 Jucai Li
Jucai Li Yanli Song
Yanli Song Lin-Feng Wang
Lin-Feng Wang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg. , 29 August 2024
Sec. Orthopedic Surgery
Volume 11 - 2024 | https://doi.org/10.3389/fsurg.2024.1443231
Background: Unilateral biportal endoscopic discectomy (UBED) is a widely accepted minimally invasive surgery for the treatment of lumbar degenerative diseases. However, some patients continue to have persistent low back pain (LBP) symptoms in the short and long term after surgery, which may be related to improper postoperative nursing and rehabilitation of patients. Further research is needed to determine whether continuous nursing can improve the symptoms of patients after UBED.
Methods: This study retrospectively enrolled 282 lumbar disc herniation (LDH) patients who underwent UBED in our hospital from January 2019 to January 2022. The patients were divided into two groups according to whether they accepted the continuous nursing program: 147 patients in the traditional nursing group and 135 patients in the continuous nursing group. Demographic characteristics, radiological parameters, and follow-up data of the patients were collected. Finally, the risk factors of LBP after UBED were analyzed.
Results: The visual analog scale (VAS) score of LBP in the continuous nursing group was 0.97 ± 1.159 at 3 months and 0.61 ± 0.954 at 12 months after operation, and VAS of leg pain was 0.23 ± 0.421 at 12 months after operation, which were better than those in the traditional nursing group (1.51 ± 1.313, 1.10 ± 1.076, 0.68 ± 0.788, respectively, p < 0.001) The Oswestry disability index (ODI) score of the continuous nursing group was lower than that of the traditional nursing group at 12 months after operation (7.36 ± 6.526 vs. 12.43 ± 6.942, p < 0.001). The rehabilitation completion (7.98 ± 1.857), efficacy satisfaction (9.13 ± 1.101), and re-herniation worry scores (1.97 ± 1.217) in the continuous nursing group were better than those in the traditional nursing group (4.14 ± 3.066, 8.28 ± 1.240, 2.79 ± 1.973, respectively, P < 0.001). The re-herniation rate within 1 year was similar between the two groups (3/135 vs. 2/147, p = 0.673). No incision infection occurred. Multivariate regression analysis showed that risk factors for persistent LBP at 3-month follow-up were degenerative disc [odds ratio (OR): 2.144, CI: 1.306–3.519, p = 0.03], Pfirrmann grade (OR: 3.073, CI: 1.427–6.614, p = 0.04), and surgical time (OR: 0.969, CI: 0.937–1.003, p = 0.74). At the 12-month follow-up, the risk factors for persistent LBP were preoperative VAS of the legs (OR: 1.261, CI: 1.000–1.591, p = 0.05) and Pfirrmann grade (OR: 3.309, CI: 1.460–7.496, p = 0.04).
Conclusion: Continuous nursing programs can improve the symptoms of short-term and long-term persistent LBP in patients after UBED, enhance the completion of rehabilitation training after UBED, alleviate patients' concerns about recurrence, and improve patients' satisfaction.
Lumbar disc herniation (LDH) is the main cause of low back pain (LBP) and leg pain. This pain is often severe and seriously affects the patient's work and quality of life (1). For patients with LDH who fail to respond to conservative treatment, surgery is often performed to remove part of the herniated intervertebral disc and relieve the compression of the lumbar plexus nerve root, thereby alleviating the pain symptoms of patients (2). To reduce the damage to soft tissue, various endoscopic techniques have been developed for spine surgery in recent years (3). Unilateral biportal endoscopic discectomy (UBED) is a representative minimally invasive surgery characterized by a short learning curve, sufficient decompression range, and low recurrence rate (4). The unilateral biportal endoscopic (UBE) technique involves creating two working channels for surgical manipulation through the gap between the multifidus muscle and the spinous process. One channel is inserted into the arthroscope to provide the operative field, and the other adjacent mini-incision channel is used for surgical manipulation to relieve nerve compression. It has been reported that patients with complete nerve root decompression have a 99.5% reduction in lower extremity pain symptoms (5).
However, after simple discectomy surgery, some patients experience persistent LBP, which seriously affects their postoperative rehabilitation progress and satisfaction (6). Although there were no separate reports on the rate of LBP relief or the probability of concurrent LBP after UBED, some studies have shown that the probability of persistent LBP after minimally invasive lumbar discectomy is approximately 8.4%–36.6% (7–9). The etiology of this type of persistent postoperative LBP is unclear. It is worth mentioning that there is a growing consensus that combining postoperative rehabilitation exercise with physical therapy, psychological intervention, and the use of painkillers can significantly improve treatment outcomes (10, 11). Early rehabilitation helps reduce muscle loss in the multifidus, erector spinae, and other lumbar back, enhance the stability of the lumbar spine (12), and promote the patients to return to normal life and work after minimally invasive lumbar surgery (13). However, due to social, family, economic, and other factors, patients are prone to some situations that are not conducive to the recovery of the disease in the postoperative recovery process. Issues such as poor compliance, inconsistent rehabilitation, failure to follow the step-by-step principle, and an incorrect understanding of the disease lead to poor long-term patient satisfaction after surgery.
Under the traditional nursing model, the hospitalization period for patients was only a few days, and the nursing care stopped on the day of discharge. However, the success of orthopedic surgery usually does not mean the end of treatment (14). Although our traditional model informs patients and their families that rehabilitation training should continue after discharge, the effectiveness of this post-discharge rehabilitation depends on the patient’s medical conditions and economic limitations. Only a few patients regularly follow the hospital rehabilitation guidance after discharge. In addition, the patient's psychological state can significantly influence postoperative rehabilitation. Negative attitudes and beliefs about chronic low back pain may lead to catastrophic thoughts and avoidance behaviors (15).
