 Xuemei Zhao
Xuemei Zhao Siyu Jin1
Siyu Jin1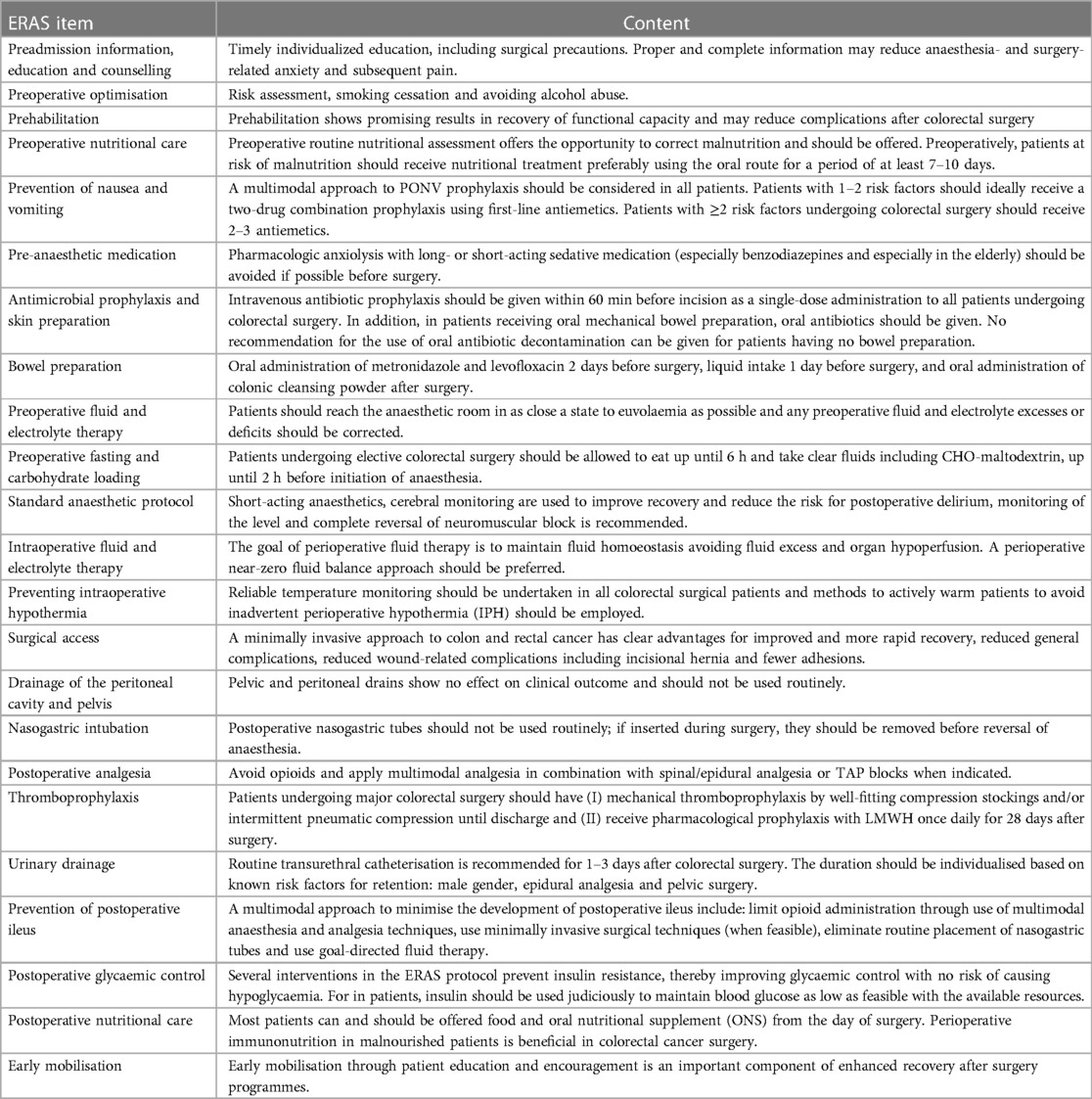

95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg. , 25 June 2024
Sec. Colorectal and Proctological Surgery
Volume 11 - 2024 | https://doi.org/10.3389/fsurg.2024.1395271
Objective: Retrospective analysis and comparison of the effects of Enhanced Recovery After Surgery (ERAS) protocol for patients having left and right colectomy surgeries.
