 Anneli Wall
Anneli Wall Jörgen Borg1,2
Jörgen Borg1,2
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Syst. Neurosci., 25 March 2015
Volume 9 - 2015 | https://doi.org/10.3389/fnsys.2015.00048
This article is part of the Research TopicAugmentation of Brain Function: Facts, Fiction and ControversyView all 150 articles
Objective: The aim of this study was to review the literature on clinical applications of the Hybrid Assistive Limb system for gait training.
Methods: A systematic literature search was conducted using Web of Science, PubMed, CINAHL and clinicaltrials.gov and additional search was made using reference lists in identified reports. Abstracts were screened, relevant articles were reviewed and subject to quality assessment.
Results: Out of 37 studies, 7 studies fulfilled inclusion criteria. Six studies were single group studies and 1 was an explorative randomized controlled trial. In total, these studies involved 140 participants of whom 118 completed the interventions and 107 used HAL for gait training. Five studies concerned gait training after stroke, 1 after spinal cord injury (SCI) and 1 study after stroke, SCI or other diseases affecting walking ability. Minor and transient side effects occurred but no serious adverse events were reported in the studies. Beneficial effects on gait function variables and independence in walking were observed.
Conclusions: The accumulated findings demonstrate that the HAL system is feasible when used for gait training of patients with lower extremity paresis in a professional setting. Beneficial effects on gait function and independence in walking were observed but data do not allow conclusions. Further controlled studies are recommended.
Normal gait depends on the functional integrity and interactions in sensory-motor neural networks at spinal and supraspinal levels (Bowden et al., 2013). This complex system may be disturbed in many neurological conditions such as stroke or spinal cord injury (SCI) resulting in limited mobility and impaired gait function, which are major challenges in neuro rehabilitation. Intensive, repetitive task specific training may drive beneficial neuroplasticity, enhance functional restitution and improve final outcome (Kwakkel et al., 2004; Langhorne et al., 2009, 2011; Peurala et al., 2014). However, there is a need for further development of training methods in response to an increasing understanding of the individual capacity for regaining functioning (Krakauer et al., 2012; Bowden et al., 2013).
Approaches to improve gait function after stroke and SCI include treadmill training with or without use of partial body weight support (BWS), yet the evidence to support this is inconclusive (Schwartz and Meiner, 2013; Dobkin et al., 2014). Gait machines (GM) may allow more reproducible gait movements compared to conventional training and reduce the burden on the therapist. GM work according to the end-effector principle (foot plates move the feet in a controlled gait pattern) or as exoskeletons, which have joints matching the limb joints and motors that drive movements over these joints to assist, e.g., leg movements (Hesse et al., 2010). A recent Cochrane review concluded that electromechanically assisted gait training in combination with physiotherapy after stroke increases the odds of achieving independent walking and most so when applied for severely impaired patients in the first 3 months after stroke (Mehrholz et al., 2013) but less clear after SCI (Mehrholz et al., 2012).
The importance of incorporating more active participation than allowed by gait machines to enhance training effects and the need for new concepts and devices are recognized (Dobkin, 2009; Pennycott et al., 2012). One new approach is represented by the Hybrid Assistive Limb system (HAL). HAL is an exoskeleton with a hybrid system allowing both a voluntary and an autonomous mode of action to support training of gait. HAL comprises a control algorithm and supporting devices, where each knee and hip joint can be controlled separately. Key features of the HAL system have been reported in detail (Kawamoto, 2002; Suzuki et al., 2007; Kawamoto et al., 2010). Movements are triggered by use of either the “Cybernic Voluntary Control” (CVC), which is based on the users voluntary activation of gait muscles as recorded by surface electromyography (EMG), or by the “Cybernic Autonomous Control” (CAC), which is based on the users weight shifting and input from force pressure sensors in the shoes. The CVC mode allows the operator to adjust the degree of support for each joint and reduce the support as training progress and to adjust settings to achieve a gait pattern that is as close as possible to normal gait. In case of complete loss of voluntary activation of gait muscles the CAC mode may be used. Gait is then initiated and sustained by input from force-pressure sensors in the shoes. HAL is manufactured in single-leg and double-leg versions and training with HAL may be performed with or without BWS.
A number of clinical studies with HAL have been conducted and there is a need for an evaluation of available data to guide further trials. The aim of this report was to provide a systematic review in order to evaluate current evidence with regard to feasibility (i.e., usability and safety) and effects and to make recommendations for further studies.
