
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Transplant., 29 September 2023
Sec. Immunosuppression
Volume 2 - 2023 | https://doi.org/10.3389/frtra.2023.1248284
This article is part of the Research TopicAntibody-Mediated RejectionView all 6 articles
 William Brandon1,†
William Brandon1,† Colin Dunn1,†
Colin Dunn1,† Srinivas Bollineni2John Joerns2Adrian Lawrence2
Srinivas Bollineni2John Joerns2Adrian Lawrence2 Manish Mohanka2Irina Timofte2
Manish Mohanka2Irina Timofte2 Fernando Torres2Vaidehi Kaza2*
Fernando Torres2Vaidehi Kaza2*
The formation of antibodies against donor human leukocyte antigens poses a challenging problem both for donor selection as well as postoperative graft function in lung transplantation. These donor-specific antibodies limit the pool of potential donor organs and are associated with episodes of antibody-mediated rejection, chronic lung allograft dysfunction, and increased mortality. Optimal management strategies for clearance of DSAs are poorly defined and vary greatly by institution; most of the data supporting any particular strategy is limited to small-scale retrospective cohort studies. A typical approach to antibody depletion may involve the use of high-dose steroids, plasma exchange, intravenous immunoglobulin, and possibly other immunomodulators or small-molecule therapies. This review seeks to define the current understanding of the significance of DSAs in lung transplantation and outline the literature supporting strategies for their management.
Rates of lung transplantation have increased considerably over recent years with nearly 34,000 transplants performed between 2010 and 2018, triple the number performed in the 1990s (1). While transplant outcomes have improved marginally over this time period, long-term graft survival been hampered by the frequent occurrence of both acute and chronic rejection. This rejection is driven by both cellular and antibody-mediated processes, the latter of which are thought to be caused primarily by donor specific antibodies (DSAs)—recipient antibodies against foreign donor antigens.
While these antibodies may target any mismatched donor epitope, those of greatest clinical significance in solid organ transplantation are DSAs against HLA antigens. There is a wealth of literature supporting the deleterious effects of anti-HLA DSAs, and even antibodies against non-donor HLA antigens have been shown to adversely affect solid organ allograft outcomes (2). Antibodies against non-HLA donor antigens have been linked to worse transplant outcomes as well, though the clinical significance of their presence is not yet as well defined; antigens previously found to be of particular importance in lung transplantation include the angiotensin type 1 receptor, endothelin type A receptor, and K-α-1-tubulin (3, 4).
The identification and quantification of DSAs is an evolving science. Historically, DSAs were identified using a complement-dependent cytotoxicity assay in which donor lymphocytes are incubated with recipient serum, complement, and a reporter dye to assess the degree of cell death mediated by recipient antibodies against exposed donor antigens. More recently, solid-phase assays have come into use whereby beads coated with HLA antigens are exposed to recipient serum before being tagged with a fluorescent anti-IgG reporter, allowing for the more precise identification of antibodies against specific HLA molecules. The amount of fluorescent signal produced by this method is expressed as the mean fluorescence intensity (MFI), a semi-quantitative measurement allowing for the rough estimation of the presence of and strength of DSAs; of note, the results produced by this method can vary widely depending on the testing methods employed and thresholds set for detection of a positive crossmatch.
As the demand for lung transplantation continues to rise, understanding the impact and management of these DSAs has become paramount. The purpose of this review is to provide a comprehensive overview of the current literature on the clinical implications and management of DSAs in lung transplantation. By synthesizing the existing evidence, this review aims to contribute to the understanding of DSAs' role in lung transplantation and guide clinical practice in optimizing patient outcomes with special attention paid to areas of recent innovation and future direction.
Given a historical hesitancy to transplant an HLA haplotype in the presence of a DSA, data regarding outcomes in patients with pre-formed DSAs are sparse. Early studies on outcomes in this population relied on the use of solid-phase assays for the retrospective identification of HLA antibodies that failed to be detected by the complement-dependent cytotoxicity assays in use at the time of transplantation. One such study showed worse 1-year post-transplant survival in patients with pre-formed DSA, with particularly limited survival in those with complement-fixing DSAs or mean fluorescence intensity greater than 5,000 units (5); another identified greater mortality and quicker onset of BOS in patients with class II DSAs, but not in those with only class I (6).
More recently, attempts have been made to transplant in the presence of donor-specific antibodies with or without changes to the induction immunosuppression regimen. One study of 18 patients with pretransplant DSA (but negative complement-dependent cytotoxicity assay) found no difference in survival or time to onset of chronic lung allograft dysfunction (CLAD) when compared to a non-DSA population after a median follow-up period of 1.4 years, however with greater incidence of antibody-mediated rejection (AMR) requiring treatment and greater need for prolonged mechanical ventilation postoperatively (7). Another group trialed transplantation in the presence of low-level [mean fluorescence intensity (MFI) < 6,000 units] DSAs without augmentation of immunosuppression and found no worse survival, time to CLAD, or incidence of AMR after greater than 2-year median followup (8).
