
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Surg. , 13 February 2023
Sec. Thoracic Surgery
Volume 10 - 2023 | https://doi.org/10.3389/fsurg.2023.1118477
This article is part of the Research Topic Current Trends in Endoscopic Thoracic Surgery: Insights From the XXI SIET National Meeting View all 18 articles
 Riccardo Orlandi1*
Riccardo Orlandi1* Federico Raveglia2
Federico Raveglia2 Matteo Calderoni2Enrico Mario Cassina2
Matteo Calderoni2Enrico Mario Cassina2 Ugo Cioffi3
Ugo Cioffi3 Angelo Guttadauro4Lidia Libretti2Emanuele Pirondini2Arianna Rimessi2Antonio Tuoro2Eliseo Passera2
Angelo Guttadauro4Lidia Libretti2Emanuele Pirondini2Arianna Rimessi2Antonio Tuoro2Eliseo Passera2
Tracheal stenosis (TS) is a debilitating disease promoted by pathologic narrowing of the trachea. The acute respiratory distress syndrome caused by COVID-19 has been demonstrated to trigger enhanced inflammatory response and to require prolonged invasive mechanical ventilation as well as high frequency of re-intubation or emergency intubation, thus increasing the rate and complexity of TS. The standard-of-care of COVID-19-related tracheal complications has yet to be established and this is a matter of concern. This review aims at collecting latest evidence on this disease, providing an exhaustive overview on its distinctive features and open issues, and investigating different diagnostic and therapeutic strategies to handle COVID-19-induced TS, focusing on endoscopic versus open surgical approach. The former encompasses bronchoscopic procedures: electrocautery or laser-assisted incisions, ballooning dilation, submucosal steroid injection, endoluminal stenting. The latter consists of tracheal resection with end-to-end anastomosis. As a rule, traditionally, the endoscopic management is restricted to short, low-grade, and simple TS, whereas the open techniques are employed in long, high-grade, and complex TS. However, the critical conditions or extreme comorbidities of several COVID-19 patients, as well as the marked inflammation in tracheal mucosa, have led some authors to apply endoscopic management also in complex TS, recording acceptable results. Although severe COVID-19 seems to be an issue of the past, its long-term complications are still unknown and considering the increased rate and complexity of TS in these patients, we strongly believe that it is worth to focus on it, attempting to find the best management strategy for COVID-19-related TS.
Tracheal stenosis (TS) is an invalidating disease characterized by emphasized tissue fibrotic reaction leading to pathologic narrowing of the trachea (1). Traditionally, iatrogenic intubation injury, prolonged intubation or tracheostomy are the most frequent causes of TS (2). Other causes include local radiotherapy, inflammatory or autoimmune diseases, idiopathic, and neoplastic diseases. Coronavirus Disease 2019 (COVID-19) has been reported to be strictly related to TS. Indeed, longer times of invasive ventilation and differed tracheostomy to promote prone position as well as higher rates of iatrogenic intubation injuries have resulted in significant rise in rate and complexity of TS in patients with severe COVID-19 (3). Experiences on COVID-19-related TS are still limited and there is lack of publications in literature on this topic: its best management has not been yet clearly established. Therefore, we performed a review to provide a brief but exhaustive overview on this relatively new disease, focusing on its distinctive features and open issues.
Rate of TS following endotracheal intubation is estimated from 10% to 22%, but only 1%–2% of cases will complain severe dyspnea (4, 5), with reported incidence of 4.9 cases per million per year (6). During the pandemic, almost half of COVID-19 patients in ICU required invasive mechanical ventilation, with mean duration of 17 days and high rate of reintubation (7). The exact number of intubated COVID-19 patients developing TS is unknown, but its incidence is reported to widely range from 3.3% (8) to 40% (9, 10). The raw incidence of TS seems to be higher in COVID-19 patients than in pre-COVID-19 era (11), and the medical community has been alerted to the possibility of an unprecedented surge in TS (12), despite the limited number of cases in literature does not allow to draw definitive conclusions in this regard. The mean age ranges from 50 (13–15) to 60 (8, 11, 16) years old, and males seem to be more prone to develop this disease, with approximately prevalence of 60%–70% (8, 11, 13, 14, 16, 17).
