 Josefa Domingos
Josefa Domingos John Dean3
John Dean3 Júlio Belo Fernandes
Júlio Belo Fernandes Catarina Godinho
Catarina Godinho
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Syst. Neurosci., 30 June 2022
Volume 16 - 2022 | https://doi.org/10.3389/fnsys.2022.916237
Physiotherapy and exercise are associated with motor and non-motor benefits in Parkinson’s disease (PD). Community exercise programs may increase ongoing exercise participation and help people with Parkinson’s disease actively participate in their health management. But there is still limited knowledge about these programs regarding their benefits, safety, implications over the long-term, and effective implementation. These questions could hold relevant clinical implications. In this perspective article, we identify the current challenges and reflect upon potential solutions to help community exercise to be implemented as an additional anchor to personalize management models for Parkinson’s disease.
Parkinson’s disease (PD) is characterized by complex motor and non-motor features, managed through pharmacological and non-pharmacological treatment options (Bloem et al., 2021). Non-pharmacological interventions such as physiotherapy, speech therapy, PD nurse specialist care, and occupational therapy help improve patients’ functioning and assist patients and their families to cope with disability (Clarke et al., 2006; Keus et al., 2014; Lennaerts et al., 2017; Radder et al., 2020). Physiotherapy is among the most studied non-pharmacological treatments and has shown benefits in improving motor impairments in transfers, posture, reaching and grasping, balance, freezing, falls, gait, and physical capacity. Exercise is often applied as part of physiotherapy interventions (Keus et al., 2014; Radder et al., 2020). There is growing evidence showing its effectiveness for several motor (Keus et al., 2014; van der Kolk et al., 2019; Radder et al., 2020) and non-motor problems (Cusso et al., 2016) but ongoing exercise is needed to maintain benefits (Keus et al., 2014).
People with PD can receive this care in a variety of ways and in a range of settings such as inpatient, outpatient, home-based care, and community care. Still, current healthcare delivery is often complex, fragmented, and imposes numerous barriers (e.g., limited expertise, poor communication, geographical distances, financial asymmetries, lack of time, and overburdened care partners; Schootemeijer et al., 2020). Depending upon the healthcare system, a patient may see their neurologist once or twice a year, for approximately 30 min each session. They may have an additional 15 h with their physiotherapist within that timeframe. But during the rest of the year, patients spend their time in self-care at home or in the community (Riggare and Hagglund, 2018; Figure 1). Noticeably, a study that followed 187 people with PD, showed that after 20 years of diagnosis, 47% were doing physiotherapy and 54% were doing some form of exercise in the community (Hassan et al., 2015). This illustrates well that, even in the later stages of the disease, people still significantly depend on local community resources.
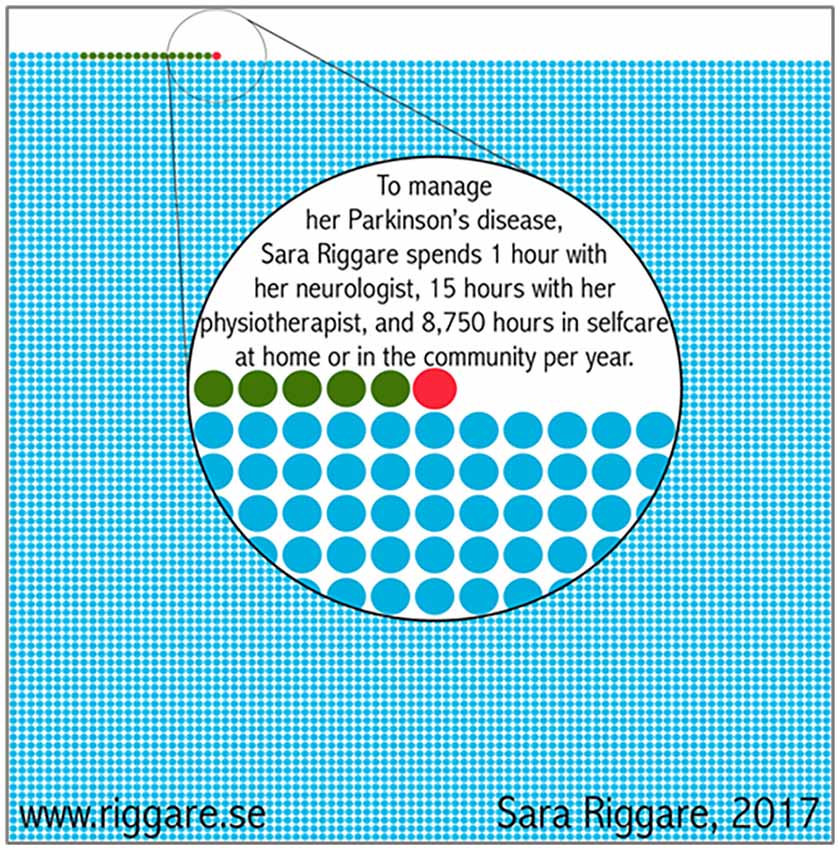
Figure 1. Patients’ perspective on common care from Sweden.
