 Xiangming Che1
Xiangming Che1 Tianzuo Li2*
Tianzuo Li2*
- 1Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing, China
- 2Beijing Shijitan Hospital, Capital Medical University, Beijing, China
Objective: To explore the influences of total intravenous anesthesia (TIVA) and inhaled-intravenous anesthesia on the prognosis of patients with lung, breast, or esophageal cancer.
Methods: In this retrospective cohort study, patients with lung, breast, or esophageal cancer who underwent surgical treatments at Beijing Shijitan Hospital between January 2010 and December 2019 were included. The patients were categorized into the TIVA group and inhaled-intravenous anesthesia group, according to the anesthesia methods used for the patients for surgery of the primary cancer. The primary outcome of this study included overall survival (OS) and recurrence/metastasis.
Results: Totally, 336 patients were included in this study, 119 in the TIVA group and 217 in the inhaled-intravenous anesthesia group. The OS of patients in the TIVA group was higher than in the inhaled-intravenous anesthesia group (P = 0.042). There were no significant differences in the recurrence/metastasis-free survival between the two groups (P = 0.296). Inhaled-intravenous anesthesia (HR = 1.88, 95%CI: 1.15–3.07, P = 0.012), stage III cancer (HR = 5.88, 95%CI: 2.57–13.43, P < 0.001), and stage IV cancer (HR = 22.60, 95%CI: 8.97–56.95, P < 0.001) were independently associated with recurrence/ metastasis. Comorbidities (HR = 1.75, 95%CI: 1.05–2.92, P = 0.033), the use of ephedrine, noradrenaline or phenylephrine during surgery (HR = 2.12, 95%CI: 1.11–4.06, P = 0.024), stage II cancer (HR = 3.24, 95%CI: 1.08–9.68, P = 0.035), stage III cancer (HR = 7.60, 95%CI: 2.64–21.86, P < 0.001), and stage IV cancer (HR = 26.61, 95%CI: 8.57–82.64, P < 0.001) were independently associated with OS.
Conclusion: In patients with breast, lung, or esophageal cancer, TIVA is preferable than inhaled-intravenous anesthesia group for longer OS,, but TIVA was not associated with the recurrence/metastasis-free survival of patients.
Background
Surgery is the backbone and the only potentially curative treatment for solid tumors like breast cancer (1), lung cancer (2), and esophageal cancer (3). Surgery also allows precise tumor staging in terms of tumor size and lymph node involvement (1–3). Surgery necessarily involves anesthesia to render the patients unconscious, blocking pain feeling, and controlling autonomic reflexes (4). Surgical stress causes transient immunosuppression through the release of hormonal mediators such as catecholamines, prostaglandins, and growth factors (5), and prostaglandins and catecholamines can activate receptors involved in the metastatic ability of cancer cells, including B2-adrenergic (6) and cyclooxygenase-2 (7) receptors. In addition, inflammation associated with surgical trauma causes the release of cytokines that can inhibit the natural killer (NK) cells (8), which are essential in the perioperative phase as they are responsible for detecting and destroying circulating tumor cells (9). Furthermore, general anesthesia involves a large number and wide variety of drugs (4), each with possible effects on cancer cells and, subsequently, on patient prognosis (10).
In vitro and in vivo studies suggested that volatile inhaled anesthetics could enhance the metastatic ability of cancer cells (11–14), but the exact molecular mechanisms remain incompletely understood. Still, isoflurane, sevoflurane, desflurane, and halothane produce an inflammatory reaction in humans (15). In addition, volatile anesthetics can upregulate the hypoxia-inducible factor 1α (HIF1α), which confers protective effects on cancer cells (9, 16), and the vascular endothelial growth factor, which can stimulate the growth of cancer cells and neovascularization (11). On the other hand, sevoflurane appears to increase cisplatin sensitivity in lung cancer cells (17). Regarding intravenous agents, propofol is the most commonly used induction and maintenance drug (18). Propofol could have antitumor effects through its anti-inflammatory and antioxidative effects (19–24). Ketamine appears to induce tumor growth by inhibiting NK cells (25, 26). The global evidence about opioids is conflicting among studies and opioids. Some but not all opioids can inhibit NK cells, inhibit the immune system, and accelerate cancer progression (27, 28).
A meta-analysis in 2019 of six studies (>7,800 patients) showed that total intravenous anesthesia (TIVA) was associated with better recurrence-free survival (RFS) compared with volatile anesthetics in breast, esophageal, and lung cancers (29), but there was substantial heterogeneity among the included studies in terms of types of cancer, types of surgery, and patient characteristics. A retrospective study in Northern Europe showed an increased risk of recurrence with volatile anesthetics compared with TIVA in patients with colorectal cancer but without differences in overall survival (OS) (30). Therefore, data is still limited. Therefore, this study aimed to explore the influences of TIVA and inhaled-intravenous anesthesia on the prognosis of patients with lung, breast, or esophageal cancer. The results could hint toward the best anesthesia regimen to improve cancer outcomes.
