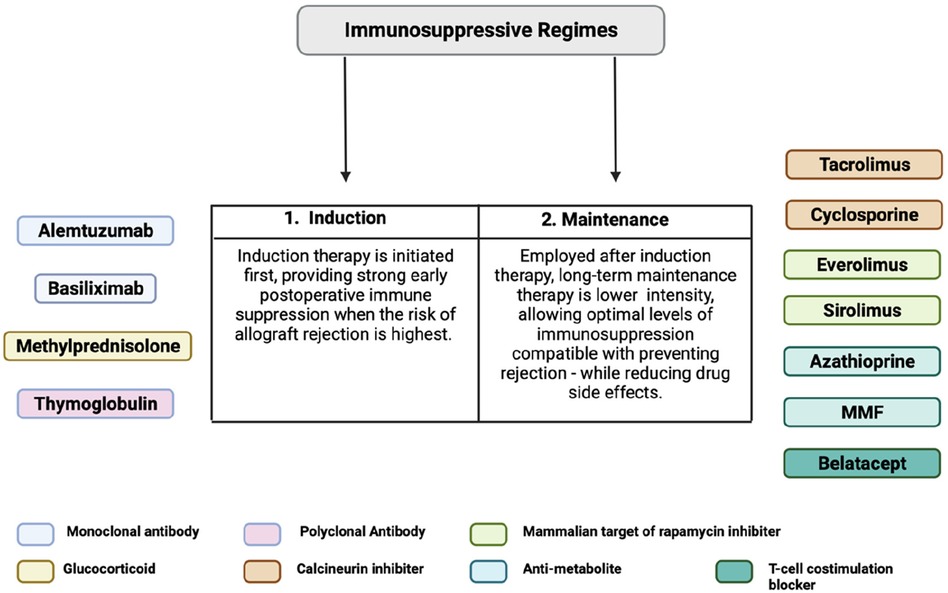
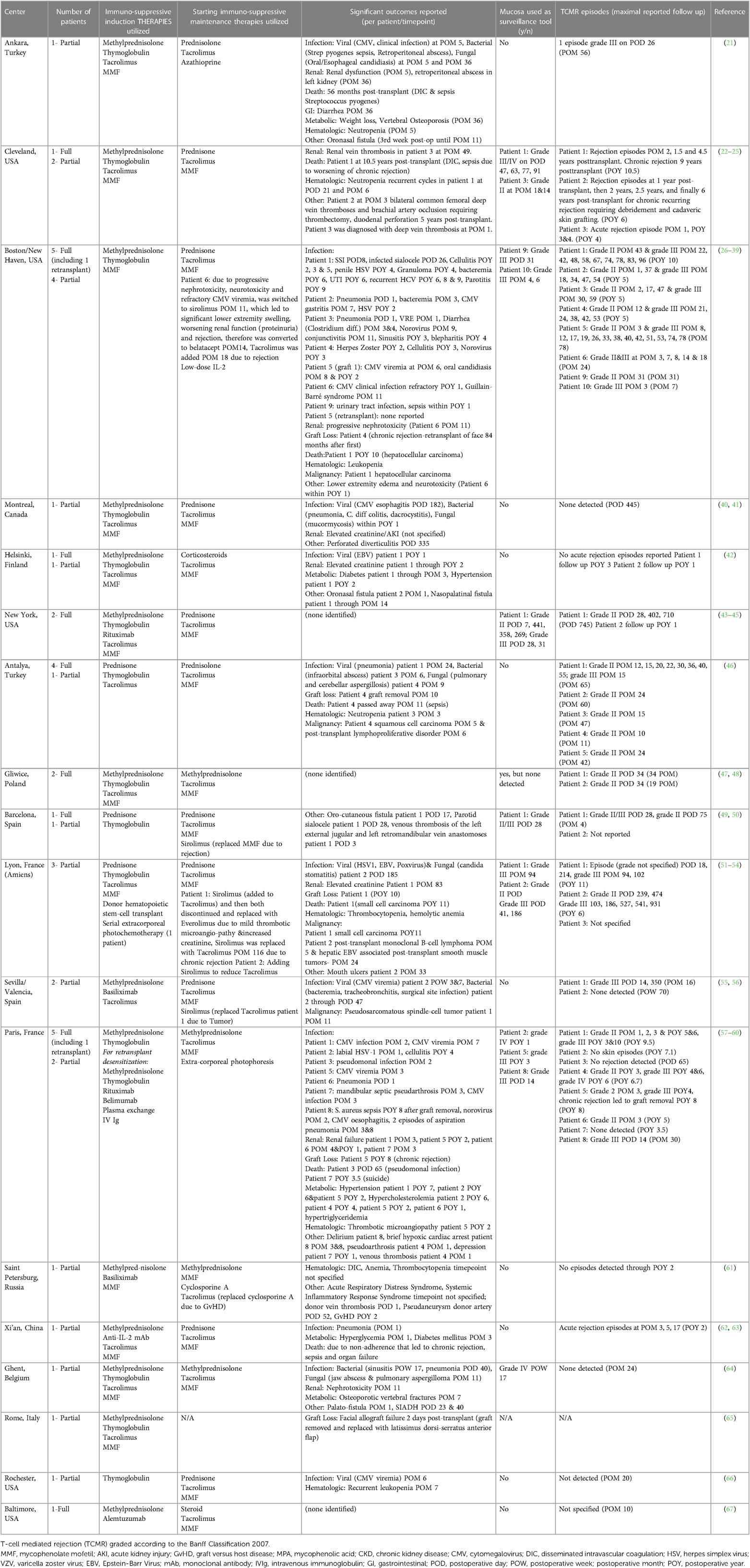
Table 1. Immunosuppressive induction and maintenance regimens and significant outcomes reported across VCA facial transplantation centers.
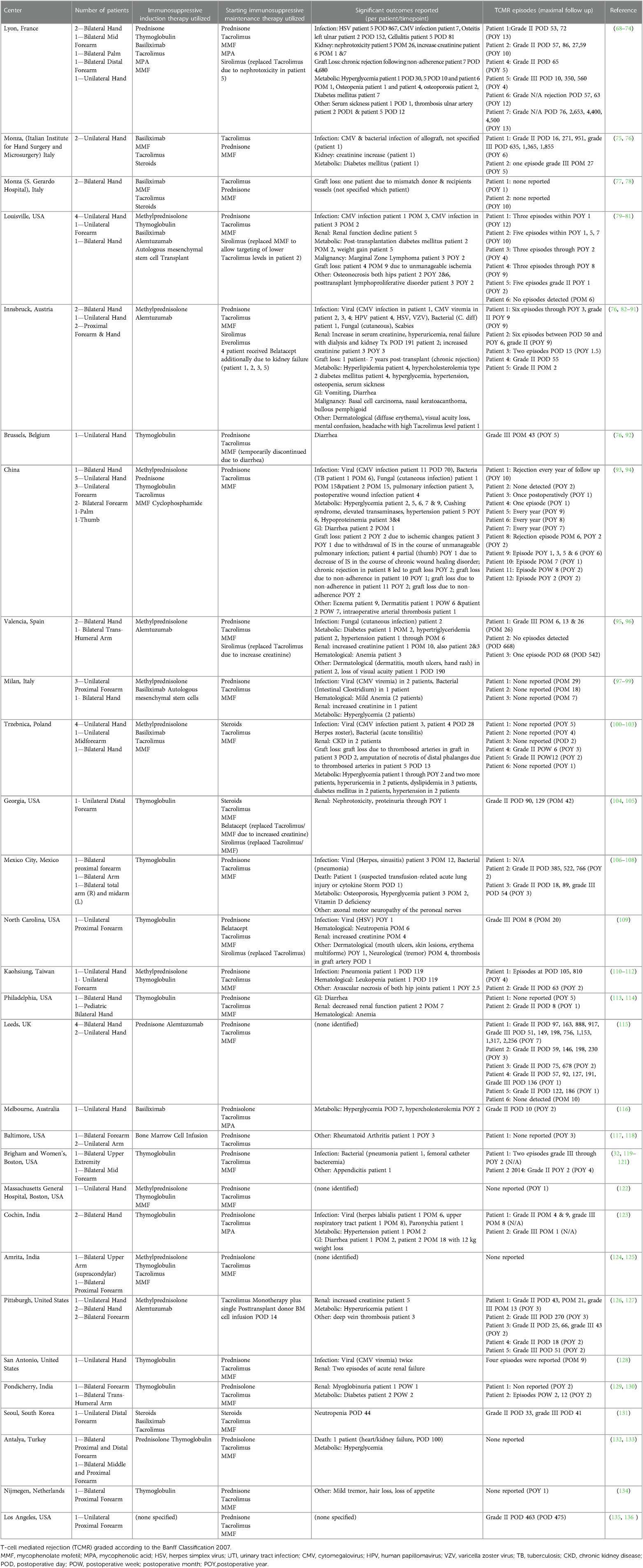
Table 2. Immunosuppressive induction and maintenance regimens and significant outcomes reported across VCA hand transplantation centers.
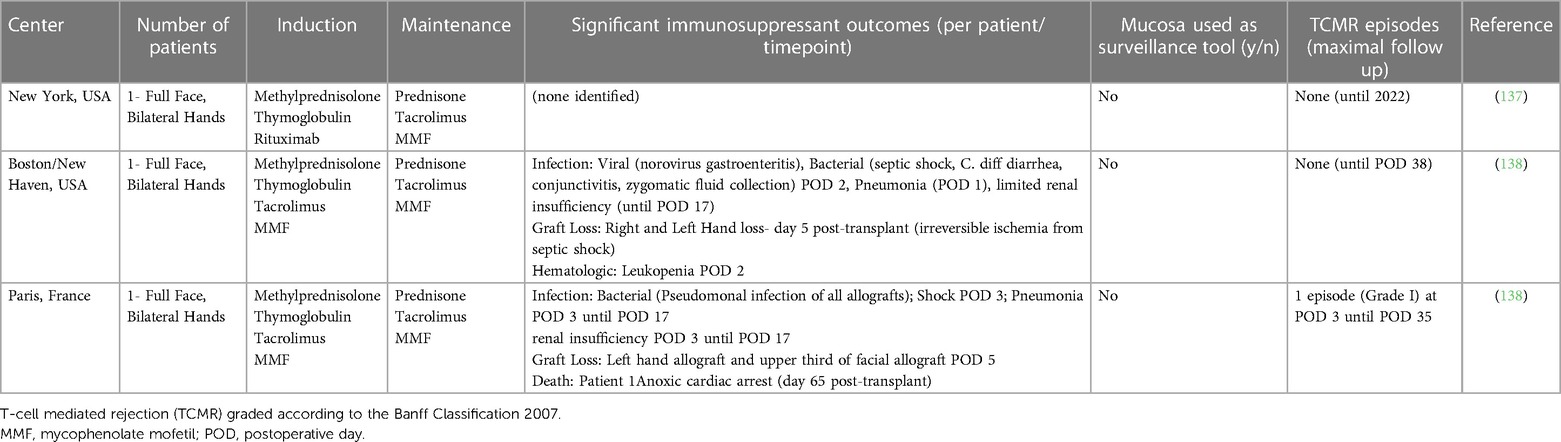
Table 3. Immunosuppressive induction and maintenance regimens and significant outcomes reported across VCA centers that performed simultaneous face and hand transplantation.