Method: Out of the patients admitted to Chengdu Shang Jin Nan Fu Hospital and West China Hospital from December 2019 to December 2022, a total of 498 who met the inclusion criteria were selected, 255 with right colectomy(RC) and 243 with left colectomy (LC). Under the conditions of strict compliance with ERAS protocol, the relevant physical indexes of RC and LC, including postoperative rehabilitation (especially median post-operative stay) and complications (especially prolonged postoperative ileus, PPOI), were statistically analyzed and compared.
Results: In terms of intraoperative variables, fluid doses were higher in the LC group than in the RC group (P < 0.05), and there was no significant difference between them in terms of operative time, blood loss, need for open surgery, peritoneal contamination, epidural catheter placement, or opioid use (P > 0.05). Compared with the RC group, the LC group had a higher intake of oral liquid at the second postoperative day (POD), and faster first flatulence (P < 0.05). 30 (11.76%) RC patients required nasogastric tube insertion, while only 3 (1.23%) patients in the LC group required the same (P < 0.05). Prolonged postoperative ileus (PPOI) occurred in 48 (18.82%) and 29 (11.93%) patients in the RC and LC groups, respectively (P < 0.05). No significant differences in terms of postoperative complications or length of hospital stay (LoS). stay were observed.
Conclusion: As the location of colon cancer changes, the effectiveness of ERAS also varies. More personalized and precise ERAS protocols can reduce the incidence of postoperative complications and promote rapid recovery after surgery.
Colorectal cancer (CRC) is the most common tumor of the digestive system, and estimates of new cases and deaths from CRC in the United States in 2024 are 152,810 and 53,010, respectively (1). At present, the main treatment for CRC is surgical tumor removal, and there are mainly two ways to do that depending on the location of the tumor, namely left colectomy (LC) and right colectomy (RC) (2, 3). Depending on tumor characteristics and surgeon experience, there are still debates about what type of surgery to choose to treat transverse colon cancer (4). Enhanced Recovery After Surgery (ERAS) is widely used due to its applicability and safety. Many studies have shown that ERAS can help improve prognostic recovery after colorectal surgery. This multimodal stress minimization method has been repeatedly proven to be able to reduce morbidity after CRC surgery, improve postoperative recovery, and shorten median median post-operative stay (5, 6). ERAS aims to bring patients back to their preoperative state quickly after surgery through multiple efforts such as minimizing perioperative fasting, encouraging exercise, and strict pain control (7). However, it is worth exploring whether we should implement different ERAS protocols depending on the location of the colon tumor. The goal of this study is to initially explore whether there are differences in the ERAS process of patients undergoing LC or RC colon cancer surgeries.
A multi-center retrospective study based on anonymized data collected. According to the The Societies present the Reporting on ERAS Compliance, Outcomes, and Elements Research (RECOvER) Checklist, our center started to systematically implement the standardized ERAS protocol for elective colectomy from 2019. Since then, we have collected demographic and perioperative data as well as functional and clinical results through bedside patient diaries and electronic charts and paid follow-up visits postoperatively (for at least 30 days) to all patients.
Patients admitted to Chengdu Shang Jin Nan Fu Hospital and West China Hospital from December 2019 to December 2022 who underwent elective colectomy (mainly laparoscopic RC or LC for cancer treatment) were selected and treated according to the standardized ERAS protocol, shown in Figure 1. Prolonged postoperative ileus (PPOI) was the primary endpoint, and the secondary endpoints was median post-operative stay (8, 9). This study involving human participants were reviewed and approved by the ethics committee of Chengdu Shang Jin Nan Fu Hospital (EC20200029), and were conducted according to established ethical guidelines.