Methods
Study design and patients
In this retrospective cohort study, patients with lung, breast, or esophageal cancer who underwent surgical treatments at Beijing Shijitan Hospital between January 2010 and December 2019 were included. The study was approved by the ethics committee of Beijing Shijitan Hospital. The requirement for informed consent was waived because of the retrospective nature of the study.
The inclusion criteria were (1) proven with lung, breast, or esophageal cancer by postoperative pathological examinations, (2) American Society of Anesthesiologists (ASA) grade I-III, and (3) complete data. The exclusion criteria were (1) underwent preoperative radiotherapy or chemotherapy, (2) underwent emergent surgeries, or 3) underwent secondary surgeries.
The patients were categorized into the TIVA group and inhaled-intravenous anesthesia group, according to the anesthesia methods used for the patients for surgery of the primary cancer.
Outcomes and data collection
The primary outcome of this study included overall survival (OS), recurrence/ metastasis. OS was the time from treatment to death from any cause. Recurrence referred to the re-appearance of the tumor at the original site. Metastasis referred to the re-appearance of tumors at distant sites.
The baseline characteristics of the patients were collected from the patient charts, including age, sex, body mass index (BMI), tumor stage and type, anesthesia method and drugs, comorbidities, and drug therapy.
Statistical analysis
SPSS 20.0 (IBM, Armonk, NY, USA) was used for statistical analysis. The Kolmogorov-Smirnov test was used for the normality test of the continuous data. Continuous data with a normal distribution were described as means and standard deviations and compared using the independent t-test. Continuous data not with a normal distribution were described as medians (P25, P75) and compared using the Mann-Whitney rank-sum test. Qualitative data were compared using the chi-square (χ2) test. The Cox proportional hazard model was used for multivariable analysis. The Kaplan-Meier survival analysis was used to compare OS and recurrence/metastasis between the two groups, and the log-rank test was used to compare the two groups. All statistical analyses were two-sided, and a two-sided P < 0.05 was considered statistically significant.
Results
Characteristics of the patients
Finally, 336 patients were included in this study, 119 in the TIVA group and 217 in the inhaled-intravenous anesthesia group. The characteristics of the patients are shown in Table 1. Compared with the inhaled-intravenous group, the TIVA group showed a lower proportion of males (42.0% vs. 58.5%, P = 0.004) and a higher frequency of comorbidities (42.0% vs. 26.3%, P = 0.003). Moreover, the tumor types of the two groups were statistically different (P < 0.001). There were no differences in the other patient characteristics.
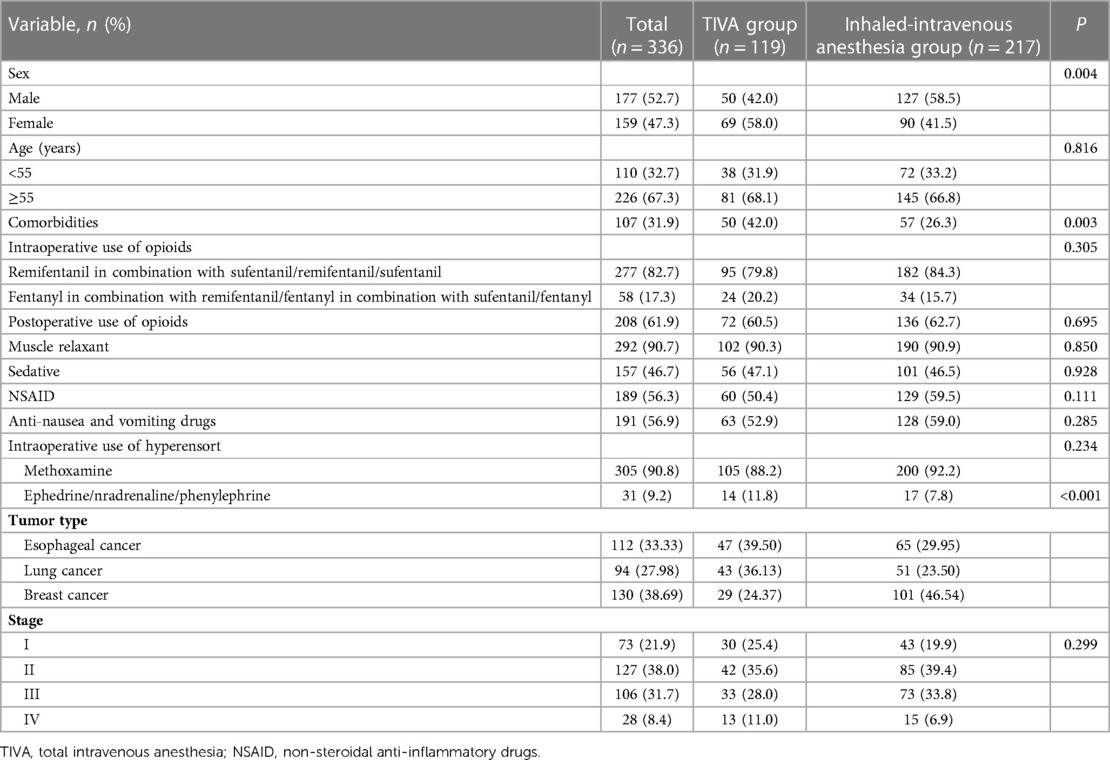
Table 1. Baseline characteristics of the patients.
