 Kristin E. Goodsell
Kristin E. Goodsell Alice J. Tao
Alice J. Tao James O. Park
James O. Park
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Surg., 06 March 2025
Sec. Surgical Oncology
Volume 12 - 2025 | https://doi.org/10.3389/fsurg.2025.1531852
This article is part of the Research TopicExtending the Limit of Liver Cancer Treatment with Surgical OptionsView all 5 articles
Hepatocellular carcinoma (HCC) is increasing in prevalence globally, and cure remains limited with non-operative treatment. Surgical intervention, through resection or transplantation, offers a potential for cure for select patients. However, many patients present with advanced or unresectable disease, and recurrence rates remain high. Recent advances in systemic therapies, particularly immune checkpoint inhibitors, have demonstrated promise in treating unresectable HCC and as adjuvant therapy. Evidence from adjuvant trials highlights the synergistic potential of combined liver-directed and systemic therapies. These findings have ignited growing interest in neoadjuvant therapy across various scenarios: (1) as a bridging strategy while awaiting transplantation, (2) for downstaging disease to enable transplantation, (3) for converting unresectable disease to a resectable state, or (4) as neoadjuvant treatment in operable cases. Early-stage trials of neoadjuvant therapy in resectable HCC have reported promising outcomes. To realize the potential of neoadjuvant treatment for HCC, thoughtfully designed, adequately powered, multi-center clinical trials are essential.
Liver cancer is the sixth most common cancer and the third leading cause of cancer-related death globally (1). Hepatocellular carcinoma (HCC), the most prevalent primary liver cancer, typically arises in patients with chronic viral infections, alcohol-related cirrhosis, or metabolic dysfunction associated steatohepatitis. Current treatments prioritize resection or ablation for early-stage disease and transplantation in suitable candidates, with liver-directed or systemic therapies reserved for more advanced disease (2). While surgical resection and transplantation offer potential curative options, overall mortality remains high due to late-stage presentation and frequent recurrence. Notably, the 5-year survival rate for HCC across all stages is approximately 20%, despite the availability of multimodal therapies (3).
The first systemic therapy for HCC, the tyrosine kinase inhibitor (TKI) sorafenib, demonstrated only modest improvement in disease progression and overall survival in advanced disease (4). Despite its limitations, sorafenib remained the only standard treatment until the advent of additional TKIs. However, as an immunogenic cancer, HCC holds great promise for immune-based therapies, such as immune checkpoint inhibitors (ICIs). Recently, the combination of anti-PD-L1 antibody atezolizumab and the VEGF inhibitor bevacizumab (atezo/bev) significantly improved outcomes in unresectable disease compared to sorafenib (5). As these novel therapies emerge as first-line systemic regimens for advanced disease, their potential application in adjuvant and neoadjuvant settings is anticipated.
In this review, we explore the rationale for neoadjuvant therapy in HCC, including its potential roles in bridging patients to transplantation, downstaging disease to enable transplantation, converting unresectable disease, and improving postoperative outcomes. We examine existing treatment modalities for HCC and the synergistic potential of strategic therapy combinations. Finally, we discuss the growing evidence supporting immune checkpoint inhibition in HCC, specifically focusing on promising data for its use in the neoadjuvant setting.
The surgical treatment of HCC includes tumor resection or liver transplantation for patients meeting criteria, historically defined by the Milan criteria (6). Neoadjuvant therapy is not currently part of standard treatment for any stage of disease; however, its application could address critical gaps in care (2, 7–9). Advances in systemic therapies highlight opportunities for neoadjuvant treatment to play a transformative role in the following scenarios: (1) bridging to transplantation, (2) downstaging disease to meet transplantation criteria, (3) converting unresectable disease, and (4) improving outcomes in resectable HCC.
Patients meeting transplant criteria remain at risk of disease progression while awaiting transplantation (10). Various bridging therapies have demonstrated efficacy in reducing waitlist dropout rates though outcomes have been inconsistent due to the lack of randomized controlled trials (10–19). A systematic review and meta-analysis suggested trends toward improved waitlist retention and post-transplant outcomes with bridging therapy (20). Future efforts should focus on integrating novel and emerging therapies into bridging protocols not only to mitigate waitlist dropout but also to enhance post-transplant survival.
For patients who exceed the Milan criteria for transplant, liver-directed therapies remain a cornerstone for attaining downstaging exception (21). While historically reliant on liver-directed approaches such as transarterial chemoembolization (TACE) or transarterial radioembolization (TARE), recent studies indicate promising outcomes with regimens incorporating ICIs and TKIs (22–24). These approaches not only improve transplant eligibility but may also enhance post-transplant survival, suggesting added therapeutic benefit beyond traditional liver-directed methods (11, 20, 22–30).
In other malignancies, such as colorectal liver metastases, neoadjuvant systemic therapies have achieved conversion rates up to 60% in phase II trials (31–34). Similarly, evidence suggests that a subset of patients with initially unresectable HCC may achieve conversion with combinations of systemic and liver-directed therapies including chemoradiation (35–38). Recent immunotherapy trials have demonstrated major pathologic responses in resectable HCC, supporting the potential for these strategies to expand the pool of patients eligible for curative surgery (39–41).
Recurrence rates following resection remain high, particularly in high-risk patients such as those with multinodular disease or portal vein tumor thrombus. A 2018 review reported 5-year survival rates for resected multinodular HCC at 35%, dropping to 23% for cases with more than three lesions (42). In other malignancies including pancreatic and colorectal cancer, neoadjuvant therapy is associated with improved outcomes, even for initially resectable disease (43, 44). For patients with HCC, there remains a clear need for improved neoadjuvant therapies for bridging, downstaging and converting disease and also for improving survival in surgical candidates by mitigating the risk of recurrence and metastasis.
Hepatocellular carcinoma presents significant challenges in the application of chemotherapy given its low sensitivity to chemotherapeutic agents and multiple mechanisms of chemoresistance (45–47). Single-agent treatments have consistently demonstrated negligible efficacy in HCC, with minimal response rates (47). Sorafenib, a small-molecule inhibitor and a standard systemic treatment for advanced HCC, extends median overall survival (OS) by only 2–3 months, with few partial responses and no complete responses (4, 30). Several mechanisms contribute to HCC's intrinsic “resistome,” enabling resistance to initial chemotherapeutic agents. These mechanisms include dysfunctional DNA repair, downregulation of apoptotic pathways, and the promotion of cancer stem cell survival (45). While combination therapies have demonstrated improved response rates, chemoresistance remains a significant barrier, as initial treatments can induce selective processes that exacerbate resistance, limiting the effectiveness of subsequent adjuvant therapy. Consequently, systemic chemotherapy plays a limited role as first-line treatment outside of advanced disease.
HCC arises commonly from background inflammation and chronic liver disease, which impairs tumor surveillance of the immune microenvironment, dysregulates immune checkpoint interactions, and abrogates T-cell response (48, 49). Overexpression of immune check point molecules programmed death 1 (PD-1), programmed death-ligand 1 (PD-L1), cytotoxic T lymphocyte-associated antigen-4 (CTLA-4) in HCC has been associated with higher recurrence rates, more aggressive disease, and poorer clinical prognosis (50, 51). Immunotherapy with immune checkpoint inhibitors (ICIs) aims to restore effective T-cell responses by targeting these dysregulated pathways.
However, as monotherapies, PD-1 inhibitors (e.g., pembrolizumab), PD-L1 inhibitors (e.g., atezolizumab), and CTLA-4 inhibitors (e.g., tremelimumab) have demonstrated only modest clinical efficacy in HCC (52–55). In the KEYNOTE-240 trial, patients with advanced HCC previously treated with sorafenib who were subsequently treated with either pembrolizumab or placebo had a median progression free survival (PFS) of 3.0 vs. 2.8 months and median OS of 13.9 months compared to 10.6 months (56). Limited efficacy of single-agent ICIs may be attributed to aberrant tumor angiogenesis, which creates a “tumor endothelial barrier” that hinders effective T-cell infiltration of tumor and dampens immune response (57, 58). To address these limitations, combination therapies incorporating agents that inhibit the VEGF pathway (e.g., bevacizumab) which promotes tumor angiogenesis, have been developed to enhance the activity of ICIs (e.g., atezolizumab) and demonstrated improved clinical response (5, 51, 59).