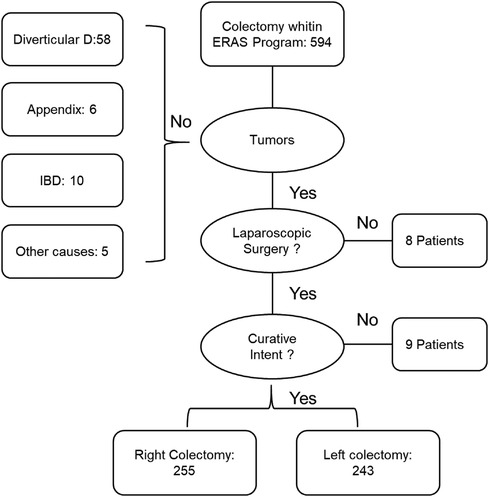
Figure 1 Flowchart to select the study population.
Exclusion criteria: (1) Tumor emergencies such as intestinal obstruction, perforation, and bleeding; (2) Multiple cancers, neoadjuvant chemoradiotherapy, extensive tumor metastasis found during surgery, etc.; (3) Inability to tolerate surgery due to severe cardiopulmonary insufficiency.
According to oncological principles, all laparoscopic surgeries are performed in the presence of at least one senior colorectal surgeon, with a 7–10 cm excisional margin on both sides of the tumor, and central ligation and lymph node resection along the corresponding blood vessels. Tumors that occur in the right transverse colon or proximal transverse colon were treated with RC (resection of the terminal ileum, right colon, and partial transverse colon, followed by ileostomy). Left-sided colon tumors were treated with LC (sigmoidectomy or left-sided colectomy, followed by first-stage colorectal anastomosis). All LCs were end-to-end colorectal anastomoses performed with conventional double staplers (10, 11).
ERAS protocol was summarized based on relevant literature and previous experience, as shown in Table 1.
The dataset used consists of multiple items which are summarized, including but not limited to time to first flatulence, stool, activity, postoperative visual analogue scale (VAS), nausea and vomiting, time to tolerance with solid food, complications, opioids (as needed), and median post-operative stay. The prerequisites for ERAS patients to be discharged include: (1) no evidence of complications; (2) tolerance to soft diet (SD); (3) unassisted walking; (4) good pain control with oral administration of drugs. RECOvER Checklist was shown in Table 2.
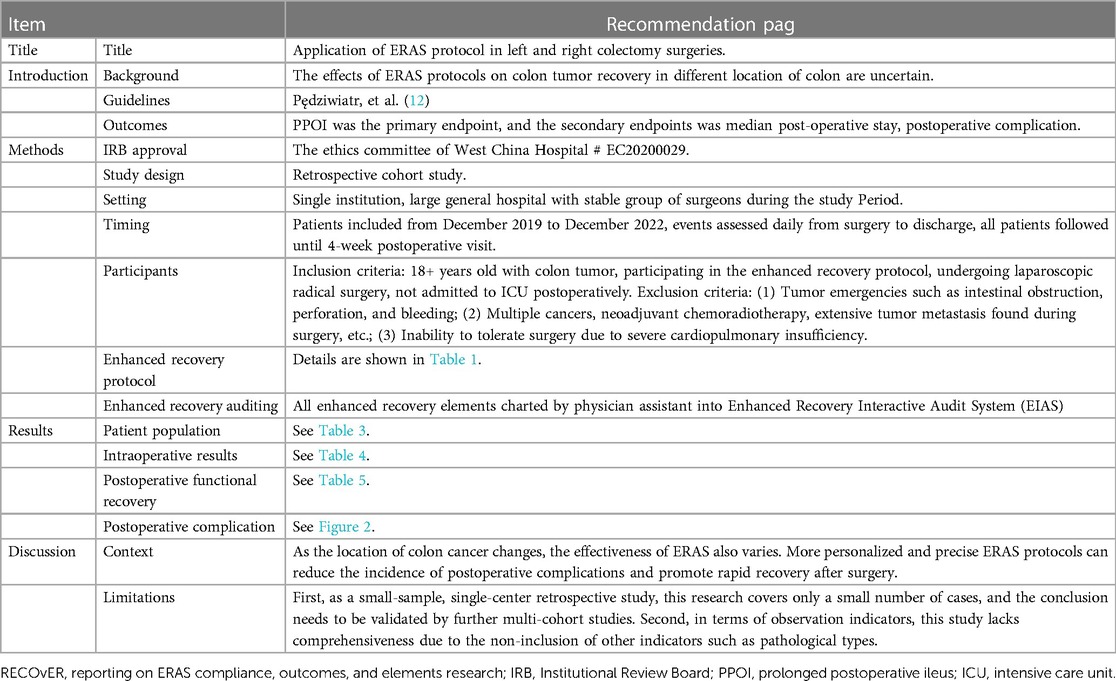
Table 2 RECOvER checklist.