A systematic search of the literature was conducted using the databases Web of Science, PubMed, and CINAHL. Both MeSH (Medical Subject Headings for Medline) terms and free text relevant for the subject were used and detected synonyms were added to the search. Search terms were (MeSH terms in bold): ((((robot OR robots OR robotic OR robotics OR robot-assisted OR exoskeleton OR machine-assisted OR electro-mechanic OR DGO OR “driven gait orthosis”))) AND (gait OR gaits OR walking OR walk OR walks OR locomotion OR “motor activity”)) AND (HAL OR “hybrid assistive limb” OR “wearable robot”). Search limitations were “Humans” and “English,” while publication date was unlimited. Using the same search terms, a search was also performed at clinicaltrials.gov, in order to identify ongoing studies and/or unpublished papers (Clinicaltrials, online). Abstracts identified were screened and studies were considered relevant if they addressed any clinical application of the HAL system regardless of study design. If needed the full text article was retrieved and assessed. Relevant studies were exported to EndNote where duplicates were identified and removed. Reference lists of these studies were manually searched for further articles. Studies were included if they were primary research articles, concerned gait training with the Hybrid Assistive Limb. Studies only reporting technology data, including only healthy subjects, single subjects or reviews were excluded. Thirty-seven articles were identified, 20 were retrieved in full text for assessment of eligibility and 13 of these did not fulfill inclusion criteria (see Figure 1). Overall 7 studies met the inclusion criteria and were subject to data extraction and analyses (Maeshima et al., 2011; Kawamoto et al., 2013; Kubota et al., 2013; Ueba et al., 2013; Aach et al., 2014; Nilsson et al., 2014; Watanabe et al., 2014). Included studies were subject to critical review by two independent reviewers.
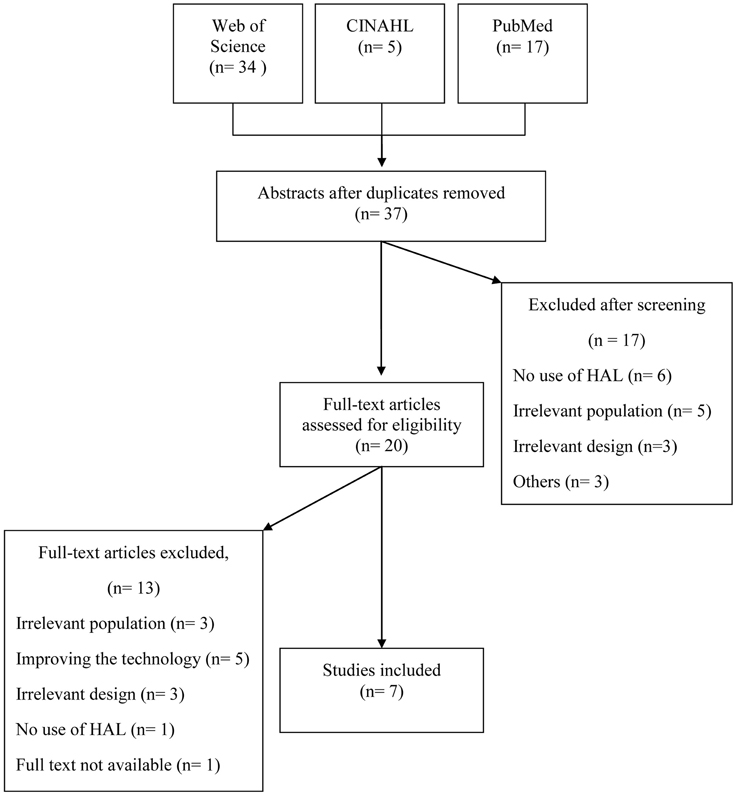
Figure 1. Presentation of the results of the systematic search of the literature.
The quality of the included studies, regarding risk of confounding and bias, was evaluated in accordance with the Scottish Intercollegiate Guidelines Network (SIGN) criteria (SIGN, online1). According to SIGN the methodological quality can be coded (++) meaning all or most of criteria fulfilled, (+) some of the criteria fulfilled or (−) few or no criteria fulfilled. The evaluation was performed independently by two investigators and in case of disagreement, a third reviewer was consulted. Since two investigators are authors of one of the included studies (Nilsson et al., 2014) this study was assessed by a fourth investigator.
Data extraction was performed by one investigator and checked by the two additional investigators. The extracted data comprised; characteristics of participants, intervention protocols and settings, outcome measures and effects and feasibility.
The 7 studies included 8–38 participants each, 6 were single group studies and 1 was a randomized controlled trial (RCT). In total, the studies involved 140 participants of whom 118 completed the intervention protocols and 107 used HAL for gait training. Extracted study data and results of the quality evaluation are presented in the Table 1. All included studies were found to have a high risk of bias and confounding according to the SIGN criteria and do not provide data for a meta-analysis.
