 Olyssa Starry
Olyssa Starry Arjun Viray
Arjun Viray Brenna Park-Egan2
Brenna Park-Egan2 Amber Collett Terway
Amber Collett Terway Timothy Oxendahl
Timothy Oxendahl Tina Burdsall
Tina Burdsall
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Sustain. Cities, 19 July 2022
Sec. Urban Greening
Volume 4 - 2022 | https://doi.org/10.3389/frsc.2022.811306
This article is part of the Research TopicSocio-Ecological Dynamics of Green Roof EcosystemsView all 8 articles
The potential for urban open spaces to convey therapeutic benefits is increasingly substantiated. More work is needed to specifically consider how low impact designs to manage stormwater such as ecoroofs perform in this context. Here, we report on a pilot study addressing: (1) factors determining whether a hospital has an ecoroof, and (2) how ecoroofs might convey therapeutic benefits. We utilized a mixed methods approach which encompassed phone interviews of hospital ecoroof managers as well as analysis of national hospital databases. We also conducted a local case study which compared cortisol samples and stress indicators from patients, staff, and caregivers visiting an ecoroof to those waiting indoors at the Oregon Health and Sciences University in Portland OR. Behavioral observations took place at this same location. In 2017, we identified 105 hospitals with ecoroofs in the contiguous United States. Our analysis of a national hospital database found two factors that significantly increased the likelihood of a hospital having an ecoroof: Medicaid discharges per year; and non-profit status. Interviews with practitioners nationally revealed a wide range of motivations but that therapy was a consideration for a majority, but notably not all, of the hospitals surveyed. They similarly noted variation in roof design, maintenance, and programming around horticultural therapy; we highlight some best practices here. Our physiological case study was limited in sample size. Preliminary findings showed that salivary cortisol levels varied by ecoroof visitor type, ranging on average from 0.09 μg/ml for caregivers to 0.30 μg/ml for patients. We did not observe any significant changes in visitor cortisol. This could be explained by low replication or the short treatment duration. Alternatively, these pilot data may indicate a gap in horticultural therapy theory vs. practice. Behavioral observations demonstrated a wide array of different uses of the ecoroof space such as cell phone use and passing by. Though preliminary, our findings suggest that therapeutic effects may vary by user type and activity and depend on roof design and goals. This study offers both information on the therapeutic potential of hospital ecoroofs as well as lessons learned regarding different approaches to researching this somewhat new topic.
The positive effects of horticultural therapy, therapy gardens, and other greenspaces are well-documented. These studies range from foundational examples in which people find pictures of greenspace more calming compared to urban environments (Ulrich, 1979), to physiological studies documenting reduced blood pressure in people who had walked through a park compared to a busy urban environment (Hartig et al., 2003), to more recent findings revisiting the positive effects of forest bathing related to the traditional Japanese practice, “Shinrin-yoku,” on human health (Park et al., 2010). These benefits are also recognized by medical practitioners. For example, patient exposure to light and landscaped areas has a profound effect on alleviating pain (Malenbaum et al., 2008; Ulrich et al., 2008). As such, hospitals are increasingly installing therapeutic landscapes such as therapeutic gardens and memory gardens (Marcus and Sachs, 2014).
A robust and growing discourse community on the relationship between open space and human health has emerged in the United States, dating back to the 1990s if not earlier. For example, since 1999 the Therapeutic Landscapes Network (The Therapeutic Landscapes Network, 2022) has been fostering a transdisciplinary dialog about how evidence-based design, primarily at healthcare facilities, can be used to foster health and wellbeing. The American Horticultural Therapy Association (The American Horticultural Therapy Association, 2022) started publishing definitions of key terms in the field in 1995, and defines horticultural therapy as, “the participation in horticultural activities facilitated by a registered horticultural therapist to achieve specific goals within an established treatment, rehabilitation, or vocational plan…” This organization further defines a therapeutic garden as being “designed for use as a component of a treatment, rehabilitation, or vocational program. A garden can be described as therapeutic in nature when it has been designed to meet the needs of a specific user or population. It is designed to accommodate participant's goals and to facilitate people-plant interactions.”
The aforementioned references and organizations do not appear to be adequately considered when creating and evaluating green infrastructure projects. In addition to urban parks and gardens that are more readily considered therapeutic, green infrastructure encompasses a variety of landscape features including ecoroofs, bioswales, and street trees, and researchers are beginning to recognize the therapeutic properties of these features (Barron et al., 2019; Wolf et al., 2020).
Ecoroofs are a type of green infrastructure that incorporate plant material on top of a substrate separated from a roof's primary water-proofing membrane by protective felt and possibly by insulation. They are recognized for providing several ecosystem services including stormwater management and habitat provisioning for urban wildlife such as insects. As the world becomes more urbanized, less open space will be available for both urban wildlife and for human interaction. This raises the question of whether ecoroofs might provide similar therapeutic benefits as bioswales and urban parks with lower required real estate investment and perhaps easier access for both humans and wildlife.
Less is known about the ability of these systems to provide therapeutic benefits, especially in a medical context. Some have suggested that installing an ecoroof may improve worker productivity or provide a view that can be conducive to test taking (Lee et al., 2015). One pioneering study (Davis, 2011) conducted a post-occupancy evaluation (POE) of one rooftop garden in Georgia designed for physical therapy. This study (Davis, 2011) offers groundbreaking information about the ways in which visitors benefitted from this space, but it also suggests room for improvement in the design process as well as maintenance strategy.