SPSS22.0 statistical software was used for data processing and analysis, the measurement data was expressed in , and t-test of independent samples was used for comparison between the two groups. Count data were expressed as a percentage, and X2 test was used. P < 0.05 indicates a statistically significant difference.
From December 2019 to December 2022, the data of 594 patients were continuously entered into the EIAS database, and the selection process is as shown in Figure 1. Of the 498 patients who met the inclusion criteria, 255 underwent RC surgery and 243 underwent LC surgery. The detailed demographic characteristics of these patients are shown in Table 3. In terms of demographic variables, there was no significant difference between the two groups (P > 0.05).
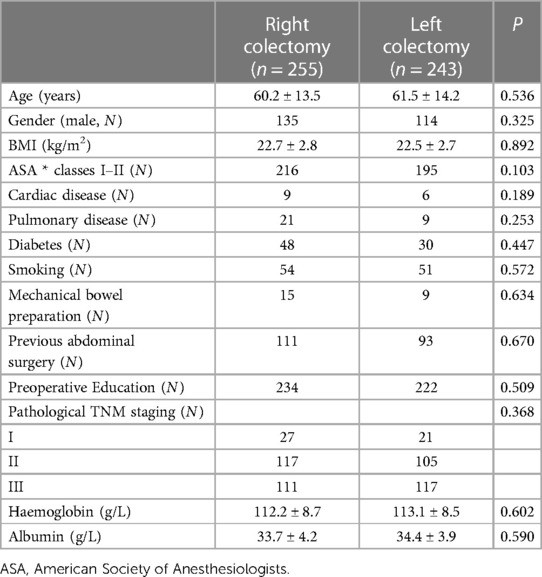
Table 3 Demographic characteristics of patients.
In terms of intraoperative variables, fluid doses were higher in the LC group than in the RC group (P < 0.05), and there was no significant difference between them in terms of operative time, blood loss, need for open surgery, peritoneal contamination, epidural catheter placement, or opioid use (P > 0.05, Table 4).

Table 4 Intraoperative results.
Compared with the RC group, the LC group had a higher intake of oral liquid at the second POD, and faster first flatulence (P < 0.05). 30 (11.76%) RC patients required nasogastric tube insertion, while only 3 (1.23%) in the LC group required the same (P < 0.05, Table 5). PPOIs occurred in 48 (18.82%) and 29 (11.93%) patients in the RC and LC groups, respectively (P < 0.05).
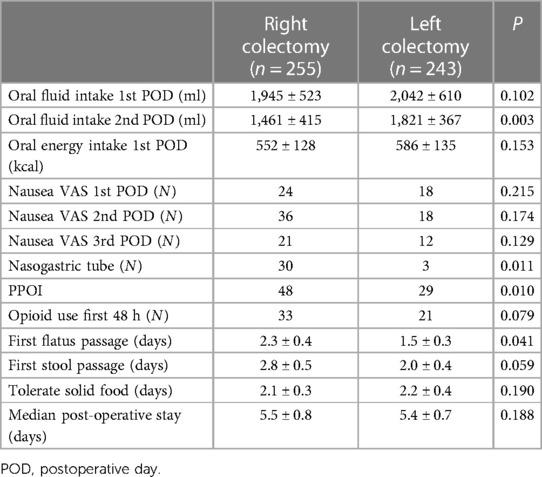
Table 5 Postoperative functional recovery.