Risk factors could be divided into patient-related versus mechanical. The formers include patient's comorbidities, poor health conditions, history of diabetes, lower levels of PaO2/FiO2 and increased hypoxia (10), obesity, severe inflammation as well as microbial dysregulation of the airways (11, 16), COVID-19-related laryngitis and laryngeal edema (14), disrupted laryngotracheal microcirculation due to prothrombotic and antifibrinolytic state, high viral replication in the tracheal epithelium (11) leading to viral tracheitis (18). Instead, the latters consist of iatrogenic lesions during intubation due to poor visibility and chaotic situations, cuff overinflation to avoid aerosol sprays, prolonged intubation, high rate of reintubation, prone position ventilation with movement of the tube, delayed tracheostomy to allow prone position and viral clearance (11), vasopressor use (8), high-dose corticosteroid resulting in mucosal atrophy and altered healing, impaired nursing service due to workload of pandemics.
TS is a pathological narrowing of the trachea, typically occurring in the upper half, at the cuff or, less frequently, at the stomal site, because of mispositioning of tracheostomy or high placement of endotracheal tube. The extension is variable. In 1965 Cooper and Grillo (19) explained the reason, by performing tracheal autoptic evaluation on 30 patients who died during invasive ventilation. The macro and microscopic examination revealed a pattern of damage to the tracheal wall at the cuff site: mucosal hemorrhage or ulceration, necrosis and dissolution of adjacent cartilaginous rings, up to scarring fibrosis. Pathophysiologic basis of this phenomenon must be searched in pressure of the cuff. Cuff pressure of endotracheal tube above the capillary perfusion pressure of tracheal mucosa ranging from 20 to 30 mmHg leads to mucosal ischemia, which, if prolonged, results in submucosal damages (20). Ongoing compression causes injury to cartilaginous rings, which are usually fed by diffusion from mucosa and sub-mucosa. Once full epithelium's depth is interested by ischemic injury, healing can no longer rely on epithelium regeneration, but it requires collagen deposition, leading to scarring (21). On the other hand, the examination of tracheal wall at the stomal site revealed granulation tissue along the stoma and the loss of support of anterior cartilaginous arch because of too large stoma or enlargement by leverage of endotracheal tube (19). Ultimately, whatever the origin, TS is mediated by pathologic deposition of collagen in the upper airway, which is triggered by fibroblasts: several cytokines have been reported to promote the profibrotic myofibroblast phenotype observed in TS (22), such as interleukin IL-1, IL-6, IL-13, fibroblast growth factor (FGF), tumor necrosis factor α (TNF-α) and transforming growth factor β (TGF-β). All these cytokines have been demonstrated to be elicited by COVID-19 (23). Recently, some Authors (11, 15) have described microscopic findings of tracheal samples in COVID-19 patients affected by TS, highlighting patchy coagulative necrosis of the epithelium, granulation tissue, extensive presence of lymphocytes, multinucleated giant cells, non-fistulized abscesses leading to cartilage lysis, as well as thrombotic vessels and lymphocytic microvasculitis. Interestingly, cells with viral cytopathic involvement have been identified (11), and viral particles in tracheal epithelial cells have been detected (24), which could support the pathogenetic role of viral tracheitis theorized by Ershadi and colleagues (18). Moreover, Roncati and colleagues (25) have recently reported, by immunohistochemistry, a high density of IgG4-secreting plasma cells on fibrotic tissue from resected tracheal samples in patients affected by COVID-19-related TS. According to Stratakos and colleagues (16), severe COVID-19 could trigger massive Th2 response, which has already been demonstrated to mediate development of TS (22), by inducing localized IgG4 overproduction with resulting fibrosis and scarring in the upper airway.
