
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Transplant. , 15 September 2023
Sec. Cell and Stem Cell Transplantation
Volume 2 - 2023 | https://doi.org/10.3389/frtra.2023.1251112
This article is part of the Research Topic Rising Stars: Cell and Stem Cell Transplantation 2022 View all 5 articles
 Francesca Gottardi1,†
Francesca Gottardi1,† Davide Leardini1,†
Davide Leardini1,† Edoardo Muratore1
Edoardo Muratore1 Francesco Baccelli1*
Francesco Baccelli1* Sara Cerasi1Francesco Venturelli1
Sara Cerasi1Francesco Venturelli1 Andrea Zanaroli1Tamara Belotti1Arcangelo Prete1
Andrea Zanaroli1Tamara Belotti1Arcangelo Prete1 Riccardo Masetti1,2
Riccardo Masetti1,2
Systemic steroids are still the first-line approach in acute graft-versus-host disease (aGvHD), and the backbone of chronic GvHD management. Refractoriness to steroid represent a major cause of morbidity and non-relapse mortality after hematopoietic stem cell transplantation (HSCT). In both backgrounds, several second-line immunosuppressive agents have been tested with variable results in terms of efficacy and toxicity. Solid evidence regarding these approaches is still lacking in the pediatric setting where results are mainly derived from adult experiences. Furthermore, the number of treated patients is limited and the incidence of acute and chronic GvHD is lower, resulting in a very heterogeneous approach to this complication by pediatric hematologists. Some conventional therapies and anti-cytokine monoclonal antibodies used in the adult setting have been evaluated in children. In recent years, the increasing understanding of the biological mechanisms underpinning the pathogenesis of GvHD justified the efforts toward the adoption of targeted therapies and non-pharmacologic approaches, with higher response rates and lower immunosuppressive effects. Moreover, many questions regarding the precise timing and setting in which to integrate these new approaches remain unanswered. This Review aims to critically explore the current evidence regarding novel approaches to treat SR-GvHD in pediatric HSCT recipients.
Despite the improvement of transplant platforms and post-transplant immunosuppression, graft-versus-host disease (GvHD) still represents a significant complication following pediatric hematopoietic stem cell transplantation (HSCT) (1–5). The incidence of acute GvHD (aGvHD) in children is approximately 50% of any grade and 20% of grade II-IV, with certain variability based on the characteristics of HSCT (6). About half of patients with grade II-IV aGvHD do not respond to first line steroids, posing a significant challenge for clinicians (7). Chronic GvHD (cGvHD) affects between 6% and 33% of the pediatric patients, with higher incidence after peripheral blood HSCT and most important risk factor represented by previous aGvHD. While mild cGvHD can be managed with topic treatment, systemic steroid, sometimes in addition to calcineurin inhibitors (CNIs) is first-line therapy in patients with moderate/severe GvHD, but, again, only about 50% patients achieve a sustained response (8, 9).
Many treatments have been tested both for acute and chronic steroid-refractory (SR) GvHD based on the increasing understanding of the biological mechanisms underpinning pathogenesis. While aGvHD is caused primarily by donor T cell activation and production of pro-inflammatory cytokines, cGvHD involves both B and T cells, macrophages, and dendritic cells (DCs) converging in activating pro-fibrotic pathways (2). Introduction of therapies targeting cytokines and T cell activation pathways in aGvHD, besides both B and T cells in cGvHD, allowed to reach higher response rates with lower immunosuppressive effects (10). Indeed, among these, the JAK inhibitor ruxolitinib modified the current approach to SR acute and chronic GvHD, being the first drug FDA and EMA approved in patients aged over 12 years for these indications (11). Moreover, BTK inhibitor ibrutinib further renewed this landscape, being the first FDA-approved for refractory cGvHD fully indicated in pediatric patients. However, there are no prospective trials comparing second-line treatments or consensus guidelines for managing SR in both chronic and acute GvHD (12). Moreover, many questions regarding the precise timing and setting in which these new approaches can be integrated remain unanswered. The evaluation of different treatments for GvHD in the pediatric setting poses peculiar problems and questions. Firstly, the number of pediatric patients receiving HSCT and developing SR GvHD is lower compared to adults, resulting in a smaller cohort of treated patients with consequent delays in drug approvals. Moreover, the biology of immune cell recovery after HSCT and the GvHD development present some differences between adults and children raising questions on the different efficacy of the same drug in the two cohorts (13, 14). Lastly, children present peculiar clinical presentation of GvHD, different pharmacokinetics and unique disease that results in different GvHD presentation and response. This review aims to criticallyexplore the current evidence on novel approaches to treat SR GvHD in pediatric HSCT recipients (summarized in Figure 1) underlying the current area of research and future perspectives.
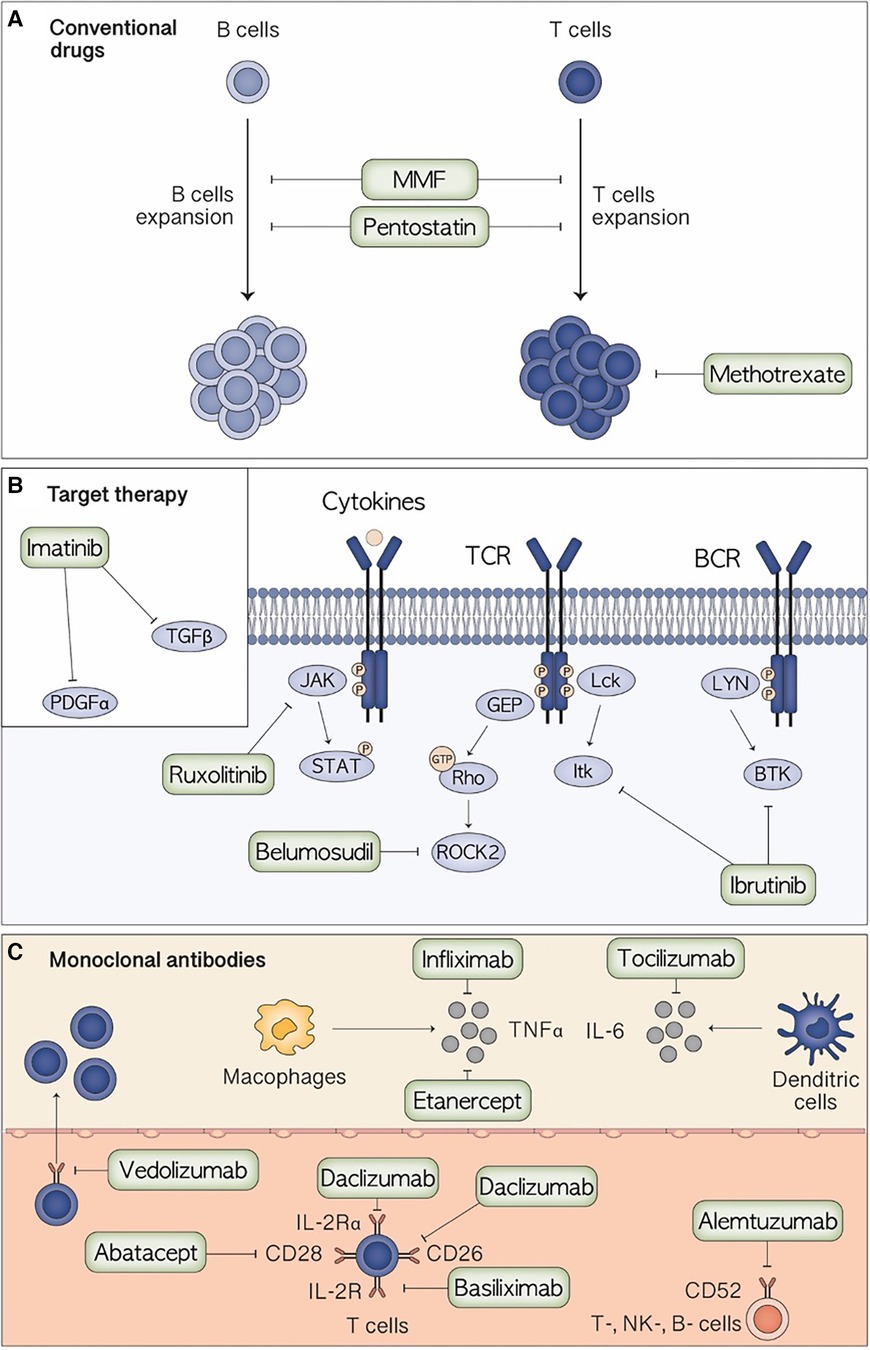
Figure 1. Mechanism of action of the main therapeutic agents for the treatment of pediatric steroid-resistant acute graft-versus-host disease.
Methotrexate (MTX) is an antifolate used at low doses for its anti-inflammatory and immunomodulatory effects: it induces a sustained suppression of T-cell activation and inhibits the production of several inflammatory cytokines that play an important role in the GvHD pathogenesis. Low-dose MTX is commonly used in GvHD prophylaxis, but evidence for its use in the treatment of GvHD is scarce, especially in the pediatric population. The main toxicities are cytopenia and nephrotoxicity. Two pediatric retrospective studies by Inagaki et al. evaluated low-dose MTX as a salvage treatment for steroid refractory and dependent acute and chronic GvHD (cGvHD), finding it tolerable and effective in reducing the dose of steroids without increasing the risk of opportunistic infections. Among 23 patients with SR aGvHD, 37% achieved complete response (CR) and 9% achieved partial response (PR) within 4 weeks without any additional agents. Resolution of aGvHD manifestations in each evaluable organ was observed in 52% with skin aGvHD and in 35% with GI aGvHD. Severe neutropenia was observed in 26% patients and thrombocytopenia in 49%. Fatal infectious complications occurred in 9% of patients. Overall response reported in pediatric cGvHD patients was 58.8% (15) (Table 1). Adult and pediatric retrospective studies were reviewed by Nassar et al. in 2014, estimating in aGvHD an overall response rate (ORR) of 69.9%, and in cGvHD 77.6%. Predictors of better response were lower grade GvHD, cutaneous involvement, and isolated organ involvement (20).
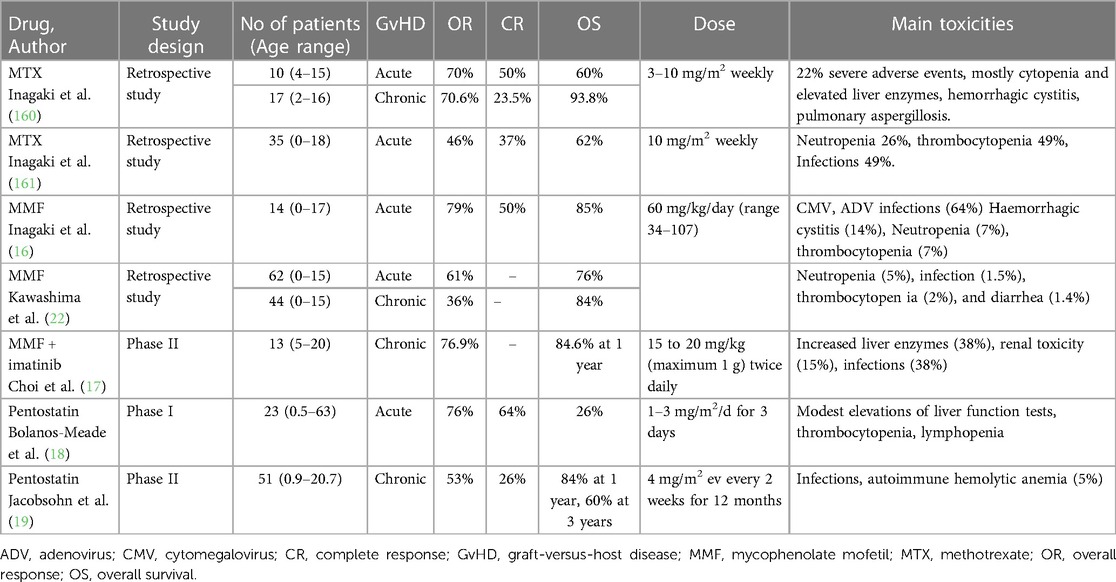
Table 1. Main pediatric studies on conventional drugs for the treatment of pediatric steroid-resistant acute graft-versus-host disease.
Mycophenolate Mofetil (MMF) is the prodrug of mycophenolic acid (MPA). After oral administration MMF is rapidly absorbed and hydrolyzed to MPA, which blocks the pathway of purine synthesis in lymphocytes by selectively and reversibly inhibiting inosine monophosphate dehydrogenase, thus suppressing T and B-cells proliferation (15, 21). MMF has been used as a component of GvHD prophylaxis regimens and as a salvage treatment for refractory aGvHD and cGvHD, with limited evidence in the pediatric population. Inagaki et al. (16) retrospective study in 2015 evaluated the efficacy of MMF in a cohort of 14 pediatric patients with SR aGvHD. At 4 weeks, 50% achieved CR, up to 79% at 8 weeks. Remarkably, favorable responses were observed in most cases of gastrointestinal (GI) aGvHD. The median maximum dose of MMF given to patients was 60 mg/kg/day divided in two doses, higher than previous studies, as poor absorption of MPA was presumed due to most of the patients suffering severe gut involvement. The most common adverse reactions during treatment were opportunistic infections and cytopenia. A Japanese retrospective study in 2018 by Kawashima et al. (22) evaluated MMF in combination with other immunosuppressive therapies. Sixty-two children were treated for steroid or steroid + CNI refractory aGvHD, with an ORR of 61%. Improvement of skin involvement was observed in 65%, intestine in 27%, and liver in 8% of patients. Combined immunosuppressants were reduced in 57% and discontinued in 18% patients. In the same study, a total of 44 children received MMF for the treatment of refractory cGvHD, of which 36% had improved subjective symptoms. Concomitant immunosuppressants were reduced in 41% and discontinued in 24% patients. Major adverse events were registered in <5% of patients and were mainly neutropenia, infection, thrombocytopenia, and diarrhea. In this study MMF seems to be less toxic in children when compared with adults, as regards renal damage (22). Choi et al. in 2021 evaluated the efficacy and safety of imatinib + MMF to treat sclerotic/fibrotic type cGvHD. A total of 13 patients were enrolled, aged 5–20 years. At 1 year, 1 patient achieved CR and 8 patients achieved PR, with an ORR of 76.9%. The highest response rate was observed in the liver, namely 70%, and the lowest in the lungs and GI tract, 41.7% and 33.3%, respectively. The median steroid dose was decreased from 1.0 to 0.21 mg/kg/day. Common adverse events included elevated liver enzymes and serum creatinine levels, and fever (17) (Table 1).