Face transplantation
A total of 18 face transplant centers were identified. Among the evaluated induction therapies as shown in Figure 3A, Thymoglobulin exhibited the highest utilization rate, being employed in 40/45 patients (88.9%). Methylprednisolone was the second most common induction immunosuppressive utilized in 33/45 (73.3%) patients. MMF, Tacrolimus, and prednisone were the next most commonly utilized agents utilized in 27/45 (60.0%), 24/45 (53.3%), and 10/45 (22.2%) patients. Other induction agents utilized in a small minority of patients included basiliximab (3/45; 6.7%), donor hematopoetic stem-cell transplant (3/45; 6.7%), rituximab (2/45; 4.4%), extracorporeal photochemotherapy (1/45; 2.2%), anti-IL-2 mAb (1/45; 2.2%), and alemtuzumab (1/45; 2.2%). A table outlining the usage of less commonly utilized agents is presented in Supplementary Figure S2. In terms of maintenance therapies as shown in Figure 3B, Tacrolimus exhibited the highest adoption rate by transplant centers, utilized in 44/45 (97.8%) patients, followed by MMF (43/45; 95.6%), prednisolone/prednisone/steroids (33/45; 73.3%), and methylprednisolone (11/45; 24.4%). Other maintenance immunosuppressive therapies that were utilized in small proportion of patients by centers included extra-corporeal photophoresis (7/45; 15.6%), sirolimus (5/45; 11.1%), belatacept (1/45; 2.2%), everolimus (1/45; 2.2%), cyclosporine A (1/45; 2.2%), azathioprine (1/45; 2.2%) (Supplementary Table S1).
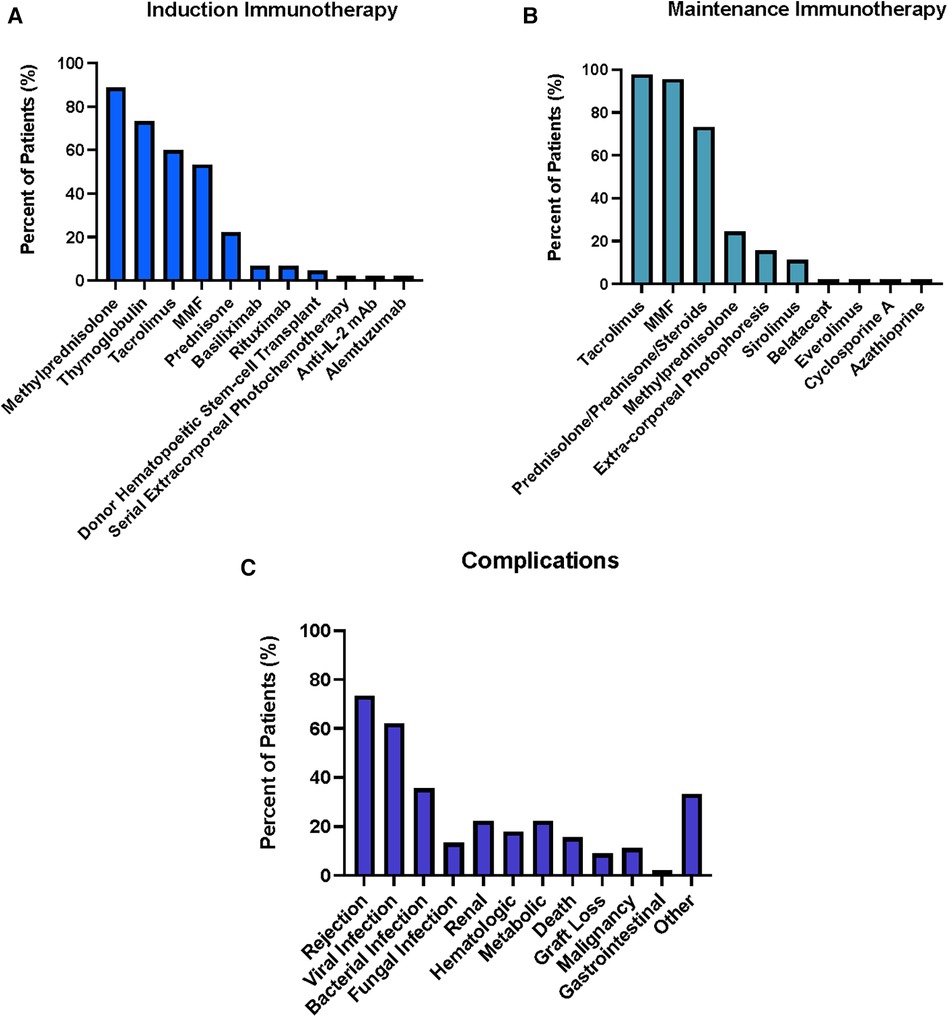
Figure 3. Summary of Induction (A) and Maintenance (B) Immunosuppressive Therapies used for 45 face transplant patients across 18 centers. Percentages represent percent of total patients treated with given immunosuppressive agent. Summary of complications (C) associated with the post-transplantation period for face transplants across international centers. Renal includes nephrotoxicity, increased creatinine levels, renal abscess, dysfunction, urinary tract infection, sepsis, acute kidney injury; Hematologic includes Neutropenia, Leucopenia, Thrombocytopenia, hemolytic anemia, thrombocyte microangiopathy; metabolic includes weight loss, osteoporosis, hypertension, hyperglycemia, diabetes mellitus, hypertriglyceridemia, hypercholesterinemia; gastrointestinal (GI) includes diarrhea, ulcer; other includes Delirium, brief hypoxic cardiac arrest, pseudoarthrosis patient, depression, venous thrombosis patient, Acute Respiratory Distress Syndrome, Systemic Inflammatory Response Syndrome, donor vein thrombosis, Pseudoaneurysm donor artery, fistula.
Among the observed complications, rejection was the most prevalent according to Figure 3C and was identified in 33/45 patients (73.3%). In detail: a total of 111 (100%) episodes of rejections were graded according to the Banff classification, additional 16 were reported without grading according to Banff. Out of all Banff graded rejection episodes, 48 episodes (43%) were grade II and 62 episodes (56%) were grade III while 1 episode (1%) was grade IV. Out of the Banff classification-graded biopsies, 25 (23%) episodes with grade II and 23 (21%) episodes grade III were seen within the first 12 months posttransplant; 12 (11%) episodes grade II and 9 (9%) episodes grade III within first 24 months; 4 (4%) episodes grade II and 5 (5%) episodes grade III in POY 3; 5 (5%) episodes grade II and 9 episodes grade III in POY 4; 1 (1%) episode grade II and 8 (8%) episodes grade III in POY 5; 1 (1%) episodes grade II, 5 (55) episodes grade III and 1 (1%) episode grade IV in POY 6; 2 (2%) episodes grade III POY 7 and 1 (1%) episode grade III POY 10. Episodes that were reported without Banff grading occurred as follows: 7 episodes within the first 12 months, 3 episodes in POY 2, 2 episodes in each POY 3 and 4, 1 episode in each POY 6 and 9. In summary, 48 (43%) of the Banff-graded biopsies occurred in the first 12 months posttransplant, 21 (19%) episodes in the second year, 9 (8%) episodes in the third year, 14 (13%) episodes in the fourth year, 9 episodes (8%) in the fifth year, 7 episodes (7%) in the sixth year, 2 (2%) in the seventh and 1 (1%) episode in the tenth year posttransplant. The next most common category of complications was infections, which was reported in 28/45 patients (62.2%). Within this category, viral infections were identified in 19/45 patients (42.2%). CMV was the most common subtype (11/45 patients; 24.5%) with CMV infections reported in 7 (15.5%) patients while CMV viremia was observed in 4 (8.8%) patients. Viral infections were followed by bacterial infections (reported in 16/45 patients; 35.6%) and fungal infections (reported in 6/45 patients, 13.3%). Renal and metabolic complications followed the infection category and were each reported in 10/45 patients (22.2%) with elevated creatinine (3/45; 6.7%), hypertension (4/45; 8.9%), and hypercholesterolemia (4/45; 8.9%) being the subcategories observed in most patients. Hematologic complications were reported in 8/45 patients (17.8%), with neutropenia/leukopenia dominating this category (reported in 5/45 patients, 11.1%). Deaths of face transplant patients were reported in a total of seven patients with three deaths occurring from systemic infections, two deaths from malignancies, one death from suicide, and one not specified. Graft loss was reported in 4/45 patients (8.9%) after a median follow up of 77.5 posttransplant months (range 10–120 months) while malignancy was reported in 5/45 patients (11.1%). Gastrointestinal (GI) complications were the least frequent complication reported, with diarrhea identified in 1/45 patient (5.6%). Other complications were identified in 15/45 patients with the most common subtype being fistula formation (5/45; 11.1%).
Hand transplantation
The induction and maintenance therapies utilized in this study demonstrated varying degrees of adoption among the 29 centers identified from the search results. The distribution of these induction and maintenance immunosuppressive therapies is summarized in Figure 4A,B. Among the induction therapies evaluated, Thymoglobulin exhibited the highest utilization, being employed in 49/91 patients (53.8%). Methylprednisolone was the second most used induction therapy utilized in 46/91 patients (50.5%), followed by MMF/MPA (32/91; 35.2%), Tacrolimus (30/91; 33.0%), Basiliximab (29/91; 31.9%), Alemtuzumab (26/91; 28.6%), and Prednisone/Prednisolone/Steroids (24/91; 26.4%). In a smaller proportion of patients autologous mesenchymal stem cell transplant (11/91; 12.1%), cyclophosphamide (11/91; 12.1%), and bone marrow cell infusion (3/91; 3.3%) were utilized as induction therapies. The most prevalent maintenance therapy observed in the study was Tacrolimus which was employed in all centers across all patients (91/91, 100%). Prednisone/Prednisolone/Steroids and MMF/MPA were the second most common agent classes utilized, identified in 86/91 (94.5%) and 82/91 (90.1%) of patients respectively. A smaller proportion of patients were treated with maintenance immunosuppressive medication utilizing sirolimus (25/91; 27.5%), everolimus (9/91; 9.9%), belatacept (6/91; 6.6%), donor bone marrow infusion (5/91; 5.5%).
