
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Surg., 28 July 2023
Sec. Neurosurgery
Volume 10 - 2023 | https://doi.org/10.3389/fsurg.2023.1222595
 Edin Nevzati1,2*†,‡
Edin Nevzati1,2*†,‡ Nicolas Poletti3,†Alexander Spiessberger4Sabrina Bäbler1,2
Nicolas Poletti3,†Alexander Spiessberger4Sabrina Bäbler1,2 Gabriela Studer5Christian Riklin6
Gabriela Studer5Christian Riklin6 Joachim Diebold7Grégoire P. Chatain8Michael Finn8Jens-Peter Witt8Manuel Moser1,2
Joachim Diebold7Grégoire P. Chatain8Michael Finn8Jens-Peter Witt8Manuel Moser1,2 Luigi Mariani3
Luigi Mariani3
Background: Tumors of the vertebral column consist of primary spinal tumors and malignancies metastasizing to the spine. Although primary spine tumors are rare, metastases to the spine have gradually increased over past decades because of aging populations and improved survival for various cancer subtypes achieved by advances in cancer therapy. Metastases to the vertebral column occur in up to 70% of cancer patients, with 10% of patients demonstrating epidural spinal cord compression. Therefore, many cancer patients may face spinal surgical intervention during their chronic illness; such interventions range from simple cement augmentation over decompression of neural elements to extended instrumentation or spinal reconstruction. However, precise surgical treatment guidelines do not exist, likely due to the lack of robust, long-term clinical outcomes data and the overall heterogeneous nature of spinal tumors. Objectives of launching the Swiss Spinal Tumor Registry (Swiss-STR) are to collect and analyze high-quality, prospective, observational data on treatment patterns, clinical outcomes, and health-related quality of life (HRQoL) in adult patients undergoing spinal tumor surgery. This narrative review discusses our rationale and process of establishing this spinal cancer registry.
Methods: A REDCap-based registry was created for the standardized collection of clinical, radiographic, surgical, histological, radio-oncologial and oncological variables, as well as patient-reported outcome measures (PROMs).
Discussion: We propose that the Swiss-STR will inform on the effectiveness of current practices in spinal oncology and their impact on patient outcomes. Furthermore, the registry will enable better categorization of the various clinical presentations of spinal tumors, thereby facilitating treatment recommendations, defining the socio-economic burden on the healthcare system, and improving the quality of care. In cases of rare tumors, the multi-center data pooling will fill significant data gaps to yield better understanding of these entities. Finally, our two-step approach first implements a high-quality registry with efficient electronic data capture strategies across hospital sites in Switzerland, and second follows with potential to expand internationally, thus fostering future international scientific collaboration to further push the envelope in cancer research.
Tumors of the vertebral column consist of primary spinal tumors and secondary malignancies metastasizing to the spine. Primary tumors arise from the spinal cord, cauda equina, nerve roots, and spinal meninges. The surrounding vertebrae and their enveloping soft tissues can also give rise to primary tumors of the vertebral column. Compared with secondary malignancies to the spine, primary spinal tumors are relatively rare (1–3) and account for less than 10% of all vertebral column tumors (4) (Figure 1). Considering the aging population along with improved survival for multiple cancer subtypes through ongoing advances in cancer therapy, the rising incidence of metastatic spine disease is predicted to continue (5).

Figure 1. Spinal tumors can occur in any part of the spine. This figure depicts a classification system of spinal tumors relative to the spinal canal and the most frequent entities.
The spine is the most common site for bone metastases (6). Up to 70% of cancer patients develop spinal metastases during the course of their disease (7), with pain as the most frequent initial symptom (8). However, epidural tumor extension can also lead to neural compression and potential neurological deficits, as up to 10% of cancer patients develop metastatic spinal cord compression (7). Furthermore, tumors affecting the osseous spine can significantly impair mechanical integrity, potentially leading to spinal instability. The treatment of metastatic spinal lesions is considered palliative and aims to alleviate pain, maintain or improve neurological function, and restore mechanical stability. For patients with oligometastatic disease, the therapeutic intention, which is usually locally curative, requires challenging surgical or radiotherapeutical treatments. Treatment decision-making is based on neurologic, mechanical, oncologic, and systemic considerations by a multidisciplinary team effort of surgeons, radiation and medical oncologists, pain specialists, and interventional radiologists (9, 10).
As modalities available to treat metastatic spine disease evolve, the guiding principle is to improve quality of life and preserve ambulation in affected patients. However, treatment modalities vary not only globally but among different institutions within individual countries. Therefore, the potential to improve patient outcome and reduce the disease-associated socio-economic burden remains exceptionally high. Unlike metastases, primary spinal tumors represent uncommon lesions that affect a minority of the population. Nonetheless, these tumors can cause significant morbidity due to limb dysfunction and increased mortality. Consequently, the rarity of these tumors can significantly constrain the extent of research, treatment decision, and health care planning to affect patient outcomes (1).