Pentostatin is a nucleoside analog that irreversibly inhibits adenosine deaminase, blocking the metabolism of 2′-deoxyadenosine, with consequent accumulation of dATP that slows lymphocyte growth and causes apoptosis (18). Pentostatin has a reasonable toxicity profile, and its side effects include thrombocytopenia, neutropenia, renal toxicity, increased hepatic liver enzymes and infections (18–25). Bolanos-Meade et al. evaluated in a phase I dose escalation study pentostatin at a dose of 1–3 mg/m2/day for 3 days to treat 23 pediatric and adult patients with SR aGvHD. ORR was 86% and CR 64% (18). Jacobsohn et al. evaluated in a phase II prospective study 51 pediatric patients with SR cGvHD, who presented a 53% ORR. Patients with rash/lichenoid changes or sclerosis had a better response rate, 50% and 59% respectively, while none of the patients with liver or lung involvement responded to this treatment (19). The results were similar to those obtained in the adult population (26). The toxicities observed were mostly infectious, but also included 3 cases of autoimmune hemolytic anemia (19) (Table 1). More studies have been conducted in the adult population, both alone and in combination, with very variable responses, and CR achieved from 13% to 70% (23, 27, 28).
Imatinib is a tyrosine kinase inhibitor widely evaluated in cGvHD. By inhibiting both platelet-derived growth factor a (PDGFa) and transforming growth factor beta (TGFbeta) intracellular signaling. Imatinib has proved to be effective in patients with cGvHD with sclerotic/fibrotic features (17, 29). Side effects observed include transaminase elevation, renal toxicity, infections, myelosuppression, and edema because of fluid retention (17, 30). Faraci et al. retrospectively studied the use of imatinib as second-line treatment of bronchiolitis obliterans in 13 children, together with CSA, tacrolimus, and methylprednisolone pulses, with an ORR of 76.9%, CR 30.8% and PR 46.1%, and an overall survival (OS) at 4 years of 83.3%, compared to 42.6% in the group without imatinib (31). As already described above, Choi et al. treated 13 pediatric patients with SR or dependent cGvHD with fibrotic/scleroderma-like features with imatinib and MMF (17) (Table 2).
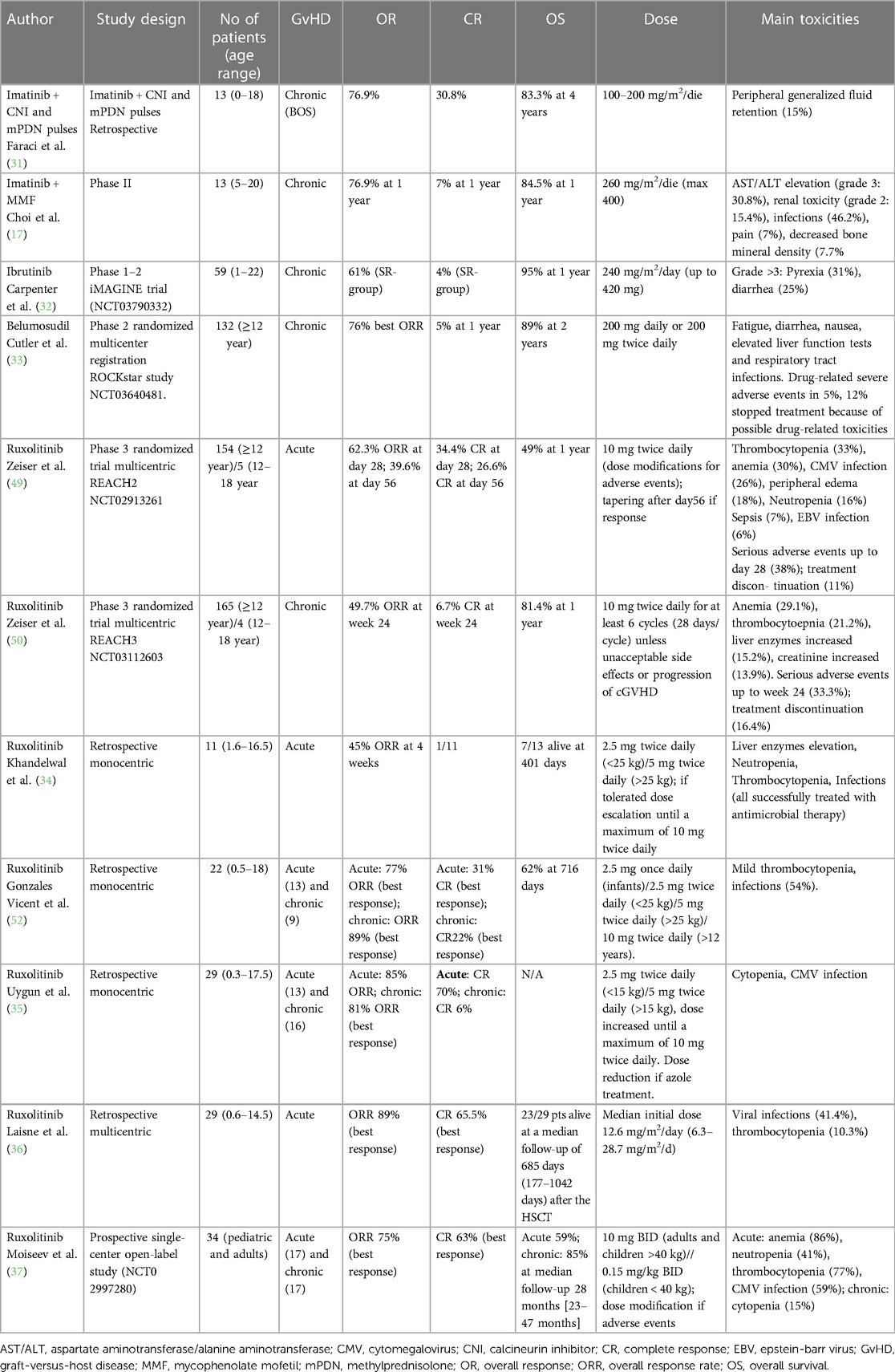
Table 2. Main pediatric studies on targeted therapy for the treatment of pediatric steroid-resistant acute graft-versus-host disease.
Ruxolitinib is an oral selective Janus kinase (JAK) 1 and 2 inhibitor, first approved for the treatment of myelofibrosis and polycythemia vera in adults (38). The JAK 1/2 kinases are involved in cellular proliferation and activation, via the activation of STAT signaling (38). This pathway is critical in T-cell function (39) and has been studied as a potential target in immune disorders (40–42), being also involved in GvHD pathogenesis (43). Ruxolitinib was demonstrated to control clinical features of GvHD (44) and demonstrated to preserve the graft vs. leukemia (GvL) effect in preclinical models (45). Subsequently, its use has been tested in adult patients with acute and chronic SR GvHD resulting to be both effective and safe (46, 47). The prospective trial REACH1 (NCT02953678), an open-label, single-arm, multicenter trial of ruxolitinib in patients 12 years and older with SR and steroid-dependent aGvHD showed an ORR at any time of 73,2% with CR of 56.3% (11, 48). Two multicenter, randomized, open-label, phase 3 trials, REACH2 (NCT02913261) and REACH3 (NCT03774082), confirmed the efficacy of ruxolitinib in acute and chronic SR GvHD, respectively. OR resulted higher than best available therapies, namely 62% vs. 39% for 28 days aGvHD response, and 49% vs. 26% for cGvHD response after 24 weeks. Failure-free survival was also higher in the ruxolitinib group (11, 49). Based on these results, ruxolitinib was thus approved for the treatment of SR acute and chronic GvHD in patients >12 years by the FDA in 2019 and subsequently by EMA (50). Pediatric studies on the use of ruxolitinib in GvHD have been increasingly reported worldwide in recent years. In the under-12-years age group, ruxolitinib has been used off-label for SR GvHD. Eleven studies evaluated children with aGvHD treated with ruxolitinib were available (34–57). Results of most relevant pediatric studies are summarized in Table 2. ORR to ruxolitinib varies from 45% to 100% and CR from 9% to 67,5%. Treatment failure (TF) was reported in a range of 17%–36% and non-response (NR) varies from 0% to 25%. The NCT02997280 prospective study by Moiseev et al. showed in multivariate analysis a lower response rate in grade III-IV, liver and grade IV GI aGvHD, while no transplantation or donor characteristics were associated with response (37). Among 29 children in the report by Laisne et al, no association of baseline characteristics, GvHD characteristics or previous immunosuppressive therapies with response to ruxolitinib was found (36). Nine studies described treatment with ruxolitinib in children with SR cGvHD (10, 35, 51, 53–58). ORR was variable from 50% to 100%, with CR from 0 to 28%. In the prospective study NCT02997280, none of the transplantation and donor characteristics were predictive for response (37). Generally favorable response rates were reported for lung GvHD/bronchiolitis obliterans (50%–90%) (10). Studies describing the use of ruxolitinib in children, generally show a good toxicity profile. Cytopenia represented the most frequent complication, mainly neutropenia and thrombocytopenia, ranging from 0 to 69% and 0 to 67%, respectively, but generally of low-moderate grade. Liver toxicity was also frequent but rarely was cause of the treatment discontinuation. Infections were also common, including bacterial, viral, and fungal infections, with few severe cases reported, including sepsis and adenovirus infections. Notably, CMV reactivation was common during ruxolitinib administration, but no CMV-related death was documented. Importantly, REACH4 (NCT03491215), a phase 1/2 open-label, single-arm, multicenter clinical trial is ongoing to evaluate addition of ruxolitinib to steroid therapy in pediatric patients with grade II-IV treatment-naïve or SR aGvHD. In a preliminary analysis on 32 patients with SR aGvHD, a OR at day 28 was 90.6% and OR at day56 was 68.8% (59).
Ibrutinib is a selective and irreversible Bruton's Tyrosine Kinase (BTK) inhibitor. BTK is predominantly expressed in B cells and its activation is critical for B-cell survival, proliferation, and migration. Ibrutinib has been originally used in B-cell malignancies, as it arrests cell growth and induces apoptosis. Thus, ibrutinib is FDA and EMA approved for chronic lymphocytic leukemia and relapsed/refractory mantle cell lymphoma (60) In addition to inhibiting BTK, ibrutinib is an irreversible inhibitor of Interleukin-2 inducible Tyrosine Kinase (ITK), involved in T-cell receptor signaling and activation, cytokine release, and proliferation (61). Ibrutinib was identified as a potential treatment for cGvHD, characterized by chronic inflammatory responses driven by alloreactive T-cells, pro-fibrotic pathways, and B-cells produced anti-host antibodies (62). A phase 2 clinical trial by Standford University in 2017 culminated in the FDA approval of ibrutinib as second line therapy for SR cGvHD in adults (63). A few years later, in 2022, ibrutinib received its approval in the US for its use in pediatric patients of 1 year and older with cGvHD after the failure of one or more lines of systemic therapy. Ibrutinib thus represents the first ever approved treatment in this specific group of patients (32, 64). Efficacy as a treatment for moderate or severe cGvHD was demonstrated in 59 patients aged 1–22 years after the failure of one or more lines of systemic therapy and in those who were newly diagnosed and previously untreated (64). In the overall population, a sustained response for ≥20 weeks was seen in 61% of those who had achieved a partial or complete response. The 12- and 18-month OS estimates in the overall population were 95% and 91%, respectively. Improvement occurred in multiple organ systems and responses lasted ≥5 months in half of the patients. Response to ibrutinib permitted reduction of glucocorticoid dose to ≤0.15 mg/kg/day in nearly two-thirds and was associated with improved quality of life. The most common adverse reactions with ibrutinib in the overall population were pyrexia (31%) and diarrhea (25%) (Table 2). Gagliardi et al. recently reported a small experience of combination therapy of ibrutinib with ruxolitinib for steroid refractory cGvHD in two pediatric patients and found this combination to be well tolerated with no significant adverse events for neither patient had to discontinue these drugs (65).
Targeted approaches that directly address inflammation and fibrosis associated with cGvHD have been developed. The rho-associated coiled-coil-containing protein kinase-2 (ROCK2) promotes the production of the proinflammatory cytokines IL-21 and IL-17, downregulates STAT5 inhibiting Treg differentiation and upregulates profibrotic gene expression (66, 67). The oral Selective ROCK2 inhibitor Belumosudil, previously known as KD025, exerts multiple effects in vitro and in preclinical models by inhibiting IL-21, IL-17, and IFNγ secretion, reducing Th17 and follicular helper cells via downregulation of STAT3, and enhancing regulatory T cells via upregulation of STAT5. It also seems to inhibit fibroblast proliferation and collagen production and reduce profibrotic M2 macrophage differentiation (68, 69). In the murine model, ROCK2 inhibition was effective in ameliorating sclerodermatous cGvHD and bronchiolitis obliterans by modulating the immune system and reducing lung and skin fibrosis (69). These promising data lead to the design of two phase 2 trials. In the phase 2 dose-finding trial including only patients older than 18 years, belumosudil treatment with 200 mg daily or twice daily resulted in a OR of 65% and 69% respectively, and it was associated with significant corticosteroid dose reduction (70). The ROCKstar phase 2 randomized multicenter registration study included patients of 12 years and older to evaluate belumosudil 200 mg daily or twice daily in patients non responder to 2 to 5 prior lines of therapy. The primary endpoint was best ORR. The trial enrolled 132 subjects, with a median follow-up of 14 months. belumosudil 200 mg daily or twice daily resulted in a the best ORR of 74% and 77% respectively, with a median duration of response of 54 weeks. Response rates were high in all affected organs and even after failure of ibrutinib and/or ruxolitinib. Patient-reported symptom reduction was also reported in 59% and 62%, respectively. Belumosudil was well tolerated in these heavily pretreated subjects, with 44% of patients continuing treatment for more than 1 year. Toxicities mostly consisted of fatigue, diarrhea, nausea, elevated liver function tests and respiratory tract infections. Drug-related severe adverse events occurred in 5% of subjects, and 12% discontinued belumosudil because of possible drug-related toxicities (33). This trial led to FDA approval for adult or pediatric patients 12 years and older with chronic GvHD after the failure of at least 2 prior lines of systemic therapy, with a starting dose of 200 mg orally once daily (67). To date, belumosudil has not been approved by EMA yet. A combined analysis from 2 prospective trials outlined best ORR for lung cGvHD of 32%, with CR of 15%. Response rates were inversely proportional to baseline National Institute of Health NIH GvHD lung score at enrollment (71). Interestingly, the introduction of belumosudil in the care of cGvHD has been associated with substantial cost savings in the US, mainly due to reduced adverse events and less healthcare resource utilization (72).