Despite the huge potential of ecoroofs to convey horticultural therapy, there are many reasons to suspect that this opportunity may not be fully utilized. As noted by Davis, 2011, not all ecoroofs can be installed in locations that are accessible, or easily viewed. Some pose safety challenges or require expensive railings to be installed. Plant species need to be selected to serve both therapeutic demands as well as the harsh environmental conditions on urban roofs.
A study at a residential facility in Singapore demonstrated that only 20% of residents visited the ecoroof installed there (Yuen and Nyuk Hien, 2005). Similar work addresses what mechanisms might explain these varying responses; for example, with respect to planting palette, Lee et al. (2014) found that respondents to their survey thought ecoroofs planted in herbaceous plants were more aesthetically pleasing than those planted in drought tolerant succulents.
To our knowledge, only one study has been conducted to date which address whether ecoroofs can provide physiological benefits such as reduced stress levels or hospital stays as has been shown with, for example, hospital room greenery. This work, in Portland's Legacy Memorial hospital found that nurses who took their break on a hospital ecoroof were less likely to show signs of burnout than when they took their breaks in an indoor breakroom (Cordoza et al., 2018).
The stresses of being a hospital resident (Gonzalez-Cabrera et al., 2018), patient (Park and Mattson, 2008), or even a caretaker (Seltzer et al., 2010) have all been demonstrated through increases in salivary cortisol. This is because when the hypothalamic-pituitary-adrenal axis is activated by a stressful event, cortisol is released into the bloodstream; the stressful event could be physical such as pain as well as psychological (Dickerson and Kemeny, 2004). This activation triggers increased metabolism and an adaptative stress response, but in the long term chronically elevated cortisol can have adverse effects such as heart disease and suppression of immune response (Dickerson and Kemeny, 2004).
Past research shows that spending time in nature, and even carrying out other horticultural activities such as creating floral arrangements (Lee, 2010), can significantly reduce cortisol levels. For example, people who are exposed to more vegetated outdoor environments tend to have lower levels of cortisol compared to those exposed to less vegetated urban environments (Roe et al., 2013; Triguero-Mas et al., 2017). Moreover, people who live in communities which provide access to green spaces not only have lower levels of perceived stress but also have greater diurnal cortisol decline (Thompson et al., 2014). Students who learn in a natural environment, such as in a forest, have greater declines in cortisol than students who learn in a traditional classroom setting (Dettweiler et al., 2017). Both the act of viewing nature videos as well as walking in nature are associated with cortisol reductions, with walking in nature showing a stronger effect (Olafsdottir et al., 2020). Recent findings also show that spending time in therapeutically designed sensory gardens can also result in a reduction of cortisol levels (Souter-Brown et al., 2021).
In this contribution to the special series on the socio-ecological dynamics of ecoroofs, we aim to situate hospital ecoroofs within their social context by (1) evaluating the factors that determine whether a hospital acquires an ecoroof and (2) exploring how the ecoroofs might provision therapeutic benefits, via physiological testing and behavioral observation.
In 2017, we identified a list of 105 hospitals in the contiguous United States with ecoroofs from an international online database of ecoroofs (greenroofs.com), through internet searches, attending trade association meetings, and referrals. To determine the context in which hospital ecoroofs are being considered therapeutically, we conducted a four-part evaluation which combines (1) regression analyses to identify factors which might predict whether a hospital acquires an ecoroof; (2) telephone interviews of hospital administrators and sustainability professionals; and (3) a local case study that included both physiological response testing and behavioral observations. This mixed methods design allowed each evaluation to build on what we learned from the others, also known as the connected contributions strategy (Morgan, 2014).
In order to identify factors that could predict the presence of a hospital ecoroof, we acquired data on over 4,000 hospitals from the American Hospital Association. This dataset included 67 of the 105 hospitals we identified as having ecoroofs (Figure 1). Hospitals whose Medicare/Medicaid information was estimated by the American Hospital Association were excluded, and facilities were included in analysis only if exact information was known. A random sample of 134 non-ecoroof hospitals were selected for a 2:1 ratio in the analysis dataset. A logistic regression prediction model was developed from the hospital ecoroof dataset. A binary outcome variable indicating the presence/absence of an ecoroof was tested against numerous predictor variables including: total facility beds, total admissions, Medicaid discharges, Medicare discharges, total average yearly patient revenue (calculated from reports spanning ~2015–2017), the hospital's census region, status as a teaching hospital (major, minor, or non-teaching), type of ownership (non-profit, government, or for-profit), and the hospital's USDA agricultural zone. Stata 15.1 was used for statistical analysis (StataCorp LLC, College Station, TX). A p-value of <0.05 was used to determine statistical significance.

Figure 1. Hospital Ecoroofs located in the contiguous United States overlain on the (unofficial) USDA Plant Hardiness map.
Each continuous independent variable was assessed for normal distribution. All of the continuous variables were observed to have a right-skewed distribution as most hospitals were similarly sized, although a few extremely large facilities were present in the dataset. We therefore log-transformed total facility beds and total patient revenue and took the square root of Medicaid and Medicare discharges to obtain normal distribution. Missing values within the dataset were identified and evaluated. It was determined that records for most hospitals in the set were 80% or more complete. Most missing data points were related to financial metrics, with a few hospitals also missing information about beds or Medicare/Medicaid discharges. About 25% of hospitals lacked information about licensed beds, so the more complete metric of total beds was used in analysis. Two hospitals for which no information was available were excluded from the dataset. The Little's Missing Completely at Random test was performed, and it was determined that the missing values were uninformative (random). Therefore, imputation was not necessary for regression analysis.