Surgical treatment in spinal oncology has gained significant attention for its ability to reduce pain, maintain or improve neurological function, restore mechanical stability, and even improve life expectancy in patients with metastatic lesions (11–14). The implementation of stereotactic body radiation therapy (SBRT) has lessened the invasiveness of surgical treatment (9). Patients with a mechanically stable vertebral body formerly underwent radiation as local single modality treatment with palliative or locally curative (i.e., ablative) intent. SBRT has improved treatment by safely delivering high doses of radiation to the tumor while minimizing radiation dose to the surrounding organs at risk, such as the spinal cord (15, 16).
Despite recent eminent progress in the field of spinal oncology, surgery in spinal malignancies remains palliative. The surgical treatment plan not only relies on neurological and biomechanical aspects but considers the systemic tumor effects and patient's expectations. It is well accepted that surgery improves quality of life (QoL) in metastatic spine disease, even for patients whose life expectancy is <3 months (17). However, the tolerance for complications is relatively low in this patient population awaiting adjuvant therapy. For example, a surgical side infection can significantly reduce the life expectancy of affected individuals (18). Therefore, a tailored surgical approach to lower perioperative morbidity is of outmost importance for this population. The broad armamentarium in spine surgery has launched healthcare providers into uncharted terrain. Therefore, more often, the spine surgeon must weigh to what extent spine surgery can be applied in a palliative situation.
The objective of the Swiss Spine Tumor Registry (Swiss-STR) is to obtain prospectively collected data in adult patients (age >18 years) undergoing surgery for tumors affecting the spine, irrespective of suffering from metastatic spine disease or primary spinal tumors. The cornerstone parameters to define crucial characteristics in spinal oncology include patient-reported outcome measures (PROMs) using established health-related quality of life (HRQoL) questionnaires, assessment of neurological performance, radiographic assessment to evaluate mechanical stability of the spine, oncological assessment, and tumor tissue (and whole blood) preservation. Standardized measuring tools of Swiss-STR are summarized (Table 1). Furthermore, the establishment of a biobank forms a main component of personalized medicine that allows for proteomic, metabolomic and epigenetic testing: these components form the three main pillars in cancer research (19).
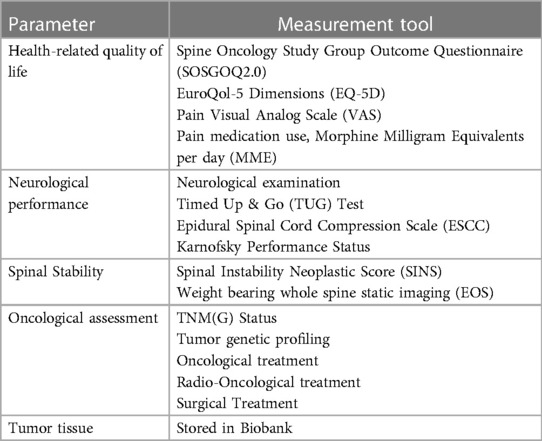
Table 1. Standardized measuring tools.
Our study protocol was reviewed by the corresponding state institutional review board (Ethical Committee of Northwestern and Central Switzerland) and deemed not to require Institutional Review Board approval, as the registry exclusively collects encrypted prospective patient data. Written informed consent by patients will be obtained.
Various assessments have been developed to quantify how spinal tumors impact the patient's psychological, socio-economical, and medical condition. The HRQoL assessment aims to record how the disease and treatment affects patients' overall function and well being. Although general questionnaires have been used to assess metrics in patients with spinal tumors, a disease-specific survey was first introduced as the Spine Oncology Study Group Outcome Questionnaire (SOSG-OQ2.0) to measure QoL in patients with spinal metastases (20–22). This 27-question survey covers six dimensions that include pain, mental health, social interaction, bowel and bladder function, physical activity and neurological function. To date, validated translations of the English SOSG-OQ2.0 are available in Italian, Thai, Chinese, Dutch, and German (23–27); the latter is used for our registry. The EuroQol-5 Dimensions Questionnaire (EQ-5D) is a well known and widely used tool of 5 questions covering 5 dimensions, namely ambulation, autonomy, activities of daily life, pain, and psychological situation. It has a high shared variance with the SOSG-OQ (21). A validated German translation of the EQ-5D will be used for our registry (28). As part of this health-related QoL assessment, the pain numeric rating scale (NRS) will be scored and pain medication, particularly opioid use, will be monitored over time.
Neurological impairment and the presence of spinal cord and/or radicular compression play a key role in treatment decision-making. In their systematic review, Nguyen et al. (29) assessed ambulation in patients with spinal metastases and found there was no standard measure of ambulation for this population. Rather, most studies included classified patients as either ambulatory or non-ambulatory, and a few designated ambulatory aided. Of the 12 prospective studies, 11 studies used direct observation to grade ambulation though the method of determination was rarely described.
Given the significance of ambulation on QoL and overall morbidity, quantification by standardized tests rather than observation (observational “in or out” criteria) or questionnaires is needed. For this measure, the widely used Timed Up & Go (TUG) test will be applied to assess ambulatory function (30). Evaluated in general oncologic patients undergoing elective surgery, the TUG better predicted postoperative morbidity than the American Society of Anaesthesiologists (ASA) Score (31). Although it has also been evaluated in degenerative spine disease (32), no studies have thus far evaluated TUG exclusively in spinal oncologic patients.
