 Ruoyun Lyu
Ruoyun Lyu Zonglin Wen
Zonglin Wen Rong Huang
Rong Huang Zhiling Yang1
Zhiling Yang1
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Surg. , 03 June 2024
Sec. Visceral Surgery
Volume 11 - 2024 | https://doi.org/10.3389/fsurg.2024.1349975
Background: About one-third of patients experience postoperative ileus (POI) after abdominal surgery, which can cause various complications and has not been treated well in clinical practice. The comprehensive treatment offered by traditional Chinese medicine may be a good choice for promoting intestinal mobility. Therefore, the aim of this study protocol is to observe the effectiveness of acupuncture combined with auricular acupressure in decreasing the incidence and related symptoms of POI.
Methods: This is a single-center, assessor-blinded, randomized controlled trial. A total of 160 participants are supposed to recruit at Shanghai Tenth People's Hospital and randomly divided into two parallel groups in a 1:1 ratio. The intervention group are planned to receive manual acupuncture combined with auricular acupressure, while the control group are planned to receive regular enhanced recovery after surgery treatment. The primary outcome is the time to first defecation and first flatus after surgery. The secondary outcomes include the length of postoperative hospital stay, intensity of postoperative abdominal pain and distension, severity of postoperative nausea and vomiting, time to tolerate diet, inflammatory index, and incidence of prolonged postoperative ileus.
Discussion: The results of this research will provide substantial evidence regarding the efficacy of comprehensive traditional Chinese treatment, specifically auricular acupressure and manual acupuncture, in treating and preventing POI.
Trial registration: ClinicalTrials.gov, Identifier: ChiCTR2300075983, registered on September 21, 2023.
Postoperative ileus (POI) is an inevitable complication after abdominal surgery, which reflects a deceleration or complete cessation of bowel movements (1). Patients may present with symptoms such as abdominal pain and distension, vomiting, anal defecation, and defecation disorders. Research shows that POI occurring within 3 days for laparoscopic surgery or occurring within 5 days for open surgery is considered physiological; however, if it continues beyond these time frames, it can be considered pathological (2). POI is closely linked with negative factors, including an extended hospital stay, a higher likelihood of hospital-acquired infections or venous thromboembolism, and an increased rate of 30-day readmissions (3–5). The incidence of pathological POI can reach up to 10%–30% (6, 7) in abdominal surgery, which has become a current topic of concern in clinics.
To reduce the occurrence of POI, the conception of the enhanced recovery after surgery (ERAS) protocol has been implemented throughout the perioperative period (8). Many strategies have been supposed to promote bowel movement after surgery; however, only a few of them show a beneficial effect, such as μ-opioid-receptor antagonists, non-steroidal anti-inflammatory drugs (NSAIDS), laparoscopic surgery, and mid-thoracic epidural anesthesia (9–11). More strategies are still under exploration.
The inflammatory phase induced by abdominal surgery greatly impacts gastrointestinal dynamics and is therefore regarded as the main period of clinical prevention and treatment of POI (12). Several systematic reviews of randomized controlled trials (RCTs) on the effect of acupuncture and related therapies on bowel function after surgery show that acupuncture has a positive effect on bowel movement, including improvement of first flatus, first defecation, and first bowel sound (13–15). Manual acupuncture (MA) studies have shown anti-inflammatory effects in the digestive system through vagus nerve activation, TLR4/MyD88/NF-κB signaling, macrophage polarization, the mitogen-activated protein kinase (MAPK) signaling pathway, and the cholinergic anti-inflammatory pathway (16–18), which can be considered as the possible mechanisms of acupuncture in the treatment of POI. Another study reveals that acupuncture of hindlimb regions inhibits the expression of GABAA receptor in DMV neurons, which excites the vagal nerve and, in turn, suppresses inflammation via activation of the α7nAChR-mediated JAK2/STAT3 signaling pathway of POI (19). Auricular acupressure (AA) is another popular complementary approach for postoperative gastrointestinal dysfunction in abdominal surgery, which is non-invasive and has been approved to decrease the incidence of postoperative constipation (20). In clinical practice, these two treatment methods are always combined for simultaneous use; however, few research studies have focused on the comprehensive effect of their combined application in the treatment of POI.
Hence, this single-center, randomized controlled trial is designed to observe the effectiveness of acupuncture combined with auricular acupressure in decreasing the incidence and related symptoms of POI.