A significant proportion of lung transplant recipients will develop DSAs after transplantation, with one study of 340 patients showing that 47% developed DSAs within the first two years at a median onset of 86 days post-transplant (9). Development of de novo DSAs has been linked with adverse transplant outcomes including CLAD and, in some studies, mortality (9–17). In one study, for example, DSA development was associated with a roughly two-fold increase in incidence of CLAD over a median 764 day follow up period (9). Numerous studies support an association between DSA formation and mortality, including two retrospective cohort studies from 2014 (15, 16) and others linking early-onset (within one month from transplant) DSA formation in particular to worse survival (13, 14). More recently, preliminary results from the HALT (HLA Antibodies after Lung Transplantation) study revealed an increased risk of acute cellular rejection after de novo DSA formation by prospectively following 119 patients with protocolized DSA surveillance, however the limited follow-up period was likely insufficient to detect differences in other meaningful transplant outcomes (10).
Several characteristics of specific donor-specific antibodies have been found to modulate their effect on transplant outcomes, including their titer, persistence, and propensity to activate the complement system (5, 12, 18). While no well-defined MFI threshold for a clinically significant DSA exists in lung transplantation, one retrospective cohort study found worse 1-year survival (33.3%) in patients with pre-formed DSAs with MFI greater than 5,000 units than in those with detectable but lower-titer DSAs (62.5%–71.4%) (5). Another study found shorter time to CLAD onset in those with de novo DSAs at a threshold MFI of only 500 units (13). Antibodies against HLA-DQ antigens appear particularly deleterious as demonstrated in studies showing greater risk for CLAD with anti-DQ DSA when compared to non-DQ DSAs (9, 18). It is otherwise clear that transient DSAs, generally defined as those present on only a single assay, are of less significance than those that are more persistent, as shown in several studies that showed less acute rejection and more CLAD-free and graft survival with only transient DSAs (11, 12, 18). Lastly, DSAs which activate the complement pathway, as demonstrated by positive C1q binding, seem especially harmful when compared to those with C1q-negative DSAs as exhibited in a recent study by Iasella et al. showing more rapid onset of CLAD in this group (18).
Considering the adverse transplant outcomes linked to DSA development, it is of considerable interest to identify patients at elevated risk for DSA formation. Retrospective cohort studies have previously identified pre-transplant HLA-DQ mismatch and postoperative platelet transfusion as risk factors for DSA development (12, 17). One study by Kulkarni and colleagues found an independent link between the growth of Pseudomonas aeruginosa, but not other organisms, on respiratory cultures and later development of DSAs, hypothesizing that the particularities of the immune response to Pseudomonas promotes an inflammatory milieu that promotes DSA formation (19). More recently, there has been considerable interest in the use of computer algorithms to estimate the risk of de novo DSA development on the basis of pre-transplant epitope mismatch loads (20, 21).
The diagnosis of antibody-mediated rejection of the lung can be challenging to make, and this was historically hindered by an absence of standardized diagnostic criteria. In 2016, the ISHLT published a consensus definition for AMR which requires the following three components in addition to graft dysfunction: presence of DSA, histology suggestive of AMR, and positive C4d staining on biopsy. Patients are classified as having either possible, probable, or definite AMR depending on whether they manifest one, two, or all of these features, respectively (22). C4d staining has come under scrutiny as a meaningful diagnostic requirement, as studies have found this feature to be poorly associated with either the presence of DSAs or other clinical or histologic features of AMR (23–26).
There has been recent interest in the use of donor-derived cell free DNA (ddcfDNA) in the diagnosis of AMR, however this has not yet seen widespread clinical utility. Donor-derived cell free DNA, as a marker of transplant injury, is elevated in cases of both ACR and AMR as well as infectious insults (27–29). One study by Agbor-Enoh and colleagues found the presence of ddcfDNA at a median of 2.8 months before a clinical diagnosis of AMR, even in the absence of spirometric or histologic changes at the time. Cases of AMR in this group were found to have a greater burden of ddcfDNA than in cases of acute cellular rejection (29). While data have been promising so far, more study will be needed to define the clinical utility of this biomarker in the diagnosis and management of rejection.
