 Runjie Hou
Runjie Hou Jijun Wang1*
Jijun Wang1* Mingyue Du
Mingyue Du Zhenyu Dong
Zhenyu Dong
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Surg., 10 December 2024
Sec. Visceral Surgery
Volume 11 - 2024 | https://doi.org/10.3389/fsurg.2024.1465731
This article is part of the Research TopicState of the Art on Damage Control Surgery and ResuscitationView all articles
Introduction: The incidence of foreign bodies within the human body is uncommon, with thermometers representing an exceptionally rare subset of such cases. The management of these cases is particularly challenging due to the fragility of mercury thermometers and the toxic nature of their contents.
Case description: A 16-year-old male adolescent presented with a three-month history of persistent, dull pain localized to the right inguinal region. Diagnostic imaging, including an abdominal upright x-ray and CT scans, revealed the presence of an intra-abdominal foreign body, specifically a thermometer. The diagnosis was subsequently confirmed intraoperatively through laparoscopic exploration. The foreign body was successfully extracted via laparoscopic intervention. The patient's postoperative course was uneventful, leading to discharge on the second day following the procedure. A one-month follow-up examination revealed no complications.
Conclusion: A comprehensive literature review was conducted, focusing on cases involving thermometers as foreign bodies. The diagnostic and treatment experiences from the present case were integrated into this analysis. Based on these findings, a summary of diagnostic and treatment strategies for thermometer-related foreign body incidents has been formulated. It is recommended that an abdominal upright x-ray examination be employed as the primary diagnostic modality. The integrity and location of the thermometer, along with the presence of associated complications, should be considered as crucial factors in determining the most appropriate treatment approach. Furthermore, it is imperative to address the psychological and mental health aspects of these cases, particularly in adolescent patients.
Foreign bodies within the human organism present significant health risks, potentially leading to severe complications such as fistula formation, necrotizing pancreatitis due to direct organ perforation, vascular perforation-induced hemorrhage, and intestinal necrosis or obstruction resulting from luminal compression (1, 2). Mercury thermometers, owing to their fragile glass composition and the presence of toxic mercury, pose an even greater threat when broken, potentially causing more severe complications compared to other foreign objects. Prompt and accurate diagnosis, coupled with appropriate therapeutic intervention, is therefore of paramount importance in such cases. This study presents a successful case of laparoscopic extraction of a thermometer acting as a foreign body. A comprehensive review of pertinent literature has been conducted, and a summary of diagnostic and treatment strategies for thermometer-related foreign body incidents has been formulated.
A 16-year-old male adolescent presented to the gastrointestinal surgery department with a three-month history of dull pain localized to the right inguinal region. Physical examination in the supine position revealed a soft abdomen without tenderness. An abdominal upright x-ray was performed, revealing a high-density foreign body shadow in the lower abdomen, consistent with the appearance of a thermometer (Figure 1). Upon detailed medical history taking, the patient admitted to inserting a mercury thermometer through the urethra three months prior, initially refraining from seeking medical attention due to embarrassment. An abdominal computed tomography (CT) scan was subsequently conducted to precisely localize the thermometer (Figure 2). Based on these findings, a decision was made to proceed with laparoscopic exploration for removal of the foreign body. Following preoperative preparation, the patient underwent general anesthesia and laparoscopic exploration the following day. Upon entering the abdominal cavity, no active bleeding, purulent exudate, or effusion was observed. An intact mercury thermometer was identified in the right iliac fossa, floating freely within the abdominal cavity (Figure 3). A self-made specimen bag was utilized to enclose the thermometer (Figure 4), which was subsequently extracted through the left trocar port (Figure 5). A thorough examination of the abdominal organs revealed an old scar at the base of the bladder, while the remaining organs appeared intact. Bladder integrity was confirmed by instilling 200 milliliters of saline through a catheter, with no observed fluid leakage. The procedure was deemed successful, and the patient was discharged the following day.
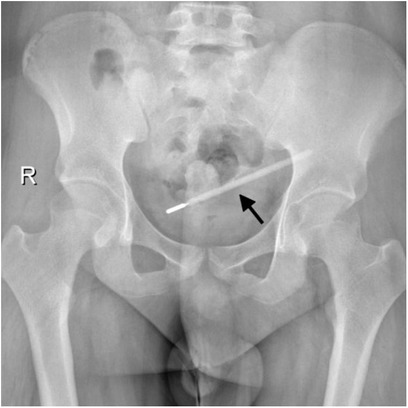
Figure 1. Abdominal upright x-ray showing a foreign body of a thermometer (the site pointed to by the arrow).

Figure 2. Ct scan showing intraperitoneal localization of the thermometer (the site pointed to by the arrow).