Full stepwise selection was performed to test the significance of each predictor variable, with a p-value of ≤ 0.05 required for inclusion in the final model. Multi-model inference was then used to examine possible combinations of predictors. Model diagnostics were performed in state to evaluate the performance of the logistic regression model. Classification was assessed using the Hosmer-Lemeshow test. Receiver operating characteristic (ROC) curve analysis and classification statistics were used to determine sensitivity and specificity. Pseudo R2 and overall misclassification rate were used to report overall model performance.
We conducted national phone surveys of hospital administrators and sustainability professionals at 21 of 105 hospitals throughout the U.S. that are known to have ecoroofs. The goal of the phone survey was to determine how ecoroofs are being used in the hospital setting. The surveys were expected to last ~30–45 min and contain both structured survey questions and open-ended questions. A modified grounded theory approach was taken to analyze the qualitative portion of the surveys where both inductive coding and a priori codes were used. Appendix 1 depicts the main study concepts and example questions developed to gain this information.
In order to verify any physiological benefits of hospital ecoroofs, we measured changes in salivary cortisol in visitors to the publicly accessible ecoroof/roof terrace on the Oregon Health and Sciences University (OHSU) Center for Health and Healing (Figure 2) and alternate indoor waiting/staff lounge areas for comparison. Salivary cortisol is an ideal stress indicator, relative to some other measures of stress response such as physiologic markers in the blood, because it changes rapidly in response to stimulus while being less invasive than a blood draw (Kirschbaum and Hellhammer, 1994).
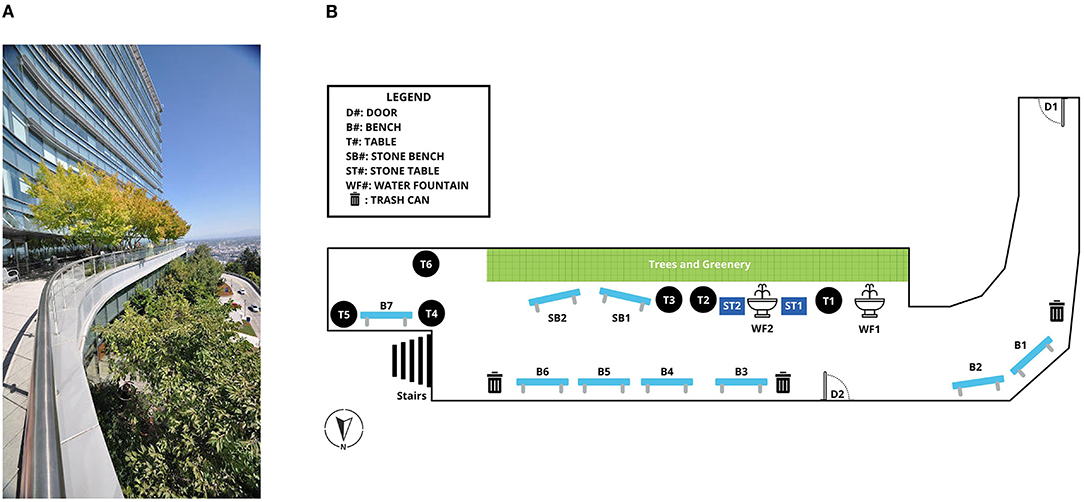
Figure 2. Case study location at the Oregon Health and Sciences University. (A) The roof includes a series of planters with healthy shade trees. (B) A diagram of the site was constructed to assist in behavioral observations.
Visitors to both areas were greeted upon arrival and asked for participatory consent. The consent form included questions to determine visitor category (i.e., as a patient, caretaker/family member, or medical professional/staff), select questions from the Y-1 State Trait anxiety Inventory (Spielberger et al., 1983) as well as some general questions about age, gender, and race. Then, a salivary sample was taken and the time noted. Fifteen minutes later, visitors were instructed to provide a second salivary sample upon leaving their respective study spaces; at this time, they were prompted to write 1–2 sentences about how they spent their time at the study site. Data were collected using the RedCap (Research electronic data collection) system. Due to funding constraints, we were only able to sample during the month of May 2019.
Samples were taken within the same 2-h window (2–4 pm), based on evidence that baseline cortisol levels fluctuate the least in the afternoon (Dickerson and Kemeny, 2004). Differences in average cortisol levels as well as survey responses provided on a Likert scale across and between visitor types were assessed via ANOVA followed by Tukey's post-hoc analysis.
Behavioral observations were conducted at the aforementioned roof terrace on OHSU (Figure 2). We spent at least 4 h conducting observations at different times of day for at least 5 days at these locations, with two researchers working together. Observations were recorded following the protocol in (Vander Poel and Griffin, 2017): We classified users into different groups based on apparel (visitor, patient, staff). Duration was defined as time passed (in minutes) from the onset of an event (enter garden) to the closure of that event (exit). An event can include multiple user groups and activities.
Categories of activities include: quick chat, work meeting, cell-phone, sit and talk, sit and relax, sit and wait, walking around, natural features, struck interaction, play, let children play, patient interaction, patient room, and lunch. To the best extent feasible, we documented these activities spatially (Figure 2).
A total of 105 hospitals with ecoroofs were identified in the contiguous United States (Figure 1). While 60 percent of these hospital ecoroofs were determined to be accessible, 40 percent were not (Table 1). Ecoroofs were also found to be located in a wide range of hospital types with the majority being located on general hospitals (Table 1). Over half of these roofs were installed during the period from 2008 to 2013 (Table 2).