Given the risks of both acute rejection and CLAD seen after transplantation in the presence of DSAs, numerous strategies for pre-transplant antibody depletion have been investigated. Optimal management of pre-transplant DSAs is poorly defined, and practice varies widely by transplant center; agents trialed include intravenous immunoglobulin (IVIG), plasma exchange (PLEX), monoclonal antibodies, and proteasome inhibitors, with only limited data supporting any particular regimen.
One study demonstrated that peri-operative desensitization in patients with pre-transplant DSAs using a combination of PLEX, IVIG, and anti-thymocyte globulin led to CLAD-free survival comparable to unsensitized patients at a median follow-up of 6.7 years (30); another similar study trialed PLEX, IVIG, anti-thymocyte globulin, and mycophenolic acid and found graft survival and spirometry parameters similar to unsensitized patients at 1 year (31). These data support the efficacy of antibody depletion in the presence of pre-transplant DSAs, however evidence supporting the routine depletion of third-party HLA antibodies preoperatively has been conflicting (32, 33).
Continued research into optimal perioperative anti-HLA antibody management will be essential to expand transplant eligibility to allosensitized patients (34). Of late, one case report showed that imlifidase, an IgG-degrading enzyme derived from Streptococcus pyogenes, was effective in depleting donor-specific antibodies to allow for safe transplant in a sensitized patient (35).
Most patients are maintained on a three-agent calcineurin inhibitor-based immunosuppression regimen for prevention of both antibody mediated and cellular rejection, however a significant fraction will still develop donor-specific antibodies at some point after transplant. The benefit of treating these de novo DSAs in the absence of clinical rejection is uncertain. Several retrospective studies have found at least similar outcomes to unsensitized patients when de novo DSAs are treated pre-emptively (36, 37), including a recent study by Keller et al. finding that treatment of clinically silent DSAs was associated with lower risk of CLAD or death (38).
While pre-emptive clearance of DSAs may be helpful, data supporting an optimal antibody depletion regimen are lacking. One study of a combination of PLEX and Rituximab demonstrated efficacy in clearing clinically silent DSAs, but failed to show an improvement in survival or incidence of rejection (39). In a head-to-head comparison of Rituximab and carfilzomib when given for pre-emptive depletion of de novo antibodies both agents were found to effectively reduce the MFI of de novo DSAs with comparable CLAD-free survival, however Rituximab was associated with less decline in spirometry and a greater duration of DSA clearance (40). Recently, a randomized controlled trial of belatacept, an inhibitor of T-cell signaling agent used in kidney transplantation, as a component of a post-transplant maintenance immunosuppression regimen was stopped early due to increased mortality; no difference in DSA formation was found (41).
Given the severity of illness associated with antibody-mediated rejection, and particularly hyperacute rejection, there is a strong impetus for antibody depletion in clinical AMR. Outcomes in AMR remain poor despite treatment, with increased risk of progression to CLAD and one study reporting a 26 percent 30-day mortality rate (23, 42–44). There is little consensus on the optimal management of AMR, however most centers rely on a combination of antibody-depleting therapies to include PLEX, IVIG, and Rituximab; a variety of other immunologic and small molecule therapies have been studied in recent years as adjuncts to these as well.
Carfilzomib, for example, was shown in a small observational study to effectively clear C1q + positivity in 10 of 14 patients with AMR when given with IVIG and PLEX, and this improvement was associated with stabilization of FEV1 (45). C5 complement inhibition has been shown to produce favorable effects in mouse models of lung transplantation with anti-C5 therapies being associated with lower rejection scores (46). Ecilizumab in particular has shown clinical promise in kidney transplantation in reducing antibody mediated rejection, however data in lung transplant is limited to case reports (47). Daratumamab has also been explored as an anti-rejection agent in kidney and heart transplant, with data suggesting it could be explored as an option for AMR in lung transplantation (48–50). One recent report compared groups treated for AMR with various antibody-depleting therapies and found that combination regimens including tocilizumab, an anti-IL 6 therapy, had greater clearance of DSAs and graft survival. Lastly, exploration of regulatory T-cells and bronchus-associated lymphoid tissue has highlighted the ability for local T-cells to reduce B-cell activity in allografts and may be a future therapeutic target (51).
As summarized above, there are only limited data supporting the choice of any specific antibody depletion regimen in lung transplantation; a selection of some of the available evidence for each is presented in Table 1.
