 Jieru Wang
Jieru Wang Guangcai Yu
Guangcai Yu Tianzi Jian
Tianzi Jian Baotian Kan
Baotian Kan Wei Li3*
Wei Li3* Xiangdong Jian
Xiangdong Jian
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Toxicol., 27 February 2025
Sec. Clinical Toxicology
Volume 7 - 2025 | https://doi.org/10.3389/ftox.2025.1557990
Background: Methemoglobinemia can be inherited or acquired. Acquired forms are more common due to drugs or poisonous substances that oxidize hemoglobin, and pesticide-related cases are notably rare.
Case Presentation: We report a 69-year-old woman who ingested 30 mL of tebufenozide and indoxacarb and was asymptomatic for 3 h; however, the patient was admitted to the hospital after 8 h, unconscious, with tachypnea, cyanosis, and 61.9% methemoglobin. The patient was administered methylene blue, mechanically ventilated, and hemoperfused. Subsequently, the patient recovered and was discharged with no discomfort and with normal laboratory test results.
Conclusion: Tebufenozide and indoxacarb may cause methemoglobinemia, leading to cyanosis, unconsciousness, and respiratory failure; therefore, they should be handled with care in clinical practice.
Methemoglobinemia is a rare clinical condition manifesting as excessive methemoglobin (MetHb) in the blood due to the oxidation of iron from the Fe2+ to the Fe3+ state (Yu et al., 2022; McNulty et al., 2022). MetHb can reduce oxygen-binding capacity and shift the oxygen dissociation curve to the left, leading to anemia, hypoxia, and tissue damage. Additionally, the hypoxia is refractory to oxygen supplementation (McNulty et al., 2022; Shi et al., 2022). Methemoglobinemia can be congenital or acquired. Acquired methemoglobinemia are more common and are frequently caused by exogenous substances such as nitrates, nitrites, local anesthetics (e.g., benzocaine, prilocaine, and lignocaine), dapsone, and aniline (which requires metabolic activation) (Kamath et al., 2022; Belzer and Krasowski, 2024). Pesticide-related methemoglobinemia are rare. We present a case involving the ingestion of tebufenozide and indoxacarb, which illustrates the intoxication mechanism and reviews diagnostic clues and treatment options.
This study was approved by the Ethics Committee of Shandong University Qilu Hospital (KYLL-202309-028). The family of the patient provided written informed consent for participation in this study, which included a data availability statement.
A 69-year-old woman (height, 160 cm; weight, 65 kg) with a history of diabetes mellitus but no hereditary disorders was admitted at a local hospital unconscious and with cyanosis 8 h after ingesting 30 mL of an insecticide (tebufenozide and indoxacarb, W/V, 8%). The patient had no discomfort and fell asleep after taking 0.8 mg of alprazolam. The patient had no significant abnormalities 5 h after ingestion of the insecticide; however, the patient became unconscious with tachypnea and cyanosis an hour later and was admitted with a Glasgow Coma Scale score of 6 (E1V2M3), body temperature of 35.5°C, heart and respiratory rate of 63 and 28 bpm, respectively, blood pressure 179/79 mmHg, and pulse oximetry of 70%. The lips and nail beds of the patient exhibited cyanosis; however, heart and chest examination results were normal. Arterial blood gas (ABG) analysis using FiO2 (fraction of inspired oxygen) at 60% revealed a pH of 7.36, arterial oxygen pressure (PaO2) of 315 mmHg, oxyhemoglobin of 36.3%, actual bicarbonate of 28.2 mmol/L, and MetHb of 61.9% (Table 1). Gastric lavage, endotracheal intubation, mechanical ventilation, and methylene blue (MB) were administered. The MetHb level of the patient decreased from 61.9% to 20.3% and 9.3% after intravenous administration of 120 and 60 mg of MB, respectively. The patient was transferred to the Shandong University of Qilu Hospital 14 h after receiving 40 mg of MB in transit. The MetHb levels after different doses of MB are shown in Figure 1. The patient and her family had no known history of hemolysis. On admission, the vitals of the patient were stable under sedation. The ABG results FiO2 40% indicated a pH of 7.47, partial oxygen pressure (PO2) of 241.8 mmHg, O2 concentration of 97.4%, and MetHb of 1.5%. Tebufenozide and indoxacarb blood levels were 0.097 μg/mL and 0.059 μg/mL, respectively. Peripheral blood cells, hepatic and renal function, myocardial enzymes, electrolytes, coagulation function, and cholinesterase levels were normal. After hemoperfusion and symptomatic treatment, the patient regained consciousness, had stable vital signs, and was disconnected from mechanical ventilation. Once the patient’s consciousness was restored, a thorough account of the poisoning was collected. The patient was discharged 4 days after insecticide ingestion with no discomfort and normal laboratory test results. Three days post-discharge, the patient underwent routine blood tests, along with liver and kidney function evaluations at a local hospital, all showing normal results. The examination 15 days after poisoning revealed no abnormalities in physical or neurological assessments. Comprehensive testing, including electrocardiogram, blood routine, urinalysis, liver and renal function, myocardial enzymes, and coagulation profile, was unremarkable.