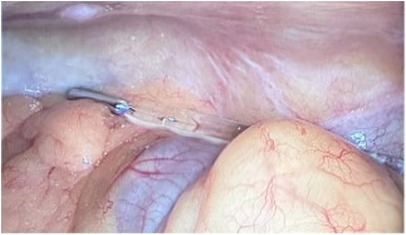
Figure 3. Exploration revealed an intact and free thermometer in the abdominal cavity.

Figure 4. Placing the thermometer in the self-made specimen bag.
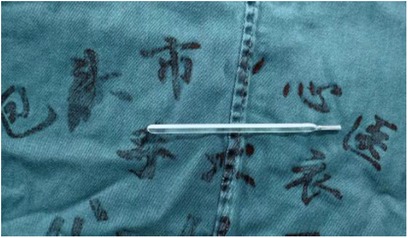
Figure 5. Removal of the thermometer.
A comprehensive literature search was conducted using the PubMed/MEDLINE database, focusing on case reports and original studies pertaining to intra-abdominal thermometer foreign bodies. The search encompassed publications from January 1, 2014, to June 28, 2024, without language restrictions. The search strategy employed the combination of terms [(thermometer) and (foreign body)]. This systematic approach yielded nine relevant articles, collectively reporting ten cases of thermometer foreign bodies. One article described two distinct cases of thermometer foreign bodies (Table 1).

Table 1. Studies on cases of foreign bodies related to thermometers throughout the literature.
Intra-abdominal foreign bodies are relatively uncommon occurrences. These foreign bodies can be classified into two categories based on their route of entry: (1) those that migrate into the abdominal cavity through perforation of natural hollow organs, such as the gastrointestinal, urinary, and reproductive tracts, and (2) those that enter directly through breaches in the skin (12). The presence of foreign bodies within the human organism poses significant health risks, potentially leading to severe complications. These complications include fistula formation, necrotizing pancreatitis due to direct organ perforation, hemorrhage resulting from vascular perforation, and intestinal necrosis or obstruction caused by compression and blockage of the intestinal lumen (1, 2). Prompt intervention is crucial upon the discovery of a foreign body to mitigate these risks.
The presence of thermometers as foreign bodies was initially documented in the mid-20th century, coinciding with the advocacy of vaginal temperature measurement for ovulation date estimation (13). In recent years, despite the gradual replacement of mercury thermometers with gallium alternatives due to environmental and toxicity concerns (14), mercury thermometers remain in use in many regions owing to their cost-effectiveness and superior accuracy. Consequently, cases of mercury thermometers as foreign bodies continue to be reported. Recent literature predominantly describes male patients inserting thermometers into the urethra for psychiatric reasons or sexual gratification, with a notable trend towards younger patients (Table 1). Thermometers, particularly those containing mercury, present unique challenges as foreign bodies compared to other objects. The fragility of their glass construction and the presence of mercury pose dual risks. While the potential for severe injury from broken glass is significant (14), it is noteworthy that based on previous reports and the findings of this case study, accidental intracorporeal thermometers have not been observed to rupture spontaneously, even after prolonged periods of up to 40 years within the body (4). This may be attributed to the thermometer's smooth shape, the protective nature of internal organs, and the lubrication provided by bodily fluids. However, the sharp configuration of thermometers renders them more susceptible to puncturing internal organs, potentially leading to fistula formation and perforation (3). The leakage of mercury from a ruptured thermometer presents an additional hazard. While the absorption rate of mercury through a healthy gastrointestinal tract is less than 0.01%, rendering mercury poisoning unlikely in cases of thermometer rupture within the gastrointestinal tract (15), the consequences of rupture within the abdominal cavity following perforation of a hollow organ would be severe. In such instances, peritoneal absorption of mercury could lead to central nervous system damage, manifesting as insomnia, fatigue, and memory loss, as well as peripheral nerve and kidney damage (16, 17). Furthermore, chronic inflammation resulting from mercury exposure could lead to the formation of difficult-to-heal fistulas, the development of granulomas, and intestinal obstruction (17).
The clinical manifestations resulting from the presence of a thermometer as a foreign body within the human organism are typically subtle, with the majority of patients remaining asymptomatic. This lack of apparent symptoms may be attributed to the thermometer's smooth surface, which minimizes irritation to internal organs. A comprehensive medical history, when obtainable, significantly enhances the formulation of diagnostic and treatment strategies. However, factors such as patient embarrassment and underlying mental health issues (3) often impede the acquisition of an accurate history of thermometer insertion. For instance, the patient in the present case initially exhibited reluctance to disclose the self-insertion of the thermometer. Nevertheless, the diagnosis of a thermometer as a foreign body can be established with relative ease, even in the absence of a detailed ingestion history. Based on previous case reports and the current study, it is evident that intra-abdominal thermometers can be readily identified on radiographic images due to their radiopaque nature and distinctive morphology. This characteristic allows for a preliminary diagnosis through a simple x-ray examination. Further evaluation of the spatial relationship between the thermometer and surrounding organs, as well as any associated injuries, can be achieved through CT scans.