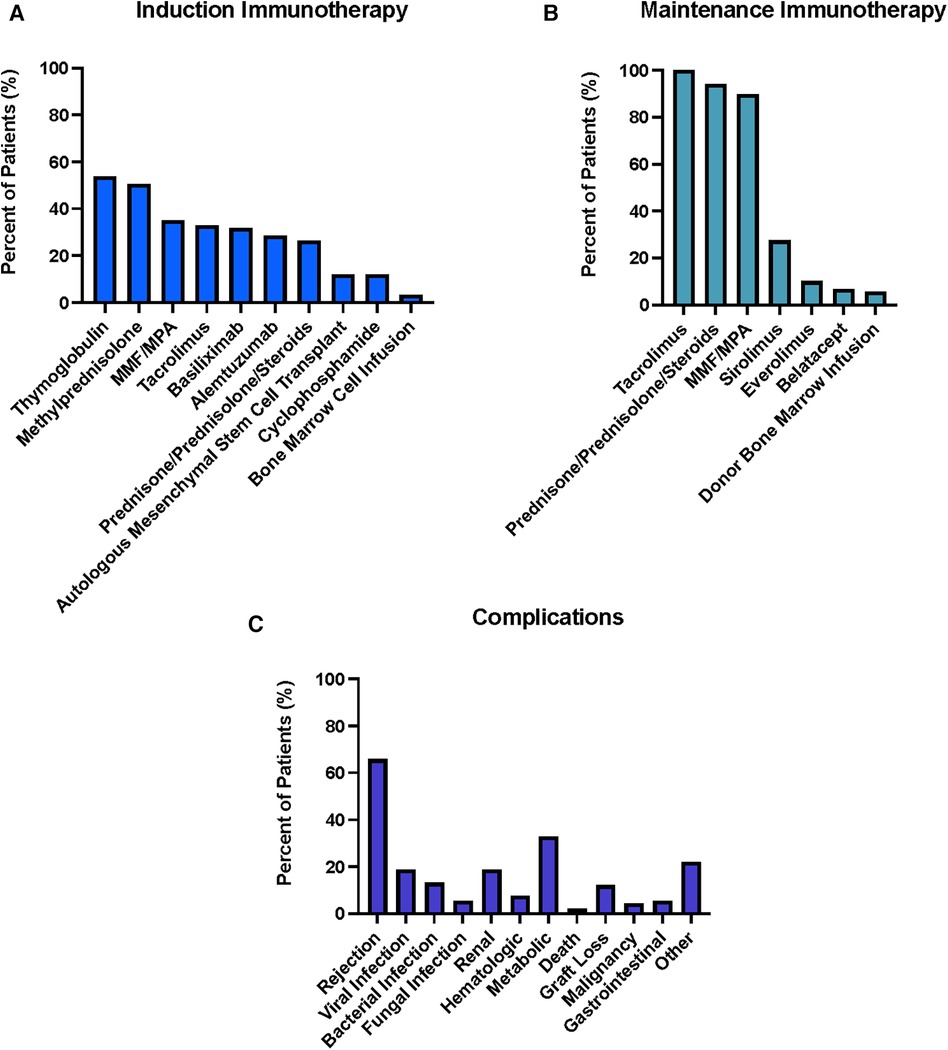
Figure 4. Summary of Induction (A) and Maintenance (B) Immunosuppressive Therapies used for 91 hand transplant patients across 29 centers. Percentages represent percent of total patients treated with given immunosuppressive agent. Summary of complications associated with the post-transplantation period for hand transplants across international centers (C). Renal includes nephrotoxicity, increased creatinine levels, kidney failure requiring kidney transplantation, urinary tract infection, sepsis, acute kidney injury, hyperuricemia, myoglobinuria, proteinuria; Hematologic includes Neutropenia, Leucopenia, anemia, proteinemia; Metabolic includes weight loss, osteoporosis, osteopenia, hypertension, hyperglycemia, diabetes mellitus, hypertriglyceridemia, hypercholesterinemia, hyperlipidemia, serum sickness, weight gain, Cushing syndrome; Gastrointestinal (GI) includes diarrhea, vomiting; Other includes donor vein thrombosis, serum sickness, osteonecrosis hip, posttransplant proliferative disorder, mental confusion, vision loss, erythema, arterial thrombosis, eczema, neuropathy, tremor, appendicitis, arthritis, deep vein thrombosis.
The distribution of complications reported by various hand VCA centers is summarized in Figure 4C. Similar to face transplantation, the most prevalent complication was rejection as well, identified in 60/91 patients (65.9%). In total 158 episodes of rejection were reported, 74 episodes without a grading while 84 episodes were reported according to the Banff classification. Out of the 84 (100%) graded rejection episodes, 39 episodes (46%) were grade II while 16 episodes (20%) were grade III within the first 12 months posttransplant; 9 episodes (11%) were grade II and 4 episodes (5%) were grade III POY 2; 5 episodes (6%) were grade II while 7 episodes (9%) were grade III POY 3; 1 episode (1%) grade III was reported for each POY 4, 5 and 6. For the non-graded episodes, 30 episodes were reported within POM 12, 8 episodes in POY 2, 7 episodes in POY 3, 4 episodes in POY 4, 6 episodes in POY 5, 5 episodes in POY 6, 6 episodes in POY 7, 3 episodes in POY 8, 2 episodes in POY 9, 1 episode in POY 10 and 2 episodes in POY 12. In summary, out of the Banff graded rejection episodes 55 episodes (66%) occurred in the first 12 months posttransplant, 13 episodes (16%) in POY 2, 12 episodes (15%) in POY 3, 1 episode (1%) in each POY 4, 5 and 6. This is followed by infections, reported in 33/91 patients (36.3%). Within the category of infection, viral infections were the most common in 18/91 patients (19.8%) with CMV being the most common subtype in 12/91 patients (13.2%). Out of the 12 reported CMV events, 7 (7.7%) patients showed clinical signs of CMV infection while a CMV viremia was detected in 5 (5.5%) patients. Additionally, bacterial and fungal infections were identified in 12/91 (13.2%) and 5/91 patients (5.5%), respectively. This was followed by the category of metabolic complications, which was reported in 30/91 patients (33.0%) with the most common entity in this category being hyperglycemia identified in 22/91 (24.2%) patients. Renal complications were identified in 17/91 patients (18.7%) followed by hematological complications in 7/91 patients (7.7%). The most common hematological complication identified was anemia (4/91patients, 4.4%). GI complications were seen in 5/91 patients (5.5%) with diarrhea being the most common subcategorization seen in all those patients. Across all patients two resulted in death (2.2%) and 11/91 resulted in graft loss (12.1%). Graft loss was observed after a median follow up of 37.8 posttransplant months (range 9–152 months). Other complications were found in 20/91 patients with the most significant subtype being skin lesions/dermatitis in 6/91 patients (6.6%).
Combined face and hand transplantation
Among the evaluated induction therapies as shown in Figure 5A, Thymoglobulin and Methylprednisolone were both utilized in all three patients (100%). Tacrolimus and MMF each exhibited utilization in 2/3 patients (66.7%) and rituximab was employed in 1/3 (33.3%) of patients to induce mature B-lymphocytes depletion. In terms of maintenance therapies, Prednisone, Tacrolimus, and MMF were each employed in all three patients (100%) as triple immunosuppressive therapy (Figure 5B).

Figure 5. Summary of Induction (A) and Maintenance (B) Immunosuppressive Therapies used for three combined face and hand transplant patients across three different centers. Percentages represent percent of total patients treated with given immunosuppressive agent. Summary of complications associated with the post-transplantation period for face/hand transplants across three international centers (C). Complications were reported in detail with kidney insufficiency (renal) and leucopenia (hematologic).
As summarized by Figure 5C, both infections and renal complications were each reported in 2/3 patients (66.7%). Graft loss was a substantial concern, also reported in 2/3 patients (66.7%) within the first five postoperative days, indicating potential challenges in graft survival and function. Death, graft rejection, and hematologic complications were all each identified in 1/3 patient (33.3%). One episode of rejection was reported for one patient (33.3%) at POD 3.
Discussion
The therapeutic paradigm and approach utilized in immunosuppression of VCAs has largely been adopted from solid organ transplant models and is outlined in Figure 2. A two-tiered approach is utilized, starting with an induction phase predominantly characterized by anti-lymphocyte mono-/polyclonal antibodies administered at high doses shortly before or at the time of transplant (18, 139). The goal of this phase is to achieve rapid and significant reductions in levels of T-cell lymphocytes soon after transplantation when risk of acute rejection is highest. Following this, a life-long maintenance phase is established utilizing a variety of agents designed to reduce T-cell functionality and activation including calcineurin inhibitors, mTOR inhibitors, and purine synthesis inhibitors (18, 19). Across both phases, steroid agents are utilized for additional immunosuppressive support. Data from SOT has demonstrated that implementation of immunosuppressive regimens has significantly improved long-term outcomes over the past three decades- offering an overall safe long-term therapy for improving allograft survival (140–142).
Face transplantation
Our results in comparing immunosuppressant regimens across all identified face transplant centers revealed that thymoglobulin and methylprednisolone were the two most common agents utilized for induction, being utilized in the vast majority of patients (>70%). Thymoglobulin first became available over 30 years ago and prior to its adaptation to VCA, has been the most widely used lymphocyte-depleting preparation in solid organ transplantation (143). Its more prominent use in VCA over other lymphocyte depleting agents such as alemtuzumab or basiliximab is largely supported by previous kidney transplantation studies highlighting the superiority of thymoglobulin across several outcomes including reduced acute rejection, graft failure, and patient death (144–146). Methylprednisolone is often utilized as the steroid of choice during the induction phase due to its capacity to be given intravenously with ease intra- or peri-operatively as well as first line bolus therapy during episodes of acute rejection. In terms of maintenance immunosuppressive therapy, Tacrolimus, MMF, and steroids were by far the three most common agents utilized. The adaptation of this “triple therapy” approach in VCA has also been drawn from SOT that implemented this maintenance model which demonstrated increased survival rate of transplants with lower toxic side effects (147, 148). As it can be seen in Figure 3A where Tacrolimus and MMF were reported the third most common agents for induction, many centers often begin the long-term maintenance therapy at the peri-operative period (starting on day of surgery) in which the induction immunosuppressants are also given.
The most common complication category reported by centers in fVCA patients after rejection was infectious, reported in over 60% of patients. The most common infection type was viral with CMV being the most prevalent subcategory. This finding mirrors that seen in SOT where CMV is noted to affect up to three-quarters of all solid organ transplant recipients (149). An international multicenter study of CMV complications in fVCA patients by Kauke-Navarro et al. identified that patients with Donor + /Recipient—CMV allotransplantation status were at increased risk of CMV-related complications and that CMV infections were most likely to occur within the first-year after transplant when antiviral prophylaxis is discontinued (16). Given its high reported prevalence across the majority of fVCA patients with 26.7%, this highlights the importance of maintaining active surveillance for both the CMV seropositivity status of donors and recipients as well as signs of active infection following face transplantation in recipients. Slightly fewer events of CMV were reported for hand transplant patients with 19.3% while CMV has not been reported in patients receiving hand and face transplantation. Theoretically, CMV is present in the mucosa of face transplants and thus the rate of transfer, and clinically relevant infection may be higher in face as demonstrated here. Reported in approximately ∼20% of centers each, the next three most common complications were renal (renal failure, increased creatinine), metabolic (hypertension, diabetes/hyperglycemia), and hematologic (leukopenia); all of which have been identified as predominant side effects across the reciprocal immunosuppression agents utilized in both SOT and VCA models (150–153).