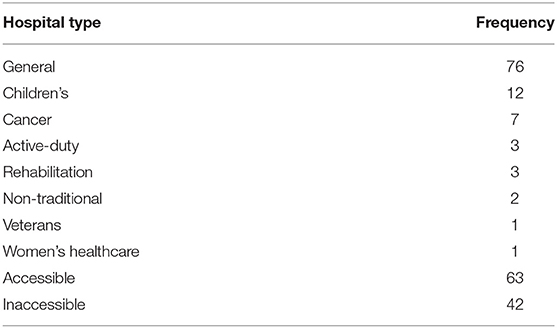
Table 1. Number of green roofs according to hospital type and their accessibility.
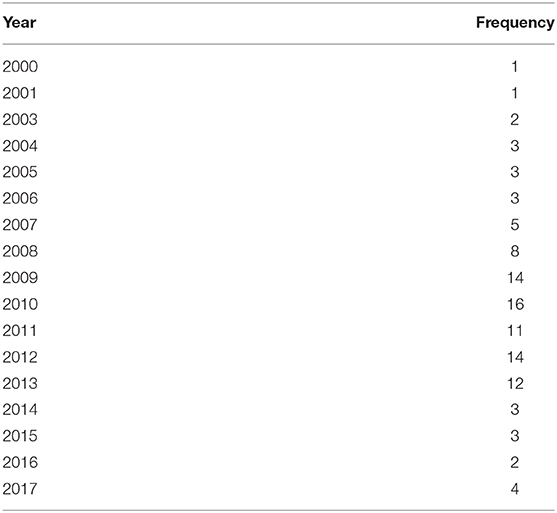
Table 2. Number of green roofs installed each year from 2000 to 2017.
The final logistic regression model contained the independent variables of hospital type (for-profit, non-profit, or government-owned, with for-profit hospitals as the reference level) and number of Medicaid discharges (Table 3).

Table 3. Results table showing the significant predictors (Medicare/Medicaid discharges and non-profit status or “type”) of hospital ecoroofs in the contiguous United States.
Based on these findings, every 100 Medicaid discharges per year is associated with a 15% increase in the likelihood of having an ecoroof at the facility. Government-run hospitals were almost three times less likely to have ecoroofs at their facilities than for-profit hospitals, and more than three times less likely when compared to non-profit hospitals.
Diagnostics performed in Stata showed fairly good predictive performance of this model, with a total area under the ROC curve of 0.848. The model showed relatively high specificity (82.03%) and sensitivity (73.13%). A Hosmer-Lemeshow goodness of fit test resulted in a p-value of 0.1907, indicating no evidence of poor fit. The model had a pseudo R2 of 0.29 and an overall correct classification rate of 78.97%.
Motivations and disincentives revealed at different stages of the design process and implementation. The 21 practitioners and administrators we were able to interview represent a slightly skewed sample in that subjects were more likely to have an accessible roof (76%) compared to our overall estimate closer to 60% accessible (Table 1). Respondents confirmed that safety and liability concerns were the main explanations in the cases of restricted use. Two respondents were care providers, 13 held positions relating to facilities or grounds and six held professional services roles. Nine held director level positions within their category and five held supervisor or manager level positions.
Respondents never had a singular motivation for initially putting resources into an ecoroof; rather, responses shared a variety of motivations (Figure 3). Still, 62 percent of respondents (13 of 21) felt their institutions considered the therapeutic benefits of an ecoroof during planning or design. Of the eight that felt therapeutic benefits were not considered, three had use consistent with therapeutic use after installation (i.e., staff seen using the space as a break area, patients able to see the roof from windows, etc.). At the same time, horticultural therapy was frequently conflated with landscape architecture or general horticulturalism. The role of a horticultural therapist may not be widely understood. In addition to therapy use, three hospitals mentioned other types of programming being conducted on their ecoroof: (1) special and appreciation events; (2) nutrition and wellness programs; and (3) educational programs (i.e., medicinal planting).
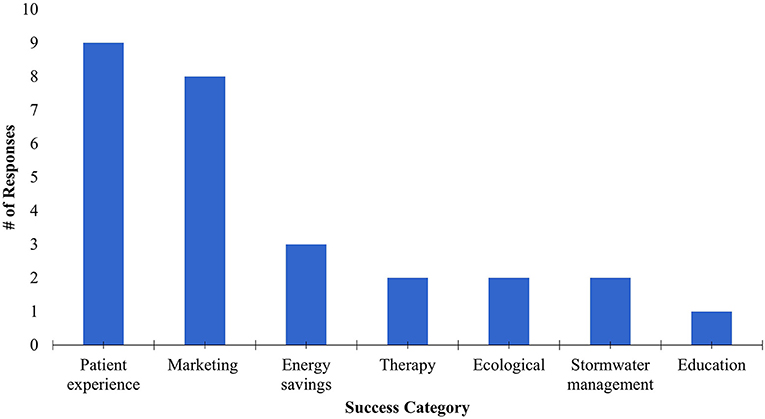
Figure 3. Hospital administrators described the ways they felt their ecoroof projects were successful. This figure categorizes their responses.