Survival
The OS of patients in the TIVA group was higher than in the inhaled-intravenous anesthesia group (P = 0.042) (Figure 1A). There were no significant differences in the recurrence/metastasis-free survival between the two groups (P = 0.296) (Figure 1B).
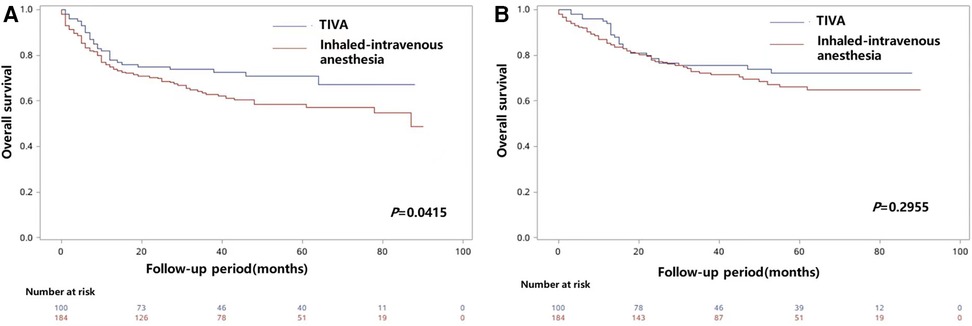
Figure 1. K-M curves of the overall survival (OS) (A) and recurrence/metastasis-free survival (B) of patients underwent different anesthesia methods.
Factors associated with recurrence/metastasis
The factors influencing recurrence/metastasis are shown in Table 2. Inhaled-intravenous anesthesia (HR = 1.88, 95%CI: 1.15–3.07, P = 0.012), stage III cancer (HR = 5.88, 95%CI: 2.57–13.43, P < 0.001), and stage IV cancer (HR = 22.60, 