The single-center, controlled, assessor-blinded, randomized trial is being executed in Shanghai Tenth People's Hospital from July 2023 and will continue until June 2026. The protocol is described in accordance with the Consolidated Standards of Reporting Trials (CONSORT) (21) guidelines and the Standards for Reporting Interventions in Controlled Trials of Acupuncture (STRICTA) (22). The study is registered at the Chinese Clinical Trial Registry (Identifier: ChiCTR2300075983) and is approved by the Ethics Committee of Shanghai Tenth People's Hospital (No. SHSY-IEC-5.0/23K82/P01). A total of 160 participants with elective laparoscopic surgery will be randomly assigned into an intervention group and a control group with a ratio of 1:1. Details of trial design and analysis plans are presented in Figure 1 and Table 1.
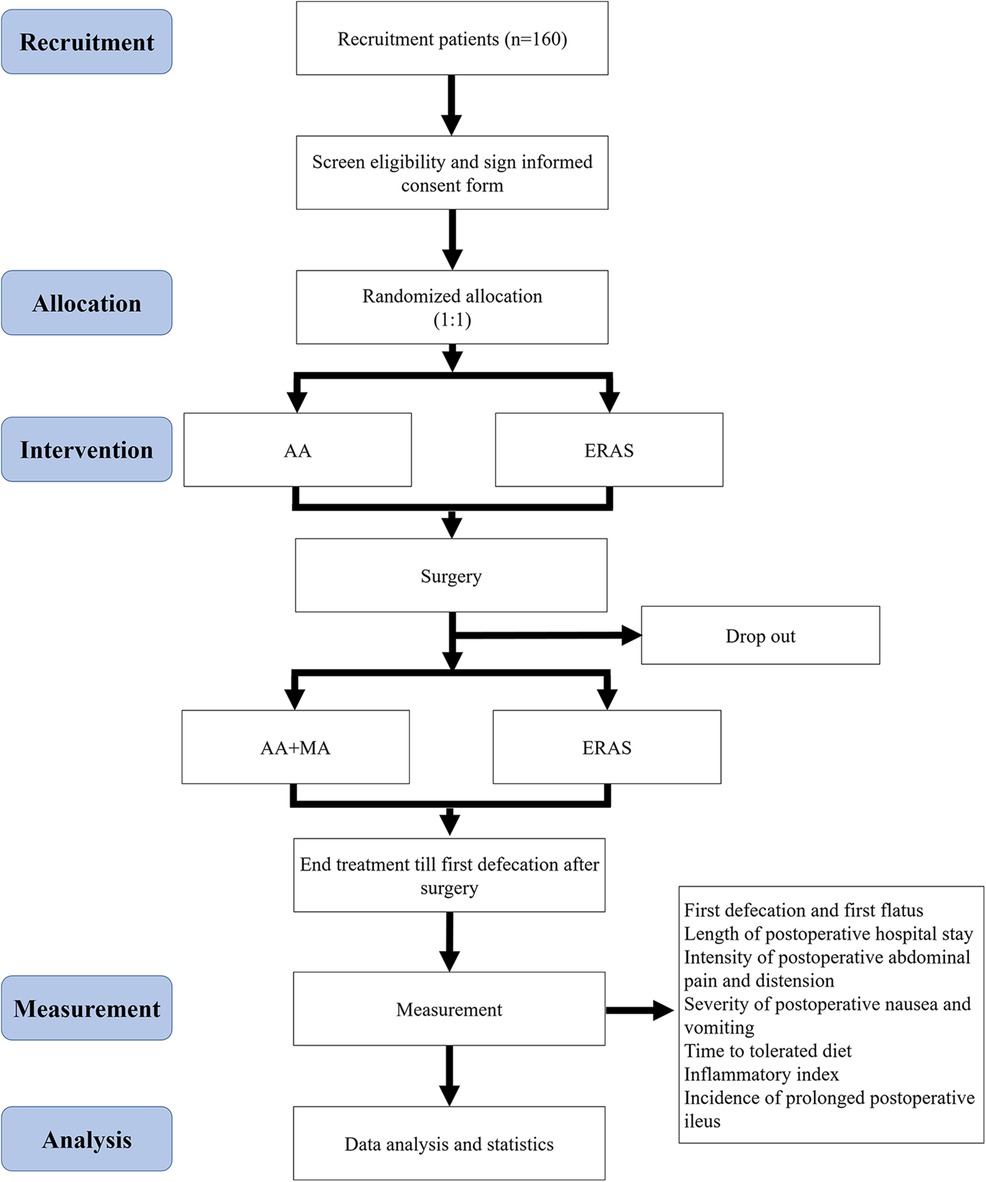
Figure 1. Flowchart of research.