Just over 50 percent of respondents (11 of 21) mentioned cost as a key factor in their decision- making regarding the installation of additional ecoroofs in the future. Twelve of 21 respondents were willing to add or would consider adding additional ecoroofs. “It is the age-old problem of funding. We really don't have a lot of extra money...I will need to make the case that we will be able to save over the long-term and those savings are going to come mainly from not having to replace a traditional roof as often.” (Hospital 15)
Interviews also indicated that a vocal champion for installation can be critical in the design process. If there was a strong champion advocating for an ecoroof, a hospital or medical facility was more likely to invest resources—especially if that champion held a senior or leadership position (i.e., CEO). However, leadership did not always have to drive interest in an ecoroof. Vocal advocates at all levels who felt they had the authority or freedom to experiment, also made successful cases for initial or additional investment in ecoroof infrastructure.
Engaging maintenance and facilities in planning and design increased perceived success of an ecoroof. Staff involved in the planning and design phases were typically senior level staff and technocrats (i.e., architects, sustainability professionals). In institutions where the specialist knowledge of groundskeepers and maintenance technicians was only engaged at the installation or day-to-day care stages, respondents noted feeling understaffed or under-resourced, and were therefore less likely to describe the institution's ecoroof a success. “I wasn't directly involved in that [decision making]; I was just given the job of installing…It's not something they're real in love with. Some of them [grounds maintenance] weren't even approving of it to begin with. It's just something they were told: that's what we're getting.” (Hospital 48).
No respondents knew of efforts to track or conduct formal counts of the number of people who access ecoroofs for a defined period of time. Respondents provided estimated ranges for accessible ecoroofs of 10–100 users per day, with at least two noting that seasonality and weather greatly impact use of a ecoroof space. The highest use ecoroofs were being intentionally used as respite or therapy spaces (including as a healing garden), as outdoor cafeterias, for educational programming or as food producing gardens.
Figure 3 depicts the various ways respondents felt their ecoroofs were successful. Utilizing grounded and a priori coding, responses describing respondents' understanding of success were categorized, and responses could receive more than one code. Patient experience was the leading way that respondents described roof success. For example, one respondent stated “I think this one is successful because you can go out, work it, touch it, feel it. And it is used as part of their therapy...They have different terrain out there so they can practice.” (Hospital 67) This statement also registered a “therapy” code in addition to a “patient experience” code. Similarly, the following statement would have been coded as patient experience as well. “For the most part it's, just relaxing. It's basically a solitude area. A decompression area. Staff use it for their lunch time, dinner breaks, breakfast break.” (Hospital 108). Other response codes that were tallied under patient experience included words and phrases such as: “patient ratings,” “pretty,” or “visual appeal.” The sum of hospitals that indicated any of these codes for each success category is depicted in Figure 3.
Many respondents also felt that their hospital ecoroofs were successful marketing tools. One hospital noted that the ecoroof is used as a place to recognize donors and supporters. Codes that placed a response in this category included words or phrases such as “marketing,” “fundraising appeal,” “prospective students,” “prospective patients,” “keeping up with others,” and “competition.” The focus on marketing appeal of eco and greenroofs raises a question of how hospital administrators understand the environmental identity of their target market groups (Shepley et al., 2020). More work is needed to consider how research is informing marketing practices. At the same time, if marketing is being used honestly and effectively, this is something that could be considered in future cost-benefit analyses (Manso et al., 2021).
Of the 35 people who participated in the physiological part of the study, there were two patients, eleven caregivers, and twenty-two medical professionals/OHSU staff. The mean age of patients was 72, the mean age of caregivers was 48, and the mean age of medical professionals/OHSU staff was 37. Three (9%) participants identified as Asian/Pacific Islander. One (3%) participant identified as Black. One (3%) participant identified as Latino/Hispanic. One (3%) participant self-identified as Multi-ethnic. Twenty-nine (83%) participants identified as White. One staff participant's cortisol level change was an outlier, with an increase of 3.13 μg/mL and is not included in subsequent analysis. This sample was double-checked and may be the result of sample contamination. We had difficulty locating a waiting room in this hospital facility that didn't have a beautiful window looking out into the Willamette Valley; therefore, only medical professionals/OHSU staff were sampled indoors (n = 11). The cortisol changes were then compared across roles.
Initial salivary cortisol levels varied by ecoroof visitor type, ranging on average from 0.09 μg/mL for caregivers to 0.30 μg/ml for patients, who were also the oldest of age in our study. For “pre” samples, salivary cortisol concentrations were higher for staff outdoors compared to caregivers outdoors (p = 0.22) and staff indoors (p = 0.21). For “post” samples, salivary cortisol remained higher in staff outdoors compared to these two groups (p = 0.12 and p = 0.19, respectively) (Figure 4). The average cortisol change among patients was a reduction of 0.032 μg/mL, and the average cortisol change among caregivers was a reduction of 0.012 μg/mL. Among those staff members who were surveyed on the ecoroof, the average cortisol difference was an increase of 0.037 μg/mL. Among those staff members who were surveyed in the waiting room, the average cortisol difference was a slight increase of 0.001 μg/mL. We did not observe any significant changes in visitor cortisol.
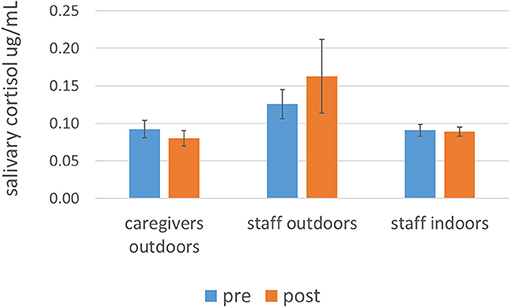
Figure 4. Average (± two times the standard error) cortisol levels for staff outdoors (n = 11), staff indoors (n = 10), caregivers outdoors (n = 11) before and after a minimum 15-min exposure to indoor and outdoor (ecoroof) waiting areas. Note results from patients, with lower replication (n = 2), are provided in the text. Significant differences in levels for staff outdoors compared to other user types, including staff indoors, can only be considered, separately for pre and post conditions, at the p = 0.22 level or less. No significant changes in cortisol level were observed.