Basiliximab, a chimeric monoclonal antibody, binds to the interleukin-2 receptor on activated cytotoxic T-cells, inhibiting lymphocyte proliferation, and reducing tissue damage, and has been considered as a treatment option for SR aGvHD in adults (73–77). Studies in the pediatric population are lacking. To date, studies including both children and adults showed good results in retrospective cohorts (75–78). A pediatric only study was carried on by Tang et al. the setting of SR-aGvHD in haploidentical HSCT. The authors retrospectively reviewed 100 patients with an ORR at day 28 of 85%, and CR in 74% of cases. OS was significantly higher in responders compared to non-responders, 81% vs. 47%. Basiliximab was well tolerated without any infusion-related side effects. CMV reactivation was the most common infection during treatment, occurring in 53% of patients, while 11% and 7% developed bacterial and fungal infections, respectively. These rates were comparable to the ones of adults (78). Daclizumab is a humanized monoclonal antibody directed vs. IL-2Ralpha. It has been tested in a prospective study in children with SR GI aGvHD with a ORR of 85%. Treatment was well tolerated, but infections were common. Four patients subsequently developed cGvHD (79). Miano et al. described 13 pediatric patients treated with daclizumab for SR aGvHD with CR 46% and ORR 92%. Even in this study, 50% of patients developed cGvHD (80) (Table 3).
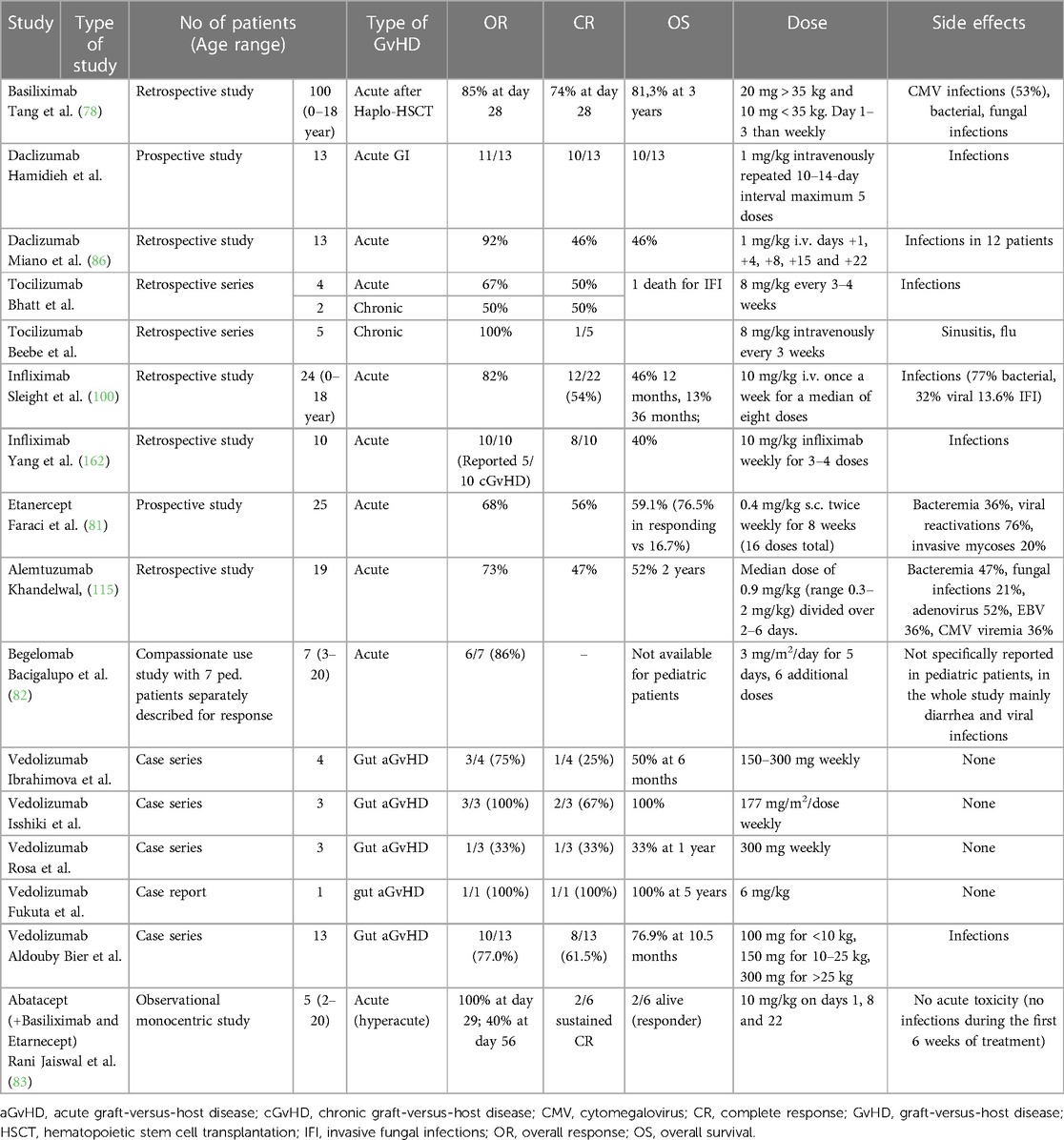
Table 3. Main pediatric studies on anti-cytokines and monoclonal antibodies for the treatment of pediatric steroid-resistant acute graft-versus-host disease.
TNFα is a key cytokine in the inflammatory cascade of GvHD. Secreted alongside interleukin-1 by macrophages residing in the host's mucosae, TNF-α triggers the proliferation of donor T-cells and stimulates the secretion of interleukin-2 and interferon-α, resulting in the amplification of T-lymphocytes and mononuclear phagocyte responses. The damage inflicted upon the intestinal mucosa facilitates the translocation of lipopolysaccharides from the normal bowel flora and other immune-stimulatory molecules from the intestinal lumen into the bloodstream. This, in turn, propagates the characteristic cytokine storm observed in aGvHD (84). Furthermore, TNFα and soluble TNFα receptor I and II have been shown to be correlated with aGvHD severity (85, 86). Thus, the use of TNFα inhibitors to manage GvHD have been suggested in the primary prophylaxis (87, 88), in first-line treatment (89, 90) and in SR aGvHD.
Infliximab is a chimeric human-murine IgG1κ monoclonal antibody that binds to the soluble and transmembrane isoforms of TNF-α and inhibits their binding with the cellular receptors (91). Its potential role in the treatment of SR GvHD has been explored since the early 2000s (92, 93). In the pediatric setting, Sleight et al. reported that weekly infusions of infliximab at the dose of 10 mg/kg are effective for children with both acute and chronic refractory GvHD, especially for children with skin and gut involvement (94) with an ORR of 82%. Nevertheless, long-term outcome was less satisfying, with common recurrence of GvHD upon discontinuation of infliximab and a significant number of infections within 100 days of the final dose, up to 77% bacterial, 32% viral and 13.6% probable proven invasive fungal infections (94). In Yang et al. experience, 10 pediatric patients with SR aGvHD were treated with a CR rate of 80%. However, infections were reported in all patients, 5 viral infections, 2 atypical mycobacterial infections. 3 invasive pulmonary aspergillosis, and 6 patients had multiple infections. Moreover, 50% developed cGvHD, 60% died during follow-up. A recent multicentric study on treatment of pediatric SR aGvHD reported that infliximab was the second most utilized therapy, in 30%, but in half of the cases was utilized in combinations with other agents, such as vedolizumab, basiliximab, etanercept, tacrolimus and/or ruxolitinib (95). Finally, infliximab-daclizumab combination was used to treat acute and chronic liver and GI SR GvHD in two children, with complete response in both (96). The use of infliximab in chronic GvHD has been less explored, with no relevant studies particularly in pediatric patients.
Etanercept is a recombinant human soluble dimeric TNFα receptor fusion protein that binds and inactivate TNFα. Most experiences in the use of Etanercept for GvHD treatment were gathered from cohort of adults (97, 98), with few reports on children alone. In adults, responses in gut SR aGvHD have been described, but appear to be associated with poor long-term survival even in responding patients (99). Notably, Faraci et al. prospectively evaluated use of etanercept in 25 children with SR aGvHD, concluding an ORR of 68% (81). It must be mentioned that clinically significant infectious complications requiring systemic treatment occurred in 68% of patients, mainly bacterial and viral reactivations. OS was 77% in responders and 17% in non-responders (Table 3).
Tocilizumab is a humanized monoclonal antibody against the inflammatory cytokine IL-6. Since GvHD is characterized by dendritic cell driven IL6 dysregulation after HSCT (100), tocilizumab has been proposed for treatment of both acute and chronic GvHD. In adults, a CR rate of 63% was reported in patients affected by SR low GI aGvHD (101) and an OR rate of 70% was reported in patients with extensive cGvHD (102). In a retrospective pediatric series, tocilizumab was administered to 6 patients with SR aGvHD and 2 with cGvHD every 3 to 4 weeks. Infections were the primary adverse events associated with tocilizumab administration. OR was 67% in aGvHD and ½ patient with cGvHD had a significant response to therapy, whereas the second had stabilization of disease that allowed for a modest reduction in immune suppressive medications. Beebe et al. reported 5 children and young adults with cGvHD treated with tocilizumab. All patients reported subjective improvement of cGvHD, reducing use of additional immunosuppression by >50%, and one patient discontinued steroids after 5 years of dependency. Treatment was affected by mild infections. Interestingly, four patients had normal IL-6 levels prior to starting treatment (103, 104) (Table 3).
Alemtuzumab (Campath-1H) is a humanized IgG1 monoclonal antibody that binds cells expressing the CD52 antigen, such as T-, NK-, and B-lymphocytes as well as a proportion of monocytes and dendritic cells (105). The effect produces an in vivo lymphocyte depletion; thus, this molecule has been commonly adopted in HSCT conditioning to promote engraftment and prevent GvHD. Even if its use is less frequent in pediatric HSCT as alternative to serotherapy in aGvHD prohylaxis, it has been used especially in reduce-intensity conditioning (RIC) and nonmalignant disease setting. Successful use of Alemtuzumab for SR aGvHD has been reported from case series including adult patients (106–108). Generally, responses were remarkable, but virus reactivation and bacterial infections were common. Also, subsequent development of chronic GvHD was observed frequently. In pediatric patients, a retrospective study reviewed 19 patients with SR aGvHD who received alemtuzumab with 47% CR and an ORR of 73%. Infectious complications were reported in OS was significantly higher in patients treated (52% vs. 0% at 2 years) (108) (Table 2).
Begelomab is a murine IgG2B monoclonal antibody directed against the CD26 surface antigen, which promotes T cell migration. Accumulation of CD26+ T cells has been proven in GVHD target organs (109). Bacigalupo et al. reported on a cohort of 69 adult patients treated with begelomab with different treatment schedules in combination with cyclosporin and steroids for steroid refractory acute GvHD. In both the prospective and compassionate groups, responses to treatment at day 28 were 75% and 61%, respectively. Responses for grade III GvHD were recorded in 83% and 73% of patients, while responses for grade IV GvHD were recorded in 66% and 56% of patients in the two groups, respectively. Interestingly, favorable responses were reported for skin, liver, and gut stage III–IV GvHD, with 64%, 56%, 68% of responses respectively. Notably, in a small subgroup of patients under 20 years of age, 87% showed response to treatment, compared to 57% and 68% in patients aged 21–40 and over 40 respectively (82). While the use of begelomab for aGvHD shows promising results, there is no clinical trial investigating the effect of begelomab in patients with cGvHD. However, preclinical models have shown that CD26 may play a role in the development of pulmonary cGvHD, and that treating human umbilical cord blood transplanted mice with the fusion protein caveolin-1-Ig, prevents the development of pulmonary cGvHD in these mice (109) (Table 3).
Vedolizumab, a monoclonal antibody targeting α4β7 integrin, has emerged as a potential therapeutic option for the management of pediatric SR GvHD. Its mechanism of action involves inhibiting of the trafficking of gut-homing lymphocytes to the gastrointestinal tract and it was first tested in ulcerative colitis and Crohn's disease (110). In the HSCT context, preclinical studies demonstrated that loss of α4β7 integrin may prevent intestinal GvHD (111) and, based on these results, was tested in patients. In adults, a Phase II study (NCT02993783) revealed low efficacy and a poor response rate, leading to the premature discontinuation of the study (112). However, other reports have shown more positive outcomes, with response rates around 27% (113). Limited evidence exists for the use of vedolizumab in children, which mainly consists of retrospective case reports or case series. Ibrahimova et al. reported four patients with SR grade III-IV gut aGvHD, out of which only 1 achieved a complete response (114). Isshiki et al. described 3 pediatric patients with grade II-IV gut acute gut GvHD who were treated with vedolizumab. Two of these patients experienced a complete response (115). Rosa et al. reported 3 pediatric patients with oncological diseases and grade IV gut aGvHD, of whom only one achieved GvHD remission and Fukuta et al. reported 1 patient with a clinical response to vedolizumab (116, 117). Aldouby Bier reported on 13 pediatric patients with SR gut aGvHD treated with vedolizumab, among whom 8 presented a clinical recovery and 2 had ongoing chronic colitis. Interestingly, these patients experienced several infectious episodes primarily associated with intestinal bacteria, which raises some potential safety concerns (Table 3).