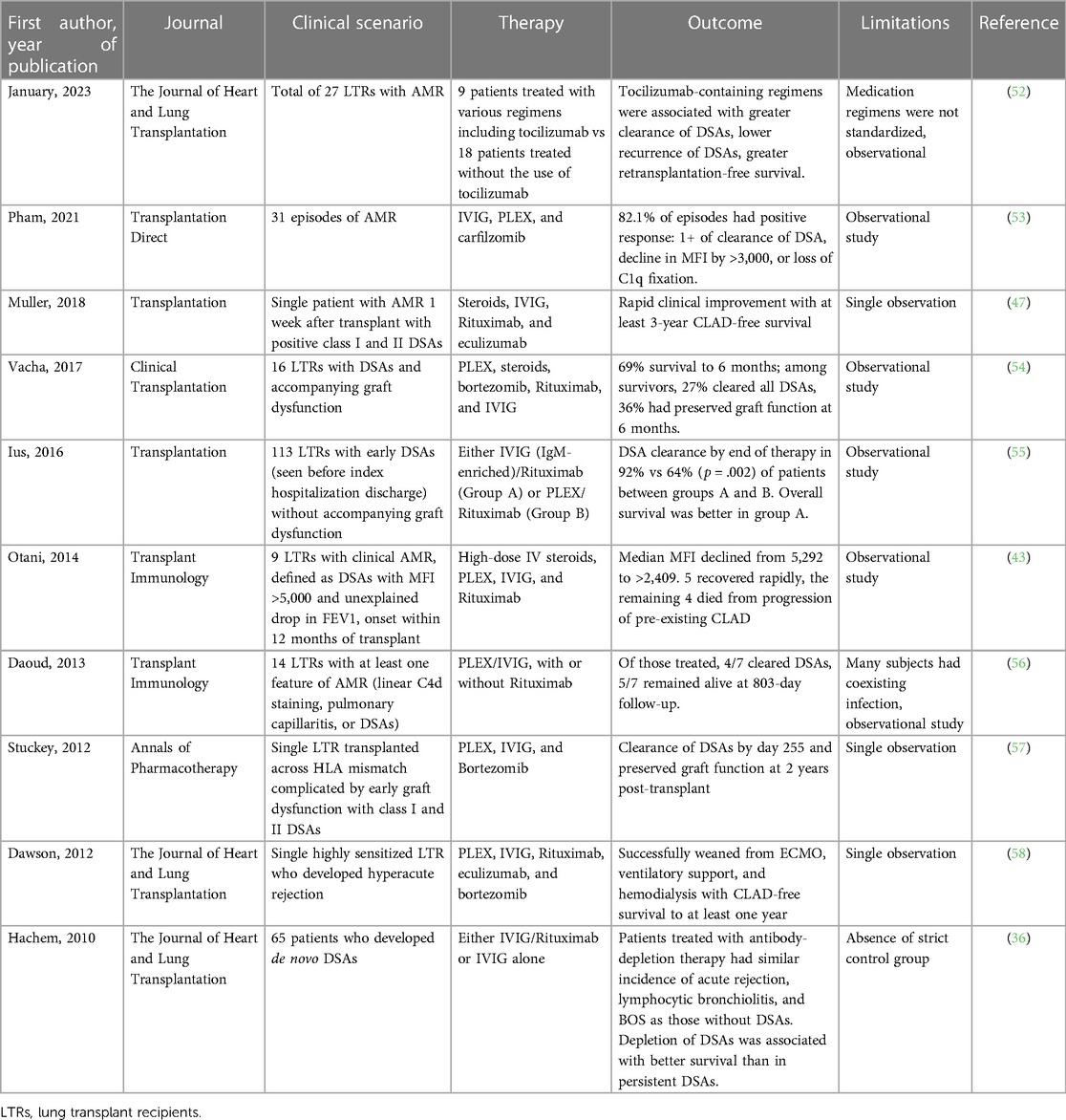
Table 1. Selection of evidence for specific antibody-depletion regimens in lung transplantation.
The development of antibodies to donor HLA antigens is a challenging problem in lung transplantation both for donor selection as well as for long-term graft function. There is a wealth of literature supporting the deleterious effects of donor-specific antibodies pre- and post-operatively, however high-quality data supporting the indications for DSA clearance and optimal treatment regimens are lacking. Areas of active research interest include the use of ddcfDNA for the identification of graft injury and computational models for the prediction of post-operative DSA development. Given the critical need for donor lungs and disappointing long-term graft function outcomes, further investigation into optimal management of DSAs will be essential both to expand the donor pool and produce more durable graft function post-operatively.