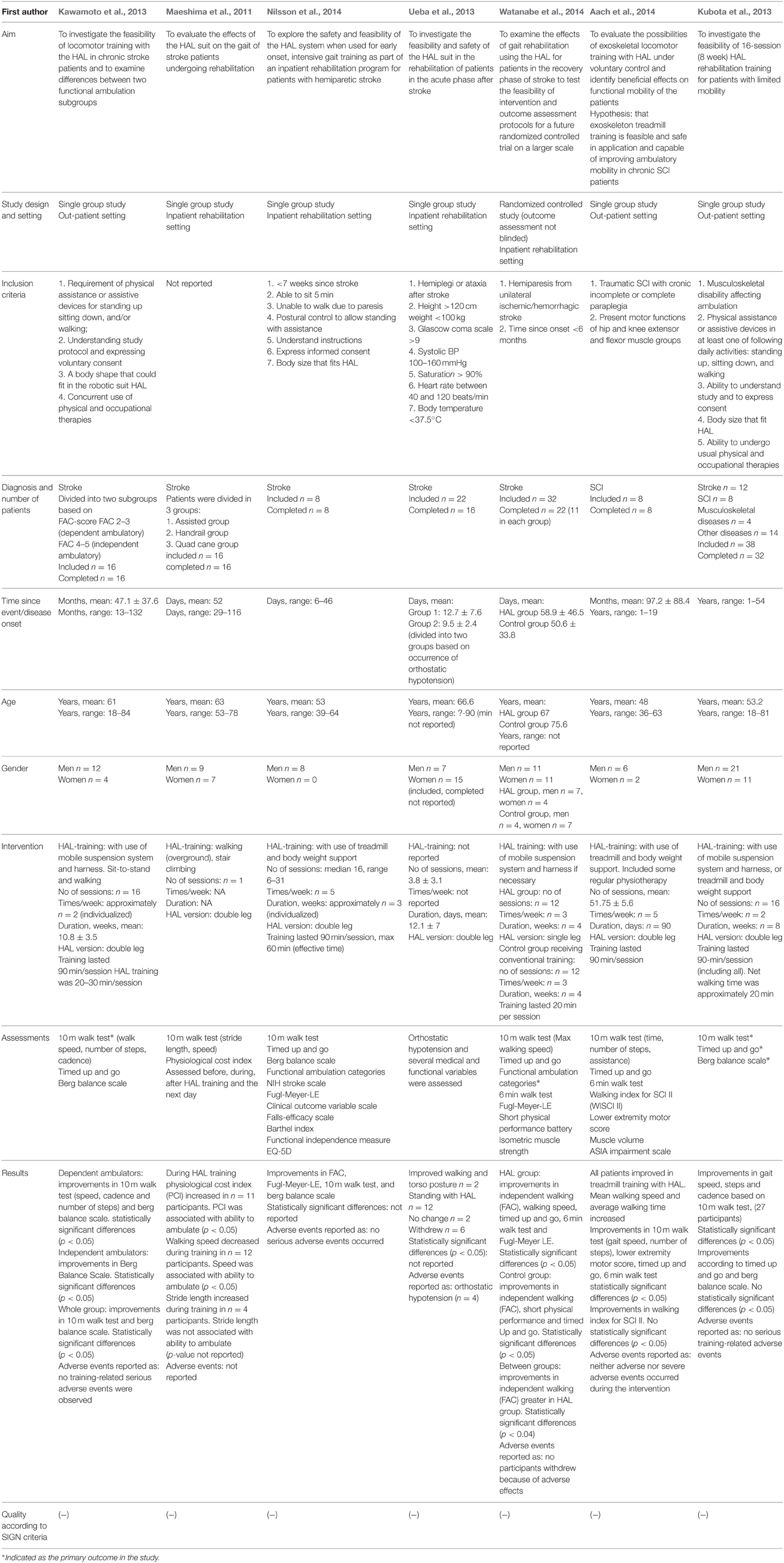
Table 1. Extracted study data.
The most frequent diagnosis reported was stroke (n = 106) followed by complete or incomplete SCI (n = 16) and other disorders (n = 18). Five of the studies included solely persons with stroke, 1 study included solely persons with SCI (Aach et al., 2014) and 1 study included persons with stroke (n = 12) and SCI (n = 8) as well as other disorders (n = 18) (Kubota et al., 2013). Mean age of the participants ranged from 48 to 67 years with a total range of 18–90 years.
In 6 of the included studies a total of 65.7% (n = 67) of the participants who completed the study intervention were men and 34.3% (n = 35) were women. Ueba et al. (2013) did not report gender for participants completing the study but among the included 32% (n = 7) were men and 68% (n = 15) were women.
The total time from disease onset to inclusion ranged from 6 days to 54 years. For persons with SCI the time from injury ranged from 1 to 19 years and for persons with stroke this time ranged from approximately 6 days to 16 years. Three studies (Maeshima et al., 2011; Nilsson et al., 2014; Watanabe et al., 2014) included persons early after stroke, with a mean range of 31–59 days since stroke onset. Two other studies included persons later than 1 year and up to 16 years after stroke onset (Kawamoto et al., 2013; Kubota et al., 2013).
The number of reported dropouts during the study interventions ranged from 6 to 10 and was 22, in total (18 with stroke, 1 with SCI and 3 participants with other diagnosis,). Reported reasons for dropouts were medical (n = 5), technical (n = 1), discharge (n = 2), personal (n = 4) and withdrawal of consent (n = 4). Another 6 participants dropped out due to inappropriate size of shoes, lumbar spondylosis which prevented correct fitting and/or depressive status.
All except 1 (Ueba et al., 2013) of the 7 studies specifically addressed gait training. The HAL training protocols showed a great variation with regard to frequency, intensity and number of sessions performed. Most studies applied HAL training ≥2 times per week during ≥4 weeks with durations of ≥20 min per session. In the studies involving persons with stroke, the total number of sessions per participant training with HAL ranged from 1 (Maeshima et al., 2011) to 31 (Nilsson et al., 2014). In studies involving persons with SCI, Aach et al. (2014) used a mean of 51.75 sessions while the number of sessions for persons with SCI in the study by Kubota et al. (2013) was 16. Data on the use of the active CVC mode and the autonomous CAC mode was not consistently reported. Based on the information provided, we anticipate that 6 of the studies used the CVC mode during training but the extent is not clear. One study (Ueba et al., 2013) did not report on modes used. Four studies reported the total length of each training sessions to be approximately 90 min including assessments, donning, doffing and effective walking time. The effective training time in these studies was approximately 20–30 min per session. Training with HAL was performed by use of BWS and/or a mobile suspension system in 5 studies, by over ground training in 1 study and was not defined in 1 study. Four studies were conducted in inpatient rehabilitation settings and 3 in out-patient care (see Table 1).