Abatacept or cytotoxic T-cell-lymphocyte-4 (CTLA4)-immunoglobulin, is a fusion protein between the extracellular domain of human CTLA4 and a modified Fc region of human IgG. It inhibits the co-stimulation of T-cells by blocking the interaction between CD28 and CD80/CD86 on antigen-presenting cells (118). Abatacept has been initially approved for the treatment of rheumatoid arthritis (119). The drug resulted able to prevent GvHD in preclinical models (120). A Phase 2 clinical trial demonstrated the safety and efficacy of abatacept in preventing aGvHD (121). Other studies have also showed the feasibility of this approach in different pediatric settings (122, 123). Abatacept has been FDA-approved for aGvHD prophylaxis (combined with a calcineurin inhibitor and MTX) in patients undergoing unrelated donor HSCT. Reports about the use of Abatacept for treatment of GvHD are limited, particularly in children. In a report on children who have received a haploidentical HSCT with post-transplant cyclophosphamide based GvHD prophylaxis, abatacept was added to etarnecept and basiliximab in 5 children with hyperacute SR GvHD reporting an overall response at day 29 and day 56 of 100% and 40%. Response was higher compared to patients treated with a “standard” protocol including anti-thymocyte globulins combined with etarnecept and basiliximab, suggesting that T costimulation blockade combined with anticytokine agents can ameliorate the response in this particularly high-risk category of patients (83). Abatacept has been described as salvage therapy in cGvHD in a recent retrospective report on 15 patients with a wide range of age (5–70 years). Abatacept resulted a promising option for cGvHD with a best ORR of 40%, particularly high in patients with bronchiolitis obliterans in which reached 89%. Unfortunately, specific data about pediatric patients treated in this study are not available (124).
Extra-corporeal photopheresis (ECP) therapy is based on exposition of peripheral blood mononuclear cells to photoactivated 8-methoxypsoralen, followed by reinfusion of treated cells, which exert an immunomodulatory effect. Non-exposed antigen presenting cells, can phagocyte treated cells, with consequent secretion of anti-inflammatory cytokines and chemokines, modulation of T cells toward a Th2 phenotype, and Treg regeneration (125). This therapy has been widely explored in SR GvHD, as generally considered a safe and effective strategy, with limited evidence of increased infectious risk in the post HSCT setting. Main limitations are related to logistic feasibility and vascular accesses, which requires patients to be sufficiently stable (126, 127). Moreover, most centers require at least 1 × 109/L WBC in the peripheral blood before initiating the ECP therapy, limiting access to patients with cytopenia, especially in aGvHD setting (128).
The earliest evidence of efficacy of ECP in pediatric aGvHD and cGvHD was reported in 2003 by Messina et al, 33 patients with aGvHD involving skin, liver and gut had CR in 76%, 60% and 75% respectively, and of 44 children with cGvHD, 15 (44%) showed a complete response and 10 (29%) a significant improvement after treatment (129). ECP feasibility and efficacy was subsequently evaluated in various retrospective studies, but the majority involved adult patients, and as a whole, there were no major changes in the technique (125, 130).
More recently, a meta-analysis of prospective clinical trials evaluating ECP in patients with SR aGvHD reported an ORR of 71% each (131). In pediatric population, a retrospective study of 15 patients was reported from Winther-Jørgensen et al. in 2019. In aGvHD group, 67% had ORR at day 28 up to 89% at last session. Among cGvHD patients, 67% reported a PR. Only few procedure-related mild side effects were registered, even in patients with low body weight. The most frequent cause of shortened or canceled ECP treatment was difficulties with vascular accesses (132). In 2022 a retrospective study evaluated a total of 701 ECP sessions performed on 33 children. In total, 97% of the sessions could be performed, while in 8% an incident was detected, most of them mild and related to catheter dysfunction. ORR was 70% with a median time to best response of 2.8 months (133) (Table 4). It has to be mentioned that, in recent years, the potential complementary mechanisms of action of ruxolitinib and ECP has been investigated on both acute and chronic GvHD. Data have been described in adult cohorts, specifically in 18 patients with severe lower GI SR aGvHD, with ORR of 55%. During treatment with ruxolitinib and ECP, an increased level of regulatory T cells could be observed elucidating direct effects of this treatment on immune response (140). In retrospective analysis of 23 patients treated with ruxolitinib-ECP combination as salvage therapy for SR cGvHD, ORR was 74% including 9% CR (141). In both studies main toxicities were non-severe cytopenia and CMV reactivations (139, 141). Data about combination in children lacks.
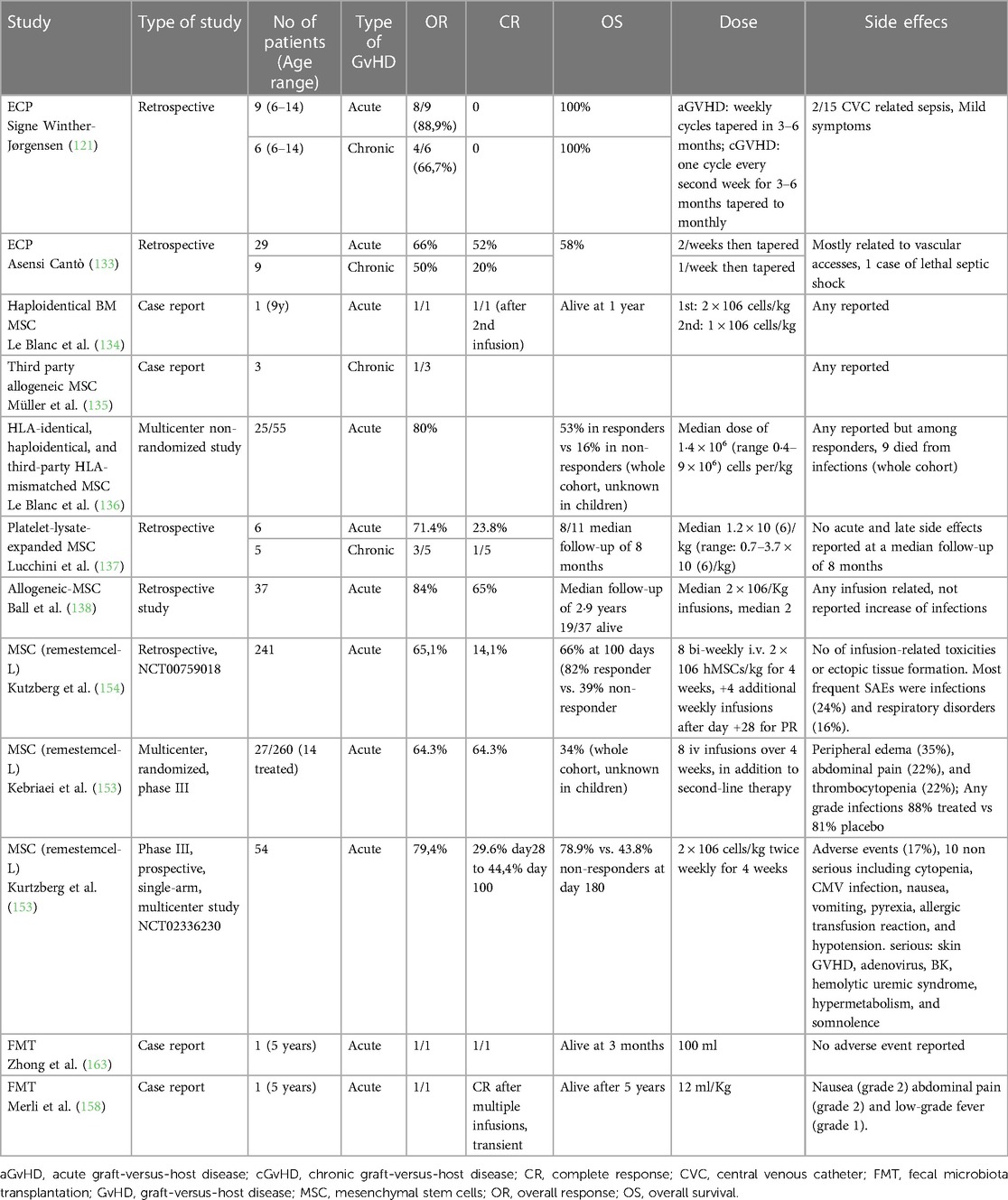
Table 4. Main pediatric studies on nonpharmacological interventions for the treatment of pediatric steroid-resistant acute graft-versus-host disease.
Mesenchymal stromal cells (MSCs) can be isolated from various tissues, such as bone marrow, adipose tissue, umbilical cord, Wharton's jelly, placenta tissue, and decidua. They have shown activity in the treatment of GvHD due to their immunomodulatory properties on T, B and NK cells and capability of influence the differentiation and function of dendritic cells. MSCs release anti-inflammatory molecules, such as IL-10 and TGF-beta, dampening the inflammatory response associated with GvHD. MSC migrate to injured tissues and promote tissue repair and regeneration through their differentiation potential. In the crosstalk with immune system, they exert paracrine activity involving secretion of hormones and peptides, transfer of mitochondria and RNA by nanotubes, microvesicles, and exosomes (142). Specific characteristics and properties of MSCs may vary depending on their origin, variability in MSC donor types, production procedures and dose, as well as variations in study design, thus comparing different products can be demanding as specifically reviewed by Kelly and Rasko in 2021 (143). From the first treatment of a 9-year-old patient with SR aGvHD, achieving CR, reported in 2004 by Le Blanc, numerous studies and clinical trials have been conducted to investigate MSCs as a treatment for GvHD and most included patients with SR-aGvHD (134, 144). In 2008 an EBMT multicenter non-randomized study evaluated MSCs from either HLA-identical, haploidentical or unrelated HLA-mismatched donors in which 25 patients were children, who were found to respond consistently better than adults, with OR 80% vs. 60% in adults (p = 0.28) (136). In 2013 a retrospective analysis of 37 children with grade III-IV SR aGvHD treated with allogeneic MSCs CR of 65% and ORR 84% were reported. Patients with CR after MSC therapy had a cumulative incidence of transplant-related mortality of 17% compared to 69% unresponsive to MSCs (p = 0.001) (138). A multicenter, randomized, phase III clinical trial assessed the use of an industrial MSC product (remestemcel-L, Prochymal) in 260 patients (145), proving safety and tolerability but failing primary clinical endpoint of durable complete response of at least 28 days after beginning treatment in the intent-to-treat population, namely 35% vs. 30% (p = 0.42). Notably, a subset analysis of pediatric patients showed a higher ORR vs. placebo, namely 64% vs. 23% (p = 0.05) [55]. In 2021, an update on 241 pediatric patients with severe SR aGvHD was reported by Kurtzberg et al. Patients received biweekly infusions of 2 million MSCs/kg for four weeks, consistent with the schedule of the previous remestemcel-L trial. A total of 156 patients (65%) presented OR, with 34 (14.1%) achieving CR and 123 (51.3%) achieving PR. Survival through day 100 was 66.9% and was significantly higher in patients with OR on Day 28 than in non-responders, namely 82% vs. 39% (p < 0.001). Infusions were well tolerated, without evidence of infusion-related toxicities or ectopic tissue formation (146). The most frequent severe adverse events were infections, 24% of patients, and respiratory disorders in 16%. Subsequently, in 2021 a phase III, prospective, single-arm, multicenter study in 54 children with primary SR aGvHD was established with OR of 70%. Based on the available evidence, an attempt to obtain FDA approval was submitted to treat children with SR aGvHD with remestemcel-L, including a whole analysis of 309 children with GvHD who received remestemcel-L., but the application was declined, as a specific randomized controlled trial have been requested (146, 147). A limited number of studies have been conducted in cGvHD in adults, with variable OR reported, from 0 to 80%. Pediatric evidence is even scarcer. In 2008 Muller et al. reported 3 patients receiving MSC for extensive cGvHD with partial response in 1 (135). In the work of Lucchini et al. 5 cGvHD patients were included with 1 CR with flare, and 2 PR. Interestingly, in vivo immunomodulation was detected in responsive group (137) (Table 4).
Gut microbiota composition has been linked to major complications in allogeneic allo-HSCT recipients (148–150). In particular, the relative abundance of specific bacterial taxa, such as Enterococcus expansion and reduction in Blautia, has been associated with aGvHD severity (151, 152). Based on this knowledge, various strategies have been developed to modulate the gut microbiota towards a protective configuration, ranging from antibiotic stewardship to nutritional modulation (153–155). Fecal microbiota transplantation (FMT) consists of the infusion of fecal microbiota from a healthy donor and has been proposed to directly restore the altered microbial composition observed in SR GI GvHD (156). In adults, encouraging preliminary data regarding feasibility and efficacy have been published, but larger prospective studies are lacking (157). To date, the use of FMT for steroid-refractory gut aGvHD in children has been reported in two 5-year-old patients. The first description was provided by Zhong et al. in 2019. FMT was performed twice on days +75 and +77 after HSCT via a nasojejunal tube from an unrelated donor and resulted in symptom remission without adverse events. Another case was described by Merli et al. in 2022. The child received FMT from his mother through upper GI endoscopy at a dose of 12 ml/kg on day +78 after HSCT after multiple lines of therapy, reaching complete remission. However, 20 days later the patient experienced gut aGvHD recurrence and underwent a second FMT from the same donor together with Begelomab, slowly reaching again remission of symptoms. About six months later, the patient developed a new flare of intestinal GvHD. The patient did not respond to steroids and mycophenolate and required surgery. Due to the persistence of symptoms, two other FMT infusions were performed from the uncle because of mother's unavailability, without clinical response. The patient then received Ustekinumab, achieving complete remission. At 5 years of follow-up, he was alive and did not present any signs of chronic GVHD, with normal intestinal function (158) (Table 4).