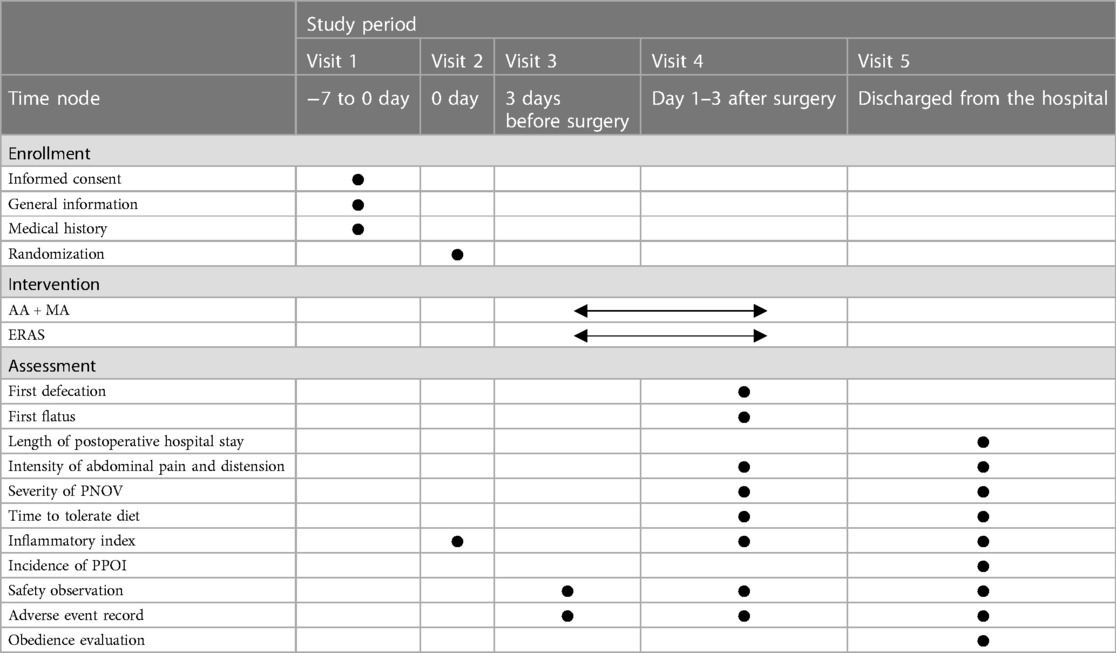
Table 1. Details of the study period.
Patients in the abdominal surgery department of Shanghai Tenth People's Hospital will be diagnosed by a surgeon. All eligible participants will be explained the trial in detail by researchers and will be required to sign informed consent prior to participation. They will also have the right to withdraw from the trial anytime.
(1) Age ranging from 18 to 80 years;
(2) Having upper gastrointestinal disease who will receive elective laparoscopic surgery, including benign hepatobiliary diseases, pancreatic diseases, gastric diseases, and malignant non-metastatic tumors;
(3) Willing to sign the informed consent form and participate in the clinical trial.
(1) A history of serious diseases such as cardiovascular, cerebrovascular, liver, kidney, hematopoietic, digestive system, or mental illness;
(2) A history of surgery in the stomach or intestine;
(3) Having taken drugs for inhibiting gastrointestinal motility for over 2 weeks in the last 3 months;
(4) Having received preoperative chemotherapy or radiotherapy;
(5) Having received relevant treatments that may influence the effect of the study;
(6) Unable to understand and fill out the scales related to the research.
The randomized program is developed using the Statistical Package for Social Sciences (SPSS) Ver. 24.0 (IBM Inc., New York, USA), and the opaque random envelope is used by the assistant to achieve the allocation concealment. The block grouping method is used to achieve randomization and set the length of the block group as 4. The random envelope is marked with the serial number of the group, and the group number is printed on the envelope. The envelopes are sequentially opened according to the time sequence of the included cases, and the control group and the intervention group are divided according to the groups in the envelope.
The participants and the acupuncturist will not be blinded because of the specialization of acupuncture manipulation. However, the data analysis and efficacy assessment will be performed by the research assistant and blinded to decrease analysis bias.
MA and auricular acupressure procedures of the intervention group will be administered by licensed acupuncturists with 5–12 years of education in acupuncture and at least 3 years of clinical experience. They will all undergo unified and standardized training before trial initiation.
The intervention group will accept AA at the small intestine (CO6), large intestine (CO7), abdomen (AH8), and sub-cortex (AT4) according to the Nomenclature and Location of Auricular Points (Table 2 and Figure 2). Vaccaria seeds (Wang-Bu-Liu-Xing) (40 mm × 40 mm) (Changshu Shenling Medical Products Factory Co., Ltd., Changshu, China) will be embedded on the surface of auricular points and maintained between the two treatments. Two ears will accept AA alternately once daily. Participants will be suggested to press each point gently for 1 min thrice daily. The treatment will start 3 days before elective laparoscopic surgery and continue until the first defecation after surgery.
