 Paolo Bellavista
Paolo Bellavista Marco Torello
Marco Torello Antonio Corradi
Antonio Corradi Luca Foschini
Luca Foschini- Dipartimento di Informatica - Scienza e Ingegneria (DISI), University of Bologna, Bologna, Italy
The recent COVID-19 pandemic in Italy has highlighted several critical issues in the management process of infected people. At the health level, the management of the COVID-19 positive was mainly delegated to the regional authorities and centrally monitored by the State. Despite requested common activities (such as diagnosis of virus positivity, active surveillance of infected people and contact tracing), Regional Health Departments were able to issue specific directives in their territories and establish priority levels for each activity according to the specific needs related to the emergency in their area. The development of novel digital tools for the management of infected people become an urgent necessity to foster more organized and integrated solutions, able to quickly process large amounts of data. Mobile Crowdsensing methodologies could effectively facilitate needed lateral interviewing activities as well as the monitoring of crowds in environments with a high concentration of virus-positive subjects (such are hospital wards but also other locations), facilitating the tracing of possible outbreaks of contagion due to advanced geolocation techniques and big data analysis methods. This paper analyzes the functionality of SWAPS (Supporting Workflows for Healthcare Personnel management), a modular and scalable web platform which facilitate and reduces the management time of COVID positive health personnel within healthcare facilities. It also analyzes the possible integrations between SWAPS and ParticipACT, an advanced MCS platform developed by the University of Bologna that can help set up the alert notification in case of entry into a COVID risk area. This article surveys the current literature on software platforms to address COVID-19 and related tracing issues and presents the practical issues and on-the-field results obtained from the research developed by the University of Bologna by assisting the deployment of the proposed solution for a big Regional Health Department in the city of Bologna.
Introduction
Italy was the first European country to face the COVID emergency in a massive proportion and the national health care system, known as Servizio Sanitario Nazionale (SSN) was unfit to face the huge amounts of requests admissions into intensive care units. According to WHO, the first case was identified on January 20, 2020, and on May 28, the observed case was 231.139 with 33,072 casualties reported nationally (WHO, 2020). The lack of specific medical tests (such as swabs) needed to identify the virus and the lack of specific treatment protocols to alleviate the severity of symptoms contributed to overwhelm the intensive care units.
To contain the spread of the virus and to ease the pressure on the SSN, the government has imposed restrictions on the mobility of individuals, prohibiting gatherings and closing non-essential services. The lockdown forced people to change daily habits pushing them to switch to online services for learning, smart working, and leisure, generating an unprecedented load on the Internet. Since 11 March, Italy faced a total lockdown, with 80–90% of people forced home, with relevant social consequences under a psychological point of view and with negative impacts on the national economy (Tropea and De Rango, 2020). Nevertheless, the measures imposed by the government significantly reduced the spread of the virus between July and September, with a relative relaxation of restrictive measures and a progressive return to a regular lifestyle. Despite those efforts, on October 31, 2020, the active cases of COVID positive reached the considerable number of 351.386, while as of 15 October was only 37,512 since January 2020 (Figure 1).
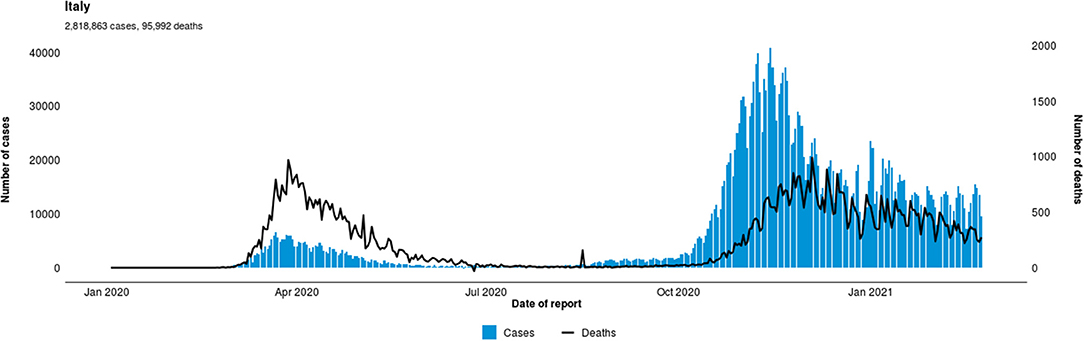
Figure 1. Situation by Country, Territory, and area sources (WHO 2020).