Continuous nursing is based on the rehabilitation characteristics of patients after discharge, through a variety of information means and personnel cooperation to establish intervention channels, so that patients can receive professional nursing intervention for a long time after discharge, promote rehabilitation, and reduce postoperative complications of patients (16). To improve the efficacy of UBED, our hospital designed a set of postoperative continuous nursing programs to guide and supervise the rehabilitation process of patients after UBED for 12 months. The purpose of this study is to investigate whether this continuous nursing program can improve the short-term and long-term LBP symptoms of patients after UBED and improve patient satisfaction.
Patients who underwent UBED for lumbar disc herniation in our hospital from January 2019 to January 2022 were included in this study. Inclusion criteria included (a) patients with lumbar disc herniation who failed to respond to conservative treatment for more than 2 months and (b) complete medical records and imaging data were available. Exclusion criteria included (a) combined with ankylosing spondylitis, gluteal fasciitis, fractures, and other diseases leading to persistent LBP; (b) patients with previous lumbar surgery; (c) patients with cardiovascular and cerebrovascular diseases and poor physical conditions; and (d) deep vein thrombosis of the lower extremities, combined with peripheral neuropathy and other diseases affecting the patient's motor function. All patients received rehabilitation training guidance before discharge and chose whether to accept a postoperative transitional care program according to their wishes. The patients were followed up at 1, 3, 6, and 12 months after operation. A total of 312 patients met the criteria. Thirty-five of these patients were excluded because they withdrew from supervised training or did not complete follow-up. In this study, 147 patients were finally included in the traditional nursing group without receiving the transitional care scheme. One hundred and thirty-five patients received a complete continuing nursing program and were included in the continuing nursing group. Among them, two patients in the routine nursing group and three patients in the continuous nursing group experienced re-herniation and underwent revision surgery during the 1-year follow-up period, and their clinical efficacy was not included in the statistics, which was only used to compare the recurrence rate of patients between the two groups.
After general anesthesia, the patient was placed in the prone position. A 5 mm entry point was cut at 1 cm above and below the point. The cephalic entry point was used as the observation port, and the caudal entry point was used as the operation port. After the blunt separation of the paraspinal muscles, a dilator was inserted to expand the channel. When the channels were satisfactory, the arthroscope was inserted into the viewing port. The next step is to look for the lower margin of the lamina of the upper vertebral body. After hemostasis, the soft tissue covering the bone and lamina space was removed. Part of the lamina and facet joints were then removed. The ligamentum flavum was carefully bitten and removed. After retracting the nerve root and exposing the disc, a discectomy was performed, and the annulus fibrosus was cauterized with bipolar electrocoagulation to cause it to shrink and form. Finally, the incision was sutured by hemostasis.
In the traditional nursing group, patients were informed of the matters to be attended to upon discharge, and a staged rehabilitation training program was informed and implemented by patients upon discharge. The web page description for rehabilitation was provided for patients to review anytime. The follow-up review was scheduled and informed by telephone. If the discomfort becomes worse, the frequency of follow-up can be increased.
In the continuous nursing group, the rehabilitation process after discharge was supervised and guided by a continuous nursing team consisting of specialist spinal nurses, spinal surgeons, and rehabilitation physicians. All patients joined the WeChat group and established real-time contact with the nursing team. The work content of the continuous nursing group was divided into three parts, including stage rehabilitation training, disease consultation, and psychological intervention.
1. Stage rehabilitation training: According to the time characteristics of disc recovery after minimally invasive discectomy surgery, the postoperative rehabilitation training of patients was divided into four stages: Stage 1, 0–2 weeks; Stage 2, 2–8 weeks; Stage 3, 8–16 weeks; and Stage 4, after 16 weeks. All patients entered the WeChat group at the corresponding period according to the rehabilitation stage. The rehabilitation training was supervised and guided by spinal specialist nurses and rehabilitation physicians in each chat group. The patients were supervised by the chat group, including video, characters, or voice, and each patient completed the appropriate rehabilitation training according to the stage missions and goals. Patients in the group spoke freely, communicated with each other, and answered and comforted other patients' questions. Missions and goals were established in Table 1.
2. Disease consultation: Provide consultation services and drug guidance for patients with LBP and leg pain during the rehabilitation process and timely answer the patient's doubts about the disease.
3. Psychological intervention: Encourage patients to carry out rehabilitation training. Provide guidance on postoperative living inconveniences. Organize patient exchange activities every month to share treatment and rehabilitation experience. Provide psychological counseling related to illness.
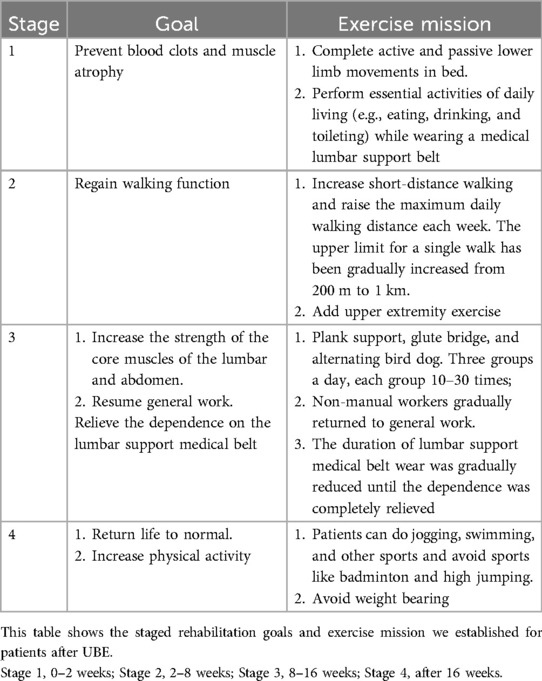
Table 1. Stage rehabilitation goal and mission.
