 Jun Lei
Jun Lei Kai Huang1
Kai Huang1
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg. , 21 March 2023
Sec. Genitourinary Surgery and Interventions
Volume 10 - 2023 | https://doi.org/10.3389/fsurg.2023.1138814
This article is part of the Research Topic Complications, Difficulties, and Limits of Minimally Invasive Urologic Pelvic Surgery View all 8 articles
Objective: To evaluate the outcomes of patient-centered enhanced recovery after surgery (ERAS) in percutaneous nephrolithotomy (PCNL) for staghorn stones.
Patients and methods: A retrospective analysis of 106 patients with staghorn calculi who underwent PCNL treatment at the Third Xiangya Hospital from October 01, 2018 to September 30, 2021 was performed. The patients were divided into the ERAS group (n = 56) and traditional group (n = 50). The ERAS program focused on a patient-centered concept, with elaboration on aspects, such as patient education, nutritional support, analgesia, body warming, early mobilization, nephrostomy tube removal, and strict follow-up.
Results: The total stone free rate and total complication rate were similar in both groups. The visual analogue scale (VAS) 6 h after surgery, ambulation off bed time, indwelling fistula time, indwelling catheter time, and postoperative hospital stays were lower in the ERAS group than in the traditional group (P < 0.05). The multiple session rate in the ERAS group (19, 28.57%) was lower than that in the traditional group (30, 60%) (P = 0.007). The 1-year stone recurrence rate in the ERAS group (7, 17.5%) was lower than that in the traditional group (14, 38.9%) (P = 0.037).
Conclusion: The patient-centered ERAS in PCNL for staghorn stones accelerated rehabilitation by relieving postoperative pain, shortening hospitalization time, accelerating early ambulation, and reducing multiple session rate and 1-year stone recurrence rate, which have socioeconomic benefits.
Staghorn calculi are large kidney stones located in the renal pelvis and extending into calices. If untreated, they may cause renal failure and even life-threatening urosepsis with time (1–3). Although the proportion of Staghorn calculi among all urinary stones has been reduced to 4% due to early and effective management of renal stones in developed countries, incidence remains 10%–20% in developing countries (4, 5). Among all treatment options for staghorn calculi, percutaneous nephrolithotomy (PCNL) is recommended as the gold standard (6, 7). However, PCNL is often performed in several stages with potential of major postoperative complications, including severe bleeding and urosepsis, occurring at a rate of 1.1%–7.0% (8, 9). Furthermore, patients with Staghorn calculi often have poor economic backgrounds and possible underlying infections and malnutrition (5, 10, 11).
First applied in Denmark by Kehlet (12), enhanced recovery after surgery (ERAS) was introduced in China by Jiang (13) in 2007. ERAS refers to the optimization of the clinical pathway during perioperative management based on evidence-based medicine practiced by multi-department collaboration in surgery, anesthesia, and nursing (12, 14). It can significantly alleviate perioperative stress response and complications, shorten hospital stay, and accelerate rehabilitation in several surgical specialties (15–18). However, the literature on the suitability of the ERAS program for use of PCNL in treating Staghorn calculi remains limited.
Therefore, to determine whether patients receiving PCNL for staghorn stones could also benefit from the ERAS protocol, this study systematically investigated the evidence and guidelines published in English and Chinese databases, developed a patient-centered ERAS protocol, and evaluated the outcomes.
A comprehensive literature review was performed on literature available in databases, such as EBSCO Medline, PubMed, Elsevier, NGC, CNKI, and Wanfang. After screening using keywords, such as “enhanced recovery after surgery,” “fast track surgery,” “kidney stone,” and “ Staghorn calculi,” one Chinese expert consensus (19), nine clinical practice guidelines (20–28), three reviews (11, 29, 30), and one randomized controlled trial (RCT) (31) were selected for developing the ERAS protocol. It is detailed in Table 1.
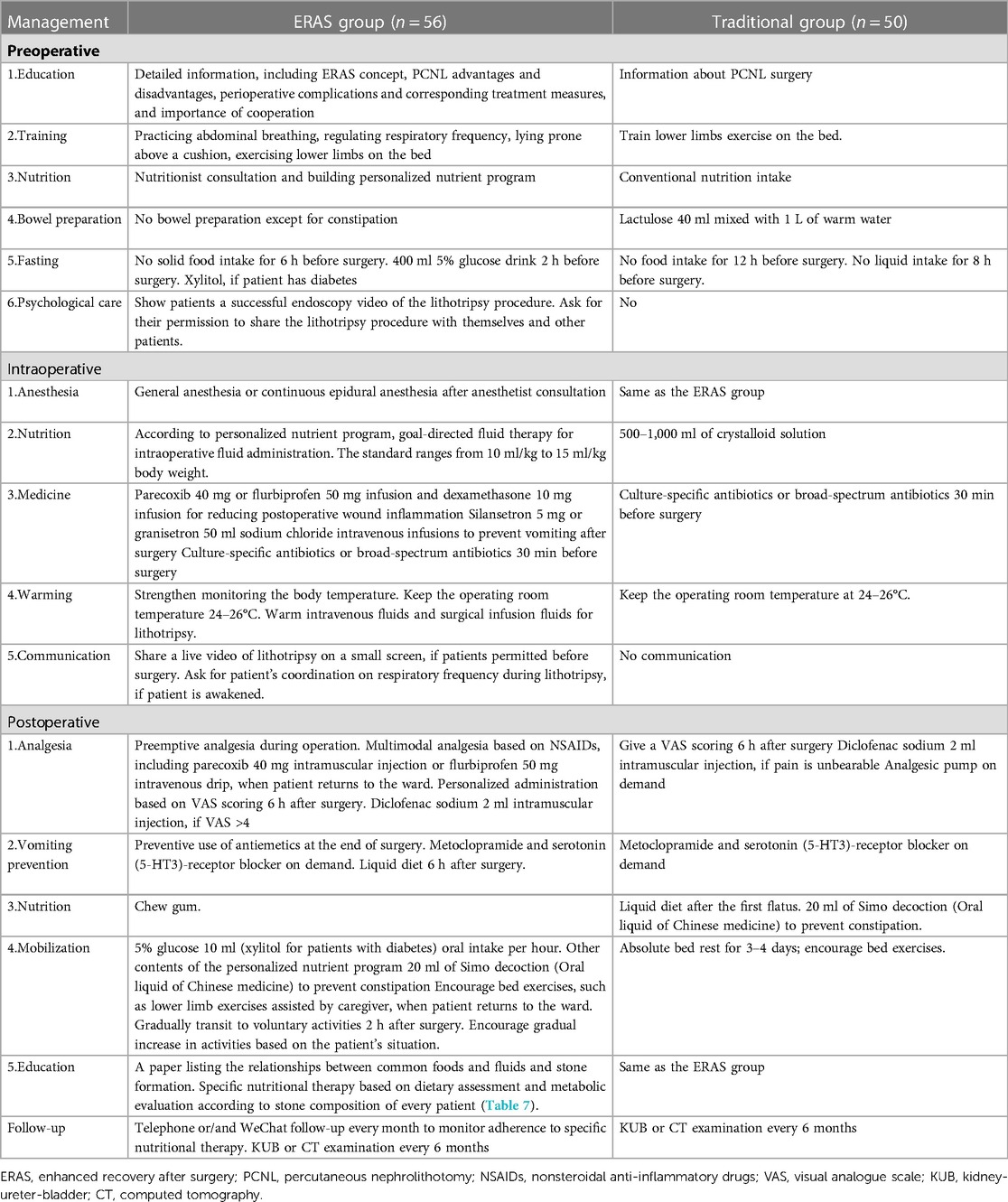
Table 1. Detailed patient-centered ERAS program.