Adjuvant systemic or radiation therapy is a standard component of treatment for many gastrointestinal and hepatobiliary malignancies, including gastric, small bowel, and colon cancer as well as gallbladder cancers and cholangiocarcinoma. Standard adjuvant therapy has been lacking in HCC given historically limited evidence supporting itsefficacy. Other adjuvant therapies aimed to address underlying hepatitis, including vitamin K, cytokine-induced killer cells, and retinoids, have shown improved outcomes in select patients but failed to demonstrate benefits in recurrence free survival (RFS) or OS (2). Although retrospective studies suggested improved postoperative RFS with adjuvant sorafenib, the multi-center phase III STORM trial failed to support these findings (60). Sorafenib demonstrated no improvement over placebo with comparable RFS (33.3 vs. 33.7 months) and OS in patients following resection or ablation (61).
Phase III IMbrave 050 was a highly anticipated adjuvant trial that included patients undergoing resection or ablation with high risk of recurrence (62). Patients were randomized to 12 months of the combination of PD-L1 inhibitor atezo/bev vs. active surveillance. At the first interim analysis with median 17.4-month follow-up, the RFS was significantly better within the treatment vs. active surveillance group (HR 0.72). At the second interim analysis with median 35.1-month follow-up, the difference in RFS was not maintained (33 months for atezo/bev and 36 months for placebo (HR 0.9); therefore, this regimen is not recommended as adjuvant therapy for HCC (63).
However, numerous adjuvant ICI trials are currently underway. These include JUPITER-4 (NCT03859128), a phase II/III trial evaluating anti-PD-1 antibody toripalimab in high-risk patients following resection; KEYNOTE-937 (NCT03867084), a phase III trial of PD-1 inhibitor pembrolizumab vs. placebo in patients with complete radiologic response after resection or ablation; CheckMate 9DX (NCT03383458), a phase III trial investigating adjuvant anti-PD-1 monoclonal antibody nivolumab in high-risk patients; and EMERALD-2 (NCT03847428), a phase III trial examining the adjuvant combination PD-L1 monoclonal antibody durvalumab and bevacizumab compared to durvalumab alone or placebo (64–67).
Liver directed therapy is the cornerstone for managing locoregional or unresectable HCC and includes transarterial chemoembolization with or without drug eluting beads (TACE, TACE-DEB), transarterial radioembolization with yttrium-90 microbeads (TARE, Y90), radiofrequency or microwave ablation (RFA, MWA), hepatic artery infusion chemotherapy (HAIC), and external beam/stereotactic body radiation therapy (EBRT/SBRT). These treatments can be administered with curative intent for smaller lesions or used alone or in combination as bridging therapy, downstaging approaches, or for controlling unresectable disease.
Thermal ablation using RFA or MWA is the primary ablative therapy, while percutaneous ethanol injection (PEI) and cryoablation are less frequently used. Thermal ablation is indicated for accessible tumors with normal tissue margin and limited by proximity to critical structures such as blood vessels, bile ducts, or adjacent organs. For smaller lesions, ablation may be performed alone with curative intent, while intermediate or larger lesions may require combination therapy.
In a 2021 meta-analysis, RFA demonstrated comparable disease-free survival (DFS) and OS compared to resection in patients meeting Milan criteria (68). Similarly, the SURF trial found no significant difference in RFS between surgery and RFA for tumors up to 3 cm (69). Interestingly, a more recent meta-analysis indicated that while OS and RFS in tumors <3 cm or > 5 cm favored surgical resection, RFA and resection were equally effective for tumors 3–5 cm (70).
A 2020 proof of concept trial suggested synergistic benefits of RFA during anti-PD-1 therapy, demonstrating more than a two-fold increase in complete and partial response rates (71). This supports the hypothesis that liver-directed therapies may generate neo-antigens, enhancing the efficacy of immunotherapies.
TACE is a mainstay of treatment for intermediate-stage HCC and requires relative isolation of blood supply to vascularized tumor targets. Bland embolization (TAE) induces ischemia and tumor necrosis and has been shown to improve survival compared to supportive care (72). TACE builds on TAE by delivering concentrated chemotherapy in conjunction with inducing ischemia and has demonstrated superior outcomes relative to TAE in unresectable HCC (73). The addition of drug eluting beads (TACE-DEB) may further enhance response rates and has been associated with longer OS in subsets of patients (74, 75). TARE, using yttrium-90 microspheres, delivers tumor targeted radiotherapy and is employed primarily for unresectable HCC (75, 76). Evidence supports that TARE can serve a neoadjuvant role prior to transplant or resection with 3-year OS > 90% in patients undergoing transplant or resection (77).
HAIC delivers high concentrations of cytotoxic drugs directly to the liver while minimizing systemic side effects. While not a standard therapy, it is recommended in certain guidelines as an alternative treatment for advanced disease (78). In a phase III clinical trial, HAIC with FOLFOX demonstrated superior OS compared to sorafenib (13.9 vs. 8.2 months) in patients with locally advanced HCC (79). Downstaging occurred in 12.3% of patients and those that underwent resection achieved an OS of 20.8 months. Another phase III trial comparing FOLFOX-HAIC to TACE found improved OS (23.1 vs. 16.1 months), PFS (9.6 vs. 5.4 months), and response rate (46% vs. 18%) for HAIC (80). A 2024 meta-analysis further suggested that HAIC combined with ICIs or targeted therapies could yield synergistic effects and produce enhanced outcomes (81).
Although not a first line treatment, SBRT is commonly used for local control and as a bridging therapy in transplant candidates. A recent phase II trial reported response rates of 62.5–78.1% in patients undergoing SBRT as bridge towards transplant (82). In locally advanced HCC, combined chemoradiation and HAIC have achieved downstaging in 78% of patients, highlighting the potential of radiotherapy as part of a multimodal regimen (36).
Histotripsy applies short, high amplitude ultrasound pulses to induce cavitation in focal tissues. This nonthermal, nonionizing technique maximizes the targeted advantages of ablative therapy while eliminating limitations such as the “heat sink effect,” off target thermal spread, and thermal fixation (83). The multicenter phase I THERESA trial was the first feasibility study and reported good concordance between tissue destruction and planned target volume without device-related adverse events (84). The prospective, multicenter, single-arm HOPE4LIVER trial also reported technical success with low treatment-related complications (85, 86). Future trials are needed to evaluate the long-term efficacy of this modality as a locoregional therapy.
Liver-directed locoregional therapies (LDT/LRT) play a critical role in bridging, downstaging, or converting unresectable disease. While randomized clinical trials are limited, evidence supports their use in bridging patients with projected long wait times (87). Patients downstaged with LRT appear to have comparable outcomes relative to patients meeting Milan Criteria upfront. Yao et al.'s protocol including TACE or RFA/PEI successfully downstaged 65% of patients with no significant difference in 1- and 5-year post-transplant survival compared to patients meeting Milan criteria upfront (93.4/77.8% vs. 94.3/81% p = 0.69) (88). Similarly, Chapman et al. reported a >40% downstaging rate with comparable 5-year recurrence (10.9% vs. 10.8%, p = 0.84) and post-transplant OS (26). Downstaging therapy with TACE/TARE +/- sorafenib has shown higher risk of recurrence but comparable OS compared to tumors meeting Milan criteria upfront (27). Conversion therapy is an area of active investigation, with emerging evidence suggesting enhanced potential when LRTs are combined with systemic treatments (36, 71, 89–92).
As discussed, multimodal treatment of HCC offers opportunities for therapeutic synergy, particularly through the combination of LDT/LRT with ICIs or targeted therapies (93). For example, TACE induces cellular damage and tumor necrosis, generating neoantigens that can prime the adaptive immune response when paired with ICI. Concurrently, TACE-induced tissue hypoxia stimulates angiogenesis, which can be mitigated by VEGF inhibitors. Similarly, LRTs such as ablation, radiation or histotripsy may generate tumor neoantigens that enhance immune responses or potentiate the effects of targeted therapies.