Data collection included three parts: demographic characteristics, radiological parameters, and follow-up changes. (1) Demographic characteristics: We collected the information of patients by reviewing the medical records, including age, gender, body mass index (BMI), smoking or drinking status, hypertension, diabetes, preoperative visual analog scale (VAS) pain scores of low back and leg, preoperative Oswestry disability index (ODI) scores, surgical level, surgical times, and estimated blood loss. (2) Radiological parameters: These included the number of degenerative changes disc (Pfirrmann grade >2), Pfirrmann grade (disc of herniation) (17), Modic change (18), fatty infiltration of the paravertebral muscles (19), edema of lumbodorsal fascia in MRI, and facet joint preservation rate (20). (3) Follow-up changes: Length of stay, VAS scores of LBP, and leg pain were evaluated at 3 months and 12 months after operation, ODI score at 12 months after operation, and re-herniation at 12 months after operation. At the 12-month follow-up, we set three self-estimated scores, including rehabilitation completion score, efficacy satisfaction score, and re-herniation worry score, which was used to assess the degree of patient approval of the surgical effect. The maximum score for each item is 10 points. The rehabilitation completion score is the patient's self-estimated of the completion of rehabilitation training. Efficacy satisfaction score is a self-evaluation of the efficacy of surgery and the improvement of symptoms within 1 year. The re-herniation worry score reflected the worry grade about the recurrence of lumbar disc herniation. Unlike the previous two scores, higher scores on this scale indicate more worry. Finally, we used logistic regression to analyze the risk factors of patients with persistent LBP (VAS >3) at 3 and 12 months after surgery. Variables including age, gender, BMI, and preoperative VAS pain scores of the low back and legs, number of degenerative changes disc, Pfirrmann grade, Modic change, fatty infiltration of the paravertebral muscles, edema of lumbodorsal fascia, and facet joint preservation rate were included in the analysis.
Statistical analysis was performed using SPSS 23.0 for Windows (IBM, Armonk, NY, USA). The continuous variables in the two groups were analyzed with the use of a one-way analysis of variance, and the results are expressed as means ± standard deviations. The chi-square test was used to compare the count data. p < 0.05 was considered statistically significant. Finally, the risk factors model of LBP was established by backward stepwise regression.
A total of 282 patients were included in this study. Five of these patients experienced re-herniation within 1 year, and their clinical results were used only to compare the re-herniation rate between the two groups. There were 145 patients in the traditional nursing group and 132 patients in the continuous nursing group, whose clinical outcomes were included in the statistical analysis. The average age was 44.4 ± 16.86 years in the traditional nursing group and 42.1 ± 12.76 years in the continuous nursing group. There were no significant differences in age, gender, BMI, and prevalence of underlying diseases between the two groups. Preoperative assessment of symptoms was similar in the two groups. Preoperative VAS (back) was 4.25 ± 1.516 in the traditional nursing group and 4.03 ± 1.446 in the continuous nursing group (p = 0.223). Preoperative VAS (leg) and preoperative ODI also had no statistical difference. Surgical records, including surgical level, surgical time, and estimated blood loss, were not significantly different (Table 2).
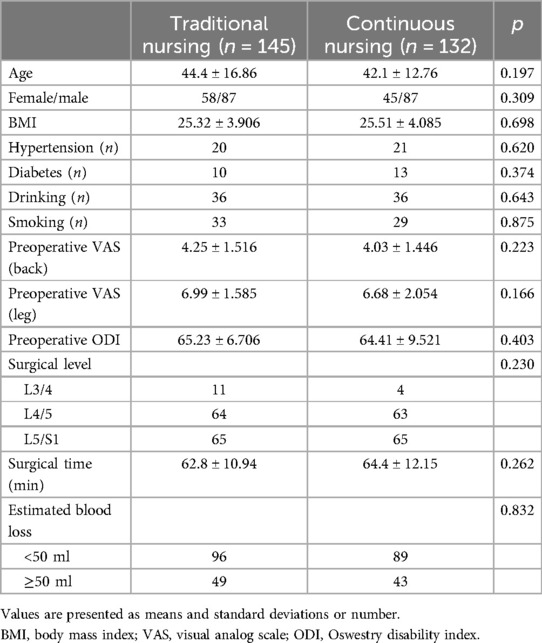
Table 2. Demographic characteristics.
There was no difference between the two groups in the number of degenerate discs, Pfirrmann grades, Modic changes, fatty infiltration of muscle, or edema of lumbodorsal fascia. Lumbar CT after surgery showed that the facet joint preservation rate was similar between the two groups (Table 3).
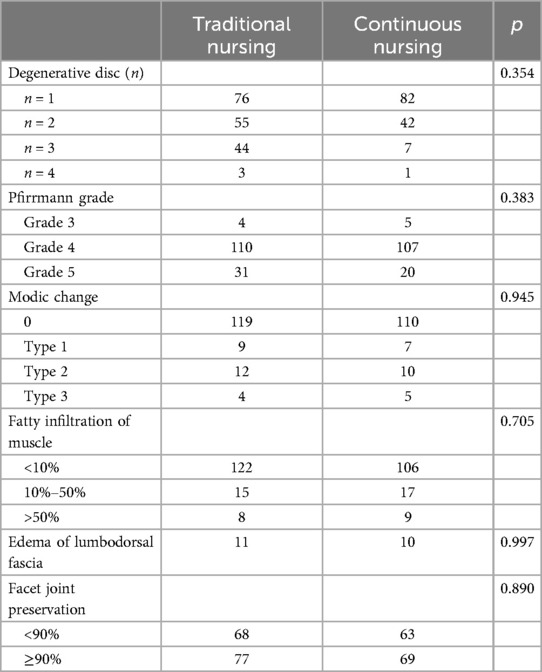
Table 3. Radiological parameters difference between the two groups.