Additionally, the Karnofsky Performance Status will be assessed as a basic performance status in oncological patients (33). Besides assessing obvious neurological deficits in the clinical assessment, an anatomical, MRI-based 6-point grading system will delineate the degree of spinal cord compression. The epidural spinal cord compression (ESCC) scale was introduced in 2010 by Bilsky et al. The rationale behind this grading system was to provide a reliable tool for assessment of spinal cord compression, and thus consistency in reporting outcomes of treated spinal tumors (34).
Mechanical instability as a result of a neoplastic process can lead to an indication for surgery, independently from the presence or absence of neural compression or estimated response to systemic and radiation treatment (35). To facilitate assessment of stability and unite reporting among health care providers, the Spinal Instability Neoplastic Score (SINS), introduced in 2010 (36), was based on conventional radiography and computed tomography (CT) scans. The SINS is calculated from 6 components and classifies lesions as stable, potentially unstable, and unstable. Although the role of sagittal imbalance has been analyzed extensively in deformity surgery (37), it has not yet in spinal tumors (38). Ideal sagittal alignment of the spine improves biomechanical efficiency and reduces energy expenditure on accessory muscles to stay erect. To analyze sagittal balance in tumor patients, data from a weight-bearing whole-spine-posture imaging is included in the registry.
In summary, all patients recruited for Swiss-STR will have baseline spinal CT, contrast-enhanced MRI, and x-ray before surgery. A postoperative MRI scan will be conducted to assess tumorreesction/resdidual tumor burden, and hardware placement will be assessed on postoperative x-ray.
The most common tumors metastasizing to the spine are prostate and lung cancer in males, and breast cancer and lung cancer in females (39, 40). Overall survival has improved significantly over the last two decades for all three pathologies (41, 42). A growing number of cancer-specific treatment options have emerged for metastatic cancer (43). Because of longer survival for cancer patients, demographics have shifted and many survivors are now older than 65. This comes with more age-related morbidity and thus more complex cases (44). A new paradigm emerged as metastatic cancer can be a chronic disease rather than a lethal diagnosis.
Scores currently available that predict survival, when deciding whether or not to operate on a patient, originated in the 1990s and early 2000s, like the Bauer-, Tokuhashi- and Tomita-Score (1995, 1990 and 2001) (13, 45, 46). Although revised scores were developed, their performance is poor because treatment options, demographics, and survival differ substantially from the time these scores were created (47). In their 2016 systematic review, Zoccali et al. found the accuracy of the Tokuhashi-Score in predicting survival was only 63%, with a decreasing trend over time (48).
This highlights the importance of developing new scoring systems with up-to-date patient data. Increasing evidence has emerged that preoperative survival estimation should rely on flexible model techniques, such as machine learning (49). Emerging new treatment options in metastatic cancer are targeted therapies and immunotherapies. An increasing number of molecular subtypes and thus potential targets exist for cancer therapy (50). In their review, Yuan et al. identified 356 clinical studies worldwide in 2019 investigating treatment of non-small cell lung cancer with combinations of immunotherapy (51). Given that the problems with targeted therapies are acquired resistances (52), there is a need to analyze a tumor's molecular evolution when metastasizing to the spine.
To evaluate the important factors affecting the outcome in our spinal tumor patients, we will document spine-related symptoms, radiological features, and treatment of the spine and also oncological, radio-oncological, and surgical details of the primary tumor, together with secondary diagnosis and general health status. The 12 most common secondary diseases and risk factors with corresponding important laboratory values and medication will be documented Supplementary Table S1. To assess nutrition status, we will collect the nutrition risk score and the Scored Patient-Generated Subjective Global Assessment (SG-SGA)- a detailed and well evaluated questionnaire to assess nutrition status in oncologic patients (53, 54). Cachexia and sarcopenia are considered important risk factors for complications not only when undergoing surgery but also radio- or chemotherapy (55). Several recent studies have shown a significant correlation between sarcopenia and postoperative complications and mortality in spinal tumor patients undergoing surgery (56, 57). The sarcopenia index of the psoas will be measured in preoperative CT scans at the L3 level as previously described (56).
Spinal oncology research based on the registry will involve collaborations with many centers in diverse locations relying on electronic networks that enable submission, analysis, and sharing of data. However, paramount importance is to secure data collection, storage, and export for any multi-center research study. Swiss-STR will use the Research Electronic Data Capture (REDCap®, Vanderbilt University) software application system that has successfully supported translational research projects between academic centers (58).
The comprehensive data collection forming the registry will be time consuming and rely on dedicated investigators and study nurses. However, extraction of data directly from electronic health record systems into REDCap has a great potential to facilitate and optimize the maintenance of the registry. After first establishing Swiss-STR at the Cantonal Hospital of Lucerne in Switzerland, patient recruitment began on January 1, 2023. Our next goal is to involve other public spine centers with expertise in spinal oncology on a national and international scale. The value of the registry heavily relies on the data quality and quality control procedures. Evaluation of data quality in tumor registries is expressed by the dimensions of comparability, completeness, validity, and timelines (59). Although these attributes primarily evolved for large scale/national registries, the principles can also be applied to institutional-based registries.