All assessments were performed without wearing HAL except for one study (Maeshima et al., 2011) where measurements were performed both with and without HAL. Outcome measures mainly related to walking ability. Most frequently used were the 10 m walking test (n = 6) (Wade et al., 1987), Timed up and Go (n = 5) (Podsiadlo and Richardson, 1991), and Berg Balance Scale (n = 3) (Berg et al., 1992). Assessments performed at baseline and after the training period were reported in all studies except 1 (Ueba et al., 2013). No study reported on a long-term follow up. The explorative RCT (Watanabe et al., 2014) compared the effect of HAL-training to the effect of conventional training in the subacute phase after stroke and included 11 participants in each group. The study shows a significant differences (p = 0.04) according to the Functional Ambulation Categories (FAC) (Holden et al., 1984) between groups, in favor for the HAL training group. This study has several limitations with regard to study sample size, varying time after stroke and lack of blinding of outcome assessments, as recognized by the authors. One other study (Nilsson et al., 2014) also used FAC and observed improvements suggesting a beneficial effect in a single group. Other studies also report on varying effects such as improvements in walking- and torso posture, gait speed, number of steps and cadence, functional ambulation/independent walking, motor function in lower extremity, activity performance and/or balance (see Table 1).
All studies except 1 (Maeshima et al., 2011) explicitly reported on adverse events. Except for transient complaints related to pressure of the suit, irritated skin, training related pain etc., no adverse events during training with HAL were reported.
The aim of this review was to explore existing evidence regarding gait training with the exoskeleton HAL (Hybrid Assistive Limb). We included 7 studies, each with small study samples but comprising a total of 140 patients. Of these, 118 completed the intervention and 107 used HAL. Studies differed in terms of aim, design, duration of intervention, patients/diagnosis, setting and participant characteristics as well as allocation, randomization, blinding and outcome measures. Only 1 study compared training with HAL with other training (Watanabe et al., 2014) but outcome assessment in that study was not blinded. Although no study provides conclusive data on the effects of gait training with HAL as compared to other training and the risk of confounding and bias was considered high, the experiences of training with HAL and the responses that were observed will be useful in the design of further studies.
In total, adult subjects within a broad age range (18–90 years) participated. Both genders were represented, however two thirds were men. Since the majority of subjects had a stroke diagnosis and gender proportions are fairly similar in this diagnostic group, the uneven distribution is surprising but only scarcely commented on in the studies.
Study participants in both post-acute and long-term after stroke onset were represented and 88 out of 106 included subjects completed the study interventions. One small experimental study included subjects with paraplegia 1–19 years after spinal cord injury where all completed the intervention (Aach et al., 2014) while no study addressed effects of training with HAL in the post-acute phase after SCI. The severity of paresis and gait problems varied both within and between the included studies, from severe (only able to maintain sitting balance) to moderate (independent walkers) and a corresponding use of HAL mode and BWS. Reasons for training of independent walkers were not stated or discussed in the included studies although plausible beneficial effects may be, e.g., an increase in walking speed and/or distance or level of independence. The reported numbers of dropouts were low and a total of 107 participants, representing a broad spectrum of motor impairments completed >1500 training sessions with the HAL system without any reported serious adverse events.
Thus, the accumulated results of the included studies demonstrate that training with the HAL system is feasible when applied in professional settings, irrespective of the patients age and sex and the severity of the lower extremity paresis. The feasibility of training with HAL in the post-acute phase after SCI will need to be explored further.
Even though not stated, the variability in applied frequency, intensity and duration of the reported training sessions and evaluations of outcome, probably reflect both theoretical and practical considerations of, e.g., training needed to achieve significant effects, participants' functional level and study resources. Reasonably, the optimal design would allow training programs to be on the edge for each participant's capacity with regard to the intensity and length of each training session. The intensity and length of the training periods must also consider the patient's functional level as well as the capacity and aims with regard to, e.g., on neuroplasticity, musculoskeletal function, cardiovascular function, gait pattern or independence in walking. Three or more sessions weekly during the training period would probably be justified from a neuroplasticity and relearning perspective (Bowden et al., 2013).
Both single- and double-leg versions of HAL were used even though not specified in all studies. Reasonably the double-leg version is most relevant for subjects with paraparesis and the single-leg version most often appropriate for subjects with one sided paresis.
Only 2 of the studies included patients early after stroke when the potential to utilize beneficial neuroplasticity processes is higher (Bowden et al., 2013) and there is a need for controlled HAL studies in this area. Post-acute studies are more challenging as they have to consider both the impact of spontaneous recovery early after the event as well as other post-acute health problems.