Table 4 presents the VAS changes and patients' satisfaction after surgery. There was no significant difference in the length of stay in the hospital between the two groups. However, at the 3-month follow-up, the VAS score of LBP in the traditional nursing group (1.51 ± 1.313) was higher than that in the continuous nursing group (0.97 ± 1.159) ( p < 0.001). VAS of leg pain relief was similar between the two groups (p = 0.689). At the 12th-month follow-up, there were significant differences in symptom relief assessment indexes between the two groups. The VAS score of LBP was 1.10 ± 1.076 in the traditional nursing group and 0.61 ± 0.954 in the continuous nursing group. The VAS score of leg pain was 0.68 ± 0.788 in the traditional nursing group and 0.23 ± 0.421 in the continuous nursing group. When the patient’s daily activity function was assessed, the ODI score was different between the two groups (12.43 ± 6.942 vs. 7.36 ± 6.526, p < 0.001). In terms of patient self-estimated scores, there were significant differences between the two groups. The rehabilitation completion score was 4.14 ± 3.066 in the traditional nursing group and 7.98 ± 1.857 in the continuous nursing group, and the efficacy satisfaction score was 8.28 ± 1.240 in the traditional nursing group and 9.13 ± 1.101 in the continuous nursing group. The re-herniation worry score was 2.79 ± 1.973 in the traditional nursing group and 1.97 ± 1.217 in the continuous nursing group. There was no significant difference in the re-herniation rate between the two groups. The re-herniation rate was 2/147 in the traditional nursing group and 3/135 in the continuous nursing group, both of which were kept at a low level, and there was no difference between the two groups.
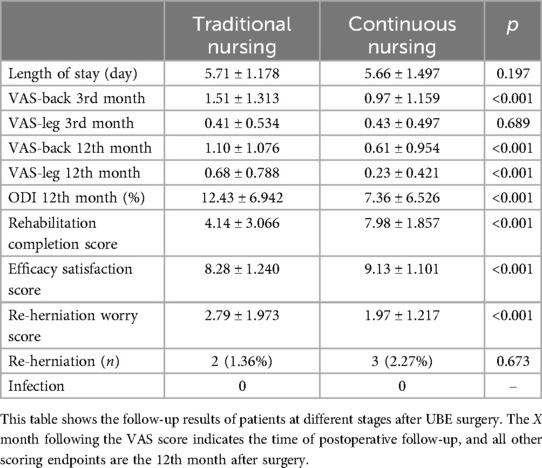
Table 4. Follow-up result of VAS changes, ODI, and self-estimated scores.
Logistic regression analysis (Tables 5, 6) showed that the risk factors of persistent LBP at 3 months (short-term) were the number of degenerative discs [odds ratio (OR): 2.144, CI: 1.306–3.519, p = 0.03], Pfirrmann grade (OR: 3.073, CI: 1.427–6.614, p = 0.04), and surgical time (OR: 0.969, CI: 0.937–1.003, p = 0.74). During the 12-month long-term follow-up, the risk factors for LBP were preoperative VAS (legs) (OR: 1.261, CI: 1.000–1.591, p = 0.05) and Pfirrmann grade (OR: 3.309, CI: 1.460–7.496, p = 0.04).
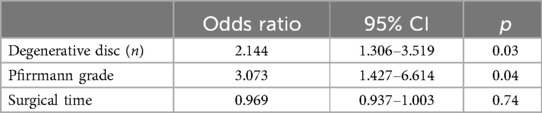
Table 5. Risk factors for short-term persistent LBP.

Table 6. Risk factors for long-lasting LBP.
The results of this study show that continuous nursing can improve the short-term and long-term LBP symptoms of patients after UBED. In addition, at the 12th-month follow-up, the continuous nursing group showed better activity function, with an ODI score of 7.36 ± 6.526, which was significantly lower than that of the traditional nursing group (4.14 ± 3.066). Through a series of methods of continuous nursing, we significantly increased the completion degree of rehabilitation after surgery, improved the compliance of patients, and improved long-term satisfaction (Table 4).
Step therapy for LDH is the accepted treatment strategy at present, and single discectomy is the median plan of step therapy, which is suitable for most patients with LDH (21). However, recurrent LBP can occur in 25%–36.6% of patients after minimally invasive lumbar discectomy (9, 22). LBP seriously affects patients’ normal work and quality of life, exacerbates the use of painkillers (23), and reduces patient satisfaction with surgery and efficacy (24). There are many reasons for chronic LBP in patients after lumbar surgery. According to the difference of source tissue, it can be divided into intervertebral disc source, paravertebral muscle source, and ligament injury. Multivariate analysis suggested that chronic LBP may be associated with disc height reduction, re-herniation, Modic changes, fat infiltration of paravertebral muscle, lumbar dorsal fascia edema, and lumbar facet joint osteoarthritis (5, 25). We suggest that a longer operation time may indicate that the patient is obese or that there are difficulties in the operation, which can cause more severe muscle damage and lead to longer back pain in the short term (Table 5). Although removal of a herniated lumbar disc can significantly relieve symptoms of leg pain, there is limited improvement in symptoms of low back pain (26). There are still some difficulties in diagnosing the etiology of LBP. It is worth mentioning that sonography measures can explore the multifidus and erector spinae muscles dynamically and non-invasively. A study used ultrasound to investigate the thickness and changes of the multifidus and erector spinae muscles in sitting and lying positions for the prediction and diagnosis of pain etiology in patients with chronic low back pain (27). Improving LBP after lumbar surgery, improving lower limb function, and reducing postoperative complications are the main objectives of postoperative nursing (28).