The data collected in the Swiss-STR adheres to agreed international guidelines in the diagnosis and treatment of spinal oncological disease, thereby ensuring comparability of entered parameters. All surgically-treated spinal oncological patients will be included in participating centers by a dedicated, clinical practice of approved staff who can complete prospective data collection. The validity/accuracy of data collection is defined as the proportion of cases in a dataset with a given characteristic which truly have the attribute (59). Participating centers will hold periodic scientific exchanges to assess the growth of the clinical database and an independent expert data-monitoring committee will assess data quality in timely defined audits, using reabstracting and recoding methods (60). The term timeline relates to the rapidity in collecting, processing, and reporting complete data out of the registry (61). As the registry is an institutional-driven prospective-data-gathering entity, data will primarily flow into data capture system to enable timely available, efficient data processing. Annual reports will provide basic epidemiological data while research projects can be coordinated and specific data can be allocated to address a scientific question.
In this review, we present our rationale for the need and process of establishing a spinal cancer registry called the Swiss-STR. Relevant information, not limited to spinal lesions, but encompassing oncological details, surgical intervention, overall performance status, and QoL will be collected in accordance with the pertinent literature on spinal oncology. The registry will provide referring caregivers and healthcare professionals with a valuable tool to standardize, assess, and compare current treatments in spinal cancer patients. Moreover, the Swiss-STR will serve as a catalyst in the development of evidence-based treatment algorithms, foster scientific collaboration among centers, and address a number of remaining open questions in the management of tumors affecting the spine.
While primary spine tumors are treated in a few, highly specialized centers, metastatic lesions to the spine are treated at many institutions that offer complex spine surgery. Recent progress in defining key parameters necessary for clear patient description has significantly facilitated communication in the field of spinal oncology (5). However, if surgery is indicated, many treatment options might be offered for similar conditions and the final management strategy for an oncological spine disorder is often decided by the spine surgeon. This scenario makes it difficult to perform a randomized cohort study of surgical techniques (62). The registry will overcome this limitation by a prospective collection consisting of large-scale, high-quality data from which the effect of confounding variables can be further adjusted. The registry will conduct primary descriptive studies in surgically treated spinal tumors and assess the effectiveness of interventions. Unbiased, continuous, and robust patient data permits monitoring of the socio-economic burden of this healthcare condition and assessing of clinical outcomes.
The heterogeneity of tumors that affect the spine and the multimodal, interdisciplinary approach in patient care presupposes precision medicine in the implementation of a purposeful oncological treatment. Molecular cancer-tissue analysis has played a role in changing the treatment paradigm: the more stochastic “one-size-fits-all” cytotoxic treatment approach is transforming toward precise assessment and identification of tumor-specific vulnerabilities to define potential drug targets.
Modern systemic treatment modalities attack cancer cells through two primary methods: (1) pathway-based targeted therapy selectively disrupts pathways necessary for cancer cell survival or growth, while (2) immunotherapy artificially modulates a patient's immune system to generate a response against cancer cells (63). However, a major limitation of targeted anticancer therapies is intrinsic or acquired drug resistance. Molecular disease monitoring represents a logical way forward to delay and ultimately overcome the development of drug resistance (64). The establishment of a biobank allows for insight into tumor biology. Subsequently, genetic, transcriptional, and proteomic analyses becomes feasible and possibly patient-derived in vitro cell models. With the available clinical data, association of genomic features with clinical information can be defined and thereby outline the importance of a simultaneous comprehensive clinical registry.
Since the initial launch of case-based cancer registries in the early 1900s (65), registries have expanded globally to yield robust evidence in healthcare research (66). Generally, three types of cancer registries exist. First, facility-based registries collect information about patients treated in that institution. Second, specialty-based registries collect data about one specific type of medical condition. Third, central registries collect information about patients in a certain geographic area (65, 67). Notably, our specialty-based registry aims to provide interested institutions with a comprehensive data assessment tool while facilitating data pooling and scientific collaboration. Although different international registries are available on spinal tumors, the Swiss-STR creates a tailored prospective-data-capture platform to facilitate fast and robust data transfer from common patient electronic charts.
Swiss-STR is an important step in documenting treatment and outcome of a complex disease that affects a broad population suffering from cancer. Furthermore, this registry will help define its socio-economic burden and reflect what is currently believed to be the best medical treatment or standard of care. Finally, the registry will help to foster research between institutions and thereby further push the envelope in spinal oncology research.
EN: Conceptualization, Methodology, Resources, Writing- Original Draft, Project administration; NP: Writing- Original Draft, Data Curation; AS: Conceptualization, Writing- Review &; Editing; SB: Data Curation, Project administration, Writing- Review & Editing; GS: Data Curation, Writing- Review & Editing; CR: Data Curation, Writing- Review & Editing; JD: Data Curation, Writing- Review & Editing; GPC: Data Curation, Writing- Review &Editing; MF: Data Curation, Writing- Review & Editing; J-PW: Data Curation, Writing- Review & Editing; MM: Conceptualization, Methodology, Writing- Review & Editing; LM: Methodology, Supervision, Project administration, Writing- Review & Editing. All authors contributed to the article and approved the submitted version.