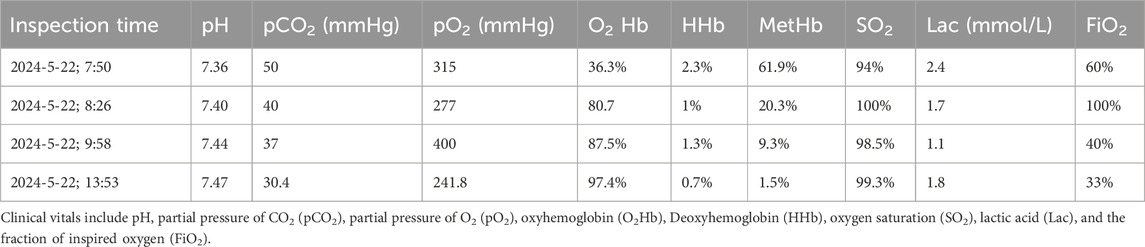
Table 1. Arterial blood gases of the patient investigated in this study.
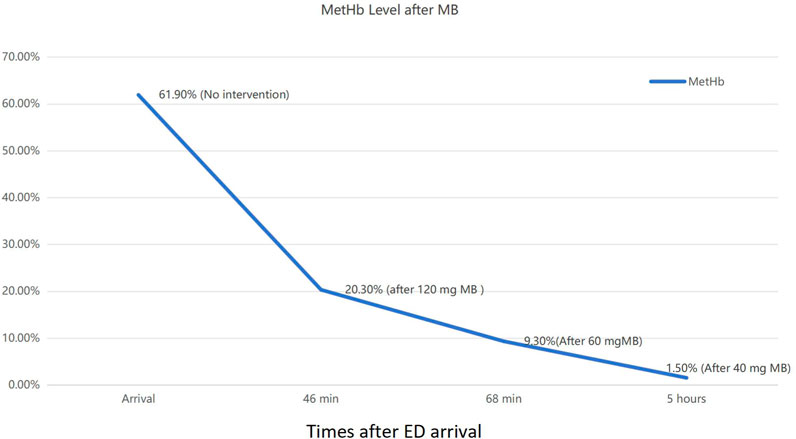
Figure 1. Patient methemoglobin (MetHb) levels after methylene blue (MB) administration.
Tebufenozide, an insect growth regulator that mimics ecdysone, causes premature and incomplete molting and controls lepidopteran pests (Yu et al., 2016). Tebufenozide is less toxic to vertebrates and invertebrates (LD50 > 5,000 mg/kg for oral uptake) than other insecticides (Addison, 1996; Abass, 2016). Potential metabolites of tebufenozide-like aromatic amines may induce methemoglobinemia; however, detoxification prevents their formation in hepatic microsomes (Abass, 2016). Therefore, although low doses of tebufenozide are not expected to cause methemoglobinemia and no cases have been reported, this association remains uncertain and requires further verification in clinical cases. Indoxacarb is a broad-spectrum non-organophosphorus oxadiazine pro-insecticide with active metabolites inhibiting voltage-gated sodium channels in insect nerve cells, impairing nerve function and leading to death (Lin et al., 2023). Indoxacarb has low mammalian toxicity, with oral absorption of approximately 60% and primary accumulation in fat tissues and red blood cells (European Food Safety Authority EFSA et al., 2018). Indoxacarb can be metabolized into active aromatic intermediates, which may lead to methemoglobinemia, hemolytic anemia, acute kidney injury, and rhabdomyolysis (Jin, 2012; Park et al., 2011; Sivanandam et al., 2024).