Offering exercise in the community to deliver accessible care close to patients’ homes can help overcome some of these barriers and may prove an attractive solution to enhance ongoing exercise. Yet, despite promising results, there is still limited data concerning the true benefits, including the implications of long-term or continuous use, as well as insufficient information regarding safety, delivery and implementation methods. Ultimately, should these programs be included in current care models per se, or should it be organized outside the care system, as an addition to formal care?
Therefore, in this viewpoint, we will reflect on key questions that may revolutionize PD care and fuel future research, including: Which community programs have been studied in PD? What are the benefits of these programs within current PD care models? What are the current drawbacks, limitations, and future needs to implement such community programs? Can technology be used to benefit access to these community programs? What initiatives/actions or possible solutions can be put in place to achieve more personalized community evidence-based care?
Community exercise programs commonly refer to the use of different exercises in a group format, delivered close to a person’s home, in community centers or local rehabilitation centers, and most frequently delivered by non-medical professionals. A wide range of Parkinson-specific community-based programs are already being used in PD. The most common ones outlined in recent literature include: dance (Kalyani et al., 2019), boxing (Combs et al., 2013; Domingos et al., 2019), Nordic walking (Granziera et al., 2021), Tai Chi (Liu et al., 2019), Qigong (Chen et al., 2020), and aquatic exercise (Perez-de la Cruz et al., 2016; Carroll et al., 2017; Kurt et al., 2018; Silva and Israel, 2019).
Dance is one of the most widely researched forms of exercise in PD and has been shown to have a beneficial effect on motor symptoms, balance, and gait (Dos Santos Delabary et al., 2018; Radder et al., 2020). It has also shown potential benefits on cognitive function, mood, and quality of life (Kalyani et al., 2019). Tai Chi and Qigong challenge primarily balance and are also recognized by international guidelines as intervention options to improve balance and gait impairments (Clarke et al., 2006; Keus et al., 2014). Tai Chi (Liu et al., 2019) and Qigong (Chen et al., 2020) compared with no exercise or sham treatment revealed a beneficial effect on motor symptoms, balance, and gait parameters. Nordic Walking (Granziera et al., 2021) when compared to no exercise or sham treatment, has also been shown to have a moderately large effect on motor symptoms and a large effect on balance (Berg Balance Scale) and gait (6-min walk test). Hydrotherapy interventions, in comparison with standard physiotherapy or no exercise, have shown a moderately large effect on the Timed Up and Go test and a moderately large effect was found for reducing the fear of falling (Radder et al., 2020). Boxing still has very limited evidence but is one of the most popular among people with PD (Domingos et al., 2019). In 2013 (Combs et al., 2013), the authors showed that boxing resulted in significant improvements in gait velocity and endurance over time, when compared to a conventional physiotherapy control group.
