
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Surg. , 04 January 2024
Sec. Otorhinolaryngology - Head and Neck Surgery
Volume 10 - 2023 | https://doi.org/10.3389/fsurg.2023.1298611
This article is part of the Research Topic Thyroid and Parathyroid Surgery: New and Emerging Concepts View all 11 articles
 Phillip Staibano1*
Phillip Staibano1* Kevin Um2Sheila Yu1
Kevin Um2Sheila Yu1 Mohit Bhandari3Michael K. Gupta1Michael Au1JEM (Ted) Young1Han Zhang1
Mohit Bhandari3Michael K. Gupta1Michael Au1JEM (Ted) Young1Han Zhang1
Intraoperative parathyroid hormone (iPTH) monitoring is standard-of-care in the surgical management of hyperparathyroidism. It involves real-time determination of circulating PTH levels to guide parathyroid gland excision. There exists several iPTH monitoring criteria, such as the Miami criteria, and a lack of standardization in the timing of post-parathyroid gland excision samples. We present a protocol of a systematic review and network meta-analysis of diagnostic test accuracy to identify the iPTH criteria and post-gland excision timepoint that best predicts surgical cure in hyperparathyroidism. The database search strategy will be developed in conjunction with a librarian specialist. We will perform a search of Medline (Ovid), EMBASE (Ovid), CINAHL, Cochrane Collaboration, and Web of Science from 1990–present. Studies will be eligible if they include adult patients diagnosed with hyperparathyroidism who undergo parathyroidectomy with iPTH monitoring. We will only include studies that report diagnostic test properties for iPTH criteria and/or post-excision sampling timepoints. All screening, full-text review, data extraction, and critical appraisal will be performed in duplicate. Critical appraisal will be performed using QUADAS-2 instrument. A descriptive analysis will present study and critical appraisal characteristics. We will perform evaluation of between-study heterogeneity using I2 and Cochrane Q and where applicable, we will perform sensitivity analysis. Our network meta-analysis will include Bayesian hierarchical framework with random effects using multiple models. Ethics approval is not required. This proposed systematic review will utilize a novel Bayesian network meta-analysis model to help standardize iPTH monitoring in hyperparathyroidism, thereby optimizing patient outcomes and healthcare expenditures.
Hyperparathyroidism is characterized by the abnormal circulating levels of parathyroid hormone (PTH) and calcium that can lead to osteoporosis, renal calculi, and cognitive deficits (1). Primary hyperparathyroidism is often caused by a single hyperfunctioning parathyroid adenoma, but in 10%–15% of cases can be caused by double adenoma and/or parathyroid hyperplasia. Secondary and tertiary hyperparathyroidism, which are associated with chronic kidney disease are often secondary to parathyroid hyperplasia (2). In all cases, however, definitive cure requires surgical extirpation of the affects parathyroid gland(s). Advances in imaging continue to improve our ability to detect parathyroid lesions and therefore guide minimally invasive surgical approaches, but current imaging modalities remain inaccurate in detecting parathyroid hyperplasia (3, 4). Patients with discordant or negative imaging, in addition to those with suspected parathyroid hyperplasia, still often require bilateral neck exploration (5).
Intraoperative PTH (iPTH), which involves the real-time sampling of circulating PTH levels to guide parathyroidectomy, improves surgical outcomes and is standard-of-care for managing primary hyperparathyroidism (6, 7). Moreover, iPTH monitoring has high sensitivity in predicting surgical cure within renal hyperparathyroidism and may assist in identifying parathyroid carcinoma (8, 9). Several iPTH criteria exist to assist surgeons in standardizing changes in circulating parathyroid level during surgery, including the Miami criteria, which defines operative success as >50% decrease in iPTH from baseline value for all hyperfunctioning glands (10).
The primary goal of this systematic review and diagnostic test accuracy network meta-analysis will be to determine the optimal iPTH criteria and post-parathyroid gland excision sampling timepoint that best predict surgical cure in primary and renal hyperparathyroidism.