Two important means of continuous nursing are supervised rehabilitation training and intervention of surface emotions. A large number of studies have shown that continuous nursing can improve the joint function of patients after knee replacement and hip replacement by enhancing postoperative rehabilitation training, the completion of rehabilitation training, and the joint function of patients after knee replacement and hip replacement (29, 30). In addition, the continuous nursing group can timely understand the psychological state of patients and carry out necessary interventions through a variety of means, relieve the anxiety and fear of patients, and effectively improve the quality of life of patients (31).
Rehabilitation training is the key method for patients after lumbar discectomy surgery. Postoperative rehabilitation training can improve blood circulation, prevent muscle atrophy, enhance strength, increase spinal stability, and improve quality of life (32). Afzal et al. (33) conducted a meta-analysis and found that postoperative rehabilitation training was recommended to start 1–2 months after surgery and last for 3 months and postoperative rehabilitation training could significantly improve patients' long-term pain scores. However, the study did not consider the effect of different surgical methods on spinal stability. The start time, duration, and exercise intensity of lumbar non-fusion postoperative rehabilitation are still not uniform and need to be further optimized. At present, there are many rehabilitation training programs after lumbar surgery, but most of them are training programs after lumbar fusion (34, 35). After fusion surgery, the muscle destruction is large, but the spinal stability is high, and the risk of recurrence is very low. Therefore, the rehabilitation training program after fusion mostly suggests that patients go to the ground early and gradually resume daily life. Unlike fusion surgery, after simple discectomy, the nucleus pulposus is partially preserved, and the annulus fibrosus has a longer healing period (36, 37). Those patients are characterized by minimal muscle destruction and better spinal stability, while the likelihood of re-herniation of the nucleus pulposus is higher (32). Although the incision of UBED healed well within 14 days after operation, many patients still maintained a worried attitude toward rehabilitation exercise because they were worried about re-herniation (38, 39). In the traditional nursing group, although each patient received good rehabilitation education and training before discharge, such a short period of training seems to be difficult to achieve satisfactory results.
The healing cycle of muscles, ligaments, and bones after orthopedic surgery is longer, and less or later rehabilitation training is often thought to lead to a poor prognosis, including local surgical pain and joint stiffness (40). Continuous nursing is thought to improve postoperative outcomes in orthopedic patients (41). Based on the characteristics of physiological structure recovery of patients after UBED, we established a series of staged rehabilitation training guidance in combination with rehabilitation medicine experts. However, in the previous outpatient follow-up process, it was found that the patient's compliance was lacking, it was difficult to consciously complete the appropriate rehabilitation training action, and there was resistance to rehabilitation training. Therefore, we set up an oversight group consisting of senior nurses, spine surgeons, and rehabilitation medicine physicians. Postoperative continuous nursing was provided to patients, rehabilitation training was supervised, psychological guidance and medication advice were provided outside the hospital, and a patient communication community was established to improve the outcome of patients after UBED. This study retrospectively analyzed the population who had previously participated in this program. It is found that continuous nursing can significantly improve postoperative persistent LBP and improve the quality of life of patients. Schwartz et al. (42) found that rehabilitation exercise after spinal surgery can reduce patients' anxiety and improve the recovery trajectory of patients after spinal surgery and recommended that patients exercise as early as possible and persist for a long time after spinal surgery. Recently, a study on the exercise mode of patients after percutaneous endoscopic lumbar discectomy found that although the training mode was designed according to the structure of the lumbar dynamic chain and the postoperative period did not increase the multifidus muscle of patients, it could promote the rehabilitation of patients and improve the activity score of patients at 6 months compared with the conventional lumbar and back muscle exercise (43). This new rehabilitation mode combines the chain movement mode of the waist, hip, and leg and provides a new idea for the rehabilitation mode of LDH in the future. Targeted therapeutic exercise can improve the long-term prognosis of patients with chronic neck pain and improve muscle and soft tissue injury (44).
It is important to note that persistent LBP is often associated with social and psychological factors. In the process of continuous nursing, we found that patients paid more attention to the condition consultation service and psychological counseling service. Fear-avoidance behaviors, kinesiophobia, and anxiety were common in patients after minimally invasive lumbar surgery. It will cause great interference to the rehabilitation process of patients. In encouraging the rehabilitation exercise of patients after lumbar surgery, the potential obstacles caused by psychological and social factors should also be alleviated (45). A previous study found that it was postoperative, rather than preoperative, fear beliefs about exercise that were associated with improved postoperative pain, disability, and quality of life. The researchers recommend screening patients for fear of exercise after cervical and lumbar surgery and incorporating cognitive behavioral techniques into postoperative rehabilitation of high-risk spinal patients (45). Another advantage, continuous nursing can reduce the economic burden of patients through family support (46).
Most of the traditional lumbar postoperative patients recover at home after discharge, and the wound healing, symptom recovery, and condition change all depend on outpatient review. A small number of patients go to community hospitals or rehabilitation hospitals for post-discharge rehabilitation treatment, which has high time and economic cost and low relative benefit. With the development of social information, the nursing mode after discharge has also been reformed. Professional nursing staff can continue nursing care with patients through various applications such as Wechat. The use of graphics, video, telephone communication, and other ways to answer patient concerns guides the rehabilitation process of patients and enriches the content of continued nursing (47, 48). It is especially beneficial for patients after orthopaedic surgery, who need to undergo a long-term rehabilitation process after discharge. High-quality popular science videos and articles can effectively increase patients' understanding of the disease, enhance patients' confidence in rehabilitation, and timely detect and intervene in poor prognosis. The Internet-based continuous nursing can simplify and enhance the medical care service after orthopedic surgery and achieve cost reduction and efficiency increase.