Treatment of SR-GvHD still represents a challenge in pediatric HSCT, particularly for very high-risk groups of severe GI-aGvHD and lung cGvHD/BOS. It is difficult to recommend a linear approach, since for long time most of the available evidence was assumed by retrospective experience, and more recent prospective study are limited by small numbers (4, 139). However, some considerations about indications can be outlined. Conventional drugs are generally affected by wider range of organ toxicity than other classes, especially in aGvHD setting. Nevertheless, an acceptable balance between efficacy and side effects has been reported in low-dose MTX for cGvHD (15, 20), and in MMF and pentostatin for aGvHD (16). Moreover, these drugs are usually easily accessible and manageable for clinicians and since few years ago represented the only choice for SR patients.
Mostly in the last 15 years, the interest to evaluate anti-cytokine therapies has grown, particularly in severe and GI aGvHD. Treatments were often translated from inflammatory bowel disease and autoimmune diseases. Even if a certain grade of activity was documented in terms of response, increase of infection rate was reported by most of the studies (81, 83, 95, 114). Overall survival in treated patients was characterized by lower trend than those observed in other classes of drugs. By a physio pathological point of view, it is worth noting that the inhibition of TNFα or other cytokines involved in GvHD does not directly affect T-cells, therefore GvHD is not eradicated. A similar phenomenon occurs in the other autoimmune diseases such as Chron's or rheumatoid arthritis. In this regard, all studies involving anti-cytokines report subsequent development of chronic GvHD in a non-neglectable percentage of patients.
Recently, introduction of targeted therapies was revolutionary for SR GvHD, reaching the lower rate of adverse events and probably the best efficacy currently available. Indeed, the advent of ruxolitinib has changed the landscape of treatment of SR acute and chronic GvHD. Pediatric experience flourished, reporting efficacy and low rate of treatment toxicity, with rare cases of treatment discontinuation (34–57). Results of the pivotal trial REACH4 (NCT03491215) will define if ruxolitinib use is destined to be introduced earlier in clinical practice, thus defining a novel concept of refractory GvHD. Furthermore, cGvHD setting has been renewed by introduction of ibrutinib. Brilliant response rates counterbalanced by a remarkably low burden of toxicity lead ibrutinib to be the first pediatric FDA-approved molecule for SR cGvHD. Promising results may also be obtained in patients with lung GvHD/BOS.
Finally, the class of non-pharmacological treatments comprise different approaches that share promising activity with relatively low toxicity but less feasibility than other therapies. ECP has been introduced since longer time in clinical practice, even if evidences in pediatric patients have been supported by only few retrospective studies (132, 162). Worst response was reported in severe aGvHD. Combination with ruxolitinib may be promising and allow to a higher rate of complete responses (139, 141). Use of MSCs has widespread in recent years (142, 143). Requirement of Good Manufacturing Practices (GMP) fulfillment for production represents a limitation for the diffusion of this approach, partially overcome by introduction of the industrial product remestemcel-L. The large prospective studies about remestemcel-L reported a low rate of adverse events with good responses, particularly in severe GI GVHD, but did not still obtain approval (146). Non-pharmacological treatments are attractive, considering the low toxicity rate due to broad immune-modulating effects rather than immune-suppressor activity. Combination or sequential use of different approaches may represent a promising tool to reach efficacious synergy and minimize side effects.
To summarize, we certainly achieved a wider range of possibilities for treatment of children with SR GvHD, even if a prevalent off-label use is currently available. In SR aGvHD, most pediatric clinicians nowadays recommend ruxolitinib as “standard” second-line therapy, similarly to the adult setting (159). Further addition of ECP or MSC can be supposed if response is unsatisfactory. Conventional and anti-cytokine therapies could also represent options, especially for gut GvHD, with careful attention to limit infections. In cGvHD, with the evidence available, both ruxolitinib and ibrutinib may be started after steroid refractoriness, conventional therapies as low dose MTX and imatinib can still represent good options, especially for lung involvement and BOS (20). ECP addition may be evaluated considering feasibility (132), and Belumosidil may be chosen in cases of sclerotic cGvHD (33).
Finally, clinical trials are currently ongoing for both SR aGvHD and cGvHD in children and adolescents. Beyond the previously mentioned pivotal trial REACH4 for aGvHD, three trials are evaluating cell therapies as MSCs (NCT04744116), decidua stroma cells (NCT04883918) and combination of MSCs with ruxolitinib in aGvHD (NCT04744116). Interestingly, a trial is assessing efficacy and safety of glucagon-like peptide-2 (GLP-2) apraglutide in gut SR aGvHD (NCT05415410). Among the most notable in refractory cGvHD, one trial is evaluating Treg enriched cell infusions (NCT05095649), and one is assessing hydrogen water, previously assessed in adult patients as a feasible and active approach with extreme safety (NCT02918188) (Table 5).

Table 5. Interventional trials in pediatric patients with steroid refractory aGvHD or cGvHD.
Best management of SR-GvHD in pediatrics is still undetermined due to lack of prospective and randomized studies. Nevertheless, differently from the past, pediatric hematologists are now equipped with a growing number of therapeutic instruments. Management of SR aGvHD have been renewed by introduction of ruxolitinib, which demonstrated remarkable efficacy and safety, potentially reducing the rate of refractory patients, if used as first-line approach. Non pharmacologic treatments, particularly MSCs may be promising for SR aGvHD even in high-risk patients, as acting by modulating rather than suppressing immune system. Cost-benefit ratio due to effort of obtaining and performing a cell therapy in this setting may be less favorable and to be reserved to selected cases. Regarding cGvHD, both ruxolitinib and ibrutinib have transformed the landscape of this complication, demonstrating good efficacy and excellent safety. Also in this context, an early introduction in clinical practice may potentially change the paradigm of “refractoriness”. New approaches might represent in the future further lines in “ruxolitinib-refractory” and “ibrutinib-refractory” GVHD. Of note, different mechanisms of action are targeted by different treatments, and exploring combinations may exploit the efficacy. Perspective trials to compare different strategies should be supported and encouraged through centers.
FG, FB, and RM: conceptualized the work. DL: conceptualized the figures and tables. FG, FB, DL, EM, SC, FV, and AZ: wrote the paper. RM, TB, and AP: critically reviewed the paper. All author contributed to the article and approved the submitted version.
This work was supported by the “Associazione di volontariato—Il Giardino degli Angeli ODV” and by the “Federide Onlus—Associazione senza fini di lucro per gli adolescenti con Linfoma di Hodgkin per la ricerca e la cura della malattia”.
The author (RM) declared that he was an editorial board member of Frontiers at the time of submission. This had no impact on the peer review process and the final decision.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Copelan EA, Chojecki A, Lazarus HM, Avalos BR. Allogeneic hematopoietic cell transplantation; the current renaissance. Blood Rev. (2019) 34:34–44. doi: 10.1016/j.blre.2018.11.001
2. Ferrara JLM, Levine JE, Reddy P, Holler E. Graft-versus-host disease. Lancet. (2009) 373:1550–61. doi: 10.1016/S0140-6736(09)60237-3
3. Zeiser R, Blazar BR. Acute graft-versus-host disease—biologic process, prevention, and therapy. N Engl J Med. (2017) 377:2167–79. doi: 10.1056/NEJMRA1609337
4. Zecca M, Locatelli F. Management of graft-versus-host disease in paediatric bone marrow transplant recipients. Paediatr Drugs. (2000 Jan-Feb) 2(1):29–55. doi: 10.2165/00148581-200002010-00004. PMID: 10937457.
5. Masetti R, Bertuccio SN, Pession A, Locatelli F. CBFA2T3-GLIS2-positive acute myeloid leukaemia. A peculiar paediatric entity. Br J Haematol. (2019) 184(3):337–47. doi: 10.1111/bjh.15725
6. Verbeek AB, Jansen SA, von Asmuth EGJ, Lankester AC, Bresters D, Bierings M, et al. Clinical features, treatment, and outcome of pediatric steroid refractory acute graft-versus-host disease: a multicenter study. Transplant Cell Ther. (2022) 28:600.e1–e9. doi: doi: 10.1016/j.jtct.2022.06.008
7. Westin JR, Saliba RM, De Lima M, Alousi A, Hosing C, Qazilbash MH, et al. Steroid-refractory acute GVHD: predictors and outcomes. Adv Hematol. (2011) 2011:601953. doi: 10.1155/2011/601953
8. Haroun E, Agrawal K, Leibovitch J, Kassab J, Zoghbi M, Dutta D, et al. Chronic graft-versus-host disease in pediatric patients: differences and challenges. Blood Rev. (2023). doi: 10.1016/J.BLRE.2023.101054
9. Garnett C, Apperley JF, Pavlu J. Treatment and management of graft-versus-host disease: improving response and survival. Ther Adv Hematol. (2013) 4:366–78. doi: 10.1177/2040620713489842/ASSET/IMAGES/LARGE/10.1177_2040620713489842-FIG1.JPEG
10. Schoettler M, Duncan C, Lehmann L, Furutani E, Subramaniam M, Margossian S. Ruxolitinib is an effective steroid sparing agent in children with steroid refractory/dependent bronchiolitis obliterans syndrome after allogenic hematopoietic cell transplantation. Bone Marrow Transplant. (2019) 54:1158–60. doi: 10.1038/s41409-019-0450-3
11. Zeiser R, von Bubnoff N, Butler J, Mohty M, Niederwieser D, Or R, et al. Ruxolitinib for glucocorticoid-refractory acute graft-versus-host disease. N Engl J Med. (2020) 382(19):1–11. doi: 10.1056/NEJMoa1917635
12. Martin PJ. How I treat steroid-refractory acute graft-versus-host disease. Blood. (2020) 135:1630–8. doi: 10.1182/BLOOD.2019000960
13. MacMillan ML, Holtan SG, Rashidi A, DeFor TE, Blazar BR, Weisdorf DJ. Pediatric acute GVHD: clinical phenotype and response to upfront steroids. Bone Marrow Transplant. (2020) 55:165–71. doi: 10.1038/s41409-019-0651-9
14. Cuvelier GDE, Li A, Drissler S, Kariminia A, Abdossamadi S, Rozmus J, et al. Age related differences in the biology of chronic graft-versus-host disease after hematopoietic stem cell transplantation. Front Immunol. (2020) 11:571884. doi: 10.3389/fimmu.2020.571884
15. Dignan FL, Clark A, Amrolia P, Cornish J, Jackson G, Mahendra P, et al. Diagnosis and management of acute graft-versus-host disease. Br J Haematol. (2012) 158:30–45. doi: 10.1111/j.1365-2141.2012.09129.x
16. Inagaki J, Kodama Y, Fukano R, Noguchi M, Okamura J. Mycophenolate mofetil for treatment of steroid-refractory acute graft-versus-host disease after pediatric hematopoietic stem cell transplantation. Pediatr Transplant. (2015) 19:652–8. doi: 10.1111/petr.12545
17. Choi JY, Kim H, Baek HJ, Kook H, Lee JM, Kim BK, et al. Open-label, multicenter phase II study of combination therapy of imatinib mesylate and mycophenolate mofetil in pediatric patients with steroid-refractory sclerotic/fibrotic type chronic graft-versus-host disease. Transplant Cell Ther. (2021) 27:925.e1–e7. doi: 10.1016/j.jtct.2021.07.019
18. Bolaños-Meade J, Jacobsohn DA, Margolis J, Ogden A, Wientjes MG, Byrd JC, et al. Pentostatin in steroid-refractory acute graft-versus-host disease. J Clin Oncol. (2005) 23:2661–8. doi: 10.1200/JCO.2005.06.130
19. Jacobsohn DA, Gilman AL, Rademaker A, Browning B, Grimley M, Lehmann L, et al. Evaluation of pentostatin in corticosteroid-refractory chronic graft-versus-host disease in children: a pediatric blood and marrow transplant consortium study. Blood. (2009) 114:4354–60. doi: 10.1182/blood-2009-05-224840
20. Nassar A, Elgohary G, Elhassan T, Nurgat Z, Mohamed SY, Aljurf M. Methotrexate for the treatment of graft-versus-host disease after allogeneic hematopoietic stem cell transplantation. J Transplant. (2014) 2014:1–10. doi: 10.1155/2014/980301