This study was approved by the Institutional Review Board of The Third Xiangya Hospital of Central South University (ID: fast I 21075). All patients with staghorn stones were informed whether to accept the ERAS protocol since October 2019. If accepted, they and their family members provided written informed consent for participation and the use of their clinical data in publications and were assigned to the ERAS group, which was administered by a dedicated team consisting of 4 urologists and 5 nurses who received professional ERAS protocol training. If patients and their family members did not agree, they were assigned to the traditional group. Because the majority of patients chose to receive the ERAS protocol, patients in the traditional group were insufficient after the ERAS protocol was carried out. Considering that there was no difference between the treatments of patients in the traditional group and the previous patients with staghorn stones, we selected October 2018 as the enrollment time point of the traditional group.
The inclusion criteria were (1) diagnosis of staghorn calculi by abdominal plain radiography (KUB), intravenous urography (IVU), or non-contrast computed tomography (CT); (2) age between 18 and 70 years; (3) planned initial therapy with PCNL; (4) ASA grade of I–III; (5) diabetes-controlled postprandial blood glucose ≤11.1 mmol/L, hypertension-controlled blood pressure ≤140/100 mmHg; and (6) absence of uncontrolled renal and cardiopulmonary insufficiency. The exclusion criteria were (1) in company with renal tumor, tuberculosis, and other urinary diseases; (2) presence of horseshoe kidney, ectopic kidney, isolated kidney, ureteropelvic junction obstruction (UPJO), scoliosis, and other severe malformations; (3) history of ipsilateral open surgery; (4) urosepsis requiring emergency surgery management; and (5) anticoagulant use in the past two weeks.
Thereafter, a retrospective analysis of 106 patients with staghorn calculi who underwent PCNL treatment in The Third Xiangya Hospital from October 2018 to September 2021 was performed. The patients were categorized by use of ERAS management (n = 56) or conventional management (n = 50). The detailed distinctions between both groups are shown in Table 1.
All patients provided detailed medical histories Preoperative examinations included routine blood tests, serum creatinine, coagulation function test, urine culture, and radiological evaluations, such as KUB, IVU and CT (mandatory), and/or urinary ultrasonography. Stone surface area was assessed as stone burden as determined by radiological examinations, such as the KUB or CT. For all patients, infections were treated and antibiotics were administered as prophylaxis preoperatively.
After anesthesia, patients were placed in the lithotomy position to complete ureteral catheterization. Thereafter, they were placed in a prone position to establish PCNL tracts. Guided by ultrasound, an experienced urologist obtained All PCNL accesses. After placing the safety wire, the tract was dilated with an 8-Fr renal sheath to 20/24 Fr. Multiple tracks could be obtained, if devised in the preoperative plan; otherwise, multiple tracks could be accessed during surgery on demand. Ultrasonic pneumatic devices or holmium laser lithotripter was used to fragment stones using 18 Fr or 20 Fr rigid ureteroscope. A nephrostomy tube and double-J internal ureteral stent were routinely inserted at the end of the first session of the PCNL.
Hematologic examinations, including routine blood tests, serum creatinine, and hepatorenal function, were performed immediately after patients returned from the ward. A visual analogue scale (VAS) was used to evaluate postoperative pain 6 h after surgery. Stones collected during operation were analyzed by infrared spectroscopy to confirm the chemical composition. Culture-specific antibiotics were administered, if preoperative urine cultures were positive, whereas broad-spectrum antibiotics were administered, if preoperative urine cultures were negative for 5–7 days. KUB or non-contrast CT (suggested) was ordered at least a day before discharge to assess the state of stone clearance and ascertain the double-J stent in the right position. Removal of the nephrostomy tube was based on whether the drainage had become roughly clear. If a secondary PCNL session was planned when the status of stone clearance had not been clarified, it was retained. All patients were followed up by KUB or CT (suggested) every 6 months. The internal double-J stent was removed a month later. The results of the examination during follow-up determined whether stones recurred a year after surgery.
