 Christian Schäfer
Christian Schäfer- Department of Gastroenterology, Robert-Bosch-Hospital, Stuttgart, Germany
The treatment of leaks in the upper gastrointestinal tract has been revolutionized by the advent of covered self-expanding metal stents (cSEMS), endoscopic vacuum therapy (EVT), and recently, vacuum stent therapy (VST). In this retrospective study, we report the experiences with EVT and VST at our institution.
Patients and methods: Twenty-two patients (15 male, 7 female) with leaks in the esophagus, at the esophago-gastric junction or anastomotic leaks underwent EVT by placing a sponge connected to a negative pressure pump into or near the leak. VST was applied in three patients.
Results: EVT led to closure of the leak in 18 of 22 Patients (82%). In 9 patients (41%), EVT was followed by application of a cSEMS. One patient (5%) died during the hospital stay due to an aorto-esophageal fistula near the leak, four others (18%) due to underlying disease. The stricture rate was 3/22 (14%). All three patients in whom VST was applied had closure of the leak and recovered. Reviewing the literature, we identified sixteen retrospective series of ten or more patients (n = 610) with an overall closure rate for EVT of 84%. In eight additional retrospective observations, a comparison between the efficacy of EVT and cSEMS therapy was performed that revealed a success rate of 89% and 69%, respectively (difference not significant, chi-square test). For VST, two small series show that closure is possible in the majority of patients.
Conclusion: EVT and VST are valuable options in the treatment of leaks in the upper gastrointestinal tract.
Introduction
Prior to the introduction of vacuum sponge or stent therapy, perforations or leaks of the upper GI tract were associated with a high risk of mortality or morbidity and often required divertive surgery (1–3).
The majority of leaks occur after oncological resection of the esophago-gastric junction or esophagus. Less common are iatrogenic perforations (e.g., after forced insertion of gastric tubes, endoscopes or transesophageal echocardiography probes into a narrowed esophagus or esophageal diverticulum) or spontaneous tears, such as Boerhaave ruptures.
Small perforations may be handled by application of a row of several through-the-scope (TTS) clips. Over-the-scope clips (OTSC) might be effective for perforations ≤1 cm provided that the clip grasps not only the mucosa, but also the muscularis propria of two opposite edges of the leak.
Larger leaks in the tubular esophagus may be temporarily “sealed” by covered self-expanding metal stents (cSEMS) applied via upper GI endoscopy thus preventing bacteria from ingested food and saliva from migrating into the mediastinum. This method, which allows regular oral food intake, is optimal for perforations of the tubular part of a non-dilated, non-operated esophagus, whereas coverage of anastomotic leaks, e.g., after esophagectomy, may be insufficient due to the wider lumen of the adapted part of the stomach so that the cSEMS might lose contact to the wall.
Endoscopic vacuum sponge therapy (EVT) is another approach to treat leaks. Previously applied to rectal leaks, it has been adapted to the upper GI tract (4–6). A sponge positioned in the leakage cavity and connected to a negative-pressure pump allows continuous debridement and accelerates the granulation and closure of the wound. For smaller defects, it might be sufficient to place the sponge into the lumen next to the leak. The sponge needs to be exchanged 2–3 times per week. During vacuum sponge therapy, enteral feeding via a nasoduodenal tube is possible, whereas oral food intake is not.
A more recent approach is the insertion of a covered stent surrounded by a small layer of sponge material connected to a transnasal suction tube (vacuum stent therapy, VST) (7, 8). With this combination of cSEMS and EVT technology, patients may be allowed to eat.
Whereas a cSEMS is easy to place, the vacuum-based technologies, EVT and VST, require advanced endoscopic skills and are only successful in a setting of good interdisciplinary cooperation with surgical and ICU partners. In addition, nutritional and anti-infective therapy should be optimized, and last but not least, the patient should be willing to undergo serial endoscopies and to accept continuous transnasal suction, which may occasionally last for several weeks.