Hand transplantation
The immunosuppressant regimens utilized for hand VCAs closely mirror those which were identified in fVCAs across different centers. The most common induction immunosuppressants used in over 50% of patients centers each was also thymoglobulin followed in conjunction with Methylprednisolone. Additionally, like face VCA, maintenance immunosuppression with the triple therapy regimen (Tacrolimus, MMF, and prednisone) was also the most common agents utilized in ∼90% of all hand VCA patients—a finding also corroborated in a separate review (154). This noted immunosuppression commonality between hand and face VCA is corroborated by a comparative study by Rifkin et al. which looked at 57 VCA and 98 kidney transplant patients and noted that hand and face VCA recipients received comparable MMF/prednisone doses and were treated with similar tacrolimus target trough levels as kidney recipients (139).
Additionally, the most common complications reported from hand VCA centers were also closely aligned with those of face VCA centers, which included infections, metabolic, and renal complications. This finding is largely congruent with the previous trends highlighted with face VCAs considering the most common immunosuppressant agents identified were the same across both face and hand VCA centers- thus a similar overall complication profile between hand and face may be expected and has been reported in similar studies (154). It's important to note that, CMV was once again the most common infection subtype reported in hand VCA centers, which further emphasizes the significance of having active CMV surveillance protocols for any type of transplant patient with VCA or SOT (155).
Hand and face transplantation
To touch on briefly, our systematic review identified three cases across three different centers were a patient received both face and hand VCAs simultaneously as outlined in Table 3. All centers utilized thymoglobulin for induction and the standard triple therapy for maintenance. Interestingly, 2/3 patients experienced loss of their graft shortly after following the operation due to infectious complications. One patient lost their bilateral hand VCAs and one patient lost their left hand VCA and part of their face VCA before passing away from anoxic cardiac arrest about two months post-transplantation. Several factors have been considered for the relative increased percentage of graft failure in this patient population including increased antigenic burden, extended anesthesia time, and large-volume resuscitations that were required. However the patient population size is far too limited for any definitive conclusions to stand (138).
Overall, our results highlight that both face and hand VCA utilize similar immunosuppression protocols for induction (thymoglobulin & methylprednisolone) and maintenance therapy (Tacrolimus, MMF, Prednisone). However, modifications to the standard triple therapy are typically considered when a patient experiences intolerance to the triple therapy, such as a decline in renal function or the development of severe, refractory diarrhea. In such cases, as depicted in Figures 3, 4, the dose of tacrolimus may be reduced while belatacept may be added, or tacrolimus can be completely discontinued and replaced with, for example, sirolimus or everolimus. It is hypothesized that due to its mechanism of action as a T-cell costimulation blocker, belatacept could also potentially reduce the incidence of AMR (antibody-mediated rejection) but may be in an inferior position preventing acute cellular rejection episodes as shown by BENEFIT study in kidney transplant patients.
Especially if patients exhibit an uneventful course, it may also be contemplated to discontinue prednisone entirely and transition to a dual therapy, consisting of, for instance, Tacrolimus and MMF. The treatment is usually adjusted to the individual's specific situation due to the absence of guidelines for low case numbers and the patient's unique characteristics and can include a number of agents highlighted in Supplementary Figure S2.
Face and hand VCA differ through the incorporation of mucosal tissue in face VCA which studies have indicated might be more immunogenic than skin alone and may reject at a higher frequency (11, 12) and indeed our results revealed that rejection episodes and clinical CMV infections were seen more often in face than in hand transplant patients indicating that the complex fVCA composition could add to immunogenicity. However, centers reported a similar distribution of the remaining most frequent patient encountered complications. That being said, it is unknown if certain immunosuppressant agents or different dosages of established immunosuppressive regimens might have better indications for mucosal-sourced VCAs such as face. However, given the small global subset continued expansion of the current VCA patient population will need to occur in order to successfully evaluate and identify such potential trends. The current challenges still revolve around the long-term toxic side effects of immunosuppressants and the occurrence of rejection reactions during the course of treatment. An ideal therapy would, therefore, shift from the approach of immunosuppression to the approach of inducing tolerance. And, thus, to make VCA more accessible to a greater number of patients, especially those for whom a cost-benefit analysis currently yields negative results.
The relative antigenicity of VCA tissues
In the field of VCA, it is widely accepted that skin is the most antigenic tissue (10, 156). As a result, clinical decisions in VCA management often rely on skin biopsy results, which are assessed using the Banff scale established in 2007, in conjunction with clinical evaluations of the graft (157).
The basis for this widely held belief and clinical practice comes from animal studies conducted with allogeneic split-thickness skin grafts in comparison to solid organ transplants in various animal models, including dog and rat (e.g., Moseley et al. 1966) (10). These studies globally indicated that skin was highly allogeneic, although some studies, like the one conducted by Lee et al., lacked conclusive evidence that skin was the most antigenic tissue in composite grafts (158, 159). Another study by Oda et al. assessed relative antigenicity in a rat hindlimb model and found that microRNA-155 expression, a marker of inflammation, was significantly higher in skin compared to bone (160). This led to the conclusion that skin was more antigenic during acute rejection.
However, it is important to note that none of these studies included models that incorporated mucosal tissue. In the context of limb VCA, skin is undeniably crucial due to its large surface area. However, in facial VCA, the addition of mucosal tissue becomes a significant consideration (11, 12).
In clinical practice, we have observed that oral mucosa in facial VCAs experiences a higher rate of rejection and more frequent rejection episodes (11–13, 161). This observations supports that mucosa is more antigenic than skin in facial VCAs. Surprisingly, there is a notable absence of studies investigating the comparative antigenicity of oral mucosa in comparison to skin. Moreover, there is a pressing need for additional research to unravel the mechanisms underlying both skin and mucosal rejection, ideally through direct comparison studies.
Limitations
Although the search criteria of our systematic review were thorough in including the large majority of face and hand VCA cases reported, not all individual cases to date were able to be identified in the literature and included in this review. Furthermore, due to nature of this review analyzing published data and not conducting a multi-center study, we did not have access to updated data directly by the centers meaning this review is unable to capture all treatment changes or complications that occurred in the patients until today. Therefore, the maximal follow up period is listed in Tables 1–3 for each patient that has been reported.
Conclusion
Although VCAs have the incredible ability to restore optimal functional and aesthetic outcomes to patients who are not candidates for other reconstructive options, they necessitate life-long adherence to immunosuppressive regimens. This review provides a contemporary update and comparison on the current immunosuppressive regimens utilized in face and hand VCAs around the world and ultimately identified that although there is notable variation between induction and maintenance immunosuppressive agents that are utilized, the most common approach across both hand and face VCA centers primarily includes utilization of thymoglobulin /methylprednisolone induction regimen with a tacrolimus/MMF/steroid maintenance regimen. Given the increased immunogenicity of VCA tissue in general and differences within VCA types such as hand compared to face that is including mucosa whose immunogenic role has not yet been fully investigate, relative to SOT, it is important that we continue to explore and develop immunosuppressive agents tailored to VCA graft types that work to provide maximal allograft health outcomes while minimizing the associated complications. Notably, facial grafts exhibited a heightened susceptibility to rejection episodes, higher grades of rejection, and clinical CMV infections, signaling a distinctive set of challenges most likely based on facial mucosa. Our study outcomes underscore the imperative need for a nuanced therapeutic approach distinct from the standard triple therapy, given the disparate composition of facial and hand grafts emphasizing the necessity for a more targeted and individualized treatment regimen to optimize outcomes in both transplantations.
Author contributions
LH: Conceptualization, Formal Analysis, Methodology, Supervision, Writing – original draft, Writing – review & editing. SB: Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing. AK: Data curation, Investigation, Writing – original draft, Writing – review & editing. AD: Writing – original draft, Writing – review & editing. JM: Data curation, Writing – original draft, Writing – review & editing. SH: Investigation, Writing – original draft, Writing – review & editing. VS: Writing – original draft, Writing – review & editing. RF: Supervision, Writing – original draft, Writing – review & editing. BP: Methodology, Supervision, Writing – original draft, Writing – review & editing. MK-N: Formal Analysis, Investigation, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
LH is receiving an individual research grant by the German Research Foundation (DFG).
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frtra.2024.1366243/full#supplementary-material
References
1. Honeyman C, Dolan R, Stark H, Fries CA, Reddy S, Allan P, et al. Abdominal wall transplantation: indications and outcomes. Curr Transplant Rep. (2020) 7(4):279–90. doi: 10.1007/s40472-020-00308-9
2. Diep GK, Berman ZP, Alfonso AR, Ramly EP, Boczar D, Trilles J, et al. The 2020 facial transplantation update: a 15-year compendium. Plast Reconstr Surg Glob Open. (2021) 9(5):e3586. doi: 10.1097/GOX.0000000000003586
3. Brännström M, Belfort MA, Ayoubi JM. Uterus transplantation worldwide: clinical activities and outcomes. Curr Opin Organ Transplant. (2021) 26(6):616–26. doi: 10.1097/MOT.0000000000000936
4. Wells MW, Rampazzo A, Papay F, Gharb BB. Two decades of hand transplantation: a systematic review of outcomes. Ann Plast Surg. (2022) 88(3):335–44. doi: 10.1097/SAP.0000000000003056
5. Lopez CD, Girard AO, Lake IV, Oh BC, Brandacher G, Cooney DS, et al. Lessons learned from the first 15 years of penile transplantation and updates to the Baltimore criteria. Nat Rev Urol. (2023) 20(5):294–307. doi: 10.1038/s41585-022-00699-7
6. UNOS. USA Kidney Transplant in 2022. (2023). Available online at: https://unos.org/news/in-focus/new-milestone-kidney-donation-and-transplant/#:∼:text=More%20than%2025%2C000%20lifesaving%20kidney,year%20for%20the%20first%20time (cited June 23, 2023).