We will conduct a diagnostic test network meta-analysis to determine the iPTH criteria and post-parathyroid gland excision sampling timepoints most predictive of surgical cure. We registered the protocol with the Open Science Framework register of systematic reviews (OSF Registration; DOI: 10.17605/OSF.IO/4WEMJ). This protocol will be published under the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis for Protocols (PRISMA-P) (11). Any notable protocol amendments will be reported and published alongside the final review, which will be reported in accordance with the PRISMA statement (12).
We will include studies that investigate adult patients (≥18 years old) diagnosed with primary, secondary, and/or tertiary hyperparathyroidism who have undergone primary or revision parathyroidectomy via traditional midline neck incision or minimally invasive approach. There will be no further restrictions on the patient population.
Our index test is the iPTH assay using any validated laboratory instrument. We will be evaluating any of the published iPTH criteria (e.g., Miami, Vienna, Rome, or Halle criteria) and/or the post-parathyroid gland excision sampling time points (e.g., 5-, 10-, 15-, 20-, and 25-min post-parathyroid gland ligation).
Our reference standard will be surgical cure following parathyroidectomy. We will define surgical cure as the resolution of hyperparathyroidism (i.e., resolution of hypercalcemia and/or hyperparathyroidism) within 3–6 months of parathyroidectomy.
Our primary outcome will be centred around diagnostic test properties for all index tests as compared to the reference standard (e.g., pooled sensitivity, specificity, positive predictive value, negative predictive value, and likelihood ratios). We will also determine diagnostic odds ratio, post-test probabilities, and superiority index.
We will consider studies eligible if they are randomized or non-randomized trials, cross-sectional, case-control, cohort studies, or case series with more than five patients. All studies must report study outcomes in a way that permits analysis of diagnostic test properties. There will be no restrictions on length of follow-up for longitudinal studies.
Google Translate may be utilized for eligible articles published in non-English languages. This software, however, may not be appropriate for all languages, and so translators may be considered depending on the number of articles retrieved, in addition to the time and costs associated with each translation.
We will exclude articles that study pediatric populations and those that do not report data in manner that permits extraction of diagnostic test properties.
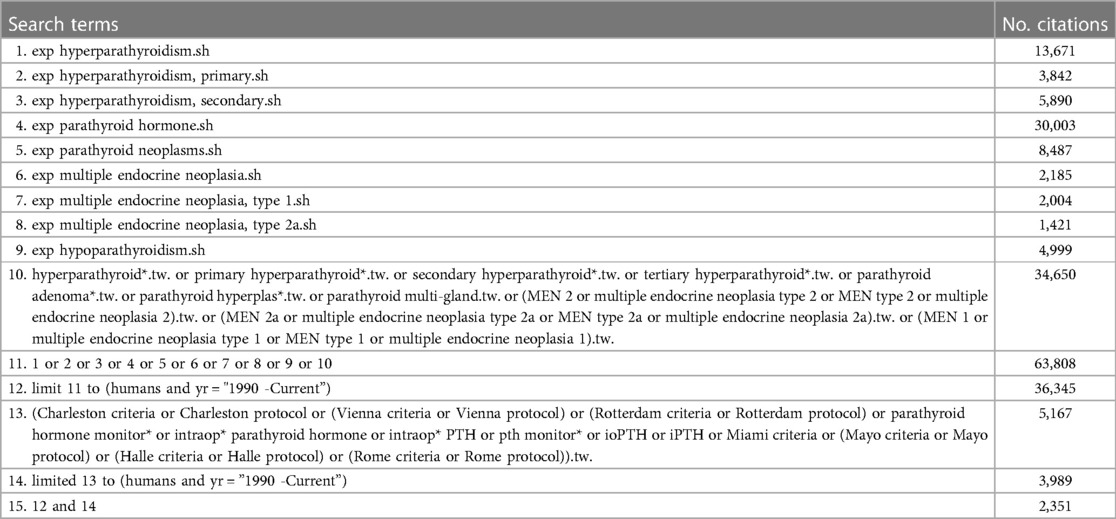
We will perform a database search of PubMed (Ovid), EMBASE (Ovid), Cochrane Central Register of Controlled Trials, and Web of Science from January 1, 1990, to July 20, 2023. We will include studies published after 1990 since operative use of PTH was first described in 1991 (13). We will include human studies and will not place any language restrictions. We will also perform a search of reference lists of relevant systematic reviews, narrative reviews, and meta-analyses. We will not perform a search of the grey literature.