In terms of postoperative morbidity, 52 (20.39%) and 45 (18.52%) patients in the RC and LC groups developed postoperative complications (P = 0.150), respectively. In the RC group, 34 (13.33%) had minor complications (6 cases of urinary tract infection, 9 cases of superficial infection at surgical site, 1 cases of acute renal failure, 18 cases of hospital-acquired pneumonia) and 18 (7.06%) had serious complications: including 12 cases (4.71%) of anastomotic leakage that required follow-up surgical intervention, 3 cases of percutaneous drainage of intra-abdominal abscess, and 3 cases of deep wound dehiscence that required surgical revision. In the LC group, 30 (12.35%) patients had minor complications (4 cases of urinary retention, 3 cases of urinary tract infections, and 8 cases of superficial surgical site infections, 15 cases of hospital-acquired pneumonia), 15 (6.17%) patients had serious complications: including 9 cases of (3.70%) anastomotic leakage that required surgical reintervention, and 6 cases of percutaneous drainage of intra-abdominal abscesses. See Figure 2 for details.
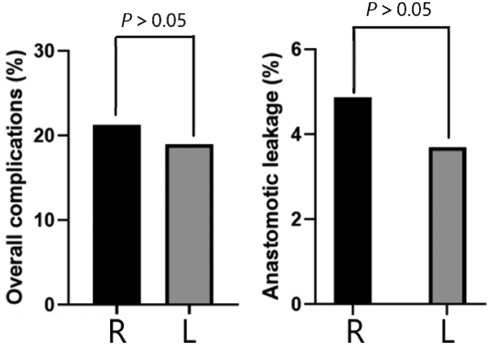
Figure 2 Postoperative complication.
Over the past two decades, there have been two major improvements/fundamental developments in the perioperative care of patients having colon surgeries, namely the introduction of laparoscopic surgery [formerly known as Fast Track (FT) surgery] and the implementation of ERAS protocols. Compared to open surgery, laparoscopic surgery results in a significantly shorter median post-operative stay and much less postoperative morbidity and pain. As reported in multiple randomized controlled trials, this is due to less surgical stress response (14, 15). And it is also found in several randomized studies evaluating the effect of ERAS protocols on the outcomes of elective colorectal surgery that the implementation of ERAS helps reduce complications and median post-operative stay and accelerate postoperative recovery (16, 17).
Studies have shown that improvement in postoperative recovery depends primarily on intraoperative factors (e.g., minimally invasive surgery and afferent nerve block) and postoperative interventions (e.g., early nutritional preparation and mobilization after “fast-track” surgery) (18). The purpose of postoperative interventions is to promote the recovery of physical functions and accelerate recovery. However, studies have shown that due to poor health and psychological burden (fear of interfering with the healing process and anxiety about the possible additional treatment of the underlying disease) in the postoperative period, it may not be the best time to ask patients to make significant changes in nutritional intake and exercise (19). In comparison, interventions in the preoperative phase (both physically and psychologically) may be more helpful for postoperative recovery and relieving some of the emotional distress associated with the anticipation and recovery process of surgery. Some studies have also shown that regardless of motor skills, patients who improved their physical functions through exercise before surgery recovered better thereafter (20). However, one-third of patients experienced deterioration before surgery. Despite exercises, these patients were still at risk of prolonged postoperative recovery. Poor preoperative physical conditions (fatigue, malnutrition, and physical performance), anxiety and depression are also important confounding factors that can lead to prolonged recovery (21, 22). These results indicate that exercise training alone is not enough to reduce stress responses in all patients, and it is also necessary to consider factors that can promote adaptation to exercises, such as nutritional preparation and coping behaviors. Based on the foregoing and our experience, we believe that personalized postoperative rehabilitation plans should be developed for different patients and rehabilitation treatment should be carried out according to the specific conditions of the patients. Early walking exercise, diet recovery, and aggressive pain control are important components of ERAS, and they have been shown to aid recovery after colorectal cancer surgery. Therefore, the ERAS protocols covered in this study all encourage patients to do walking exercise, active diet recovery, and pain control as early as possible.