Community programs are spreading globally as a practical and cost-effective way to assist people with PD living in the community to actively participate in their health management. These community programs are a critical exercise resource for people with PD for several reasons.
First, they offer a means of ongoing care that may help preserve the patient’s physical and mental wellbeing by promoting an active lifestyle and by enhancing long-term exercise adherence. Physiotherapy and exercise interventions can improve physical functioning (Keus et al., 2014; Radder et al., 2020) but, as mentioned previously, continuous exercise is needed to maintain results. Compliance with such prolonged programs remains a critical challenge in PD (Keus et al., 2014; Schootemeijer et al., 2020). One possible solution to promote a sustained adherence to exercise is through continuous participation in these community exercise programs.
Second, people with PD have reported that they are more willing to participate in exercise programs that cost less and involve less travel (Ypinga et al., 2018). Given that community exercises are often close to participant’s home, these programs improve accessibility, and reduce transportation needs in people already dealing with increased mobility limitations, cognitive challenges, and reduced driving capacity and also reduce care partner burden.
Third, if these programs are appropriately designed and delivered, they can have a powerful impact on clinical outcomes and improve patient overall satisfaction with healthcare (Ypinga et al., 2018). For example, community programs such as dance or Tai Chi have been shown to potentially reduce fall risk factors such as balance, gait, and cognition (Kalyani et al., 2019). As a result, their usefulness to society increases tremendously given the physical and mental impact they may have on preventing falls.
Fourth, health care systems benefit from cost savings achieved from community care. Policy makers throughout the world are keen to implement and spread low-cost models to improve the quality of care (Bloem et al., 2017). Ultimately, favoring the use of community exercise programs with improved quality and safety can complement current healthcare options in a more beneficial manner but also help to ascertain an affordable healthcare.
We identify several challenges that can slow the implementation of quality care at four different levels: research, instructor, organizational, and patient.
At the research level, the extent to which general exercise programs in the community can be translated into sustainable, adequate, and safe exercise programs specific to PD is still unclear. There is limited evidence on the optimal design, delivery, and implementation of PD-specific exercise programs that are easily accessible and generalizable to a large proportion of people with PD. Having more funding opportunities for studying non-pharmacological interventions is critical to generate further research, properly designed, sufficiently powered, and with proper regard for safety issues. Several questions should fuel this future research, including: Which type of exercises do people with PD prefer (and why)? Exactly what types of benefits do different exercises provide to specific phenotypes or stages of PD? What is the potential impact of demographics and subpopulation characteristics such as age, gender. and educational level, and disease-specific disabilities on the preference for this type of programs? Do program and participant characteristics influence people’s willingness to participate in these exercise programs? Given the overall financial costs, safety issues, and progressive nature of PD, which professionals should develop and who should deliver these community programs? Is there a need for added expertise, training, or clinical education for those applying for these programs in order to guarantee safety issues? With mobility difficulties and encroaching disability, how can technology support access to online community expert care? Should we wait for more robust evidence to implement these programs?
Importantly, although several studies have been conducted on the feasibility of some programs (Combs et al., 2013), there is virtually no satisfactory evidence to guide the implementation of specific evidence-based practices with clarity. Recommendations on how to adapt research exercise protocols into applicable to a “real-world” community setting, integrating the complexity of context and people participating, are urgently needed to inform future implementation efforts. Considerations need to be made for differences among certain disease severities, PD phenotype subpopulations, individuals who have cognitive impairment and practice setting (for example, rural as opposed to urban settings). People with PD are typically motivated to take part in research studies but following participation in an exercise intervention study, there is a general decline in activity levels. Research has shown that in order to maintain ongoing activity and keep physically active beyond the research setting, people with PD want evidence supporting the benefits of exercise as well as greater availability of programs closer to home, and guidance from health care providers toward exercise studies (Valadas et al., 2011). People with PD also considered that these exercise programs should consist of activities that are enjoyable, safe, and adaptable to the abilities of the individual, as well as include social engagement and social support (Zaman et al., 2021).