General characteristics, including age, sex, body mass index (BMI), American Society of Anesthesiologists (ASA) classification, stone size, staghorn calculi type, stone burden, distance of tract, and stone CT value, were used to evaluate baseline characteristics. Stone burden, tract length, and CT value were obtained from measurements on CT by two different urologists. The following formula was used to calculate the stone burden: length × width × π × 0.25 (32). Residual stone fragments smaller than 4 mm in diameter, which did not require surgical intervention, were counted in clearance.
Postoperative clinical data, such as operative time, multi-tract rate, hemoglobin decrease, multiple session rate, total stone free rate, and 1-year recurrence rate, were recorded. Additionally, recovery data, such as VAS 6 h after surgery, ambulation off bed time, indwelling fistula time, indwelling catheter time, hospital stay, and complications were subsequently recorded for comparison between both groups.
IBM SPSS version 26.0 software (IBM Corp., Armonk, NY, USA) was used for all statistical analyses. Measurement data were expressed as mean ± standard deviation (SD). Two independent sample t-test was used to compare the differences between the groups. Categorical data were expressed as frequencies and percentages. The Chi-square test (χ2) was applied to compare the differences between both groups. P < 0.05 indicated that the differences between both groups had statistical significance.
The preoperative characteristics of patients, including age, BMI, and stone CT value, were not different between both groups (P > 0.05) (Table 2). The postoperative surgical parameters of both groups are listed in Table 3. All patients successfully underwent PCNL. No intraoperative conversion to open surgery was required. No differences in operative time, tract size, tract number, multi-tract rate, hemoglobin decrease, and total stone free rate between both groups were recorded. However, the multiple session rate of the ERAS group (19, 28.57%) was lower than that of the traditional group (30, 60%) (P = 0.007). Additionally, the 1-year recurrence rate in the ERAS group (7, 17.5%) was lower than that in the traditional group (14, 38.9%) (P = 0.037). Table 4 shows the postoperative recovery parameters. No differences in hematuria duration and total hospital stay were between both groups were recorded. However, VAS 6 h after surgery (1.32 ± 0.66 in the ERAS group; 2.24 ± 0.82 in the traditional group), ambulation off bed time (1.64 ± 0.61days in the ERAS group; 2.86 ± 0.67 days in the traditional group), indwelling fistula time (3.14 ± 2.54 days in the ERAS group; 4.82 ± 3.27 days in the traditional group), indwelling catheter time (2.37 ± 1.13 days in the ERAS group; 4.98 ± 1.47 days in the traditional group), and postoperative hospital stay (6.67 ± 2.09 days in the ERAS group; 7.96 ± 2.02 days in the traditional group) were different (P < 0.05) between both groups. Generally, these indicators were lower in the ERAS group than in the traditional group. The postoperative complications of both groups are listed in Table 5. Additionally, seven cases of fever were recorded in the ERAS group. Among these patients, one, four, and two cases were associated with urosepsis, prolonged hematuria, and transfusion, respectively. One patient with severe hematuria underwent digital subtraction angiography (DSA) embolization. Furthermore, one patient was diagnosed with hydrothorax without surgical intervention 2 days after operation. In the traditional group, six and seven cases of fever and prolonged hematuria, respectively, were recorded. Four cases were associated with transfusion, whereas one patient with hematuria underwent DSA embolization. In both groups, all complications were treated medically. No ICU admission or deaths were recorded. In Table 6, the stone composition of both groups are listed. After analyses by infrared spectroscopy, most stones were mixed stones. In this study, the stones were mainly composed of calcium, uric acid, struvite, and cystine. In the ERAS group, 37 calcium-based, six uric acid, and 13 struvite stones were identified; whereas in the traditional group, 31 calcium-based, two uric acid, one cystine, and 16 struvite stones were identified.
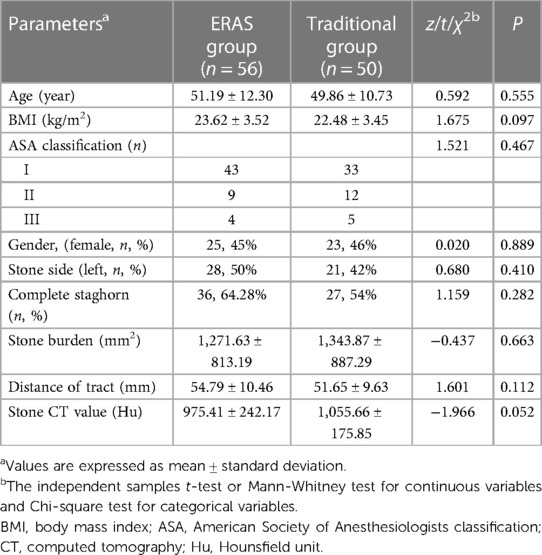
Table 2. Preoperative characteristics of patients.
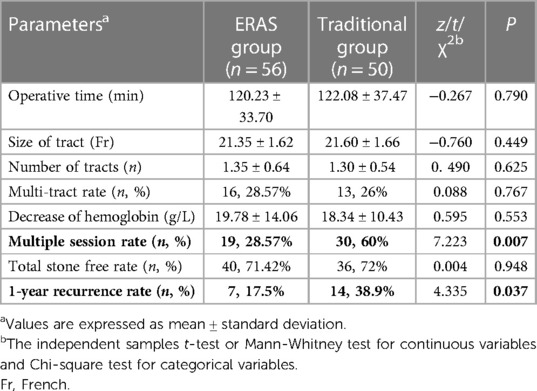
Table 3. Postoperative surgical parameters.