These combined therapies have primarily been studied in intermediate to advanced and unresectable HCC (71). Interim analysis from the multi-center phase III LAUNCH trial demonstrated improved PFS (10.6 vs. 6.4 months, HR 0.43) and OS (17.8 vs. 11.5 months, HR 0.45) in patients treated with lenvatinib plus TACE vs. lenvatinib alone (94). Several ongoing or recently completed trials are evaluating the impact of combined therapies. The phase III EMERALD-1 trial (NCT03778957) examines TACE and durvalumab, with or without bevacizumab, or TACE alone (95). Interim analysis showed improved PFS for TACE plus durvalumab and bevacizumab vs. TACE alone (15.0 vs. 8.2 months, HR 0.77). The phase III LEAP-012 trial (NCT04246177) evaluates TACE plus lenvatinib and pembrolizumab vs. TACE plus placebo (96). Interim analysis demonstrated improved PFS for the combination (14.6 vs. 10.0 months, HR 0.66) (97). EMERALD-3 (NCT05301842) is a phase III trial comparing TACE plus tremelimumab plus durvalumab +/- lenvatinib vs. TACE monotherapy (98). The phase III CheckMate-74W trial (NCT04340193) sought to compare TACE with nivolumab and ipilimumab vs. nivolumab alone or placebo but was terminated due to slow accrual. The TACE-3 (NCT04268888) phase II/III trial will assess nivolumab in combination with TACE/TAE (99).
Collectively, these findings underscore the potential of multimodal approaches to enhance outcomes in HCC, supporting the concept of synergy between LDTs and systemic therapies and potential use in the neoadjuvant setting.
Several early phase trials have evaluated immune-based therapies in the neoadjuvant setting for HCC, with promising preliminary findings and no significant delays to surgery.
The phase Ib PRIME-HCC trial (NCT03682276) evaluated ipilimumab and nivolumab prior to resection, reporting no delays in surgery due to immune checkpoint inhibition (40, 100). All patients had pathologic responses seen on surgical specimens, with 78% achieving partial and 22% complete responses. A phase Ib/II trial in resectable disease evaluated the safety/efficacy of toripalimab vs. toripalimab plus lenvatinib (NCT03867370) (101). Among patients who proceeded to surgery, 20% had major pathological responses. In the Phase II trial of camrelizumab plus apatinib (NCT04297202) for resectable disease, most patients completed treatment, and no surgical delays were reported (102). More than 20% of patients had a partial or complete pathological response, and circulating tumor DNA (ctDNA) positivity correlated with a lack of major pathological response. In the phase II trial for cemiplimab (NCT03916627) in resectable disease, one patient had surgery delayed due to medication adverse effects, however, there were no grade 4 or 5 adverse effects observed (39). Notably, 35% of patients achieved significant or partial pathologic response. Another phase II trial (NCT03222076) explored neoadjuvant and adjuvant nivolumab plus ipilimumab vs. nivolumab monotherapy in resectable disease (41, 103). No patients experienced delays in surgery due to medication effects. Major pathological response was observed in a subset of patients in both groups (27% nivolumab plus ipilimumab vs. 33% nivolumab), and PFS was higher in the combination group (19.5 vs. 9.4 months).
Whereas most trials for neoadjuvant therapy involve resectable disease, one phase Ib trial evaluated cabozantinib and nivolumab in borderline resectable or locally advanced HCC (NCT03299946) (104). Of the 14 patients treated, 12 underwent successful surgical resection with negative margins. Notably, 25% of patients had a major pathologic response and 1 patient had a complete pathologic response, highlighting the potential for converting borderline resectable or locally advanced cases using neoadjuvant therapy. Enrichment in effector T cells, tertiary lymphoid structures, and distinct B cell and plasma cell profiles was found in responders (105).
Other studies have examined the use of LRTs alone or in conjunction with systemic therapy in the neoadjuvant setting. A retrospective analysis noted that combination of TACE and HAIC vs. TACE alone led to enhanced conversion rates for initially unresectable disease (106). A phase II trial combining lenvatinib, toripalimab and FOLFOX-HAIC in advanced HCC demonstrated response rates exceeding 60% (107).
In summary, these studies underscore the feasibility and safety of neoadjuvant immune-based and combination therapies, with minimal delays to surgery. Notably, initial evidence supports the potential for converting borderline or unresectable HCC to resectable cases. Additionally, biomarkers such as ctDNA. have emerged as valuable tools for monitoring treatment response, detecting disease recurrence or progression, and ultimately informing clinical and surgical decision making. Ongoing and future trials are needed to shed light on optimal strategies for leveraging novel anti-cancer therapies.
Neoadjuvant immunotherapy has the potential to transform the management of HCC. By inducing immediate tumor reduction, expanding effector and memory CD4 + and CD8+ T cell populations, and enhancing interferon-gamma and granzyme B activity, it primes the immune system to eliminate residual micrometastatic disease and reduces the risk of recurrence (39, 51, 104).
Particularly when combined with other treatment modalities, neoadjuvant immunotherapy has shown potential to amplify anti-tumor effects while minimizing toxicity to functional liver parenchyma. Multiple trials are underway to further explore the effects of combination therapy (Table 1), including dual immunotherapies, immunotherapy with anti-VEGF agents, and immunotherapy with LDTs, including HAIC, TACE, TARE, and ablation. LRTs can stimulate the immune response by releasing tumor antigens from tumor debris, potentiating antitumor immune responses and reducing the risk of micrometastatic recurrence (108). The synergistic effects of immunotherapy and locoregional therapy may enable downstaging advanced disease for curative intent resection or bridging to transplant (109). However, many current trials have small cohorts and lack comparison groups, limiting the validation of specific combinations, optimal regimens, and treatment durations.
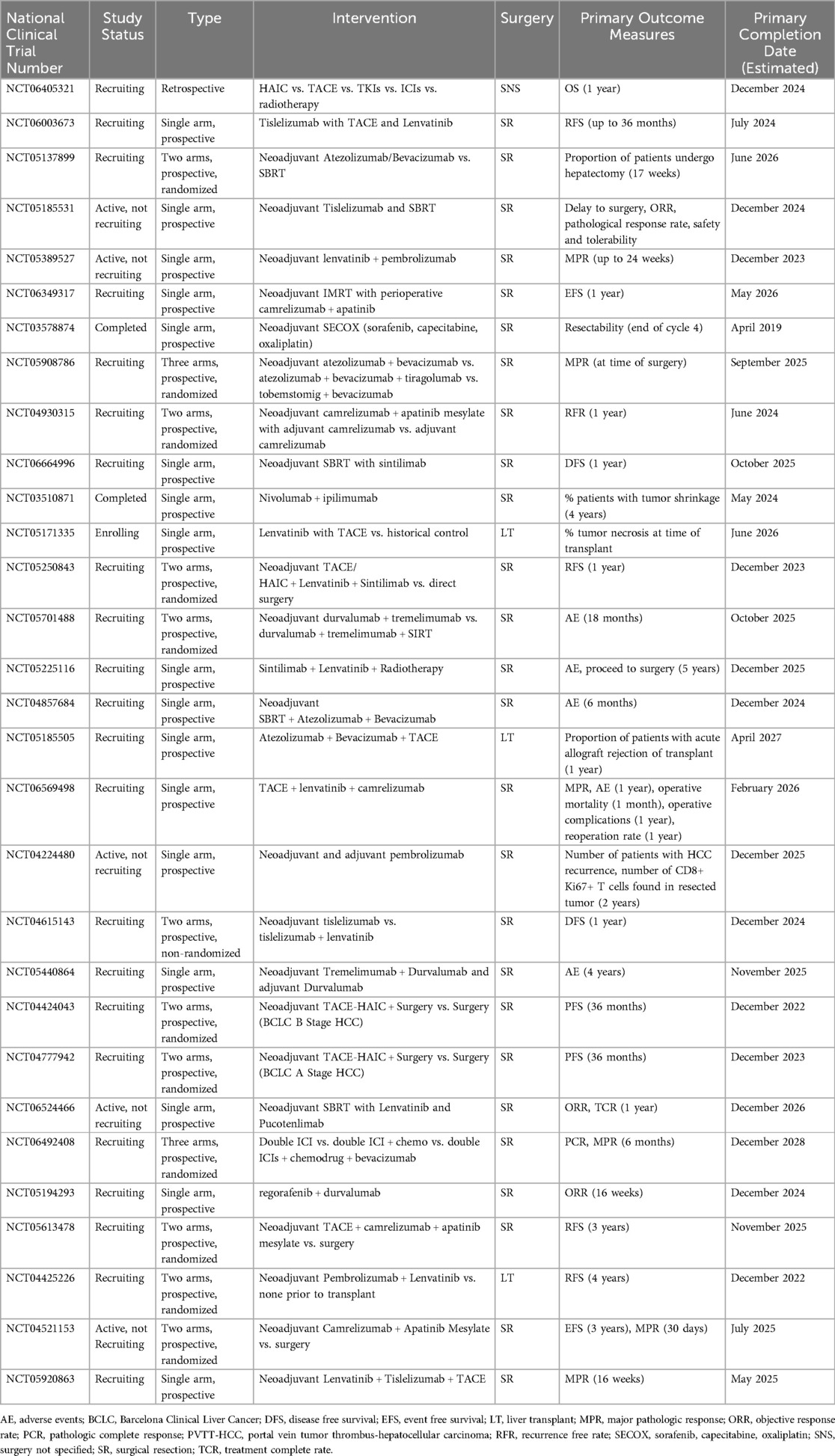
Table 1. Neoadjuvant trials in hepatocellular carcinoma.