The following case series illustrates the efficacy and the restraints of vacuum sponge and vacuum stent therapy.
Methods
From our endoscopic records, we identified patients with leaks in the upper GI tract that were treated either with EVT or VST at the Robert-Bosch-Krankenhaus, Stuttgart, Germany, between 2010 and 2022.
Endoscopic vacuum therapy (EVT)
From 2010 to 2014, we used a self-made sponge device derived from the Endosponge® rectal vacuum therapy set (B. Braun, Melsungen, Germany). The cylindrical sponge that had been trimmed to the size of the leakage cavity was removed from the original suction tube, because the latter was too short for intraesophageal placement. The tip of a nasogastric tube that had been inserted transnasally and led out through the mouth was sutured into the sponge. The surgical thread at the distal end of the sponge was knotted several times and grasped outside the patient using a gastroscope armed with a forceps. Under endoscopic guidance the sponge was placed into the leakage cavity of the upper GI tract. After initiating suction via the tube [minus 125 mmHg, using an electric vacuum pump (4)], the gastroscope could be removed. The sponge was exchanged three times per week.
In recent years, a simplified system with a smaller sponge attached to an extra-long plastic tube (Esosponge®, B. Braun, Melsungen, Germany) was used that could be placed via an overtube. The gastroscope armed with the overtube was advanced into the leakage cavity. After withdrawal of the scope, the overtube was left with the tip in the leakage cavity. Using a pusher, the sponge was advanced to its final position. Once the overtube and the pusher had been removed, the suction tube was deviated transnasally and connected to the vacuum pump. Continuous suction was applied (minus 125 mmHg) and the position of the sponge was controlled by endoscopy. The sponge was renewed three times per week (i.e., maximum intervals of three days), since longer intervals led to increased clogging and ineffectivity of the vacuum sponge.
Vacuum stent therapy (VST)
The Vac-Stent® (Microtech, Düsseldorf, Germany) is a covered self-expanding stent (interior lumen diameter 12 mm) and surrounded by a 5 cm long vacuum sponge layer attached to a suction tube (7). The device can be introduced transorally like a standard metal stent. Subsequently, the suction tube needs to be redirected through the nose. Initial suction was applied at −125 mmHg, and then lowered to −75 mmHg. After 7 days, the stent was removed. If there was still a visible leak, the therapy was repeated.
Additional measures for patients undergoing EVT or VST
In most patients, pleural effusions were drained by thoracic tubes, since anastomotic or other leaks usually communicate with the thoracic cavities. If more than one thoracic tube was required, each tube was connected to an independent suction device to avoid inadequate drainage. If there were signs of infection, antibiotic therapy was initiated. Adequate nutrition was provided by enteral feeding via a nasoduodenal or nasogastric tube that was placed prior to EVT. Sometimes parenteral nutrition was applied. In VST peroral feeding was allowed.
Optimization of vacuum therapy: In standard EVT, excess luminal fluid resulting from saliva or regurgitation of gastric fluid may impede the efficacy of suction. In some patients with excess saliva production, a transdermal scopolamine patch was applied. If regurgitation of excessive gastric fluid was thought to impede the vacuum effect of the sponge, an additional Esosponge® that was connected to a separate vacuum pump was positioned in the stomach. In one case with additional sponge, the patient received a feeding jejunostomy to enable enteral feeding.
Statistics
For the evaluation of the retrospective studies comparing EVT vs. cSEMS, chi-square test was used.
Results
Endoscopic vacuum therapy
In the past 13 years, 22 patients, 15 male and 7 female, with a mean age of 67.8 years were treated with EVT. Four of these patients had been referred from other hospitals to our institution.