We will include relevant search terms and MeSH headlines. All terms will be exploded when appropriate. We did evaluate the quality of the search by determining its ability to capture three pre-selected candidate articles. We will include the following example terms: primary, secondary, renal, and tertiary hyperparathyroidism, intraoperative parathyroid hormone monitoring, and iPTH criteria (e.g., Miami, Rome, Halle, etc.). The Medline search algorithm is presented in Appendix A.
A single reviewer will implement the search strategy with the help of librarian specialist and manage all citations. These combined citations will be exported into an article management software, Covidence (Melbourne, Australia), which removes duplicate articles. All extracted data will be managed in a piloted, customized Excel (Redmond, Washington, USA) spreadsheet.
We will begin screening with a pilot screening aid to assess agreement between two reviewers using 10% of the articles. We will define good agreement as a two-reviewer consensus rate of 75% based on the inclusion and exclusion decisions of reviewers. If this pilot identifies discrepancies of >75%, then we will consider modifying the inclusion criteria and report these protocol deviations in the final review.
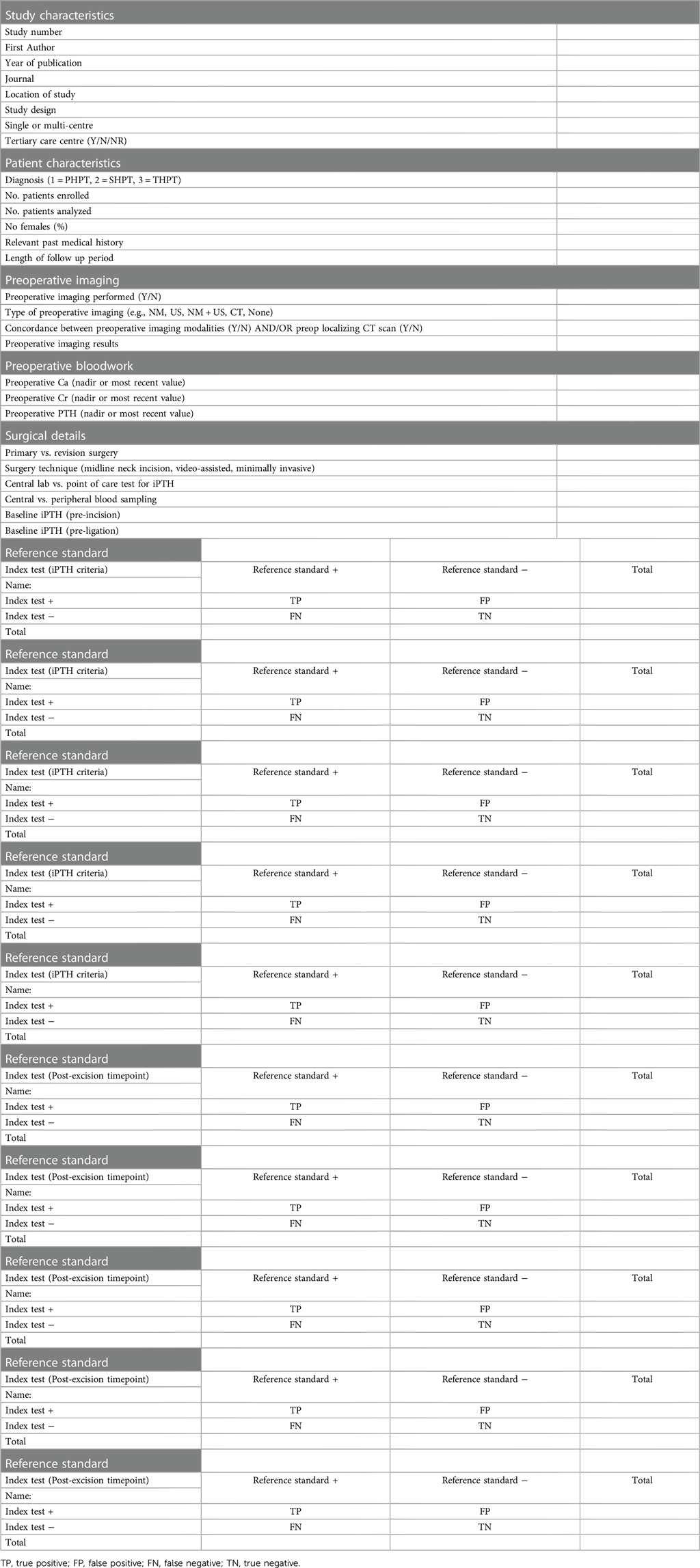
We will pilot a tailored extraction form by evaluating five articles to assess agreement between the reviewers. This extraction pilot will be evaluated by third reviewer and if deemed congruent between reviewers, then extraction for all full-text articles will proceed. We will evaluate study characteristics (e.g., name of first author, year of publication, country, gold standard, index tests), patient characteristics (e.g., gender, mean age, sample, method, cut-off level, type of disease, type of surgery, details of preoperative workup), and outcomes (i.e., true positive, false positive, true negative, false negative). All final extraction information will be performed by two reviewers and evaluated by a third reviewer. We have included the extraction form in Appendix B.