Identifying novel HCC biomarkers may enable early detection, the development of targeted therapy, and the identification of tumor resistance. Recent advances in sequencing technologies and ctDNA detection methods have broadened the potential role of liquid biopsies. ctDNA-based liquid biopsies can identify new biomarkers, measure treatment response, estimate tumor mutational burden, and assess minimal residual disease to predict recurrence risk or need for adjuvant immunotherapy (109–113).
Beyond ICIs, other immune interventions that are being explored include allogenic natural killer (NK) cells, chimeric antigen receptor T (CAR-T) cells, oncolytic viruses, and vaccines (114). The Phase IIb TRAVERSE study investigated a vaccinia virus-based oncolytic immunotherapy (pexastimogene devacirepvec) in patients who progressed on sorafenib. While it did not improve OS compared to best supportive care, it demonstrated induction of a T-cell response (115). The use of CAR-T-cell therapy in solid tumors has so far been limited, but preclinical models have demonstrated potential for further applications which are being explored in clinical trials (116, 117).
Hepatocellular carcinoma is projected to increase in incidence and mortality. The armamentarium for the treatment of unresectable, recurrent, and metastatic disease has expanded. Neoadjuvant and combination therapies have the potential to redefine HCC management, offering improved outcomes for resectable, borderline resectable, and advanced disease. ICIs have shown safety and efficacy in early trials, while combinations with anti-VEGF agents, LRTs like TACE and ablation, and systemic treatments enhance anti-tumor effects while preserving liver function. LRTs stimulate immune responses by generating tumor neoantigens, further boosting the impact of immunotherapy. Emerging biomarkers like ctDNA enable precise monitoring of treatment response and recurrence risk. Novel approaches, including CAR-T cells and oncolytic viruses, are expanding therapeutic possibilities. While current trials face limitations, these advancements highlight the transformative potential of multimodal strategies in improving surgical outcomes, reducing recurrence, and achieving curative results in advanced HCC. Continued research will be vital to optimize and standardize these approaches to change the surgical—and survival—landscape for this deadly disease.
KG: Conceptualization, Investigation, Writing – original draft, Writing – review & editing, Data curation. AT: Conceptualization, Writing – original draft, Writing – review & editing, Data curation, Investigation. JP: Conceptualization, Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2024) 74(3):229–63. doi: 10.3322/caac.21834
2. Llovet JM, Pinyol R, Yarchoan M, Singal AG, Marron TU, Schwartz M, et al. Adjuvant and neoadjuvant immunotherapies in hepatocellular carcinoma. Nat Rev Clin Oncol. (2024) 21(4):294–311. doi: 10.1038/s41571-024-00868-0
3. Surveillance, Epidemiology, and End Results (SEER) Program SEER*Stat Database: Incidence - SEER 17 Regs Research Data+Hurricane Katrina Impacted Louisiana Cases, November 2023 Sub (2000-2021), National Cancer Institute, DCCPS, Surveillance Research Program, Surveillance Systems Branch, released April 2024, based on the November 2023 submission. Available online at: www.seer.cancer.gov
4. Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc J-F, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. (2008) 359(4):378–90. doi: 10.1056/NEJMoa0708857
5. Finn RS, Qin S, Ikeda M, Galle PR, Ducreux M, Kim TY, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. (2020) 382(20):1894–905. doi: 10.1056/NEJMoa1915745
6. Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, Bozzetti F, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. (1996) 334(11):693–700. doi: 10.1056/NEJM199603143341104
7. Xu L, Chen L, Zhang W. Neoadjuvant treatment strategies for hepatocellular carcinoma. World J Gastrointest Surg. (2021) 13(12):1550–66. doi: 10.4240/wjgs.v13.i12.1550
8. Yin Z, Chen D, Liang S, Li X. Neoadjuvant therapy for hepatocellular carcinoma. J Hepatocell Carcinoma. (2022) 9:929–46. doi: 10.2147/JHC.S357313
9. Chick RC, Ruff SM, Pawlik TM. Neoadjuvant systemic therapy for hepatocellular carcinoma. Front Immunol. (2024) 15:1355812. doi: 10.3389/fimmu.2024.1355812
10. Yao FY, Bass NM, Nikolai B, Merriman R, Davern TJ, Kerlan R, et al. A follow-up analysis of the pattern and predictors of dropout from the waiting list for liver transplantation in patients with hepatocellular carcinoma: implications for the current organ allocation policy. Liver Transpl. (2003) 9(7):684–92. doi: 10.1053/jlts.2003.50147
11. Pompili M, Francica G, Ponziani FR, Iezzi R, Avolio AW. Bridging and downstaging treatments for hepatocellular carcinoma in patients on the waiting list for liver transplantation. World J Gastroenterol. (2013) 19(43):7515–30. doi: 10.3748/wjg.v19.i43.7515
12. Fujiki M, Aucejo F, Choi M, Kim R. Neo-adjuvant therapy for hepatocellular carcinoma before liver transplantation: where do we stand? World J Gastroenterol. (2014) 20(18):5308–19. doi: 10.3748/wjg.v20.i18.5308
13. Mazzaferro V, Battiston C, Perrone S, Pulvirenti A, Regalia E, Romito R, et al. Radiofrequency ablation of small hepatocellular carcinoma in cirrhotic patients awaiting liver transplantation: a prospective study. Ann Surg. (2004) 240(5):900–9. doi: 10.1097/01.sla.0000143301.56154.95
14. DuBay DA, Sandroussi C, Kachura JR, Ho CS, Beecroft JR, Vollmer CM, et al. Radiofrequency ablation of hepatocellular carcinoma as a bridge to liver transplantation. HPB (Oxford). (2011) 13(1):24–32. doi: 10.1111/j.1477-2574.2010.00228.x
15. Tsochatzis E, Garcovich M, Marelli L, Papastergiou V, Fatourou E, Rodriguez-Peralvarez ML, et al. Transarterial embolization as neo-adjuvant therapy pretransplantation in patients with hepatocellular carcinoma. Liver Int. (2013) 33(6):944–9. doi: 10.1111/liv.12144
16. Graziadei IW, Sandmueller H, Waldenberger P, Koenigsrainer A, Nachbaur K, Jaschke W, et al. Chemoembolization followed by liver transplantation for hepatocellular carcinoma impedes tumor progression while on the waiting list and leads to excellent outcome. Liver Transpl. (2003) 9(6):557–63. doi: 10.1053/jlts.2003.50106