In our study, there were no significant differences between the groups in terms of time to first ventilation or bowel movement and time to tolerate solid foods, and the composite marker PPOI showed a clear trend towards slow bowel recovery after RC. Postoperative ileus (POI) has no internationally accepted clinical definition. As a quasi-physiological state of coordinated bowel motility arrest after surgical intervention, it usually disappears on the third day after laparoscopic surgery (23). PPOI refers to the inadequate recovery of POI on day 3 postoperatively, which impedes efficient delivery of intestinal contents or tolerance of oral intake of food. We consider this metric to be more reliable than some other commonly used indicators: the timing of first ventilation and stool is an inaccurate marker of bowel recovery, as patients may pass a small amount of gas or stool on the first day postoperatively but still have paralytic ileus for two to three days after surgery (24). Therefore, understanding the potential dangers of PPOIs is clinically relevant and can help surgeons avoid PPOIs through specific measures such as the use of prokinetic drugs and adjustment of postoperative food intake. In addition, the use of MBP may cause a delay in the first bowel movement. Times to solid food tolerance and appetite recovery may also be unreliable and subjective markers of bowel function recovery, as they lack quantitative definitions (25). Therefore, if these markers were used alone, the sensitivity to measure intestinal recovery would be low, and the curve of differences between groups would flatten. For these reasons, we believe that composite PPOIs are more adequate in terms of the condition assessment of patients. In terms of intraoperative variables, fluid doses were higher in the LC group than in the RC group (P < 0.05). Compared with the RC group, the LC group had a higher intake of oral liquid at the second POD, and faster first flatulence (P < 0.05). Postoperative complications occurred in 28.24% and 18.52% of patients with RC and LC, respectively, with no significant difference (P > 0.05). The main purpose of perioperative bowel preparation for colon cancer surgery is to rid the large bowel of solid feces and lower the bacterial content. However, this practice in fact liquefies the feces which increases the risk of surgical spilling and does not reduce the number of bacterial organisms in the bowel. This has been phased out in our latest ERAS agreement. The purpose of placing abdominal drainage is to observe and assist in the treatment of abdominal bleeding, anastomotic leakage, chyle leak, etc. after the surgery (to ensure adequate drainage and increase the success rate of conservative treatment). Therefore, in this study, there was no difference in the overall incidence of complications between the two groups, but there were differences between them in some specific complications, such as those requiring nasogastric tube insertion and the proportion of PPOI.
First, as a small-sample, single-center retrospective study, this research covers only a small number of cases, and the conclusion needs to be validated by further multi-cohort studies. Second, in terms of observation indicators, this study lacks comprehensiveness due to the non-inclusion of other indicators such as pathological types.
In summary, despite the wide application and proven effects of ERAS protocol in the field of CRC surgery, we should develop more individualized ERAS protocols by also considering different tumor locations and surgical protocols.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by this study involving human participants were reviewed and approved by the ethics committee of Chengdu Shang Jin Nan Fu Hospital (EC20200029), and were conducted according to established ethical guidelines. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