This study describes a continuous nursing program for the lumbar spine after UBED, focusing on the three key issues of stage rehabilitation training, disease consultation, and psychological intervention after UBED and establishing a convenient contact channel to guide and help patients. Compared with the traditional post-discharge nursing model, continuous nursing effectively improved the short- and long-term LBP symptoms of patients after UBED, reduced the mobility disorders of patients, improved the satisfaction of patients with surgery, and did not increase the probability of re-herniation of patients. Risk factor analysis of LBP in UBED also showed that patients with more and more severe disc degeneration and severe lower extremity symptoms before surgery were more likely to have persistent LBP symptoms after surgery. This also suggests that nursing staff, for patients with such high-risk factors, should strengthen postoperative nursing and follow-up, try to improve patient symptoms, and improve patient satisfaction.
Based on the results of this study, we recommend continuing nursing for patients after minimally invasive lumbar surgery. Through WeChat, telephone, and other means of communication and supervision, patients received staged rehabilitation training (Table 1), to provide a long-term consulting platform and timely intervention in patients with negative emotions.
Our study has some limitations: (1) This study provided a model of continuous nursing after UBED. However, due to policy issues, the cost and effectiveness were not considered. (2) This study is a single-center retrospective study and only discusses patients after UBED. Further research is needed to verify the clinical significance of transitional care for patients after other LDH surgical methods and patients in different medical centers. (3) In this study, the use of the WeChat platform to clock in supervision can not effectively supervise the completion of the actual rehabilitation training of patients. (4) Although most of our results were statistically significant, we lacked an exploration of the minimal clinically important difference (MCID) of these results. Whether the clinical significance of continuous nursing can be further improved remains to be discussed.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the Medical Ethics Committee of the Third Hospital of Hebei Medical University. The studies were conducted in accordance with the local legislation and institutional requirements. The Ethics Committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because Informed consent was obtained from the subjects by telephone.
JL: Data curation, Investigation, Methodology, Project administration, Software, Supervision, Validation, Writing – original draft, Writing – review & editing. YS: Data curation, Investigation, Methodology, Resources, Writing – review & editing. LW: Investigation, Methodology, Project administration, Resources, Software, Writing – review & editing. DS: Investigation, Methodology, Project administration, Writing – review & editing. LW: Conceptualization, Data curation, Formal Analysis, Project administration, Resources, Validation, Writing – original draft, Writing – review & editing.
The authors declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Benzakour T, Igoumenou V, Mavrogenis AF, Benzakour A. Current concepts for lumbar disc herniation. Int Orthop. (2019) 43:841–51. doi: 10.1007/s00264-018-4247-6
2. Coumans JV. Comparing surgical approaches to lumbar disc herniations. J Neurol Neurosurg Psychiatry. (2017) 88:1003. doi: 10.1136/jnnp-2017-316108
3. Ahn Y. Current techniques of endoscopic decompression in spine surgery. Ann Transl Med. (2019) 7:S169. doi: 10.21037/atm.2019.07.98
4. He D, Cheng X, Zheng S, Deng J, Cao J, Wu T, et al. Unilateral biportal endoscopic discectomy versus percutaneous endoscopic lumbar discectomy for lumbar disc herniation: a systematic review and meta-analysis. World Neurosurg. (2023) 173:e509–20. doi: 10.1016/j.wneu.2023.02.087
5. Chen Z, He L, Di J, Huang L, Feng F, Yang B, et al. Lumbar facet joint osteoarthritis as the underlying reason for persistent low back pain after minimally invasive discectomy. Arch Orthop Trauma Surg. (2023) 143:3811–21. doi: 10.1007/s00402-022-04595-y
6. Hiranaka Y, Miyazaki S, Inoue S, Ryu M, Yurube T, Kakutani K, et al. Preoperative low back pain affects postoperative patient satisfaction following minimally invasive transforaminal lumbar interbody fusion surgery. Asian Spine J. (2023) 17:750–60. doi: 10.31616/asj.2022.0313
7. Peul WC, van den Hout WB, Brand R, Thomeer RT, Koes BW. Prolonged conservative care versus early surgery in patients with sciatica caused by lumbar disc herniation: two year results of a randomised controlled trial. Br Med J. (2008) 336:1355–8. doi: 10.1136/bmj.a143
8. Shamim MS, Parekh MA, Bari ME, Enam SA, Khursheed F. Microdiscectomy for lumbosacral disc herniation and frequency of failed disc surgery. World Neurosurg. (2010) 74:611–6. doi: 10.1016/j.wneu.2010.06.016