Outcome measures in the included studies primarily relate to aspects of gait function and walking. Most frequently used was the 10 m walking test, which is a measure of over ground walking speed. Six studies report a positive impact on gait function after HAL training, 5 of these specifically on walking speed and 2 studies report increased level of independence in walking according to the FAC (Nilsson et al., 2014; Watanabe et al., 2014). FAC is the most commonly used outcome measure in studies of walking after robotic training for patients with severe to moderate walking limitations in both the acute and chronic phase after stroke (Geroin et al., 2013). FAC takes the persons level of independence and amount of personal assistance required into account, which from the individuals' perspective is more important than walking speed. However, gait speed may be associated with functional ambulation ability (Perry et al., 1995; Dobkin et al., 2014) and a gait speed improvement may generate improved function and quality of life (Schmid et al., 2007). Therefore, we suggest both the FAC and the 10 m walking test to be used in further studies. In studies including participants with severely impaired gait function at baseline and who are unable to walk 10 m, the 2 min walk test (Kosak and Smith, 2005) is an option to be considered in order to achieve baseline data also when participants cannot walk (i.e., 0 m in 2 min). The potential effect of HAL training on movement related function such as gait pattern is poorly addressed in the included studies. Future studies should consider using assessments that cover also these aspects, for example by use of 3-dimensional motion analysis.
Data on self-perceived aspects of the training were scarce and we found no data on perceived activity performance, participation in everyday life, health or cost-effectiveness that need to be approached in future studies. Further, no study reported on potential effects on cardiovascular, metabolic, emotional or cognitive functions of training with the HAL system. The possible additional value of training with HAL in these areas should be of interest in future studies.
Further, controlled studies should compare training with the HAL system with the most relevant alternative training method. As pointed out, gait machines such as the Lokomat differs from the HAL system in terms of the degree of active patient participation. Comparison studies of these gait machines would be of interest. However, until now, studies using Lokomat have not consistently demonstrated effects, regarding sensory-motor function, gait speed, balance and/or mobility, that are superior to those achieved with conventional training (Swinnen et al., 2010; Ucar et al., 2014; van Nunen et al., 2014) although there might be other advantages such as less therapist burden. Thus, further studies that compare the effects of training with the HAL system to the effects of well designed “conventional training” are justified. Moreover, studies combining robotics with other therapeutic interventions with increasing evidence support, such as Fluoxetine (Chollet et al., 2011), BMI (Brain-Machine Interface) (Shindo et al., 2011; Noda et al., 2012) or brain stimulation (Liew et al., 2014) are also of great interest.
Currently, there are a number of exoskeletons at various stages of development or clinical applications. In addition to differences in mechanical design and control strategies existing exoskeletons uses different activation systems to produce movement of the limb. The most common are hydraulic, pneumatic, and electric motor actuator. In a recent review by Chen et al. (2013) focused on lower extremity robots, the authors divides exoskeletons in different subgroups depending on their functioning and design and conclude that real-time control strategies with timely assistance are a new promising area in rehabilitation therapy. The importance of incorporating more active participation in electromechanical gait training (Dobkin, 2009; Pennycott et al., 2012) as well as of allowing variation of the task during training to promote adequate motor learning (Hidler and Sainburg, 2011) has also been addressed previously.
Some recently developed designs of exoskeletons have taken this into account by establishing intention-based control strategies. In the Ekso (Ekso Bionics, online2), ReWalk (Rewalk, online3), and in Indego (Indego, online4) stepping is initiated by shifting of bodyweight. In Indego, shifting of body weight is used in combination with functional electric stimulation (FES). Another exoskeleton the MINDWALKER (Mindwalker, online5) uses EEG and EMG based control.
Recent studies using Ekso for patients in different stages after SCI conclude that the system is safe and show improvements in walking while wearing Ekso (Ekso Clinical Research, online6). For inpatient rehabilitation after stroke the authors find Ekso safe to use and indicate that the training may have an effect on cadence as a result of training with Ekso (Ekso Clinical Research, online). However, the number of participant in these studies are limited and do not allow any further conclusions. Ongoing studies after both SCI and severe stroke (Clinicaltrials, online) will evaluate potential effects on ambulation and mobility.
Indego has been introduces in single-subject clinical trials in SCI patients (Quintero et al., 2011; Farris et al., 2014). An ongoing study will evaluate the safety and effectiveness of using Indego for non-ambulatory or poorly ambulatory SCI patients during standing and walking (Clinicaltrials, online7).
In a study by Zeilig et al. (2012) ReWalk was found to be well tolerated and did not cause any adverse events among persons with SCI. This was repeated in a study by Spungen et al. (ReWalk Peer Reviewed Publications, online8) where persons with motor-complete paraplegia performed different community-based activities while wearing ReWalk. Several ongoing studies where ReWalk is used after SCI are registered at Clinicaltrials.gov.
Like the HAL, exoskeletons such as the powered knee-ankle-foot-orthosis (KAFO) (Sawicki and Ferris, 2009) and NEUROExos (Cain et al., 2007) use EMG activity to detect a person's intended movement. In both KAFO and NEUROExos EMG activity is used to control the activation of a pneumatic power system to provide torque over the ankle and/or knee joint. In HAL the wearer's joint torque is estimated from the EMG signals on both hip and knee muscles and an electrical motor actuator is used to generate power over these joints (Suzuki et al., 2007).
This brief survey of other exoskeletons points to a general need for randomized controlled studies where exoskeletons that allow active participation are compared to other types of interventions as well as for studies with larger study populations.