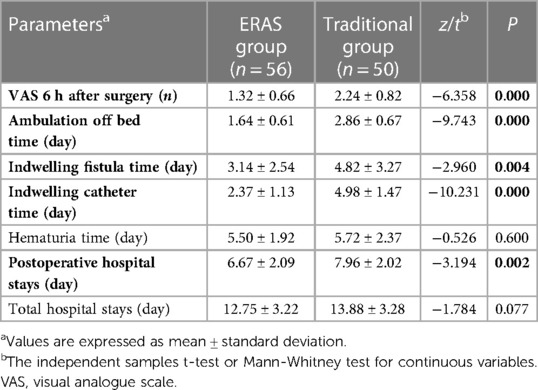
Table 4. Postoperative recovery parameters.
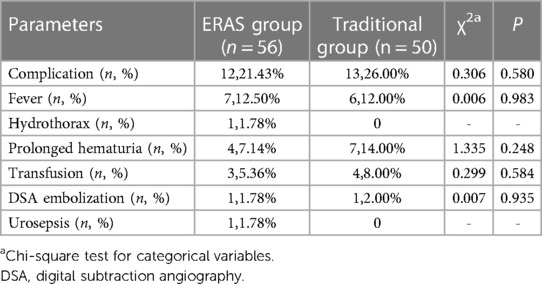
Table 5. Postoperative complications.
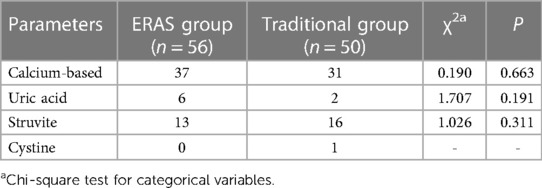
Table 6. Stone composition.
ERAS is a program with a series of standardized protocols developed by multi-department collaboration. It aims to improve the outcomes of patient recovery after surgery by minimizing the negative stress effects of surgery, effective analgesia, early mobilization, and early nutrition intake (33). In the past few years, the ERAS program has gradually been applied in the management of prostate cancer and bladder tumor by urologists (29, 34, 35). However, few studies have reported the implementation of ERAS in PCNL for treating staghorn calculi. Besides, the current ERAS program for surgery pays much attention to multi-department collaboration, without much focus on patient participation. This study explored a patient-centered ERAS in PCNL for staghorn calculi based on existing protocols suited for the actual conditions. Patient-centered care is the core concept, and the key principle is attention to patient participation during the whole treatment process, ranging from medical decision making to follow-up. In the ERAS program, the main method is full elimination of the information barrier on diseases and therapies between patients and medical staff through adequate education and communication using various approaches, such as multimedia.
Patient education is an integral part of the ERAS program, especially in patient-centered ERAS, and encompasses the whole process of diagnosis and treatment. The formation and recurrence of urinary calculi have a chronic pathologic basis and are closely related to nutrient intake (11, 29, 36). The contents of our patient education in the ERAS group included not only the ERAS concept, advantages and disadvantages of PCNL, perioperative complications and corresponding treatment measures, and importance of cooperation but also the relationship between the formation and recurrence of urinary calculi and nutrition. Additionally, the importance of nutritional therapy outside the hospital based on different stone compositions in preventing stone recurrence was emphasized repeatedly in every follow-up session by call or WeChat. Only 30.2% of patients were found to be adherent to the strict and complex nutritional therapies 6 months after surgery (36). Therefore, this study simplified the nutritional therapies and performed a strict supervision during every follow-up session to improve adherence and participation of patients on nutritional therapy (Table 7). Beyond these interventions, we showed patients the endoscopy video of a successful lithotripsy procedure to eliminate their preoperative tension and improve their confidence in the surgery. Subsequently, we improved the training exercises of patients involved in abdominal breathing, respiratory frequency regulation, prone positioning above a cushion, and lower limb stretching on the bed in preparation for early ambulation.
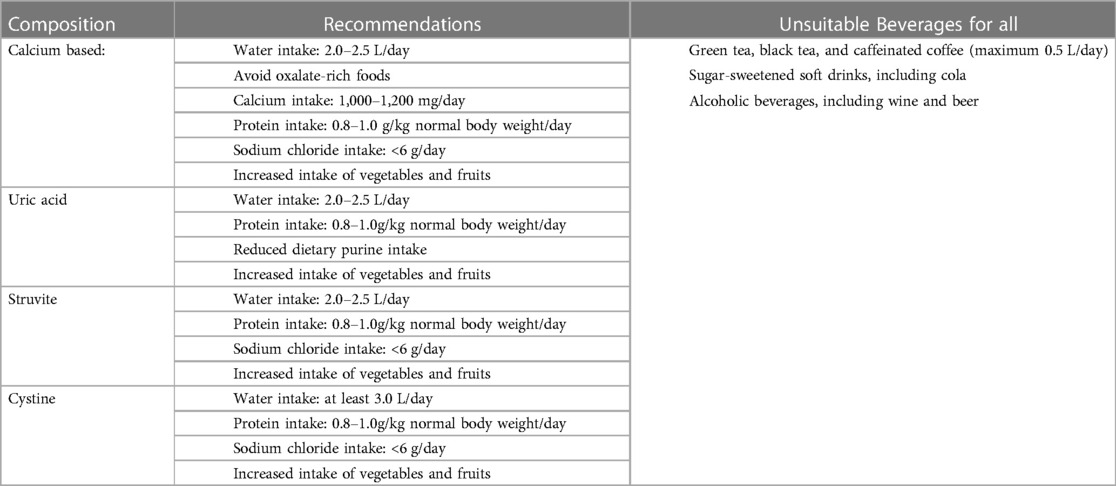
Table 7. Nutritional recommendations summarized for different stone compositions.