All included authors contributed to either the conception, writing, or editing of this product. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Chambers DC, Perch M, Zuckermann A, Cherikh WS, Harhay MO, Hayes D, et al. The international thoracic organ transplant registry of the international society for heart and lung transplantation: thirty-eighth adult lung transplantation report—2021; focus on recipient characteristics. J Heart Lung Transplant. (2021) 40(10):1060–72. doi: 10.1016/j.healun.2021.07.021
2. Hourmant M, Cesbron-Gautier A, Terasaki PI, Mizutani K, Moreau A, Meurette A, et al. Frequency and clinical implications of development of donor-specific and non-donor-specific HLA antibodies after kidney transplantation. J Am Soc Nephrol. (2005) 16(9):2804–12. doi: 10.1681/ASN.2004121130
3. Hachem RR, Tiriveedhi V, Patterson GA, Aloush A, Trulock EP, Mohanakumar T. Antibodies to K-α 1 tubulin and collagen V are associated with chronic rejection after lung transplantation. Am J Transplant. (2012) 12(8):2164–71. doi: 10.1111/j.1600-6143.2012.04079.x
4. Reinsmoen NL, Mirocha J, Ensor CR, Marrari M, Chaux G, Levine DJ, et al. A 3-center study reveals new insights into the impact of non-HLA antibodies on lung transplantation outcome. Transplantation. (2017) 101(6):1215–21. doi: 10.1097/TP.0000000000001389
5. Smith JD, Ibrahim MW, Newell H, Danskine AJ, Soresi S, Burke MM, et al. Pre-transplant donor HLA-specific antibodies: characteristics causing detrimental effects on survival after lung transplantation. J Heart Lung Transplant. (2014) 33(10):1074–82. doi: 10.1016/j.healun.2014.02.033
6. Brugière O, Suberbielle C, Thabut G, Lhuillier E, Dauriat G, Metivier AC, et al. Lung transplantation in patients with pretransplantation donor-specific antibodies detected by luminex assay. Transplantation. (2013) 95(5):761–5. doi: 10.1097/TP.0b013e31827afb0f
7. Courtwright AM, Cao S, Wood I, Mallidi HR, Kawasawa J, Moniodis A, et al. Clinical outcomes of lung transplantation in the presence of donor-specific antibodies. Ann Am Thorac Soc. (2019) 16(9):1131–7. doi: 10.1513/AnnalsATS.201812-869OC
8. Courtwright AM, Kamoun M, Diamond JM, Kearns J, Ahya VN, Christie JD, et al. Lung transplantation outcomes after crossing low-level donor specific antibodies without planned augmented immunosuppression. Clin Transplant. (2021) 35(11):e14447. doi: 10.1111/ctr.14447
9. Tikkanen JM, Singer LG, Kim SJ, Li Y, Binnie M, Chaparro C, et al. De novo DQ donor-specific antibodies are associated with chronic lung allograft dysfunction after lung transplantation. Am J Respir Crit Care Med. (2016) 194(5):596–606. doi: 10.1164/rccm.201509-1857OC
10. Hachem RR, Kamoun M, Budev MM, Askar M, Ahya VN, Lee JC, et al. Human leukocyte antigens antibodies after lung transplantation: primary results of the HALT study. Am J Transplant. (2018) 18(9):2285–94. doi: 10.1111/ajt.14893
11. Verleden SE, Vanaudenaerde BM, Emonds MP, Van Raemdonck DE, Neyrinck AP, Verleden GM, et al. Donor-specific and -nonspecific HLA antibodies and outcome post lung transplantation. Eur Respir J. (2017) 50(5):761–5. doi: 10.1183/13993003.01248-2017
12. Islam AK, Sinha N, DeVos JM, Kaleekal TS, Jyothula SS, Teeter LD, et al. Early clearance vs persistence of de novo donor-specific antibodies following lung transplantation. Clin Transplant. (2017) 31(8). doi: 10.1111/ctr.13028 [Epub ahead of print]28658512
13. Le Pavec J, Suberbielle C, Lamrani L, Feuillet S, Savale L, Dorfmüller P, et al. De-novo donor-specific anti-HLA antibodies 30 days after lung transplantation are associated with a worse outcome. J Heart Lung Transplant. (2016) 35(9):1067–77. doi: 10.1016/j.healun.2016.05.020
14. Ius F, Sommer W, Tudorache I, Kühn C, Avsar M, Siemeni T, et al. Early donor-specific antibodies in lung transplantation: risk factors and impact on survival. J Heart Lung Transplant. (2014) 33(12):1255–63. doi: 10.1016/j.healun.2014.06.015