We would like to thank Dr. Irène Frank from the Clinical Trial Unit Lucerne and Franziska Thoms for their support in developing the registry. We would like to thank Majlinda Kalanderi for the medical illustrations. We would like to thank Mary Kemper for her assistance with medical editing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fsurg.2023.1222595/full#supplementary-material
1. Duong LM, McCarthy BJ, McLendon RE, Dolecek TA, Kruchko C, Douglas LL, et al. Descriptive epidemiology of malignant and nonmalignant primary spinal cord, spinal meninges, and cauda equina tumors, United States, 2004–2007. Cancer. (2012) 118(17):4220–7. doi: 10.1002/cncr.27390
2. Ropper AE, Cahill KS, Hanna JW, McCarthy EF, Gokaslan ZL, Chi JH. Primary vertebral tumors: a review of epidemiologic, histological, and imaging findings, part I: benign tumors. Neurosurgery. (2011) 69(6):1171–80. doi: 10.1227/NEU.0b013e31822b8107
3. Ropper AE, Cahill KS, Hanna JW, McCarthy EF, Gokaslan ZL, Chi JH. Primary vertebral tumors: a review of epidemiologic, histological and imaging findings, part II: locally aggressive and malignant tumors. Neurosurgery. (2012) 70(1):211–9. doi: 10.1227/NEU.0b013e31822d5f17
4. Hsu W, Kosztowski TA, Zaidi HA, Dorsi M, Gokaslan ZL, Wolinsky JP. Multidisciplinary management of primary tumors of the vertebral column. Curr Treat Options Oncol. (2009) 10(1–2):107–25. doi: 10.1007/s11864-009-0102-8
5. Barzilai O, Boriani S, Fisher CG, Sahgal A, Verlaan JJ, Gokaslan ZL, et al. Essential concepts for the management of metastatic spine disease: what the surgeon should know and practice. Global Spine J. (2019) 9(1 Suppl):98S–107S. doi: 10.1177/2192568219830323
6. Hatrick NC, Lucas JD, Timothy AR, Smith MA. The surgical treatment of metastatic disease of the spine. Radiother Oncol. (2000) 56(3):335–9. doi: 10.1016/S0167-8140(00)00199-7
7. Jacobs WB, Perrin RG. Evaluation and treatment of spinal metastases: an overview. Neurosurg Focus. (2001) 11(6):e10. doi: 10.3171/foc.2001.11.6.11
8. Bollen L, Dijkstra SPD, Bartels R, de Graeff A, Poelma DLH, Brouwer T, et al. Clinical management of spinal metastases-the Dutch national guideline. Eur J Cancer. (2018) 104:81–90. doi: 10.1016/j.ejca.2018.08.028
9. Laufer I, Rubin DG, Lis E, Cox BW, Stubblefield MD, Yamada Y, et al. The NOMS framework: approach to the treatment of spinal metastatic tumors. Oncologist. (2013) 18(6):744–51. doi: 10.1634/theoncologist.2012-0293
10. Sciubba DM, Pennington Z, Colman MW, Goodwin CR, Laufer I, Patt JC, et al. Spinal metastases 2021: a review of the current state of the art and future directions. Spine J. (2021) 21(9):1414–29. doi: 10.1016/j.spinee.2021.04.012
11. Patchell RA, Tibbs PA, Regine WF, Payne R, Saris S, Kryscio RJ, et al. Direct decompressive surgical resection in the treatment of spinal cord compression caused by metastatic cancer: a randomised trial. Lancet. (2005) 366(9486):643–8. doi: 10.1016/S0140-6736(05)66954-1
12. Kim CH, Chung CK, Jahng TA, Kim HJ. Resumption of ambulatory status after surgery for nonambulatory patients with epidural spinal metastasis. Spine J. (2011) 11(11):1015–23. doi: 10.1016/j.spinee.2011.09.007
13. Tomita K, Kawahara N, Kobayashi T, Yoshida A, Murakami H, Akamaru T. Surgical strategy for spinal metastases. Spine (Phila Pa 1976). (2001) 26(3):298–306. doi: 10.1097/00007632-200102010-00016
14. Falicov A, Fisher CG, Sparkes J, Boyd MC, Wing PC, Dvorak MF. Impact of surgical intervention on quality of life in patients with spinal metastases. Spine (Phila Pa 1976). (2006) 31(24):2849–56. doi: 10.1097/01.brs.0000245838.37817.40
15. Bilsky MH, Yamada Y, Yenice KM, Lovelock M, Hunt M, Gutin PH, et al. Intensity-modulated stereotactic radiotherapy of paraspinal tumors: a preliminary report. Neurosurgery. (2004) 54(4):823–30; discussion 30–1. doi: 10.1227/01.NEU.0000114263.01917.1E
16. Yamada Y, Bilsky MH, Lovelock DM, Venkatraman ES, Toner S, Johnson J, et al. High-dose, single-fraction image-guided intensity-modulated radiotherapy for metastatic spinal lesions. Int J Radiat Oncol Biol Phys. (2008) 71(2):484–90. doi: 10.1016/j.ijrobp.2007.11.046
17. Dea N, Versteeg AL, Sahgal A, Verlaan JJ, Charest-Morin R, Rhines LD, et al. Metastatic spine disease: should patients with short life expectancy be denied surgical care? An international retrospective cohort study. Neurosurgery. (2020) 87(2):303–11. doi: 10.1093/neuros/nyz472
18. Quraishi NA, Ahmed MS, Arealis G, Boszczyk BM, Edwards KL. Does surgical site infection influence neurological outcome and survival in patients undergoing surgery for metastatic spinal cord compression? Eur Spine J. (2019) 28(4):792–7. doi: 10.1007/s00586-018-5797-4
19. Baghel R, Maan K, Haritwal T, Rana P. Chapter 2—integration of epigenomics and metabolomics: from biomarkers discovery to personalized medicine. In: Agrawala PK, Rana P, editors. Epigenetics and metabolomics. 28. London: Academic Press (Elsevier) (2021). p. 31–73.