95%CI: 8.97–56.95, P < 0.001) were independently associated with recurrence/metastasis. The factors influencing OS are shown in Table 3. Comorbidities (HR = 1.75, 95%CI: 1.05–2.92, P = 0.033), the use of ephedrine, noradrenaline or phenylephrine during surgery (HR = 2.12, 95%CI: 1.11–4.06, P = 0.024), stage II cancer (HR = 3.24, 95%CI: 1.08–9.68, P = 0.035), stage III cancer (HR = 7.60, 95%CI: 2.64–21.86, P < 0.001), and stage IV cancer (HR = 26.61, 95%CI: 8.57–82.64, P < 0.001) were independently associated with OS.
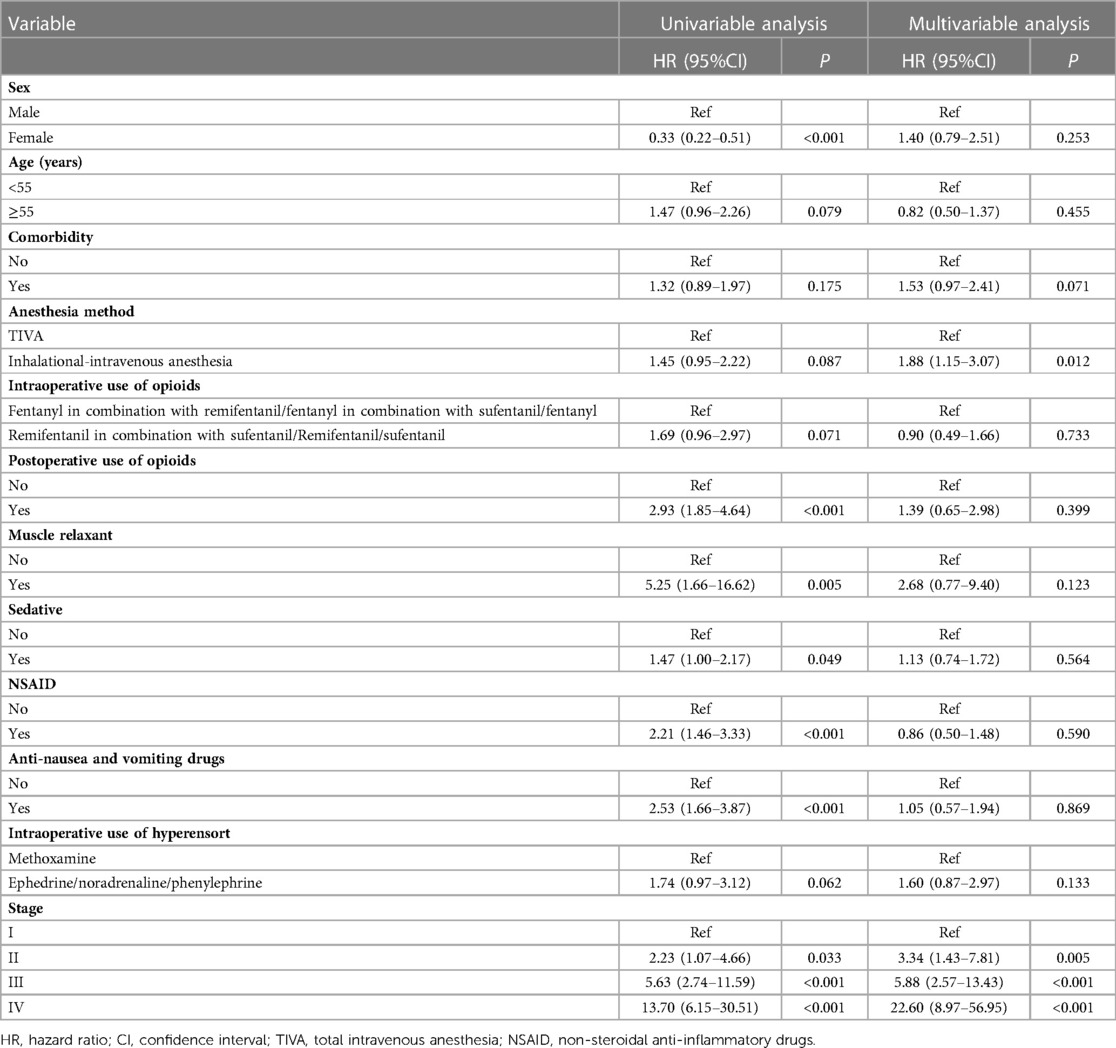
Table 2. Influencing factors of recurrence/metastasis of patients.
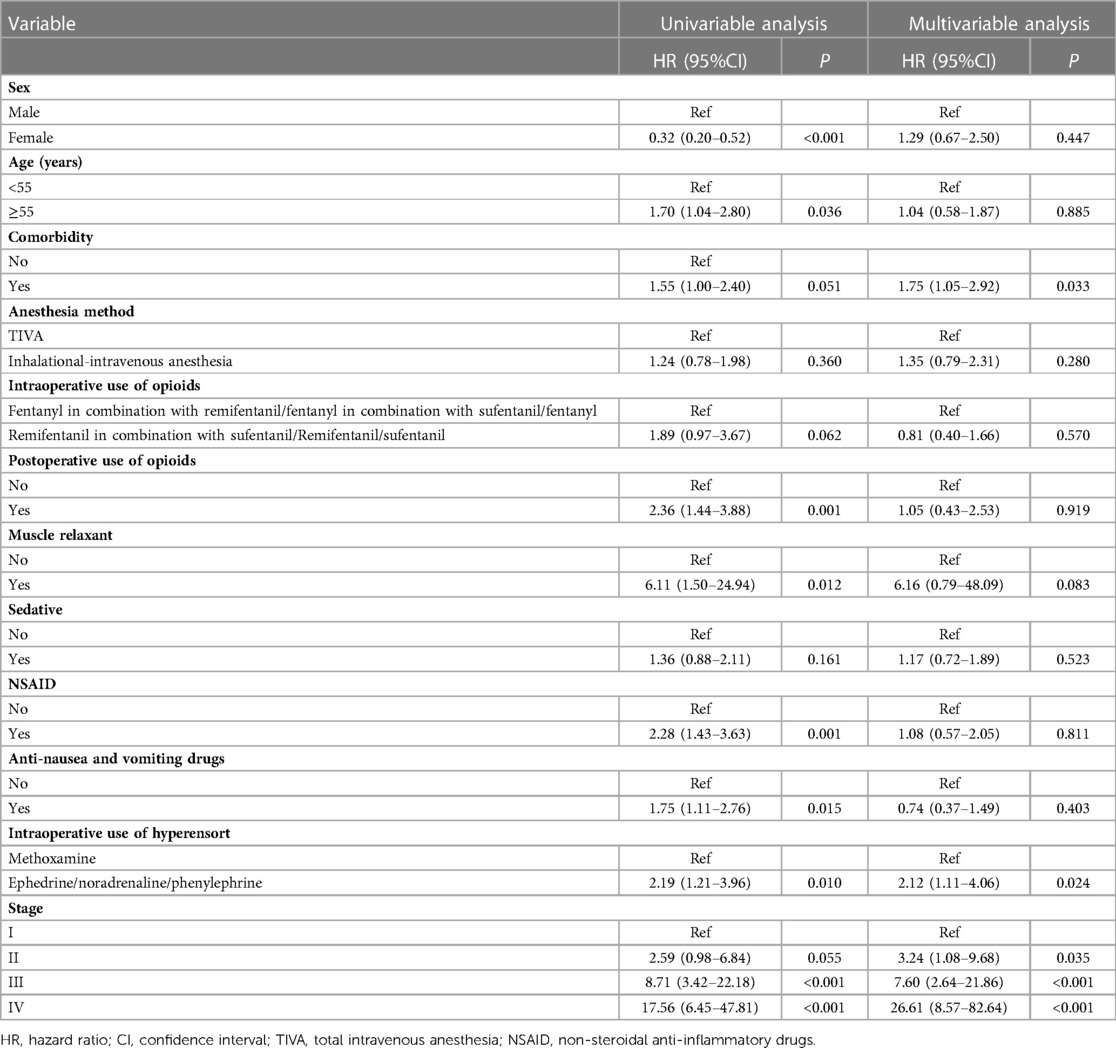
Table 3. Prognostic analysis of the survival of patients.