Between June and October, the number of cases stabilized at 20-30 units per day against the hundreds of cases daily detected during the so-called “first wave”. A new outbreak of the virus has been underway since October 2020. Total cases went from 314,861 (October 1) to 679,430 (November 1) the trend is currently up (WHO, 2020).
In anticipation of a “second wave,” the government has promoted research projects at national and regional level to develop suitable technological solutions to counter the spread of the virus. Meanwhile, the government also independently implemented contact monitoring tools (Presidenza del Consiglio dei Ministri., 2020; Tropea and De Rango, 2020) such as “Immuni,” a non-mandatory smartphone application that leverage on Bluetooth Low Energy (BLE) technology (De Rosa, 2020). The choice of adopting BLE-based technologies instead GPS positioning was necessary due to stringent privacy requirements and data protection issues. Immuni uses a DP-3T model, acronym for Decentralized Privacy-Preserving Proximity Tracing, where data are stored directly on mobile devices to protect user's identity. The smartphones will send, receive, and store anonymous alphanumeric keys of the people met, while the server will only receive the strings sent by the phone of a positive patient when this indicates his positivity. The server forwards to the apps of all connected devices a key of the positive ones and, in case a match is found by the application, the system notifies the user the possibility of a risky contact (Tropea and De Rango, 2020). Despite the government effort, Immuni did not immediately receive a positive reception due people distrust the security in the management of personal data.
The management of COVID-19 (COVID+) infected healthcare personnel become crucial: as a possible carrier of contagion, healthcare staff are suspended from work, causing also serious consequences on the operational capabilities of the treatment centers. In this scenario, the management of infected healthcare personnel was supported by very heterogeneous and not integrated digital tools such as text documents and spreadsheets. The rapid choice of these tools was motivated to remedy to no integration of the entir process, before the pandemic. Having to operate in an emergency, the operators tried to make up for this lack without success. Moreover, because of different needs and requirements of the different hospitals, it was not possible to organize a homogeneous structure for needed data, by making extremely difficult a direct comparison between the information released by individual regional departments also due to the frequent errors in the data entry carried out manually by the operators and without any check on the correctness of the information.
In the following sections, we present a specific population particularly subject to virus exposure, the health staff and describe two applications related to the COVID emergency: SWAPS, a management platform for healthcare personnel affected by contagion and ParticipACT, an advanced crowdsensing platform based on cloud technology that can facilitate contact tracing and identify possible high-risk contagion areas.
Context
Health personnel are the most exposed subjects to the risk of contagion to COVID-19, with serious consequences on the stability of the national healthcare system because of the growing of hospitalized patients. As carrier of contagion, health personnel could easily contribute to spreading more the virus in hospitals, so increasing the risk of overexposure of already hospitalized patients with serious diseases with even lethal consequences. Moreover, the management of infected medical personnel has proved to be a crucial element for maintaining the full operation of the health system and reduce infection rate and deaths.
During the first wave, management of COVID+ was centrally monitored by the State but mainly delegated to regional authorities and regional health departments, due to the different levels of contagion among the Italian regions. The Italian national health care system is a regionally based health service. While the national level ensures the general objectives and fundamental principles of the whole health care system, regional governments in Italy are responsible for ensuring the delivering of all health services and benefits to the population. It happens the health care facilities can vary in quality in different regions of Italy.
Although some common activities have been centrally standardized (such as diagnosis of virus positivity, active surveillance of infected people and contact tracing), Regional Health Departments issue-specific local directives in their territories to establish priority levels for each activity according to the contingency needs. In particular, the management of infected health personnel was mainly based on a set of specific procedures designed to minimize the risk of spreading the infection and respecting the local requirements and organizations.
The process includes a series of activities identified by the top management of the national healthcare system:
• Management of positive operators: it provides for the request for home isolation or hospitalization; the preparation of administrative documents for suspension from work and an initial screening of contacts to identify other infected subjects.
• Swab management: it is the exclusive task of the Occupational Medicine department to plan the execution of swabs using a dedicated agenda updated daily.
• Management of serologies. It consists of mass screening of healthcare professionals through a rapid blood test for anti-Coronavirus antibodies. In case of positivity, the Operators are suspended, and the buffer is programmed to confirm the diagnosis.
Nevertheless, it was impossible to develop a homogeneous and functional data collection system at a correct technological level: each local health department has developed its data collection methodologies, based on common technologies available (text documents, spreadsheets, etc.) without any agreement on adequate data structuring methodology between the different authorities involved. This caused a slowdown in data at general level) and an increasing delay in reporting COVID-positive medical personnel, facilitating the spread of the virus in hospital wards.