Survey responses also did not reveal much difference between the user groups. However, one trait (worriedness) showed a potential significant difference (p = 0.07) between ecoroof (both caregivers and staff) and waiting room users; users of the ecoroof felt slightly more worried than those in the waiting room. However, none of the qualitative responses clarified from where this difference might arise.
In total, behavioral observations were made for 281 hospital roof visitors. The average time spent in the green roof was 8.58 min for patients, 22.83 min for visitors, and 5.88 min by staff. The most frequent activities in which visitors engaged included looking at the view, passing through, and eating/drinking. The most frequent activities in which staff engaged included passing through, eating/drinking, and talking on their phones. Patients primarily used the space for eating/drinking.
Although early ecoroofs in the United States were fairly similar in design based on the intent to maximize stormwater management, new and exciting designs are emerging including a growing number of hospital ecoroofs. We thought revenue might be a stronger predictor of hospital ecoroof construction given their higher initial price tag compared to traditional roofing. Instead, non-profit hospitals with Medicare/Medicaid patients were more likely to have ecoroofs. More work is needed to explain these findings, but we suggest that these projects might be driven by donors or funders who might be more willing to factor in the myriad of ecoroof benefits into cost-benefit analyses (Figure 3, City of Portland, 2008; Manso et al., 2021).
We are inspired by the efforts of those that are seeking to bring horticultural therapy and traditional knowledge back into hospitals (Viray, 2018). Our interviews revealed a plethora of qualitative evidence that visitors are utilizing hospital ecoroofs. Future work should continue to document these ecoroof resources not only at the site scale but also regionally and nationally.
We are also humbled by the barriers that exist to provisioning this therapy, not the least of which is cost. Davis (2011) suggest that including horticultural therapy on insurance coverage could be a step to remedy this, and we agree. Logistical challenges with respect to access, and even more importantly, lack of awareness and education about the hospital greenspaces, can also limit these spaces from being used to their maximum potential.
Lack of change in salivary cortisol of roof visitors was surprising. We acknowledge here that the short duration of our sampling period and low replication likely also affected our results. In future work, extending our sampling period should be able to easily increase participation. Although previous studies have seen differences in cortisol over short time periods (Park et al., 2007), a more recent review paper suggests that therapeutic effects on cortisol are more commonly recognized over longer time periods and these effects can be long-lasting (Antonelli and Barbieri, 2019). Ideally, future work would consider how much of a “dose” of ecoroof exposure is needed to elicit both short-term and long-term effects on cortisol levels.
The results from this pilot study provide some interesting directions for further study. The cortisol levels we measured overall were in the low range of clinically normal. Replication was low, but patients in our study were the oldest participants and had the highest cortisol levels overall (data not shown, n = 2); this was expected given the positive relationship between age and cortisol. Patients also showed the greatest decline in levels over time; perhaps the other visitors simply had less to gain from the experience. Higher initial cortisol levels in staff monitored outdoors compared to caretakers and staff indoors suggests they may be self-selecting a therapeutic location. More staff and caretakers surveyed outdoors reported being worried (p = 0.07) than staff surveyed indoors. Staff cortisol levels also increased during our study period. Antonelli and Barbieri (2019) suggest that cortisol can decrease in anticipation of a forest bathing experience; our data suggests the inverse might also be true.
Another explanation for our lack of therapeutic effect on ecoroof visitor salivary cortisol is that user experience could have affected our results (Stone and Roberts, 2020). Although the roof greenery where we tested includes large trees and a striking view into the Willamette Valley (Figure 2), there is also a lot of exposed concrete and high throughflow activity. Many visitors in our study, including more than half of the staff sampled outdoors, reported that they were there taking in the scenery, but our behavioral observations also indicated others, not in our study, checking their phones or eating.
Future work might further consider the psychological and potentially also physiological mechanisms via which time spent on hospital ecoroofs can facilitate the healing process in hospitals. The groundwork on design elements that are key in this process has already been set (Marcus and Sachs, 2014), and many of these could translate to the roof.
Our pilot study reveals numerous nuances to the practice of installing hospitals for the purpose of therapeutic benefits. We have only begun to elucidate the numerous social and ecological factors that dictate the installation, maintenance, and use of these systems. Likewise, much work is still needed to determine the ways in which ecoroofs could be implemented to achieve similar results to forest bathing or horticultural therapy gardens on the ground.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Portland State University and Oregon Health and Science University Institutional Review Boards. Written informed consent, or verbal consent in the case of the phone interviews, was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
OS is the primary organizer of the project; she organized the structure of the paper and was the main contributor to the intro, discussion, and results pertaining to cortisol analysis. TB is the co-PI on the project and contributed to project management and oversaw the construction of the interview questions. AT led the interview piece of the project and finalized the analysis of these data. BP-E conducted the logistic regression and managed the hospital data. TO and AV conducted phone interviews, behavioral observations, and helped with literature review. AV also assisted with project management and his undergraduate honors thesis provides the basis for some of the work included here. All authors contributed to the article and approved the submitted version.