Discussion
The results suggest that i in patients with breast, lung, or esophageal cancer, TIVA is preferable than inhaled-intravenous anesthesia group for longer OS, but TIVA was not associated the recurrence/metastasis-free survival of patients.In addition, the use of ephedrine, noradrenaline, or phenylephrine during surgery was independently associated with OS.
Surgery and the associated trauma and metabolic stress are well-known to be associated with changes which may causean increased risk of enhancing the metastatic abilities of cancer cells (5–7). The ensuing inflammation will decrease the activity of NK cells (8), leading to a decreased ability to destroy the tumor cells that might be released while manipulating the tumor during resection (9). Hence, intraoperative strategies that could increase the likelihood of the circulating tumor cells being destroyed are clinically relevant.
The tumor has to be resected, and its manipulation is inevitable. Whether cancer cells will detach during resection depends on factors like tumor stage, stage, histological grade, and histological subtype (31, 32). Besides the surgeon's experience in oncological surgery, these factors are mostly non-modifiable. On the other hand, a large number and wide variety of drugs are available for general anesthesia (4), each with possible effects on cancer cells, and it is possible to select the anesthetics to optimize the risk of metastatic spread (10).
Although the exact mechanisms remain mostly unknown, preclinical studies have already demonstrated that inhaled anesthetics enhance the metastatic ability of cancer cells (11–14). This effect could be mediated, at least in part, by inflammation induced by these agents (15), as well as by an upregulation of HIF1α that triggers a wide variety of resistance and survival mechanisms in cancer cells (9, 11, 16). Nevertheless, inhaled anesthetics can have other effects on specific cancer. For instance, sevoflurane increases cisplatin sensitivity in lung cancer cells but induces cisplatin resistance in renal cancer (17). The present study was limited to three types of cancer, and the variety of chemotherapeutic drugs used in these patients precluded any subgroup analyses. Nevertheless, all patients received the optimal adjuvant treatments according to the available guidelines (1–3), and it can be assumed that each patient achieved the best outcomes possible.
Regarding intravenous agents, propofol could have antitumor effects through its anti-inflammatory and antioxidative effects (19–24), but ketamine appears to induce tumor growth by inhibiting NK cells (25, 26). Opioids seem to have various effects on cancer cells that depend upon the type of opioids in specific cancer types (27, 28). In the present study, remifentanil was not associated with OS or recurrence/metastasis compared with fentanyl.
The present study showed that TIVA was associated with a better prognosis than inhaled-intravenous anesthesia in patients with breast, lung, or esophageal cancer. It is supported by a recent meta-analysis of six studies involving >7,800 patients with breast, esophageal, and lung cancers, with better RFS with TIVA than with inhaled anesthesia (29). Of note, the previous meta-analysis involved substantial heterogeneity in its analyses, and the results must be taken cautiously and confirmed. A retrospective study in Northern Europe showed an increased risk of recurrence with volatile anesthetics compared with TIVA in patients with colorectal cancer but without differences in overall survival (OS) (30). In this study, similarly, we found that inhaled-intravenous anesthesia was independently associated with recurrence/metastasis, which was consistent with the retrospective study in Northern Europe. We believe the reason why conclusion of this present study was different from previous researches could possibly be that the patients were from a single center and the resulting sample size was small, which needs to be improved in future study. Large studies on breast, gastric, liver, colon, and rectal cancers have indicated increased mortality in cancer patients undergoing inhalation anesthesia (33–37). The lack of association between anesthesia type and OS could be attributed by postoperative complications like wound complications, pulmonary infections, and anastomotic leaks (38, 39), as well as short and long-term complications associated with adjuvant treatments (40, 41). The results could also be influenced by relativelyshort follow-ups, preventing the observation of long-term events. In addition, older patients with comorbidities have a risk of dying from causes other than cancer (42, 43). Retrospective studies of patients with esophageal cancer showed increased mortality with inhaled anesthesia but fewer myocardial infarctions, which could influence OS (37, 44, 45). Hence, the lack of association between inhaled anesthesia and OS could be due to a decrease in other postoperative events such as myocardial infarctions. It was worth noting that in the past before BIS monitoring was popular, more short-term surgeries were done using TIVA. BIS had been used to monitor the depth of anesthesia since 2010 in this study center; unfortunately, relevant data were not collected during this study. However, we found that there was no significant difference in tumor stage between the two groups, which means that the complexity of surgery was equal for both groups.