It should be noted that each of these activities could be carried out independently of the others, although with the obligation to progressively notify their progress.
According to data provided by Sant'Orsola-Malpighi hospital—one of the big health centers in Emilia-Romagna region with over 8.000 employees—the communication between activities is based on tools inadequate to guarantee satisfactory results: the actors of the process (health professionals) submit reports of their tasks either on spreadsheets or via shared text files. Often a data must also be reported on two separate spreadsheets, with a consequent waste of time with no control over any typing errors or omissions in the double data entry. The used sharing software tools do not guarantee against errors resulting from data overwriting due to concurrent access by multiple users to the same information. Since the process information is distributed in multiple documents, the manual data crossing operations are quite onerous. Moreover, some bureaucratic procedures are still being processed only via paper documents. Finally, some routine activities (i.e., sending emails) contribute to waste lot of useful time of operators and medical center administrative staff.
The development of digital tools for the management of infected healthcare personnel become an urgent necessity to foster more organized and integrated solutions, able to process huge amount of heterogeneous information, especially in anticipation of a second wave. As highlighted in previous analysis on the pandemic emergency in Spain (Cano et al., 2020), smart city technologies and Mobile Crowdsensing methodologies represent a good alternative to ensure the success of quarantine periods, providing innovative approaches that could be able to reduce the negative impact both on the economy and on the population.
Details
Swaps
SWAPS (Supporting Workflows for Healthcare Personnel management) is a research project developed by University of Bologna and funded by POR-FESR Emilia-Romagna 2014–2020 with specific call related to COVID-19 emergency in June 2020. The main objective of the project is the automation of the procedure for the management of infections in healthcare personnel adopted by the Sant'Orsola-Malpighi Hospital.
The procedures requires that any health operator recognized positive in a diagnostic swab for SARS-CoV-2 RNA is suspended from the job and, depending on the severity of the infected person's condition, either quarantined in his home or hospitalized.
In the event of symptoms, a healthcare professional is required to report to the appropriate department (by phone or email). The department then proceeds to book the diagnostic swab and prepare the necessary documents for temporary suspension from work. This procedure currently requires manual interaction between different spreadsheets and databases: the management of the infected subject, tested in a protected environment, requires an average of 5:32 min per case. Timing that increases significantly (up to 10 times) in an unprotected environment, effectively slowing down the entire process.
The need of developing tools capable of promoting data aggregation while, at the same time, facilitating the management of workflows of infected personal has prompted the University of Bologna, with the collaboration of Policlinico Sant'Orsola-Malpighi to design and develop SWAPS (Figure 2).
SWAPS provide the following services:
- Sequencing and synchronization of process activities. All formal steps part of the contagion management procedures, as well as their sequencing, will be coded within one application that is also be responsible out of a centralized and automated coordination of all activities and govern their progress within the required time frame.
- Supervision of data entry. Each user will be required to perform her duties according to the timing required by the application. The user will be able to report on their activities (reporting) through available online preset forms and tools that will help them in entering data and in the notification tasks.
- Data collection and integration. The data collected during the reporting phase will be appropriately stored and integrated into a single database that will support the operation of the entire process and will provide the input for all analytical investigations aimed at assessing the effectiveness and efficiency of the process.
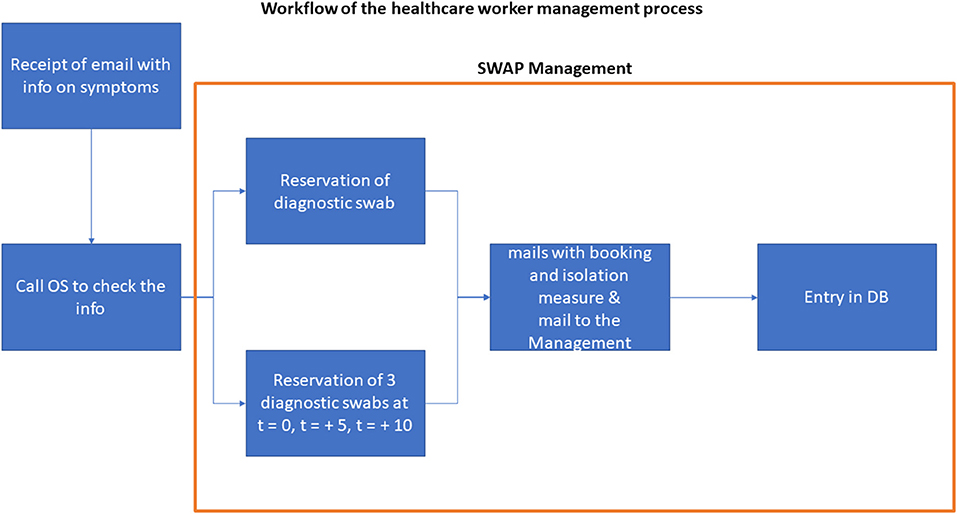
Figure 2. Workflow of the healthcare worker management process with SWAPS.