17. Hayashi PH, Ludkowski M, Forman LM, Osgood M, Johnson S, Kugelmas M, et al. Hepatic artery chemoembolization for hepatocellular carcinoma in patients listed for liver transplantation. Am J Transplant. (2004) 4(5):782–7. doi: 10.1111/j.1600-6143.2004.00413.x
18. Sandroussi C, Dawson LA, Lee M, Guindi M, Fischer S, Ghanekar A, et al. Radiotherapy as a bridge to liver transplantation for hepatocellular carcinoma. Transpl Int. (2010) 23(3):299–306. doi: 10.1111/j.1432-2277.2009.00980.x
19. Kulik LM, Atassi B, van Holsbeeck L, Souman T, Lewandowski RJ, Mulcahy MF, et al. Yttrium-90 microspheres (TheraSphere) treatment of unresectable hepatocellular carcinoma: downstaging to resection, RFA and bridge to transplantation. J Surg Oncol. (2006) 94(7):572–86. doi: 10.1002/jso.20609
20. Kulik L, Heimbach JK, Zaiem F, Almasri J, Prokop LJ, Wang Z, et al. Therapies for patients with hepatocellular carcinoma awaiting liver transplantation: a systematic review and meta-analysis. Hepatology. (2018) 67(1):381–400. doi: 10.1002/hep.29485
21. OPTN Policy Notice Clarification of HCC Downstaging Protocol for Standard Exceptions. Rockville, MD: Organ Procurement and Transplantation Network, Health Resources and Services Administration, U.S. Department of Health & Human Services (2019). Availble online at: https://optn.transplant.hrsa.gov/media/3123/policynotice_20190801_liver.pdf
22. Finkenstedt A, Vikoler A, Portenkirchner M, Mülleder K, Maglione M, Margreiter C, et al. Excellent post-transplant survival in patients with intermediate stage hepatocellular carcinoma responding to neoadjuvant therapy. Liver Int. (2016) 36(5):688–95. doi: 10.1111/liv.12966
23. Golse N, Radenne S, Rode A, Ducerf C, Mabrut JY, Merle P. Liver transplantation after neoadjuvant sorafenib therapy: preliminary experience and literature review. Exp Clin Transplant. (2018) 16(2):227–36. doi: 10.6002/ect.2015.0299
24. Gabr A, Kulik L, Mouli S, Riaz A, Ali R, Desai K, et al. Liver transplantation following yttrium-90 radioembolization: 15-year experience in 207-patient cohort. Hepatology. (2021) 73(3):998–1010. doi: 10.1002/hep.31318
25. Qiao ZY, Zhang ZJ, Lv ZC, Tong H, Xi ZF, Wu HX, et al. Neoadjuvant programmed cell death 1 (PD-1) inhibitor treatment in patients with hepatocellular carcinoma before liver transplant: a cohort study and literature review. Front Immunol. (2021) 12:653437. doi: 10.3389/fimmu.2021.653437
26. Chapman WC, Garcia-Aroz S, Vachharajani N, Fowler K, Saad N, Lin Y, et al. Liver transplantation for advanced hepatocellular carcinoma after downstaging without up-front stage restrictions. J Am Coll Surg. (2017) 224(4):610–21. doi: 10.1016/j.jamcollsurg.2016.12.020
27. Kim Y, Stahl CC, Makramalla A, Olowokure OO, Ristagno RL, Dhar VK, et al. Downstaging therapy followed by liver transplantation for hepatocellular carcinoma beyond milan criteria. Surgery. (2017) 162(6):1250–8. doi: 10.1016/j.surg.2017.08.007
28. Rudnick SR, Russo MW. Liver transplantation beyond or downstaging within the milan criteria for hepatocellular carcinoma. Expert Rev Gastroenterol Hepatol. (2018) 12(3):265–75. doi: 10.1080/17474124.2018.1417035
29. Parikh ND, Waljee AK, Singal AG. Downstaging hepatocellular carcinoma: a systematic review and pooled analysis. Liver Transpl. (2015) 21(9):1142–52. doi: 10.1002/lt.24169
30. Kardashian A, Florman SS, Haydel B, Ruiz RM, Klintmalm GB, Lee DD, et al. Liver transplantation outcomes in a U.S. Multicenter cohort of 789 patients with hepatocellular carcinoma presenting beyond milan criteria. Hepatology. (2020) 72(6):2014–28. doi: 10.1002/hep.31210
31. Pozzo C, Basso M, Cassano A, Quirino M, Schinzari G, Trigila N, et al. Neoadjuvant treatment of unresectable liver disease with irinotecan and 5-fluorouracil plus folinic acid in colorectal cancer patients. Ann Oncol. (2004) 15(6):933–9. doi: 10.1093/annonc/mdh217
32. Folprecht G, Grothey A, Alberts S, Raab HR, Köhne CH. Neoadjuvant treatment of unresectable colorectal liver metastases: correlation between tumour response and resection rates. Ann Oncol. (2005) 16(8):1311–9. doi: 10.1093/annonc/mdi246
33. Alberts SR, Horvath WL, Sternfeld WC, Goldberg RM, Mahoney MR, Dakhil SR, et al. Oxaliplatin, fluorouracil, and leucovorin for patients with unresectable liver-only metastases from colorectal cancer: a north central cancer treatment group phase II study. J Clin Oncol. (2005) 23(36):9243–9. doi: 10.1200/JCO.2005.07.740
34. Adam R, Delvart V, Pascal G, Valeanu A, Castaing D, Azoulay D, et al. Rescue surgery for unresectable colorectal liver metastases downstaged by chemotherapy: a model to predict long-term survival. Ann Surg. (2004) 240(4):644–57. discussion 57-8. doi: 10.1097/01.sla.0000141198.92114.f6
35. Lau WY, Ho SK, Yu SC, Lai EC, Liew CT, Leung TW. Salvage surgery following downstaging of unresectable hepatocellular carcinoma. Ann Surg. (2004) 240(2):299–305. doi: 10.1097/01.sla.0000133123.11932.19
36. Lee HS, Choi GH, Choi JS, Kim KS, Han KH, Seong J, et al. Surgical resection after down-staging of locally advanced hepatocellular carcinoma by localized concurrent chemoradiotherapy. Ann Surg Oncol. (2014) 21(11):3646–53. doi: 10.1245/s10434-014-3652-3
37. Lee BH, Lee DS, Cho CW, Yun SS. Role and limitation of neoadjuvant hepatic arterial infusion chemotherapy in advanced hepatocelluar carcinoma patients with child-pugh class A. World J Surg Oncol. (2019) 17(1):143. doi: 10.1186/s12957-019-1685-6
38. Li G, Shu B, Zheng Z, Yin H, Zhang C, Xiao Y, et al. Safety and efficacy of radiotherapy combined with lenvatinib plus PD-1 inhibitors as neo-adjuvant therapy in hepatocellular carcinoma with portal vein thrombus: protocol of an open-label, single-arm, prospective, multi-center phase I trial. Front Oncol. (2022) 12:1051916. doi: 10.3389/fonc.2022.1051916
39. Marron TU, Fiel MI, Hamon P, Fiaschi N, Kim E, Ward SC, et al. Neoadjuvant cemiplimab for resectable hepatocellular carcinoma: a single-arm, open-label, phase 2 trial. Lancet Gastroenterol Hepatol. (2022) 7(3):219–29. doi: 10.1016/S2468-1253(21)00385-X
40. D'Alessio A, Pai M, Spalding D, Rajagopal P, Talbot T, Goldin R, et al. Preliminary results from a phase ib study of neoadjuvant ipilimumab plus nivolumab prior to liver resection for hepatocellular carcinoma: the PRIME-HCC trial. J Clin Oncol. (2022) 40(16_suppl):4093. doi: 10.1200/JCO.2022.40.16_suppl.4093