The use of ephedrine, noradrenaline, or phenylephrine during surgery was associated with increased mortality in patients with gastric cancer (46). In the present study, the use of ephedrine, noradrenaline, or phenylephrine during surgery was independently associated with OS. This association is probably associated with greater hemodynamic instability in the patients, but this parameter was difficult to assess from the patient charts.
Previous data analysis has found that differences in anesthesia type do exist, such differences as recurrence and metastasis outcomes and OS among different tumor type distribution. Therefore, variable of tumor type was included in the multivariate regression in the prognostic analysis. And the results showed that after tumor type and other factors were adjusted, the risk of recurrence and metastasis was increased in the intravenous-inhalational anesthesia group compared with the intravenous anesthesia group (OR = 1.88, 95%CI: 1.15–3.07).
In the present study, the tumor stage was the strongest factor associated with recurrence/metastasis and OS. These results go with common sense since the tumor stage is an important prognostic factor for patients with cancer and is among the most widely used prognosis system (1–3). Nevertheless, the results suggest that inhaled-intravenous anesthesia is a risk factor for OS that is independent of the tumor stage.
This study has limitations. It was a retrospective study limited to the data available in the patient charts, and it has the inherent selection bias of retrospective study. The patients were from a single center, and the resulting sample size was small. Additional prospective, multicenter, randomized controlled trials with larger sample sizes are needed to provide high-grade evidence.
In conclusion, the results suggest that in patients with breast, lung, or esophageal cancer, TIVA is associated with relatively higher OS than inhaled-intravenous anesthesia, while we did not find the association between TIVA and the recurrence/metastasis-free survival of patients. The use of ephedrine, noradrenaline, or phenylephrine during surgery was independently associated with OS.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Ethics statement
The studies involving human participants were reviewed and approved by The study was approved by the ethics committee of Beijing Shijitan Hospital. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
CX and LT: carried out the studies, participated in collecting data, and drafted the manuscript. CX and LT: performed the statistical analysis and participated in its design. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. (2022) NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines). Breast Cancer. Version 4.2022. Fort Washington: National Comprehensive Cancer Network.
2. (2022) NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines). Non-Small Cell Lung Cancer. Version 3.2022. Fort Washington: National Comprehensive Cancer Network.
3. (2022) NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines). Esophageal and Esophagogastric Junction Cancers. Version 3.2022. Fort Washington: National Comprehensive Cancer Network.
4. Smith G, D’Cruz JR, Rondeau B, Goldman J. General anesthesia for surgeons. Treasure island (FL): StatPearls (2022).
5. Alazawi W, Pirmadjid N, Lahiri R, Bhattacharya S. Inflammatory and immune responses to surgery and their clinical impact. Ann Surg. (2016) 264:73–80. doi: 10.1097/SLA.0000000000001691
6. Perez-Sayans M, Somoza-Martin JM, Barros-Angueira F, Diz PG, Gandara Rey JM, García-García A. Beta-adrenergic receptors in cancer: therapeutic implications. Oncol Res. (2010) 19:45–54. doi: 10.3727/096504010X12828372551867
7. Wu WK, Sung JJ, Lee CW, Yu J, Cho CH. Cyclooxygenase-2 in tumorigenesis of gastrointestinal cancers: an update on the molecular mechanisms. Cancer Lett. (2010) 295:7–16. doi: 10.1016/j.canlet.2010.03.015
8. Angka L, Khan ST, Kilgour MK, Xu R, Kennedy MA, Auer RC. Dysfunctional natural killer cells in the aftermath of cancer surgery. Int J Mol Sci. (2017) 18:1787–808. doi: 10.3390/ijms18081787
9. Tavare AN, Perry NJ, Benzonana LL, Takata M, Ma D. Cancer recurrence after surgery: direct and indirect effects of anesthetic agents. Int J Cancer. (2012) 130:1237–50. doi: 10.1002/ijc.26448
10. Montejano J, Jevtovic-Todorovic V. Anesthesia and cancer, friend or foe? A narrative review. Front Oncol. (2021) 11:803266. doi: 10.3389/fonc.2021.803266