Most leaks were postsurgical (n = 14), occurring after resection of cancer of the tubular esophagus, the esophagogastric junction or the stomach, other patients (n = 4) developed leaks after endoscopic procedures, e.g., dilations, or forced placement of a nasogastric tube after hiatal hernia repair, or had a spontaneous rupture of the esophagus due to increased pressure (Boerhaave rupture) or inflammation (n = 4). In each individual patient, the decision to apply EVT was made jointly by the endoscopist (gastroenterologist) and the abdominal (or thoracic) surgeon.
In some patients, other leakage therapies had been tried without success, like the application of a large over-the-scope clip (OTSC, n = 3), placement of a covered self-expanding metal stent (cSEMS, n = 2) or surgical redo (n = 2). EVT usually started out with intracavitary sponge placement. Only two patients received intraluminal sponge therapy from the beginning because of a very small opening of the leak. The duration of EVT is reflected by the number of procedures ranging from 3 to 23 with a median number of 6 procedures. The majority of the patients (n = 18) received unilateral or bilateral thoracic drains to reduce pleural effusions.
Nine of 22 (41%) patients received a cSEMS as sequential therapy, for various reasons: In three patients, EVT failed, in one patient a stricture was opened by stent insertion, one patient had a bleeding aortoesophageal fistula. In the other four patients, cSEMS was used to cover minor residual blindly ending fistulae after successful EVT in order to reinstitute oral intake. In two patients (9%) additional surgery was necessary (surgical removal of solid food from the thoracic cavity).
Successful leakage closure—with or without sequential cSEMS—was achieved in 18 of 22 patients (82%).
In four patients (18%) the leakage could not be closed, i.e., we observed either no reduction in cavity size or fistula complications. One of these patients (aged 76 years, but without any additional risk factors) with a continuing anastomotic leak after 18 sponge placements received a cSEMS that allowed peroral nutrition and discharge from the hospital in a stable condition. The other three patients died within a short period (<2 months) after unsuccessful leakage treatment: One patient with an anastomotic leak developed fatal bleeding due to an aorto-esophageal fistula after five sponge placements that could not be stopped by cSEMS treatment. Two patients with persistent leaks had significant comorbidity that led to ventilatory and finally multiorgan failure (one patient with an anastomotic leak who had severe COPD and one patient with a spontaneous leak due to pleural empyema who had morbid obesity with a BMI > 40).
In addition to these three fatalities, two other patients died despite successful EVT due to septic port infection and progressive duodenal cancer, respectively.
Three patients (14%) developed a stenotic stricture that was successfully treated either with balloon dilation or, as mentioned above, placement of a removable cSEMS.
Vacuum stent therapy
VST was applied in three patients, one with a perforation due to transesophageal echocardiography, and two with postoperative anastomotic leaks. In two patients, EVT and/or cSEMS had been tried unsuccessfully beforehand. In these two patients, the duration of VST had to be extended to 2 weeks requiring an exchange of the vacuum stent after the first week. Closure was achieved in all three patients.
Discussion and review of the literature
The series presented in this paper confirms previous observations that EVT may substantially contribute to the healing of life-threatening leaks of the esophagus and the esophagogastric junction. Our findings are comparable to retrospective data from other groups.
EVT case series
Table 1 summarizes several publications of case series of 10 or more patients, in whom EVT was applied. As in our study, most of these patients were male and suffered from postoperative anastomotic leaks. In our and other series, closure rates around 80% were achieved. Not only by us, but also by half of the other groups, EVT was combined with sequential cSEMS placement.