7. Murray JE, Merrill JP, Dammin GJ, Dealy JB Jr, Alexandre GW, Harrison JH. Kidney transplantation in modified recipients. Ann Surg. (1962) 156(3):337–55. doi: 10.1097/00000658-196209000-00002
8. Hatzinger M, Stastny M, Grützmacher P, Sohn M. Die geschichte der nierentransplantation. Urologe. (2016) 55(10):1353–59. German. doi: 10.1007/s00120-016-0205-3
9. Kueckelhaus M, Fischer S, Seyda M, Bueno EM, Aycart MA, Alhefzi M, et al. Vascularized composite allotransplantation: current standards and novel approaches to prevent acute rejection and chronic allograft deterioration. Transpl Int. (2016) 29(6):655–62. doi: 10.1111/tri.12652
10. Moseley RV, Sheil AG, Mitchell RM, Murray JE. Immunologic relationships between skin and kidney homografts in dogs on immunosuppressive therapy. Transplantation. (1966) 4(6):678–87. doi: 10.1097/00007890-196611000-00003
11. Kauke-Navarro M, Tchiloemba B, Haug V, Kollar B, Diehm Y, Safi AF, et al. Pathologies of oral and sinonasal mucosa following facial vascularized composite allotransplantation. J Plast Reconstr Aesthet Surg. (2021) 74(7):1562–71. doi: 10.1016/j.bjps.2020.11.028
12. Kauke M, Safi AF, Zhegibe A, Haug V, Kollar B, Nelms L, et al. Mucosa and rejection in facial vascularized composite allotransplantation: a systematic review. Transplantation. (2020) 104(12):2616–24. doi: 10.1097/TP.0000000000003171
13. Moktefi A, Hivelin M, Grimbert P, Carmagnat M, Sbidian E, Papouin B, et al. Face transplantation: a longitudinal histological study focusing on chronic active and mucosal rejection in a series with long-term follow-up. Am J Transplant. (2021) 21(9):3088–100. doi: 10.1111/ajt.16489
14. Huelsboemer L, Kauke-Navarro M, Reuter S, Stoegner VA, Feldmann J, Hirsch T, et al. Tolerance induction in vascularized composite allotransplantation-A brief review of preclinical models. Transpl Int. (2023) 36:10955. doi: 10.3389/ti.2023.10955
15. Kauke M, Safi AF, Panayi AC, Palmer WJ, Haug V, Kollar B, et al. A systematic review of immunomodulatory strategies used in skin-containing preclinical vascularized composite allotransplant models. J Plast Reconstr Aesthet Surg. (2022) 75(2):586–604. doi: 10.1016/j.bjps.2021.11.003
16. Kauke-Navarro M, Panayi AC, Formica R, Marty F, Parikh N, Foroutanjazi S, et al. Cytomegalovirus-related complications and management in facial vascularized composite allotransplantation: an international multicenter retrospective cohort study. Transplantation. (2022) 106(10):2031–43. doi: 10.1097/TP.0000000000004132
17. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Br Med J. (2021) 372:n71. doi: 10.1136/bmj.n71
18. Hussain Y, Khan H. Immunosuppressive drugs. Ency Infect Immun. (2022):726–40. doi: 10.1016/B978-0-12-818731-9.00068-9
19. Nelson J, Alvey N, Bowman L, Schulte J, Segovia MC, McDermott J, et al. Consensus recommendations for use of maintenance immunosuppression in solid organ transplantation: endorsed by the American college of clinical pharmacy, American society of transplantation, and the international society for heart and lung transplantation. Pharmacotherapy: J Human Pharmacol Drug Therapy. (2022) 42(8):599–633. doi: 10.1002/phar.2716
20. Kirk AD. Induction immunosuppression. Transplantation. (2006) 82(5):593–602. doi: 10.1097/01.tp.0000234905.56926.7f
21. Ozmen S, Findikcioglu K, Sibar S, Tuncer S, Ayhan S, Guz G, et al. First composite woman-to-woman facial transplantation in Turkey: challenges and lessons to be learned. Ann Plast Surg. (2023) 90(1):87–95. doi: 10.1097/SAP.0000000000003323
22. Knackstedt R, Siemionow M, Djohan R, Schwarz G, Gharb BB, Rampazzo A, et al. Youngest composite full-face transplant: a model for vascularized composite allograft in younger populations. Ann Plast Surg. (2022) 89(5):564–72. doi: 10.1097/SAP.0000000000003312
23. Siemionow MZ, Papay F, Djohan R, Bernard S, Gordon CR, Alam D, et al. First U.S. Near-total human face transplantation: a paradigm shift for massive complex injuries. Plast Reconstr Surg. (2010) 125(1):111–22. doi: 10.1097/PRS.0b013e3181c15c4c
24. Siemionow M, Papay F, Alam D, Bernard S, Djohan R, Gordon C, et al. Near-total human face transplantation for a severely disfigured patient in the USA. Lancet. (2009) 374(9685):203–9. doi: 10.1016/S0140-6736(09)61155-7
25. Chang IA, Bassiri Gharb B, Bergfeld WF, Sardiña LA, Djohan RS, Gastman BR, et al. Maxillary and mandibular healing after facial allotransplantation. J Craniofac Surg. (2022) 33(8):2427–32. doi: 10.1097/SCS.0000000000008831
26. Kauke M, Panayi AC, Tchiloemba B, Diehm YF, Haug V, Kollar B, et al. Face transplantation in a black patient—racial considerations and early outcomes. N Engl J Med. (2021) 384(11):1075–6. doi: 10.1056/NEJMc2033961
27. Tasigiorgos S, Kollar B, Turk M, Perry B, Alhefzi M, Kiwanuka H, et al. Five-year follow-up after face transplantation. N Engl J Med. (2019) 380(26):2579–81. doi: 10.1056/NEJMc1810468
28. Haug V, Kollar B, Obed D, Kiwanuka H, Turk M, Wo L, et al. The evolving clinical presentation of acute rejection in facial transplantation. JAMA Facial Plast Surg. (2019) 21(4):278–85. doi: 10.1001/jamafacial.2019.0076
29. Krezdorn N, Murakami N, Pomahac B, Riella LV. Immunological characteristics of a patient with belatacept-resistant acute rejection after face transplantation. Am J Transplant. (2016) 16(11):3305–7. doi: 10.1111/ajt.13977
30. Alhefzi M, Aycart MA, Bueno EM, Kueckelhaus M, Fischer S, Snook RJ, et al. Guillain-Barré syndrome associated with resistant cytomegalovirus infection after face transplantation. Transpl Infect Dis. (2016) 18(2):288–92. doi: 10.1111/tid.12516
31. Aycart MA, Alhefzi M, Kueckelhaus M, Krezdorn N, Bueno EM, Caterson EJ, et al. A retrospective analysis of secondary revisions after face transplantation: assessment of outcomes, safety, and feasibility. Plast Reconstr Surg. (2016) 138(4):690e–701e. doi: 10.1097/PRS.0000000000002605
32. Diaz-Siso JR, Fischer S, Sisk GC, Bueno E, Kueckelhaus M, Talbot S, et al. Initial experience of dual maintenance immunosuppression with steroid withdrawal in vascular composite tissue allotransplantation. Am J Transplant. (2015) 15(5):1421–31. doi: 10.1111/ajt.13103
33. Chandraker A, Arscott R, Murphy GF, Lian CG, Bueno EM, Marty FM, et al. The management of antibody-mediated rejection in the first presensitized recipient of a full-face allotransplant. Am J Transplant. (2014) 14(6):1446–52. doi: 10.1111/ajt.12715
34. Diaz-Siso JR, Parker M, Bueno EM, Sisk GC, Pribaz JJ, Eriksson E, et al. Facial allotransplantation: a 3-year follow-up report. J Plast Reconstr Aesthet Surg. (2013) 66(11):1458–63. doi: 10.1016/j.bjps.2013.06.046
35. Pomahac B, Pribaz J, Eriksson E, Bueno EM, Diaz-Siso JR, Rybicki FJ, et al. Three patients with full facial transplantation. N Engl J Med. (2012) 366(8):715–22. doi: 10.1056/NEJMoa1111432
36. Pomahac B, Pribaz J, Eriksson E, Annino D, Caterson S, Sampson C, et al. Restoration of facial form and function after severe disfigurement from burn injury by a composite facial allograft. Am J Transplant. (2011) 11(2):386–93. doi: 10.1111/j.1600-6143.2010.03368.x
37. Murakami N, Borges TJ, Win TS, Abarzua P, Tasigiorgos S, Kollar B, et al. Low-dose interleukin-2 promotes immune regulation in face transplantation: a pilot study. Am J Transplant. (2023) 23(4):549–58. doi: 10.1016/j.ajt.2023.01.016
38. Kauke M, Panayi AC, Safi AF, Haug V, Perry B, Kollar B, et al. Full facial retransplantation in a female patient-technical, immunologic, and clinical considerations. Am J Transplant. (2021) 21(10):3472–80. doi: 10.1111/ajt.16696
39. Kollar B, Rizzo NM, Borges TJ, Haug V, Abdulrazzak O, Kauke M, et al. Accelerated chronic skin changes without allograft vasculopathy: a 10-year outcome report after face transplantation. Surgery. (2020) 167(6):991–8. doi: 10.1016/j.surg.2020.01.010
40. Govshievich A, Saleh E, Boghossian E, Collette S, Desy D, Dufresne S, et al. Face transplant: current update and first Canadian experience. Plast Reconstr Surg. (2021) 147(5):1177–88. doi: 10.1097/PRS.0000000000007890
41. Roy SF, Krishnan V, Trinh VQ, Collette S, Dufresne SF, Borsuk DE, et al. Lymphocytic vasculitis associated with mild rejection in a vascularized composite allograft recipient: a clinicopathological study. Transplantation. (2020) 104(7):e208–13. doi: 10.1097/TP.0000000000003241
42. Lindford AJ, Mäkisalo H, Jalanko H, Lauronen J, Anttila VJ, Juteau S, et al. The Helsinki approach to face transplantation. J Plast Reconstr Aesthet Surg. (2019) 72(2):173–80. doi: 10.1016/j.bjps.2018.08.030
43. Kantar RS, Ceradini DJ, Gelb BE, Levine JP, Staffenberg DA, Saadeh PB, et al. Facial transplantation for an irreparable central and lower face injury: a modernized approach to a classic challenge. Plast Reconstr Surg. (2019) 144(2):264e–83e. doi: 10.1097/PRS.0000000000005885
44. Chaudhry A, Sosin M, Bojovic B, Christy MR, Drachenberg CB, Rodriguez ED. Defining the role of skin and mucosal biopsy in facial allotransplantation: a 2-year review and analysis of histology. Plast Reconstr Surg. (2015) 136(3):559–67. doi: 10.1097/PRS.0000000000001529
45. Farber SJ, Kantar RS, Diaz-Siso JR, Rodriguez ED. Face transplantation: an update for the United States trauma system. J Craniofac Surg. (2018) 29(4):832–8. doi: 10.1097/SCS.0000000000004615
46. Özkan Ö, Özkan Ö, Ubur M, Hadimioğlu N, Cengiz M, Afşar İ. Face allotransplantation for various types of facial disfigurements: a series of five cases. Microsurgery. (2018) 38(8):834–43. doi: 10.1002/micr.30272
47. Maciejewski A, Krakowczyk Ł, Szymczyk C, Wierzgoń J, Grajek M, Dobrut M, et al. The first immediate face transplant in the world. Ann Surg. (2016) 263(3):e36–9. doi: 10.1097/SLA.0000000000001597
48. Krakowczyk Ł, Maciejewski A, Szymczyk C, Oleś K, Półtorak S. Face transplant in an advanced neurofibromatosis type 1 patient. Ann Transplant. (2017) 22:53–7. doi: 10.12659/AOT.900617