21. Gatza E, Reddy P, Choi SW. Prevention and treatment of acute graft-versus-host disease in children, adolescents, and young adults. Biol Blood Marrow Transplant. (2020) 26:e101–12. doi: 10.1016/j.bbmt.2020.01.004
22. Kawashima N, Iida M, Suzuki R, Fukuda T, Atsuta Y, Hashii Y, et al. Prophylaxis and treatment with mycophenolate mofetil in children with graft-versus-host disease undergoing allogeneic hematopoietic stem cell transplantation: a nationwide survey in Japan. Int J Hematol. (2019) 109:491–8. doi: 10.1007/s12185-019-02601-5
23. Schmitt T, Luft T, Hegenbart U, Tran TH, Ho AD, Dreger P. Pentostatin for treatment of steroid-refractory acute GVHD: a retrospective single-center analysis. Bone Marrow Transplant. (2011) 46:580–5. doi: 10.1038/bmt.2010.146
24. Pidala J, Kim J, Roman-Diaz J, Shapiro J, Nishihori T, Bookout R, et al. Pentostatin as rescue therapy for glucocorticoid-refractory acute and chronic graft-versus-host disease. Ann Transplant. (2010) 15:21–9.21183872
25. Alam N, Atenafu EG, Tse G, Viswabandya A, Gupta V, Kim D, et al. Limited benefit of pentostatin salvage therapy for steroid-refractory grade III-IV acute graft-versus-host disease. Clin Transplant. (2013) 27:930–7. doi: 10.1111/ctr.12268
26. Jacobsohn DA, Chen AR, Zahurak M, Piantadosi S, Anders V, Bolaños-Meade J, et al. Phase II study of pentostatin in patients with corticosteroid-refractory chronic graft-versus-host disease. J Clin Oncol. (2007) 25:4255–61. doi: 10.1200/JCO.2007.10.8456
27. Klein SA, Bug G, Mousset S, Hofmann WK, Hoelzer D, Martin H. Long term outcome of patients with steroid-refractory acute intestinal graft versus host disease after treatment with pentostatin. Br J Haematol. (2011) 154:143–6. doi: 10.1111/j.1365-2141.2010.08495.x
28. Ragon BK, Mehta RS, Gulbis AM, Saliba RM, Chen J, Rondon G, et al. Pentostatin therapy for steroid-refractory acute graft versus host disease: identifying those who may benefit. Bone Marrow Transplant. (2018) 53:315–25. doi: 10.1038/s41409-017-0034-z
29. Svegliati S, Olivieri A, Campelli N, Luchetti M, Poloni A, Trappolini S, et al. Stimulatory autoantibodies to PDGF receptor in patients with extensive chronic graft-versus-host disease. Blood. (2007) 110:237–41. doi: 10.1182/blood-2007-01-071043
30. Olivieri A, Locatelli F, Zecca M, Sanna A, Cimminiello M, Raimondi R, et al. Imatinib for refractory chronic graft-versus-host disease with fibrotic features. Blood. (2009) 114:709–18. doi: 10.1182/blood-2009-02-204156
31. Faraci M, Ricci E, Bagnasco F, Pierri F, Giardino S, Girosi D, et al. Imatinib melylate as second-line treatment of bronchiolitis obliterans after allogenic hematopoietic stem cell transplantation in children. Pediatr Pulmonol. (2020) 55:631–7. doi: 10.1002/ppul.24652
32. Carpenter PA, Kang HJ, Yoo KH, Zecca M, Cho B, Lucchini G, et al. Ibrutinib treatment of pediatric chronic graft-versus-host disease: primary results from the phase 1/2 iMAGINE study. Transplant Cell Ther. (2022) 28:771.e1–771.e10. doi: 10.1016/j.jtct.2022.08.021
33. Cutler C, Lee SJ, Arai S, Rotta M, Zoghi B, Lazaryan A, et al. Belumosudil for chronic graft-versus-host disease after 2 or more prior lines of therapy: the ROCKstar study. Blood. (2021) 138:2278–89. doi: 10.1182/BLOOD.2021012021
34. Khandelwal P, Teusink-Cross A, Davies SM, Nelson AS, Dandoy CE, El-Bietar J, et al. Ruxolitinib as salvage therapy in steroid-refractory acute graft-versus-host disease in pediatric hematopoietic stem cell transplant patients. Biol Blood Marrow Transplant. (2017) 23:1122–7. doi: 10.1016/j.bbmt.2017.03.029
35. Uygun V, Karasu G, Daloğlu H, Öztürkmen S, Kılıç SÇ, Yalçın K, et al. Ruxolitinib salvage therapy is effective for steroid-refractory graft-versus-host disease in children: a single-center experience. Pediatr Blood Cancer. (2020) 67:e28190. doi: 10.1002/pbc.28190
36. Laisne L, Neven B, Dalle JH, Galambrun C, Esvan M, Renard C, et al. Ruxolitinib in children with steroid-refractory acute graft-versus-host disease: a retrospective multicenter study of the pediatric group of SFGM-TC. Pediatr Blood Cancer. (2020) 67:1–7. doi: 10.1002/pbc.28233
37. Moiseev IS, Morozova EV, Bykova TA, Paina OV, Smirnova AG, Dotsenko AA, et al. Long-term outcomes of ruxolitinib therapy in steroid-refractory graft-versus-host disease in children and adults. Bone Marrow Transplant. (2020) 55:1379–87. doi: 10.1038/s41409-020-0834-4
38. Abboud R, Choi J, Ruminski P, Schroeder MA, Kim S, Abboud CN, et al. Insights into the role of the JAK/STAT signaling pathway in graft-versus-host disease. Ther Adv Hematol. (2020) 11:2040620720914489. doi: 10.1177/2040620720914489
39. Bousoik E, Montazeri Aliabadi H. “Do we know jack” about JAK? A closer look at JAK/STAT signaling pathway. Front Oncol. (2018) 8:287. doi: 10.3389/fonc.2018.00287
40. Massa M, Rosti V, Campanelli R, Fois G, Barosi G. Rapid and long-lasting decrease of T-regulatory cells in patients with myelofibrosis treated with ruxolitinib. Leukemia. (2014) 28:449–51. doi: 10.1038/leu.2013.296
41. McLornan DP, Khan AA, Harrison CN. Immunological consequences of JAK inhibition: friend or foe? Curr Hematol Malig Rep. (2015) 10:370–9. doi: 10.1007/s11899-015-0284-z
42. Keohane C, Kordasti S, Seidl T, Perez Abellan P, Thomas NSB, Harrison CN, et al. JAK Inhibition induces silencing of T helper cytokine secretion and a profound reduction in T regulatory cells. Br J Haematol. (2015) 171:60–73. doi: 10.1111/bjh.13519
43. Mannina D, Kröger N. Janus kinase inhibition for graft-versus-host disease: current Status and future prospects. Drugs. (2019) 79:1499–509. doi: 10.1007/s40265-019-01174-1
44. Spoerl S, Mathew NR, Bscheider M, Schmitt-Graeff A, Chen S, Mueller T, et al. Activity of therapeutic JAK 1/2 blockade in graft-versus-host disease. Blood. (2014) 123:3832–42. doi: 10.1182/blood-2013-12-543736
45. Choi J, Cooper ML, Alahmari B, Ritchey J, Collins L, Holt M, et al. Pharmacologic blockade of JAK1/JAK2 reduces GvHD and preserves the graft-versus-leukemia effect. PLoS One. (2014) 9:2–7. doi: 10.1371/journal.pone.0109799
46. Zeiser R, Burchert A, Lengerke C, Verbeek M, Maas-Bauer K, Metzelder SK, et al. Ruxolitinib in corticosteroid-refractory graft-versus-host disease after allogeneic stem cell transplantation: a multicenter survey. Leukemia. (2015) 29:2062–8. doi: 10.1038/leu.2015.212
47. Streiler C, Shaikh F, Davis C, Abhyankar S, Brownback KR. Ruxolitinib is an effective steroid sparing agent in bronchiolitis obliterans due to chronic graft-versus-host-disease. Bone Marrow Transplant. (2020) 55:1194–6. doi: 10.1038/s41409-019-0662-6
48. Jagasia M, Perales MA, Schroeder MA, Ali H, Shah NN, Bin CY, et al. Ruxolitinib for the treatment of steroid-refractory acute GVHD (REACH1): a multicenter, open-label phase 2 trial. Blood. (2020) 135:1739–49. doi: 10.1182/BLOOD.2020004823
49. Zeiser R, Polverelli N, Ram R, Hashmi SK, Chakraverty R, Middeke JM, et al. Ruxolitinib for glucocorticoid-refractory chronic graft-versus-host disease. N Engl J Med. (2021) 385:228–38. doi: 10.1056/nejmoa2033122
50. Przepiorka D, Luo L, Subramaniam S, Qiu J, Gudi R, Cunningham LC, et al. FDA approval summary: ruxolitinib for treatment of steroid-refractory acute graft-versus-host disease. Oncologist. (2020) 25:e328–34. doi: 10.1634/theoncologist.2019-0627
51. González Vicent M, Molina B, González de Pablo J, Castillo A, Díaz MÁ. Ruxolitinib treatment for steroid refractory acute and chronic graft vs host disease in children: clinical and immunological results. Am J Hematol. (2019) 94:319–26. doi: 10.1002/ajh.25376
52. Meng G, Wang J, Wang X, Wang Y, Wang Z. Ruxolitinib treatment for SR-aGVHD in patients with EBV-HLH undergoing allo-HSCT. Ann Hematol. (2020) 99:343–9. doi: 10.1007/s00277-019-03864-y
53. Mozo Y, Bueno D, Sisinni L, Fernández-Arroyo A, Rosich B, Martínez AP, et al. Ruxolitinib for steroid-refractory graft versus host disease in pediatric HSCT: high response rate and manageable toxicity. Pediatr Hematol Oncol. (2021) 38:331–45. doi: 10.1080/08880018.2020.1868637
54. Yang W, Zhu G, Qin M, Li Z, Wang B, Yang J, et al. The effectiveness of ruxolitinib for acute/chronic graft-versus-host disease in children: a retrospective study. Drug Des Devel Ther. (2021) 15:743–52. doi: 10.2147/DDDT.S287218
55. Marcuzzi A, Rimondi E, Melloni E, Gonelli A, Grasso AG, Barbi E, et al. New applications of JAK/STAT inhibitors in pediatrics : current use of ruxolitinib. Pharmaceuticals. (2022) 15(3):1–14. doi: 10.3390/ph15030374
56. Wei C, Zhang X, Liang D, Yang J, Du J, Yue C, et al. Ruxolitinib for treatment of steroid-refractory graft-versus-host disease: real-world data from Chinese patients. Drug Des Devel Ther. (2021) 15:4875–83. doi: 10.2147/DDDT.S338752
57. Escamilla Gómez V, García-Gutiérrez V, López Corral L, García Cadenas I, Pérez Martínez A, Márquez Malaver FJ, et al. Ruxolitinib in refractory acute and chronic graft-versus-host disease: a multicenter survey study. Bone Marrow Transplant. (2020) 55:641–8. doi: 10.1038/s41409-019-0731-x
58. Wang YZM, Teusink-Cross A, Elborai Y, Krupski MC, Nelson AS, Grimley MS, et al. Ruxolitinib for the treatment of chronic GVHD and overlap syndrome in children and young adults. Transplantation. (2022) 106:412–9. doi: 10.1097/TP.0000000000003768
59. Locatelli F, Kang HJ, Bruno B, Gandemer V, Rialland F, Faraci M, et al. Ruxolitinib in pediatric patients with treatment-naïve or steroid-refractory acute graft-versus-host disease: primary findings from the phase I/II REACH4 study. Blood. (2022) 140:1376–8. doi: 10.1182/BLOOD-2022-155708
60. Kostareva I, Kirgizov K, Machneva E, Ustyuzhanina N, Nifantiev N, Skvortsova Y, et al. Novel and promising strategies for therapy of post-transplant chronic GVHD. Pharmaceuticals. (2022) 15:1–19. doi: 10.3390/ph15091100
61. Teusink-Cross A, Davies SM, Grimley MS, Chandra S, Flannery A, Dandoy CE, et al. Ibrutinib for the treatment of chronic graft-vs-host disease in pediatric hematopoietic stem cell transplant patients: a single-center experience. Pediatr Transplant. (2020) 24:1–9. doi: 10.1111/petr.13692
62. Jaglowski SM, Blazar BR. How ibrutinib, a B-cell malignancy drug, became an FDA-approved second-line therapy for steroid-resistant chronic GVHD. Blood Adv. (2018) 2:2012–9. doi: 10.1182/bloodadvances.2018013060
63. Miklos D, Cutler CS, Arora M, Waller EK, Jagasia M, Pusic I, et al. Ibrutinib for chronic graft-versus-host disease after failure of prior therapy. Blood. (2017) 130:2243–50. doi: 10.1182/blood-2017-07-793786
64. Keam SJ. Ibrutinib: pediatric first approval. Pediatric Drugs. (2022) 25(1):127–33. doi: 10.1007/s40272-022-00543-w
65. Gagliardi TA, Milner J, Cairo MS, Steinberg A. Concomitant ruxolitinib and ibrutinib for graft-versus-host disease (GVHD): the first reported use in pediatric patients. Cureus. (2022) 2:8–11. doi: 10.7759/cureus.29195
66. Martini DJ, Bin CY, DeFilipp Z. Recent FDA approvals in the treatment of graft-versus-host disease. Oncologist. (2022) 27:685–93. doi: 10.1093/ONCOLO/OYAC076
67. Zeiser R, Lee SJ. Three US food and drug administration–approved therapies for chronic GVHD. Blood. (2022) 139:1642–5. doi: 10.1182/BLOOD.2021014448
68. Zanin-Zhorov A, Weiss JM, Nyuydzefe MS, Chen W, Scher JU, Mo R, et al. Selective oral ROCK2 inhibitor down-regulates IL-21 and IL-17 secretion in human T cells via STAT3-dependent mechanism. Proc Natl Acad Sci U S A. (2014) 111:16814–9. doi: 10.1073/PNAS.1414189111
69. Flynn R, Paz K, Du J, Reichenbach DK, Taylor PA, Panoskaltsis-Mortari A, et al. Targeted rho-associated kinase 2 inhibition suppresses murine and human chronic GVHD through a Stat3-dependent mechanism. Blood. (2016) 127:2144–54. doi: 10.1182/BLOOD-2015-10-678706
70. Jagasia M, Lazaryan A, Bachier CR, Salhotra A, Weisdorf DJ, Zoghi B, et al. ROCK2 inhibition with belumosudil (KD025) for the treatment of chronic graft-versus-host disease. J Clin Oncol. (2021) 39:1888–98. doi: 10.1200/JCO.20.02754
71. DeFilipp Z, Kim HT, Yang Z, Noonan J, Blazar BR, Lee SJ, et al. Clinical response to belumosudil in bronchiolitis obliterans syndrome: a combined analysis from 2 prospective trials. Blood Adv. (2022) 6:6263–70. doi: 10.1182/BLOODADVANCES.2022008095/486557