Drawing from previous reports and the present case, a summary of treatment modalities for thermometer foreign bodies has been compiled (Figure 6). The initial step involves determining the integrity of the thermometer. In cases where the thermometer is found to be broken, immediate open surgery is warranted, with potential removal of contaminated organs if necessary. For intact thermometers that have not penetrated the bladder, uterus, digestive tract, or other hollow organs, endoscopic intervention is the preferred approach (5, 7). When the thermometer has penetrated hollow organs and entered the abdominal cavity, laparoscopic exploration and removal are favored to minimize surgical trauma. To mitigate the risk of thermometer breakage and its consequent serious complications during laparoscopic exploration, a protective cover can be fabricated to encase the thermometer prior to extraction. In scenarios where the thermometer is found to be firmly adherent to organs and difficult to separate, partially embedded in the intestinal tract or bladder, or has caused complications such as perforation or obstruction, prompt open surgery should be performed instead of attempting laparoscopic removal to avoid exacerbating the damage (10). Furthermore, addressing the patient's mental health is of paramount importance. Patients presenting with bladder and urethral foreign bodies, particularly male patients, often exhibit concomitant psychiatric disorders (18, 19), necessitating a comprehensive evaluation of their mental state. Adolescent patients, who are often driven by sexual curiosity (5), require appropriate psychological counseling to prevent the recurrence of foreign body insertion. This multifaceted approach ensures not only the physical removal of the foreign body but also addresses the underlying psychological factors that may have contributed to the incident.
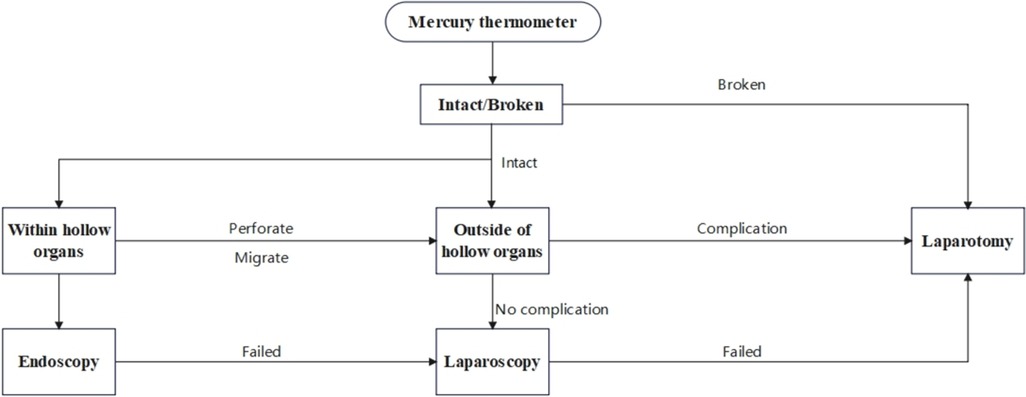
Figure 6. Management of mercury thermometer foreign bodies,recommended by the authors.
A systematic strategy for the diagnosis and management of thermometer foreign bodies has been formulated based on a comprehensive review of relevant literature from the past decade, coupled with the clinical insights gained from the present case study. Abdominal upright x-ray examination is recommended as the primary diagnostic modality. The integrity and location of the thermometer, along with the presence of any associated complications, are identified as critical factors influencing the selection of appropriate treatment strategies. Furthermore, significant emphasis is placed on the psychological and mental health status of patients, particularly adolescents, necessitating the provision of tailored psychological counseling and therapeutic interventions.