There is a clear need to enhance expertise among professionals delivering exercise programs to people with PD. International Physiotherapy guidelines advise patients to participate in the ongoing unsupervised exercise in their communities while also recommending people with PD to access expert care (Keus et al., 2014). Notably, there is an optimal minimal level of disease-specific expertise necessary, particularly with respect to the safe integration of exercises and reducing the risk of falls and other possibly dangerous issues (Keus et al., 2014). For example, being aware that cardiorespiratory regulation during exercise can be altered in people with PD when compared to age-matched controls (Sabino-Carvalho et al., 2018; Sabino-Carvalho and Vianna, 2020). The autonomic dysfunction can lead to inadequate hemodynamic responses, the failure to match the metabolic demands of working skeletal muscle, and exercise intolerance (Sabino-Carvalho et al., 2021). Better knowledge and understanding of these responses during exercise in this population is critical to guarantee safety during exercise. This means there is a need to be able to refer patients to a supportive and safe exercise environment that is preferably led by professionals with relevant Parkinson-specific training. By referring people with PD to attend exercise programs without expertise, health professionals could ultimately put the person’s safety at risk (Nijkrake et al., 2009; Keus et al., 2014). Importantly, people with PD have perceived the lack of PD expertise in community care programs as a primary area of weakness. Many individuals with PD express a strong interest in accessing this type of expertise within their community (Hirsch, 2009). Experience of working with the PD population is a significant source of expertise in and of itself; Nijkrake and colleagues have noted that physiotherapists with an annual treatment volume of at least seven people with PD report higher self-perceived expertise (Nijkrake et al., 2009; Ypinga et al., 2018). Presumably, this level of contact will not be difficult for many community exercise programs to achieve. Nonetheless, an effective educational component will be needed to complement this experiential expertise and bridge any gaps along the continuum of care. It is incumbent upon community exercise instructors to recognize limitations in their knowledge base, improve their ability to instruct and modify exercise approaches appropriately to maximize benefits, and to closely review their clinical needs in conjunction with their personal preferences in order to produce long-term benefits (Hirsch, 2009). Also, the instructors’ skills to identify good evidence from flawed evidence is essential given the current proliferation of scientific articles on exercise and PD. The provision of high-quality care is best achieved through evidence-based practice (Emparanza et al., 2015; NICE, 2015; Dean et al., 2021) and instructors should too practice in an evidence-informed manner. In addition, these instructors should seek additional guidance from other professionals when needed (Keus et al., 2014). Specific training, adequate ongoing educational support, and continuous contact with people with PD will be needed to practice in a manner that is supported by the emerging evidence (Nijkrake et al., 2009).
Additionally, to enhance accessibility to expertise, the use of technology specifically designed for use by people with PD may have an enormous role. Providing a co-approach combining technology and local in-person care community-based programs, which could be easily implemented in senior centers, is an intuitive example of how the use of technology can allow for access to expertise worldwide and ultimately may shape the near future. It would allow for more patients with PD to take part in such programs and also access PD expert care. Because technology raises concerns regarding usability and compliance in the more elderly population, having community centers organize spaces with technology and human support could significantly improve its successful implementation. The presence of a person for technical support represents a unique ability to provide a safe, facilitated, and remote intervention.
At the organizational level, among others, there is a lack of clear strategies to facilitate the quick dissemination of novel evidence-based practices into an ever-increasing number of unmonitored community programs. Clear leadership at the organizational level would help maintain patients’ trust in clinical practice and long-term adherence. An organized infrastructure could provide support to exercise instructors and other implementers to introduce updated practices and embrace additional changes whenever new evidence emerges. Additionally, raising awareness about these programs increases the public interest in these exercise programs, which will in turn influence the course of clinical research and consequently develop clinical practice. In this regard, patients’ associations could be excellent advocates, both informing and stimulating patients and their families.