This work comes from the National Institutes of Health Common Fund and Office of Scientific Workforce Diversity under the following awards: UL1GM118964, RL5GM118963, and TL4GM118965. AT was also supported by startup funds from OS which were matched by the Yale School of Forestry and Environmental Studies Carpenter-Sperry Fund.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
This support also enabled collaboration between the authors and Dr. Mary Samuels at OHSU, who facilitated the cortisol study. Kelsey Zionskowski and Brandon Labadie conducted the cortisol sampling and visitor surveys. Advice from leaders in horticultural therapy such as Dr. Naomi Sachs and Theresia Hazen, M.Ed., HTR, QMHP was invaluable. Additional student support on this project was provided by Mackenzie Grey, Jeremiah Graff, and Rosemary Wood.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frsc.2022.811306/full#supplementary-material
Antonelli, M., and Barbieri Donelli, D. (2019). Effects of forest bathing (shinrin-yoku) on levels of cortisol as a stress biomarker: a systematic review and meta-analysis. Int. J. Biometeorol. 63, 1117–1134. doi: 10.1007/s00484-019-01717-x
Barron, S., Nitoslawski, S., Wolf, K. S., Woo, A., Desautels, E., and Sheppard, S. R. J. (2019). Greening blocks: a conceptual typology of practical design interventions to integrate health and climate resilience co-benefits. Int. J. Environ. Res. Public Health 16:4241. doi: 10.3390/ijerph16214241
City of Portland (2008). Cost Benefit Analysis of Ecoroofs. Available online at: https://www.portlandoregon.gov/bes/article/261053
Cordoza, M., Ulrich, R. S., Manulik, B. J., Gardiner, S. K., Fitzpatrick, P. S., Hazen, T. M., et al. (2018). Impact of nurses taking daily work breaks in a hospital garden on burnout. Am. J. Crit. Care 27, 508–512. doi: 10.4037/ajcc2018131
Davis, B. E.. (2011). Rooftop hospital gardens for physical therapy: a post-occupancy evaluation. Health Environ. Res. Des. 4, 14–43. doi: 10.1177/193758671100400303
Dettweiler, U., Becker, C., Auestad, B. H., Simon, P., and Kirsch, P. (2017). Stress in School. Some empirical hints on the circadian cortisol rhythm of children in outdoor and indoor classes. Int. J. Environ. Res. Public. Health 14:475. doi: 10.3390/ijerph14050475
Dickerson, S. S., and Kemeny, M. E. (2004). Acute stressors and cortisol responses: a theoretical integration and synthesis of laboratory research. Psychol. Bull. 130, 355–391. doi: 10.1037/0033-2909.130.3.355
Gonzalez-Cabrera, J. M., Fernández-Prada, M., Concepción, I., Molina-Ruano, R., Salinero-Bachiller, M., and Peinado, J. M. (2018). Acute stress and anxiety in medical residents on the emergency department duty. Int. J. Environ. Res. Health 15:506. doi: 10.3390/ijerph15030506
Hartig, T., Evans, G. W., Jamner, L. D., Davis, D. S., and Gärling, T. (2003). Tracking restoration in natural and urban field settings. J. Environ. Psychol. 23, 109–123. doi: 10.1016/S0272-4944(02)00109-3
Kirschbaum, C., and Hellhammer, D. H. (1994). Salivary cortisol in psychoneuroendocrine research: Recent developments and applications. Psychoneuroendocrinology 19, 313–333. doi: 10.1016/0306-4530(94)90013-2
Lee, K., Williams, K. J. H., Sargent, L. D., Farrell, C., and Williams, N. S. (2014). Living roofpreference is influenced by plant characteristics and diversity. Landsc. Urban Plan. 122, 152–159 doi: 10.1016/j.landurbplan.2013.09.011
Lee, K. E., Williams, K. J., Sargent, L. D., Williams, N. S., and Johnson, K. A. (2015). 40-second green roof views sustain attention: the role of micro-breaks in attention restoration. J. Environ. Psychol. 42, 182–189. doi: 10.1016/j.jenvp.2015.04.003
Lee, M.-J.. (2010). Effects of various horticultural activities on the autonomic nervous system and cortisol response of mentally challenged adults. Horttechnology 20, 971–976. doi: 10.21273/HORTSCI.20.6.971
Malenbaum, S., Keefe, F. J., Williams, A. C., Ulrich, R., and Somers, T. J. (2008). Pain in its environmental context: implications for designing environments to enhance pain control. Pain 134, 241–244. doi: 10.1016/j.pain.2007.12.002
Manso, M., Teotonio, I., Silva, C. M., and Cruz, C. O. (2021). Green roof and green wall benefits and costs: a review of the quantitative evidence. Renewable Sustain. Energy Rev. 135:110111. doi: 10.1016/j.rser.2020.110111
Marcus, C. C., and Sachs, N. A. (2014). Therapeutic Landscapes: An evidence-Based Approach to Designing Healing Gardens and Restorative Outdoor Spaces. Hoboken, NJ: John Wiley and Sons.