41. Kaseb AO, Hasanov E, Cao HST, Xiao L, Vauthey JN, Lee SS, et al. Perioperative nivolumab monotherapy versus nivolumab plus ipilimumab in resectable hepatocellular carcinoma: a randomised, open-label, phase 2 trial. Lancet Gastroenterol Hepatol. (2022) 7(3):208–18. doi: 10.1016/S2468-1253(21)00427-1
42. Glantzounis GK, Paliouras A, Stylianidi MC, Milionis H, Tzimas P, Roukos D, et al. The role of liver resection in the management of intermediate and advanced stage hepatocellular carcinoma. A systematic review. Eur J Surg Oncol. (2018) 44(2):195–208. doi: 10.1016/j.ejso.2017.11.022
43. Deig CR, Sutton TL, Beneville B, Trone K, Stratton A, Gunesch AN, et al. Neoadjuvant therapy is associated with improved chemotherapy delivery and overall survival compared to upfront resection in pancreatic cancer without increasing perioperative complications. Cancers (Basel). (2022) 14(3):609. doi: 10.3390/cancers14030609
44. Morton D, Seymour M, Magill L, Handley K, Glasbey J, Glimelius B, et al. Preoperative chemotherapy for operable colon cancer: mature results of an international randomized controlled trial. J Clin Oncol. (2023) 41(8):1541–52. doi: 10.1200/JCO.22.00046
45. Marin JJG, Herraez E, Lozano E, Macias RIR, Briz O. Models for understanding resistance to chemotherapy in liver cancer. Cancers (Basel). (2019) 11(11):1677. doi: 10.3390/cancers11111677
46. Sheng J, Qin H, Zhang K, Li B, Zhang X. Targeting autophagy in chemotherapy-resistant of hepatocellular carcinoma. Am J Cancer Res. (2018) 8(3):354–65.29636994
47. Lohitesh K, Chowdhury R, Mukherjee S. Resistance a major hindrance to chemotherapy in hepatocellular carcinoma: an insight. Cancer Cell Int. (2018) 18(1):44. doi: 10.1186/s12935-018-0538-7
48. Ringelhan M, Pfister D, O’Connor T, Pikarsky E, Heikenwalder M. The immunology of hepatocellular carcinoma. Nat Immunol. (2018) 19(3):222–32. doi: 10.1038/s41590-018-0044-z
49. Jilkova Z M, Aspord C, Decaens T. Predictive factors for response to PD-1/PD-L1 checkpoint inhibition in the field of hepatocellular carcinoma: current Status and challenges. Cancers (Basel). (2019) 11(10):1554. doi: 10.3390/cancers11101554
50. Gao Q, Wang X-Y, Qiu S-J, Yamato I, Sho M, Nakajima Y, et al. Overexpression of PD-L1 significantly associates with tumor aggressiveness and postoperative recurrence in human hepatocellular carcinoma. Clin Cancer Res. (2009) 15(3):971–9. doi: 10.1158/1078-0432.CCR-08-1608
51. Zhu AX, Abbas AR, de Galarreta MR, Guan Y, Lu S, Koeppen H, et al. Molecular correlates of clinical response and resistance to atezolizumab in combination with bevacizumab in advanced hepatocellular carcinoma. Nat Med. (2022) 28(8):1599–611. doi: 10.1038/s41591-022-01868-2
52. Zhu AX, Finn RS, Edeline J, Cattan S, Ogasawara S, Palmer D, et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): a non-randomised, open-label phase 2 trial. Lancet Oncol. (2018) 19(7):940–52. doi: 10.1016/S1470-2045(18)30351-6
53. Verset G, Borbath I, Karwal M, Verslype C, Van Vlierberghe H, Kardosh A, et al. Pembrolizumab monotherapy for previously untreated advanced hepatocellular carcinoma: data from the open-label, phase II KEYNOTE-224 trial. Clin Cancer Res. (2022) 28(12):2547–54. doi: 10.1158/1078-0432.CCR-21-3807
54. Abou-Alfa GK, Lau G, Kudo M, Chan SL, Kelley RK, Furuse J, et al. Tremelimumab plus durvalumab in unresectable hepatocellular carcinoma. NEJM Evid. (2022) 1(8):EVIDoa2100070. doi: 10.1056/EVIDoa2100070
55. Sangro B, Chan SL, Kelley RK, Lau G, Kudo M, Sukeepaisarnjaroen W, et al. Four-year overall survival update from the phase III HIMALAYA study of tremelimumab plus durvalumab in unresectable hepatocellular carcinoma. Ann Oncol. (2024) 35(5):448–57. doi: 10.1016/j.annonc.2024.02.005
56. Finn RS, Ryoo B-Y, Merle P, Kudo M, Bouattour M, Lim HY, et al. Pembrolizumab as second-line therapy in patients with advanced hepatocellular carcinoma in KEYNOTE-240: a randomized, double-blind, phase III trial. J Clin Oncol. (2019) 38(3):193–202. doi: 10.1200/JCO.19.01307
57. Motz GT, Santoro SP, Wang L-P, Garrabrant T, Lastra RR, Hagemann IS, et al. Tumor endothelium FasL establishes a selective immune barrier promoting tolerance in tumors. Nat Med. (2014) 20(6):607–15. doi: 10.1038/nm.3541
58. Morse MA, Sun W, Kim R, He AR, Abada PB, Mynderse M, et al. The role of angiogenesis in hepatocellular carcinoma. Clin Cancer Res. (2019) 25(3):912–20. doi: 10.1158/1078-0432.CCR-18-1254
59. Ikeda M, Sung MW, Kudo M, Kobayashi M, Baron AD, Finn RS, et al. A phase 1b trial of lenvatinib (LEN) plus pembrolizumab (PEM) in patients (pts) with unresectable hepatocellular carcinoma (uHCC). J Clin Oncol. (2018) 36(15_suppl):4076. doi: 10.1200/JCO.2018.36.15_suppl.4076
60. Huang S, Li D, Zhuang L, Sun L, Wu J. A meta-analysis of the efficacy and safety of adjuvant sorafenib for hepatocellular carcinoma after resection. World J Surg Oncol. (2021) 19(1):168. doi: 10.1186/s12957-021-02280-9
61. Bruix J, Takayama T, Mazzaferro V, Chau GY, Yang J, Kudo M, et al. Adjuvant sorafenib for hepatocellular carcinoma after resection or ablation (STORM): a phase 3, randomised, double-blind, placebo-controlled trial. Lancet Oncol. (2015) 16(13):1344–54. doi: 10.1016/S1470-2045(15)00198-9
62. Qin S, Chen M, Cheng AL, Kaseb AO, Kudo M, Lee HC, et al. Atezolizumab plus bevacizumab versus active surveillance in patients with resected or ablated high-risk hepatocellular carcinoma (IMbrave050): a randomised, open-label, multicentre, phase 3 trial. Lancet. (2023) 402(10415):1835–47. doi: 10.1016/S0140-6736(23)01796-8
63. Yopp A K, Chen M, Cheng M, Kaseb A, Lee AO, Qin HC, et al. LBA39 - updated efficacy and safety data from IMbrave050: phase III study of adjuvant atezolizumab (atezo)+bevacizumab (bev) vs active surveillance in patients (pts) with resected or ablated high-risk hepatocellular carcinoma (HCC). Ann Oncol. (2024) 35:1–72. doi: 10.1016/j.annonc.2023.11.002
64. Shanghai Junshi Bioscience Co., Ltd. Toripalimab or Placebo as Adjuvant Therapy in Hepatocellular Carcinoma After Radical Resection (JUPITER 04). Available online at: https://clinicaltrials.gov/study/NCT03859128 (Accessed November 18, 2024).
65. Goyal L, Vogel A, Zhu AX, Cheng A-L, Yau T, Zhou J, et al. P024 KEYNOTE-937 trial in progress: adjuvant pembrolizumab for hepatocellular carcinoma and complete radiologic response after surgical resection or local ablation. Gut. (2021) 70(Suppl 3):A22–A.