Symptoms can widely vary depending on site and extension of airway stenosis (8): occlusive TS localized within 2–3 cm from vocal cords will occur during the hospitalization with difficulties in extubating the patient or weaning tracheostomy; whereas progressive TS localized beyond 3 cm from vocal cords will show up with progressive shortness of breath after discharging. Manifestations will also depend on the degree of obstruction, which in turn influences airflow rate and pressure changes (8, 17): mild stenosis (<50%) will be broadly asymptomatic since the pressure at the stenosis is comparable to that at the glottic plane; moderate stenosis (51%–70%) will result in fluctuating symptoms, based on significant pressure drop manifesting under exertion or other contexts requiring higher airflow rate; severe stenosis (>71%) will produce symptoms even at rest, due to massive pressure drop. The typical presentation consists of dyspnea, wheezing and stridor on physical examination occurring after several days from extubating (8, 9, 14). Symptoms may include dysphonia and communication difficulties (22), hoarseness, dry cough, and swallowing problems (12). Symptoms can occur immediately after extubating or they can be delayed up to 6 months or even within a few years from ventilation weaning (26). TS at the stomal site could be more subtle and less rapidly progressive, leading to functional impairment up to years or even decades later (8). COVID-19-related TS has more severe clinical presentations than other TS because of more complex stenotic airway segments (11) and delayed diagnosis, since symptoms of TS could be initially misdiagnosed as post-COVID-19 respiratory symptoms (16, 17). Whatever the symptoms, without proper management, TS can lead to life-threatening situations due to impaired respiratory function (22).
Clinically, TS are divided into simple (or web-like) and complex stenosis: the formers are less than 1 cm long circumferential stenosis, without any cartilage involvement; the latters are more than 1 cm long articulated and mixed stenosis, with involvement of cartilage (17). TS could potentially affect each segment of the trachea. The majority of COVID-19-related TS is complex (8, 13, 16), with higher incidence of associated tracheomalacia, vocal cord paralysis and tracheoesophageal fistula (13), and localized in the upper third segment (8, 13, 14, 17). The stenotic segment is highly variable in extension, but it is most reported as around 2 cm long (8, 11, 13, 16). The most critical factor in TS is assessing tracheal width in the stenotic segment, which is graded according to Cotton-Myer Classification System, based on endoscopic tracheal evaluation (27): I, cross sectional area (CSA) obstruction <50%; II, CSA obstruction 51%–70%; III, CSA obstruction 71%–99%; IV complete obstruction without detectable lumen. Most patients with COVID-19-related TS are graded III (8, 13, 14). Appropriate diagnostic investigations are mandatory to properly classify the TS and to subsequently tailor the best treatment option for each patient: an accurate physical examination, a thorough radiologic assessment and an extensive endoscopic evaluation are the pillars of an adequate preoperative workup (12). The use of laryngoscopy or flexible bronchoscopy is of utmost importance, enabling to gather several dynamic details on vocal mobility, swallowing function, local inflammation, localization, extent and degree of TS, presence of airway lesions, malacic or scar tissue. Endoscopy is the gold standard and should always be performed. CT scan (more rarely MRI) of the trachea can be highly relevant and complementary, mainly in case of complete TS obstruction, providing the possibility to measure extent and narrowing of TS, or in case of suspected laryngo-tracheal framework alteration. In case of apparent TS, a thorough airway evaluation under general anesthesia should be considered. Pulmonary functions should be multidisciplinary assessed, through routine lung function tests, differentiating TS from other respiratory diseases (12).
The optimal management of TS is still a matter of debate, irrespective of the disease which led to invasive ventilation, and clear guidelines on the best treatment option are still demanded, even more so in COVID-19-related TS. Table 1 gathers main case-series studies available in literature on this topic. Currently, treatment of this disease must be personalized, based on patient's clinical conditions and morbidities, and on anatomic characteristics of the stenotic segment. An early specialistic referral and thorough clinical, radiologic, and endoscopic evaluation are mandatory to plan the best therapeutic management. Main treatment options are endoscopic versus surgical procedures. As a rule, endoscopic approach is recommended as first-line definitive treatment in shorter than 2 cm, low-graded intrinsic and well localized TS, or in heavily comorbid patients on poor general conditions, otherwise it is suggested as bridge therapy for definitive surgery. On the other hand, surgery is recommended in longer than 2 cm, high-graded, complex TS, extended to different segments or associated with malacia, altered laryngo-tracheal framework, as well as in case of unsuccessful multiple endoscopic attempts (12). Another available therapeutic option is the tracheostomy, which should be reserved to selected cases. Indeed, the right planning of the treatment procedure would avoid a tracheostomy or redo-tracheostomy with further tracheal damages; anyway, if needed, tracheostomy should be performed into the stenotic or affected segment not to injury healthy tracheal segments (12), through either open or percutaneous techniques, since they have shown to have comparable results in terms of perioperative mortality and morbidity rates in general population (34), and there are no current evidences on the preferable approach to adopt in COVID-19 patients (35). Eventually, treatment options for COVID-19-related TS are like those adopted for any-causes TS (31).