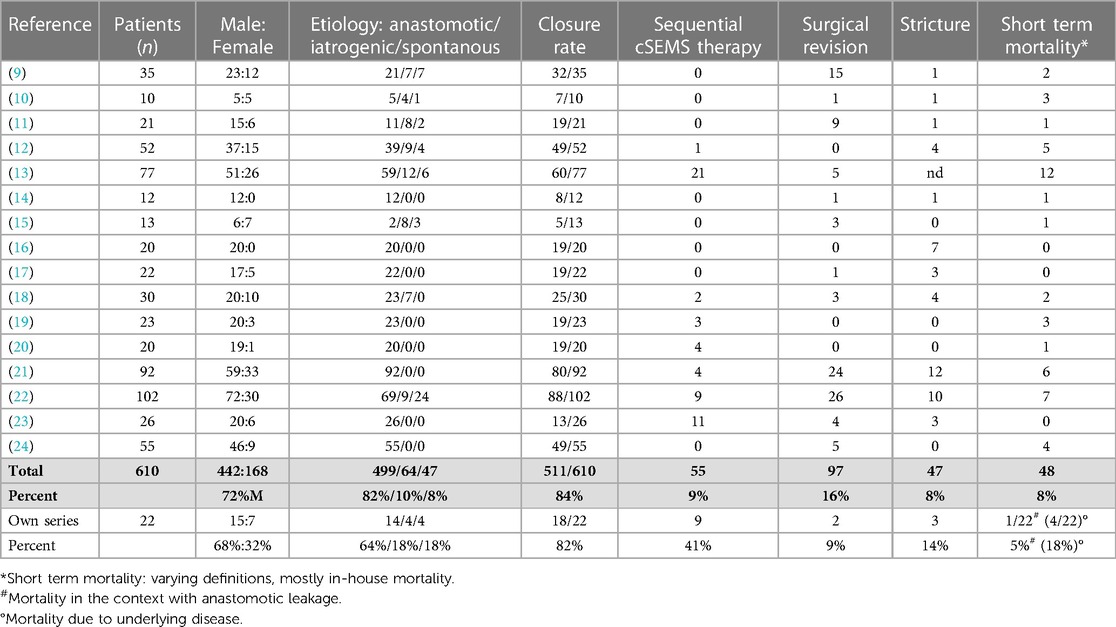
Table 1. EVT in patients with leaks in the upper gastrointestinal tract. Case series (≥ 10 patients).
Serious adverse events due to EVT were rarely reported by others. In our series, one patient developed an aorto-esophageal fistula with fatal bleeding that could not be stopped by cSEMS. In this case, non-adequate debridement or EVT itself might have contributed to the erosion of the aortic wall. Otherwise, the mortality rate in our series reflects demographic factors and severe comorbidities (old age, COPD, extreme obesity, progressive cancer).
A frequent chronic complication is the development of stenotic strictures. In our group, 3 out of 23 patients had to be treated by repeated balloon dilation or cSEMS insertion. This is comparable to the average stricture rate reported by others. Other complications, such as airway leaks, were not observed.
Early diagnosis of leaks and immediate action after the diagnosis may significantly improve the outcome of EVT and reduce in-hospital mortality. This is suggested by a retrospective study in 156 patients (not included in Table 1) with leaks of various etiologies comparing early experience with EVT with an optimized concept in recent years showing a significant reduction of the 30 day in-hospital mortality and improvement of leakage resolution (25). In the latter group the time gap between diagnosis of leakage and start of EVT had been significantly shortened compared to the early period (0.3 vs. 7.2 days).
Retrospective comparison EVT vs. cSEMS
Is EVT better than or equal to cSEMS therapy in patients with esophageal and esophagogastric leaks? So far, only retrospective comparisons are available, as listed in Table 2. Most of these evaluations dealt with patients who developed anastomotic leaks after resective surgery for malignant tumors of the esophago-gastric junction or the esophagus.