To facilitate people with PD access to such programs society needs to build solutions for critical barriers impacting participation, including financial, traveling, physical and cultural barriers (Schootemeijer et al., 2020; Domingos et al., 2022). Evidence-based practices should be covered as a health insurance benefit. Health systems can implement new care models that shift funding using a mix of nonprofit and volunteer-run initiatives or integrated as part of the healthcare systems. Community initiatives (e.g., developing the concept of an exercise bus; creating safe places for exercise and walking paths that are accessible for parking) to support transportation can be put in place to reduce challenges in access. Technology is another way to facilitate access to specialized care and favor long adherence (Speelman et al., 2014). Several reports have shown the benefits of telemonitoring and telerehabilitation as a means to provide specialized care to patients who have difficulty accessing it, particularly during the coronavirus disease 2019 (COVID-19) pandemic (Helmich and Bloem, 2020; Domingos et al., 2022). Future studies may look to the potential value of applying technology to facilitate patient access to telemonitoring and specialized community-based programs in their homes (Speelman et al., 2014) or in community centers with remote trainers (Achey et al., 2014). Importantly, online programs should always include teaching courses on how to use technology to bypass limitations in its use by elderly populations.
At the patient level, we will need to find solutions to bypass the several factors that may interfere with the ability of patients to participate, such as: fluctuations (motor symptoms or other) from day to day, concerns about becoming injured or falling, lacking sufficient time to exercise regularly, and perceive social stigma when exercising in public (Schootemeijer et al., 2020).
We also need to improve the awareness of people with PD with regard to evidence-based exercise programs and where such programs can be received. Society counts on the active participation of informed people with PD to make the right decisions for their health, capable of working as partners with all professionals (medical and non-medical) to optimize results (van der Kolk et al., 2019; Domingos et al., 2022). Yet, given the recent proliferation of exercise programs (with or without evidence), people with PD are faced with the challenge of how to choose. Making sense of these programs may also be complicated by the tendency among popular media to promote research results without consideration of the quality of the study design or the expertise of the research team. As a result, certain media sources might highlight a new exercise approach or other intervention that is unproven, and which may go on to run the risk of failing to produce the desired outcomes. For people with PD, this may result in disappointment and blunting of enthusiasm for participation in other interventions that could be more beneficial or more directly applicable to their specific deficits. In addition, financial resources utilized in the pursuit of less effective or possibly unhelpful exercise approaches will not be available for approaches with a proven track record of benefit.
Due to the complexity of these many factors, people with PD should count on health professionals and clinicians to advise them on trustworthy sources of information and options on care. Some guidance can also be achieved through awareness campaigns, research-based guidance programs (Domingos et al., 2021), or patient helplines. When providing care, health or other non-health professionals should use safe evidence-based practices. Such programs must be made available and accessible to people with PD all-inclusive to promote better care for people with PD, improve wellbeing, and ultimately reduce costs to health care systems. Additionally, care should be provided by professionals with PD expertise for better outcomes, reducing the use of unnecessary procedures and unrealistic expectations in people with PD, particularly for those with less favorable profiles for certain exercises.
We might be limited to understand the many heterogeneous factors that can interplay, several courses of action may already be possible to address the gap between expertise, evidence, dissemination, and implementation into community exercise practices. We summarize these potential actions discussed above in Table 1.
Table 1. Summary of potential courses of action needed to improve quality community care.
Community exercise programs are growing in popularity and in research interest. These new initiatives increase optimism about the possibility of developing programs that are cost-effective, easily accessible and a means of providing structured, ongoing exercise programs for people with PD. Some changes in thinking by the healthcare community are needed to delineate how community services can better complement current clinical care and to prepare for their integration. These changes require shifting views, changing behaviors, incentives, and capacities to support this change, and developing novel models that allow these two areas to interact and coordinate effectively.
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
JDo: conceptualization, writing—original draft preparation. JDe: writing—original draft preparation, writing—review and editing. JF: writing—review and editing, supervision. JM: writing—review and editing. CG: conceptualization, writing—review and editing, supervision. All authors contributed to the article and approved the submitted version.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. This publication is financed by national funds through the FCT-Foundation for Science and Technology, I.P., under the project UIDB/04585/2020.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to thank the Centro de InvestigaçãoInterdisciplinarEgas Moniz (CiiEM) for the support provided for the publication of this article.