RH: Conceptualization, Formal Analysis, Software, Visualization, Writing – original draft, Writing – review & editing. JW: Conceptualization, Writing – review & editing. JG: Investigation, Software, Visualization, Writing – review & editing. MD: Formal Analysis, Visualization, Writing – review & editing. ZD: Software, Writing – review & editing. XS: Funding acquisition, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Bozorgmehr R, Bahadorinia M, Pouyanfar S, Ahmadinejad M, Bahri MH, Bagherpour JZ. A rare case of abdominal foreign bodies; laparoscopic removal of a sewing needle. Ann Med Surg (Lond). (2022) 82:104747. doi: 10.1016/j.amsu.2022.104747
2. Moreno Barrueco M, Berdugo Hurtado F, López Peña C, Bailon Gaona MC. Acute necrotizing pancreatitis secondary to a pancreatic foreign body. Rev Esp Enferm Dig. (2023) 116(7):392–3. doi: 10.17235/reed.2023.9868/2023
3. Tao C, Cao Y. Mercury thermometer as a rare cause of urinary tract foreign body: a case study. Asian J Surg. (2024) 47(8):3807–8. doi: 10.1016/j.asjsur.2024.04.138
4. Schulte K, Wolf HW. Occurrence of multiple fistulas decades after ingestion and neglect of numerous thermometers: a case report. Surg Case Rep. (2024) 10(1):4. doi: 10.1186/s40792-023-01801-w
5. Jiang C, Zhang T, Chen Y, Ke C. Self-insertion of a thermometer to the urinary bladder in a 12-year-old boy. Asian J Surg. (2023) 46(6):2370–1. doi: 10.1016/j.asjsur.2022.12.016
6. Yang L, Li W. Unusual cervical foreign body - a neglected thermometer for 5 years: a case report. World J Clin Cases. (2021) 9(30):9129–33. doi: 10.12998/wjcc.v9.i30.9129
7. Yang G, Li D, Sun L, Zhang Y, Xu A, Qian H. Transurethral cystoscopic removal foreign body (thermometer) with a stone extractor: a case. Urol Case Rep. (2019) 26:100959. doi: 10.1016/j.eucr.2019.100959
8. Bogdanovic J, Sekulic V, Kokovic T, Djozic S, Vulin D. Successful laparoscopic removal of a self-inflicted thermometer that spontaneously migrated into the peritoneal cavity. Urol J. (2017) 14(6):5071–2. doi: 10.22037/uj.v14i6.3828
9. Lambropoulos V, Fotoulaki M, Kepertis C, Neofytou A, Spyridakis I. An unusual foreign body within the appendix. Med J Malaysia. (2016) 71(5):298–9.28064301
10. Nie J, Zhang B, Duan YC, Hu YH, Gao XY, Gong J, et al. Intestinal obstruction due to migration of a thermometer from bladder to abdominal cavity: a case report. World J Gastroenterol. (2014) 20(9):2426–8. doi: 10.3748/wjg.v20.i9.2426
11. Dardamanis M, Balta L, Zacharopoulos V, Tatsi V, Tzima H. An unexpected foreign body (a thermometer) in the bladder: a case report. Urol Case Rep. (2014) 2(2):65–6. doi: 10.1016/j.eucr.2014.01.004
12. Luks B, Dworzyńska A, Dobrogowski M, Pomorski L. Discovery of a glass splinter in the abdominal cavity after an old impalement injury: a case report and literature review. Am J Case Rep. (2020) 21:e922599. doi: 10.12659/AJCR.922599
13. Krugman PI, Rieser C. Thermometer in the urinary bladder. Fertil Steril. (1952) 3(3):263–5. doi: 10.1016/S0015-0282(16)30907-4
14. Nadine A, Lois L, Michael S, David H, Patrick J, Amir K. Glass thermometer injuries: it is not just about the mercury. Pediatr Emerg Care. (2009) 25(10):645–7. doi: 10.1097/PEC.0b013e3181b920cc
15. Uysalol M, Parlakgül G, Yılmaz Y, Çıtak A, Uzel N. A 3 year-old male child ingested approximately 750 grams of elemental mercury. Balkan Med J. (2016) 33(4):467–9. doi: 10.5152/balkanmedj.2016.15197
16. Haas NS, Shih R, Gochfeld M. A patient with postoperative mercury contamination of the peritoneum. J Toxicol Clin Toxicol. (2003) 41(2):175–80. doi: 10.1081/CLT-120019134
17. Mazer-Amirshahi M, Bleecker ML, Barrueto F Jr. Intraperitoneal elemental mercury exposure from a mercury-weighted bougie. J Med Toxicol. (2013) 9(3):270–3. doi: 10.1007/s13181-013-0303-1
18. Rodríguez D, Thirumavalavan N, Pan S, Apoj M, Butaney M, Gross MS, et al. Epidemiology of genitourinary foreign bodies in the United States emergency room setting and its association with mental health disorders. Int J Impot Res. (2020) 32(4):426–33. doi: 10.1038/s41443-019-0194-z
Keywords: abdominal cavity, foreign body, adolescent, laparoscopy, mercury thermometer, management strategy
Citation: Hou R, Wang J, Guo J, Du M, Dong Z and Song X (2024) Case report and literature review: removal of a mercury thermometer from the abdomen of a 16-year-old boy under laparoscopy. Front. Surg. 11:1465731. doi: 10.3389/fsurg.2024.1465731
Received: 16 July 2024; Accepted: 11 November 2024;
Published: 10 December 2024.
Edited by:
Gabriel Sandblom, Karolinska Institutet (KI), SwedenReviewed by:
Javier Arredondo Montero, Complejo Asistencial Universitario de León (CHLeon), SpainCopyright: © 2024 Hou, Wang, Guo, Du, Dong and Song. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jijun Wang, d2FuZ2ppanVuMjAwNEBzaW5hLmNvbQ==
†This author share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.