20. Paulino Pereira NR, Janssen SJ, Raskin KA, Hornicek FJ, Ferrone ML, Shin JH, et al. Most efficient questionnaires to measure quality of life, physical function, and pain in patients with metastatic spine disease: a cross-sectional prospective survey study. Spine J. (2017) 17(7):953–61. doi: 10.1016/j.spinee.2017.02.006
21. Janssen SJ, Teunis T, van Dijk E, Ferrone ML, Shin JH, Hornicek F, et al. Validation of the spine oncology study group-outcomes questionnaire to assess quality of life in patients with metastatic spine disease. Spine J. (2017) 17(6):768–76. doi: 10.1016/j.spinee.2015.07.456
22. Versteeg AL, Sahgal A, Rhines LD, Sciubba DM, Schuster JM, Weber MH, et al. Psychometric evaluation and adaptation of the spine oncology study group outcomes questionnaire to evaluate health-related quality of life in patients with spinal metastases. Cancer. (2018) 124(8):1828–38. doi: 10.1002/cncr.31240
23. Brodano GB, Pesce E, Griffoni C, Carretta E, Noli LE, Errani C, et al. Adaptation and validation of the spine oncology study group outcomes questionnaire in Italian language. Global Spine J. (2022):21925682221083913. doi: 10.1177/21925682221083913.35344384
24. Luksanapruksa P, Phikunsri P, Trathitephun W, Santipas B, Suvithayasiri S, Wattanapaiboon K, et al. Validity and reliability of the Thai version of the spine oncology study group outcomes questionnaire version 2.0 to assess quality of life in patients with spinal metastasis. Spine J. (2021) 21(11):1920–4. doi: 10.1016/j.spinee.2021.05.010
25. Zhai S, Xu N, Liu S, Liu Z, Liu X, Wei F. Cross-cultural adaptation and validation of the Chinese version of the spine oncology study group outcomes questionnaire. Front Oncol. (2022) 12:1016258. doi: 10.3389/fonc.2022.1016258
26. Gal R, van der Velden JM, Bach DC, Verlaan JJ, Geuze RE, Rutges JP, et al. Translation and validation of the Dutch spine oncology study group outcomes questionnaire (SOSGOQ2.0) to evaluate health-related quality of life in patients with symptomatic spinal metastases. BMC Musculoskelet Disord. (2022) 23(1):1009. doi: 10.1186/s12891-022-05837-1
27. Datzmann T, Kisel W, Kramer J, Dreimann M, Muller-Broich JD, Netzer C, et al. eCross-cultural adaptation of the spine oncology-specific SOSGOQ2.0 questionnaire to German language and the assessment of its validity and reliability in the clinical setting. BMC Cancer. (2021) 21(1):1044. doi: 10.1186/s12885-021-08578-x
28. Greiner W, Claes C, Busschbach JJ, von der Schulenburg JM. Validating the EQ-5D with time trade off for the German population. Eur J Health Econ. (2005) 6(2):124–30. doi: 10.1007/s10198-004-0264-z
29. Nguyen L, Agaronnik N, Ferrone ML, Katz JN, Schoenfeld AJ. Evaluating ambulatory function as an outcome following treatment for spinal metastases: a systematic review. Spine J. (2021) 21(9):1430–9. doi: 10.1016/j.spinee.2021.05.001
30. Bohannon RW. Reference values for the timed up and go test: a descriptive meta-analysis. J Geriatr Phys Ther. (2006) 29(2):64–8. doi: 10.1519/00139143-200608000-00004
31. Huisman MG, van Leeuwen BL, Ugolini G, Montroni I, Spiliotis J, Stabilini C, et al. “Timed up & go”: a screening tool for predicting 30-day morbidity in onco-geriatric surgical patients? A multicenter cohort study. PLoS One. (2014) 9(1):e86863. doi: 10.1371/journal.pone.0086863
32. Gautschi OP, Smoll NR, Corniola MV, Joswig H, Chau I, Hildebrandt G, et al. Validity and reliability of a measurement of objective functional impairment in lumbar degenerative disc disease: the timed up and go (TUG) test. Neurosurgery. (2016) 79(2):270–8. doi: 10.1227/NEU.0000000000001195
33. Bollen L, Jacobs WCH, Van der Linden YM, Van der Hel O, Taal W, Dijkstra PDS. A systematic review of prognostic factors predicting survival in patients with spinal bone metastases. Eur Spine J. (2018) 27(4):799–805. doi: 10.1007/s00586-017-5320-3