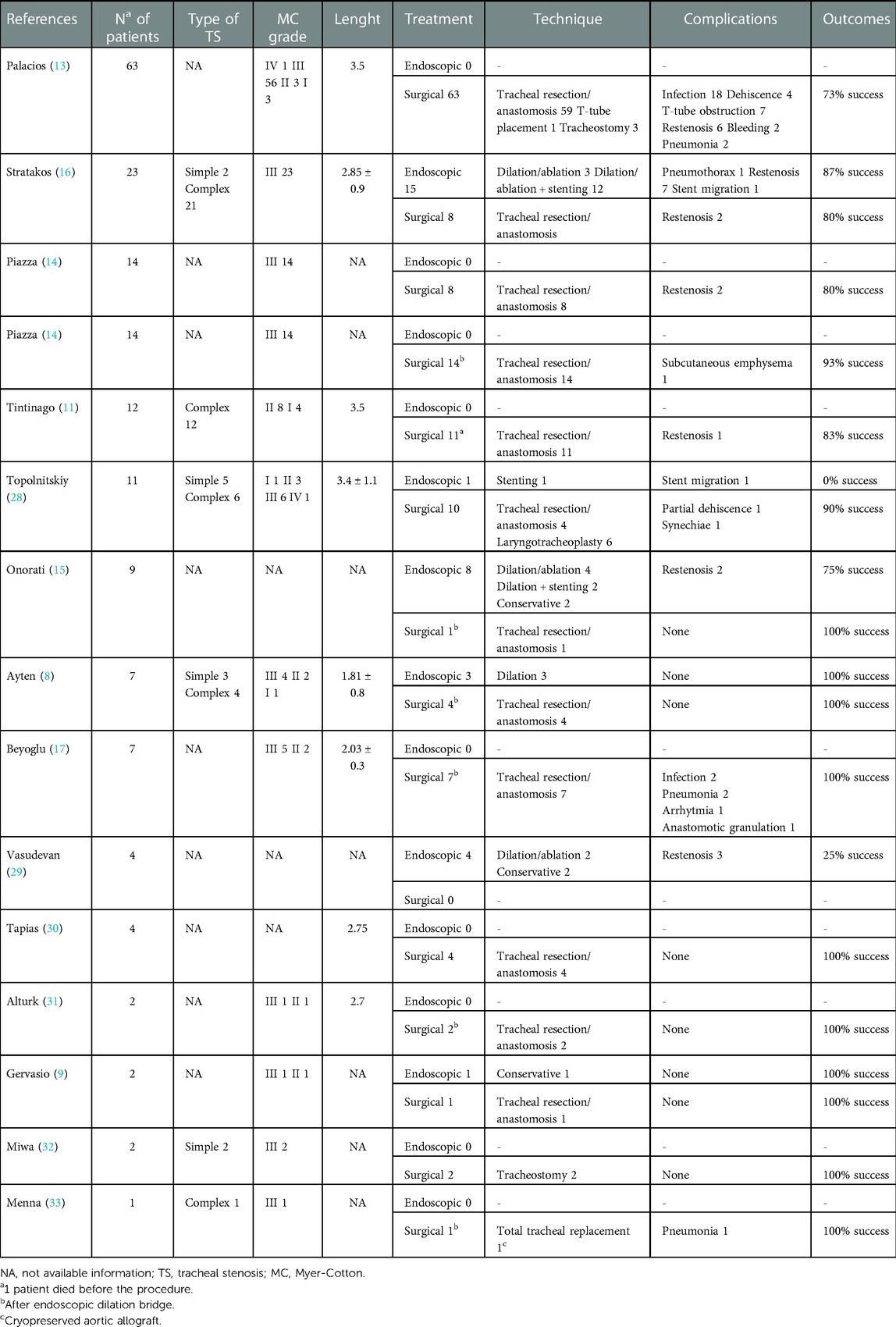
Table 1. Main studies reporting the management of COVID-19-related tracheal stenosis.