Nutrition is essential for postoperative recovery of patients who have undergone surgery. Preoperative nutritional inadequacy is often an important cause of postoperative metabolic stress and insulin resistance, which often lead to weakness and increased mortality in severe cases (37). PCNL is a major surgery in urology. Therefore, nutritional management, which involves interdisciplinary collaboration, was a key component of ERAS in PCNL for staghorn calculi. Excessive intraoperative or postoperative fluid infusion can cause several complications, such as intestinal edema, hypervolemia, coagulation dysfunction, and wound healing delays; whereas restricted fluid intake can relieve pain and quicken recovery (38). Hence, nutritionists are consulted to assess patients' nutritional conditions with the aim of forming a personalized nutrition plan after hospitalization. In the ERAS group, 400 ml of 5% glucose drinks was administered 2 h before surgery, and intraoperative restricted fluid infusion with a standard of 10–15 ml/kg body weight was administered. Early oral intake can increase gastrointestinal activity, promote bowel movement, facilitate higher cognitive function, reduce infectious complications, and improve patient satisfaction (38, 39). Therefore, patients in the ERAS group consumed liquid diets 6 h after surgery and chewed gum.
Preoperative fasting and intestinal preparation are important components of the nutritional plan. Traditional preoperative fasting and intestinal preparation for PCNL are mainly used to prevent anesthetic aspiration and reduce postoperative infection. In fact, enema and long-term fasting before surgery often cause complications, such as pain, bleeding, infection, intestinal mucosal architectural change, electrolyte disturbance, and dehydration (40, 41). In the ERAS group, no preoperative intestinal preparation and routine fasting was performed. No anesthetic aspiration occurred during surgery.
The maintenance of normal body temperature is necessary for life (42). The incidence of hypothermia of varied degrees, which most surgical patients experience during the perioperative period, is 4%–90% (43). Additionally, routine fluid intake during surgery and endoscopic procedures, such as PCNL, require continuous irrigation of fluids for better visualization and removal of stones and blood clots. This often causes a drop in body temperature (44). Perioperative hypothermia is closely associated with multiple complications, including surgical site infection, coagulopathy, slow drug metabolism, increased cardiovascular events, and prolonged hospital stay (45). The maintenance of perioperative body temperature is a core component of clinical pathways in the ERAS program (46). Therefore, body temperature was strictly monitored, the operating room temperature was kept as 24–26°C, and intravenous fluids and surgical infusion fluids were warmed when lithotripsy was performed in the ERAS group to reduce postoperative complications.
Analgesia is an important part of the ERAS program. Few studies reported that the incidence of moderate-to-severe pain after PCNL was approximately 60%, which affected patients, regarding postoperative rehabilitation, daily activities, quality of life, and social and economic conditions (47, 48). Opioids used in traditional analgesia have side effects, such as nausea, vomiting, and intestinal ileus. Therefore, nonsteroidal anti-inflammatory drugs (NSAID), such as parecoxib and flurbiprofen, are recommended (48). Preemptive analgesia during operation, multimodal analgesia based on NSAIDs, and personalized administration based on VAS scoring were performed in the ERAS group.
Adequate analgesia can contribute to early mobilization and diminish postoperative stress response (48). Early mobilization has positive effects on muscle strength, bowel function, cardiovascular and respiratory functions, psychological well-being, and venous thromboembolism prevention (39). Hence, patients in the ERAS group underwent training exercises before surgery. They were encouraged to perform bed exercises, such as lower limb exercises aided by caregivers, which gradually transit to voluntary activities 2 h after surgery. In this study, the VAS 6 h after surgery was lower in the ERAS group (1.32 ± 0.66) than in the traditional group (2.24 ± 0.82) (P < 0.05). The ambulation off bed time (1.64 ± 0.61 days) in the ERAS group was lower than that in the traditional group (2.86 ± 0.67 days) (P < 0.05). These findings showed a trend of postoperative pain relief and early ambulation off bed in the ERAS group.
Indwelling nephrostomy after PCNL was supposed to press the puncture tract, strengthen drainage and hemostasis, reduce urine extravasation, lower the risk of infection, and improve convenience of the secondary procedure in the traditional concept (49). According to a recent study, early removal of the nephrostomy tube or tubeless nephrostomy does not increase the risk of bleeding, infection, and urine extravasation (50). Due to the high probability of a secondary session in PCNL for staghorn calculi, all patients underwent indwelled nephrostomy after surgery in this study. Additionally, early removal of nephrostomy was encouraged in the ERAS group. No difference in decrease of hemoglobin, hematuria time, and complications were recorded (P > 0.05). The indwelling fistula time (3.14 ± 2.54 days), indwelling catheter time (2.37 ± 1.13 days), postoperative hospital stay (6.67 ± 2.09 days) in the EARS group were lower than those (4.82 ± 3.27 days, 4.98 ± 1.47 days, and 7.96 ± 2.02 days) in the traditional group (P < 0.05). In the ERAS group, the outcomes showed a trend of decrease in discomfort, acceleration to early exercise, and reduction of postoperative hospitalization time.
PCNL of staghorn calculi often requires multiple procedures to achieve a satisfactory stone clearance rate (6, 7). However, multiple sessions of PCNL increase costs and risk of complications. The stone burden, stone CT value, tract size, and tract number may be the contributory factors. In this study, no differences in stone burden, stone CT value, tract size, and tract number between both groups were recorded (P > 0.05). The multiple session rate in the ERAS group (19, 28.57%) was lower than that in the traditional group (30, 60%, P = 0.007). Three possible explanations were considered. First, a combination of pneumatic and holmium laser lithotripsy was used in PCNL for staghorn calculi. The former has been shown to have a higher efficiency in the removal of staghorn calculi (51). Therefore, adequate preoperative nutritional support allowed patients in the ERAS group to tolerate longer periods of pneumatic lithotripsy. Second, after preoperative education and communication, the patients could coordinate with the surgeon by voluntary regulation of the respiratory frequency during the lithotripsy procedure. Third, a higher CT value was associated with harder stones (52). The CT value in the ERAS group (975.41 ± 242.17) was lower than that in the traditional group (1,055.66 ± 175.85) (Although P = 0.052). This may affect the efficiency of lithotripsy to an extent.