Since the Hybrid Assistive Limb was developed and is most frequently used in Japan there might be studies published in Japanese journals that were not included in this review. Of note, in 6 of the included studies, the inventor and CEO of the company, Professor Y. Sankai, behind the Hybrid Assistive Limb system is one co-author. No studies using qualitative approach were discovered, which could have been due to the search strategy used. However, even when a broader search was performed, no qualitative studies appeared.
This review identified consistent evidence that the use of the HAL system is feasible when used for gait training in hospital and rehabilitation settings. Data suggest that such training may have beneficial effects on gait function and independence in walking after stroke and after spinal cord injury, but do not allow any conclusions in this respect. Further, well designed controlled studies in these areas are recommended to explore effect sizes and to be followed by larger, confirmatory studies.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. ^SIGN. Scottish Intercollegiate Guidelines Network. Available online at: http://www.sign.ac.uk/methodology/checklists.html [Accessed Dec 2014].
2. ^Ekso Bionics. Available online at: http://intl.eksobionics.com/ekso. [Accessed March 2015].
3. ^ReWalk. Available online at: http://www.rewalk.com/products/rewalk-rehabilitation/. [Accessed March 2015].
4. ^Indego. Available online at: http://www.indego.com/indego/en/home. [Accessed March 2015].
5. ^Mindwalker. Available online at: https://mindwalker-project.eu/. [Accessed March 2015].
6. ^Ekso Clinical Research, Summary of Findings. Available online at: http://intl.eksobionics.com/clinical-research-summary-download. [Accessed March 2015].
7. ^Clinicaltrials.gov. Available online at: https://www.clinicaltrials.gov/ [Accessed Dec 2014].
8. ^ReWalk, Peer Reviewed Publications. Available online at: http://www.rewalk.com/technology/peer-reviewed-publications-copy/. [Accessed March 2015].
Aach, M., Cruciger, O., Sczesny-Kaiser, M., Hoffken, O., Meindl, R. C., Tegenthoff, M., et al. (2014). Voluntary driven exoskeleton as a new tool for rehabilitation inchronicspinal cord injury: a pilot study. Spine J. 14, 2847–2853. doi: 10.1016/j.spinee.2014.03.042
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Berg, K. O., Maki, B. E., Williams, J. I., Holliday, P. J., and Wood-Dauphinee, S. L. (1992). Clinical and laboratory measures of postural balance in an elderly population. Arch. Phys. Med. Rehabil. 73, 1073–1080.
Bowden, M. G., Woodbury, M. L., and Duncan, P. W. (2013). Promoting neuroplasticity and recovery after stroke: future directions for rehabilitation clinical trials. Curr. Opin. Neurol. 26, 37–42. doi: 10.1097/WCO.0b013e32835c5ba0
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Cain, S. M., Gordon, K. E., and Ferris, D. P. (2007). Locomotor adaptation to a powered ankle-foot orthosis depends on control method. J. Neuroeng. Rehabil. 4:48. doi: 10.1186/1743-0003-4-48
Chen, G., Chan, C. K., Guo, Z., and Yu, H. (2013). A review of lower extremity assistive robotic exoskeletons in rehabilitation therapy. Crit. Rev. Biomed. Eng. 41, 343–363. doi: 10.1615/CritRevBiomedEng.2014010453
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Chollet, F., Tardy, J., Albucher, J. F., Thalamas, C., Berard, E., Lamy, C., et al. (2011). Fluoxetine for motor recovery after acute ischaemic stroke (FLAME): a randomised placebo-controlled trial. Lancet Neurol. 10, 123–130. doi: 10.1016/S1474-4422(10)70314-8
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Dobkin, B. H. (2009). Motor rehabilitation after stroke, traumatic brain, and spinal cord injury: common denominators within recent clinical trials. Curr. Opin. Neurol. 22, 563–569. doi: 10.1097/WCO.0b013e3283314b11
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Dobkin, B. H., Nadeau, S. E., Behrman, A. L., Wu, S. S., Rose, D. K., Bowden, M., et al. (2014). Prediction of responders for outcome measures of locomotor Experience Applied Post Stroke trial. J. Rehabil. Res. Dev. 51, 39–50. doi: 10.1682/JRRD.2013.04.0080
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Farris, R. J., Quintero, H. A., Murray, S. A., Ha, K. H., Hartigan, C., and Goldfarb, M. (2014). A preliminary assessment of legged mobility provided by a lower limb exoskeleton for persons with paraplegia. IEEE Trans. Neural Syst. Rehabil. Eng. 22, 482–490. doi: 10.1109/TNSRE.2013.2268320
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Geroin, C., Mazzoleni, S., Smania, N., Gandolfi, M., Bonaiuti, D., Gasperini, G., et al. (2013). Systematic review of outcome measures of walking training using electromechanical and robotic devices in patients with stroke. J. Rehabil. Med. 45, 987–996. doi: 10.2340/16501977-1234
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Hesse, S., Waldner, A., and Tomelleri, C. (2010). Innovative gait robot for the repetitive practice of floor walking and stair climbing up and down in stroke patients. J. Neuroeng. Rehabil. 7:30. doi: 10.1186/1743-0003-7-30
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Hidler, J., and Sainburg, R. (2011). Role of Robotics in Neurorehabilitation. Top. Spinal Cord Inj. Rehabil. 17, 42–49. doi: 10.1310/sci1701-42
Holden, M. K., Gill, K. M., Magliozzi, M. R., Nathan, J., and Piehl-Baker, L. (1984). Clinical gait assessment in the neurologically impaired. Reliability and meaningfulness. Phys. Ther. 64, 35–40.