Achey, M., Aldred, J. L., Aljehani, N., Bloem, B. R., Biglan, K. M., Chan, P., et al. (2014). The past, present and future of telemedicine for Parkinson’s disease. Mov. Disord. 29, 871–883. doi: 10.1002/mds.25903
Bloem, B. R., Okun, M. S., and Klein, C. (2021). Parkinson’s disease. Lancet 397, 2284–2303. doi: 10.1016/S0140-6736(21)00218-X
Bloem, B. R., Rompen, L., Vries, N. M., Klink, A., Munneke, M., and Jeurissen, P. (2017). ParkinsonNet: a low-cost health care innovation with a systems approach from the Netherlands. Health Aff. (Millwood) 36, 1987–1996. doi: 10.1377/hlthaff.2017.0832
Carroll, L. M., Volpe, D., Morris, M. E., Saunders, J., and Clifford, A. M. (2017). Aquatic exercise therapy for people with parkinson disease: a randomized controlled trial. Arch. Phys. Med. Rehabil. 98, 631–638. doi: 10.1016/j.apmr.2016.12.006
Chen, S., Zhang, Y., Wang, Y. T., Liu, X., Song, W., and Du, X. (2020). The effect of Qigong-based therapy on patients with Parkinson’s disease: a systematic review and meta-analysis. Clin. Rehabil. 34, 1436–1448. doi: 10.1177/0269215520946695
Clarke, C., Sullivan, T., and Mason, A. (2006). National Clinical Guideline For Diagnosis And Management In Primary And Secondary Care. London: Royal College of Physicians.
Combs, S. A., Diehl, M. D., Chrzastowski, C., Didrick, N., McCoin, B., Mox, N., et al. (2013). Community-based group exercise for persons with Parkinson disease: a randomized controlled trial. NeuroRehabilitation 32, 117–124. doi: 10.3233/NRE-130828
Cusso, M. E., Donald, K. J., and Khoo, T. K. (2016). The impact of physical activity on non-motor symptoms in Parkinson’s disease: a systematic review. Front. Med. (Lausanne) 3:35. doi: 10.3389/fmed.2016.00035
Dean, J., Gallagher-Ford, L., and Connor, L. (2021). Evidence-based practice: a new dissemination guide. Worldviews Evid. Based Nurs. 18, 4–7. doi: 10.1111/wvn.12489
Domingos, J., Dean, J., Cruickshank, T. M., Smilowska, K., Fernandes, J. B., and Godinho, C. (2021). A novel boot camp program to help guide personalized exercise in people with Parkinson disease. J. Pers. Med. 11:938. doi: 10.3390/jpm11090938
Domingos, J., Familia, C., Fernandes, J. B., Dean, J., and Godinho, C. (2022). Is being physically active enough or do people with Parkinson’s disease need structured supervised exercise? Lessons learned from COVID-19. Int. J. Environ. Res. Public Health 19:2396. doi: 10.3390/ijerph19042396
Domingos, J., Radder, D., Riggare, S., Godinho, C., Dean, J., Graziano, M., et al. (2019). Implementation of a community-based exercise program for Parkinson patients: using boxing as an example. J. Parkinsons Dis. 9, 615–623. doi: 10.3233/JPD-191616