Nutritional intake after discharge is closely related to the recurrence rate of kidney stones (11, 29). The 5-year recurrence rate of calculi ranges from 31.5% to 50%, whereas the 20-year recurrence rate is as high as 75% (53, 54). The 1-year recurrence rate (7, 17.5%) in the ERAS group was lower than that in the traditional group (14, 38.9%) (P = 0.037). The monthly follow-up, which encouraged patients to actively or passively adhere to nutritional recommendations, could account for these findings.
The study had few limitations. First, this study was a single-center retrospective study. Second, the study used a small sample size. Third, the follow-up period was short-term; it was 1 year post-surgery. Further multi-center studies with a robust design, adequate sample size, and long follow-up period are required to confirm the conclusions and develop the ERAS protocols in PCNL for staghorn calculi.
The patient-centered ERAS in PCNL for staghorn calculi accelerated rehabilitation by relieving postoperative pain, shortening hospitalization time, accelerating early ambulation, and reducing multiple session rate and 1-year stone recurrence rate, which have socioeconomic benefits.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by Institutional Review Board of The Third Xiangya Hospital of Central South University. The patients/participants provided their written informed consent to participate in this study.
GY had full access to all the data in this study and takes responsibility for the integrity of the data. JL contributed to study concept and design and the drafting of manuscript. KH was involved acquisition of data. JL and KH carried out statistical analysis. YD performed critical revision of the manuscript for important intellectual content. GY and YD performed supervision. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Healy KA, Ogan K. Pathophysiology and management of infectious staghorn calculi. Urol Clin North Am. (2007) 34(3):363–74. doi: 10.1016/j.ucl.2007.05.006
2. Teichman JM, Long RD, Hulbert JC. Long-term renal fate and prognosis after staghorn calculus management. J Urol. (1995) 153(5):1403–7. doi: 10.1016/S0022-5347(01)67413-5
3. Koga S, Arakaki Y, Matsuoka M, Ohyama C. Staghorn calculi–long-term results of management. Br J Urol. (1991) 68(2):122–4. doi: 10.1111/j.1464-410x.1991.tb15278.x
4. Rieu P. Infective lithiasis. Ann Urol (Paris). (2005) 39(1):16–29. doi: 10.1016/j.anuro.2005.01.001
5. Zeng G, Mai Z, Xia S, Wang Z, Zhang K, Wang L, et al. Prevalence of kidney stones in China: an ultrasonography based cross-sectional study. BJU Int. (2017) 120(1):109–16. doi: 10.1111/bju.13828
6. Assimos D, Krambeck A, Miller NL, Monga M, Murad MH, Nelson CP, et al. Surgical management of stones: american urological association/endourological society guideline, PART I. J Urol. (2016) 196(4):1153–60. doi: 10.1016/j.juro.2016.05.090
7. Turk C, Petrik A, Sarica K, Seitz C, Skolarikos A, Straub M, et al. EAU Guidelines on interventional treatment for urolithiasis. Eur Urol. (2016) 69(3):475–82. doi: 10.1016/j.eururo.2015.07.041
8. Ghani KR, Sammon JD, Bhojani N, Karakiewicz PI, Sun M, Sukumar S, et al. Trends in percutaneous nephrolithotomy use and outcomes in the United States. J Urol. (2013) 190(2):558–64. doi: 10.1016/j.juro.2013.02.036
9. Gadzhiev N, Malkhasyan V, Akopyan G, Petrov S, Jefferson F, Okhunov Z. Percutaneous nephrolithotomy for staghorn calculi: troubleshooting and managing complications. Asian J Urol. (2020) 7(2):139–48. doi: 10.1016/j.ajur.2019.10.004
10. Flannigan R, Choy WH, Chew B, Lange D. Renal struvite stones–pathogenesis, microbiology, and management strategies. Nat Rev Urol. (2014) 11(6):333–41. doi: 10.1038/nrurol.2014.99
11. Siener R. Nutrition and kidney stone disease. Nutrients. (2021) 13(6):1197. doi: 10.3390/nu13061917
12. Kehlet H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br J Anaesth. (1997) 78(5):606–17. doi: 10.1093/bja/78.5.606
13. Jiang Z, Li J. Current Status of enhanced recovery after surgery in China. Zhonghua Wei Chang Wai Ke Za Zhi. (2016) 19(3):246–9. doi: 10.3760/cma.j.issn.1671-0274.2016.03.002
14. McLeod RS, Aarts MA, Chung F, Eskicioglu C, Forbes SS, Conn LG, et al. Development of an enhanced recovery after surgery guideline and implementation strategy based on the knowledge-to-action cycle. Ann Surg. (2015) 262(6):1016–25. doi: 10.1097/SLA.0000000000001067
15. Dickson EL, Stockwell E, Geller MA, Vogel RI, Mullany SA, Ghebre R, et al. Enhanced recovery program and length of stay after laparotomy on a gynecologic oncology service: a randomized controlled trial. Obstet Gynecol. (2017) 129(2):355–62. doi: 10.1097/AOG.0000000000001838