SWAPS adopt tools and techniques typical of the Business Process Management (BPM) methodology. The BPM methodology includes five work phases that follow one another according to the following circular scheme: design, modeling, execution, monitoring, and optimization. A process-oriented methodological approach aims to continuously improve the process by monitoring its performance and remodeling interventions to aligning the process with the desired performance. Furthermore, such approach promotes and favors interventions to recalibrate the process, should the project requirements and objectives differ from the initial ones. The software application of SWAPS is process-based and inherit the advantages deriving from the adoption of the BPM methodology. In particular:
a) The application will lend itself to fine-tuning interventions of processes aimed at improving its performance even after its release.
b) The application can be easily adapted to accommodate the requirements and objectives of any other subjects who wish to adopt it to manage the contagion control of their workforce (e.g., other territorial Occupational Medicines, nursing homes, law enforcement agencies, etc.)
These peculiar characteristics make the application stand out from the classic “special-purpose” solutions, whose degree of flexibility and adaptation to new operating contexts is much lower.
From an architectural point of view, the application will follow the classic approach of Web-based applications at three logical levels:
• Front End. It represents the level of interfacing with the user being responsible for the production of the so-called user views, that is, all the web pages that offer the user the way to interact with the application and activate her functions.
• Back End. This is the level where the business logic of the application resides, and it communicates both with the Front End and with the Database to ensure the correct logical functioning of the application on the one hand and the consistency of the application status on the other.
• Database. It is the level that permanently maintains the data and the state of the application.
• As for implementation, AGILE development methodologies are adopted with short and frequent software release cycles. As for the technologies and tools useful for development, the following choices are envisaged: for the Front End, the choice will fall on Html 5 with Bootstrap and JQuery support; the development of the Back End will be based on the Java 8 EE, together with Tomcat, Spring boot and Spring MVC, while Oracle 11g XE was used for the implementation of the Database.
Semi-finished products are used which offer a ready-to-use solution for infrastructural aspects: the application artifact can be easily docked; Basic navigation: filters, CRUD operations, extractions in Xls; Security ensured through profiling, user management, profile management and related qualifications. Through the proposed architecture it is possible to build a completely modular system, that can manage different compartments in a completely independent way. In this way, if the organizational procedures should change, eliminating or adding specific procedures, the entire system will not require any software intervention and will be able to continue to operate efficiently.
The solutions provided with SWAPS facilitate the process management by reducing workload for each operator and the average management time. Performance tests conducted on a sample of over thirty cases have shown a significant reduction in the management times of symptomatic operators with a reduction of 1:37 min compared to the condition in a protected environment. In general, both in a protected and unprotected environment, the management process is stable over a time frame of 3:55 min.
The serological management process, i.e., the booking of rapid antigen tests to allow the health worker to reintegrate in the workplace, shows a greater variance: in a protected environment the management of 15 positive cases takes about 5:43 min while with SWAPS timing drops to 1:16 min. The data were obtained by comparing the performance with and without SWAPS of the operators of Unità Operativa di Medicina del Lavoro of Sant'Orsola-Malpighi Polyclinic which is the department in charge of handling reports on infected cases within hospital staff (Figure 3).