49. Barret JP, Serracanta J. Lefort I osteotomy and secondary procedures in full-face transplant patients. J Plast Reconstr Aesthet Surg. (2013) 66(5):723–5. doi: 10.1016/j.bjps.2012.08.046
50. Barret JP, Gavaldà J, Bueno J, Nuvials X, Pont T, Masnou N, et al. Full face transplant: the first case report. Ann Surg. (2011) 254(2):252–6. doi: 10.1097/SLA.0b013e318226a607
51. Petruzzo P, Testelin S, Kanitakis J, Badet L, Lengelé B, Girbon JP, et al. First human face transplantation: 5 years outcomes. Transplantation. (2012) 93(2):236–40. doi: 10.1097/TP.0b013e31823d4af6
52. Dubernard JM, Lengelé B, Morelon E, Testelin S, Badet L, Moure C, et al. Outcomes 18 months after the first human partial face transplantation. N Engl J Med. (2007) 357(24):2451–60. doi: 10.1056/NEJMoa072828
53. Petruzzo P, Kanitakis J, Testelin S, Pialat JB, Buron F, Badet L, et al. Clinicopathological findings of chronic rejection in a face grafted patient. Transplantation. (2015) 99(12):2644–50. doi: 10.1097/TP.0000000000000765
54. Morelon E, Petruzzo P, Kanitakis J, Dakpé S, Thaunat O, Dubois V, et al. Face transplantation: partial graft loss of the first case 10 years later. Am J Transplant. (2017) 17(7):1935–40. doi: 10.1111/ajt.14218
55. BenMarzouk-Hidalgo OJ, Cordero E, Gómez-Cía T, Sánchez M, González-Padilla JD, Infante-Cossio P, et al. First face composite-tissue transplant recipient successfully treated for cytomegalovirus infection with preemptive valganciclovir treatment. Antimicrob Agents Chemother. (2011) 55(12):5949–51. doi: 10.1128/AAC.05335-11
56. Cavadas PC, Ibáñez J, Thione A. Surgical aspects of a lower face, mandible, and tongue allotransplantation. J Reconstr Microsurg. (2012) 28(1):43–7. doi: 10.1055/s-0031-1284236
57. Lantieri L, Hivelin M, Audard V, Benjoar MD, Meningaud JP, Bellivier F, et al. Feasibility, reproducibility, risks and benefits of face transplantation: a prospective study of outcomes. Am J Transplant. (2011) 11(2):367–78. doi: 10.1111/j.1600-6143.2010.03406.x
58. Lantieri L, Meningaud JP, Grimbert P, Bellivier F, Lefaucheur JP, Ortonne N, et al. Repair of the lower and middle parts of the face by composite tissue allotransplantation in a patient with massive plexiform neurofibroma: a 1-year follow-up study. Lancet. (2008) 372(9639):639–45. doi: 10.1016/S0140-6736(08)61277-5
59. Lantieri L, Grimbert P, Ortonne N, Suberbielle C, Bories D, Gil-Vernet S, et al. Face transplant: long-term follow-up and results of a prospective open study. Lancet. (2016) 388(10052):1398–407. doi: 10.1016/S0140-6736(16)31138-2
60. Lantieri L, Cholley B, Lemogne C, Guillemain R, Ortonne N, Grimbert P, et al. First human facial retransplantation: 30-month follow-up. Lancet. (2020) 396(10264):1758–65. doi: 10.1016/S0140-6736(20)32438-7
61. Volokh M, Manturova N, Fisun A, Uyba V, Voskanyan S, Khubulava G, et al. First Russian experience of composite facial tissue allotransplantation. Plast Reconstr Surg Glob Open. (2019) 7(11):e2521. doi: 10.1097/GOX.0000000000002521
62. Guo S, Han Y, Zhang X, Lu B, Yi C, Zhang H, et al. Human facial allotransplantation: a 2-year follow-up study. Lancet. (2008) 372(9639):631–8. doi: 10.1016/S0140-6736(08)61276-3
64. Roche NA, Vermeersch HF, Stillaert FB, Peters KT, De Cubber J, Van Lierde K, et al. Complex facial reconstruction by vascularized composite allotransplantation: the first Belgian case. J Plast Reconstr Aesthet Surg. (2015) 68(3):362–71. doi: 10.1016/j.bjps.2014.11.005
65. Santanelli di Pompeo F, Longo B, Giovanoli P, Plock JA, Campanale A, Laporta R, et al. Facial transplantation: nonimmune-related hyperacute graft failure-the role of perfusion injury: a case report. Ann Plast Surg. (2021) 86(4):469–75. doi: 10.1097/SAP.0000000000002632
66. Razonable RR, Amer H, Mardini S. Application of a new paradigm for cytomegalovirus disease prevention in mayo clinic’s first face transplant. Mayo Clin Proc. (2019) 94(1):166–70. doi: 10.1016/j.mayocp.2018.09.017
67. Dorafshar AH, Bojovic B, Christy MR, Borsuk DE, Iliff NT, Brown EN, et al. Total face, double jaw, and tongue transplantation: an evolutionary concept. Plast Reconstr Surg. (2013) 131(2):241–51. doi: 10.1097/PRS.0b013e3182789d38
68. Dubernard JM, Owen E, Herzberg G, Lanzetta M, Martin X, Kapila H, et al. Human hand allograft: report on first 6 months. Lancet. (1999) 353(9161):1315–20. doi: 10.1016/S0140-6736(99)02062-0
69. Kanitakis J, Jullien D, Nicolas JF, Frances C, Claudy A, Revillard JP, et al. Sequential histological and immunohistochemical study of the skin of the first human hand allograft. Transplantation. (2000) 69(7):1380–5. doi: 10.1097/00007890-200004150-00029
70. Petruzzo P, Revillard JP, Kanitakis J, Lanzetta M, Hakim NS, Lefrançois N, et al. First human double hand transplantation: efficacy of a conventional immunosuppressive protocol. Clin Transplant. (2003) 17(5):455–60. doi: 10.1034/j.1399-0012.2003.00005.x
71. Dubernard JM, Petruzzo P, Lanzetta M, Parmentier H, Martin X, Dawahra M, et al. Functional results of the first human double-hand transplantation. Ann Surg. (2003) 238(1):128–36. doi: 10.1097/01.SLA.0000078945.70869.82
72. Kanitakis J, Morelon E. Scabies in a bilateral hand allograft recipient: an additional mimicker of acute skin rejection in vascularized composite allotransplantation. Transpl Infect Dis. (2017) 19(3). doi: 10.1111/tid.12683
73. Herzberg G, Weppe F, Masson N, Gueffier X, Erhard L. Clinical evaluation of two bilateral hand allotransplantations at six and three years follow-up. Chir Main. (2008) 27(2-3):109–17. doi: 10.1016/j.main.2008.02.002
74. Petruzzo P, Gazarian A, Kanitakis J, Parmentier H, Guigal V, Guillot M, et al. Outcomes after bilateral hand allotransplantation: a risk/benefit ratio analysis. Ann Surg. (2015) 261(1):213–20. doi: 10.1097/SLA.0000000000000627
75. Kanitakis J, Karayannopoulou G, Lanzetta M, Petruzzo P. Graft vasculopathy in the skin of a human hand allograft: implications for diagnosis of rejection of vascularized composite allografts. Transpl Int. (2014) 27(11):e118–23. doi: 10.1111/tri.12399
76. Schneeberger S, Gorantla VS, van Riet RP, Lanzetta M, Vereecken P, van Holder C, et al. Atypical acute rejection after hand transplantation. Am J Transplant. (2008) 8(3):688–96. doi: 10.1111/j.1600-6143.2007.02105.x
77. Del Bene M, Musumarra G, di Caprio AP, et al. Double hand transplant monza. In: Gurunian R, et al., editors. Reconstructive Transplantation. Cham: Springer International Publishing (2023). p. 259–67.
78. Landin L, Bonastre J, Casado-Sanchez C, Diez J, Ninkovic M, Lanzetta M, et al. Outcomes with respect to disabilities of the upper limb after hand allograft transplantation: a systematic review. Transpl Int. (2012) 25(4):424–32. doi: 10.1111/j.1432-2277.2012.01433.x
79. Jones JW, Gruber SA, Barker JH, Breidenbach WC. Successful hand transplantation. One-year follow-up. Louisville hand transplant team. N Engl J Med. (2000) 343(7):468–73. doi: 10.1056/NEJM200008173430704
80. Breidenbach WC, Gonzales NR, Kaufman CL, Klapheke M, Tobin GR, Gorantla VS. Outcomes of the first 2 American hand transplants at 8 and 6 years posttransplant. J Hand Surg Am. (2008) 33(7):1039–47. doi: 10.1016/j.jhsa.2008.02.015
81. Kaufman CL, Breidenbach W. World experience after more than a decade of clinical hand transplantation: update from the Louisville hand transplant program. Hand Clin. (2011) 27(4):417–21, vii–viii. doi: 10.1016/j.hcl.2011.08.004
82. Schneeberger S, Landin L, Kaufmann C, Gorantla VS, Brandacher G, Cavadas P, et al. Alemtuzumab: key for minimization of maintenance immunosuppression in reconstructive transplantation? Transplant Proc. (2009) 41(2):499–502. doi: 10.1016/j.transproceed.2009.01.018
83. Schneeberger S, Petruzzo P, Morelon E, Hautz T, Kanitakis J, Weissenbacher A, et al. 20-Year Follow-up of two cases of bilateral hand transplantation. N Engl J Med. (2020) 383(18):1791–2. doi: 10.1056/NEJMc2017711
84. Weissenbacher A, Hautz T, Zelger B, Zelger BG, Mayr V, Brandacher G, et al. Antibody-mediated rejection in hand transplantation. Transpl Int. (2014) 27(2):e13–7. doi: 10.1111/tri.12233
85. Grahammer J, Weissenbacher A, Zelger BG, Zelger B, Boesmueller C, Ninkovic M, et al. Benefits and limitations of belatacept in 4 hand-transplanted patients. Am J Transplant. (2017) 17(12):3228–35. doi: 10.1111/ajt.14440
86. Brandacher G, Ninkovic M, Piza-Katzer H, Gabl M, Hussl H, Rieger M, et al. The innsbruck hand transplant program: update at 8 years after the first transplant. Transplant Proc. (2009) 41(2):491–4. doi: 10.1016/j.transproceed.2009.01.013
87. Bonatti H, Brandacher G, Margreiter R, Schneeberger S. Infectious complications in three double hand recipients: experience from a single center. Transplant Proc. (2009) 41(2):517–20. doi: 10.1016/j.transproceed.2009.01.014
88. Schneeberger S, Ninkovic M, Piza-Katzer H, Gabl M, Hussl H, Rieger M, et al. Status 5 years after bilateral hand transplantation. Am J Transplant. (2006) 6(4):834–41. doi: 10.1111/j.1600-6143.2006.01266.x
89. Schneeberger S, Lucchina S, Lanzetta M, Brandacher G, Bösmüller C, Steurer W, et al. Cytomegalovirus-related complications in human hand transplantation. Transplantation. (2005) 80(4):441–7. doi: 10.1097/01.tp.0000168454.68139.0a
90. Gabl M, Pechlaner S, Lutz M, Bodner G, Piza H, Margreiter R. Bilateral hand transplantation: bone healing under immunosuppression with tacrolimus, mycophenolate mofetil, and prednisolone. J Hand Surg Am. (2004) 29(6):1020–7. doi: 10.1016/j.jhsa.2004.05.007
91. Margreiter R, Brandacher G, Ninkovic M, Steurer W, Kreczy A, Schneeberger S. A double-hand transplant can be worth the effort! Transplantation. (2002) 74(1):85–90. doi: 10.1097/00007890-200207150-00015