34. Bilsky MH, Laufer I, Fourney DR, Groff M, Schmidt MH, Varga PP, et al. Reliability analysis of the epidural spinal cord compression scale. J Neurosurg Spine. (2010) 13(3):324–8. doi: 10.3171/2010.3.SPINE09459
35. Barzilai O, Fisher CG, Bilsky MH. State of the art treatment of spinal metastatic disease. Neurosurgery. (2018) 82(6):757–69. doi: 10.1093/neuros/nyx567
36. Fisher CG, DiPaola CP, Ryken TC, Bilsky MH, Shaffrey CI, Berven SH, et al. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the spine oncology study group. Spine (Phila Pa 1976). (2010) 35(22):E1221–9. doi: 10.1097/BRS.0b013e3181e16ae2
37. Le Huec JC, Thompson W, Mohsinaly Y, Barrey C, Faundez A. Sagittal balance of the spine. Eur Spine J. (2019) 28(9):1889–905. doi: 10.1007/s00586-019-06083-1
38. Sankey EW, Park C, Howell EP, Pennington Z, Abd-El-Barr M, Karikari IO, et al. Importance of spinal alignment in primary and metastatic spine tumors. World Neurosurg. (2019) 132:118–28. doi: 10.1016/j.wneu.2019.08.161
39. Macedo F, Ladeira K, Pinho F, Saraiva N, Bonito N, Pinto L, et al. Bone metastases: an overview. Oncol Rev. (2017) 11(1):321. doi: 10.4081/oncol.2017.321
40. Kakhki VR, Anvari K, Sadeghi R, Mahmoudian AS, Torabian-Kakhki M. Pattern and distribution of bone metastases in common malignant tumors. Nucl Med Rev Cent East Eur. (2013) 16(2):66–9. doi: 10.5603/NMR.2013.0037
41. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. (2016) 66(1):7–30. doi: 10.3322/caac.21332
42. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. (2019) 69(1):7–34. doi: 10.3322/caac.21551
43. Schanne DH, Heitmann J, Guckenberger M, Andratschke NHJ. Evolution of treatment strategies for oligometastatic NSCLC patients—a systematic review of the literature. Cancer Treat Rev. (2019) 80:101892. doi: 10.1016/j.ctrv.2019.101892
44. Parry C, Kent EE, Mariotto AB, Alfano CM, Rowland JH. Cancer survivors: a booming population. Cancer Epidemiol Biomarkers Prev. (2011) 20(10):1996–2005. doi: 10.1158/1055-9965.EPI-11-0729
45. Tokuhashi Y, Matsuzaki H, Toriyama S, Kawano H, Ohsaka S. Scoring system for the preoperative evaluation of metastatic spine tumor prognosis. Spine (Phila Pa 1976). (1990) 15(11):1110–3. doi: 10.1097/00007632-199011010-00005
46. Bauer HC, Wedin R. Survival after surgery for spinal and extremity metastases. Prognostication in 241 patients. Acta Orthop Scand. (1995) 66(2):143–6. doi: 10.3109/17453679508995508
47. Leithner A, Radl R, Gruber G, Hochegger M, Leithner K, Welkerling H, et al. Predictive value of seven preoperative prognostic scoring systems for spinal metastases. Eur Spine J. (2008) 17(11):1488–95. doi: 10.1007/s00586-008-0763-1
48. Zoccali C, Skoch J, Walter CM, Torabi M, Borgstrom M, Baaj AA. The Tokuhashi score: effectiveness and pitfalls. Eur Spine J. (2016) 25(3):673–8. doi: 10.1007/s00586-015-4339-6
49. Karhade AV, Thio Q, Ogink PT, Bono CM, Ferrone ML, Oh KS, et al. Predicting 90-day and 1-year mortality in spinal metastatic disease: development and internal validation. Neurosurgery. (2019) 85(4):E671–E81. doi: 10.1093/neuros/nyz070
50. Liu B, Saber A, Haisma HJ. CRISPR/Cas9: a powerful tool for identification of new targets for cancer treatment. Drug Discov Today. (2019) 24(4):955–70. doi: 10.1016/j.drudis.2019.02.011
51. Yuan M, Huang LL, Chen JH, Wu J, Xu Q. The emerging treatment landscape of targeted therapy in non-small-cell lung cancer. Signal Transduct Target Ther. (2019) 4:61. doi: 10.1038/s41392-019-0099-9
52. Majeed U, Manochakian R, Zhao Y, Lou Y. Targeted therapy in advanced non-small cell lung cancer: current advances and future trends. J Hematol Oncol. (2021) 14(1):108. doi: 10.1186/s13045-021-01121-2
53. Jager-Wittenaar H, Ottery FD. Assessing nutritional status in cancer: role of the patient-generated subjective global assessment. Curr Opin Clin Nutr Metab Care. (2017) 20(5):322–9. doi: 10.1097/MCO.0000000000000389