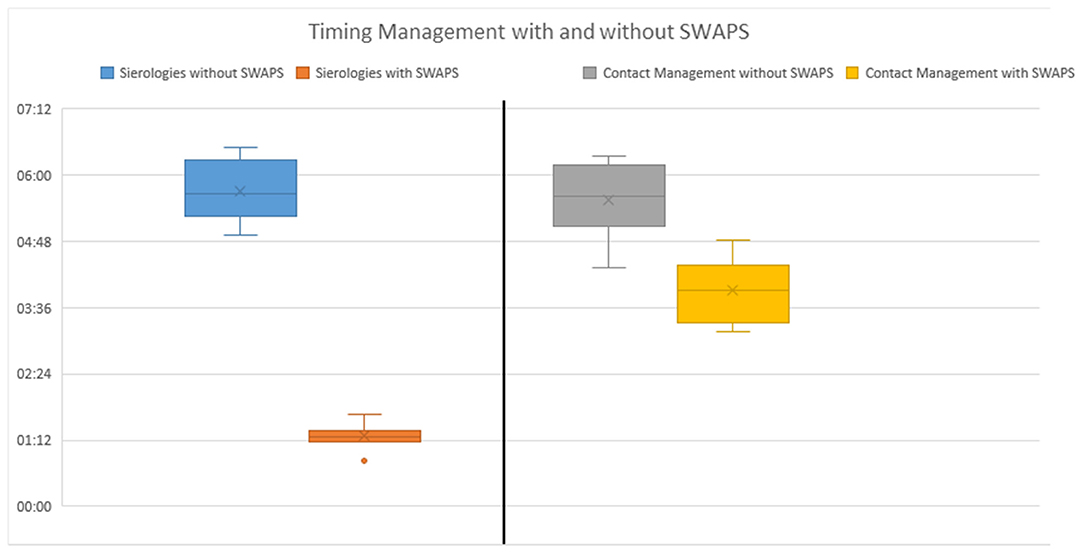
Figure 3. Timing management with and without SWAPS.
Obviously, during the implementation stage, some features have been given priority over others due to the need to implement the prototype as soon as possible and start field tests. SWAPS is currently used successfully within the Sant'Orsola-Malpighi Hospital and the platform ensures management of over 8.000 healthcare personnel through management of COVID-19 pathologies, booking exams and active surveillance of the course of the disease as well as an automated contact tracing system capable of reporting possible cases at risk.
Let us conclude reporting some considerations on SWAPS main pros and cons. SWAPS presents as its main advantages the intuitive Graphical User Interface (GUI) that eases the data entry process as well as the monitoring of the current epidemic situation. Moreover, SWAPS is designed as a fully customizable modular structure, capable of adding or deleting specific functions for future new diagnostic methodologies and this feature makes the platform usable also for epidemiological phenomena other than COVID-19. At the same time, SWAPS still has some limitations, especially for what concerns its management. For examples, although the application is cloud-ready and deployable as a container-based application, at the current stage it was not necessary to replicate the core parts for the sake of scalability issues. Hence, the fine tuning for large deployments is part of the ongoing efforts on application management and operations, and the execution of wider tests on scalability performances.
Participact
Mobile Crowdsensing (MCS) methodologies represent a precious opportunity to quickly identify possible risks even in a limited location (Capponi et al., 2019). Thanks to 4G and GPS technologies, it is possible to delimit a risk area even within a small hospital and the possibilities increase exponentially with 5G technology. Crowdsensing solutions enable large-scale data collection, from collaborative actions through mobile devices such as smartphones (Cano et al., 2020) and in the event of an epidemic it can be very effective for delimiting areas subject to high density of individuals, helping decision makers to design alternative solutions (diverting traffic, limiting the openings of commercial structures and so on). This use of a participatory tool involves the population in collecting information that aims to improve people quality of life (Guo et al., 2015; Bellavista et al., 2018, 2020; Belli et al., 2018) and leverages on the willingness of individuals to actively participate in a data collection through a mobile application, joining campaigns or tasks defined by the MCS administrator (Bellavista et al., 2015).
MCS can be enabled with two different approaches: opportunistic and participatory. Opportunistic sensing scenario involves users carrying mobile devices with applications running in the background, continuously collect sensors readings such as GPS, accelerometers and so on depending on administrators' strategies (Marjanović et al., 2018). Participatory sensing requires active involvement of users: the admin can start a campaign to define the tasks to be performed while the user must enable sensors readings on a specific target such as to take a picture in a specific place or to answer to a questionary. In the unlikely event of a pandemic emergency, the authorities may be forced toward opportunistic sensing methodologies to identify risk areas and put in place restrictive measures to contain the virus. However, it is necessary to stress that even opportunistic crowdsensing could not be effective if user smartphones are not using active support for MCS applications and, therefore, the success depends on the level of civic awareness (Bellavista et al., 2020).
The University of Bologna worked on several versions of ParticipACT, a crowdsensing application already extensively tested in the field in different conditions such as urban traffic, accessibility for impaired people, quality of services offered to the public (Bellavista et al., 2020).