Conservative procedures consist of rigid bronchoscopy with tracheal dilation by ballooning or mucosal resection through electrocautery, cryoablation or laser, resection of granulation tissue, stenting, intralesional mucosal steroid injection (12). The best endoscopic technique, which could be variably combined, depends on experience of the center and on type of TS. Onorati and colleagues (15) favor endoscopic treatment in COVID-19-related TS, mainly in case of persistent local inflammation of the trachea, reporting encouraging results through bronchoscopic procedures (balloon dilation, stenting, and resection of granuloma) on 8 patients, with 75% success and 25% complication rates. Ayten and colleagues (8) showed 100% success rate in patients affected by simple TS undergoing 1–3 bronchoscopy dilation procedures; they suggest applying endoscopic procedures as first-line therapy in web-like TS smaller than 1 cm and without malacia. Mattioli and colleagues (3) suggest to avoide surgery as primary choice in COVID-19 patients, because of their heavy comorbidities and debilitated conditions, proposing to use balloon dilation procedures with intralesional corticosteroid injection, even in case of complex TS, particularly in “young and thin” stenosis, allowing to heal some patients, or at least to buy time delaying surgery to gain better clinical conditions. Indeed, according to authors supporting conservative treatments, surgical procedures should be reserved to selected fit patients without significative comorbidities (3). Stratakos and colleagues (16) reported 88% success rate after endoscopic dilation and silicon stenting in 15 patients, with 60% complication rate mainly related to stent obstruction due to mucous accumulation and pseudomembranous. Tracheal resection and anastomosis are contraindicated in TS longer than 5–6 cm (8, 14, 31), because of the marked increase in anastomotic complications, and in such contexts, endoscopy could be considered with salvage intent before performing definitive tracheostomy or Montgomery T-tube placement. Since patients could relapse after endoscopic management, it is advisable to strictly follow-up them: they are thought to require an overage of 3.5 review flexible bronchoscopy procedures within the first 6 months (16). Medical therapy with antibiotics and intravenous steroid injection can be considered as ancillary: some authors (9, 15) reported clinical improvement and successful discharge of patients without further need for invasive procedures.
Surgical approaches include right thoracotomy, cervicotomy, cervical collar T-incision with or without manubrium split, median sternotomy, depending on experience of the center and localization of the stenotic segment. Whatever the chosen approach, the tracheal stenotic segment must be released, the damaged rings are removed, then end-to-end anastomosis is performed with 3–0 monofilament sutures by continuous as well as interrupted sutures (36). Traditionally, tracheal resection with end-to-end anastomosis is considered the gold standard treatment in TS (11), even if there are no specific guidelines. Several authors (8, 11–14, 17, 31) believe that surgical treatment is the standard of care also in COVID-19-related TS, especially in complex and articulated stenosis with cartilaginous involvement. In these cases, some authors (8, 13) consider endoscopic procedures even contraindicated, since the high rate of recurrence and the potential increase of the injured segment could decrease the chance of successful surgery. Others (11, 14, 31) rather suggest performing bronchoscopic dilation preoperatively in symptomatic patients as a bridge to definitive surgery, also in reiterated sessions. Concerning the timing of surgery, prevailing indication is to repair TS as early as possible, after the patient has tested negative for SARS-CoV-2 and as soon as he has recovered from the hospitalization (11, 17), if local inflammation is off and chronic steroid course can be discontinued to avoid anastomotic healing complications (15). Beyoglu and colleagues (17) propose to consider the time elapsed between the dilating procedure and the recurrence of symptoms to choose the right timing for surgical procedure: surgery should be planned if the time span between two consecutive sessions is less than 2 weeks. Different studies have reported complication rate of 15%–45% after tracheal resection and anastomosis for any-causes TS (37). Regarding COVID-19-related TS, complication rates range from less than 15% (8, 14) to over 40% (13, 17), whereas the reported success rate is around 80% (11, 13, 16), with 30-day mortality rate of 0%. In case of TS recurrence after surgery, which is reported to occur in 10%–20% of patients (13, 14, 16), dilating rigid bronchoscopy and eventually stenting is indicated as second-line treatments; in case of further failure definitive tracheostomy or Montgomery T-tube placement must be considered.