54. De Groot LM, Lee G, Ackerie A, van der Meij BS. Malnutrition screening and assessment in the cancer care ambulatory setting: mortality predictability and validity of the patient-generated subjective global assessment short form (PG-SGA SF) and the GLIM criteria. Nutrients. (2020) 12(8). doi: 10.3390/nu12082287
55. Bossi P, Delrio P, Mascheroni A, Zanetti M. The spectrum of malnutrition/cachexia/sarcopenia in oncology according to different cancer types and settings: a narrative review. Nutrients. (2021) 13(6). doi: 10.3390/nu13061980
56. Bourassa-Moreau E, Versteeg A, Moskven E, Charest-Morin R, Flexman A, Ailon T, et al. Sarcopenia, but not frailty, predicts early mortality and adverse events after emergent surgery for metastatic disease of the spine. Spine J. (2020) 20(1):22–31. doi: 10.1016/j.spinee.2019.08.012
57. Zakaria HM, Wilkinson BM, Pennington Z, Saadeh YS, Lau D, Chandra A, et al. Sarcopenia as a prognostic factor for 90-day and overall mortality in patients undergoing spine surgery for metastatic tumors: a multicenter retrospective cohort study. Neurosurgery. (2020) 87(5):1025–36. doi: 10.1093/neuros/nyaa245
58. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. (2009) 42(2):377–81. doi: 10.1016/j.jbi.2008.08.010
59. Bray F, Parkin DM. Evaluation of data quality in the cancer registry: principles and methods. Part I: comparability, validity and timeliness. Eur J Cancer. (2009) 45(5):747–55. doi: 10.1016/j.ejca.2008.11.032
60. Brewster D, Crichton J, Muir C. How accurate are Scottish cancer registration data? Br J Cancer. (1994) 70(5):954–9. doi: 10.1038/bjc.1994.428
61. Smith-Gagen J, Cress RD, Drake CM, Felter MC, Beaumont JJ. Factors associated with time to availability for cases reported to population-based cancer registries. Cancer Causes Control. (2005) 16(4):449–54. doi: 10.1007/s10552-004-5030-0
62. Choi D, Crockard A, Bunger C, Harms J, Kawahara N, Mazel C, et al. Review of metastatic spine tumour classification and indications for surgery: the consensus statement of the global spine tumour study group. Eur Spine J. (2010) 19(2):215–22. doi: 10.1007/s00586-009-1252-x
63. Dugger SA, Platt A, Goldstein DB. Drug development in the era of precision medicine. Nat Rev Drug Discov. (2018) 17(3):183–96. doi: 10.1038/nrd.2017.226
64. Groenendijk FH, Bernards R. Drug resistance to targeted therapies: deja vu all over again. Mol Oncol. (2014) 8(6):1067–83. doi: 10.1016/j.molonc.2014.05.004
65. Zachary I, Boren SA, Simoes E, Jackson-Thompson J, Davis JW, Hicks L. Information management in cancer registries: evaluating the needs for cancer data collection and cancer research. Online J Public Health Inform. (2015) 7(2):e213. doi: 10.5210/ojphi.v7i2.5664
66. Dreyer NA, Garner S. Registries for robust evidence. JAMA. (2009) 302(7):790–1. doi: 10.1001/jama.2009.1092
Keywords: cancer, spinal tumor, spinal metastatic disease, spine surgery, radiation oncology, registry, quality of life
Citation: Nevzati E, Poletti N, Spiessberger A, Bäbler S, Studer G, Riklin C, Diebold J, Chatain GP, Finn M, Witt J-P, Moser M and Mariani L (2023) Establishing the Swiss Spinal Tumor Registry (Swiss-STR): a prospective observation of surgical treatment patterns and long-term outcomes in patients with primary and metastatic spinal tumors. Front. Surg. 10:1222595. doi: 10.3389/fsurg.2023.1222595
Received: 14 May 2023; Accepted: 12 July 2023;
Published: 28 July 2023.
Edited by:
Alessandro Di Rienzo, Marche Polytechnic University, ItalyReviewed by:
Hassan Othman, University Hospitals Coventry and Warwickshire NHS Trust, United Kingdom© 2023 Nevzati, Poletti, Spiessberger, Bäbler, Studer, Riklin, Diebold, Chatain, Finn, Witt, Moser and Mariani. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Edin Nevzati ZWRpbi5uZXZ6YXRpQGx1a3MuY2g=
†These authors have contributed equally to this work
‡ORCID Edin Nevzati orcid.org/0000-0001-8943-0290
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.