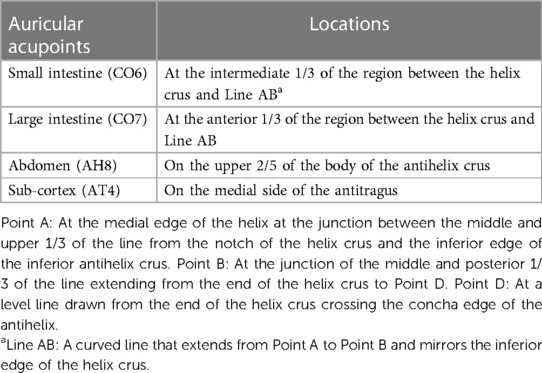
Table 2. Location of auricular acupoints.
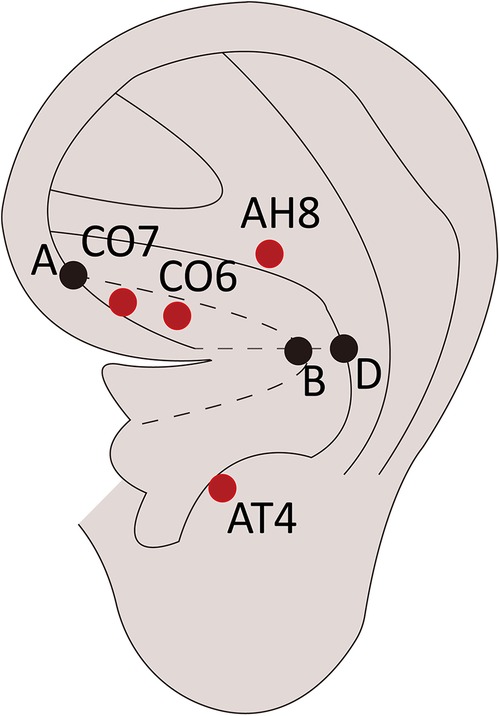
Figure 2. Location of auricular acupoints.
The intervention group will also accept MA at Zusanli (ST36), Shangjuxu (ST37), Xiajuxu (ST39), Hegu (LI4), and Taichong (LR3) according to Acupuncture and Moxibustion (23) (Table 3 and Figure 3). A single-use stainless steel needle (0.25 mm × 40 mm) (Suzhou Medical Products Factory Co., Ltd., Suzhou, China) will be used, and Deqi sensation (a sensation of sourness, numbness, or distension) should be achieved during the process. The needle should be retained for 20 min and then withdrawn quickly. Patients will receive MA once a day for consecutive days after surgery until the first defecation after surgery.
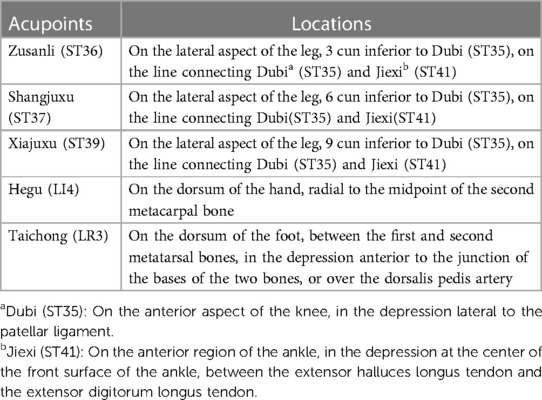
Table 3. Location of acupoints.
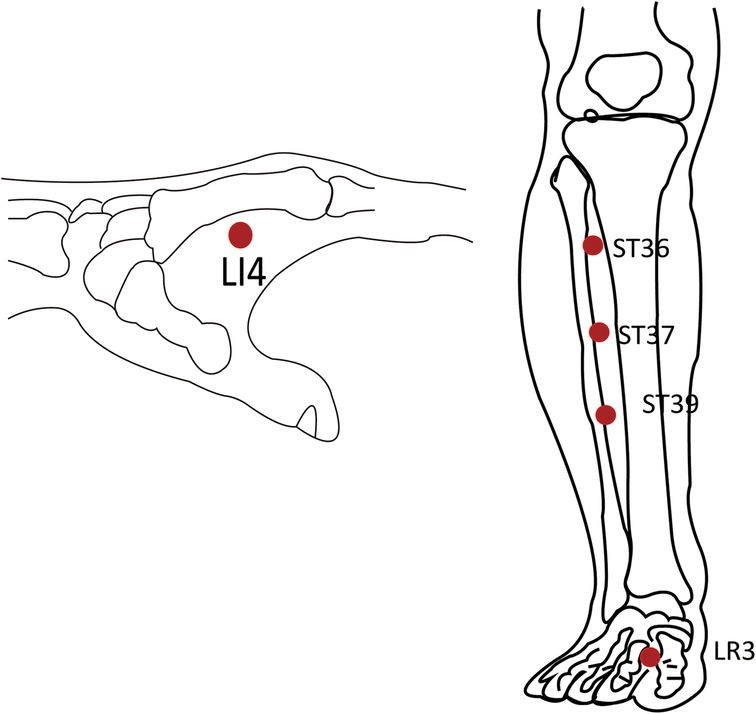
Figure 3. Location of acupoints.