Two reviewers will critically appraise the selected studies using the Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) instrument (14). All disagreements will be solved by consensus review between the two reviewers and/or by a third reviewer. The methodological quality of individual studies will be reported in the final text and tables.
A descriptive synthesis will present the characteristics of included studies, critical appraisal results, and descriptions of the main findings. Where applicable, the descriptive synthesis will be summarized according to each iPTH criteria and/or post-gland excision sampling timepoint.
We will perform our network meta-analysis of diagnostic test accuracy using a Bayesian hierarchical framework with random effects using multiple models (15, 16). We will implement our analysis through a Markov Chain Monte Carlo simulation in WinBUGS, OpenBUGS, and R. Within our network diagram, the size of nodes will be proportional to the number of participants and the line connecting nodes will be proportional to the number of direct comparisons.
We will perform pairwise pooled analysis of diagnostic test characteristics, including sensitivity, specificity, likelihood ratios, diagnostic odds ratio, superiority index, and the area under the receiver operating curve. We will evaluate between-study heterogeneity using Cochrane Q and the inconsistency index (whereby I2 = 25%, 50%, and 75% will be indicative of low, moderate, and high statistical heterogeneity, respectively).
Our reference standard will be the resolution of hyperparathyroidism, as measured by circulating intact PTH level and/or corrected calcium level, at 3–6 months following surgery. Against this reference standard, we will be comparing the relative diagnostic outcomes for each index test. There remains controversy in the ideal pooled statistic for which to compare diagnostic test (17). Diagnostic odds ratio has been used to rank diagnostic tests, but its utility is hampered by its inability to weigh sensitivity and specificity independently and its lack of clinical applicability (18). An alternative statistic for ranking is the superiority index, which applies greater weight to index tests that perform well with both diagnostic test measures and lesser weight to those tests that perform well in one measure but poorly in another or perform poorly in both (19). Subgroup analysis may be challenging in the context of the chosen Bayesian network, but we will plan to perform sensitivity analyses, where applicable.
If there are at least ten studies of the index test are included in the meta-analysis, then we will perform a Deeks' test of asymmetry and funnel plot analysis to evaluate for publication bias (20).
We will report findings within the final publication in accordance with the PRISMA statement for diagnostic test accuracy meta-analysis (PRISMA-DTA) (21). A PRISMA flow diagram will be used for reporting the screening and article selection process, including the number of citations at each stage and the reasons for exclusion (i.e., full-text stage only). The discussion will include a summary of the major findings, the methodological limitations, and the application of these findings to clinical practice. The findings will be published in a peer-reviewed scientific journal and presented at national and/or international meetings. The published findings from the review will be disseminated to existing endocrine and otolaryngology–head and neck surgery networks.