11. Benzonana LL, Perry NJ, Watts HR, Yang B, Perry IA, Coombes C, et al. Isoflurane, a commonly used volatile anesthetic, enhances renal cancer growth and malignant potential via the hypoxia-inducible factor cellular signaling pathway in vitro. Anesthesiology. (2013) 119:593–605. doi: 10.1097/ALN.0b013e31829e47fd
12. Buckley A, McQuaid S, Johnson P, Buggy DJ. Effect of anaesthetic technique on the natural killer cell anti-tumour activity of serum from women undergoing breast cancer surgery: a pilot study. Br J Anaesth. (2014) 113(Suppl 1):i56–62. doi: 10.1093/bja/aeu200
13. Desmond F, McCormack J, Mulligan N, Stokes M, Buggy DJ. Effect of anaesthetic technique on immune cell infiltration in breast cancer: a follow-up pilot analysis of a prospective, randomised, investigator-masked study. Anticancer Res. (2015) 35:1311–9. PMID: 25750280
14. Ecimovic P, McHugh B, Murray D, Doran P, Buggy DJ. Effects of sevoflurane on breast cancer cell function in vitro. Anticancer Res. (2013) 33:4255–60. doi: 10.1097/COC.0b013e31821dee4e
15. Kurosawa S, Kato M. Anesthetics, immune cells, and immune responses. J Anesth. (2008) 22:263–77. doi: 10.1007/s00540-008-0626-2
16. Huang H, Benzonana LL, Zhao H, Watts HR, Perry NJ, Bevan C, et al. Prostate cancer cell malignancy via modulation of HIF-1alpha pathway with isoflurane and propofol alone and in combination. Br J Cancer. (2014) 111:1338–49. doi: 10.1038/bjc.2014.426
17. Ciechanowicz S, Zhao H, Chen Q, Cui J, Mi E, Lian Q, et al. Differential effects of sevoflurane on the metastatic potential and chemosensitivity of non-small-cell lung adenocarcinoma and renal cell carcinoma in vitro. Br J Anaesth. (2018) 120:368–75. doi: 10.1016/j.bja.2017.11.066
19. Kim R. Anesthetic technique and cancer recurrence in oncologic surgery: unraveling the puzzle. Cancer Metastasis Rev. (2017) 36:159–77. doi: 10.1007/s10555-016-9647-8
20. Jaura AI, Flood G, Gallagher HC, Buggy DJ. Differential effects of serum from patients administered distinct anaesthetic techniques on apoptosis in breast cancer cells in vitro: a pilot study. Br J Anaesth. (2014) 113(Suppl 1):i63–67. doi: 10.1093/bja/aet581
21. Chen Y, Liang M, Zhu Y, Zhou D. The effect of propofol and sevoflurane on the perioperative immunity in patients under laparoscopic radical resection of colorectal cancer. Zhonghua Yi Xue Za Zhi. (2015) 95:3440–4.26813135
22. Baki ED, Aldemir M, Kokulu S, Koca HB, Ela Y, Sıvacı RG, et al. Comparison of the effects of desflurane and propofol anesthesia on the inflammatory response and s100beta protein during coronary artery bypass grafting. Inflammation. (2013) 36:1327–33. doi: 10.1007/s10753-013-9671-6
23. Liu S, Gu X, Zhu L, Wu G, Zhou H, Song Y, et al. Effects of propofol and sevoflurane on perioperative immune response in patients undergoing laparoscopic radical hysterectomy for cervical cancer. Medicine. (2016) 95:e5479. doi: 10.1097/MD.0000000000005479
24. Liu TC. Influence of propofol, isoflurane and enflurance on levels of serum interleukin-8 and interleukin-10 in cancer patients. Asian Pac J Cancer Prev. (2014) 15:6703–7. doi: 10.7314/APJCP.2014.15.16.6703
25. Melamed R, Bar-Yosef S, Shakhar G, Shakhar K, Ben-Eliyahu S. Suppression of natural killer cell activity and promotion of tumor metastasis by ketamine, thiopental, and halothane, but not by propofol: mediating mechanisms and prophylactic measures. Anesth Analg. (2003) 97:1331–9. doi: 10.1213/01.ANE.0000082995.44040.07
26. He H, Chen J, Xie WP, Cao S, Hu HY, Yang LQ, et al. Ketamine used as an acesodyne in human breast cancer therapy causes an undesirable side effect, upregulating anti-apoptosis protein Bcl-2 expression. Genet Mol Res. (2013) 12:1907–15. doi: 10.4238/2013.January.4.7
27. Boland JW, Pockley AG. Influence of opioids on immune function in patients with cancer pain: from bench to bedside. Br J Pharmacol. (2018) 175:2726–36. doi: 10.1111/bph.13903
28. Nguyen J, Luk K, Vang D, Soto W, Vincent L, Robiner S, et al. Morphine stimulates cancer progression and mast cell activation and impairs survival in transgenic mice with breast cancer. Br J Anaesth. (2014) 113(Suppl 1):i4–13. doi: 10.1093/bja/aeu090
29. Yap A, Lopez-Olivo MA, Dubowitz J, Hiller J, Riedel B, Wigmore T, et al. Anesthetic technique and cancer outcomes: a meta-analysis of total intravenous versus volatile anesthesia. Can J Anaesth. (2019) 66:546–61. doi: 10.1007/s12630-019-01330-x