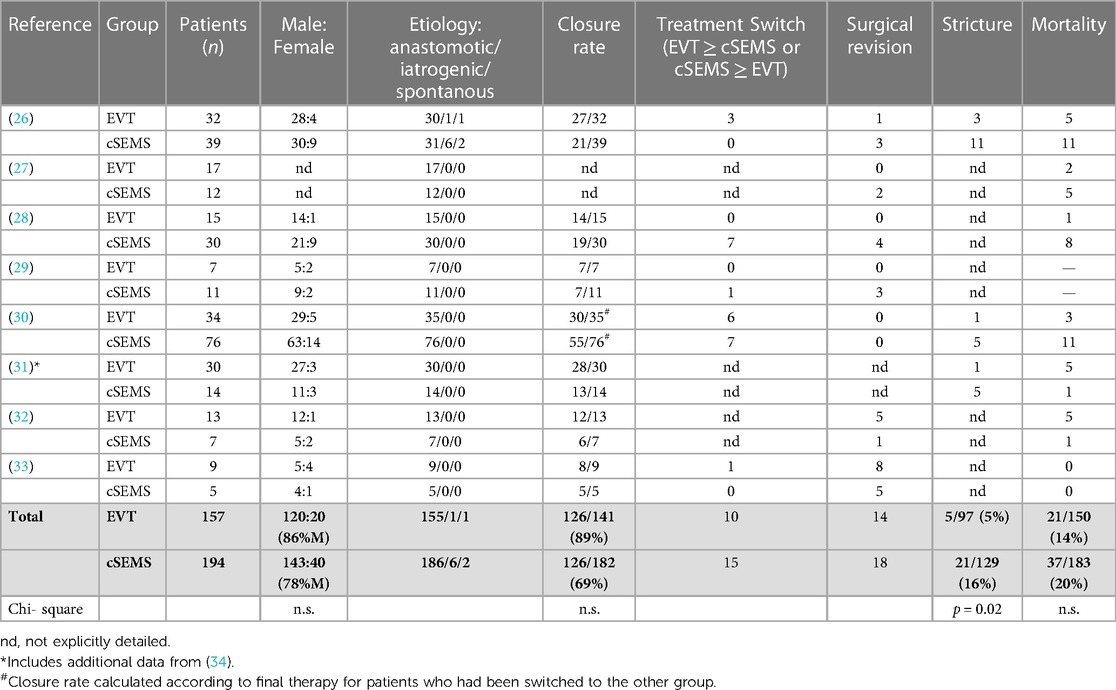
Table 2. Retrospective comparisons of cSEMS vs. EVT.
Despite the fact that each retrospective study used different criteria and definitions, it is obvious that EVT is at least non-inferior to cSEMS therapy, the reported numbers suggest even a slightly higher closure rate and a lower mortality rate, although this difference is not significant. The only significant difference was found for the stricture rate that was higher in the cSEMS group. A caveat for these retrospective studies is that patients of different eras may have been compared. For the future, sufficiently powered prospective randomized studies are needed that also allow subgroup analyses for different etiologies and locations of the leaks.
Experiences with VST
A recent development is the vacuum stent therapy (VST) combining cSEMS and vacuum sponge technology. In our hospital, the experience is limited, but all three patients who have been treated with this method had closure of their leak and recovered. Although the effective length of the sponge material around the shaft of the vacuum stent is relatively short (5 cm), lesions that were not too large could be effectively sealed.
In the pilot study reported by Lange et al. (7), three patients with different etiologies (anastomotic leak, Boerhaave tear, one patient with a migrated LINX anti-reflux device which had been removed surgically and left a postoperative transmural opening) showed that VST induced granulation and closure of the gap.
Another retrospective report on a series of 10 patients published by Chon et al. confirmed the effectiveness of VST (8). Out of ten patients (five with anastomotic insufficiencies, five of other origin incl. Boerhaave syndrome) seven were treated successfully by VST. In the remaining three patients with VST failure, two were switched to EVT and one had to undergo esophagectomy.
These two reports, along with our experience, show that VST is technically feasible and leads to closure of tears or leaks in the esophagus or at the esophageal junction in most, but not all patients. Possibly, technical improvements, e.g., longer stents, may be more effective in covering larger leaks.
In summary, the therapeutic strategies developed for leaks of the esophagus and the esophagogastric junction have dramatically improved the clinical outcome. However, the experience is based on retrospective non-randomized observations. Larger prospective randomized comparative trials are needed to determine the optimal strategy for leaks of different etiologies and locations.