66. Exposito MJ, Akce M, Alvarez J, Assenat E, Balart L, Baron A, et al. Abstract No. 526 CheckMate-9DX: phase 3, randomized, double-blind study of adjuvant nivolumab vs placebo for patients with hepatocellular carcinoma (HCC) at high risk of recurrence after curative resection or ablation. J Vasc Interv Radiol. (2019) 30(3):S227–S8. doi: 10.1016/j.jvir.2018.12.607
67. Knox J, Cheng A, Cleary S, Galle P, Kokudo N, Lencioni R, et al. A phase 3 study of durvalumab with or without bevacizumab as adjuvant therapy in patients with hepatocellular carcinoma at high risk of recurrence after curative hepatic resection or ablation: eMERALD-2. Ann Oncol. (2019) 30:iv59–60. doi: 10.1093/annonc/mdz155.216
68. Jia Z, Zhang H, Li N. Evaluation of clinical outcomes of radiofrequency ablation and surgical resection for hepatocellular carcinoma conforming to the milan criteria: a systematic review and meta-analysis of recent randomized controlled trials. J Gastroenterol Hepatol. (2021) 36(7):1769–77. doi: 10.1111/jgh.15440
69. Takayama T, Hasegawa K, Izumi N, Kudo M, Shimada M, Yamanaka N, et al. Surgery versus radiofrequency ablation for small hepatocellular carcinoma: a randomized controlled trial (SURF trial). Liver Cancer. (2022) 11(3):209–18. doi: 10.1159/000521665
70. Gani RA, Teressa M, Budiman RA, Kalista KF, Lesmana CRA. Meta analysis of radiofrequency ablation versus surgical resection in small and large nodule of hepatocellular carcinoma. HPB (Oxford). (2024) 26(10):1216–28. doi: 10.1016/j.hpb.2024.06.009
71. Lyu N, Kong Y, Li X, Mu L, Deng H, Chen H, et al. Ablation reboots the response in advanced hepatocellular carcinoma with stable or atypical response during PD-1 therapy: a proof-of-concept study. Front Oncol. (2020) 10:580241. doi: 10.3389/fonc.2020.580241
72. Huang YH, Chen CH, Chang TT, Chen SC, Chiang JH, Lee HS, et al. The role of transcatheter arterial embolization for patients with unresectable hepatocellular carcinoma: a nationwide, multicentre study evaluated by cancer stage. Aliment Pharmacol Ther. (2005) 21(6):687–94. doi: 10.1111/j.1365-2036.2005.02404.x
73. Llovet JM, Real MI, Montaña X, Planas R, Coll S, Aponte J, et al. Arterial embolisation or chemoembolisation versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: a randomised controlled trial. Lancet. (2002) 359(9319):1734–9. doi: 10.1016/S0140-6736(02)08649-X
74. Lammer J, Malagari K, Vogl T, Pilleul F, Denys A, Watkinson A, et al. Prospective randomized study of doxorubicin-eluting-bead embolization in the treatment of hepatocellular carcinoma: results of the PRECISION V study. Cardiovasc Intervent Radiol. (2010) 33(1):41–52. doi: 10.1007/s00270-009-9711-7
75. Yang B, Liang J, Qu Z, Yang F, Liao Z, Gou H. Transarterial strategies for the treatment of unresectable hepatocellular carcinoma: a systematic review. PLoS One. (2020) 15(2):e0227475. doi: 10.1371/journal.pone.0227475
76. Ibrahim SM, Lewandowski RJ, Sato KT, Gates VL, Kulik L, Mulcahy MF, et al. Radioembolization for the treatment of unresectable hepatocellular carcinoma: a clinical review. World J Gastroenterol. (2008) 14(11):1664–9. doi: 10.3748/wjg.14.1664
77. Salem R, Johnson GE, Kim E, Riaz A, Bishay V, Boucher E, et al. Yttrium-90 radioembolization for the treatment of solitary, unresectable HCC: the LEGACY study. Hepatology. (2021) 74(5):2342–52. doi: 10.1002/hep.31819
78. Iwamoto H, Shimose S, Shirono T, Niizeki T, Kawaguchi T. Hepatic arterial infusion chemotherapy for advanced hepatocellular carcinoma in the era of chemo-diversity. Clin Mol Hepatol. (2023) 29(3):593–604. doi: 10.3350/cmh.2022.0391
79. Lyu N, Wang X, Li JB, Lai JF, Chen QF, Li SL, et al. Arterial chemotherapy of oxaliplatin plus fluorouracil versus sorafenib in advanced hepatocellular carcinoma: a biomolecular exploratory, randomized, phase III trial (FOHAIC-1). J Clin Oncol. (2022) 40(5):468–80. doi: 10.1200/JCO.21.01963
80. Li QJ, He MK, Chen HW, Fang WQ, Zhou YM, Xu L, et al. Hepatic arterial infusion of oxaliplatin, fluorouracil, and leucovorin versus transarterial chemoembolization for large hepatocellular carcinoma: a randomized phase III trial. J Clin Oncol. (2022) 40(2):150–60. doi: 10.1200/JCO.21.00608
81. Cao YZ, Zheng GL, Zhang TQ, Shao HY, Pan JY, Huang ZL, et al. Hepatic arterial infusion chemotherapy with anti-angiogenesis agents and immune checkpoint inhibitors for unresectable hepatocellular carcinoma and meta-analysis. World J Gastroenterol. (2024) 30(4):318–31. doi: 10.3748/wjg.v30.i4.318
82. Lee VH-F, Vardhanabhuti V, Wong TC-L, Lam K-O, Choi HC-W, Chiu KW-H, et al. Stereotactic body radiotherapy and liver transplant for liver cancer: a nonrandomized controlled trial. JAMA Network Open. (2024) 7(6):e2415998. doi: 10.1001/jamanetworkopen.2024.15998
83. Sandilos G, Butchy MV, Koneru M, Gongalla S, Sensenig R, Hong YK. Histotripsy – hype or hope? Review of innovation and future implications. J Gastrointest Surg. (2024) 28(8):1370–5. doi: 10.1016/j.gassur.2024.05.038
84. Vidal-Jove J, Serres X, Vlaisavljevich E, Cannata J, Duryea A, Miller R, et al. First-in-man histotripsy of hepatic tumors: the THERESA trial, a feasibility study. Int J Hyperthermia. (2022) 39(1):1115–23. doi: 10.1080/02656736.2022.2112309
85. Wah TM, Pech M, Thormann M, Serres X, Littler P, Stenberg B, et al. A multi-centre, single arm, non-randomized, prospective European trial to evaluate the safety and efficacy of the HistoSonics system in the treatment of primary and metastatic liver cancers (#HOPE4LIVER). Cardiovasc Intervent Radiol. (2023) 46(2):259–67. doi: 10.1007/s00270-022-03309-6
86. Mendiratta-Lala M, Wiggermann P, Pech M, Serres-Créixams X, White SB, Davis C, et al. The #HOPE4LIVER single-arm pivotal trial for histotripsy of primary and metastatic liver tumors. Radiology. (2024) 312(3):e233051. doi: 10.1148/radiol.233051
87. Di Martino M, Ferraro D, Pisaniello D, Arenga G, Falaschi F, Terrone A, et al. Bridging therapies for patients with hepatocellular carcinoma awaiting liver transplantation: a systematic review and meta-analysis on intention-to-treat outcomes. J Hepatobiliary Pancreat Sci. (2023) 30(4):429–38. doi: 10.1002/jhbp.1248
88. Yao FY, Mehta N, Flemming J, Dodge J, Hameed B, Fix O, et al. Downstaging of hepatocellular cancer before liver transplant: long-term outcome compared to tumors within milan criteria. Hepatology. (2015) 61(6):1968–77. doi: 10.1002/hep.27752
89. Song T, Lang M, Lu W, Zhang T, Li H, Wu Q, et al. Conversion of initially unresectable hepatocellular carcinoma (HCC) with triple-combination therapy (lenvatinib, anti-PD-1 antibodies, and transarterial therapy): a retrospective analysis. J Clin Oncol. (2022) 40(4_suppl):413. doi: 10.1200/JCO.2022.40.4_suppl.413
90. Chiang CL, Chiu KWH, Chan KSK, Lee FAS, Li JCB, Wan CWS, et al. Sequential transarterial chemoembolisation and stereotactic body radiotherapy followed by immunotherapy as conversion therapy for patients with locally advanced, unresectable hepatocellular carcinoma (START-FIT): a single-arm, phase 2 trial. Lancet Gastroenterol Hepatol. (2023) 8(2):169–78. doi: 10.1016/S2468-1253(22)00339-9
91. Hamaoka M, Kobayashi T, Kuroda S, Iwako H, Okimoto S, Kimura T, et al. Hepatectomy after down-staging of hepatocellular carcinoma with portal vein tumor thrombus using chemoradiotherapy: a retrospective cohort study. Int J Surg. (2017) 44:223–8. doi: 10.1016/j.ijsu.2017.06.082
92. Tan DJH, Lim WH, Yong JN, Ng CH, Muthiah MD, Tan EX, et al. UNOS down-staging criteria for liver transplantation of hepatocellular carcinoma: systematic review and meta-analysis of 25 studies. Clin Gastroenterol Hepatol. (2023) 21(6):1475–84. doi: 10.1016/j.cgh.2022.02.018
93. Kumar P, Wehrle CJ, Sun K, Jiao C, Panconesi R, Zhang M, et al. Combining liver-directed and immunotherapy in advanced hepatocellular carcinoma: a review and future directions. Surgical Oncology Insight. (2024) 1(4):100100. doi: 10.1016/j.soi.2024.100100
94. Peng Z, Fan W, Zhu B, Wang G, Sun J, Xiao C, et al. Lenvatinib combined with transarterial chemoembolization as first-line treatment for advanced hepatocellular carcinoma: a phase III, randomized clinical trial (LAUNCH). J Clin Oncol. (2022) 41(1):117–27. doi: 10.1200/JCO.22.00392
95. Lencioni R, Kudo M, Erinjeri J, Qin S, Ren Z, Chan S, et al. EMERALD-1: a phase 3, randomized, placebo-controlled study of transarterial chemoembolization combined with durvalumab with or without bevacizumab in participants with unresectable hepatocellular carcinoma eligible for embolization. J Clin Oncol. (2024) 42(3_suppl):LBA432–LBA. doi: 10.1200/JCO.2024.42.3_suppl.LBA432
96. Llovet JM, Vogel A, Madoff DC, Finn RS, Ogasawara S, Ren Z, et al. Randomized phase 3 LEAP-012 study: transarterial chemoembolization with or without lenvatinib plus pembrolizumab for intermediate-stage hepatocellular carcinoma not amenable to curative treatment. Cardiovasc Intervent Radiol. (2022) 45(4):405–12. doi: 10.1007/s00270-021-03031-9
97. Llovet J, Finn RS, Ren Z, Guo Y, Han G, Lin H, et al. LBA3 transarterial chemoembolization (TACE) with or without lenvatinib (len)+pembrolizumab (pembro) for intermediate-stage hepatocellular carcinoma (HCC): phase III LEAP-012 study. Ann Oncol. (2024) 35:S1229. doi: 10.1016/j.annonc.2024.08.2277
98. Abou-Alfa GK, Fan J, Heo J, Arai Y, Erinjeri JP, Kuhl CK, et al. 727TiP A randomised phase III study of tremelimumab (T) plus durvalumab (D) with or without lenvatinib combined with concurrent transarterial chemoembolisation (TACE) versus TACE alone in patients (pts) with locoregional hepatocellular carcinoma (HCC): eMERALD-3. Ann Oncol. (2022) 33:S874. doi: 10.1016/j.annonc.2022.07.851
99. Nivolumab in Combination With TACE/TAE for Patients With Intermediate Stage HCC (TACE-3). Available online at: https://clinicaltrialsgov/study/NCT04268888. (accessed November 11, 2024).