Kawamoto, H. (2002). “Power assist system HAL-3 for gait disorder person,” in Lecture Notes in Computer Science, ICCHP 2002, LNCS 2398, eds K. Miesenberger, J. Klaus, and W. Zagler (Berlin; Heidelberg: Springer-Verlag), 196–203.
Kawamoto, H., Kamibayashi, K., Nakata, Y., Yamawaki, K., Ariyasu, R., Sankai, Y., et al. (2013). Pilot study of locomotion improvement using hybrid assistive limb in chronic stroke patients. BMC Neurol. 13:141. doi: 10.1186/1471-2377-13-141
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Kawamoto, H., Taal, S., Niniss, H., Hayashi, T., Kamibayashi, K., Eguchi, K., et al. (2010). “Voluntary motion support control of Robot Suit HAL triggered by bioelectrical signal for hemiplegia,” in Conference Proceedings:Annual International Conference of the IEEE Engineering in Medicine and Biology Society. IEEE Engineering in Medicine and Biology Society. Annual Conference (Buenos Aires), 462–466.
Kosak, M., and Smith, T. (2005). Comparison of the 2-, 6-, and 12-minute walk tests in patients with stroke. J. Rehabil. Res. Dev. 42, 103–107. doi: 10.1682/JRRD.2003.11.0171
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Krakauer, J. W., Carmichael, S. T., Corbett, D., and Wittenberg, G. F. (2012). Getting neurorehabilitation right: what can be learned from animal models? Neurorehabil. Neural Repair 26, 923–931. doi: 10.1177/1545968312440745
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Kubota, S., Nakata, Y., Eguchi, K., Kawamoto, H., Kamibayashi, K., Sakane, M., et al. (2013). Feasibility of rehabilitation training with a newly developed wearable robot for patients with limited mobility. Arch. Phys. Med. Rehabil. 94, 1080–1087. doi: 10.1016/j.apmr.2012.12.020
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Kwakkel, G., van Peppen, R., Wagenaar, R. C., Wood Dauphinee, S., Richards, C., Ashburn, A., et al. (2004). Effects of augmented exercise therapy time after stroke: a meta-analysis. Stroke 35, 2529–2539. doi: 10.1161/01.STR.0000143153.76460.7d
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Langhorne, P., Bernhardt, J., and Kwakkel, G. (2011). Stroke rehabilitation. Lancet 377, 1693–1702. doi: 10.1016/S0140-6736(11)60325-5
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Langhorne, P., Coupar, F., and Pollock, A. (2009). Motor recovery after stroke: a systematic review. Lancet Neurol. 8, 741–754. doi: 10.1016/S1474-4422(09)70150-4
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Liew, S. L., Santarnecchi, E., Buch, E. R., and Cohen, L. G. (2014). Non-invasive brain stimulation in neurorehabilitation: local and distant effects for motor recovery. Front. Hum. Neurosci. 8:378. doi: 10.3389/fnhum.2014.00378
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Maeshima, S., Osawa, A., Nishio, D., Hirano, Y., Takeda, K., Kigawa, H., et al. (2011). Efficacy of a hybrid assistive limb in post-stroke hemiplegic patients: a preliminary report. BMC Neurol. 11:116. doi: 10.1186/1471-2377-11-116
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Mehrholz, J., Elsner, B., Werner, C., Kugler, J., and Pohl, M. (2013). Electromechanical-assisted training for walking after stroke: updated evidence. Stroke 44, e127–e128. doi: 10.1161/STROKEAHA.113.003061
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Mehrholz, J., Kugler, J., and Pohl, M. (2012). Locomotor training for walking after spinal cord injury. Cochrane Database Syst. Rev. 11:CD006676. doi: 10.1002/14651858.CD006676.pub3
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Nilsson, A., Vreede, K. S., Haglund, V., Kawamoto, H., Sankai, Y., and Borg, J. (2014). Gait training early after stroke with a new exoskeleton—the hybrid assistive limb: a study of safety and feasibility. J. Neuroeng. Rehabil. 11:92. doi: 10.1186/1743-0003-11-92
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Noda, T., Sugimoto, N., Furukawa, J., Sato, M., Sang-Ho, H., and Morimoto, J. (2012). “Brain-controlled exoskeleton robot for BMI rehabilitation. Humanoid Robots (Humanoids),” in 12th IEEE-RAS International Conference (Osaka), 21–27. doi: 10.1109/HUMANOIDS.2012.6651494
Pennycott, A., Wyss, D., Vallery, H., Klamroth-Marganska, V., and Riener, R. (2012). Towards more effective robotic gait training for stroke rehabilitation: a review. J. Neuroeng. Rehabil. 9:65. doi: 10.1186/1743-0003-9-65
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Perry, J., Garrett, M., Gronley, J. K., and Mulroy, S. J. (1995). Classification of walking handicap in the stroke population. Stroke 26, 982–989. doi: 10.1161/01.STR.26.6.982
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Peurala, S. H., Karttunen, A. H., Sjogren, T., Paltamaa, J., and Heinonen, A. (2014). Evidence for the effectiveness of walking training on walking and self-care after stroke: a systematic review and meta-analysis of randomized controlled trials. J. Rehabil. Med. 46, 387–399. doi: 10.2340/16501977-1805
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Podsiadlo, D., and Richardson, S. (1991). The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 39, 142–148.