This proposed meta-analysis has been registered in OSF and this protocol was developed to adhere to the PRISMA-P guidelines. Our proposed study will utilize pooled network analyses to determine the iPTH protocol and post-gland excision sampling timepoints most predictive of surgical cure in hyperparathyroidism. A network meta-analytic approach will permit direct and indirect comparisons and will facilitate ranking of iPTH criteria and, where applicable, post- excision sampling timepoints. These results will help to standardize the application of iPTH assays, optimize the use of these assays, and streamline healthcare expenditures in the management of hyperparathyroidism. Standardization of iPTH protocols may facilitate application in surgery for atypical parathyroid tumours and parathyroid carcinoma (22). In terms of possible final study limitations, there is the potential for inconsistent quality and selection bias in the reporting of included observational studies. We will employ a novel Bayesian statistical model to perform this network meta-analysis and provide a ranking of multiple diagnostic tests. Though hierarchical Bayesian models have been suggested for network meta-analysis, methodological challenges remain and so, development of our model will facilitate reproduction in future studies (23).
This study is exempt from institutional research board approval.
PS: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. KU: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. SY: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. MB: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. MG: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. MA: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. JY: Conceptualization, Writing – original draft, Writing – review & editing, Resources. HZ: Conceptualization, Methodology, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Bilezikian JP, Cusano NE, Khan AA, Liu JM, Marcocci C, Bandeira F. Primary hyperparathyroidism. Nat Rev Dis Primers. (2016) 2:16033. doi: 10.1038/nrdp.2016.33
2. Cannata-Andia JB, Carrera F. The pathophysiology of secondary hyperparathyroidism and the consequences of uncontrolled mineral metabolism in chronic kidney disease: the role of COSMOS. NDT Plus. (2008) 1:i2–6. doi: 10.1093/ndtplus/sfm037
3. Chan RK, Ruan DT, Gawande AA, Moore FD Jr. Surgery for hyperparathyroidism in image-negative patients. Arch Surg. (2008) 143:335–7. doi: 10.1001/archsurg.143.4.335
4. Walsh NJ, Sullivan BT, Duke WS, Terris DJ. Routine bilateral neck exploration and four-gland dissection remains unnecessary in modern parathyroid surgery. Laryngoscope Investig Otolaryngol. (2019) 4:188–92. doi: 10.1002/lio2.223
5. Khokar AM, Kuchta KM, Moo-Young TA, Winchester DJ, Prinz RA. Increasing trend of bilateral neck exploration in primary hyperparathyroidism. Am J Surg. (2020) 219:466–70. doi: 10.1016/j.amjsurg.2019.09.039
6. Wilhelm SM, Wang TS, Ruan DT, Lee JA, Asa SL, Duh QY, et al. The American association of endocrine surgeons guidelines for definitive management of primary hyperparathyroidism. JAMA Surg. (2016) 151:959–68. doi: 10.1001/jamasurg.2016.2310
7. Medas F, Cappellacci F, Canu GL, Noordzij JP, Erdas E, Calo PG. The role of rapid intraoperative parathyroid hormone (ioPTH) assay in determining outcome of parathyroidectomy in primary hyperparathyroidism: a systematic review and meta-analysis. Int J Surg. (2021) 92:106042. doi: 10.1016/j.ijsu.2021.106042
8. Silveira AA, Brescia MDG, Do Nascimento CP Jr, Arap SS, Montenegro FLM. Critical analysis of the intraoperative parathyroid hormone decrease during parathyroidectomy for secondary and tertiary hyperparathyroidism. Surgery. (2020) 168:1079–85. doi: 10.1016/j.surg.2020.06.043
9. Laforgia R, Tomasicchio G, Cavalera F, Sblendorio M, Spadone A, Anelli FM, et al. Management and surgical treatment of parathyroid carcinoma: a 6-year experience of a single centre of endocrine surgery unit. Front Endocrinol (Lausanne). (2023) 14:1278178. doi: 10.3389/fendo.2023.1278178