100. Pinato DJ, Cortellini A, Sukumaran A, Cole T, Pai M, Habib N, et al. PRIME-HCC: phase ib study of neoadjuvant ipilimumab and nivolumab prior to liver resection for hepatocellular carcinoma. BMC Cancer. (2021) 21(1):301. doi: 10.1186/s12885-021-08033-x
101. Shi Y, Ji Y, Liu W, Pang YR, Ding ZB, Fu XT, et al. A phase ib/II, open-label study evaluating the efficacy and safety of toripalimab injection (JS001) or combination with lenvatinib as a neoadjuvant therapy for patients with resectable hepatocellular carcinoma (HCC). in: proceedings of the American association for cancer research annual meeting 2021; 2021 apr 10-15 and may 17-21. Philadelphia (PA): AACR. Cancer Res. (2021) 81(13_Suppl):486. doi: 10.1158/1538-7445.AM2021-486
102. Xia Y, Tang W, Qian X, Li X, Cheng F, Wang K, et al. Efficacy and safety of camrelizumab plus apatinib during the perioperative period in resectable hepatocellular carcinoma: a single-arm, open label, phase II clinical trial. J Immunother Cancer. (2022) 10(4):e004656. doi: 10.1136/jitc-2022-004656
103. Kaseb AO, Tran Cao HS, Mohamed YI, Qayyum A, Vence LM, Blando JM, et al. Final results of a randomized, open label, perioperative phase II study evaluating nivolumab alone or nivolumab plus ipilimumab in patients with resectable HCC. J Clin Oncol. (2020) 38(15_suppl):4599. doi: 10.1200/JCO.2020.38.15_suppl.4599
104. Yarchoan M, Zhu Q, Durham JN, Gross N, Charmsaz S, Leatherman JM, et al. Feasibility and efficacy of neoadjuvant cabozantinib and nivolumab in patients with borderline resectable or locally advanced hepatocellular carcinoma (HCC). J Clin Oncol. (2021) 39(3_suppl):335. doi: 10.1200/JCO.2021.39.3_suppl.335
105. Ho WJ, Zhu Q, Durham J, Popovic A, Xavier S, Leatherman J, et al. Neoadjuvant cabozantinib and nivolumab converts locally advanced HCC into resectable disease with enhanced antitumor immunity. Nat Cancer. (2021) 2(9):891–903. doi: 10.1038/s43018-021-00234-4
106. Li B, Qiu J, Zheng Y, Shi Y, Zou R, He W, et al. Conversion to resectability using transarterial chemoembolization combined with hepatic arterial infusion chemotherapy for initially unresectable hepatocellular carcinoma. Ann Surg Open. (2021) 2(2):e057. doi: 10.1097/AS9.0000000000000057
107. Lai Z, He M, Bu X, Xu Y, Huang Y, Wen D, et al. Lenvatinib, toripalimab plus hepatic arterial infusion chemotherapy in patients with high-risk advanced hepatocellular carcinoma: a biomolecular exploratory, phase II trial. Eur J Cancer. (2022) 174:68–77. doi: 10.1016/j.ejca.2022.07.005
108. den Brok MHMGM, Sutmuller RPM, van der Voort R, Bennink EJ, Figdor CG, Ruers TJM, et al. In situ tumor ablation creates an antigen source for the generation of antitumor immunity. Cancer Res. (2004) 64(11):4024–9. doi: 10.1158/0008-5472.CAN-03-3949
109. Raj R, Wehrle CJ, Aykun N, Stitzel H, Ma WW, Krishnamurthi S, et al. Immunotherapy plus locoregional therapy leading to curative-intent hepatectomy in HCC: proof of concept producing durable survival benefits detectable with liquid biopsy. Cancers (Basel). (2023) 15(21):5220. doi: 10.3390/cancers15215220
110. Labgaa I, Villacorta-Martin C, D’Avola D, Craig AJ, von Felden J, Martins-Filho SN, et al. A pilot study of ultra-deep targeted sequencing of plasma DNA identifies driver mutations in hepatocellular carcinoma. Oncogene. (2018) 37(27):3740–52. doi: 10.1038/s41388-018-0206-3
111. Jardim DL, Goodman A, de Melo Gagliato D, Kurzrock R. The challenges of tumor mutational burden as an immunotherapy biomarker. Cancer Cell. (2021) 39(2):154–73. doi: 10.1016/j.ccell.2020.10.001
112. Xu Y, Cai J, Zhong K, Wen Y, Cai L, He G, et al. Plasma-only circulating tumor DNA analysis detects minimal residual disease and predicts early relapse in hepatocellular carcinoma patients undergoing curative resection. Front Oncol. (2023) 13. doi: 10.3389/fonc.2023.1119744
113. Ao H, Xin Z, Jian Z. Liquid biopsy to identify biomarkers for immunotherapy in hepatocellular carcinoma. Biomark Res. (2021) 9(1):91. doi: 10.1186/s40364-021-00348-y
114. Foerster F, Gairing SJ, Ilyas SI, Galle PR. Emerging immunotherapy for HCC: a guide for hepatologists. Hepatology. (2022) 75(6):1604–26. doi: 10.1002/hep.32447
115. Moehler M, Heo J, Lee HC, Tak WY, Chao Y, Paik SW, et al. Vaccinia-based oncolytic immunotherapy pexastimogene devacirepvec in patients with advanced hepatocellular carcinoma after sorafenib failure: a randomized multicenter phase IIb trial (TRAVERSE). OncoImmunology. (2019) 8(8):1615817. doi: 10.1080/2162402X.2019.1615817
116. Sun B, Yang D, Dai H, Liu X, Jia R, Cui X, et al. Eradication of hepatocellular carcinoma by NKG2D-based CAR-T cells. Cancer Immunol Res. (2019) 7(11):1813–23. doi: 10.1158/2326-6066.CIR-19-0026
Keywords: neoadjuvant therapy, hepatocellular carcinoma, unresectable hepatocellular carcinoma, immunotherapy, targeted therapy
Citation: Goodsell KE, Tao AJ and Park JO (2025) Neoadjuvant therapy for hepatocellular carcinoma—priming precision innovations to transform HCC treatment. Front. Surg. 12:1531852. doi: 10.3389/fsurg.2025.1531852
Received: 21 November 2024; Accepted: 18 February 2025;
Published: 6 March 2025.
Edited by:
Tan To Cheung, The University of Hong Kong, Hong Kong SAR, ChinaReviewed by:
Tevfiktolga Sahin, İnönü University, TürkiyeCopyright: © 2025 Goodsell, Tao and Park. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kristin E. Goodsell, Z29vZHNrQHV3LmVkdQ==; Alice J. Tao, YWxpY2V0OEB1dy5lZHU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.