15. Safavi S, Robinson DR, Soresi S, Carby M, Smith JD. De novo donor HLA-specific antibodies predict development of bronchiolitis obliterans syndrome after lung transplantation. J Heart Lung Transplant. (2014) 33(12):1273–81. doi: 10.1016/j.healun.2014.07.012
16. Morrell MR, Pilewski JM, Gries CJ, Pipeling MR, Crespo MM, Ensor CR, et al. De novo donor-specific HLA antibodies are associated with early and high-grade bronchiolitis obliterans syndrome and death after lung transplantation. J Heart Lung Transplant. (2014) 33(12):1288–94. doi: 10.1016/j.healun.2014.07.018
17. Snyder LD, Wang Z, Chen DF, Reinsmoen NL, Finlen-Copeland CA, Davis WA, et al. Implications for human leukocyte antigen antibodies after lung transplantation: a 10-year experience in 441 patients. Chest. (2013) 144(1):226–33. doi: 10.1378/chest.12-0587
18. Iasella CJ, Ensor CR, Marrari M, Mangiola M, Xu Q, Nolley E, et al. Donor-specific antibody characteristics, including persistence and complement-binding capacity, increase risk for chronic lung allograft dysfunction. J Heart Lung Transplant. (2020) 39(12):1417–25. doi: 10.1016/j.healun.2020.09.003
19. Kulkarni HS, Tsui K, Sunder S, Ganninger A, Tague LK, Witt CA, et al. Pseudomonas aeruginosa and acute rejection independently increase the risk of donor-specific antibodies after lung transplantation. Am J Transplant. (2020) 20(4):1028–38. doi: 10.1111/ajt.15687
20. Lobashevsky A, Niemann M, Kowinski B, Higgins N, Abdel-Wareth L, Atrabulsi B, et al. Formation of donor-specific antibodies depends on the epitope load of mismatched HLAs in lung transplant recipients: a retrospective single-center study. Clin Transplant. (2022) 36(9):e14755. doi: 10.1111/ctr.14755
21. Bedford A, Jervis S, Worthington J, Lowe M, Poulton K. Human leukocyte antigen epitope mismatch loads and the development of de novo donor-specific antibodies in cardiothoracic organ transplantation. Int J Immunogenet. (2022) 49(1):30–8. doi: 10.1111/iji.12563
22. Levine DJ, Glanville AR, Aboyoun C, Belperio J, Benden C, Berry GJ, et al. Antibody-mediated rejection of the lung: a consensus report of the international society for heart and lung transplantation. J Heart Lung Transplant. (2016) 35(4):397–406. doi: 10.1016/j.healun.2016.01.1223
23. Aguilar PR, Carpenter D, Ritter J, Yusen RD, Witt CA, Byers DE, et al. The role of C4d deposition in the diagnosis of antibody-mediated rejection after lung transplantation. Am J Transplant. (2018) 18(4):936–44. doi: 10.1111/ajt.14534
24. Roberts JA, Barrios R, Cagle PT, Ge Y, Takei H, Haque AK, et al. The presence of anti-HLA donor-specific antibodies in lung allograft recipients does not correlate with C4d immunofluorescence in transbronchial biopsy specimens. Arch Pathol Lab Med. (2014) 138(8):1053–8. doi: 10.5858/arpa.2013-0539-OA
25. Yousem SA, Zeevi A. The histopathology of lung allograft dysfunction associated with the development of donor-specific HLA alloantibodies. Am J Surg Pathol. (2012) 36(7):987–92. doi: 10.1097/PAS.0b013e31825197ae
26. Wallace WD, Li N, Andersen CB, Arrossi AV, Askar M, Berry GJ, et al. Banff study of pathologic changes in lung allograft biopsy specimens with donor-specific antibodies. J Heart Lung Transplant. (2016) 35(1):40–8. doi: 10.1016/j.healun.2015.08.021
27. Jang MK, Tunc I, Berry GJ, Marboe C, Kong H, Keller MB, et al. Donor-derived cell-free DNA accurately detects acute rejection in lung transplant patients, a multicenter cohort study. J Heart Lung Transplant. (2021) 40(8):822–30. doi: 10.1016/j.healun.2021.04.009
28. Khush KK, De Vlaminck I, Luikart H, Ross DJ, Nicolls MR. Donor-derived, cell-free DNA levels by next-generation targeted sequencing are elevated in allograft rejection after lung transplantation. ERJ Open Res. (2021) 7(1). doi: 10.1183/23120541.00462-2020
29. Agbor-Enoh S, Jackson AM, Tunc I, Berry GJ, Cochrane A, Grimm D, et al. Late manifestation of alloantibody-associated injury and clinical pulmonary antibody-mediated rejection: evidence from cell-free DNA analysis. J Heart Lung Transplant. (2018) 37(7):925–32. doi: 10.1016/j.healun.2018.01.1305