XZ: Conceptualization, Data curation, Formal Analysis, Methodology, Software, Writing – original draft. SJ: Conceptualization, Data curation, Formal Analysis, Methodology, Project administration, Software, Writing – original draft. MP: Data curation, Formal Analysis, Methodology, Project administration, Software, Writing – original draft. JW: Conceptualization, Formal Analysis, Methodology, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Siegel RL, Giaquinto AN, Jemal A. Cancer statistics. CA Cancer J Clin. (2024) 74(1):12–49. doi: 10.3322/caac.21820
2. Geltzeiler CB, Rotramel A, Wilson C, Deng L, Whiteford MH, Frankhouse J. Prospective study of colorectal enhanced recovery after surgery in a community hospital. JAMA Surg. (2014), 149(9):955–61. doi: 10.1001/jamasurg.2014.675
3. Bourgouin S, Monchal T, Schlienger G, Franck L, Lacroix G, Balandraud P. Eligibility criteria for ambulatory colectomy. J Visc Surg. (2022) 159(1):21–30. doi: 10.1016/j.jviscsurg.2020.11.012
4. van Rooijen S, Carli F, Dalton S, Thomas G, Bojesen R, Le Guen M, et al. Multimodal prehabilitation in colorectal cancer patients to improve functional capacity and reduce postoperative complications: the first international randomized controlled trial for multimodal prehabilitation. BMC Cancer. (2019) 19(1):98. doi: 10.1186/s12885-018-5232-6
5. Bakker N, Cakir H, Doodeman HJ, Houdijk AP. Eight years of experience with enhanced recovery after surgery in patients with colon cancer: impact of measures to improve adherence. Surgery. (2015) 157(6):1130–6. doi: 10.1016/j.surg.2015.01.016
6. Martínez AB, Longás J, Ramírez JM. A model for lymphocyte activation in open versus laparoscopic surgery in colorectal cancer patients in enhanced recovery after surgery (ERAS) protocols. Int J Colorectal Dis. (2017) 32(6):913–6. doi: 10.1007/s00384-016-2731-2
7. Lohsiriwat V, Lertbannaphong S, Polakla B, Riansuwan W. Implementation of enhanced recovery after surgery and its increasing compliance improved 5-year overall survival in resectable stage III colorectal cancer. Updates Surg. (2021) 73(6):2169–79. doi: 10.1007/s13304-021-01004-8
8. Jones D, Musselman R, Pearsall E, McKenzie M, Huang H, McLeod RS. Ready to go home? Patients’ experiences of the discharge process in an enhanced recovery after surgery (ERAS) program for colorectal surgery. J Gastrointest Surg. (2017) 21(11):1865–78. doi: 10.1007/s11605-017-3573-0
9. De Crignis L, Slim K, Cotte E, Meillat H, Dupré A. Impact of surgical indication on patient outcomes and compliance with enhanced recovery program for colorectal surgery: a francophone multicenter retrospective analysis. J Surg Oncol. (2020) 122(5):928–33. doi: 10.1002/jso.26097
10. Kim MK, Kim JG, Lee G, Won DD, Lee YS, Kye BH, et al. Comparison of the effects of an ERAS program and a single-port laparoscopic surgery on postoperative outcomes of colon cancer patients. Sci Rep. (2019) 9(1):11998. doi: 10.1038/s41598-019-48526-1
11. Lohsiriwat V, Jitmungngan R, Chadbunchachai W, Ungprasert P. Enhanced recovery after surgery in emergency resection for obstructive colorectal cancer: a systematic review and meta-analysis. Int J Colorectal Dis. (2020) 35(8):1453–61. doi: 10.1007/s00384-020-03652-5
12. Pedziwiatr M, Mavrikis J, Witowski J, Adamos A, Major P, Nowakowski M, et al. Current status of enhanced recovery after surgery (ERAS) protocol in gastrointestinal surgery. Med Oncol. (2018) 35(6):95. doi: 10.1007/s12032-018-1153-0
13. Meillat H, Brun C, Zemmour C, de Chaisemartin C, Turrini O, Faucher M, et al. Laparoscopy is not enough: full ERAS compliance is the key to improvement of short-term outcomes after colectomy for cancer. Surg Endosc. (2020) 34(5):2067–75. doi: 10.1007/s00464-019-06987-5
14. Gustafsson UO, Scott MJ, Hubner M, Nygren J, Demartines N, Francis N, et al. Guidelines for perioperative care in elective colorectal surgery: enhanced recovery after surgery (ERAS®) society recommendations: 2018. World J Surg. (2019) 43(3):659–95. doi: 10.1007/s00268-018-4844-y