Author contributions
Single author publication. More than 80% of the endoscopical procedures reported in the paper were performed by the author himself.
Acknowledgments
The author acknowledges the excellent technical assistance of the endoscopic staff at our hospital.
Conflict of interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Griffin SM, Lamb PJ, Dresner SM, Richardson DL, Hayes N. Diagnosis and management of a mediastinal leak following radical oesophagectomy. Br J Surg. (2001) 88(10):1346–51. doi: 10.1046/j.0007-1323.2001.01918.x
2. Crestanello JA, Deschamps C, Cassivi SD, Nichols FC, Allen MS, Schleck C, et al. Selective management of intrathoracic anastomotic leak after esophagectomy. J Thorac Cardiovasc Surg. (2005) 129(2):254–60. doi: 10.1016/j.jtcvs.2004.10.024
3. Page RD, Shackcloth MJ, Russell GN, Pennefather SH. Surgical treatment of anastomotic leaks after oesophagectomy. Eur J Cardiothorac Surg. (2005) 27(2):337–43. doi: 10.1016/j.ejcts.2004.10.053
4. Loske G, Schorsch T, Müller C. Endoscopic vacuum sponge therapy for esophageal defects. Surg Endosc. (2010) 24(10):2531–5. doi: 10.1007/s00464-010-0998-x
5. Kuehn F, Loske G, Schiffmann L, Gock M, Klar E. Endoscopic vacuum therapy for various defects of the upper gastrointestinal tract. Surg Endosc. (2017) 31(9):3449–58. doi: 10.1007/s00464-016-5404-x
6. Wedemeyer J, Schneider A, Manns MP, Jackobs S. Endoscopic vacuum-assisted closure of upper intestinal anastomotic leaks. Gastrointest Endosc. (2008) 67(4):708–11. doi: 10.1016/j.gie.2007.10.064
7. Lange J, Dormann A, Bulian DR, Hügle U, Eisenberger CF, Heiss MM. VACStent: combining the benefits of endoscopic vacuum therapy and covered stents for upper gastrointestinal tract leakage. Endosc Int Open. (2021) 9(6):E971–6. doi: 10.1055/a-1474-9932
8. Chon SH, Töx U, Lorenz F, Rieck I, Wagner BJ, Kleinert R, et al. A novel hybrid stent with endoscopic vacuum therapy for treating leaks of the upper gastrointestinal tract. Visc Med. (2021) 37(5):403–9. doi: 10.1159/000512320
9. Schorsch T, Müller C, Loske G. Endoskopische vakuumtherapie von perforationen und anastomoseninsuffizienzen des Ösophagus [endoscopic vacuum therapy of perforations and anastomotic insufficiency of the esophagus]. Chirurg. (2014) 85(12):1081–93. (in German). doi: 10.1007/s00104-014-2764-4
10. Möschler O, Nies C, Mueller MK. Endoscopic vacuum therapy for esophageal perforations and leakages. Endosc Int Open. (2015) 3(6):E554–8. doi: 10.1055/s-0034-1392568
11. Kuehn F, Schiffmann L, Janisch F, Schwandner F, Alsfasser G, Gock M, et al. Surgical endoscopic vacuum therapy for defects of the upper gastrointestinal tract. J Gastrointest Surg. (2016) 20(2):237–43. doi: 10.1007/s11605-015-3044-4
12. Laukoetter MG, Mennigen R, Neumann PA, Dhayat S, Horst G, Palmes D, et al. Successful closure of defects in the upper gastrointestinal tract by endoscopic vacuum therapy (EVT): a prospective cohort study. Surg Endosc. (2017) 31(6):2687–96. doi: 10.1007/s00464-016-5265-3
13. Bludau M, Fuchs HF, Herbold T, Maus MKH, Alakus H, Popp F, et al. Results of endoscopic vacuum-assisted closure device for treatment of upper GI leaks. Surg Endosc. (2018) 32(4):1906–14. doi: 10.1007/s00464-017-5883-4