Methemoglobinemia severity directly correlates with MetHb levels, affecting tissue oxygen delivery. Possible symptoms include: asymptomatic, pale or gray skin, and low pulse oximetry (MetHb < 10%); cyanosis, dark brown blood, tachycardia, lightheadedness, anxiety, and confusion (MetHb ≥ 10%); fatigue, dyspnea, chest pain, dizziness, headache, and syncope (MetHb ≥ 30%); tachypnea, acidosis, dysrhythmias, delirium, seizures, and coma (MetHb ≥ 50%); and severe hypoxemia or death (MetHb ≥ 70%) (Iolascon et al., 2021; Khan et al., 2020). Other symptoms used for the diagnosis include central cyanosis (Iolascon et al., 2021), chocolate-colored arterial blood (Warren and Blackwood, 2019), an oxygen saturation gap (Das and Singh, 2024), and low pulse oximeter readings (SpO2) (Ward et al., 2019). These abnormalities, which are not influenced by cardiac or respiratory factors, do not improve effectively with supplemental oxygen. Notably, the saturation gap, which is the difference between PaO2 and SpO2, may increase with oxygen therapy (Das and Singh, 2024). Standard pulse oximeters cannot differentiate between bound hemoglobin forms, including dyshemoglobins, which are unsuitable for evaluating methemoglobinemia severity (Ward et al., 2019). In our case, the percentages of O2Hb, HHb, and MetHb do not add up to 100%, with a total exceeding 100%. We speculate that the differences observed may arise from the interference of methemoglobin with certain measurement parameters.
Treatment of methemoglobinemia should be based on the symptoms of the patient, MetHb levels, and underlying causes. MB administration is the primary treatment for symptomatic patients with MetHb levels >20% and asymptomatic patients with MetHb levels >30% (Khan et al., 2020). Before administering MB the patient’s G6PD Deficiency should be assessed. This is crucial as G6PD deficiency can influence the response to MB treatment and predispose individuals to hemolysis. MB is administered intravenously at an initial dose of 1–2 mg/kg for over >3–5 min, with a maximum dose of 5.5 mg/kg, as doses exceeding 7 mg/kg can worsen the condition (Iolascon et al., 2021). MetHb levels require repeated tests every 30 min, and if no significant decrease is observed, re-administration is necessary (Tseung et al., 2023). The patient was administered 40 mg of methylene blue, reducing the MetHb level from 9.3% to 1.5%, demonstrating the therapeutic potential of methylene blue at doses below the commonly cited range of 1–2 mg/kg body weight. Ascorbic acid can substitute MB or can be contraindicated to reduce oxidative stress and MetHb levels. There is no standardized optimal ascorbic acid dosage, and its effects are slower than those of MB. Previous case reports suggested that effective doses range from 1 to 10 g (Park et al., 2017; Park et al., 2014). N-acetylcysteine is reported to treat methemoglobinemia, but some studies have indicated that it does not reduce MetHb levels in vitro or in human volunteers (Dötsch et al., 2000; Tanen et al., 2000).
Timely clearance of poisons is crucial for minimizing systemic effects and enhancing patient outcomes due to their dose-dependent toxicity. Gastric lavage and bowel irrigation can remove poisons from the gastrointestinal tract before absorption by the body (Zellner et al., 2019; Carboni Bisso et al., 2020). Blood purification can remove absorbed poisons from the bloodstream and ameliorate metabolic imbalances (Saleh et al., 2022). Although indoxacarb is lipid-soluble, the concentration of indoxacarb in plasma was found to be about one-fifth of its concentration in red blood cells (Ai et al., 2024), indicating that its plasma protein binding rate is relatively low. This suggesting that hemoperfusion should not be utilized as a primary therapeutic measure for tebufenozide-indoxacarb poisoning. Blood transfusions and exchanges can restore normal hemoglobin levels; however, their effectiveness may be compromised by residual poisons. Although high-flow oxygen does not increase oxygen saturation levels, it can increase dissolved oxygen concentration, as indicated by the PO2, which is the form available to tissues; thus, it can partially alleviate tissue hypoxia (Lien et al., 2021). Mechanical ventilation and extracorporeal membrane oxygenation can increase dissolved oxygen levels and provide essential life support, benefiting patients with refractory methemoglobinemia (Lien et al., 2021; Zuo et al., 2023). Additionally, methemoglobinemia-related complications such as hemolytic anemia, acute kidney injury, and toxic encephalopathy require monitoring and timely intervention.