30. Aversa M, Martinu T, Patriquin C, Cypel M, Barth D, Ghany R, et al. Long-term outcomes of sensitized lung transplant recipients after peri-operative desensitization. Am J Transplant. (2021) 21(10):3444–8. doi: 10.1111/ajt.16707
31. Tinckam KJ, Keshavjee S, Chaparro C, Barth D, Azad S, Binnie M, et al. Survival in sensitized lung transplant recipients with perioperative desensitization. Am J Transplant. (2015) 15(2):417–26. doi: 10.1111/ajt.13076
32. Appel JZ, Hartwig MG, Davis RD, Reinsmoen NL. Utility of peritransplant and rescue intravenous immunoglobulin and extracorporeal immunoadsorption in lung transplant recipients sensitized to HLA antigens. Hum Immunol. (2005) 66(4):378–86. doi: 10.1016/j.humimm.2005.01.025
33. Snyder LD, Gray AL, Reynolds JM, Arepally GM, Bedoya A, Hartwig MG, et al. Antibody desensitization therapy in highly sensitized lung transplant candidates. Am J Transplant. (2014) 14(4):849–56. doi: 10.1111/ajt.12636
34. Tague LK, Witt CA, Byers DE, Yusen RD, Aguilar PR, Kulkarni HS, et al. Association between allosensitization and waiting list outcomes among adult lung transplant candidates in the United States. Ann Am Thorac Soc. (2019) 16(7):846–52. doi: 10.1513/AnnalsATS.201810-713OC
35. Roux A, Bunel V, Belousova N, Messika J, Tanaka S, Salpin M, et al. First use of imlifidase desensitization in a highly sensitized lung transplant candidate: a case report. Am J Transplant. (2023) 23(2):294–7. doi: 10.1016/j.ajt.2022.11.025
36. Hachem RR, Yusen RD, Meyers BF, Aloush AA, Mohanakumar T, Patterson GA, et al. Anti-human leukocyte antigen antibodies and preemptive antibody-directed therapy after lung transplantation. J Heart Lung Transplant. (2010) 29(9):973–80. doi: 10.1016/j.healun.2010.05.006
37. Ius F, Verboom M, Sommer W, Poyanmehr R, Knoefel AK, Salman J, et al. Preemptive treatment of early donor-specific antibodies with IgA- and IgM-enriched intravenous human immunoglobulins in lung transplantation. Am J Transplant. (2018) 18(9):2295–304. doi: 10.1111/ajt.14912
38. Keller M, Yang S, Ponor L, Bon A, Cochrane A, Philogene M, et al. Preemptive treatment of de novo donor-specific antibodies in lung transplant patients reduces subsequent risk of chronic lung allograft dysfunction or death. Am J Transplant. (2023) 23(4):559–64. doi: 10.1016/j.ajt.2022.12.019
39. Ius F, Sommer W, Tudorache I, Kühn C, Avsar M, Siemeni T, et al. Preemptive treatment with therapeutic plasma exchange and rituximab for early donor-specific antibodies after lung transplantation. J Heart Lung Transplant. (2015) 34(1):50–8. doi: 10.1016/j.healun.2014.09.019
40. Razia D, Hu C, Cherrier L, Nasar A, Walia R, Tokman S. Carfilzomib versus rituximab for treatment of de novo donor-specific antibodies in lung transplant recipients. Transpl Immunol. (2022) 75:101703. doi: 10.1016/j.trim.2022.101703
41. Huang HJ, Schechtman K, Askar M, Bernadt C, Mittler B, Dore P, et al. A pilot randomized controlled trial of de novo belatacept-based immunosuppression following anti-thymocyte globulin induction in lung transplantation. Am J Transplant. (2022) 22(7):1884–92. doi: 10.1111/ajt.17028
42. Witt CA, Gaut JP, Yusen RD, Byers DE, Iuppa JA, Bennett Bain K, et al. Acute antibody-mediated rejection after lung transplantation. J Heart Lung Transplant. (2013) 32(10):1034–40. doi: 10.1016/j.healun.2013.07.004
43. Otani S, Davis AK, Cantwell L, Ivulich S, Pham A, Paraskeva MA, et al. Evolving experience of treating antibody-mediated rejection following lung transplantation. Transpl Immunol. (2014) 31(2):75–80. doi: 10.1016/j.trim.2014.06.004
44. Bery AI, Hachem RR. Antibody-mediated rejection after lung transplantation. Ann Transl Med. (2020) 8(6):411. doi: 10.21037/atm.2019.11.86
45. Ensor CR, Yousem SA, Marrari M, Morrell MR, Mangiola M, Pilewski JM, et al. Proteasome inhibitor carfilzomib-based therapy for antibody-mediated rejection of the pulmonary allograft: use and short-term findings. Am J Transplant. (2017) 17(5):1380–8. doi: 10.1111/ajt.14222