To prevent COVID-19-related TS, the most critical element is to carefully manage mechanical risk factors listed above, especially choosing the appropriate endotracheal tube for each patient and strictly monitoring cuff pressure (17). The quality of care in COVID-19 has significantly improved since start of the pandemic, and this should slow down the presumed increase in TS rate. Anyway, an early diagnosis is of utmost importance, and therefore each patient with medical history of COVID-19-related invasive ventilation should be clinically, radiologically, and eventually endoscopically followed up to early detect any signs of TS (10, 12), suspecting TS in case of breathing distress after mechanical ventilation weaning (31). Topical or systemic use of steroids, as well as antibiotics and anti-inflammatory drugs, together with early endoscopic dilation and local debridement, could avoid progression to major TS (12).
COVID-19-related TS may become a relevant pathology within the next few years: it has distinctive features which differentiate it from other-causes TS, and it is worth to hold attention on its development. An early diagnosis is fundamental, and it is based on clinical, radiological, and endoscopic investigations. Patients diagnosed with COVID-19-related TS should be referred to experienced tertiary centers. Treatment should be personalized and tailored on each patient, through multidisciplinary discussion. Therapeutic options consist of endoscopic or surgical procedures, which could provide high success and low complication rates when performed on selected patient in right timing.
RO, FR, and ElP contributed to conception and design of the study. RO and ElP wrote the first draft of the manuscript. RO, FR, ElP wrote sections of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
and Acronyms TS, tracheal stenosis; COVID-19, coronavirus disease 2019; ICU, intensive care unit; CSA, cross sectional area.
1. Grillo HC. The management of tracheal stenosis following assisted respiration. J Thorac Cardiovasc Surg. (1969) 57(1):52–71. doi: 10.1016/S0022-5223(19)42762-1
2. Cooper JD, Grillo HC. The evolution of tracheal injury due to ventilatory assistance through cuffed tubes: a pathologic study. Ann Surg. (1969) 169(3):334–48. doi: 10.1097/00000658-196903000-00007
3. Mattioli F, Marchioni A, Andreani A, Cappiello G, Fermi M, Presutti L. Post-intubation tracheal stenosis in COVID-19 patients. Eur Arch Otorhinolaryngol. (2021) 278(3):847–8. doi: 10.1007/s00405-020-06394-w
4. Goldenberg D, Ari EG, Golz A, Danino J, Netzer A, Joachims HZ. Tracheotomy complications: a retrospective study of 1130 cases. Otolaryngol Head Neck Surg. (2000) 123(4):495–500. doi: 10.1067/mhn.2000.105714
5. Li M, Yiu Y, Merrill T, Yildiz V, deSilva B, Matrka L. Risk factors for posttracheostomy tracheal stenosis. Otolaryngol Head Neck Surg. (2018) 159(4):698–704. doi: 10.1177/0194599818794456
6. Nouraei SA, Ma E, Patel A, Howard DJ, Sandhu GS. Estimating the population incidence of adult post-intubation laryngotracheal stenosis. Clin Otolaryngol. (2007) 32(5):411–2. doi: 10.1111/j.1749-4486.2007.01484.x
7. Möhlenkamp S, Thiele H. Ventilation of COVID-19 patients in intensive care units. Herz. (2020) 45(4):329–31. doi: 10.1007/s00059-020-04923-1
8. Ayten O, Iscanli IGE, Canoglu K, Ozdemir C, Saylan B, Caliskan T, et al. Tracheal stenosis after prolonged intubation due to COVID-19. J Cardiothorac Vasc Anesth. (2022) 36(8 Pt B):2948–53. doi: 10.1053/j.jvca.2022.02.009