16. Frees SK, Aning J, Black P, Struss W, Bell R, Chavez-Munoz C, et al. A prospective randomized pilot study evaluating an ERAS protocol versus a standard protocol for patients treated with radical cystectomy and urinary diversion for bladder cancer. World J Urol. (2018) 36(2):215–20. doi: 10.1007/s00345-017-2109-2
17. Pang KH, Groves R, Venugopal S, Noon AP, Catto JWF. Prospective implementation of enhanced recovery after surgery protocols to radical cystectomy. Eur Urol. (2018) 73(3):363–71. doi: 10.1016/j.eururo.2017.07.031
18. Powell AC, Stopfkuchen-Evans M, Urman RD, Bleday R. Decreasing the surgical stress response and an initial experience from the enhanced recovery after surgery colorectal surgery program at an academic institution. Int Anesthesiol Clin. (2017) 55(4):163–78. doi: 10.1097/AIA.0000000000000162
19. EGfERa S. Chinese Expert consensus on enhanced recovery after surgery in perioperative management. Surg J Chin. (2016) 54(06):413–8. doi: 10.3760/cma.j.issn.0529-5815.2016.06.004
20. Cerantola Y, Valerio M, Persson B, Jichlinski P, Ljungqvist O, Hubner M, et al. Guidelines for perioperative care after radical cystectomy for bladder cancer: enhanced recovery after surgery {ERAS[(R)]} society recommendations. Clin Nutr. (2013) 32(6):879–87. doi: 10.1016/j.clnu.2013.09.014
21. Melloul E, Hubner M, Scott M, Snowden C, Prentis J, Dejong CH, et al. Guidelines for perioperative care for liver surgery: enhanced recovery after surgery (ERAS) society recommendations. World J Surg. (2016) 40(10):2425–40. doi: 10.1007/s00268-016-3700-1
22. Lassen K, Coolsen MM, Slim K, Carli F, de Aguilar-Nascimento JE, Schafer M, et al. Guidelines for perioperative care for pancreaticoduodenectomy: enhanced recovery after surgery [ERAS(R)] society recommendations. Clin Nutr. (2012) 31(6):817–30. doi: 10.1016/j.clnu.2012.08.011
23. Thorell A, MacCormick AD, Awad S, Reynolds N, Roulin D, Demartines N, et al. Guidelines for perioperative care in bariatric surgery: enhanced recovery after surgery (ERAS) society recommendations. World J Surg. (2016) 40(9):2065–83. doi: 10.1007/s00268-016-3492-3
24. Gustafsson UO, Scott MJ, Schwenk W, Demartines N, Roulin D, Francis N, et al. Guidelines for perioperative care in elective colonic surgery: enhanced recovery after surgery [ERAS(R)] society recommendations. Clin Nutr. (2012) 31(6):783–800. doi: 10.1016/j.clnu.2012.08.013
25. Nygren J, Thacker J, Carli F, Fearon KC, Norderval S, Lobo DN, et al. Guidelines for perioperative care in elective rectal/pelvic surgery: enhanced recovery after surgery [ERAS(R)] society recommendations. Clin Nutr. (2012) 31(6):801–16. doi: 10.1016/j.clnu.2012.08.012
26. Nelson G, Altman AD, Nick A, Meyer LA, Ramirez PT, Achtari C, et al. Guidelines for pre- and intra-operative care in gynecologic/oncology surgery: enhanced recovery after surgery [ERAS(R)] society recommendations–part I. Gynecol Oncol. (2016) 140(2):313–22. doi: 10.1016/j.ygyno.2015.11.015
27. Nelson G, Altman AD, Nick A, Meyer LA, Ramirez PT, Achtari C, et al. Guidelines for postoperative care in gynecologic/oncology surgery: enhanced recovery after surgery [ERAS(R)] society recommendations–part II. Gynecol Oncol. (2016) 140(2):323–32. doi: 10.1016/j.ygyno.2015.12.019
28. Melloul E, Lassen K, Roulin D, Grass F, Perinel J, Adham M, et al. Guidelines for perioperative care for pancreatoduodenectomy: enhanced recovery after surgery (ERAS) recommendations 2019. World J Surg. (2020) 44(7):2056–84. doi: 10.1007/s00268-020-05462-w
29. D'Alessandro C, Ferraro PM, Cianchi C, Barsotti M, Gambaro G, Cupisti A. Which diet for calcium stone patients: a real-world approach to preventive care. Nutrients. (2019) 11(5):1182. doi: 10.3390/nu11051182
30. Chen T, Zhu Z, Du J. Efficacy of intercostal nerve block for pain control after percutaneous nephrolithotomy: a systematic review and meta-analysis. Front Surg. (2021) 8:623605. doi: 10.3389/fsurg.2021.623605
31. Li Q, Wan L, Liu S, Li M, Chen L, Hou Z, et al. Clinical efficacy of enhanced recovery after surgery in percutaneous nephrolithotripsy: a randomized controlled trial. BMC Urol. (2020) 20(1):162. doi: 10.1186/s12894-020-00728-w
32. Ito H, Kawahara T, Terao H, Ogawa T, Yao M, Kubota Y, et al. The most reliable preoperative assessment of renal stone burden as a predictor of stone-free status after flexible ureteroscopy with holmium laser lithotripsy: a single-center experience. Urology. (2012) 80(3):524–8. doi: 10.1016/j.urology.2012.04.001
33. Hjort Jakobsen D, Rud K, Kehlet H, Egerod I. Standardising fast-track surgical nursing care in Denmark. Br J Nurs. (2014) 23(9):471–6. doi: 10.12968/bjon.2014.23.9.471
34. Wallace BK, Li G, McKiernan JM, DeCastro GJ, Anderson CB. Radical cystectomy in a cohort of octogenarians managed in the ERAS era. Urol Oncol. (2021) 39(5):299 e1–e6. doi: 10.1016/j.urolonc.2020.09.009.