72. Bachier CR, Skaar JR, Dehipawala S, Miao B, Ieyoub J, Taitel H. Budget impact analysis of belumosudil for chronic graft-versus-host disease treatment in the United States. J Med Econ. (2022) 25:857–63. doi: 10.1080/13696998.2022.2087408
73. Wang JZ, Liu KY, Xu LP, Liu DH, Han W, Chen H, et al. Basiliximab for the treatment of steroid-refractory acute graft-versus-host disease after unmanipulated HLA-mismatched/haploidentical hematopoietic stem cell transplantation. Transplant Proc. (2011) 43:1928–33. doi: 10.1016/J.TRANSPROCEED.2011.03.044
74. Massenkeil G, Rackwitz S, Genvresse I, Rosen O, Dörken B, Arnold R. Basiliximab is well tolerated and effective in the treatment of steroid-refractory acute graft-versus-host disease after allogeneic stem cell transplantation. Bone Marrow Transplant. (2002) 30:899–903. doi: 10.1038/SJ.BMT.1703737
75. Funke VAM, de Medeiros CR, Setúbal DC, Ruiz J, Bitencourt MA, Bonfim CM, et al. Therapy for severe refractory acute graft-versus-host disease with basiliximab, a selective interleukin-2 receptor antagonist. Bone Marrow Transplant. (2006) 37:961–5. doi: 10.1038/SJ.BMT.1705306
76. Liu SN, Zhang XH, Xu LP, Wang Y, Yan CH, Chen H, et al. Prognostic factors and long-term follow-up of basiliximab for steroid-refractory acute graft-versus-host disease: updated experience from a large-scale study. Am J Hematol. (2020) 95:927–36. doi: 10.1002/AJH.25839
77. Mo XD, Hong SD, Zhao YL, Jiang EL, Chen J, Xu Y, et al. Basiliximab for steroid-refractory acute graft-versus-host disease: a real-world analysis. Am J Hematol. (2022) 97:458–69. doi: 10.1002/AJH.26475
78. Tang FF, Cheng YF, Xu LP, Zhang XH, Yan CH, Han W, et al. Basiliximab as treatment for steroid-refractory acute graft-versus-host disease in pediatric patients after haploidentical hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. (2020) 26:351–7. doi: 10.1016/J.BBMT.2019.10.031
79. Hamidieh AA, Hadjibabaie M, Ghehi MT, Jalili M, Hosseini A, Pasha F, et al. Long-term follow-up of children treated with daclizumab for steroid-refractory gastrointestinal GvHD in a prospective study. Pediatr Transplant. (2012) 16:664–9. doi: 10.1111/J.1399-3046.2012.01753.X
80. Miano M, Cuzzubbo D, Terranova P, Giardino S, Lanino E, Morreale G, et al. Daclizumab as useful treatment in refractory acute GVHD: a paediatric experience. Bone Marrow Transplantation. (2009) 43(5 ):423–7. doi: 10.1038/bmt.2008.331
81. Faraci M, Calevo MG, Giardino S, Leoni M, Ricci E, Castagnola E, et al. Etanercept as treatment of steroid-refractory acute graft-versus-host disease in pediatric patients. Biol Blood Marrow Transplant. (2019) 25:743–8. doi: 10.1016/j.bbmt.2018.11.017
82. Bacigalupo A, Angelucci E, Raiola AM, Varaldo R, Di Grazia C, Gualandi F, et al. Treatment of steroid resistant acute graft versus host disease with an anti-CD26 monoclonal antibody-begelomab. Bone Marrow Transplant. (2020) 55:1580–7. doi: 10.1038/S41409-020-0855-Z
83. Jaiswal SR, Zaman S, Chakrabarti A, Sehrawat A, Bansal S, Gupta M, et al. T cell costimulation blockade for hyperacute steroid refractory graft versus-host disease in children undergoing haploidentical transplantation. Transpl Immunol. (2016) 39:46–51. doi: 10.1016/j.trim.2016.08.009
84. Patriarca F, Sperotto A, Damiani D, Morreale G, Bonifazi F, Olivieri A, et al. Infliximab treatment for steroid-refractory acute graft-versus-host disease. Haematologica. (2004) 89:1352–9.15531458
85. Kayaba H, Hirokawa M, Watanabe A, Saitoh N, Changhao C, Yamada Y, et al. Serum markers of graft-versus-host disease after bone marrow transplantation. J Allergy Clin Immunol. (2000) 106:S40–4. doi: 10.1067/MAI.2000.106060
86. Sakata N, Yasui M, Okamura T, Inoue M, Yumura-Yagi K, Kawa K. Kinetics of plasma cytokines after hematopoietic stem cell transplantation from unrelated donors: the ratio of plasma IL-10/sTNFR level as a potential prognostic marker in severe acute graft-versus-host disease. Bone Marrow Transplant. (2001) 27:1153–61. doi: 10.1038/SJ.BMT.1703060
87. Hamadani M, Hofmeister CC, Jansak B, Phillips G, Elder P, Blum W, et al. Addition of infliximab to standard acute graft-versus-host disease prophylaxis following allogeneic peripheral blood cell transplantation. Biol Blood Marrow Transplant. (2008) 14:783–9. doi: 10.1016/J.BBMT.2008.04.006
88. Choi SW, Stiff P, Cooke K, Ferrara JLM, Braun T, Kitko C, et al. TNF-inhibition with etanercept for graft-versus-host disease prevention in high-risk HCT: lower TNFR1 levels correlate with better outcomes. Biol Blood Marrow Transplant. (2012) 18:1525–32. doi: 10.1016/J.BBMT.2012.03.013
89. Couriel DR, Saliba R, de Lima M, Giralt S, Andersson B, Khouri I, et al. A phase III study of infliximab and corticosteroids for the initial treatment of acute graft-versus-host disease. Biol Blood Marrow Transplant. (2009) 15:1555–62. doi: 10.1016/J.BBMT.2009.08.003
90. Alousi AM, Weisdorf DJ, Logan BR, Bolaños-Meade J, Carter S, DiFronzo N, et al. Etanercept, mycophenolate, denileukin, or pentostatin plus corticosteroids for acute graft-versus-host disease: a randomized phase 2 trial from the blood and marrow transplant clinical trials network. Blood. (2009) 114:511–7. doi: 10.1182/BLOOD-2009-03-212290
91. Knight DM, Trinh H, Le J, Siegel S, Shealy D, McDonough M, et al. Construction and initial characterization of a mouse-human chimeric anti-TNF antibody. Mol Immunol. (1993) 30:1443–53. doi: 10.1016/0161-5890(93)90106-L
92. Kobbe G, Schneider P, Rohr U, Fenk R, Neumann F, Aivado M, et al. Treatment of severe steroid refractory acute graft-versus-host disease with infliximab, a chimeric human/mouse antiTNFalpha antibody. Bone Marrow Transplant. (2001) 28:47–9. doi: 10.1038/SJ.BMT.1703094
93. Yamane T, Yamamura R, Aoyama Y, Nakamae H, Hasegawa T, Sakamoto C, et al. Infliximab for the treatment of severe steroid refractory acute graft-versus-host disease in three patients after allogeneic hematopoietic transplantation. Leuk Lymphoma. (2003) 44:2095–7. doi: 10.1080/1042819031000123483
94. Sleight BS, Chan KW, Braun TM, Serrano A, Gilman AL. Infliximab for GVHD therapy in children. Bone Marrow Transplant. (2007) 40(5):473–80. doi: 10.1038/sj.bmt.1705761
95. Verbeek AB, Jansen SA, von Asmuth EGJ, Lankester AC, Bresters D, Bierings M, et al. Clinical features, treatment, and outcome of pediatric steroid refractory acute graft-versus-host disease: a multicenter study. Transplant Cell Ther. (2022) 28:600.e1–e9. doi: 10.1016/J.JTCT.2022.06.008
96. Rodriguez V, Anderson PM, Trotz BA, Arndt CAS, Allen JA, Khan SP. Use of infliximab-daclizumab combination for the treatment of acute and chronic graft-versus-host disease of the liver and gut. Pediatr Blood Cancer. (2007) 49:212–5. doi: 10.1002/PBC.20648
97. Kennedy GA, Butler J, Western R, Morton J, Durrant S, Hill GR. Combination antithymocyte globulin and soluble TNFalpha inhibitor (etanercept) +/− mycophenolate mofetil for treatment of steroid refractory acute graft-versus-host disease. Bone Marrow Transplant. (2006) 37:1143–7. doi: 10.1038/SJ.BMT.1705380
98. Busca A, Locatelli F, Marmont F, Ceretto C, Falda M. Recombinant human soluble tumor necrosis factor receptor fusion protein as treatment for steroid refractory graft-versus-host disease following allogeneic hematopoietic stem cell transplantation. Am J Hematol. (2007) 82:45–52. doi: 10.1002/AJH.20752
99. De Jong CN, Saes L, Klerk CPW, Van der Klift M, Cornelissen JJ, Broers AEC. Etanercept for steroid-refractory acute graft-versus-host disease: a single center experience. PLoS One. (2017) 12:e0187184. doi: 10.1371/JOURNAL.PONE.0187184
100. Wilkinson AN, Chang K, Kuns RD, Henden AS, Minnie SA, Ensbey KS, et al. IL-6 dysregulation originates in dendritic cells and mediates graft-versus-host disease via classical signaling. Blood. (2019) 134:2092–106. doi: 10.1182/BLOOD.2019000396
101. Ganetsky A, Frey NV, Hexner EO, Loren AW, Gill SI, Luger SM, et al. Tocilizumab for the treatment of severe steroid-refractory acute graft-versus-host disease of the lower gastrointestinal tract. Bone Marrow Transplant. (2018) 54(2):212–7. doi: 10.1038/s41409-018-0236-z
102. Kattner AS, Holler E, Holler B, Klobuch S, Weber D, Martinovic D, et al. IL6-receptor Antibody tocilizumab as salvage therapy in severe chronic graft-versus-host disease after allogeneic hematopoietic stem cell transplantation: a retrospective analysis. Ann Hematol. (2020) 99:847. doi: 10.1007/S00277-020-03968-W
103. Beebe KL, Miller HK, Ngwube A, Salzberg D, Stahlecker J, McNulty A, et al. Tocilizumab in the treatment of pediatric chronic gvhd. Biol Blood Marrow Transplant. (2018) 24:S207. doi: 10.1016/j.bbmt.2017.12.174
104. Bhatt S, Schulz G, Towerman A, Hente M, Shenoy S. Tocilizumab for the treatment of steroid refractory acute graft versus host disease: a pediatric experience. Biol Blood Marrow Transplant. (2016) 22:S389–90. doi: 10.1016/j.bbmt.2015.11.910
105. Hu Y, Turner MJ, Shields J, Gale MS, Hutto E, Roberts BL, et al. Investigation of the mechanism of action of alemtuzumab in a human CD52 transgenic mouse model. Immunology. (2009) 128:260. doi: 10.1111/J.1365-2567.2009.03115.X
106. Schub N, Günther A, Schrauder A, Claviez A, Ehlert C, Gramatzki M, et al. Therapy of steroid-refractory acute GVHD with CD52 antibody alemtuzumab is effective. Bone Marrow Transplant. (2011) 46:143–7. doi: 10.1038/BMT.2010.68
107. Gómez-Almaguer D, Ruiz-Argüelles GJ, del Carmen Tarín-Arzaga L, González-Llano O, Gutiérrez-Aguirre H, Cantú-Rodríguez O, et al. Alemtuzumab for the treatment of steroid-refractory acute graft-versus-host disease. Biol Blood Marrow Transplant. (2008) 14:10–5. doi: 10.1016/J.BBMT.2007.08.052
108. Khandelwal P, Lawrence J, Filipovich AH, Davies SM, Bleesing JJ, Jordan MB, et al. The successful use of alemtuzumab for treatment of steroid-refractory acute graft-versus-host disease in pediatric patients. Pediatr Transplant. (2014) 18:94–102. doi: 10.1111/PETR.12183
109. Hatano R, Ohnuma K, Yamamoto J, Dang NH, Yamada T, Morimoto C. Prevention of acute graft-versus-host disease by humanized anti-CD26 monoclonal antibody. Br J Haematol. (2013) 162:263–77. doi: 10.1111/BJH.12378
110. Feagan BG, Rutgeerts P, Sands BE, Hanauer S, Colombel J-F, Sandborn WJ, et al. Vedolizumab as induction and maintenance therapy for ulcerative colitis. N Engl J Med. (2013) 369:699–710. doi: 10.1056/nejmoa1215734
111. Waldman E, Lu SX, Hubbard VM, Kochman AA, Eng JM, Terwey TH, et al. Absence of beta7 integrin results in less graft-versus-host disease because of decreased homing of alloreactive T cells to intestine. Blood. (2006) 107:1703–11. doi: 10.1182/blood-2005-08-3445
112. Fløisand Y, Schroeder MA, Chevallier P, Selleslag D, Devine S, Renteria AS, et al. A phase 2a randomized clinical trial of intravenous vedolizumab for the treatment of steroid-refractory intestinal acute graft-versus-host disease. Bone Marrow Transplant. (2021) 56:2477–88. doi: 10.1038/s41409-021-01356-0
113. Li ACW, Dong C, Tay ST, Ananthakrishnan A, Ma KSK. Vedolizumab for acute gastrointestinal graft-versus-host disease: a systematic review and meta-analysis. Front Immunol. (2022) 13:1–12. doi: 10.3389/fimmu.2022.1025350
114. Ibrahimova A, Davies SM, Lane A, Jordan MB, Lake K, Litts B, et al. Α4β7 integrin expression and blockade in pediatric and young adult gastrointestinal graft-versus-host disease. Pediatr Blood Cancer. (2021) 68:1–8. doi: 10.1002/pbc.28968
115. Isshiki K, Kamiya T, Endo A, Okamoto K, Osumi T, Kawai T, et al. Vedolizumab therapy for pediatric steroid-refractory gastrointestinal acute graft-versus-host disease. Int J Hematol. (2022) 115:590–4. doi: 10.1007/s12185-021-03245-0
116. Rosa M, Jarmoliński T, Miśkiewicz-Migoń I, Liszka K, Miśkiewicz-Bujna J, Panasiuk A, et al. Vedolizumab in highly resistant acute gastrointestinal graft-versus-host disease after allogeneic stem cell transplantation: a single-center pediatric series. Adv Clin Exp Med. (2022) 31. doi: 10.17219/acem/146321
117. Fukuta T, Muramatsu H, Yamashita D, Sajiki D, Maemura R, Tsumura Y, et al. Vedolizumab for children with intestinal graft-versus-host disease: a case report and literature review. Int J Hematol. (2023) 118(3):411–7. doi: 10.1007/s12185-023-03590-2
118. Inamoto Y, Zeiser R, Chan GC. Novel treatment for graft-versus-host disease. Blood Cell Ther. (2021) 4(4):101–9. doi: 10.31547/bct-2021-022