The control group will receive regular treatment of ERAS 3 days before surgery because patients are always admitted to the hospital several days earlier for standard preoperative blood testing and bowel preparation, including taking oral anti-inflammatory drugs, having liquid food 72 h before the operation, accepting enema 24 h before the operation, using intravenous antibiotics to preventing infection, and so on. In addition, the control group will be initiated on a liquid diet within 24 h after surgery to stimulate bowel movement.
Patients in both groups will receive the same postoperative procedures in mobilization to avoid bias in evaluating the onset of POI, including getting out of bed within 24 h after surgery and walking three times a day for a distance of 50–100 m after 48 h.
The primary outcomes are the time to first defecation and first flatus, which is regarded as a bowel function indicator. This time is calculated from the end of laparoscopic surgery and will be recorded by nurses with accuracy to the hour.
The length of postoperative hospital stay is an important index used to determine the clinical effect of treatment, which is relatively objective and intuitive (24–26).
The abdominal pain will be assessed by the visual analog scale (VAS), which has been proven less vulnerable to confounding factors and ceiling effects than other pain scales (27–29). The intensity of abdominal distension can be divided into four grades: no symptoms, mild, moderate, and severe. Both indexes will be obtained 1 day after surgery and at the time of discharge.
The simplified postoperative nausea and vomiting (PONV) impact scale, which consists of two questions, will be used to evaluate postoperative nausea and vomiting (30). Clinical PONV can be defined when the impact scale score is more than 5.
Postoperative ileus can result in delays in time to mobilization and resumption of oral intake, which may further affect patient's satisfaction and wound recovery (31). Therefore, the time to tolerate diet will be recorded as a reference.
The inflammatory index includes white blood cell (WBC) count and the levels of C-reactive protein (CRP), interleukin-6 (IL-6), procalcitonin (PCT), and tumor necrosis factor-α (TNF-α), which will be obtained at baseline, 1 day after surgery, and at the time of discharge.
Prolonged postoperative ileus (PPOI) can be diagnosed when at least two of the following symptoms occur after 96 h postoperatively: nausea or vomiting, inability to tolerate any oral diet over the last 24 h, abdominal bloating and distension, or radiological confirmation (32).
Acupuncture may cause several adverse reactions or adverse events (33), such as bleeding, pain, dizziness, syncope, needle-sticking, and the like. Therefore, clinical safety will be monitored throughout the trial, and all adverse events will be reported. The patients with adverse reactions may receive relevant treatment, and the possible reasons for adverse events will be discussed to avoid the next occurrence. The number and type of all adverse reactions and events will be summarized during the final safety assessment. The participants will be withdrawn from the study if they experience severe adverse events, and relevant information will be immediately reported to the primary investigator.
Before the start of the trial, all members of this study will have special training on clinical trial operation and quality control. A data and safety monitoring board will also be established to ensure data safety and protect the rights and health of all the participants. This independent advisory group will check the data and monitor the execution of scientific and ethical standards of the RCT once a week. Participants’ information will be saved in the specified file folder and provided only with the permission of the data and safety monitoring board.
Our primary outcome is the time to first defecation. The unpublished experimental data on the effects of AA combined with MA, based on a 2-week prior pilot experiment, were used for the sample size calculation. The time to first defecation is 77.8 ± 15.6 h in the intervention group and 85.1 ± 13.35 h in the control group. We chose the two-sample t-test model with a two-tailed test, and the relevant calculating parameters are a significance level of 0.05, a power of 0.80, and an allocation ratio of 1:1. The required number of participants per group is 72. Considering a dropout rate of 10%, the sample size for this trial is 80. Thus, a total of 160 participants will be recruited.
The principle of intention-to-treat (ITT) analysis will be followed in the process of statistical analysis. The last observation carried forward (LOCF) analysis will be applied for missing data in ITT analysis. Supplementary per-protocol analysis will also be carried out. All the statistical analyses will be performed using SPSS Ver. 24.0 with a significance level of 0.05.