14. Noh SM, Ahn JY, Lee JH, Jung HY, AlGhamdi Z, Kim HR, et al. Endoscopic vacuum-assisted closure therapy in patients with anastomotic leakage after esophagectomy: a single-center experience. Gastroenterol Res Pract. (2018) 2018:1697968. doi: 10.1155/2018/1697968
15. Still S, Mencio M, Ontiveros E, Burdick J, Leeds SG. Primary and rescue endoluminal vacuum therapy in the management of esophageal perforations and leaks. Ann Thorac Cardiovasc Surg. (2018) 24(4):173–9. doi: 10.5761/atcs.oa.17-00107
16. Min YW, Kim T, Lee H, Min BH, Kim HK, Choi YS, et al. Endoscopic vacuum therapy for postoperative esophageal leak. BMC Surg. (2019) 19(1):37. doi: 10.1186/s12893-019-0497-5
17. Jeon JH, Jang HJ, Han JE, Park YS, Seong YW, Cho S, et al. Endoscopic vacuum therapy in the management of postoperative leakage after esophagectomy. World J Surg. (2020) 44(1):179–85. doi: 10.1007/s00268-019-05228-z
18. Jung CFM, Müller-Dornieden A, Gaedcke J, Kunsch S, Gromski MA, Biggemann L, et al. Impact of endoscopic vacuum therapy with low negative pressure for esophageal perforations and postoperative anastomotic esophageal leaks. Digestion. (2021) 102(3):469–79. doi: 10.1159/000506101
19. Hayami M, Klevebro F, Tsekrekos A, Samola Winnberg J, Kamiya S, Rouvelas I, et al. Endoscopic vacuum therapy for anastomotic leak after esophagectomy: a single-center's early experience. Dis Esophagus. (2021) 34(9):doaa122. doi: 10.1093/dote/doaa122
20. Chon SH, Brunner S, Müller DT, Lorenz F, Stier R, Streller L, et al. Time to endoscopic vacuum therapy-lessons learned after > 150 robotic-assisted minimally invasive esophagectomies (RAMIE) at a German high-volume center. Surg Endosc. (2023) 37(1):741–8. doi: 10.1007/s00464-022-09754-1
21. Reimer S, Lock JF, Flemming S, Weich A, Widder A, Plaßmeier L, et al. Endoscopic management of large leakages after upper gastrointestinal surgery. Front Surg. (2022) 9:885244. doi: 10.3389/fsurg.2022.885244
22. Richter F, Hendricks A, Schniewind B, Hampe J, Heits N, von Schönfels W, et al. Eso-Sponge® for anastomotic leakage after oesophageal resection or perforation: outcomes from a national, prospective multicentre registry. BJS Open. (2022) 6(2):zrac030. doi: 10.1093/bjsopen/zrac030
23. Seika P, Biebl M, Raakow J, Berndt N, Feldbrügge L, Maurer MM, et al. The association between neoadjuvant radio-chemotherapy and prolonged healing of anastomotic leakage after esophageal resection treated with EndoVAC therapy. J Clin Med. (2022) 11(16):4773. doi: 10.3390/jcm11164773.36013012
24. Zhang CC, Liesenfeld L, Klotz R, Koschny R, Rupp C, Schmidt T, et al. Feasibility, effectiveness, and safety of endoscopic vacuum therapy for intrathoracic anastomotic leakage following transthoracic esophageal resection. BMC Gastroenterol. (2021) 21(1):72. doi: 10.1186/s12876-021-01651-6
25. Reimer S, Seyfried F, Flemming S, Brand M, Weich A, Widder A, et al. Evolution of endoscopic vacuum therapy for upper gastrointestinal leakage over a 10-year period: a quality improvement study. Surg Endosc. (2022) 36(12):9169–78. doi: 10.1007/s00464-022-09400-w