46. Shiina Y, Suzuki H, Hata A, Kaiho T, Matsumoto H, Toyoda T, et al. Antibodies against complement component C5 prevent antibody-mediated rejection after lung transplantation in murine orthotopic models with skin-graft-induced pre-sensitization. Gen Thorac Cardiovasc Surg. (2022) 70(12):1032–41. doi: 10.1007/s11748-022-01844-0
47. Muller YD, Aubert JD, Vionnet J, Rotman S, Sadallah S, Aubert V, et al. Acute antibody-mediated rejection 1 week after lung transplantation successfully treated with eculizumab, intravenous immunoglobulins, and rituximab. Transplantation. (2018) 102(6):e301–3. doi: 10.1097/TP.0000000000002165
48. Aguilera Agudo C, Gómez Bueno M, Krsnik Castello I. Daratumumab for antibody-mediated rejection in heart transplant-A novel therapy: successful treatment of antibody-mediated rejection. Transplantation. (2021) 105(3):e30–1. doi: 10.1097/TP.0000000000003505
49. Doberer K, Kläger J, Gualdoni GA, Mayer KA, Eskandary F, Farkash EA, et al. CD38 antibody daratumumab for the treatment of chronic active antibody-mediated kidney allograft rejection. Transplantation. (2021) 105(2):451–7. doi: 10.1097/TP.0000000000003247
50. Fenton M, Shaw K, Murchan H, Duignan S, Dunne E, McMahon CJ. Daratumumab provides transient response of antibody mediated rejection post pediatric orthotopic heart transplantation. J Heart Lung Transplant. (2022) 41(10):1529–30. doi: 10.1016/j.healun.2022.06.017
51. Li W, Gauthier JM, Higashikubo R, Hsiao HM, Tanaka S, Vuong L, et al. Bronchus-associated lymphoid tissue-resident Foxp3+ T lymphocytes prevent antibody-mediated lung rejection. J Clin Invest. (2019) 129(2):556–68. doi: 10.1172/JCI122083
52. January SE, Fester KA, Halverson LP, Witt CA, Byers DE, Vazquez-Guillamet R, et al. Tocilizumab for antibody mediated rejection treatment in lung transplantation. J Heart Lung Transplant. (2023). doi: 10.1016/j.healun.2023.05.012 [Epub ahead of print]37268051
53. Pham C, Pierce BJ, Nguyen DT, Graviss EA, Huang HJ. Assessment of carfilzomib treatment response in lung transplant recipients with antibody-mediated rejection. Transplant Direct. (2021) 7(4):e680. doi: 10.1097/TXD.0000000000001131
54. Vacha M, Chery G, Hulbert A, Byrns J, Benedetti C, Finlen Copeland CA, et al. Antibody depletion strategy for the treatment of suspected antibody-mediated rejection in lung transplant recipients: does it work? Clin Transplant. (2017) 31(3). doi: 10.1111/ctr.12886 [Epub ahead of print]27988971
55. Ius F, Sommer W, Kieneke D, Tudorache I, Kühn C, Avsar M, et al. IgM-enriched human intravenous immunoglobulin-based treatment of patients with early donor specific anti-HLA antibodies after lung transplantation. Transplantation. (2016) 100(12):2682–92. doi: 10.1097/TP.0000000000001027
56. Daoud AH, Betensley AD. Diagnosis and treatment of antibody mediated rejection in lung transplantation: a retrospective case series. Transpl Immunol. (2013) 28(1):1–5. doi: 10.1016/j.trim.2012.11.009
57. Stuckey LJ, Kamoun M, Chan KM. Lung transplantation across donor-specific anti-human leukocyte antigen antibodies: utility of bortezomib therapy in early graft dysfunction. Ann Pharmacother. (2012) 46(1):e2. doi: 10.1345/aph.1Q509
Keywords: donor-specific antibodies, antibody-mediated rejection, lung transplant, desensitization, immunology, donor-derived cell free DNA
Citation: Brandon W, Dunn C, Bollineni S, Joerns J, Lawrence A, Mohanka M, Timofte I, Torres F and Kaza V (2023) Management of donor-specific antibodies in lung transplantation. Front. Transplant. 2:1248284. doi: 10.3389/frtra.2023.1248284
Received: 27 June 2023; Accepted: 23 August 2023;
Published: 29 September 2023.
Edited by:
Thalachallour Mohanakumar, St. Joseph’s Hospital and Medical Center, United StatesReviewed by:
Letizia Corinna Morlacchi, Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico di Milano, Italy© 2023 Brandon, Dunn, Bollineni, Joerns, Lawrence, Mohanka, Timofte, Torres and Kaza. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vaidehi Kaza dmFpZGVoaS5rYXphQHV0c291dGh3ZXN0ZXJuLmVkdQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.