ParticipACT is a socio/technical-aware crowdsensing platform to investigate in a real-world scenario the social and technical issues of crowdsensing (Cardone et al., 2016b) and was successful integrated into several different contexts, both in Italy (specifically Bologna) and Brazil (in the State of Santa Catarina). Main contexts include urban traffic and urban mobility issues (Buosi et al., 2018), impaired mobility (Cortellazzi et al., 2016), smart cities management (Gomes et al., 2016) and even social network analysis (Gomes et al., 2018).
The platform perfectly follows all the guidelines of a good crowdsensing system:
• The client application in dealing with users and with data gathering operations has a very low footprint on its user's device, in terms of resource consumption and of user's actions needed to collect data, employing a high-performance sensing module called MoST (Cardone et al., 2016a) (Figure 4).
• The server component follows the openness paradigm, and it thus results easily extensible and transparent. Furthermore, the collected data can be shared with other trusted players, such as other crowdsensing platforms and trusted entities of the smart city.
• The system also assures security and privacy of its users. Integrity and confidentiality are guaranteed through the usage of mechanisms for authentication and secure storage of collected data.
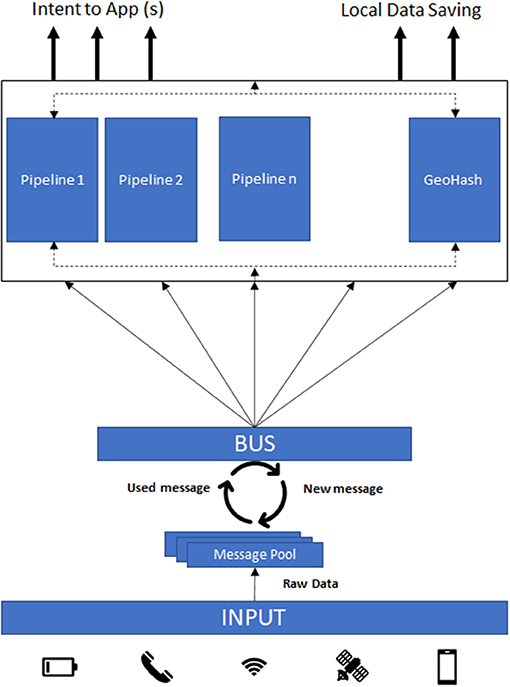
Figure 4. MoST architecture.
The server is accessible only by authorized entities, such as administrators and researchers, that can define which actions a user has to complete to carry out a so-called campaign. A campaign is a collection of tasks, that a user must accomplish to collect data and send its contribution to the server. Researchers can customize campaigns choosing tasks to be completed by a selected group of users, a geofence zone of activation and/or completion, and a time frame in which the actions must be completed.
A recent investigation focuses on possible exploitation of GeoHash Notification API provided by Google and Apple on coronavirus to monitor the COVID-19 risk in areas of varying size. GeoHASH was successfully integrated within MoST (Figure 4) to facilitate further integrations. GeoHash allows the monitoring of areas in any proportion, from entire cities to medium-size neighborhoods, down to even rooms. This feature allows you to start a specific geo-localized campaign with ParticipACT, and to prepare a notification that signals the user that he has entered a high-density area, to make him aware of the risk of contracting a specific pathology (in this case COVID).
Discussion
As highlighted, both SWAPS and ParticipACT share a very similar architecture which facilitates an integration process we are currently working on. While there are no impediments for this integration at the architecture level, we must point out that there are other problems that can spoil or slow down the process. The first is mainly bureaucratic dynamic requirements: the COVID+ management methodologies constantly evolve, depending on the levels of emergency and political-health decisions which may change the requirements for the suspension or reintegration of health personnel in the workplace. To overcome these dynamicity problems, SWAPS has been designed to have a modular and customizable structure. However, it is complicated to foresee new forms of control (new methodologies for swabs, serological, ultrasound scans, etc.) and this requires continuous addition of new features.
Another problem concerns the management of personal data. SWAPS and ParticipACT use different data structures: while the former mainly concern health data with a high level of protection, and structured data according to the involved personnel (doctors, nurses, health workers, administrative staff, etc.), the latter are structured to guarantee a certain level of data pseudonymization, while guaranteeing the user to be able to identify himself through specific usernames. In addition to the various infrastructures necessary for the storage and ownership of the data, it is necessary to point out that, to comply with the General Data Protection Regulation issued by European Union, it is not possible to directly connect a SWAPS user to a ParticipACT user.