26. Brangewitz M, Voigtländer T, Helfritz FA, Lankisch TO, Winkler M, Klempnauer J, et al. Endoscopic closure of esophageal intrathoracic leaks: stent versus endoscopic vacuum-assisted closure, a retrospective analysis. Endoscopy. (2013) 45(6):433–8. doi: 10.1055/s-0032-1326435
27. Schniewind B, Schafmayer C, Voehrs G, Egberts J, von Schoenfels W, Rose T, et al. Endoscopic endoluminal vacuum therapy is superior to other regimens in managing anastomotic leakage after esophagectomy: a comparative retrospective study. Surg Endosc. (2013) 27(10):3883–90. doi: 10.1007/s00464-013-2998-0
28. Mennigen R, Harting C, Lindner K, Vowinkel T, Rijcken E, Palmes D, et al. Comparison of endoscopic vacuum therapy versus stent for anastomotic leak after esophagectomy. J Gastrointest Surg. (2015) 19(7):1229–35. doi: 10.1007/s11605-015-2847-7
29. Hwang JJ, Jeong YS, Park YS, Yoon H, Shin CM, Kim N, et al. Comparison of endoscopic vacuum therapy and endoscopic stent implantation with self-expandable metal stent in treating postsurgical gastroesophageal leakage. Medicine. (2016) 95(16):e3416. doi: 10.1097/MD.0000000000003416
30. Berlth F, Bludau M, Plum PS, Herbold T, Christ H, Alakus H, et al. Self-expanding metal stents versus endoscopic vacuum therapy in anastomotic leak treatment after oncologic gastroesophageal surgery. J Gastrointest Surg. (2019) 23(1):67–75. doi: 10.1007/s11605-018-4000-x
31. Eichelmann AK, Ismail S, Merten J, Slepecka P, Palmes D, Laukötter MG, et al. Economic burden of endoscopic vacuum therapy compared to alternative therapy methods in patients with anastomotic leakage after esophagectomy. J Gastrointest Surg. (2021) 25(10):2447–54. doi: 10.1007/s11605-021-04955-w
32. El-Sourani N, Miftode S, Bockhorn M, Arlt A, Meinhardt C. Endoscopic management of anastomotic leakage after esophageal surgery: ten year analysis in a tertiary university center. Clin Endosc. (2022) 55(1):58–66. doi: 10.5946/ce.2021.099
33. Senne M, Werner CR, Schempf U, Thiel K, Königsrainer A, Wichmann D. Comparison of two endoscopic therapeutic interventions as primary treatment for anastomotic leakages after total gastrectomy. Cancers. (2022) 14(12):2982. doi: 10.3390/cancers14122982
34. Scognamiglio P, Reeh M, Melling N, Kantowski M, Eichelmann AK, Chon SH, et al. Management of intra-thoracic anastomotic leakages after esophagectomy: updated systematic review and meta-analysis of endoscopic vacuum therapy versus stenting. BMC Surg. (2022) 22(1):309. doi: 10.1186/s12893-022-01764-z
Keywords: endoscopic vacuum therapy (EVT), cSEMS, esophageal leak, anastomotic leak (AL), OTSC (over-the-scope clip), esophageal stricture
Citation: Schäfer C (2023) Don't be afraid of black holes: Vacuum sponge and vacuum stent treatment of leaks in the upper GI tract—a case series and mini-review. Front. Surg. 10:1168541. doi: 10.3389/fsurg.2023.1168541
Received: 17 February 2023; Accepted: 4 April 2023;
Published: 3 May 2023.
Edited by:
Christian Gutschow, University Hospital Zürich, SwitzerlandReviewed by:
Wietse Eshuis, Amsterdam University Medical Center, Netherlands© 2023 Schäfer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christian Schäfer Q2hyaXN0aWFuLnNjaGFlZmVyQHJiay5kZQ==