119. Pombo-Suarez M, Gomez-Reino JJ. Abatacept For the treatment of rheumatoid arthritis. Expert Rev Clin Immunol. (2019) 15:319–26. doi: 10.1080/1744666X.2019.1579642
120. Blazar B, Taylor P, Linsley P, Vallera D. In vivo blockade of CD28/CTLA4: B7/BB1 interaction with CTLA4-Ig reduces lethal murine graft-versus-host disease across the major histocompatibility complex barrier in mice. Blood. (1994) 83:3815–25. doi: 10.1182/blood.v83.12.3815.3815
121. Watkins B, Qayed M, McCracken C, Bratrude B, Betz K, Suessmuth Y, et al. Phase II trial of costimulation blockade with Abatacept for prevention of acute GVHD. J Clin Oncol. (2021) 39:1865–77. doi: 10.1200/JCO.20.01086
122. Stenger EO, Watkins B, Rogowski K, Chiang K-Y, Haight AE, Leung K, et al. Abatacept GVHD prophylaxis in unrelated hematopoietic cell transplantation for pediatric bone marrow failure. Blood Adv. (2023) 7:2196–205. doi: 10.1182/bloodadvances.2022008545
123. Ngwube A, Shah N, Godder K, Jacobsohn D, Hulbert ML, Shenoy S. Abatacept Is effective as GVHD prophylaxis in unrelated donor stem cell transplantation for children with severe sickle cell disease. Blood Adv. (2020) 4:3894–9. doi: 10.1182/bloodadvances.2020002236
124. Wertheimer T, Dohse M, Afram G, Weber D, Heidenreich M, Holler B, et al. Abatacept As salvage therapy in chronic graft-versus-host disease—a retrospective analysis. Ann Hematol. (2021) 100:779–87. doi: 10.1007/s00277-021-04434-x
125. Greinix HT, Ayuk F, Zeiser R. Extracorporeal photopheresis in acute and chronic steroid-refractory graft-versus-host disease: an evolving treatment landscape. Leukemia. (2022) 36:2558–66. doi: 10.1038/s41375-022-01701-2
126. Abu-Dalle I, Reljic T, Nishihori T, Antar A, Bazarbachi A, Djulbegovic B, et al. Extracorporeal photopheresis in steroid-refractory acute or chronic graft-versus-host disease: results of a systematic review of prospective studies. Biol Blood Marrow Transplant. (2014) 20:1677–86. doi: 10.1016/j.bbmt.2014.05.017
127. Shapiro RM, Antin JH. Therapeutic options for steroid-refractory acute and chronic GVHD: an evolving landscape. Expert Rev Hematol. (2020) 13:519–32. doi: 10.1080/17474086.2020.1752175
128. Arora S, Setia R. Extracorporeal photopheresis: review of technical aspects. Asian J Transfus Sci. (2017) 11:81. doi: 10.4103/AJTS.AJTS_87_16
129. Messina C, Locatelli F, Lanino E, Uderzo C, Zacchello G, Cesaro S, et al. Extracorporeal photochemotherapy for paediatric patients with graft-versus-host disease after haematopoietic stem cell transplantation. Br J Haematol. (2003) 122:118–27. doi: 10.1046/J.1365-2141.2003.04401.X
130. Greinix HT, van Besien K, Elmaagacli AH, Hillen U, Grigg A, Knobler R, et al. Progressive improvement in cutaneous and extracutaneous chronic graft-versus-host disease after a 24-week course of extracorporeal photopheresis—results of a crossover randomized study. Biol Blood Marrow Transplant. (2011) 17:1775–82. doi: 10.1016/J.BBMT.2011.05.004
131. Zhang H, Chen R, Cheng J, Jin N, Chen B. Systematic review and meta-analysis of prospective studies for ECP treatment in patients with steroid-refractory acute GVHD. Patient Prefer Adherence. (2015) 9:105–11. doi: 10.2147/PPA.S76563
132. Winther-Jørgensen S, Nygaard M, Heilmann C, Ifversen M, Sørensen K, Müller K, et al. Feasibility of extracorporeal photopheresis in pediatric patients with graft-versus-host disease after hematopoietic stem cell transplantation. Pediatr Transplant. (2019) 23:e13416. doi: 10.1111/PETR.13416
133. Asensi Cantó P, Sanz Caballer J, Fuentes Socorro C, Solves Alcaína P, Lloret Madrid P, Solís Ruíz J, et al. Role of extracorporeal photopheresis in the management of children with graft-vs-host disease. J Clin Apher. (2022) 37:573–83. doi: 10.1002/JCA.22012
134. Le Blanc K, Rasmusson I, Sundberg B, Götherström C, Hassan M, Uzunel M, et al. Treatment of severe acute graft-versus-host disease with third party haploidentical mesenchymal stem cells. Lancet. (2004) 363:1439–41. doi: 10.1016/S0140-6736(04)16104-7
135. Müller I, Kordowich S, Holzwarth C, Isensee G, Lang P, Neunhoeffer F, et al. Application of multipotent mesenchymal stromal cells in pediatric patients following allogeneic stem cell transplantation. Blood Cells Mol Dis. (2008) 40:25–32. doi: 10.1016/J.BCMD.2007.06.021
136. Le Blanc K, Frassoni F, Ball L, Locatelli F, Roelofs H, Lewis I, et al. Mesenchymal stem cells for treatment of steroid-resistant, severe, acute graft-versus-host disease: a phase II study. Lancet. (2008) 371:1579–86. doi: 10.1016/S0140-6736(08)60690-X
137. Lucchini G, Introna M, Dander E, Rovelli A, Balduzzi A, Bonanomi S, et al. Platelet-lysate-expanded mesenchymal stromal cells as a salvage therapy for severe resistant graft-versus-host disease in a pediatric population. Biol Blood Marrow Transplant. (2010) 16:1293–301. doi: 10.1016/J.BBMT.2010.03.017
138. Ball LM, Bernardo ME, Roelofs H, van Tol MJD, Contoli B, Zwaginga JJ, et al. Multiple infusions of mesenchymal stromal cells induce sustained remission in children with steroid-refractory, grade III–IV acute graft-versus-host disease. Br J Haematol. (2013) 163:501–9. doi: 10.1111/BJH.12545
139. Niemeyer CM, Loh ML, Cseh A, Cooper T, Dvorak CC, Chan R, et al. Criteria for evaluating response and outcome in clinical trials for children with juvenile myelomonocytic leukemia. Haematologica. (2015) 100(1):17–22. doi: 10.3324/haematol.2014.109892
140. Modemann F, Ayuk F, Wolschke C, Christopeit M, Janson D, von Pein UM, et al. Ruxolitinib plus extracorporeal photopheresis (ECP) for steroid refractory acute graft-versus-host disease of lower GI-tract after allogeneic stem cell transplantation leads to increased regulatory T cell level. Bone Marrow Transplant. (2020) 55:2286–93. doi: 10.1038/S41409-020-0952-Z
141. Maas-Bauer K, Kiote-Schmidt C, Bertz H, Apostolova P, Wäsch R, Ihorst G, et al. Ruxolitinib–ECP combination treatment for refractory severe chronic graft-versus-host disease. Bone Marrow Transplant. (2020) 56(4 ):909–16. doi: 10.1038/s41409-020-01122-8
142. Cheung TS, Bertolino GM, Giacomini C, Bornhäuser M, Dazzi F, Galleu A. Mesenchymal stromal cells for graft versus host disease: mechanism-based biomarkers. Front Immunol. (2020) 11:1338. doi: 10.3389/FIMMU.2020.01338/FULL
143. Kelly K, Rasko JEJ. Mesenchymal stromal cells for the treatment of graft versus host disease. Front Immunol. (2021) 12:761616. doi: 10.3389/FIMMU.2021.761616/BIBTEX
144. Murata M, Teshima T. Treatment of steroid-refractory acute graft-versus-host disease using commercial mesenchymal stem cell products. Front Immunol. (2021) 12:724380. doi: 10.3389/FIMMU.2021.724380/FULL
145. Kebriaei P, Hayes J, Daly A, Uberti J, Marks DI, Soiffer R, et al. A phase 3 randomized study of remestemcel-L versus placebo added to second-line therapy in patients with steroid-refractory acute graft-versus-host disease. Biol Blood Marrow Transplant. (2020) 26:835. doi: 10.1016/J.BBMT.2019.08.029
146. Kurtzberg J, Prockop S, Chaudhury S, Horn B, Nemecek E, Prasad V, et al. Study 275: updated expanded access program for remestemcel-L in steroid-refractory acute graft-versus-host disease in children. Biol Blood Marrow Transplant. (2020) 26:855. doi: 10.1016/J.BBMT.2020.01.026
147. Kurtzberg J, Abdel-Azim H, Carpenter P, Chaudhury S, Horn B, Mahadeo K, et al. A phase 3, single-arm, prospective study of remestemcel-L, ex vivo culture-expanded adult human mesenchymal stromal cells for the treatment of pediatric patients who failed to respond to steroid treatment for acute graft-versus-host disease. Biol Blood Marrow Transplant. (2020) 26:845. doi: 10.1016/J.BBMT.2020.01.018
148. Masetti R, D’Amico F, Zama D, Leardini D, Muratore E, Ussowicz M, et al. Febrile neutropenia duration is associated with the severity of gut Microbiota dysbiosis in pediatric allogeneic hematopoietic stem cell transplantation recipients. Cancers. (2022) 14:1932. doi: 10.3390/cancers14081932
149. Masetti R, Zama D, Leardini D, Muratore E, Turroni S, Prete A, et al. The gut microbiome in pediatric patients undergoing allogeneic hematopoietic stem cell transplantation. Pediatr Blood Cancer. (2020) 67(12):e28711. doi: 10.1002/pbc.28711
150. Masetti R, Biagi E, Zama D, Muratore E, Amico FD, Leardini D, et al. Early modifications of the gut microbiome in children with hepatic sinusoidal obstruction syndrome after hematopoietic stem cell transplantation. Sci Rep. (2021) 11(1):1–11. doi: 10.1038/s41598-021-93571-4
151. Stein-Thoeringer CK, Nichols KB, Lazrak A, Docampo MD, Slingerland AE, Slingerland JB, et al. Lactose drives Enterococcus expansion to promote graft-versus-host disease. Science. (2019) 366:1143–9. doi: 10.1126/science.aax3760
152. Jenq RR, Taur Y, Devlin SM, Ponce DM, Goldberg JD, Ahr KF, et al. Intestinal blautia is associated with reduced death from graft-versus-host disease. Biol Blood Marrow Transplant. (2015) 21:1373–83. doi: 10.1016/j.bbmt.2015.04.016
153. Muratore E, Baccelli F, Leardini D, Campoli C, Belotti T, Viale P, et al. Antimicrobial stewardship interventions in pediatric oncology: a systematic review. J Clin Med. (2022) 11:4545. doi: 10.3390/jcm11154545
154. Muratore E, Leardini D, Baccelli F, Venturelli F, Prete A, Masetti R. Nutritional modulation of the gut microbiome in allogeneic hematopoietic stem cell transplantation recipients. Front Nutr. (2022) 9:993668. doi: 10.3389/FNUT.2022.993668
155. Fabozzi F, Trovato CM, Diamanti A, Mastronuzzi A, Zecca M, Tripodi SI, et al. Management of nutritional needs in pediatric oncology : a consensus statement. Cancers. (2022) 14(14):3378. doi: 10.3390/cancers14143378
156. DeFilipp Z, Hohmann E, Jenq RR, Chen Y-B. Fecal microbiota transplantation: restoring the injured microbiome after allogeneic hematopoietic cell transplantation. Biol Blood Marrow Transplant. (2019) 25:e17–22. doi: 10.1016/j.bbmt.2018.10.022
157. Pession A, Zama D, Muratore E, Leardini D, Gori D, Guaraldi F, et al. Fecal microbiota transplantation in allogeneic hematopoietic stem cell transplantation recipients: a systematic review. J Pers Med. (2021) 11:100. doi: 10.3390/jpm11020100
158. Merli P, Massa M, Russo A, Rea F, Del Chierico F, Galaverna F, et al. Fecal microbiota transplantation for the treatment of steroid-refractory, intestinal, graft-versus-host disease in a pediatric patient. Bone Marrow Transplant. (2022) 57:1600–3. doi: 10.1038/S41409-022-01752-0
159. Mohty M, Holler E, Jagasia M, Jenq R, Malard F, Martin P, et al. Refractory acute graft-versus-host disease: a new working definition beyond corticosteroid refractoriness. Blood. (2020) 136:1903–6. doi: 10.1182/BLOOD.2020007336
160. Inagaki J, Nagatoshi Y, Hatano M, Isomura N, Sakiyama M, Okamura J. Low-dose MTX for the treatment of acute and chronic graft-versus-host disease in children. Bone Marrow Transplant. (2008) 41(6):571–7. doi: 10.1038/sj.bmt.1705922
161. Inagaki J, Fukano R, Kodama Y, Nishimura M, Shimokawa M, Okamura J. Safety and efficacy of low-dose methotrexate for pediatric patients with steroid-refractory acute graft-versus-host disease after hematopoietic stem cell transplantation. Ann Hematol. (2014) 93(4):645–51. doi: 10.1007/s00277-013-1923-x
162. Yang J, Cheuk DK, Ha SY, Chiang AK, Lee TL, Ho MH, Chan GC. Infliximab for steroid refractory or dependent gastrointestinal acute graft-versus-host disease in children after allogeneic hematopoietic stem cell transplantation. Pediatr Transplant. (2012 Nov) 16(7):771–8. doi: 10.1111/j.1399-3046.2012.01756.x
Keywords: GvHD, steroid-refractory, children, pediatric HSCT, ruxolitinib
Citation: Gottardi F, Leardini D, Muratore E, Baccelli F, Cerasi S, Venturelli F, Zanaroli A, Belotti T, Prete A and Masetti R (2023) Treatment of steroid-refractory graft versus host disease in children. Front. Transplant. 2:1251112. doi: 10.3389/frtra.2023.1251112
Received: 30 June 2023; Accepted: 17 August 2023;
Published: 15 September 2023.
Edited by:
Maria Teresa Lupo Stanghellini, San Raffaele Hospital (IRCCS), Italy© 2023 Gottardi, Leardini, Muratore, Baccelli, Cerasi, Venturelli, Zanaroli, Belotti, Prete and Masetti. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francesco Baccelli ZnJhbmNlc2NvLmJhY2NlbGxpMkBzdHVkaW8udW5pYm8uaXQ=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.