Quintero, H. A., Farris, R. J., Hartigan, C., Clesson, I., and Goldfarb, M. (2011). A powered lower limb orthosis for providing legged mobility in paraplegic individuals. Top Spinal Cord Inj. Rehabil. 17, 25–33. doi: 10.1310/sci1701-25
Sawicki, G. S., and Ferris, D. P. (2009). A pneumatically powered knee-ankle-foot orthosis (KAFO) with myoelectric activation and inhibition. J. Neuroeng. Rehabil. 6:23. doi: 10.1186/1743-0003-6-23
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Schmid, A., Duncan, P. W., Studenski, S., Lai, S. M., Richards, L., Perera, S., et al. (2007). Improvements in speed-based gait classifications are meaningful. Stroke 38, 2096–2100. doi: 10.1161/STROKEAHA.106.475921
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Schwartz, I., and Meiner, Z. (2013). The influence of locomotor treatment using robotic body-weight-supported treadmill training on rehabilitation outcome of patients suffering from neurological disorders. Harefuah 152, 166–171, 182, 181.
Shindo, K., Kawashima, K., Ushiba, J., Ota, N., Ito, M., Ota, T., et al. (2011). Effects of neurofeedback training with an electroencephalogram-based brain-computer interface for hand paralysis in patients with chronic stroke: a preliminary case series study. J. Rehabil. Med. 43, 951–957. doi: 10.2340/16501977-0859
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Suzuki, K., Mito, G., Kawamoto, H., Hasegawa, Y., and Sankai, Y. (2007). Intention-based walking support for paraplegia patients with Robot Suit HAL. Adv. Robot. 21, 1441–1469. doi: 10.1163/156855307781746061
Swinnen, E., Duerinck, S., Baeyens, J. P., Meeusen, R., and Kerckhofs, E. (2010). Effectiveness of robot-assisted gait training in persons with spinal cord injury: a systematic review. J. Rehabil. Med. 42, 520–526. doi: 10.2340/16501977-0538
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Ucar, D. E., Paker, N., and Bugdayci, D. (2014). Lokomat: a therapeutic chance for patients with chronic hemiplegia. NeuroRehabilitation 34, 447–453. doi: 10.3233/NRE-141054
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Ueba, T., Hamada, O., Ogata, T., Inoue, T., Shiota, E., and Sankai, Y. (2013). Feasibility and safety of acute phase rehabilitation after stroke using the hybrid assistive limb robot suit. Neurol. Med. Chir. (Tokyo) 53, 287–290. doi: 10.2176/nmc.53.287
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
van Nunen, M. P., Gerrits, K. H., Konijnenbelt, M., Janssen, T. W., and De Haan, A. (2014). Recovery of walking ability using a robotic device in subacute stroke patients: a randomized controlled study. Disabil. Rehabil. Assist. Technol. 10, 141–148. doi: 10.3109/17483107.2013.873489
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Wade, D. T., Wood, V. A., Heller, A., Maggs, J., and Langton Hewer, R. (1987). Walking after stroke. Measurement and recovery over the first 3 months. Scand. J. Rehabil. Med. 19, 25–30.
Watanabe, H., Tanaka, N., Inuta, T., Saitou, H., and Yanagi, H. (2014). Locomotion improvement using a hybrid assistive limb in recovery phase stroke patients: a randomized controlled pilot study. Arch. Phys. Med. Rehabil. 95, 2006–2012. doi: 10.1016/j.apmr.2014.07.002
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Zeilig, G., Weingarden, H., Zwecker, M., Dudkiewicz, I., Bloch, A., and Esquenazi, A. (2012). Safety and tolerance of the ReWalk™ exoskeleton suit for ambulation by people with complete spinal cord injury: a pilot study. J. Spinal Cord Med. 35, 96–101. doi: 10.1179/2045772312Y.0000000003
PubMed Abstract | Full Text | CrossRef Full Text | Google Scholar
Keywords: rehabilitation, robotics, gait, walking, locomotion, paresis, review, gait machine
Citation: Wall A, Borg J and Palmcrantz S (2015) Clinical application of the Hybrid Assistive Limb (HAL) for gait training—a systematic review. Front. Syst. Neurosci. 9:48. doi: 10.3389/fnsys.2015.00048
Received: 23 December 2014; Accepted: 10 March 2015;
Published: 25 March 2015.
Edited by:
Mikhail Lebedev, Duke University, USAReviewed by:
Jun Morimoto, ATR Computational Neuroscience Labs, JapanCopyright © 2015 Wall, Borg and Palmcrantz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anneli Wall, Department of Rehabilitation Medicine, Danderyd University Hospital, Danderyds Sjukhus, Rehabiliteringsmedicinska Universitetskliniken, Hus 39, plan 3, Stockholm 18288, SwedenYW5uZWxpLndhbGxAZHMuc2U=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.