92. Schuind F, Van Holder C, Mouraux D, Robert C, Meyer A, Salvia P, et al. The first Belgian hand transplantation–37 month term results. J Hand Surg Br. (2006) 31(4):371–6. doi: 10.1016/J.JHSB.2006.01.003
93. Xiang DY, Pei GX. Serial monitoring of co-stimulating signals in double hand allograft: a case report. Transplant Proc. (2009) 41(2):554–6. doi: 10.1016/j.transproceed.2009.01.017
94. Pei G, Xiang D, Gu L, Wang G, Zhu L, Yu L, et al. A report of 15 hand allotransplantations in 12 patients and their outcomes in China. Transplantation. (2012) 94(10):1052–9. doi: 10.1097/TP.0b013e31826c3915
95. Landin L, Cavadas PC, Rodriguez-Perez JC, Garcia-Bello MA, Garcia-Cosmes P, Thione A, et al. Improvement in renal function after late conversion to sirolimus-based immunosuppression in composite tissue allotransplantation. Transplantation. (2010) 90(6):691–2. doi: 10.1097/TP.0b013e3181ebf7ae
96. Cavadas PC, Ibáñez J, Thione A, Alfaro L. Bilateral trans-humeral arm transplantation: result at 2 years. Am J Transplant. (2011) 11(5):1085–90. doi: 10.1111/j.1600-6143.2011.03503.x
97. Del Bene M, Di Caprio AP, Melzi ML, Pioltelli PE, Bonomi S. Autologous mesenchymal stem cells as a new strategy in immunosuppressant therapy in double hand allotransplantation. Plast Reconstr Surg. (2013) 131(2):305e–7e. doi: 10.1097/PRS.0b013e318278d648
98. Lanzetta M, Nolli R, Vitale G, Magni F, Radaelli I, Stroppa L, et al. Hand transplantation: the milan experience. Comp Prof Pedagogy. (2007) 12(79):762–72. doi: 10.2478/v10035-007-0118-3
99. Lanzetta M, Pozzo M, Bottin A, Merletti R, Farina D. Reinnervation of motor units in intrinsic muscles of a transplanted hand. Neurosci Lett. (2005) 373(2):138–43. doi: 10.1016/j.neulet.2004.10.001
100. Jablecki J, Kaczmarzyk L, Domanasiewicz A, Chelmoński A, Kaczmarzyk J. Unilateral hand transplant-results after 41 months. Transplant Proc. (2013) 45(1):440–3. doi: 10.1016/j.transproceed.2012.06.075
101. Kamińska D, Kościelska-Kasprzak K, Myszka M, Banasik M, Chełmoński A, Boratyńska M, et al. Significant infections after hand transplantation in a Polish population. Transplant Proc. (2014) 46(8):2887–9. doi: 10.1016/j.transproceed.2014.08.028
102. Boratyńska M, Obremska M, Małecki R, Gacka M, Magott M, Kamińska D, et al. Impact of immunosuppressive treatment on the cardiovascular system in patients after hand transplantation. Transplant Proc. (2014) 46(8):2890–3. doi: 10.1016/j.transproceed.2014.09.004
103. Jablecki J. World experience after more than a decade of clinical hand transplantation: update on the Polish program. Hand Clin. (2011) 27(4):433–42, viii. doi: 10.1016/j.hcl.2011.08.003
104. Cendales L, Bray R, Gebel H, Brewster L, Elbein R, Farthing D, et al. Tacrolimus to belatacept conversion following hand transplantation: a case report. Am J Transplant. (2015) 15(8):2250–5. doi: 10.1111/ajt.13217
105. Loftus MJ. My Left Hand. (2011). Available online at: https://magazine.emory.edu/issues/2011/summer/of-note/transplant/index.html (cited June 20, 2023).
106. Iglesias M, Butron P, Moran-Romero M, Cruz-Reyes A, Alberu-Gomez J, Leal-Villalpando P, et al. Bilateral forearm transplantation in Mexico: 2-year outcomes. Transplantation. (2016) 100(1):233–8. doi: 10.1097/TP.0000000000000827
107. Iglesias M, Leal P, Butron P, Santander-Flores S, Ricano-Enciso D, Gonzalez-Chavez MA, et al. Severe complications after bilateral upper extremity transplantation: a case report. Transplantation. (2014) 98(3):e16–7. doi: 10.1097/TP.0000000000000258
108. Iglesias M, Ramirez-Berumen M, Butron P, Alberu-Gomez J, Salazar-Hernandez F, Macias-Gallardo J, et al. Functional outcomes 18 months after total and midarm transplantation: a case report. Transplant Proc. (2018) 50(3):950–8. doi: 10.1016/j.transproceed.2017.12.027
109. Cendales LC, Ruch DS, Cardones AR, Potter G, Dooley J, Dore D, et al. De novo belatacept in clinical vascularized composite allotransplantation. Am J Transplant. (2018) 18(7):1804–9. doi: 10.1111/ajt.14910
110. Kuo YR, Chen CC, Chen YC, Yeh MC, Lin PY, Lee CH, et al. The first hand allotransplantation in Taiwan: a report at 9 months. Ann Plast Surg. (2016) 77 Suppl 1:S12–5. doi: 10.1097/SAP.0000000000000758
111. Kuo YR, Chen CC, Wang JW, Chang JK, Huang YC, Pan CC, et al. Bone infarction of the hip after hand allotransplantation: a case report. Microsurgery. (2019) 39(4):349–53. doi: 10.1002/micr.30375
112. Chen YT, Huang SC, Chen CC, Lim LM, Lu PL, Hou YP, et al. Topical tacrolimus and steroids modulate T cells in acute rejection of hand allotransplantation: two case reports. Microsurgery. (2020) 40(2):217–23. doi: 10.1002/micr.30439
113. Azoury SC, Johnson FB, Levine M, Veasey S, McAndrew C, Shaked A, et al. Successful transatlantic bilateral hand transplant in a young female highly sensitized to HLA class II antigens. Transpl Immunol. (2021) 65:101377. doi: 10.1016/j.trim.2021.101377
114. Levy TJ, Tyner CE, Amaral S, Lefkowitz DS, Kessler SK, Levin LS. 5-Year Activity and participation outcomes of the first successful pediatric bilateral hand transplantation: a case report. Phys Occup Ther Pediatr. (2022) 42(6):663–79. doi: 10.1080/01942638.2022.2057210
115. Clark B, Carter C, Wilks DJ, Lobb M, Hughes P, Baker R, et al. The Leeds hand transplant programme: review of the laboratory management of the first six cases. Int J Immunogenet. (2020) 47(1):28–33. doi: 10.1111/iji.12466
116. Dwyer KM, Webb AR, Furniss HS, Anjou KE, Gibbs-Dwyer JM, McCombe DB, et al. First hand transplant procedure in Australia: outcome at 2 years. Med J Aust. (2013) 199(4):285–7. doi: 10.5694/mja12.11554
117. Adler BL, Albayda J, Shores JT, Lee WPA, Brandacher G, Bingham CO 3rd. Erosive rheumatoid arthritis after bilateral hand transplantation. Ann Intern Med. (2017) 167(3):216–8. doi: 10.7326/L16-0588
118. Shores JT, Higgins JP, Lee WP. Above-elbow (supracondylar) arm transplantation: clinical considerations and surgical technique. Tech Hand Up Extrem Surg. (2013) 17(4):221–7. doi: 10.1097/BTH.0000000000000026
119. Singh M, Sisk G, Carty M, Sampson C, Blazar P, Dyer G, et al. Functional outcomes after bilateral hand transplantation: a 3.5-year comprehensive follow-up. Plast Reconstr Surg. (2016) 137(1):185–9. doi: 10.1097/PRS.0000000000001872
120. Lopdrup RG, Turk M, Win TS, Marty FM, Molway D, Tullius SG, et al. Seasonal variability precipitating hand transplant rejection? Transplantation. (2017) 101(10):e313. doi: 10.1097/TP.0000000000001877
121. Fallahian F, Molway D, Jadeja S, Clark R, Marty FM, Riella LV, et al. Eponychial lesions following bilateral upper extremity vascular composite allotransplantation: a case report. Case Reports Plast Surg Hand Surg. (2018) 5(1):14–7. doi: 10.1080/23320885.2018.1431047
122. Eberlin KR, Leonard DA, Austen WG Jr, Yaremchuk MJ, Mudgal CS, Winograd JM, et al. The volar forearm fasciocutaneous extension: a strategy to maximize vascular outflow in post-burn injury hand transplantation. Plast Reconstr Surg. (2014) 134(4):731–5. doi: 10.1097/PRS.0000000000000508
123. Iyer S, Sharma M, Kishore P, Mathew J, Janarthanan R, Reddy R, et al. First two bilateral hand transplantations in India (part 4): immediate post-operative care, immunosuppression protocol and monitoring. Indian J Plast Surg. (2017) 50(2):168–72. doi: 10.4103/ijps.IJPS_96_17
124. Sharma M, Iyer S, Kishore P, Mathew J, Janarthanan R, Maharaja N, et al. Indian Subcontinent’s first bilateral supracondylar level upper limb transplantation. Indian J Plast Surg. (2019) 52(3):285–95. doi: 10.1055/s-0039-3401466
125. Sharma M, Iyer S, Purushottaman K, Vijayaraghavan S, Matthew J, Dudipala RR, et al. Indian Subcontinent’s first proximal forearm level double upper extremity transplantation. Indian J Plast Surg. (2019) 52(3):277–84. doi: 10.1055/s-0039-3401474
126. Schneeberger S, Gorantla VS, Brandacher G, Zeevi A, Demetris AJ, Lunz JG, et al. Upper-extremity transplantation using a cell-based protocol to minimize immunosuppression. Ann Surg. (2013) 257(2):345–51. doi: 10.1097/SLA.0b013e31826d90bb
127. Lang RS, Gorantla VS, Esper S, Montoya M, Losee JE, Hilmi IA, et al. Anesthetic management in upper extremity transplantation: the Pittsburgh experience. Anesth Analg. (2012) 115(3):678–88. doi: 10.1213/ANE.0b013e31825da401
128. Tuder D, Pederson WC, Abrahamian GA, Ingari JV, Bagg MC, Person DW, et al. San antonio military and civilian hand transplantation program: a case report. Transplant Proc. (2011) 43(9):3561–2. doi: 10.1016/j.transproceed.2011.08.048
129. Mt F, Sivakumar DK, Mohapatra D, Chittoria R. Intergender hand transplant: a sex congruent hand transformation. Ann Plast Surg. (2021) 86(2):223–5. doi: 10.1097/SAP.0000000000002515
130. Dinesh KS, Aggarwal A, Chittoria RK, Thiruvoth FM, Mohapatra DP, Chavan V, et al. Cadaveric bilateral transhumeral upper limb transplantation: journey to the next level. Indian J Plast Surg. (2020) 53(1):119–23. doi: 10.1055/s-0040-1708115
131. Lee N, Baek WY, Choi YR, Joo DJ, Lee WJ, Hong JW. One year experience of the hand allotransplantation first performed after Korea organ transplantation act (KOTA) amendment. Arch Plast Surg. (2023) 50(4):415–21. doi: 10.1055/a-2059-5570
132. Ozkan O, Demirkan F, Ozkan O, Dinckan A, Hadimioglu N, Tuzuner S, et al. The first (double) hand transplantation in Turkey. Transplant Proc. (2011) 43(9):3557–60. doi: 10.1016/j.transproceed.2011.08.045
133. Uysal H, Savkliyildiz A, Ozkan O, Colak OH, Barcin E, Senol U, et al. Complementary phenomena: phantom hand and phantom face. Cogn Behav Neurol. (2021) 34(2):150–9. doi: 10.1097/WNN.0000000000000258
134. Hummelink S, Kruit AS, Hovius SER, Ulrich DJO. Designing and utilizing 3D-printed skin incision guides during the first Dutch bilateral hand-arm transplantation. J Plast Reconstr Aesthet Surg. (2021) 74(11):2965–8. doi: 10.1016/j.bjps.2021.03.076