The integration of the two applications will bring benefits to two very different types of users: while SWAPS will improve the management process of infected health workers within hospitals, ParticipACT is able to detect and notify possible risk areas (even limited to individual buildings) in which to identify possible subjects affected by contagion and concentrate efforts to identify possible infected. The combination of these two characteristics can guarantee a faster management of cases of infection and less clogging of hospital structures.
However, SWAPS is able to collect all the data on the infected personal, including the hospital departments in which they operate. This information, adequately pseudomized, is ready to be shared with ParticipACT, which, by processing the data, builds areas (also inside hospitals) where the risk of contagion can be considered high. This feature allows ParticipACT server to activate a specific task on the ParticipACT app that automatically notifies users to avoid entering the risk zone within the hospital (Figure 5).
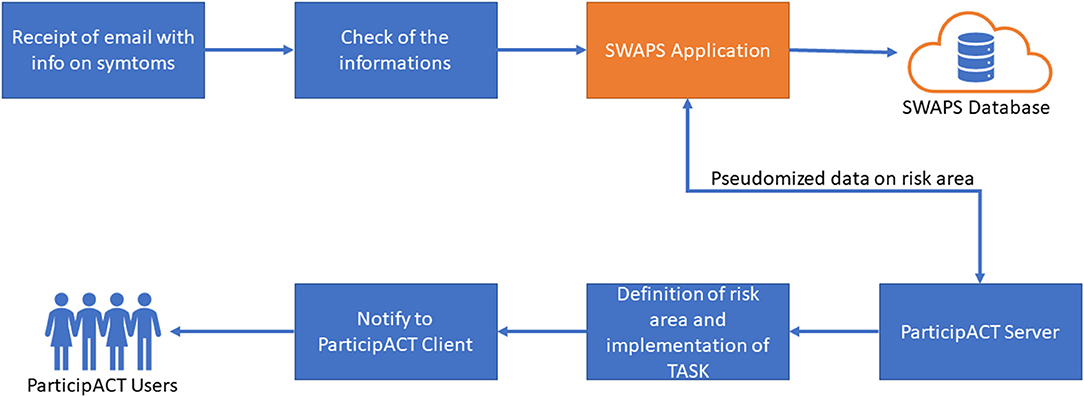
Figure 5. Workflow of SWAPS/ParticipACT integration.
The research group will broaden the research toward increasingly innovative solutions along interdisciplinary lines that also consider the psychological component of the epidemiological phenomenon.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Author Contributions
MT contributed to the writing and composition part of the paper. AC and PB for the part relating to ParticipACT. LF for the part relating to SWAPS. This work was performed equally among all authors.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We want to thank the administrative staff of Policlinico Sant'Orsola-Malpighi for their support in the development of SWAPS. Moreover, this article takes up much of the previous studies on issues related to MCS and the development of innovative solutions for smart cities, without which it would not be possible to develop the innovative management and monitoring systems.
References
Bellavista, P., Cardone, G., Corradi, A., Foschini, L., and Iannello, R. (2015). “Crowdsensing in smart cities: technical challenges, open issues, and emerging solution guidelines,” in Handbook of Research on Social, Economic, and Environmental Sustainability in the Development of Smart Cities, eds A. Vesco and F. Ferrero (IGI Global), 23. doi: 10.4018/978-1-4666-8282-5.ch015
Bellavista, P., Corradi, A., Foschini, L., Gomez, H. E., Lamberti, E., Klein, G., et al. (2020). “Virtual environments as enablers of civic awareness and engagement,” in International Journal of Urban Planning and Smart Cities, 22–34. doi: 10.4018/IJUPSC.2020010102
Bellavista, P., Corradi, A., Foschini, L., Noor, A., and Zanni, A. (2018). “Participact for smart and connected communities: exploiting social networks with profile extension in crowdsensing systems,” in The Workshop Program of the 19th International Conference. doi: 10.1145/3170521.3170526
Belli, D., Chessa, S., Foschini, L., and Girolami, M. (2018). “A social-based approach to mobile edge computing,” in IEEE Symposium on Computers and Communications, 292–297. doi: 10.1109/ISCC.2018.8538763
Buosi, M., Cilloni, M., Corradi, A., De Rolt, C., da Silva Dias, L., Foschini, L., et al. (2018). “A crowdsensing campaign and data analytics for assisting urban mobility pattern determination,” in IEEE Symposium on Computers and Communications, 224–229. doi: 10.1109/ISCC.2018.8538483