10. Khan ZF, Lew JI. Intraoperative parathyroid hormone monitoring in the surgical management of sporadic primary hyperparathyroidism. Endocrinol Metab (Seoul). (2019) 34:327–39. doi: 10.3803/EnM.2019.34.4.327
11. Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. (2015) 4:1. doi: 10.1186/2046-4053-4-1
12. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. (2010) 8:336–41. doi: 10.1016/j.ijsu.2010.02.007
13. Irvin GL 3rd, Dembrow VD, Prudhomme DL. Operative monitoring of parathyroid gland hyperfunction. Am J Surg. (1991) 162:299–302. doi: 10.1016/0002-9610(91)90135-Z
14. Whiting PF, Rutjes AW, Westwood ME, Mallett S, Deeks JJ, Reitsma JB, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. (2011) 155:529–36. doi: 10.7326/0003-4819-155-8-201110180-00009
15. Menten J, Lesaffre E. A general framework for comparative Bayesian meta-analysis of diagnostic studies. BMC Med Res Methodol. (2015) 15:70. doi: 10.1186/s12874-015-0061-7
16. Owen RK, Cooper NJ, Quinn TJ, Lees R, Sutton AJ. Network meta-analysis of diagnostic test accuracy studies identifies and ranks the optimal diagnostic tests and thresholds for health care policy and decision-making. J Clin Epidemiol. (2018) 99:64–74. doi: 10.1016/j.jclinepi.2018.03.005
17. Ge L, Pan B, Song F, Ma J, Zeraatkar D, Zhou J, et al. Comparing the diagnostic accuracy of five common tumour biomarkers and CA19-9 for pancreatic cancer: a protocol for a network meta-analysis of diagnostic test accuracy. BMJ Open. (2017) 7:e018175. doi: 10.1136/bmjopen-2017-018175
18. Glas AS, Lijmer JG, Prins MH, Bonsel GJ, Bossuyt PM. The diagnostic odds ratio: a single indicator of test performance. J Clin Epidemiol. (2003) 56:1129–35. doi: 10.1016/S0895-4356(03)00177-X
19. Deutsch R, Mindt MR. Quantifying relative superiority among many binary-valued diagnostic tests in the presence of a gold standard. J Data Sci. (2021) 7:161–77. doi: 10.6339/JDS.2009.07(2).450
20. Van Enst WA, Ochodo E, Scholten RJ, Hooft L, Leeflang MM. Investigation of publication bias in meta-analyses of diagnostic test accuracy: a meta-epidemiological study. BMC Med Res Methodol. (2014) 14:70. doi: 10.1186/1471-2288-14-70
21. Mcinnes MDF, Moher D, Thombs BD, Mcgrath TA, Bossuyt PM, Clifford T, et al. Preferred reporting items for a systematic review and meta-analysis of diagnostic test accuracy studies: the PRISMA-DTA statement. JAMA. (2018) 319:388–96. doi: 10.1001/jama.2017.19163
22. Gurrado A, Pasculli A, Avenia N, Bellantone R, Boniardi M, Merante Boschin I, et al. Parathyroid retrospective analysis of neoplasms incidence (pTRANI study): an Italian multicenter study on parathyroid carcinoma and atypical parathyroid tumour. J Clin Med. (2023) 12(19):6297. doi: 10.3390/jcm12196297
23. Ma X, Lian Q, Chu H, Ibrahim JG, Chen Y. A Bayesian hierarchical model for network meta-analysis of multiple diagnostic tests. Biostatistics. (2018) 19:87–102. doi: 10.1093/biostatistics/kxx025
.
.
Keywords: parathyroid, hyperparathyroidism, network meta-analysis, surgery, intraoperative parathyroid hormone (PTH) assay
Citation: Staibano P, Um K, Yu S, Bhandari M, Gupta MK, Au M, (Ted) Young J and Zhang H (2024) Intraoperative parathyroid hormone monitoring in parathyroidectomy for hyperparathyroidism: a protocol for a network meta-analysis of diagnostic test accuracy. Front. Surg. 10:1298611. doi: 10.3389/fsurg.2023.1298611
Received: 21 September 2023; Accepted: 11 December 2023;
Published: 4 January 2024.
Edited by:
Angela Pezzolla, Azienda Ospedaliero Universitaria Consorziale Policlinico di Bari, ItalyReviewed by:
Marco Bononi, Sapienza University of Rome, Italy© 2024 Staibano, Um, Yu, Bhandari, Gupta, Au, (Ted) Young and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Phillip Staibano cGhpbGxpcC5zdGFpYmFub0BtZWRwb3J0YWwuY2E=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.