First, the different baseline characteristics of the two groups will be described, and data will be presented as mean or median with standard deviation or interquartile range for continuous variables and as frequency distributions for categorical variables. Moreover, the histograms, boxes, and other representations will also be considered for the graphic analysis of corresponding data. A two-sample t-test for quantitative data or a chi-squared test for qualitative data will be performed as a homogeneity test, and the covariance analysis will also be performed if an adjustment is needed for a baseline characteristic.
Second, the analyses will focus on whether statistically better treatment outcomes could be achieved in the intervention group. P-values less than 0.05 will be considered statistically significant, and tests will be two-sided.
In terms of the changes in the measurement data, the two-sample t-test or the Wilcoxon rank-sum test will be used to compare the two groups and to determine differences according to normality. The mean change and the interaction between groups and observed time frames will be analyzed using a two-factor repeated measure analysis. If necessary, a mixed model approach will also be used.
Finally, safety analysis will be performed using the chi-squared test or Fisher's exact test based on the frequency and percentage of all recorded adverse events between the two groups.
The above plan is what we intend to do; however, the final analyses reported may differ from those planned, allowing for post-hoc analysis where it is indicated.
Based on the conception of ERAS, the treatment is designed to start before surgery to reduce the incidence of POI, which happens to have the same view as traditional Chinese medicine, “treat before disease attacks.” In addition, the study also set the ERAS group as the contrast, which may relatively objectively assess the effectiveness and safety of the two treatments.
As acupuncture has been widely accepted and applied in various diseases worldwide, other traditional Chinese therapies can also be taken into consideration, such as auricular acupressure. Auricular acupressure is low-cost, non-invasive, and has been approved for effectiveness in the digestive system (34). In clinical treatment, these two therapies are always combined to treat digestive diseases; however, few research studies have focused on such comprehensive therapy. Therefore, this study is supposed to approve the comprehensive effect of manual acupuncture combined with auricular acupressure in treating postoperative ileus.
The limitation of the study is that due to the specialization of acupuncture manipulation, double-blindness is hard to perform, so assessor-blindness is designed to decrease bias, and we have not set the sham-acupuncture group for the consideration of acceptability of postoperative patients.
To summarize, this trial aims to investigate the efficacy and safety of manual acupuncture combined with auricular acupressure in improving the symptoms and reducing the incidence of postoperative ileus. The results will be revealed at the end of the study and are expected to provide an alternative treatment option for preoperative patients, as well as contribute to the development of enhanced recovery after surgery.
The study is currently in the recruitment phase. The first patient was enrolled in November 2023, and the study is expected to end in March 2026.
The studies involving humans were approved by the Ethics Committee of the Shanghai Tenth People's Hospital (No. SHSY-IEC-5.0/23K82/P01). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
RL: Writing – original draft. ZW: Writing – review & editing. RH: Data curation, Writing – review & editing. ZY: Project administration, Writing – review & editing. YC: Funding acquisition, Supervision, Writing – review & editing.
The authors declare that financial support was received for the research, authorship, and/or publication of this article.
The study was supported by the Program for Research-Oriented Physician of Shanghai Tenth People’s Hospital (No. 2023YJXYSC012) and Management subject of Shanghai Association of Chinese integrative medicine (2023 YYGL 09).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
AA, auricular acupressure; CONSORT, Consolidated Standards of Reporting Trials; CRF, case report form; CRP, C-reactive protein; ERAS, enhanced recovery after surgery; IL-6, interleukin-6; ITT, intention-to-treat; LOCF, last observation carried forward; MA, manual acupuncture; PCT, procalcitonin; PNOV, postoperative nausea and vomiting; POI, postoperative ileus; PPOI, prolonged postoperative ileus; STRICTA, Reporting Interventions in Controlled Trials of Acupuncture; TNF-α, tumor necrosis factor-α; WBC, white blood cell; VAS, visual analog scale.