15. Pellegrino L, Pagano E, Allaix ME, Morino M, Muratore A, Massucco P, et al. Perioperative care in colorectal cancer surgery before a structured implementation program of the ERAS protocol in a regional network. The piemonte EASY-NET project. Healthcare (Basel). (2021) 10(1):72. doi: 10.3390/healthcare10010072
16. Chen JS, Sun SD, Wang ZS, Cai TH, Huang LK, Sun WX, et al. The factors related to failure of enhanced recovery after surgery (ERAS) in colon cancer surgery. Langenbecks Arch Surg. (2020) 405(7):1025–30. doi: 10.1007/s00423-020-01975-z
17. Tejedor P, González Ayora S, Ortega López M, León Arellano M, Guadalajara H, García-Olmo D, et al. Implementation barriers for enhanced recovery after surgery (ERAS) in rectal cancer surgery: a comparative analysis of compliance with colon cancer surgeries. Updates Surg. (2021) 73(6):2161–8. doi: 10.1007/s13304-021-01115-2
18. Salem ME, Yin J, Goldberg RM, Pederson LD, Wolmark N, Alberts SR, et al. Evaluation of the change of outcomes over a 10-year period in patients with stage III colon cancer: pooled analysis of 6,501 patients treated with fluorouracil, leucovorin, and oxaliplatin in the ACCENT database. Ann Oncol. (2020) 31(4):480–6. doi: 10.1016/j.annonc.2019.12.007
19. Ripollés-Melchor J, Abad-Motos A, Zorrilla-Vaca A. Enhanced recovery after surgery (ERAS) in surgical oncology. Curr Oncol Rep. (2022) 24(9):1177–87. doi: 10.1007/s11912-022-01282-4
20. Meillat H, Braticevic C, Zemmour C, Brun C, Cécile M, Faucher M, et al. Real-world implementation of a geriatric-specific ERAS protocol in patients undergoing colonic cancer surgery. Eur J Surg Oncol. (2021) 47(5):1012–8. doi: 10.1016/j.ejso.2020.11.128
21. Bellato V, An Y, Cerbo D, Campanelli M, Franceschilli M, Khanna K, et al. Feasibility and outcomes of ERAS protocol in elective cT4 colorectal cancer patients: results from a single-center retrospective cohort study. World J Surg Oncol. (2021) 19(1):196. doi: 10.1186/s12957-021-02282-7
22. Skelton WP 4th, Franke AJ, Iqbal A, George TJ. Comprehensive literature review of randomized clinical trials examining novel treatment advances in patients with colon cancer. J Gastrointest Oncol. (2020) 11(4):790–802. doi: 10.21037/jgo-20-184
23. Kloosterman WP, Coebergh van den Braak RRJ, Pieterse M, van Roosmalen MJ, Sieuwerts AM, Stangl C, et al. A systematic analysis of oncogenic gene fusions in primary colon cancer. Cancer Res. (2017) 77(14):3814–22. doi: 10.1158/0008-5472.CAN-16-3563
24. Vendler MMI, Haidari TA, Waage JE, Kleif J, Kristensen B, Gögenur I, et al. Incidence of venous thromboembolic events in enhanced recovery after surgery for colon cancer: a retrospective, population-based cohort study. Colorectal Dis. (2017) 19(11):O393–401. doi: 10.1111/codi.13910
25. Sánchez-Iglesias JL, Gómez-Hidalgo NR, Bebia V, Ramirez JM, Pérez-Benavente A, Nelson G, et al. Discontinuation of mechanical bowel preparation in advanced ovarian cancer surgery: an enhanced recovery after surgery (ERAS) initiative. Clin Transl Oncol. (2023) 25(1):236–42. doi: 10.1007/s12094-022-02934-4
Keywords: colorectal cancer, Enhanced Recovery After Surgery, postoperative rehabilitation, postoperative complications, surgery
Citation: Zhao X, Jin S, Peng M and Wang J (2024) A retrospective study on the efficacy of the ERAS protocol in patients who underwent laparoscopic left and right colectomy surgeries. Front. Surg. 11:1395271. doi: 10.3389/fsurg.2024.1395271
Received: 3 March 2024; Accepted: 25 April 2024;
Published: 25 June 2024.
Edited by:
Raffaele De Luca, Bari Giovanni Paolo II Cancer Institute, National Cancer Institute (IRCCS), ItalyReviewed by:
Andrea Marco Tamburini, San Raffaele Hospital (IRCCS), Italy© 2024 Zhao, Jin, Peng and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jingjing Wang, d2FuZ2ppbmdqaW5nXzMyMUBzaW5hLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.