35. Zhao Y, Zhang S, Liu B, Li J, Hong H. Clinical efficacy of enhanced recovery after surgery (ERAS) program in patients undergoing radical prostatectomy: a systematic review and meta-analysis. World J Surg Oncol. (2020) 18(1):131. doi: 10.1186/s12957-020-01897-6
36. Dauw CA, Yi Y, Bierlein MJ, Yan P, Alruwaily AF, Ghani KR, et al. Factors associated with preventive pharmacological therapy adherence among patients with kidney stones. Urology. (2016) 93:45–9. doi: 10.1016/j.urology.2016.03.030
37. Weimann A, Braga M, Carli F, Higashiguchi T, Hubner M, Klek S, et al. ESPEN Guideline: clinical nutrition in surgery. Clin Nutr. (2017) 36(3):623–50. doi: 10.1016/j.clnu.2017.02.013
38. Azhar RA, Bochner B, Catto J, Goh AC, Kelly J, Patel HD, et al. Enhanced recovery after urological surgery: a contemporary systematic review of outcomes, key elements, and research needs. Eur Urol. (2016) 70(1):176–87. doi: 10.1016/j.eururo.2016.02.051
39. Huang Z, Yi L, Zhong Z, Zhu L, Zhao H, Li Y, et al. Comparison of fast-track versus conventional surgery protocol for patients undergoing robot-assisted laparoscopic radical prostatectomy: a Chinese experience. Sci Rep. (2018) 8(1):8017. doi: 10.1038/s41598-018-26372-x
40. Holte K, Nielsen KG, Madsen JL, Kehlet H. Physiologic effects of bowel preparation. Dis Colon Rectum. (2004) 47(8):1397–402. doi: 10.1007/s10350-004-0592-1
41. Bucher P, Gervaz P, Egger JF, Soravia C, Morel P. Morphologic alterations associated with mechanical bowel preparation before elective colorectal surgery: a randomized trial. Dis Colon Rectum. (2006) 49(1):109–12. doi: 10.1007/s10350-005-0215-5
42. Sun Z, Honar H, Sessler DI, Dalton JE, Yang D, Panjasawatwong K, et al. Intraoperative core temperature patterns, transfusion requirement, and hospital duration in patients warmed with forced air. Anesthesiology. (2015) 122(2):276–85. doi: 10.1097/ALN.0000000000000551
43. Ribeiro E, Ferreira RC, Montanari FL, Botelho M, Correia MDL, Duran ECM. Conceptual and operational definition of the components of the nursing diagnosis hypothermia (00006) in the perioperative period. Rev Bras Enferm. (2021) 74(2):e20190684. doi: 10.1590/0034-7167-2019-0684
44. Kati B, Buyukfirat E, Pelit ES, Yagmur I, Demir M, Albayrak IH, et al. Percutaneous nephrolithotomy with different temperature irrigation and effects on surgical complications and anesthesiology applications. J Endourol. (2018) 32(11):1050–3. doi: 10.1089/end.2018.0581
45. Ruetzler K, Kurz A. Consequences of perioperative hypothermia. Handb Clin Neurol. (2018) 157:687–97. doi: 10.1016/B978-0-444-64074-1.00041-0
46. Ljungqvist O, Scott M, Fearon KC. Enhanced recovery after surgery: a review. JAMA Surg. (2017) 152(3):292–8. doi: 10.1001/jamasurg.2016.4952
47. Wu H, Ding T, Yan S, Huang Z, Zhang H. Risk factors for moderate-to-severe postoperative pain after percutaneous nephrolithotomy: a retrospective cohort study. Sci Rep. (2022) 12(1):8366. doi: 10.1038/s41598-022-12623-5
48. Nimmo SM, Foo ITH, Paterson HM. Enhanced recovery after surgery: pain management. J Surg Oncol. (2017) 116(5):583–91. doi: 10.1002/jso.24814
49. Isac W, Rizkala E, Liu X, Noble M, Monga M. Tubeless percutaneous nephrolithotomy: outcomes with expanded indications. Int Braz J Urol. (2014) 40(2):204–11. doi: 10.1590/S1677-5538.IBJU.2014.02.10
50. Etemadian M, Soleimani MJ, Haghighi R, Zeighami MR, Najimi N. Does bleeding during percutaneous nephrolithotomy necessitate keeping the nephrostomy tube? A randomized controlled clinical trial. Urol J. (2011) 8(1):21–6. Available from: https://journals.sbmu.ac.ir/urolj/index.php/uj/article/view/927/527.21404198
51. Wollin DA, Lipkin ME. Emerging technologies in ultrasonic and pneumatic lithotripsy. Urol Clin North Am. (2019) 46(2):207–13. doi: 10.1016/j.ucl.2018.12.006
52. Karalar M, Tuzel E, Keles I, Okur N, Sarici H, Ates M. Effects of parenchymal thickness and stone density values on percutaneous nephrolithotomy outcomes. Med Sci Monit. (2016) 22:4363–8. doi: 10.12659/msm.898212
53. Bartoletti R, Cai T, Mondaini N, Melone F, Travaglini F, Carini M, et al. Epidemiology and risk factors in urolithiasis. Urol Int. (2007) 79(Suppl 1):3–7. doi: 10.1159/000104434
Keywords: patient-centered, eras, PCNL, staghorn, recurrence
Citation: Lei J, Huang K, Dai Y and Yin G (2023) Evaluating outcomes of patient-centered enhanced recovery after surgery (ERAS) in percutaneous nephrolithotomy for staghorn stones: An initial experience. Front. Surg. 10:1138814. doi: 10.3389/fsurg.2023.1138814
Received: 6 January 2023; Accepted: 3 March 2023;
Published: 21 March 2023.
Edited by:
Luigi Schips, University of Studies G. d'Annunzio Chieti and Pescara, ItalyReviewed by:
Panagiotis Mourmouris, National and Kapodistrian University of Athens, Greece© 2023 Lei, Huang, Dai and Yin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Guangming Yin eWluZ2dtNzVAMTI2LmNvbQ==
Specialty Section: This article was submitted to Genitourinary Surgery, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.