1. Hedrick TL, McEvoy MD, Mythen MMG, Bergamaschi R, Gupta R, Holubar SD, et al. American Society for Enhanced Recovery and Perioperative Quality Initiative Joint Consensus Statement on postoperative gastrointestinal dysfunction within an enhanced recovery pathway for elective colorectal surgery. Anesth Analg. (2018) 126:1896–907. doi: 10.1213/ANE.0000000000002742
2. Bragg D, El-Sharkawy AM, Psaltis E, Maxwell-Armstrong CA, Lobo DN. Postoperative ileus: recent developments in pathophysiology and management. Clin Nutr. (2015) 34:367–76. doi: 10.1016/j.clnu.2015.01.016
3. Chapman SJ, Pericleous A, Downey C, Jayne DG. Postoperative ileus following major colorectal surgery. Br J Surg. (2018) 105:797–810. doi: 10.1002/bjs.10781
4. Alhashemi M, Fiore JF Jr., Safa N, Al Mahroos M, Mata J, Pecorelli N, et al. Incidence and predictors of prolonged postoperative ileus after colorectal surgery in the context of an enhanced recovery pathway. Surg Endosc. (2019) 33:2313–22. doi: 10.1007/s00464-018-6514-4
5. Traeger L, Koullouros M, Bedrikovetski S, Kroon HM, Thomas ML, Moore JW, et al. Cost of postoperative ileus following colorectal surgery: a cost analysis in the Australian public hospital setting. Colorectal Dis. (2022) 24(11):1416–26. doi: 10.1111/codi.16235
6. Venara A, Meillat H, Cotte E, Ouaissi M, Duchalais E, Mor-Martinez C, et al. Incidence and risk factors for severity of postoperative ileus after colorectal surgery: a prospective registry data analysis. World J Surg. (2020) 44:957–66. doi: 10.1007/s00268-019-05278-3
7. Su'a BU, Pollock TT, Lemanu DP, MacCormick AD, Connolly AB, Hill AG. Chewing gum and postoperative ileus in adults: a systematic literature review and meta-analysis. Int J Surg. (2015) 14:49–55. doi: 10.1016/j.ijsu.2014.12.032
8. Sommer NP, Schneider R, Wehner S, Kalff JC, Vilz TO. State-of-the-art colorectal disease: postoperative ileus. Int J Colorectal Dis. (2021) 36:2017–25. doi: 10.1007/s00384-021-03939-1
9. Steele SR, Brady JT, Cao Z, Baumer DL, Robinson SB, Yang HK, et al. Evaluation of healthcare use and clinical outcomes of alvimopan in patients undergoing bowel resection: a propensity score-matched analysis. Dis Colon Rectum. (2018) 61:1418–25. doi: 10.1097/DCR.0000000000001181
10. Bahadur A, Mallick BK, Heda A, Pathak A, Heda S, Mundhra R. Comparison of the outcomes of enhanced recovery after surgery and traditional recovery pathway in robotic hysterectomy for benign indications: a randomised controlled trial. J Minim Invasive Gynecol. (2024):S1553-4650(24)00198-5. doi: 10.1016/j.jmig.2024.04.019
11. Thierry G, Beck F, Hardy PY, Kaba A, Blanjean A, Vandermeulen M, et al. Impact of enhanced recovery program implementation on postoperative outcomes after liver surgery: a monocentric retrospective study. Surg Endosc. (2024). doi: 10.1007/s00464-024-10796-w
12. Kim Y, Kim YM, Kim JH, Youn YH, Kim JW, Park H. Peri-operative inflammatory marker as a predictive factor for prolonged post-operative ileus after gastrectomy for gastric cancer. J Neurogastroenterol Motil. (2021) 27(4):588–95. doi: 10.5056/jnm20203
13. Liu Y, May BH, Zhang AL, Guo X, Lu C, Xue CC, et al. Acupuncture and related therapies for treatment of postoperative ileus in colorectal cancer: a systematic review and meta-analysis of randomized controlled trials. Evid Based Complement Alternat Med. (2018) 2018:3178472. doi: 10.1155/2018/3178472
14. Emile SH, Horesh N, Garoufalia Z, Gefen R, Ray-Offor E, Wexner SD. Strategies to reduce ileus after colorectal surgery: a qualitative umbrella review of the collective evidence. Surgery. (2024) 175:280–8. doi: 10.1016/j.surg.2023.10.005
15. Zhao X, Si S, Liu X, Liu J, Zhang D, Mu Y, et al. Does invasive acupuncture improve postoperative ileus after colorectal cancer surgery? A systematic review and meta-analysis. Front Med. (2023) 10:1201769. doi: 10.3389/fmed.2023.1201769
16. Oh JE, Kim SN. Anti-inflammatory effects of acupuncture at ST36 point: a literature review in animal studies. Front Immunol. (2022) 12:813748. doi: 10.3389/fimmu.2021.813748
17. Yaklai K, Pattanakuhar S, Chattipakorn N, Chattipakorn SC. The role of acupuncture on the gut-brain-microbiota axis in irritable bowel syndrome. Am J Chin Med. (2021) 49:285–314. doi: 10.1142/S0192415X21500154