Dos Santos Delabary, M., Komeroski, I. G., Monteiro, E. P., Costa, R. R., and Haas, A. N. (2018). Effects of dance practice on functional mobility, motor symptoms and quality of life in people with Parkinson’s disease: a systematic review with meta-analysis. Aging Clin. Exp. Res. 30, 727–735. doi: 10.1007/s40520-017-0836-2
Emparanza, J. I., Cabello, J. B., and Burls, A. J. (2015). Does evidence-based practice improve patient outcomes? An analysis of a natural experiment in a Spanish hospital. J. Eval. Clin. Pract. 21, 1059–1065. doi: 10.1111/jep.12460
Granziera, S., Alessandri, A., Lazzaro, A., Zara, D., and Scarpa, A. (2021). Nordic walking and walking in Parkinson’s disease: a randomized single-blind controlled trial. Aging Clin. Exp. Res. 33, 965–971. doi: 10.1007/s40520-020-01617-w
Hassan, A., Wu, S. S., Schmidt, P., Simuni, T., Giladi, N., Miyasaki, J. M., et al. (2015). The profile of long-term Parkinson’s disease survivors with 20 years of disease duration and beyond. J. Parkinsons Dis. 5, 313–319. doi: 10.3233/JPD-140515
Helmich, R. C., and Bloem, B. R. (2020). The impact of the COVID-19 pandemic on Parkinson’s disease: hidden sorrows and emerging opportunities. J. Parkinsons Dis. 10, 351–354. doi: 10.3233/JPD-202038
Hirsch, M. A. (2009). Community-based rehabilitation for Parkinson’s disease: from neurons to neighborhoods. Parkinsonism Relat. Disord. 15, S114–117. doi: 10.1016/S1353-8020(09)70795-3
Kalyani, H. H. N., Sullivan, K. A., Moyle, G., Brauer, S., Jeffrey, E. R., and Kerr, G. K. (2019). Impacts of dance on cognition, psychological symptoms and quality of life in Parkinson’s disease. NeuroRehabilitation 45, 273–283. doi: 10.3233/NRE-192788
Keus, S., Munneke, M., Graziano, M., Paltamaa, J., Pelosin, E., Domingos, J., et al. (2014). European Physiotherapy Guideline for Parkinson’s Disease. The Netherlands: KNGF/ParkinsonNet.
Kurt, E. E., Buyukturan, B., Buyukturan, O., Erdem, H. R., and Tuncay, F. (2018). Effects of Ai Chi on balance, quality of life, functional mobility and motor impairment in patients with Parkinson’s disease. Disabil. Rehabil. 40, 791–797. doi: 10.1080/09638288.2016.1276972
Lennaerts, H., Groot, M., Rood, B., Gilissen, K., Tulp, H., van Wensen, E., et al. (2017). A guideline for Parkinson’s disease nurse specialists, with recommendations for clinical practice. J. Parkinsons Dis. 7, 749–754. doi: 10.3233/JPD-171195
Liu, H. H., Yeh, N. C., Wu, Y. F., Yang, Y. R., Wang, R. Y., and Cheng, F. Y. (2019). Effects of tai chi exercise on reducing falls and improving balance performance in Parkinson’s disease: a meta-analysis. Parkinsons Dis. 2019:9626934. doi: 10.1155/2019/9626934
NICE, National Institute for Health and Care Excellence. (2015). Practical steps to improving the quality of care and services using NICE guidance Available online at: https://intopractice.nice.org.uk/practical-steps-improving-quality-of-care-services-using-nice-guidance/index.html. Accessed May, 2022.