This study described the successful treatment of methemoglobinemia caused by ingestion of tebufenozide and indoxacarb using MB, and mechanical ventilation. Although insecticides rarely cause methemoglobinemia, this case illustrates that they must be considered as causal agents.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
This study was approved by the Ethics Committee of Shandong University Qilu Hospital (KYLL-202309-028). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
JW: Writing - original draft, Writing - review and editing, Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization. GY: Writing - original draft, Writing - review and editing, Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization. TJ: Writing - original draft, Writing - review and editing, Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization. BK: Writing - original draft, Writing - review and editing, Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization. WL: Writing - original draft, Writing - review and editing, Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization. XJ: Writing - original draft, Writing - review and editing, Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
We would like to thank Editage (www.editage.cn) for English language editing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abass, K. M. (2016). An investigation into the formation of tebufenozide's toxic aromatic amine metabolites in human in vitro hepatic microsomes. Pestic. Biochem. Physiol. 133, 73–78. doi:10.1016/j.pestbp.2016.03.001
Addison, J. A. (1996). Safety testing of tebufenozide, a new molt-inducing insecticide, for effects on nontarget forest soil invertebrates. Ecotoxicol. Environ. Saf. 33 (1), 55–61. doi:10.1006/eesa.1996.0006
Ai, J., Li, J., Chang, A. K., Pei, Y., Li, H., Liu, K., et al. (2024). Toxicokinetics and bioavailability of indoxacarb enantiomers and their new metabolites in rats. Pestic. Biochem. Physiol. 203, 106024. doi:10.1016/j.pestbp.2024.106024
Belzer, A., and Krasowski, M. D. (2024). Causes of acquired methemoglobinemia A retrospective study at a large academic hospital. Toxicol. Rep. 12, 331–337. doi:10.1016/j.toxrep.2024.03.004
Carboni Bisso, I., Gemelli, N., Cordero, M. P., Barrios, C., and Pina, D. (2020). Whole bowel irrigation in dapsone intoxication with persistent methemoglobinemia. Am. J. Emerg. Med. 38 (10), 2246.e1–2246.e2. doi:10.1016/j.ajem.2020.05.056
Das, P., and Singh, G. (2024). Central cyanosis in acquired methemoglobinemia. N. Engl. J. Med. 390 (14), 1311. doi:10.1056/NEJMicm2304082
Dötsch, J., Demirakça, S., Kratz, M., Repp, R., Knerr, I., and Rascher, W. (2000). Comparison of methylene blue, riboflavin, and N-acetylcysteine for the reduction of nitric oxide-induced methemoglobinemia. Crit. Care Med. 28 (4), 958–961. doi:10.1097/00003246-200004000-00008
European Food Safety Authority (EFSA), Arena, M., Auteri, D., Barmaz, S., Bellisai, G., Brancato, A., Brocca, D., et al. (2018). Peer review of the pesticide risk assessment of the active substance indoxacarb. EFSA J. 16 (1), e05140. doi:10.2903/j.efsa.2018.5140
Iolascon, A., Bianchi, P., Andolfo, I., Russo, R., Barcellini, W., Fermo, E., et al. (2021). Recommendations for diagnosis and treatment of methemoglobinemia. Am. J. Hematol. 96 (12), 1666–1678. doi:10.1002/ajh.26340
Jin, K. (2012). Rhabdomyolysis, methemoglobinemia and acute kidney injury after indoxacarb poisoning. Clin. Toxicol. (Phila). 50 (3), 227. doi:10.3109/15563650.2012.657759
Kamath, S. D., Sunny, S., and Upadhyay, A. (2022). A case report of cyanosis with refractory hypoxemia: is it methemoglobinemia? Cureus 14 (11), e32053. doi:10.7759/cureus.32053
Khan, F. A., McIntyre, C., Khan, A. M., and Maslov, A. (2020). Headache and methemoglobinemia. Headache 60 (1), 291–297. doi:10.1111/head.13696
Lien, Y. H., Lin, Y. C., and Chen, R. J. (2021). A case report of acquired methemoglobinemia rescued by veno-venous extracorporeal membrane oxygenation. Med. Baltim. 100 (15), e25522. doi:10.1097/MD.0000000000025522