18. Wang L, Yang JW, Lin LT, Huang J, Wang XR, Su XT, et al. Acupuncture attenuates inflammation in microglia of vascular dementia rats by inhibiting miR-93-mediated TLR4/MyD88/NF-κB signaling pathway. Oxid Med Cell Longevity. (2020) 2020:8253904. doi: 10.1155/2020/8253904
19. Yang NN, Yang JW, Ye Y, Huang J, Wang L, Wang Y, et al. Electroacupuncture ameliorates intestinal inflammation by activating α7nAChR-mediated JAK2/STAT3 signaling pathway in postoperative ileus. Theranostics. (2021) 11:4078–89. doi: 10.7150/thno.52574
20. Li Y, Qi D, Gong L, Qu H, Xu B, Wen X, et al. Effect of auricular points treatment combined with acupoints application in patients with constipation after lung cancer surgery. J Cancer Res Ther. (2017) 13:844–8. doi: 10.4103/jcrt.JCRT_709_17
21. Schulz KF, Altman DG, Moher D. CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials. Int J Surg. (2011) 9:672–7. doi: 10.1016/j.ijsu.2011.09.004
22. MacPherson H, Altman DG, Hammerschlag R, Youping L, Taixiang W, White A, et al. Revised standards for reporting interventions in clinical trials of acupuncture (STRICTA): extending the CONSORT statement. J Evid Based Med. (2010) 3:140–55. doi: 10.1111/j.1756-5391.2010.01086.x
24. Shin AY, Rao IJ, Bassett HK, Chadwick W, Kim J, Kipps AK, et al. Target-based care: an intervention to reduce variation in postoperative length of stay. J Pediatr. (2021) 228:208–12. doi: 10.1016/j.jpeds.2020.09.017
25. Abeles A, Kwasnicki RM, Pettengell C, Murphy J, Darzi A. The relationship between physical activity and post-operative length of hospital stay: a systematic review. Int J Surg. (2017) 44:295–302. doi: 10.1016/j.ijsu.2017.06.085
26. Xu X, Cheung DST, Smith R, Lai AYK, Lin CC. The effectiveness of pre- and post-operative rehabilitation for lung cancer: a systematic review and meta-analysis on postoperative pulmonary complications and length of hospital stay. Clin Rehabil. (2022) 36:172–89. doi: 10.1177/02692155211043267
27. Heller GZ, Manuguerra M, Chow R. How to analyze the visual analogue scale: myths, truths and clinical relevance. Scand J Pain. (2016) 13:67–75. doi: 10.1016/j.sjpain.2016.06.012
28. Suther KR, Hopp E, Smevik B, Fiane AE, Lindberg HL, Larsen S, et al. Can visual analogue scale be used in radiologic subjective image quality assessment? Pediatr Radiol. (2018) 48:1567–75. doi: 10.1007/s00247-018-4187-8
29. Voutilainen A, Pitkaaho T, Kvist T, Vehvilainen-Julkunen K. How to ask about patient satisfaction? The visual analogue scale is less vulnerable to confounding factors and ceiling effect than a symmetric Likert scale. J Adv Nurs. (2016) 72:946–57. doi: 10.1111/jan.12875
30. Myles PS, Wengritzky R. Simplified postoperative nausea and vomiting impact scale for audit and post-discharge review. Br J Anaesth. (2012) 108:423–9. doi: 10.1093/bja/aer505
31. Yao LY, Gough AE, Zaghiyan KN, Fleshner PR. Prospective randomized trial of immediate postoperative use of regular diet versus clear liquid diet in major colorectal surgery. Dis Colon Rectum. (2023) 66(12):1547–54. doi: 10.1097/DCR.0000000000002737
32. Venara A, Neunlist M, Slim K, Barbieux J, Colas PA, Hamy A, et al. Postoperative ileus: pathophysiology, incidence, and prevention. J Visc Surg. (2016) 153:439–46. doi: 10.1016/j.jviscsurg.2016.08.010
33. Wang C, Liu B, Liu Y, He L, Li H, Liu J. Analysis on the concepts related to adverse events and adverse reactions of acupuncture. Zhongguo Zhen Jiu. (2018) 38(1):87–90. doi: 10.13703/j.0255-2930.2018.01.023
Keywords: postoperative ileus, acupuncture, auricular acupressure, ERAS, protocol
Citation: Lyu R, Wen Z, Huang R, Yang Z and Chen Y (2024) Effectiveness of acupuncture combined with auricular acupressure in the treatment of postoperative ileus: a study protocol for a randomized controlled trial. Front. Surg. 11:1349975. doi: 10.3389/fsurg.2024.1349975
Received: 29 December 2023; Accepted: 20 May 2024;
Published: 3 June 2024.
Edited by:
Gabriel Sandblom, Karolinska Institutet (KI), SwedenReviewed by:
Tomas Aukstikalnis, Vilnius University, Lithuania© 2024 Lyu, Wen, Huang, Yang and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yingqun Chen, ZHIuY2hlbnlxQHZpcC4xNjMuY29t
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.