Nijkrake, M. J., Keus, S. H., Oostendorp, R. A., Overeem, S., Mulleners, W., Bloem, B. R., et al. (2009). Allied health care in Parkinson’s disease: referral, consultation and professional expertise. Mov. Disord. 24, 282–286. doi: 10.1002/mds.22377
Perez-de la Cruz, S., Garcia Luengo, A. V., and Lambeck, J. (2016). Effects of an Ai Chi fall prevention programme for patients with Parkinson’s disease. Neurologia 31, 176–182. doi: 10.1016/j.nrl.2015.05.009
Radder, D. L. M., Ligia Silva de Lima, A., Domingos, J., Keus, S. H. J., van Nimwegen, M., Bloem, B. R., et al. (2020). Physiotherapy in Parkinson’s disease: a meta-analysis of present treatment modalities. Neurorehabil. Neural Repair 34, 871–880. doi: 10.1177/1545968320952799
Riggare, S., and Hagglund, M. (2018). Precision medicine in Parkinson’s disease - exploring patient-initiated self-tracking. J. Parkinsons Dis. 8, 441–446. doi: 10.3233/JPD-181314
Sabino-Carvalho, J. L., Fisher, J. P., and Vianna, L. C. (2021). Autonomic function in patients with Parkinson’s disease: from rest to exercise. Front. Physiol. 12:626640. doi: 10.3389/fphys.2021.626640
Sabino-Carvalho, J. L., Teixeira, A. L., Samora, M., Daher, M., and Vianna, L. C. (2018). Blunted cardiovascular responses to exercise in Parkinson’s disease patients: role of the muscle metaboreflex. J. Neurophysiol. 120, 1516–1524. doi: 10.1152/jn.00308.2018
Sabino-Carvalho, J. L., and Vianna, L. C. (2020). Altered cardiorespiratory regulation during exercise in patients with Parkinson’s disease: a challenging non-motor feature. SAGE Open Med. 8:2050312120921603. doi: 10.1177/2050312120921603
Schootemeijer, S., van der Kolk, N. M., Ellis, T., Mirelman, A., Nieuwboer, A., Nieuwhof, F., et al. (2020). Barriers and motivators to engage in exercise for persons with Parkinson’s disease. J. Parkinsons Dis. 10, 1293–1299. doi: 10.3233/JPD-202247
Silva, A. Z. D., and Israel, V. L. (2019). Effects of dual-task aquatic exercises on functional mobility, balance and gait of individuals with Parkinson’s disease: a randomized clinical trial with a 3-month follow-up. Complement. Ther. Med. 42, 119–124. doi: 10.1016/j.ctim.2018.10.023
Speelman, A. D., van Nimwegen, M., Bloem, B. R., and Munneke, M. (2014). Evaluation of implementation of the ParkFit program: a multifaceted intervention aimed to promote physical activity in patients with Parkinson’s disease. Physiotherapy 100, 134–141. doi: 10.1016/j.physio.2013.05.003
Valadas, A., Coelho, M., Mestre, T., Guedes, L. C., Finisterra, M., Noronha, A., et al. (2011). What motivates Parkinson’s disease patients to enter clinical trials? Parkinsonism Relat. Disord. 17, 667–671. doi: 10.1016/j.parkreldis.2011.05.023
van der Kolk, N. M., de Vries, N. M., Kessels, R. P. C., Joosten, H., Zwinderman, A. H., Post, B., et al. (2019). Effectiveness of home-based and remotely supervised aerobic exercise in Parkinson’s disease: a double-blind, randomised controlled trial. Lancet Neurol. 18, 998–1008. doi: 10.1016/S1474-4422(19)30285-6
Ypinga, J. H. L., de Vries, N. M., Boonen, L., Koolman, X., Munneke, M., Zwinderman, A. H., et al. (2018). Effectiveness and costs of specialised physiotherapy given via ParkinsonNet: a retrospective analysis of medical claims data. Lancet Neurol. 17, 153–161. doi: 10.1016/S1474-4422(17)30406-4
Keywords: Parkinson’s disease, community exercise programs, physiotherapy, exercise, dance, boxing, nordic walking, tai chi
Citation: Domingos J, Dean J, Fernandes JB, Massano J and Godinho C (2022) Community Exercise: A New Tool for Personalized Parkinson’s Care or Just an Addition to Formal Care? Front. Syst. Neurosci. 16:916237. doi: 10.3389/fnsys.2022.916237
Received: 08 April 2022; Accepted: 30 May 2022;
Published: 30 June 2022.
Edited by:
Oscar Arias-Carrion, Hospital General Dr. Manuel Gea Gonzalez, MexicoReviewed by:
Jeann Lúccas Sabino-Carvalho, University of Brasilia, BrazilCopyright © 2022 Domingos, Dean, Fernandes, Massano and Godinho. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Josefa Domingos, ZG9taW5nb3Nqb3NlZmFAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.