30. Hasselager RP, Hallas J, Gogenur I. Inhalation or total intravenous anaesthesia and recurrence after colorectal cancer surgery: a propensity score matched danish registry-based study. Br J Anaesth. (2021) 126:921–30. doi: 10.1016/j.bja.2020.11.019
31. Tohme S, Simmons RL, Tsung A. Surgery for cancer: a trigger for metastases. Cancer Res. (2017) 77:1548–52. doi: 10.1158/0008-5472.CAN-16-1536
32. Alieva M, van Rheenen J, Broekman MLD. Potential impact of invasive surgical procedures on primary tumor growth and metastasis. Clin Exp Metastasis. (2018) 35:319–31. doi: 10.1007/s10585-018-9896-8
33. Wu ZF, Lee MS, Wong CS, Lu CH, Huang YS, Lin KT, et al. Propofol-based total intravenous anesthesia is associated with better survival than desflurane anesthesia in colon cancer surgery. Anesthesiology. (2018) 129:932–41. doi: 10.1097/ALN.0000000000002357
34. Enlund M, Berglund A, Andreasson K, Cicek C, Enlund A, Bergkvist L. The choice of anaesthetic–sevoflurane or propofol–and outcome from cancer surgery: a retrospective analysis. Ups J Med Sci. (2014) 119:251–61. doi: 10.3109/03009734.2014.922649
35. Zheng X, Wang Y, Dong L, Zhao S, Wang L, Chen H, et al. Effects of propofol-based total intravenous anesthesia on gastric cancer: a retrospective study. Onco Targets Ther. (2018) 11:1141–8. doi: 10.2147/OTT.S156792
36. Wigmore TJ, Mohammed K, Jhanji S. Long-term survival for patients undergoing volatile versus IV anesthesia for cancer surgery: a retrospective analysis. Anesthesiology. (2016) 124:69–79. doi: 10.1097/ALN.0000000000000936
37. Lai HC, Lee MS, Lin C, Lin KT, Huang YH, Wong CS, et al. Propofol-based total intravenous anaesthesia is associated with better survival than desflurane anaesthesia in hepatectomy for hepatocellular carcinoma: a retrospective cohort study. Br J Anaesth. (2019) 123:151–60. doi: 10.1016/j.bja.2019.04.057
38. Beecher SM, O’Leary DP, McLaughlin R, Sweeney KJ, Kerin MJ. Influence of complications following immediate breast reconstruction on breast cancer recurrence rates. Br J Surg. (2016) 103:391–8. doi: 10.1002/bjs.10068
39. Mirnezami A, Mirnezami R, Chandrakumaran K, Sasapu K, Sagar P, Finan P. Increased local recurrence and reduced survival from colorectal cancer following anastomotic leak: systematic review and meta-analysis. Ann Surg. (2011) 253:890–9. doi: 10.1097/SLA.0b013e3182128929
40. Haidinger R, Bauerfeind I. Long-term Side effects of adjuvant therapy in primary breast cancer patients: results of a web-based survey. Breast Care. (2019) 14:111–6. doi: 10.1159/000497233
41. Azim HA Jr, de Azambuja E, Colozza M, Bines J, Piccart MJ. Long-term toxic effects of adjuvant chemotherapy in breast cancer. Ann Oncol. (2011) 22:1939–47. doi: 10.1093/annonc/mdq683
42. Luna CM, Palma I, Niederman MS, Membriani E, Giovini V, Wiemken TL, et al. The impact of age and comorbidities on the mortality of patients of different age groups admitted with community-acquired pneumonia. Ann Am Thorac Soc. (2016) 13:1519–26. doi: 10.1513/AnnalsATS.201512-848OC
43. Williams GR, Mackenzie A, Magnuson A, Olin R, Chapman A, Mohile S, et al. Comorbidity in older adults with cancer. J Geriatr Oncol. (2016) 7:249–57. doi: 10.1016/j.jgo.2015.12.002
44. Jun IJ, Jo JY, Kim JI, Chin JH, Kim WJ, Kim HR, et al. Impact of anesthetic agents on overall and recurrence-free survival in patients undergoing esophageal cancer surgery: a retrospective observational study. Sci Rep. (2017) 7:14020. doi: 10.1038/s41598-017-14147-9
45. Yuki K, Eckenhoff RG. Mechanisms of the immunological effects of volatile anesthetics: a review. Anesth Analg. (2016) 123:326–35. doi: 10.1213/ANE.0000000000001403
Keywords: breast neoplasia, esophageal neoplasia, lung neoplasia, inhaled anesthesia, intravenous anesthesia, prognosis
Citation: Che X and Li T (2023) Total versus inhaled intravenous anesthesia methods for prognosis of patients with lung, breast, or esophageal cancer: A cohort study. Front. Surg. 10:1155351. doi: 10.3389/fsurg.2023.1155351
Received: 31 January 2023; Accepted: 17 March 2023;
Published: 11 April 2023.
Edited by:
Li Hecheng, Shanghai Jiao Tong University, ChinaReviewed by:
Feifei Lou, Fudan University, ChinaRunsen Jin, Shanghai Jiao Tong University, China
Chenyang Dai, Tongji University, China
© 2023 Che and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tianzuo Li bGl0ekBianNqdGguY24=
Specialty Section: This article was submitted to Surgical Oncology, a section of the journal Frontiers in Surgery