9. Gervasio CF, Averono G, Robiolio L, Bertoletti M, Colageo U, De Col L, et al. Tracheal stenosis after tracheostomy for mechanical ventilation in COVID-19 pneumonia: a report of 2 cases from northern Italy. Am J Case Rep. (2020) 21:e926731. doi: 10.12659/AJCR.926731
10. Fiacchini G, Tricò D, Ribechini A, Forfori F, Brogi E, Lucchi M, et al. Evaluation of the incidence and potential mechanisms of tracheal complications in patients with COVID-19. JAMA Otolaryngol Head Neck Surg. (2021) 147(1):70–6. doi: 10.1001/jamaoto.2020.4148
11. Tintinago LF, Victoria W, Escobar Stein J, Gonzales LF, Fernandez MI, Candelo E. Laryngotracheal stenoses post-acute respiratory distress syndrome due to COVID-19: clinical presentation, histopathological findings and management. A series of 12 cases. Indian J Otolaryngol Head Neck Surg. (2022) 74(Suppl 2):3262–7. doi: 10.1007/s12070-022-03076-3
12. Piazza C, Filauro M, Dikkers FG, Nouraei SAR, Sandu K, Sittel C, et al. Long-term intubation and high rate of tracheostomy in COVID-19 patients might determine an unprecedented increase of airway stenoses: a call to action from the European laryngological society. Eur Arch Otorhinolaryngol. (2021) 278(1):1–7. doi: 10.1007/s00405-020-06112-6
13. Palacios JM, Bellido DA, Valdivia FB, Ampuero PA, Figueroa CF, Medina C, et al. Tracheal stenosis as a complication of prolonged intubation in coronavirus disease 2019 (COVID-19) patients: a Peruvian cohort. J Thorac Dis. (2022) 14(4):995–1008. doi: 10.21037/jtd-21-1721
14. Piazza C, Lancini D, Filauro M, Sampieri C, Bosio P, Zigliani G, et al. Post-COVID-19 airway stenosis treated by tracheal resection and anastomosis: a bicentric experience. Acta Otorhinolaryngol Ital. (2022) 42(2):99–105. doi: 10.14639/0392-100X-N1952
15. Onorati I, Bonnet N, Radu DM, Freynet O, Guiraudet P, Kambouchner M, et al. Case report: laryngotracheal post-intubation/tracheostomy stenosis in COVID-19 patients. Front Surg. (2022) 9:874077. doi: 10.3389/fsurg.2022.874077
16. Stratakos G, Anagnostopoulos N, Alsaggaf R, Koukaki E, Bakiri K, Emmanouil P, et al. COVID-19 patients presenting with post-intubation upper airway complications: a parallel epidemic? J Clin Med. (2022) 11(6):1719. doi: 10.3390/jcm11061719
17. Beyoglu MA, Sahin MF, Turkkan S, Yazicioglu A, Yekeler E. Complex post-intubation tracheal stenosis in COVID-19 patients. Indian J Surg. (2022) 84(4):805–13. doi: 10.1007/s12262-022-03498-x
18. Ershadi R, Rafieian S, Sarbazzadeh J, Vahedi M. Tracheal stenosis following mild-to-moderate COVID-19 infection without history of tracheal intubation: a case report. Gen Thorac Cardiovasc Surg. (2022) 70(3):303–7. doi: 10.1007/s11748-021-01747-6
19. Cooper JD. Tracheal injuries complicating prolonged intubation and tracheostomy. Thorac Surg Clin. (2018) 28(2):139–44. doi: 10.1016/j.thorsurg.2018.01.001
20. Sultan P, Carvalho B, Rose BO, Cregg R. Endotracheal tube cuff pressure monitoring: a review of the evidence. J Perioper Pract. (2011) 21(11):379–86. doi: 10.1177/175045891102101103
21. Delaere P, De Leyn P. Surgical anatomy of the trachea and techniques of resection and reconstruction. In: LoCicero J 3rd, Feins RH, Colson YL, Rocco G, editors. Shields’ general thoracic surgery, 8th ed. Philadelphia: Wolters Kluwer (2019). p. 1782–811.