Cano, J. C., Cecilia, J. M., Hernandez-Orallo, E., Calafate, C. T., and Manzoni, P. (2020). Mobile crowdsensing approaches to address the COVID-19 pandemic in Spain. IET Smart Cities 2, 58–63. doi: 10.1049/iet-smc.2020.0037
Capponi, A., Fiandrino, C., Kantarci, B., Foschini, L., Kliazovich, D., and Bouvry, P. (2019). A survey on mobile crowdsensing systems: challenges, solutions, and opportunities. IEEE Commun. Surv. Tutor. 21, 2419–2465. doi: 10.1109/COMST.2019.2914030
Cardone, G., Cirri, A., Corrad, A., Foschini, L., and Montanari, R. (2016a). “Activity recognition for smart city scenarios: Google play services vs. most facilities,” in 2014 IEEE Symposium on Computers and Communications (ISCC), 1–6. doi: 10.1109/ISCC.2014.6912458
Cardone, G., Corradi, A., Foschini, L., and Raffaele, I. (2016b). ParticipAct: a large-scale crowdsensing platform. IEEE Trans. Emerg. Topics Comp. 4, 21–32. doi: 10.1109/TETC.2015.2433835
Cortellazzi, J., Luca, F., De Rolt, C., Corradi, A., Alperstedt Neto, C. A., and Alperstedt, G. A. (2016). “Crowdsensing and proximity services for impaired mobility,” in IEEE Symposium on Computers and Communication, 44–49. doi: 10.1109/ISCC.2016.7543712
De Rosa, P. (2020). Immuni Documentation. Available online at: https://github.com/immuni-app/immuni-documentation (accessed October 30, 2020).
Gomes, E., Dantas, M., de Macedo, D. J., De Rolt, C., Brocardo, M. L., and Foschini, L. (2016). “Towards an infrastructure to support big data for a smart city project,” in IEEE 25th International Conference on Enabling Technologies: Infrastructure for Collaborative Enterprises, 107–112. doi: 10.1109/WETICE.2016.31
Gomes, E., Penz, D., Gomes, V. E., De Rolt, R., and Dantas, M. (2018). “Evaluating the tools to analyze the data from the ParticipACT Brazil Project: a test with Elasticseach Tools Ecosystem with Twitter data,” in IEEE Symposium on Computers and Communications, 1286–1291. doi: 10.1109/ISCC.2018.8538622
Guo, B., Wang, Z., Zhiwen, Y., Yu, W., Yen, N. Y., Huang, R., et al. (2015). Mobile crowd sensing and computing: the review of an emerging human-powered sensing paradigm. ACM Comput. Surv. 48, 1–31. doi: 10.1145/2818183
Marjanović, M., Antonić, A., and Žarko, I. P. (2018). Edge computing architecture for mobile crowdsensing. IEEE Access 6, 10662–10674. doi: 10.1109/ACCESS.2018.2799707
Presidenza del Consiglio dei Ministri. (2020). Immuni. Available online at: https://www.immuni.italia.it/ (accessed November 10, 2020).
Tropea, M., and De Rango, F. (2020). COVID-19 in Italy: current state, impact and ICT-based solutions. IET Smart Cities 2:52. doi: 10.1049/iet-smc.2020.0052
WHO. (2020). World Health Organization, Coronavirus Disease (COVID-19) Dashboard. Available online at: https://covid19.who.int/table (accessed November 17, 2020).
Keywords: COVID-19, digital transformation, wearable IOT sensors, contact tracing, urban technologies, mobile crowdsensing, mobile crowdsensing
Citation: Bellavista P, Torello M, Corradi A and Foschini L (2021) Smart Management of Healthcare Professionals Involved in COVID-19 Contrast With SWAPS. Front. Sustain. Cities 3:638743. doi: 10.3389/frsc.2021.638743
Received: 07 December 2020; Accepted: 02 July 2021;
Published: 05 August 2021.
Edited by:
Somayeh Mohammady, Technological University Dublin, IrelandReviewed by:
Longbiao Chen, Xiamen University, ChinaMuhammad Asif, Islamia University, Pakistan
Hafiz Abdul Sattar Hashmi, Islamia University Bahawalpur, Pakistan, in collaboration With reviewer MA
Copyright © 2021 Bellavista, Torello, Corradi and Foschini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marco Torello, bWFyY28udG9yZWxsb0B1bmliby5pdA==