Morgan, D.. (2014). Integrating Qualitative and Quantitative Methods: A Pragmatic Approach. Thousand Oaks, CA: Sage Publishing. doi: 10.4135/9781544304533
Olafsdottir, G., Cloke, P., Schulz, A., van Dyck, Z., Eysteinsson, T., Thorleifsdottir, B., et al. (2020). Health benefits of walking in nature: a randomized controlled study under conditions of real-life stress. Environ. Behav. 52, 248–274. doi: 10.1177/0013916518800798
Park, B. J., Tsunetsugu, Y., Kasetani, T., Hirano, H., Kagawa, T., Sato, M., et al. (2007). Physiological effects of shinrin-yoku (taking in the atmosphere of the forest)—using salivary cortisol and cerebral activity as indicators. J. Physiol. Anthropol. 26, 123–128. doi: 10.2114/jpa2.26.123
Park, B. J., Tsunetsugu, Y., Kasetani, T., Kagawa, T., and Miyazaki, Y. (2010). The physiological effects of Shinrin-yoku (taking in the forest atmosphere or forest bathing): evidence from field experiments in 24 forests across Japan. Environ. Health Prev. Med. 15, 18–26. doi: 10.1007/s12199-009-0086-9
Park, S. H., and Mattson, R. H. (2008). Effects of flowering and foliage plants in hospital rooms onpatients recovering from abdominal surgery. Horttechnology 18, 563–568. doi: 10.21273/HORTTECH.18.4.563
Roe, J. J., Thompson, C. W., Aspinall, P. A., Brewer, M. J., Duff, E. I., Miller, D., et al. (2013). Green space and stress: evidence from cortisol measures in deprivedurban communities. Int. J. Environ. Res. Public Health. 10, 4086–4103. doi: 10.3390/ijerph10094086
Seltzer, M. M., Greenberg, J. S., Hong, J., Smith, L. E., Almeida, D. M., Coe, C., et al. (2010). Maternal cortisol levels and behavior problems in adolescents and adults with ASD. J. Autism. Dev. Disord. 40, 457–469. doi: 10.1007/s10803-009-0887-0
Shepley, M. M., Peditto, K., Sachs, N. A., Pham, Y., Barankevich, R., Crouppen, G., et al. (2020). Staff and resident perceptions of mental and behavioural health environments. Build. Res. Inf. 50, 89–104. doi: 10.1080/09613218.2021.1963653
Souter-Brown, G., Hinckson, E., and Duncan, S. (2021). Effects of a sensory garden on workplace wellbeing: a randomised control trial. Landsc. Urban Plan. 207:103997. doi: 10.1016/j.landurbplan.2020.103997
Spielberger, C. D., Gorsuch, R. L., Lushene, R., Vagg, P. R., and Jacobs, G. A. (1983). Manual for the State-Trait Anxiety Inventory. Palo Alto, CA: Consulting Psychologists Press.
Stone, E. A., and Roberts, J. D. (2020). Park spaces and the user experience reconsidering the body in park analysis tools. Nat. Cult. 15, 123–133. doi: 10.3167/nc.2020.150201
The American Horticultural Therapy Association (2022). Definitions and Positions. Available online at: https://www.ahta.org/ahta-definitions-and-positions/ (accessed March 23, 2022).
The Therapeutic Landscapes Network (2022). History. Available online at: https://healinglandscapes.org/about/history/ (accessed March 23, 2022)
Thompson, C. W., Aspinall, P., and Roe, J. (2014). Access to green space in disadvantaged urban communities: evidence of salutogenic effects based on biomarker and self-report measures of wellbeing. Procedia Soc. Behav. Sci. 153, 10–22. doi: 10.1016/j.sbspro.2014.10.036
Triguero-Mas, M., Gidlow, C. J., Martínez, D., de Bont, J., Carrasco-Turigas, G., Martínez-Íñiguez, T., et al. (2017). The effect of randomised exposure to different types of natural outdoor environments compared to exposure to an urban environment on people with indications of psychological distress in Catalonia. PLoS ONE 12:e0172200. doi: 10.1371/journal.pone.0172200
Ulrich, R. S.. (1979). Visual landscapes and psychological well-being. Landsc. Res. 4, 17–23. doi: 10.1080/01426397908705892
Ulrich, R. S., Zimring, C., Zhu, X., DuBose, J., Seo, H. B., Choi, Y. S., et al. (2008). A review of the research literature on evidence-based healthcare design. HERD 1, 61–125. doi: 10.1177/193758670800100306
Vander Poel, K., and Griffin, C. (2017). “Aligning the design intent with the actual use of ahealing garden in a pediatric hospital,” in Proceedings of the AARC (Architectural Researchcenters Consortium) Conference, Salt Lake City, UT.
Viray, A.. (2018). Current and Potential Uses of Greenroofs on Hospitals. Undergraduate Honors Thesis, Portland State University.
Wolf, K. L., Lam, S. T., McKeen, J. K., Richardson, G. R., van den Bosch, M., and Bardekjian, A. C. (2020). Urban trees and human health: a scoping review. Int. J. Environ. Res. Public Health 17:4371. doi: 10.3390/ijerph17124371
Keywords: ecoroof, therapeutic, landscape, hospital, greenspace
Citation: Starry O, Viray A, Park-Egan B, Terway AC, Oxendahl T and Burdsall T (2022) A Pilot Study Considering Ecoroofs as Therapeutic Landscapes. Front. Sustain. Cities 4:811306. doi: 10.3389/frsc.2022.811306
Received: 08 November 2021; Accepted: 24 May 2022;
Published: 19 July 2022.
Edited by:
Jason M. Aloisio, Independent researcher, New York City, United StatesReviewed by:
Michelle Kondo, US Forest Service Research and Development, United StatesCopyright © 2022 Starry, Viray, Park-Egan, Terway, Oxendahl and Burdsall. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Olyssa Starry, b3N0YXJyeUBwZHguZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.