135. Albin A. Patient makes dramatic recovery from amputation to transplanted hand, in UCLA Newsroom. (2017).
136. Kim JY, Lei Z, Maienschein-Cline M, Chlipala GE, Balamurugan A, McDiarmid SV, et al. Longitudinal analysis of the T-cell receptor repertoire in graft-infiltrating lymphocytes following hand transplantation. Transplantation. (2021) 105(7):1502–9. doi: 10.1097/TP.0000000000003535
137. Ramly EP, Alfonso AR, Berman ZP, Diep GK, Bass JL, Catalano LW 3rd, et al. The First Successful Combined Full Face and Bilateral Hand Transplant. Plast Reconstr Surg. (2022) 150(2):414–28. doi: 10.1097/PRS.0000000000009369
138. Carty MJ, Hivelin M, Dumontier C, Talbot SG, Benjoar MD, Pribaz JJ, et al. Lessons learned from simultaneous face and bilateral hand allotransplantation. Plast Reconstr Surg. (2013) 132(2):423–32. doi: 10.1097/PRS.0b013e318295883d
139. Rifkin WJ, Manjunath AK, Kantar RS, Jacoby A, Kimberly LL, Gelb BE, et al. A comparison of immunosuppression regimens in hand, face, and kidney transplantation. J Surg Res. (2021) 258:17–22. doi: 10.1016/j.jss.2020.08.006
140. Hariharan S, Israni AK, Danovitch G. Long-term survival after kidney transplantation. N Engl J Med. (2021) 385(8):729–43. doi: 10.1056/NEJMra2014530
141. Skalická B, Málek I, Kubánek M, Vymětalová J, Kautzner J. Long-term efficacy and safety of conversion to tacrolimus in heart transplant recipients with ongoing or recurrent acute cellular rejection. Physiol Res. (2010) 59(3):379–84. doi: 10.33549/physiolres.931736
142. Koch RO, Graziadei IW, Schulz F, Nachbaur K, Königsrainer A, Margreiter R, et al. Long-term efficacy and safety of mycophenolate mofetil in liver transplant recipients with calcineurin inhibitor-induced renal dysfunction. Transpl Int. (2004) 17(9):518–24. doi: 10.1111/j.1432-2277.2004.tb00481.x
143. Mourad G, Morelon E, Noël C, Glotz D, Lebranchu Y. The role of thymoglobulin induction in kidney transplantation: an update. Clin Transplant. (2012) 26(5):E450–64. doi: 10.1111/ctr.12021
144. Bazerbachi F, Selzner M, Boehnert MU, Marquez MA, Norgate A, McGilvray ID, et al. Thymoglobulin versus basiliximab induction therapy for simultaneous kidney-pancreas transplantation: impact on rejection, graft function, and long-term outcome. Transplantation. (2011) 92(9):1039–43. doi: 10.1097/TP.0b013e3182313e4f
145. Lee H, Lee S, Jeon JS, Kwon SH, Noh H, Han DC, et al. Thymoglobulin versus basiliximab induction therapy in low-risk kidney transplant recipients: a single-center experience. Transplant Proc. (2018) 50(5):1285–8. doi: 10.1016/j.transproceed.2018.02.088
146. Asderakis A, Sabah TK, Watkins WJ, Khalid U, Szabo L, Stephens MR, et al. Thymoglobulin versus alemtuzumab versus basiliximab kidney transplantation from donors after circulatory death. Kidney International Reports. (2022) 7(4):732–40. doi: 10.1016/j.ekir.2022.01.1042
147. Bonastre J, Landin L, Diez J, Casado-Sanchez C, Casado-Perez C. Factors influencing acute rejection of human hand allografts: a systematic review. Ann Plast Surg. (2012) 68(6):624–9. doi: 10.1097/SAP.0b013e318255a411
148. Wang S, Xiong Y, Wang Y, Chen J, Yang J, Sun B. Evaluation of PLGA microspheres with triple regimen on long-term survival of vascularized composite allograft—an experimental study. Transpl Int. (2020) 33(4):450–61. doi: 10.1111/tri.13574
149. Fisher RA. Cytomegalovirus infection and disease in the new era of immunosuppression following solid organ transplantation. Transpl Infect Dis. (2009) 11(3):195–202. doi: 10.1111/j.1399-3062.2009.00372.x
150. Hecking M, Sharif A, Eller K, Jenssen T. Management of post-transplant diabetes: immunosuppression, early prevention, and novel antidiabetics. Transpl Int. (2021) 34(1):27–48. doi: 10.1111/tri.13783
151. Gijsen VM, Hesselink DA, Croes K, Koren G, de Wildt SN. Prevalence of renal dysfunction in tacrolimus-treated pediatric transplant recipients: a systematic review. Pediatr Transplant. (2013) 17(3):205–15. doi: 10.1111/petr.12056
152. Brum S, Nolasco F, Sousa J, Ferreira A, Possante M, Pinto JR, et al. Leukopenia in kidney transplant patients with the association of valganciclovir and mycophenolate mofetil. Transplant Proc. (2008) 40(3):752–4. doi: 10.1016/j.transproceed.2008.02.048
153. Howsare M, Jones CM, Ramirez AM. Immunosuppression maintenance in vascularized composite allotransplantation: what is just right? Curr Opin Organ Transplant. (2017) 22(5):463–9. doi: 10.1097/MOT.0000000000000456
154. Milek D, Reed LT, Echternacht SR, Shanmugarajah K, Cetrulo CL, Lellouch AG, et al. A systematic review of the reported complications related to facial and upper extremity vascularized composite allotransplantation. J Surg Res. (2023) 281:164–75. doi: 10.1016/j.jss.2022.08.023
155. Kotton CN, Torre-Cisneros J, Aguado JM, Alain S, Baldanti F, Baumann G, et al. Cytomegalovirus in the transplant setting: where are we now and what happens next? A report from the international CMV symposium 2021. Transpl Infect Dis. (2022) 24(6):e13977. doi: 10.1111/tid.13977
156. Murray JE. Organ transplantation (skin, kidney, heart) and the plastic surgeon. Plast Reconstr Surg. (1971) 47(5):425–31. doi: 10.1097/00006534-197105000-00003
157. Cendales LC, Kanitakis J, Schneeberger S, Burns C, Ruiz P, Landin L, et al. The banff 2007 working classification of skin-containing composite tissue allograft pathology. Am J Transplant. (2008) 8(7):1396–400. doi: 10.1111/j.1600-6143.2008.02243.x
158. Robbins NL, Wordsworth MJ, Parida BK, Kaplan B, Gorantla VS, Weitzel EK, et al. Is skin the most allogenic tissue in vascularized composite allotransplantation and a valid monitor of the deeper tissues? Plast Reconstr Surg. (2019) 143(4):880e–6e. doi: 10.1097/PRS.0000000000005436
159. Lee WP, Yaremchuk MJ, Pan YC, Randolph MA, Tan CM, Weiland AJ. Relative antigenicity of components of a vascularized limb allograft. Plast Reconstr Surg. (1991) 87(3):401–11. doi: 10.1097/00006534-199103000-00001
160. Oda H, Ikeguchi R, Aoyama T, Ohta S, Noguchi T, Kaizawa Y, et al. Relative antigenicity of components in vascularized composite allotransplants: an experimental study of microRNAs expression in rat hind limb transplantation model. Microsurgery. (2019) 39(4):340–8. doi: 10.1002/micr.30408
Keywords: face transplant, hand transplant, vascularized composite allograft (VCA), immunosuppressive therapy, outcome
Citation: Huelsboemer L, Boroumand S, Kochen A, Dony A, Moscarelli J, Hauc SC, Stögner VA, Formica RN, Pomahac B and Kauke-Navarro M (2024) Immunosuppressive strategies in face and hand transplantation: a comprehensive systematic review of current therapy regimens and outcomes. Front. Transplant. 3:1366243. doi: 10.3389/frtra.2024.1366243
Received: 5 January 2024; Accepted: 21 February 2024;
Published: 6 March 2024.
Edited by:
Palmina Petruzzo, University of Cagliari, ItalyReviewed by:
Franka Messner, Medical University of Innsbruck, AustriaJérôme Duisit, Centre Hospitalier Universitaire (CHU) de Rennes, France
© 2024 Huelsboemer, Boroumand, Kochen, Dony, Moscarelli, Hauc, Stögner, Formica, Pomahac and Kauke-Navarro. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Martin Kauke-Navarro a2F1a2UtbmF2YXJyby5tYXJ0aW5AeWFsZS5lZHU=
†These authors have contributed equally to this work and share first authorship
‡These authors have contributed equally to this work and share last authorship
Abbreviations AKI, acute kidney injury; AMR, antibody-mediated rejection; CKD, chronic kidney disease; CMV, cytomegalovirus; DIC, disseminated intravascular coagulation; EBV, epstein-barr virus; fVCA, facial vascularized composite allotransplant; GI, gastrointestinal; GvHD, graft vs. host disease; HPV, human papillomavirus; HSV, herpes simplex virus; IL, interleukin; IS, immunosuppressant; IVIg, intravenous immunoglobulin; mAb, monoclonal antibody; MMF, mycophenolate mofetil; MPA, mycophenolic acid; POD, postoperative days; POM, postoperative month; POW, postoperative week; POY, postoperative year; PRISMA, preferred reporting items for systematic reviews and meta-analysis; SOT, solid organ transplantation; TB, tuberculosis; TCMR, T-cell mediated rejection; UTI, urinary tract infection; VCA, vascularized composite allotransplantation; VZV, varicella zoster virus; %, percent.