Lin, Q., Deng, P., Feng, T., Ou, G., Mou, L., and Zhang, Y. (2023). Enantioselectivity of indoxacarb enantiomers in Bombyx mori larvae: toxicity, bioaccumulation, and biotransformation. Pest Manag. Sci. 79 (7), 2353–2364. doi:10.1002/ps.7412
McNulty, R., Kuchi, N., Xu, E., and Gunja, N. (2022). Food-induced methemoglobinemia: a systematic review. J. Food Sci. 87 (4), 1423–1448. doi:10.1111/1750-3841.16090
Park, E. J., Lee, M., and Min, Y. G. (2017). Successful treatment of NO-induced methemoglobinemia with low-dose vitamin C. Clin. Toxicol. (Phila) 55 (7), 686. doi:10.1080/15563650.2017.1315126
Park, J. S., Kim, H., Lee, S. W., and Min, J. H. (2011). Successful treatment of methemoglobinemia and acute renal failure after indoxacarb poisoning. Clin. Toxicol. (Phila) 49 (8), 744–746. doi:10.3109/15563650.2011.602080
Park, S. Y., Lee, K. W., and Kang, T. S. (2014). High-dose vitamin C management in dapsone-induced methemoglobinemia. Am. J. Emerg. Med. 32, 684.e1–684.e6843. doi:10.1016/j.ajem.2013.11.036
Saleh, D., Lucyk, S., and McGillis, E. (2022). Methemoglobinemia caused by sodium nitrite overdose. CMAJ 194 (30), E1066–E1067. doi:10.1503/cmaj.220434
Shi, L., Yu, G., Zhao, L., Wen, Z., Li, Y., Kan, B., et al. (2022). Methemoglobinemia and delayed encephalopathy after 5-bromo-2-nitropyridine poisoning: a rare case report. Front. Public Health 10, 942003. doi:10.3389/fpubh.2022.942003
Sivanandam, L. K., Arunkumar, H., Marlecha, P., Madamanchi, V., Maheshwari, C., Naseer, M. Q., et al. (2024). Indoxacarb poisoning causing methemoglobinemia treated with parenteral vitamin C: a case report. J. Med. Case Rep. 18 (1), 157. doi:10.1186/s13256-024-04455-w
Tanen, D. A., LoVecchio, F., and Curry, S. C. (2000). Failure of intravenous N-acetylcysteine to reduce methemoglobin produced by sodium nitrite in human volunteers: a randomized controlled trial. Ann. Emerg. Med. 35 (4), 369–373. doi:10.1016/s0196-0644(00)70056-4
Tseung, S. B., Ng, W. Y., Leung, H. S., Tong, H. F., Mak, T. W., and Ching, C. K. (2023). Interference of methylene blue therapy on methaemoglobin measurement. Pathology 55 (3), 400–402. doi:10.1016/j.pathol.2022.07.018
Ward, J., Motwani, J., Baker, N., Nash, M., Ewer, A. K., and Toldi, G. (2019). Congenital methemoglobinemia identified by pulse oximetry screening. Pediatrics 143 (3), e20182814. doi:10.1542/peds.2018-2814
Warren, O. U., and Blackwood, B. (2019). Acquired methemoglobinemia. N. Engl. J. Med. 381 (12), 1158. doi:10.1056/NEJMicm1816026
Yu, G., Li, Y., Cui, S., Jian, T., Kan, B., and Jian, X. (2022). Two cases of methaemoglobinaemia and haemolysis due to poisoning after skin absorption of 4-chloro-1-nitrobenzene. Clin. Toxicol. (Phila) 60 (8), 970–973. doi:10.1080/15563650.2022.2062375
Yu, X., Zhang, Y., Yang, M., Guo, J., Xu, W., Gao, J., et al. (2016). Cytotoxic effects of tebufenozide in vitro bioassays. Ecotoxicol. Environ. Saf. 129, 180–188. doi:10.1016/j.ecoenv.2016.03.025
Zellner, T., Prasa, D., Färber, E., Hoffmann-Walbeck, P., Genser, D., and Eyer, F. (2019). The use of activated charcoal to treat intoxications. Dtsch. Arztebl Int. 116 (18), 311–317. doi:10.3238/arztebl.2019.0311
Keywords: methemoglobinemia, tebufenozide, indoxacarb, pesticide, poisoning
Citation: Wang J, Yu G, Jian T, Kan B, Li W and Jian X (2025) Case report: Pesticide-related methemoglobinemia: Tebufenozide and indoxacarb poisoning. Front. Toxicol. 7:1557990. doi: 10.3389/ftox.2025.1557990
Received: 09 January 2025; Accepted: 10 February 2025;
Published: 27 February 2025.
Edited by:
Marcelo Dutra Arbo, Federal University of Rio Grande do Sul, BrazilReviewed by:
Anas Mohammed Muthanikkatt, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), IndiaCopyright © 2025 Wang, Yu, Jian, Kan, Li and Jian. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiangdong Jian, amlhbnhpYW5nZG9uZ3ZpcEB2aXAuMTYzLmNvbQ== Wei Li, cGx1bXNob3dAMTYzLmNvbQ==
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.