9. Zhong D, Ke ZY, Chen Q, Liu Y, Lin L, Wang Y. A clinical nomogram for predicting the residual low back pain after percutaneous endoscopic surgery for lumbar disc herniation. Int Orthop. (2023) 47:819–30. doi: 10.1007/s00264-022-05658-w
10. Oosterhuis T, Costa LO, Maher CG, de Vet HC, van Tulder MW, Ostelo RW. Rehabilitation after lumbar disc surgery. Cochrane Database Syst Rev. (2014) 2014:D3007. doi: 10.1002/14651858.CD003007.pub3
11. Williamson E, White L, Rushton A. A survey of post-operative management for patients following first time lumbar discectomy. Eur Spine J. (2007) 16:795–802. doi: 10.1007/s00586-006-0207-8
12. Kose HC, Aydin SO. Magnetic resonance imaging evaluation of multifidus muscle in patients with low back pain after microlumbar discectomy surgery. J Clin Med. (2023) 12(19):6122. doi: 10.3390/jcm12196122
13. Huysmans E, Goudman L, Van Belleghem G, De Jaeger M, Moens M, Nijs J, et al. Return to work following surgery for lumbar radiculopathy: a systematic review. Spine J. (2018) 18:1694–714. doi: 10.1016/j.spinee.2018.05.030
14. Jonas SC, Whitehouse MR, Bick S, Bannister GC, Baker RP. An 18-year comparison of hybrid total hip replacement and Birmingham hip resurfacing in active young patients. Hip Int. (2019) 29:630–7. doi: 10.1177/1120700018814710
15. Darlow B, Perry M, Stanley J, Mathieson F, Melloh M, Baxter GD, et al. Cross-sectional survey of attitudes and beliefs about back pain in New Zealand. BMJ Open. (2014) 4:e4725. doi: 10.1136/bmjopen-2013-004725
16. Garcia AN, Simon CB, Yang ZL, Niedzwiecki D, Cook CE, Gottfried O. Classification of older adults who underwent lumbar-related surgery using pre-operative biopsychosocial predictors and relationships with surgical recovery: an observational study conducted in the United States. Health Soc Care Community. (2022) 30:e1570–84. doi: 10.1111/hsc.13584
17. Pfirrmann CW, Metzdorf A, Zanetti M, Hodler J, Boos N. Magnetic resonance classification of lumbar intervertebral disc degeneration. Spine (Phila Pa 1976). (2001) 26:1873–8. doi: 10.1097/00007632-200109010-00011
18. Modic MT, Masaryk TJ, Ross JS, Carter JR. Imaging of degenerative disk disease. Radiology. (1988) 168:177–86. doi: 10.1148/radiology.168.1.3289089
19. Faur C, Patrascu JM, Haragus H, Anglitoiu B. Correlation between multifidus fatty atrophy and lumbar disc degeneration in low back pain. BMC Musculoskelet Disord. (2019) 20:414. doi: 10.1186/s12891-019-2786-7
20. Pao JL, Lin SM, Chen WC, Chang CH. Unilateral biportal endoscopic decompression for degenerative lumbar canal stenosis. J Spine Surg. (2020) 6:438–46. doi: 10.21037/jss.2020.03.08
21. Zhang AS, Xu A, Ansari K, Hardacker K, Anderson G, Alsoof D, et al. Lumbar disc herniation: diagnosis and management. Am J Med. (2023) 136:645–51. doi: 10.1016/j.amjmed.2023.03.024
22. Parker SL, Mendenhall SK, Godil SS, Sivasubramanian P, Cahill K, Ziewacz J, et al. Incidence of low back pain after lumbar discectomy for herniated disc and its effect on patient-reported outcomes. Clin Orthop Relat Res. (2015) 473:1988–99. doi: 10.1007/s11999-015-4193-1
23. Kalakoti P, Hendrickson NR, Bedard NA, Pugely AJ. Opioid utilization following lumbar arthrodesis: trends and factors associated with long-term use. Spine (Phila Pa 1976). (2018) 43:1208–16. doi: 10.1097/BRS.0000000000002734
24. Lehrich BM, Goshtasbi K, Brown NJ, Shahrestani S, Lien BV, Ransom SC, et al. Predictors of patient satisfaction in spine surgery: a systematic review. World Neurosurg. (2021) 146:e1160–70. doi: 10.1016/j.wneu.2020.11.125
25. Wang H, Zhou X, Li X, Xu Z, Meng Q, Wang J, et al. Risk factors for short-term and long-term low back pain after transforaminal endoscopic lumbar discectomy. J Pain Res. (2023) 16:3505–17. doi: 10.2147/JPR.S422595
26. Levi D, Carnahan D, Horn S, Levin J. Is a history of severe episodic low back pain an indicator of a discogenic etiology? Pain Med. (2018) 19:1334–9. doi: 10.1093/pm/pnx147
27. Sanchez RE, Alonso PJ, Munoz FA, Battaglino A, Castaldo M, Cleland JA, et al. Reliability of sonography measures of the lumbar multifidus and transversus abdominis during static and dynamic activities in subjects with non-specific chronic low back pain. Diagnostics (Basel). (2021) 11(4):632. doi: 10.3390/diagnostics11040632
28. Braxton EJ, Wohlfeld BJ, Blumenthal S, Bozzio A, Buttermann G, Guyer R, et al. Postoperative care pathways following lumbar total disc replacement: results of a modified Delphi approach. Spine (Phila Pa 1976). (2019) 44 Suppl 24:S1–12. doi: 10.1097/BRS.0000000000003276
29. Westby MD, Brittain A, Backman CL. Expert consensus on best practices for post-acute rehabilitation after total hip and knee arthroplasty: a Canada and United States Delphi study. Arthritis Care Res (Hoboken). (2014) 66:411–23. doi: 10.1002/acr.22164
30. Gonzalez-Quevedo D, Diaz-Ramos M, Chato-Astrain J, Sanchez-Porras D, Tamimi I, Campos A, et al. Improving the regenerative microenvironment during tendon healing by using nanostructured fibrin/agarose-based hydrogels in a rat achilles tendon injury model. Bone Joint J. (2020) 102-B:1095–106. doi: 10.1302/0301-620X.102B8.BJJ-2019-1143.R2