22. Davis RJ, Hillel AT. Inflammatory pathways in the pathogenesis of iatrogenic laryngotracheal stenosis: what do we know? Transl Cancer Res. (2020) 9(3):2108–16. doi: 10.21037/tcr.2020.01.21
23. Hasanvand A. COVID-19 and the role of cytokines in this disease. Inflammopharmacology. (2022) 30(3):789–98. doi: 10.1007/s10787-022-00992-2
24. Bradley BT, Maioli H, Johnston R, Chaudhry I, Fink SL, Xu H, et al. Histopathology and ultrastructural findings of fatal COVID-19 infections in Washington state: a case series. Lancet. (2020) 396(10247):320–32. doi: 10.1016/S0140-6736(20)31305-2
25. Roncati L, Bergonzini G, Lusenti B, Nasillo V, Paolini A, Zanelli G, et al. High density of IgG4-secreting plasma cells in the fibrotic tissue from a surgically resected tracheal ring impaired by complex subglottic stenosis post-tracheostomy as immune expression of a Th2 response due to severe COVID-19. Ann Hematol. (2021) 100(10):2659–60. doi: 10.1007/s00277-020-04231-y
26. Stoelben E, Koryllos A, Beckers F, Ludwig C. Benign stenosis of the trachea. Thorac Surg Clin. (2014) 24(1):59–65. doi: 10.1016/j.thorsurg.2013.09.001
27. Myer CM 3rd, O'Connor DM, Cotton RT. Proposed grading system for subglottic stenosis based on endotracheal tube sizes. Ann Otol Rhinol Laryngol. (1994) 103(4 Pt 1):319–23. doi: 10.1177/000348949410300410
28. Topolnitskiy E, Chekalkin T, Marchenko E, Volinsky A. Treatment of post-resuscitation cicatricial tracheal stenosis after suffering severe COVID-19 associated pneumonia: a report of 11 cases. Respir Med Case Rep. (2022) 40:101768. doi: 10.1016/j.rmcr.2022.101768
29. Vasudevan A, Achu R, Perry A, Yarrington C, Norris M, Tracy L, et al. Impact of pregnancy on airway complications after intubation for COVID-19 infection: a case series. Am J Otolaryngol. (2022) 43(5):103522. doi: 10.1016/j.amjoto.2022.103522
30. Tapias LF, Lanuti M, Wright CD, Hron TA, Ly A, Mathisen DJ, et al. COVID-19-related post-intubation tracheal stenosis: early experience with surgical treatment. Ann Surg. (2022) 275(1):e271–3. doi: 10.1097/SLA.0000000000004884
31. Alturk A, Bara A, Darwish B. Post-intubation tracheal stenosis after severe COVID-19 infection: a report of two cases. Ann Med Surg. (2021) 67:102468. doi: 10.1016/j.amsu.2021.102468
32. Miwa M, Nakajima M, Kaszynski R H, Hamada S, Nakano T, Shirokawa M, et al. Two cases of post-intubation laryngotracheal stenosis occurring after severe COVID-19. Intern Med. (2021) 60(3):473–7. doi: 10.2169/internalmedicine.6105-20
33. Menna C, Andreetti C, Ibrahim M, Ciccone AM, D'Andrilli A, Maurizi G, et al. Successful total tracheal replacement by cryopreserved aortic allograft in a patient post-COVID-19 infection. Chest. (2021) 160(6):e613–7. doi: 10.1016/j.chest.2021.08.037
34. Johnson-Obaseki S, Veljkovic A, Javidnia H. Complication rates of open surgical versus percutaneous tracheostomy in critically ill patients. Laryngoscope. (2016) 126(11):2459–67. doi: 10.1002/lary.26019
35. David AP, Russell MD, El-Sayed IH, Russell MS. Tracheostomy guidelines developed at a large academic medical center during the COVID-19 pandemic. Head Neck. (2020) 42(6):1291–6. doi: 10.1002/hed.26191
36. Delaere P, De Leyn P. Surgical anatomy of the trachea and techniques of resection and reconstruction. In: LoCicero J 3rd, Feins RH, Colson YL, Rocco G, editors. Shields’ general thoracic surgery, 8th ed. Philadelphia: Wolters Kluwer (2019). p. 1782–811.
Keywords: tracheal stenosis, thoracic surgery, endoscopic thoracic surgery, COVID-19, tracheal procedures
Citation: Orlandi R, Raveglia F, Calderoni M, Cassina EM, Cioffi U, Guttadauro A, Libretti L, Pirondini E, Rimessi A, Tuoro A and Passera E (2023) Management of COVID-19 related tracheal stenosis: The state of art. Front. Surg. 10:1118477. doi: 10.3389/fsurg.2023.1118477
Received: 7 December 2022; Accepted: 24 January 2023;
Published: 13 February 2023.
Edited by:
Alex Volinsky, University of South Florida, United StatesReviewed by:
Dania Nachira, Agostino Gemelli University Polyclinic (IRCCS), Italy© 2023 Orlandi, Raveglia, Calderoni, Cassina, Cioffi, Guttadauro, Libretti, Pirondini, Rimessi, Tuoro and Passera. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Riccardo Orlandi cmljY2FyZG8ub3JsYW5kaUB1bmltaS5pdA==
Specialty Section: This article was submitted to Thoracic Surgery, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.