31. Carroll A, Dowling M. Discharge planning: communication, education and patient participation. Br J Nurs. (2007) 16:882–6. doi: 10.12968/bjon.2007.16.14.24328
32. Zhu Y, Xia S, Yang W, Shi F, Ji H. Early efficacy of postoperative rehabilitation training for lumbar disc herniation. BMC Sports Sci Med Rehabil. (2023) 15:97. doi: 10.1186/s13102-023-00704-5
33. Afzal K, Khattak HG, Sajjad AG, Hussain SA, Sarfraz Z, Sarfraz A, et al. Impact of active physiotherapy rehabilitation on pain and global and functional improvement 1–2 months after lumbar disk surgery: a systematic review and meta-analysis. Healthcare (Basel). (2022) 10(10):1943. doi: 10.3390/healthcare10101943
34. Liu SK, Song YL, Ding WY, Yang DL, Ma L, Yang SD. The effect of systematic lower-limb rehabilitation training in elderly patients undergoing lumbar fusion surgery: a retrospective study. Oncotarget. (2017) 8:112720–6. doi: 10.18632/oncotarget.22746
35. Wang H, Huo Y, Zhao Y, Zhang B, Yang D, Yang S, et al. Clinical rehabilitation effect of postoperative lower-limb training on the patients undergoing OLIF surgery: a retrospective study. Pain Res Manag. (2020) 2020:1065202. doi: 10.1155/2020/1065202
36. Hajilo P, Imani B, Zandi S, Mehrafshan A. Comparing the intraoperative and postoperative complications of the scalpel and electrocautery techniques for severing the inner layers of the lumbar disc during discectomy surgery. Front Surg. (2023) 10:1264519. doi: 10.3389/fsurg.2023.1264519
37. Ahlgren BD, Lui W, Herkowitz HN, Panjabi MM, Guiboux JP. Effect of anular repair on the healing strength of the intervertebral disc: a sheep model. Spine (Phila Pa 1976). (2000) 25:2165–70. doi: 10.1097/00007632-200009010-00004
38. Johansson AC, Linton SJ, Rosenblad A, Bergkvist L, Nilsson O. A prospective study of cognitive behavioural factors as predictors of pain, disability and quality of life one year after lumbar disc surgery. Disabil Rehabil. (2010) 32:521–9. doi: 10.3109/09638280903177243
39. Svensson GL, Lundberg M, Ostgaard HC, Wendt GK. High degree of kinesiophobia after lumbar disc herniation surgery: a cross-sectional study of 84 patients. Acta Orthop. (2011) 82:732–6. doi: 10.3109/17453674.2011.636674
40. Padua L, Aprile I, Cecchi F, Molino LR, Arezzo MF, Pazzaglia C. Pain in postsurgical orthopedic rehabilitation: a multicenter study. Pain Med. (2012) 13:769–76. doi: 10.1111/j.1526-4637.2012.01395.x
41. Pritwani S, Pandey S, Shrivastava P, Kumar A, Malhotra R, Maddison R, et al. Challenges in rehabilitation and continuum of care provision after knee replacement: a mixed-methods study from a low- and middle-income country. Disabil Rehabil. (2024) 46(13):2890–900. doi: 10.1080/09638288.2023.2236012
42. Schwartz CE, Stark RB, Balasuberamaniam P, Shrikumar M, Wasim A, Finkelstein JA. Moving toward better health: exercise practice is associated with improved outcomes after spine surgery in people with degenerative lumbar conditions. Can J Surg. (2021) 64:E419–27. doi: 10.1503/cjs.010620
43. Lyu Z, Bai J, Chen S, Liu J, Yu W. Efficacy of lumbar kinetic chain training for staged rehabilitation after percutaneous endoscopic lumbar discectomy. BMC Musculoskelet Disord. (2021) 22:793. doi: 10.1186/s12891-021-04674-y
44. Bertozzi L, Gardenghi I, Turoni F, Villafane JH, Capra F, Guccione AA, et al. Effect of therapeutic exercise on pain and disability in the management of chronic nonspecific neck pain: systematic review and meta-analysis of randomized trials. Phys Ther. (2013) 93:1026–36. doi: 10.2522/ptj.20120412
45. Madera M, Brady J, Deily S, McGinty T, Moroz L, Singh D, et al. The role of physical therapy and rehabilitation after lumbar fusion surgery for degenerative disease: a systematic review. J Neurosurg Spine. (2017) 26:694–704. doi: 10.3171/2016.10.SPINE16627
46. Lage DE, Jernigan MC, Chang Y, Grabowski DC, Hsu J, Metlay JP, et al. Living alone and discharge to skilled nursing facility care after hospitalization in older adults. J Am Geriatr Soc. (2018) 66:100–5. doi: 10.1111/jgs.15150
47. Yao J, He W, Chen H, Qi Y. Nursing effect of continuous nursing intervention based on “internet plus” on patients with severe adrenal tumor. Medicine (Baltimore). (2023) 102:e33187. doi: 10.1097/MD.0000000000033187
Keywords: UBE surgery, continuous nursing, low back pain, lumbar disc herniation, rehabilitation training
Citation: Li J, Song Y, Wu L, Su D and Wang L-F (2024) Effects of a new continuous nursing program on the short-term and long-term low back pain in patients after UBED: a retrospective study based on 282 patients. Front. Surg. 11:1443231. doi: 10.3389/fsurg.2024.1443231
Received: 3 June 2024; Accepted: 6 August 2024;
Published: 29 August 2024.
Edited by:
Giacomo Rossettini, University of Verona, ItalyReviewed by:
Jorge Hugo Villafañe, Fondazione Don Carlo Gnocchi Onlus (IRCCS), ItalyCopyright: © 2024 Li, Song, Wu, Su and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lin-Feng Wang, d2FuZ2xpbmZlbmdsYW9zaGlAMTYzLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.